Embed Size (px)
Citation preview
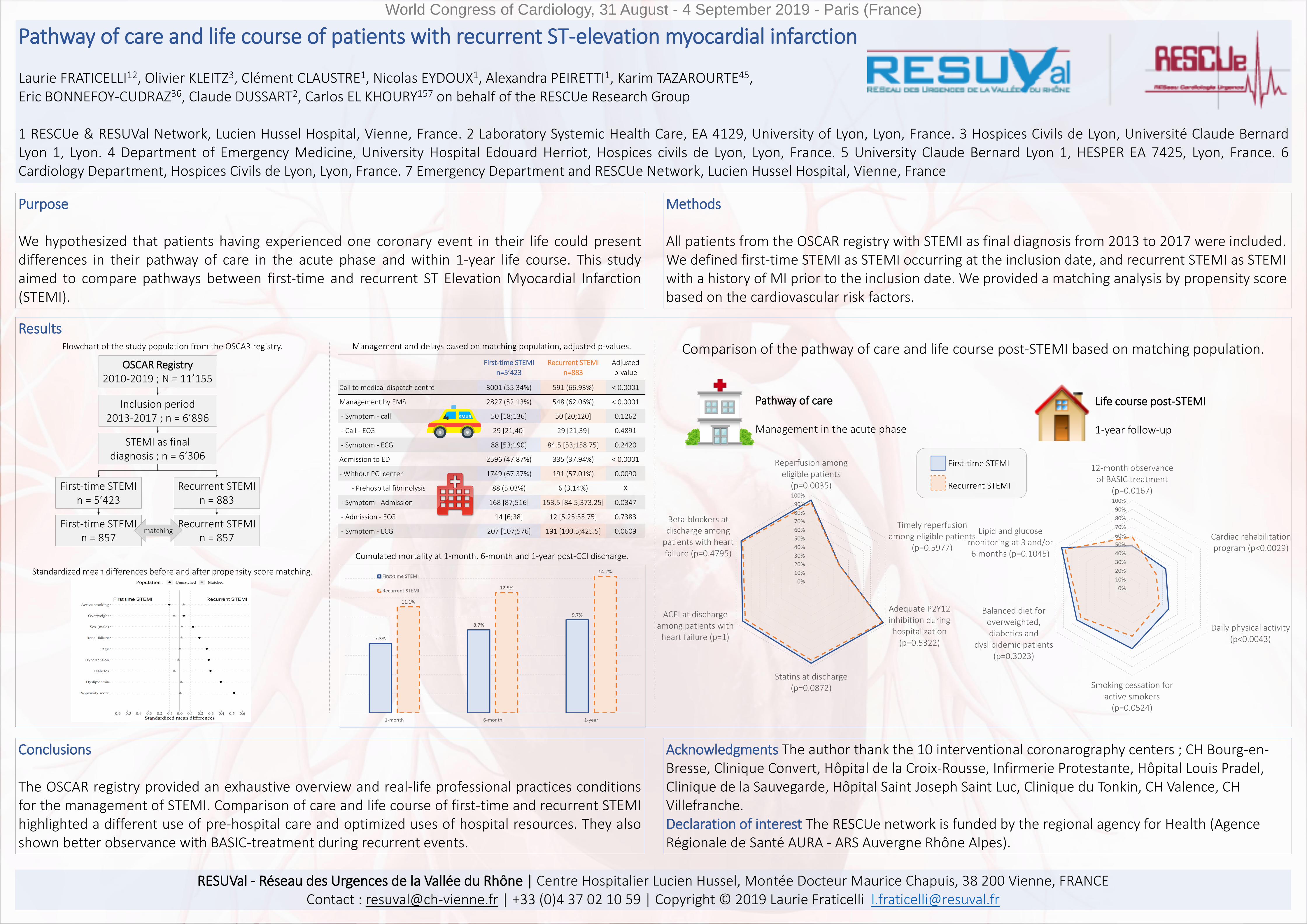
Pathway of care and life course of patients with recurrent ST-elevation myocardial infarction
Laurie FRATICELLI12, Olivier KLEITZ3, Clément CLAUSTRE1, Nicolas EYDOUX1, Alexandra PEIRETTI1, Karim TAZAROURTE45, Eric BONNEFOY-CUDRAZ36, Claude DUSSART2, Carlos EL KHOURY157 on behalf of the RESCUe Research Group
1 RESCUe & RESUVal Network, Lucien Hussel Hospital, Vienne, France. 2 Laboratory Systemic Health Care, EA 4129, University of Lyon, Lyon, France. 3 Hospices Civils de Lyon, Université Claude BernardLyon 1, Lyon. 4 Department of Emergency Medicine, University Hospital Edouard Herriot, Hospices civils de Lyon, Lyon, France. 5 University Claude Bernard Lyon 1, HESPER EA 7425, Lyon, France. 6Cardiology Department, Hospices Civils de Lyon, Lyon, France. 7 Emergency Department and RESCUe Network, Lucien Hussel Hospital, Vienne, France
Purpose
We hypothesized that patients having experienced one coronary event in their life could presentdifferences in their pathway of care in the acute phase and within 1-year life course. This studyaimed to compare pathways between first-time and recurrent ST Elevation Myocardial Infarction(STEMI).
World Congress of Cardiology, 31 August - 4 September 2019 - Paris (France)
Methods
All patients from the OSCAR registry with STEMI as final diagnosis from 2013 to 2017 were included. We defined first-time STEMI as STEMI occurring at the inclusion date, and recurrent STEMI as STEMI with a history of MI prior to the inclusion date. We provided a matching analysis by propensity score based on the cardiovascular risk factors.
Results
Conclusions
The OSCAR registry provided an exhaustive overview and real-life professional practices conditionsfor the management of STEMI. Comparison of care and life course of first-time and recurrent STEMIhighlighted a different use of pre-hospital care and optimized uses of hospital resources. They alsoshown better observance with BASIC-treatment during recurrent events.
Acknowledgments The author thank the 10 interventional coronarography centers ; CH Bourg-en-Bresse, Clinique Convert, Hôpital de la Croix-Rousse, Infirmerie Protestante, Hôpital Louis Pradel, Clinique de la Sauvegarde, Hôpital Saint Joseph Saint Luc, Clinique du Tonkin, CH Valence, CH Villefranche. Declaration of interest The RESCUe network is funded by the regional agency for Health (AgenceRégionale de Santé AURA - ARS Auvergne Rhône Alpes).
OSCAR Registry2010-2019 ; N = 11’155
Inclusion period 2013-2017 ; n = 6’896
STEMI as final diagnosis ; n = 6’306
First-time STEMIn = 5’423
Recurrent STEMI n = 883
First-time STEMIn = 857
Recurrent STEMI n = 857
matching
Standardized mean differences before and after propensity score matching.
Flowchart of the study population from the OSCAR registry. Management and delays based on matching population, adjusted p-values.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Reperfusion amongeligible patients
(p=0.0035)
Timely reperfusionamong eligible patients
(p=0.5977)
Adequate P2Y12inhibition duringhospitalization
(p=0.5322)
Statins at discharge(p=0.0872)
ACEI at dischargeamong patients with
heart failure (p=1)
Beta-blockers atdischarge among
patients with heartfailure (p=0.4795)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12-month observanceof BASIC treatment
(p=0.0167)
Cardiac rehabilitationprogram (p<0.0029)
Daily physical activity(p<0.0043)
Smoking cessation foractive smokers
(p=0.0524)
Balanced diet foroverweighted,diabetics and
dyslipidemic patients(p=0.3023)
Lipid and glucosemonitoring at 3 and/or6 months (p=0.1045)
First-time STEMI
Recurrent STEMI
Pathway of care
Management in the acute phase
Life course post-STEMI
1-year follow-up
Comparison of the pathway of care and life course post-STEMI based on matching population.
Cumulated mortality at 1-month, 6-month and 1-year post-CCI discharge.
First-time STEMI
n=5’423
Recurrent STEMI
n=883
Adjusted
p-value
Call to medical dispatch centre 3001 (55.34%) 591 (66.93%) < 0.0001
Management by EMS 2827 (52.13%) 548 (62.06%) < 0.0001
- Symptom - call 50 [18;136] 50 [20;120] 0.1262
- Call - ECG 29 [21;40] 29 [21;39] 0.4891
- Symptom - ECG 88 [53;190] 84.5 [53;158.75] 0.2420
Admission to ED 2596 (47.87%) 335 (37.94%) < 0.0001
- Without PCI center 1749 (67.37%) 191 (57.01%) 0.0090
- Prehospital fibrinolysis 88 (5.03%) 6 (3.14%) X
- Symptom - Admission 168 [87;516] 153.5 [84.5;373.25] 0.0347
- Admission - ECG 14 [6;38] 12 [5.25;35.75] 0.7383
- Symptom - ECG 207 [107;576] 191 [100.5;425.5] 0.0609
RESUVal - Réseau des Urgences de la Vallée du Rhône | Centre Hospitalier Lucien Hussel, Montée Docteur Maurice Chapuis, 38 200 Vienne, FRANCEContact : [email protected] | +33 (0)4 37 02 10 59 | Copyright © 2019 Laurie Fraticelli [email protected]





























