Embed Size (px)
Citation preview

Unnecessary procedures such as elective labor induction have risen sharply in the United States over the past two decades with associated increases in cesarean births and late preterm births (Martin, Hamilton et al., 2009; Martin, Kirmeyer, Osterman, & Shepherd, 2009). The
reported rate of labor induction in the United States has more than doubled since 1990 from 9.5% to 22.5% in 2006 (most recent year for which induction data are available) (Martin, Hamilton et al.). During this same period, the cesarean birth rate increased 33% from 23.5% to 31.1% (Kozak & Lawrence, 1999; Martin, Hamilton et al.), and the percentage of late preterm vaginal births for which labor was induced increased 130%, from 7.5% to 17.3% (Martin, Kir-meyer et al.).
ABSTRACTPurpose: To reduce elective induc-tions among nulliparous women in a community hospital by adding standardized education regarding induction risks to prepared child-birth classes.Study Design and Methods: Elective induction rates were compared between class attendees and nonattendees before and after the standardized content was added to prepared childbirth classes. A sur-vey of nulliparous women’s deci-sions regarding elective induction was conducted.Results: Elective induction rates of 3,337 nulliparous women were evaluated over a 14-month period (n = 1,694, 7 months before adding content to classes; n = 1,643, 7 months after). Rates did not differ between class attendees (35.2%, n = 301) and nonattendees (37.2%, n = 312, p = .37) before the content was included. However, after stan-dardized education was added, class attendees were less likely to have elective induction (27.9%, n = 239) than nonattendees (37%, n = 292, p < .00). Sixty-three percent of wom-en who attended the classes and did not have elective induction indicated that the classes were infl uential in their decision. Physicians offered the option of elective induction to 69.5% (n = 937) of survey participants. This was a factor in women’s decisions; 43.2% (n = 404) of those offered the option had elective induction, whereas 90.8% (n = 374) of those not offered the option did not have elective induction.Clinical Implications: Education regarding elective induction offered during prepared childbirth classes was associated with a decreased rate among nulliparous women who attended classes when compared to those who did not attend. Patient education may be benefi cial in reducing elective inductions.Key words: Elective labor induction; Nulliparous women; Patient educa-tion; Prepared childbirth classes
188 volume 35 | number 4 July/August 2010
Copyright © 2010 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

July/August 2010 MCN 189
It has been estimated that approximately 10% of elec-tive births are performed before 39 completed weeks of gestation (Clark et al., 2009), despite long-standing recommendations against this practice from the American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists (AAP & ACOG, 1983; ACOG 1999). These babies are more likely to suffer symptoms of iatrogenic prematurity requiring admission
to a special care nursery or neonatal intensive care unit (Clark et al.). From 1992 to 2002, the mean gestational age for singleton births in the United States decreased from 40 weeks to 39 weeks, in part related to the rise in medical procedures such as labor induction and cesar-ean births (Davidoff et al., 2006). Although precise data are unknown due to inability to abstract indications for induction from certifi cates of live births, approximately one half to two thirds of labor inductions are performed for nonmedical indications (Clark et al.; Moore & Ray-burn, 2006). The incidence of elective and medically indi-cated induction varies widely by institution (community or academic), area of the country (region, state, rural, or urban setting), and individual care providers (Glantz, 2005). The overall rate of induction is rising faster than the rate of pregnancy complications that would suggest a need for a medically indicated induction (Caughey et al., 2009; Martin, Hamilton et al., 2009).
There is evidence that elective labor induction signifi -cantly increases risk of cesarean birth for nulliparous women (Clark et al., 2009; Luthy, Malmgren, & Zingheim, 2004; Reisner, Wallin, Zingheim, & Luthy, 2009; Shin, Brubaker, & Ackerson, 2004; Vahratian, Zhang, Troendle, Sciscione, & Hoffman, 2005, Vrouenraets et al., 2005). Use of phar-macologic agents required for labor induction increases risk of complications related to excessive uterine activity, fe-tal heart rate abnormalities, and cesarean birth for failure to progress in labor and/or concern regarding fetal status (Bakker, Kurver, Kuik, & Van Geijn, 2007; Oscarsson, Amer-Wahlin, Rydhstroem, & Kallen, 2006; Simpson & James,
2008; Vahratian et al.; Vrouenraets et al.). Cesarean birth after labor is associated with increased maternal and neona-tal morbidity and mortality, as well as an increase in inpa-tient length of stay and healthcare costs (Allen, O’Connell, & Baskett, 2006a, 2006b; Cheesman, Brady, Flood, & Li, 2009; Deneux-Tharaux, Carmona, Bouvier-Colle, & Breart, 2006; Getahun, Oyelese, Salihu, & Ananth, 2006; Lydon-Rochelle, Holt, Easterling, & Martin, 2001).
The primary purpose of this study was to test an edu-cational intervention in the context of prepared childbirth classes to decrease the rate of elective labor induction among nulliparous women at our community hospital. The project was initiated after numerous discussions at de-partment meetings where physicians indicated they often felt pressure from nulliparous women to induce their labor electively. In 2004, the medical center instituted a policy discouraging elective births before 39 completed weeks of gestation with requirements that a form with the indica-tion for labor induction, gestational age, and cervical sta-tus be faxed to the unit before an elective induction could be scheduled. Mean gestational age for elective induction was 39.6 weeks (SD = .8) in 2007 and 2008, so the issue was not elective induction before 39 completed weeks, but rather elective induction specifi cally for nulliparous wom-en. Physicians were concerned about the increased risk of cesarean birth for this patient population. Education about risks of elective labor induction during childbirth classes was identifi ed as one possible way to minimize these types of requests. We hypothesized that women who were pro-vided thorough information on risks of elective induction would be less likely to ask their physician for an induction of labor. A secondary aim was to explore reasons why nul-liparous women choose to have an elective labor induction.
Although risks of elective induction have been studied, there are limited data as to whether patient education can be helpful in discouraging elective induction, and little is known about reasons nulliparas choose this method of labor. No studies of U.S. women’s decisions regarding
Kathleen Rice Simpson, PhD, RNC, FAAN, Gloria Newman, MSN, RNC, and Octavio R. Chirino, MD, FACOG, FACS
Patient Education to Reduce Elective Inductions
Copyright © 2010 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

190 volume 35 | number 4 July/August 2010
A power analysis determined that a sample size of 300 (n = 150 women per group) was necessary to achieve a power of .80 at the .05 level of signifi cance to detect a difference of at least 10% in induction rates between class attendees and nonattendees. As there were four types of prepared childbirth classes in which the content was of-fered (traditional 6-week format, 6-week format for women who preferred minimal intervention during labor, 4-week format, and 1-day format), a sample of approxi-mately 1,300 patients was desired in order to have at least 150 patients in each subgroup of class attendees to be able to further evaluate the rate of elective induction between types of classes. The Statistical Program for Social Sciences (SPSS 16.0 for Windows; SPSS, Chicago, IL) was used for data analysis. Descriptive data, paired t-tests, and χ2 anal-ysis were used to evaluate data between the two groups.
Specifi c risks of elective induction presented during the class included cesarean birth with longer postpartum recovery, pain, and potential complications as well as other associated risks such as longer labor, use of pharmaco-logic agents and their effects on the mother and fetus, and neonatal morbidity. Benefi ts included advance plan-ning and timing with personal schedules. Women were encouraged to discuss the labor induction process with their physician during their prenatal visits. As prepara-tion for a discussion about elective induction if suggested by their physician, they were given cards with “talking points” listing potential questions they could ask includ-ing indication, what to expect during labor induction, potential methods, as well as risks, benefi ts, and alterna-tives such as waiting for spontaneous labor (Table 1).
The content of the slide presentation and written mate-rials was based on current evidence and recommendations regarding appropriate candidates and timing for elective induction as well as associated risks of the procedure from ACOG (1999, 2001), AWHONN (2009; [Simpson] 2009), the National Institute of Child Health and Human Development (Raju, Higgins, Stark, & Leveno, 2005), and the March of Dimes (2008a, 2008b, 2008c, 2008d). A literacy expert assisted with development of the presen-tation. All but 6 of the 37 slides in fi nal presentation were
elective induction or educational interventions to as-sist women in the decision-making process were found searching the electronic databases PubMed, CINAHL, and the Cochrane Library from January 1988 to No-vember 2009 using the terms elective labor induction, women’s/patients’ choices/decisions for labor/childbirth, patient education and prepared childbirth classes.
Given that there are known associated clinical, opera-tional, and economic implications of elective induction, evaluation of efforts to discourage nulliparous women from choosing this method of labor is warranted. The childbearing woman is a key member of the perinatal team; providing as much accurate information as pos-sible to assist with her decision-making regarding elec-tive induction is consistent with patient advocacy as sup-ported by the Association of Women’s Health, Obstetric and Neonatal Nurses ([AWHONN], 2009) and ACOG (2008, 2009), and is a component of patient education standards from the Joint Commission (TJC, 2009).
Study Design and MethodsInstitutional review board approval was obtained at St. John’s Mercy Medical Center in St. Louis, MO, which is a community teaching hospital with an average of over 8,000 births per year where private attending obstetri-cians are the primary care providers for 95% of child-bearing women. Baseline data indicated that the elective induction rate for nulliparous women at our hospital was approximately 36%, with no difference between those who attended prepared childbirth classes (35%) and those who did not attend (37%; p = .37). Based on data that approximately 50% of nulliparous women at St. John’s Mercy attend prepared childbirth classes, we developed a standardized 40-minute educational session regarding risks and benefits of elective induction for those who attend classes and then compared elective in-duction rates between class attendees who were exposed to the education and nonattendees who did not receive the education over a 7-month period. These rates were also compared for class attendees and nonattendees using the prior 7-month period as a baseline.
Education about risks of elective labor induction presented during childbirth classes was identifi ed as one possible way to minimize requests from nulliparous women to have their labor induced.
Copyright © 2010 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

July/August 2010 MCN 191
determined to be at or below the eighth-grade readability level. A decision was made to include these six slides based on the known level of education of the population served (mean years of education = at least some college).
The classes were provided by 15 Lamaze certifi ed childbirth educators. A series of meetings were held with the childbirth educators before incorporating the educa-tion into the classes to review the content and emphasize importance of presenting the information in a standard-ized objective format. One of the investigators attended selected class sessions over the course of the 7 months to monitor consistency and objectivity in presentation of the information.
Nulliparous women who gave birth in the 7-month pe-riod after the content was added to the classes were invited to participate in a survey to explore the genesis of the deci-sion to related to an elective induction of labor (Table 2 for selected items from the survey). Potential responses to structured survey items were derived from common rea-sons nulliparous women at our hospital indicate that they choose to have an elective induction as noted via review of medical records (indication for induction per patient) and discussions with clinicians. Content validity of the survey was determined through a review and revision process by obstetricians, childbirth educators, labor nurses, and pa-tients. The survey was pilot tested during the fi rst week, and minor changes were made to several items based on patient and research nurse feedback. The survey can be ob-tained via e-mail to the primary author.
Our data indicated that mean gestational age of wom-en in the fi rst prepared childbirth class was approximate-ly 32 weeks; therefore, the second 7-month comparison group and survey period began 9 weeks after the stand-ardized labor induction education content was added to prepared childbirth classes to ensure that all potential survey participants were exposed to the intervention. Inclusion criteria were nulliparity, singleton pregnan-cy, gestation ≥37 weeks, live birth, and English speak-ing. Eligible patients were identifi ed from the daily log. During the inpatient postpartum stay, eligible patients were approached by a research nurse, provided informa-tion about the survey, and invited to participate. If they agreed, the survey was provided, selected clinical data in-cluding indication for induction were collected from the medical record, and the completed survey was obtained during the inpatient stay. Indications for induction (elec-tive vs. medically indicated) in the medical record were coded based on those listed in the ACOG (1999) practice bulletin Induction of Labor.
Baseline data on elective induction rates of those who attended prepared childbirth classes and those who did not attend were obtained from a review of the birth log, prepared childbirth class rosters, and medical records of all women meeting inclusion criteria in the 7 months im-mediately before the survey period, before the standard-ized educational content on elective induction was added to the childbirth classes. From November 1, 2006 to May 31, 2007 there were 5,309 births, 1,694 of which met inclusion criteria. Women were invited to participate
■ What is the reason you are suggesting induction and is it a serious problem?
■ How does an induction occur? Can you tell me about the process?
■ What are the risks or side effects associated with this method of induction?
■ What is the next step if the induction doesn’t work? ■ What are the alternatives to induction including
waiting? Would I be at risk or would my baby be at risk if we wait?
Table 1.Talking Points for Women to Discuss With Their Caregiver if Labor Induction Is Suggested
Selected Patient Survey Items
All Women
During your pregnancy did your physician offer you the option of having your labor induced? Y/N
If yes, when during your pregnancy did your physician offer you this option?
■ Early in my pregnancy ■ During the middle of my pregnancy ■ A few weeks before my due date ■ Right around my due date ■ After my due date had passed
Women Who Did Not Have Induction
If your labor was not induced, was this your decision or your physician’s decision? ■ My decision (I did not ask my physician to induce
my labor) ■ My decision (My physician suggested labor
induction, but I did not want my labor induced) ■ My physician’s decision (I asked my physician for a
labor induction, but he or she said no)
If you attended prepared childbirth classes, did the infor-mation you received in the classes in any way infl uence your decision to not have your labor induced? Y/N
Women Who Had Labor Induction
What was the main reason that your labor was induced?
If your labor was induced, was this primarily your deci-sion or your physician’s decision?
■ My decision (I asked my physician to induce my labor and he or she agreed)
■ My physician’s decision (My physician suggested labor induction or said that I needed to be induced and I agreed)
Table 2.Selected Patient Survey Items
Copyright © 2010 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
192 volume 35 | number 4 July/August 2010
in the survey from June 1, 2007 to January 31, 2008 during which there were 5,274 births, 1,643 of which met inclusion criteria. Eighty-two percent (n = 1,349) of eligible women completed the survey. Various reasons patients offered for not participating were postoperative pain, fatigue, breastfeeding diffi culties, multiple visitors, and time constraints.
ResultsDuring the first and second 7-month periods, 51% (n = 856) and 52% (n = 854), respectively, of women who met inclusion criteria attended hospital-sponsored prepared childbirth classes. Fifty-five percent (n = 741) of women who participated in the survey attended classes. Survey participants who attended classes were significantly older (M = 27.2 years) than those who did not attend (M = 24.8 years; p < .00) and had significantly more years of education (attended class = 89% some college; did not attend class = 40% some college; p < .00). Sixty-seven per-cent and 25% of class attendees completed college and had a graduate or professional degree, respectively, com-pared to 25% and 11% for the same education levels in the group that did not attend classes (p < .00).
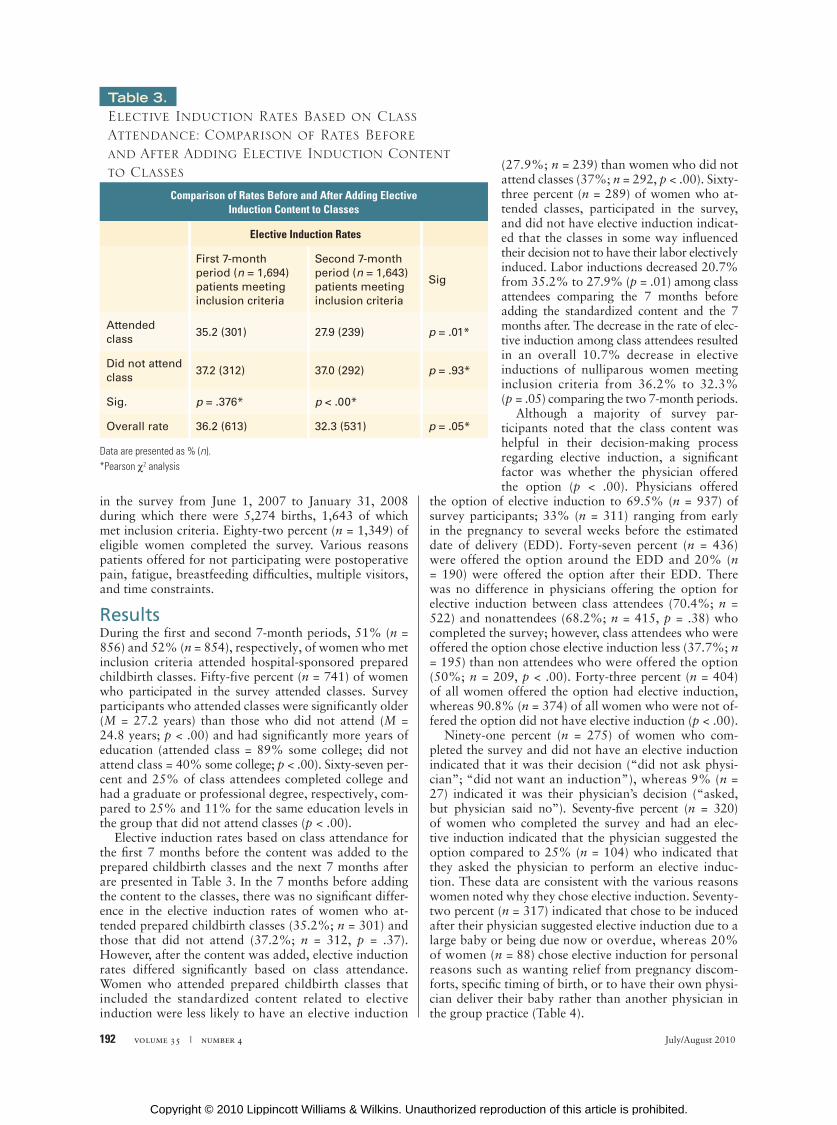
Elective induction rates based on class attendance for the fi rst 7 months before the content was added to the prepared childbirth classes and the next 7 months after are presented in Table 3. In the 7 months before adding the content to the classes, there was no signifi cant differ-ence in the elective induction rates of women who at-tended prepared childbirth classes (35.2%; n = 301) and those that did not attend (37.2%; n = 312, p = .37). However, after the content was added, elective induction rates differed signifi cantly based on class attendance. Women who attended prepared childbirth classes that included the standardized content related to elective induction were less likely to have an elective induction
(27.9%; n = 239) than women who did not attend classes (37%; n = 292, p < .00). Sixty-three percent (n = 289) of women who at-tended classes, participated in the survey, and did not have elective induction indicat-ed that the classes in some way infl uenced their decision not to have their labor electively induced. Labor inductions decreased 20.7% from 35.2% to 27.9% (p = .01) among class attendees comparing the 7 months before adding the standardized content and the 7 months after. The decrease in the rate of elec-tive induction among class attendees resulted in an overall 10.7% decrease in elective inductions of nulliparous women meeting inclusion criteria from 36.2% to 32.3% (p = .05) comparing the two 7-month periods.
Although a majority of survey par-ticipants noted that the class content was helpful in their decision-making process regarding elective induction, a signifi cant factor was whether the physician offered the option (p < .00). Physicians offered
the option of elective induction to 69.5% (n = 937) of survey participants; 33% (n = 311) ranging from early in the pregnancy to several weeks before the estimated date of delivery (EDD). Forty-seven percent (n = 436) were offered the option around the EDD and 20% (n = 190) were offered the option after their EDD. There was no difference in physicians offering the option for elective induction between class attendees (70.4%; n = 522) and nonattendees (68.2%; n = 415, p = .38) who completed the survey; however, class attendees who were offered the option chose elective induction less (37.7%; n = 195) than non attendees who were offered the option (50%; n = 209, p < .00). Forty-three percent (n = 404) of all women offered the option had elective induction, whereas 90.8% (n = 374) of all women who were not of-fered the option did not have elective induction (p < .00).
Ninety-one percent (n = 275) of women who com-pleted the survey and did not have an elective induction indicated that it was their decision (“did not ask physi-cian”; “did not want an induction”), whereas 9% (n = 27) indicated it was their physician’s decision (“asked, but physician said no”). Seventy-fi ve percent (n = 320) of women who completed the survey and had an elec-tive induction indicated that the physician suggested the option compared to 25% (n = 104) who indicated that they asked the physician to perform an elective induc-tion. These data are consistent with the various reasons women noted why they chose elective induction. Seventy-two percent (n = 317) indicated that chose to be induced after their physician suggested elective induction due to a large baby or being due now or overdue, whereas 20% of women (n = 88) chose elective induction for personal reasons such as wanting relief from pregnancy discom-forts, specifi c timing of birth, or to have their own physi-cian deliver their baby rather than another physician in the group practice ( Table 4).
Comparison of Rates Before and After Adding Elective Induction Content to Classes
Elective Induction Rates
First 7-month period (n = 1,694) patients meeting inclusion criteria
Second 7-month period (n = 1,643) patients meeting inclusion criteria
Sig
Attended class
35.2 (301) 27.9 (239) p = .01*
Did not attend class
37.2 (312) 37.0 (292) p = .93*
Sig. p = .376* p < .00*
Overall rate 36.2 (613) 32.3 (531) p = .05*
Table 3.Elective Induction Rates Based on Class Attendance: Comparison of Rates Before and After Adding Elective Induction Content to Classes
Data are presented as % (n).*Pearson χ2 analysis
Copyright © 2010 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

July/August 2010 MCN 193
class attendance; rather class attendance was per patient choice. Among patients who participated in the survey, class attendees were slightly older and had a higher level of education than those who did not attend. However, although the elective induction rate was essentially the same between class attendees and nonattendees before the study intervention, a signifi cant difference in elective induction rates was noted between these two groups after the standardized educational content on elective induc-tion was added to the classes.
The potential of patient education to reduce elective in-duction rates has not been well studied. Despite availabil-ity of prepared childbirth classes in many settings, the high percentage of women who receive prenatal care (Martin, Hamilton et al., 2009) with the opportunity for educa-tion, and patient information materials from the March of Dimes (2008a, 2008b, 2008c, 2008d), ACOG (2001), and Lamaze International (2007) delineating the risks of elec-tive induction, until now none of these mediums have been tested for effi cacy in discouraging women from choosing to have an elective induction. Much more data are needed on effective patient education methods, settings, and ma-terials to help women make informed decisions. Further there are limited data based on direct feedback from wom-en who undergo labor induction that can assist clinicians in offering effective guidance in patients’ decision-making regarding method of labor. Future research involving discussions with women as they are making the decision about whether or not to have an elective induction may be useful in gaining more insight on this topic. Based on results of this study, pregnant women who are provided standardized evidence-based education regarding specifi c risks and benefi ts of elective induction in the context of prepared childbirth classes may be less likely to choose this method of labor and thereby decrease their exposure to the potential associated risks of this elective procedure. Patient education may be an effective tool in decreasing elective inductions among nulliparous women. ✜
Kathleen Rice Simpson is a Perinatal Clinical Nurse Spe-cialist, Gloria Newman is Manager, Women’s and Chil-dren’s Education, and Octavio R. Chirino is Chairman, Department of Obstetrics and Gynecology, St. John’s
Clinical ImplicationsStandardized information based on cur-rent evidence and recommendations from professional organizations regarding risks and benefi ts of elective induction present-ed during prepared childbirth classes was benefi cial in discouraging some women from choosing this option for labor in this study and may be applicable to other set-tings where prepared childbirth classes are offered (Table 5). Patient education before clinical procedures is important to promote informed consent (TJC, 2009). Before in-duction, ACOG (2009) and AWHONN (Simpson, 2009) recommend counseling women regarding indications, pharmaco-logic agents and methods, and possible need for repeat induction or cesarean birth. Nulliparous women with an unfavorable cervix should be counseled about a twofold increased risk of cesarean birth (ACOG). Women who participated in the recent Listening to Mothers Survey II (Declercq, Sakala, Corry, & Applebaum, 2006) over-whelmingly expressed a desire for information regarding potential risks of elective induction; nearly all fi rst time mothers surveyed wanted to know every complication (74.7%) or most complications (24%) of labor induc-tion. Standardized evidence-based information provided in prepared childbirth classes can meet these desires and serve as a foundation for the discussion between the physician/nurse midwife and the patient regarding elec-tive induction recommended by ACOG and AWHONN (Simpson). Nurses working in the prenatal clinic or offi ce setting can reinforce this information and follow up with patients who have additional questions.
Although education provided in prepared childbirth classes can be helpful for women in making the choice of whether or not to have their labor electively induced, the physician is a powerful infl uence. Contrary to the initial perceptions of our physicians that most elective inductions are performed based on requests from patients, physicians offered the option to nearly 70% of women who partici-pated in the survey. It is possible that patients perceive the offer of the option for elective induction as a recommen-dation that they actually have the procedure, particularly if they are told they are due now, overdue, or their baby is getting too big. When the option for elective induction was offered by their physician, women were signifi cantly more likely to choose elective induction than when the option was not offered. Offering the option in the absence of patient request, especially before cervical readiness has been achieved, may lead to unnecessary elective inductions with the associated increased risk of cesarean birth and increased healthcare costs (Allen et al., 2006b; Clark et al., 2009; Reisner et al., 2009). With the ongoing decline in the vaginal birth after cesarean birth rate (Martin, Ham-ilton et al., 2009; Menacker, 2005), subsequent births are most likely to be via cesarean as well.
There are several limitations to this study. Patients were not randomly selected for prepared childbirth
Reasons Women Chose Elective Induction
n (%)
My physician said my baby was getting too big 219 (49.5)
My physician said I was due now or overdue 98 (22.2)
I wanted relief from pregnancy discomforts 51 (11.7)
I’m not sure why my labor was induced 30 (6.8)
I wanted to have my physician deliver my baby 20 (4.5)
I wanted to time the birth for personal reasons 17 (3.8)
Did not answer 7 (1.6)
442 (100)
Table 4.Reasons Women Chose Elective Induction
Copyright © 2010 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

194 volume 35 | number 4 July/August 2010
tive term delivery. American Journal of Obstetrics and Gynecology, 200(2), 156.e1-156.e4.
Davidoff, M. J., Dias, T., Damus, K., Russell, R., Bettegowda, V. R., Dolan, S. et al. (2006). Changes in the gestational age distribution among U.S. singleton births: Impact on rates of late preterm birth, 1992 to 2002. Seminars in Perinatology, 30(1), 8-15.
Declercq, E. R, Sakala, C., Corry, M. P., & Applebaum, S. (2006). Listening to mothers: Report of the second national US survey of women’s childbearing experiences. New York: Childbirth Connections.
Deneux-Tharaux, C., Carmona, E., Bouvier-Colle, & Breart, G. (2006). Postpartum maternal mortality and cesarean delivery. Obstetrics and Gynecology, 108(3, Pt. 1), 541-548.
Getahun, D., Oyelese, Y., Salihu, H. M., & Ananth, C. V. (2006). Previous cesarean delivery and risks of placenta previa and placental abrup-tion. Obstetrics and Gynecology, 107(4), 771-778.
Glantz, J. C. (2005). Elective induction vs spontaneous labor: Associations and outcomes. Journal of Reproductive Medicine, 50(4), 235-240.
Joint Commission. (2009). Joint Commission standards. Oakbrook Ter-race, IL: Author.
Kozak, L. J., & Lawrence, L. (1999). National hospital discharge survey: Annual summary, 1997. Vital and Health Statistics, 13(144), 1-54.
Lamaze Institute for Normal Birth. (2007).The six care practices that sup-port normal birth. Washington, DC: Lamaze International.
Luthy, D. A., Malmgren, J. A., & Zingheim, R. W. (2004). Cesarean delivery after elective induction in nulliparous women: The physician effect. American Journal of Obstetrics and Gynecology, 191(5), 1511-1515.
Lydon-Rochelle, M., Holt, V. L., Easterling, T. R., & Martin, D. P. (2001). First-birth cesarean and placental abruption or previa at second birth. Obstetrics and Gynecology, 97(5, Pt. 1), 765-769.
March of Dimes Foundation. (2008a). 9 questions to help you get your 9 months. White Plains, NY: Author.
March of Dimes Foundation. (2008b). Inducing labor. White Plains, NY: Author.
March of Dimes Foundation. (2008c). Induction by request. White Plains, NY: Author.
March of Dimes Foundation. (2008d). Healthy babies are worth the wait. White Plains, NY: Author.
Martin, J. A., Hamilton, B. E., Sutton P. D., Ventura, S. J., Menacker, F., Kirmeyer, S., et al. (2009). Births: Final data for 2006. National Vital Statistics Report; 57(7), 1-102.
Martin, J. A., Kirmeyer, S., Osterman, M., & Shepherd, R. A. (2009). Born a bit too early: Recent trends in late preterm births (NCHS data brief, No 24). Hyattsville, MD: National Center for Health Statistics.
Menacker, F. (2005). Trends in cesarean rates for first births and repeat cesarean rates for low-risk women: United States, 1990-2003. Na-tional Vital Statistics Report, 54(4), 1-9.
Moore, L. E., & Rayburn, W. F. (2006). Elective induction of labor. Clinical Obstetrics and Gynecology, 49(3), 698-704.
Oscarsson, M. E., Amer-Wahlin, I., Rydhstroem, H., & Kallen, M. (2006). Outcome in obstetrical care related to oxytocin use: A population-based study. Acta Obstetricia et Gynecologica Scandinavica, 85(9), 1094-1098.
Raju, T. N. K., Higgins, R. D., Stark, A. R., & Leveno, K. J. (2006). Optimiz-ing care and outcomes for late preterm (near-term) infants: A sum-mary of the workshop sponsored by the National Institute of Child Health and Human Development. Pediatrics, 118(3), 1207-1214.
Reisner, D. P., Wallin, T. K., Zingheim, R. W., & Luthy, D. A. (2009). Reduc-tion of elective inductions in a large community hospital. American Journal of Obstetrics and Gynecology, 200(6), 674.e1-674.e7.
Shin, K. S., Brubaker, K. L., & Ackerson, L. M. (2004). Risk of cesarean delivery in nulliparous women at greater than 41 weeks gestational age with an unengaged vertex. American Journal of Obstetrics and Gynecology, 190(1), 129-134.
Simpson, K. R. (2009). Cervical ripening, induction and augmentation of labor: (AWHONN Practice Monograph; 3rd ed.). Washington, DC: As-sociation of Women’s Health, Obstetric and Neonatal Nurses.
Simpson, K. R., & James, D. C. (2008). Effects of oxytocin-induced uterine hyperstimulation on fetal oxygen status and fetal heart rate patterns during labor. American Journal of Obstetrics and Gynecology, 199(1), 34.e1-34.e5.
Vahratian, A., Zhang, J., Troendle, J. F., Sciscione, A. C., & Hoffman, M. K. (2005). Labor progression and risk of cesarean delivery in electively induced nulliparas. Obstetrics and Gynecology, 105(4), 698-704.
Vrouenraets, F. P. J. M., Roumen, F. J. M. E., Dehing, C. J. G., van den Akker, E. S. A., Aarts, M. J. B., & Scheve, E. J. T. (2005). Bishop score and risk of cesarean delivery after induction of labor in nulliparous women. Obstetrics and Gynecology, 105(4), 690-697.
Mercy Medical Center, St. Louis, MO. Dr. Simpson can be reached via e-mail at [email protected].
The authors have disclosed that there are no fi nancial relationships related to this article.
Funding provided by Lamaze International and the Department of Obstetrics and Gynecology at St. John’s Mercy Medical Center in St. Louis, MO.
References
Allen, V. M., O’Connell, C. M., & Baskett, T. F. (2006a). Maternal morbidity associated with cesarean delivery without labor compared with in-duction of labor at term. Obstetrics and Gynecology, 108(2), 286-294.
Allen, V. M., O’Connell, C. M., & Baskett, T. F. (2006b). Cumulative economic implications of initial method of delivery. Obstetrics and Gynecology, 108(3, Pt. 1), 549-555.
American Academy of Pediatrics [AAP] and American College of Obste-tricians and Gynecologists [ACOG]. (1983). Guidelines for perinatal care. Elk Grove Village, IL: Author.
American College of Obstetricians and Gynecologists [ACOG]. (1999). Induction of labor (Practice Bulletin No. 10). Washington, DC: Author.
American College of Obstetricians and Gynecologists [ACOG]. (2001). La-bor induction. (Patient Education Pamphlet). Washington, DC: Author.
American College of Obstetricians and Gynecologists [ACOG]. (2009). Induction of labor. (Practice Bulletin No. 107). Washington, DC: Author.
American College of Obstetricians and Gynecologists [ACOG]. (2008). Sur-gery and patient choice. (Committee Opinion No. 395). Washington, DC: Author.
Association of Women’s Health, Obstetric and Neonatal Nurses [AWHONN]. (2005). Late preterm birth initiative. Washington, DC: Author.
Association of Women’s Health, Obstetric and Neonatal Nurses [AWHONN]. (2009). Standards for professional nursing practice (7th ed.). Washington, DC: Author.
Bakker, P. C., Kurver, P. H., Kuik, D. J., & Van Geijn, H. P. (2007). Elevated uterine activity increases the risk of fetal acidosis at birth. American Journal of Obstetrics and Gynecology, 196(4), 313.e1-313.e6.
Caughey, A. B., Sundaram, V., Kaimal, A. J., Cheng, Y. W., Gienger, A., Little, S. E. et al. (2009). Maternal and neonatal outcomes of elective induction of labor (Evidence Report/ Technology Assessment No. 176). Rockville, MD: Agency for Healthcare Research and Quality.
Cheesman, K., Brady, J. E., Flood, P., & Li, G. (2009). Epidemiology of anesthesia-related complications in labor and delivery, New York State, 2002-2005. Anesthesia and Analgesia, 109(4), 1174-1181.
Clark, S. L., Miller, D. D., Belfort, M. A., Dildy, G. A., Frye, D. K., & Meyers, J. A. (2009). Neonatal and maternal outcomes associated with elec-
Standardized evidence-based information regard-ing risks of elective labor induction provided in prepared childbirth classes may be helpful in dis-couraging nulliparous women from choosing to have an elective induction.
Physicians offering the option of elective labor in-duction to nulliparous women in the absence of pa-tient requests may be associated with an increased likelihood of women having an elective induction.
Hearing from their physicians that they are due now or overdue or that their baby is getting too big may be associated with women’s choices to have an elective induction.
Patient education may be one method to decrease the rate of elective induction for nulliparous women.
Clinical Implications
For 15 additional continuing nursing education articles on topics related to obstetrics, go to nursingcenter.com/ce.
Copyright © 2010 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.