Embed Size (px)
Citation preview

------------------------
CNorthShore 9Leaith Centers Vaccine Consent Form
I have been given a copy of the Vaccine Information Statements (VIS) sheets on the vaccines checked below I have read and understand the information in the VIS(S) and have been asked if I had any questions I authorize the administration of this vaccine as directed by the manufacturer
Patient Information First Name Last Name
DOB Age
DI Pentacel Pediarix
DIAP Kinrix __Proquad
TDAP Twinrix PoliolIPV
TD HEPA HEPB
RIB PCV 713 Rotavirus
MMR Varicella Cervarix
Gardasil PPV23 __Meningococcal(Menactra)
Influenza Comvax
Other_______---__-----_______
Your next vaccinations are due on
x______________ _ Date
Signature ofPatient or ParentGuardian
Vaccines administered by __________ ____ Date
VFC COMM CLINIC SITE ____________ _____
To ensure quality care bring vaccine record to every visit
Approved June 2013
Information for Health Professionals about the Screening Checklist for Contraindications (Children amp Teens) he you interested in knowing why we included a certain question on the screening checklist If 50 read the information below If you
want to find out even more consult the references listed at the bottom of this page
I Is the child sick today [aIvaccines] occurred within 6 weeks of a prior infiuenza vaccination vaccinate with TlV if at high
There is no evidence that acute illness reduces vaccine efftcacy or increases vaccine risk for severe infiuenza complications
adverse events (I 2) However as a precaution with moderate or severe arute illshyness all vaccines should be delayed until the illness has improved Mild illnesses (such as otitis media upper respiratory infections and diarrhea) are NOT contraindications to vaccination Do not withhold vaccination if a peron is taking antibiotics
2 Does the child have allergies to medications food a vaccine component or latex [01 vaccines]
If a person reports they have an allergy to egg ask if they can eat lightly cooked eggs (eg scrambled eggs) If they can trivalent innuenza vaccine (TIV) may be admin- istered If after eating eggs or egg-containing foods they have a reaction consisting of only hives TIV may be given and the person should be observed for at least 30 minutes If a person experiences a serious systemic or anaphylactic reaction (eg hives and either swelling of the lips or tongue arute respiratory distress or collapse) after eating eggs do not administer TlV or live attenuated influenza vaccine (LAIV) It is possible that they may be eligible to be given TIV but only after they have seen a physician with expertise in the management of aJlergic conditions If a peron has anashyphylaxis after eating gelatin do not administer LAIV measles-mumps-rubella (MMR) MMR +varicella (MMRV) or variceJla vaccine A local reaction is not a contraindication For a table of vaccines supplied in vials or syringes that contain latex go to wwwcdc govvaccinespubspinkbookJdownloadsappendicesB1atextablepdf For an extensive
table of vaccine components see reference 3
3 Has the child had a serious reaction to a vaccine in the past [01 vaccines] History of anaphyfactic reaction (see question 2) to a previous dose of vaccine or vaccine component is a contraindication for subsequent doses (I) Hisshytory of encephalopathy within 7 days following DTPJDTaP is a contraindication fOl further doses of pertussis-containing vaccine Precautions to DTaP (not T dap) include the following (a) seizure within 3 days of a dose (b) pale or limp episode or collapse within 48 hours of a dose (c) continuous crying for 3 or more hours within 48 hours of a dose and (d) fever of IOSF (40degC) within 48 hours of a previous dose There are other adverse events that might have OCCUlTed following vaccination that constitute contraindiGitions or precautions to fUture doses Under normal circumstances vacshycines are defelTed when a precaution is presenl However situations may arise when the benefrt outweighs the risk (eg during a community pertussis outbreak)
4 Has the child had a health problem with lung heart kidshyney or metabolic disease (eg diabetes) asthma or a blood disorder Is heshe on long-term aspirin therapy [LAIV]
Children with any of tl1e health conditions listed above should not be given the intranashysal live attenuated innuenza vaccine (LAIV) These children should be vaccinated with the injectable influenza vaccine
S If the child to be vaccinated is between the ages of 2 and 4 years has a healthcare provider told you that the child had wheezing or asthma in the past 12 months [lAIV]
Children who have had a wheezing episode within the past I 2 months should not be given the live attenuated infiuenza vaccine Instead these children should be given the
inactivated influenza vaccine
6 If your child is a baby have you ever been told that he or she has had intussusception [Rowvirvs]
Infants who have a history of intussusception (ie the telescoping of one portion of the intestine into another) should not be given rotavirus vaccine
h
7 Has the child a sibling or a parent had a seizure has the child had brain or other nervous system problem [OToP Td Tdop
TIV LA~I MMRV) DTaP and Tdap are contraindicated in children who have a history of encephalopathy within 7 days following DTPDT~P An unstable progressive neuroshylogic problem is a precaution to the use of DTaP and Tdap For children wi th stable neurologic disorders (induding seizures) unrelated to vaccination or for children with a family history ofseizures vaccinate as usual (exception children with a personal or family [r e parent or sibling] history of seizures generally should not be vaccinated with MMRV they should receive separate MMR and VM vaccines) A history of Guillain-Barre syndrome (GBS) is a consideration with the following I) T dT dap if GBS has OCCUlTed within 6 weeks of a tetanus-contning vaccine and decision is made to continue vaccination give age-appropriate T dap instead of T d if no history of prior Tdap to improve pertussis protection 2) Influenza vaccine (TIV or LAIV) ~ GBS has
8 Does the child have cancer leukemia HIVAIDS or any other immune system problem [lAIV MMR MMRV W vAAJ live virus vaccines (eg MMR MMRV varicella rotavirus and the intranasal live atshytenuated influenza vaccine [LAIV]) are usually contraindicated in immunocompromised children However there are exceptions For example MMR is recommended for asymptomatic HIV-infected children who do not have evidence of severe immunosupshypression Likewise varicella vaccine should be considered for HIV-infected d1ild-en with age-specific CD4+ T-Iymphocyte percentage at 15 or greater and may be considered for children age 8 years and older with CD4+ T-Iymphocyte counts of greater than or equal to 200 celisJlL Immunosuppressed children should not receive lAN I nfants who have been diagnosed with severe combined immunodenciency (SClD) should not be given a live vinus vaccine induding rotavirus (fV) vaccine For details consult the ACIP recommendabons (4 S 6)
9 In the past 3 months has the child taken medications that weaken their immune system such as cortisone prednisone other steroids or anticancer drugs or had radiation treatshyments [LAN MMR WARV VAR]
Live virus vaccines (eg MMR MIIRV varicella LAlV) should be postponed until after chemotherapy or long-terrr high-dose steroid therapy has ended For details and length of time 0 postpone consult the ACIP statemenr( I) To nnd speciAc vaccination schedules for stem cell transplant (bone marrow transplant) patients see reference 7 lAlV can be given only to healthy non-pregnant individuals age 2-49 years
10 In the past year has the child received a transfusion of blood or blood products or been given immune (gamma) globulin or an antiviral drug [lAIY NrMR MMW VAA]
Certain live virus vaccines (eg lAIV MMR MMRV varicella) may need to be defmed depending on several variables Consuk the most CUtTent ACIP feurocommendations or tl1e curshyrent Red Book for the most current information on intervals between antiviral drugs immune globulin or blood product administration and live virus vaccines (I 2)
I I Is the childteen pregnant or is there a chance she could become pregnant during the next month [lAV MMR MMRV liAR]
Live vinus vaccines (eg MMR MMRV varicella LAIV) are contraindicated one month before and dUling pregnancy because of the theoretical risk of virus transmission to the fetus ( I 6) Sexually active young women who receive a live virus vaccine should be instructed to practice careful contraception for one month following receipt of the vacshycine (5 8) On theoretical grounds inactivated poliovirus vaccine should not be given during pregnancy however it may be given if risk of disease is imminent (eg bwel to endemic areas) and immediate protection is needed Use ofTd or Tdap is not contrashyindicated in pr-egnancy At the providers discretion either- vaccine may be administered during the 2nd or 3rd trimester (9)
12 Has the child received vaccinations in the past 4 weeks [NV MJoAR MNrW VAR yellow (ever]
If the child was given either live attenuated influenza vaccine (lAIV) or an injectable live virus vaccine (eg MMR MMRV varicella yellow fever) in the past 4 veeks V1ey should wait 28 days before receiving another vaccination of this type Inactivated vacshycin~ may be given at the same time or at any spacing interval
Re(elPncps
1 CDC General recommendations on immunization at NINw cdcgovjvaccinespubsaci~listhtm
2 MP Rtd BooJc Report of he Commil1ie on Inectious Diseo-~s at AIwaJpredbookorg 3 Table ofVaccine Components wwwccJcgovfiaccinespubspinlcbookdoVJllbadsappencJices1B1
excipent-table-2pdi 4 CDC Measles mumps and rubela-vaccine u-e andstrategies forelimina1ion of motasles rubena and
congenital rubeJJa syndrome and control of mumps MMWR 1998 47 (RR-8) S CDC PrE~mjon of ~ella Recomrnendations of Lhe Advisory Commit1~e on Immunization Pracshy
tices MMWR 2007 56 (RR-I)
6 CDC Prevention and Control of innueHza-RECOmmtll(latlons of ACIP ot wWlIaJcgovnulpror~shysionaislvaccination
7 CDC Excerpl from Guidelines (or preventing opportunistic inrections among hematopoietic stem cel trgtnsplant recipients MMWR 2000 49 (AA-I 0) wwwcdcgovvlccinepubOawn-loadsm_hsa-recspdf
8 CDC floife to readers Revised ACiP reccmmendaUoll ror avoiding preglMICY arler receiving a nJbeCa-containing vaccine MMWR 200 I SO (49)
9 CDC Pre~l1Uofl ur pertu~js t~lanus antl diphheria among pregnant and postpartum vIOmen and thi infanlS Recommendations of the ACiP MMWR 2008 57 (RR-4)
Immunization Action Coalibon bull Item P4060 bull p2
Patient name Date of birth __1__ I (mo) (day) (yr)
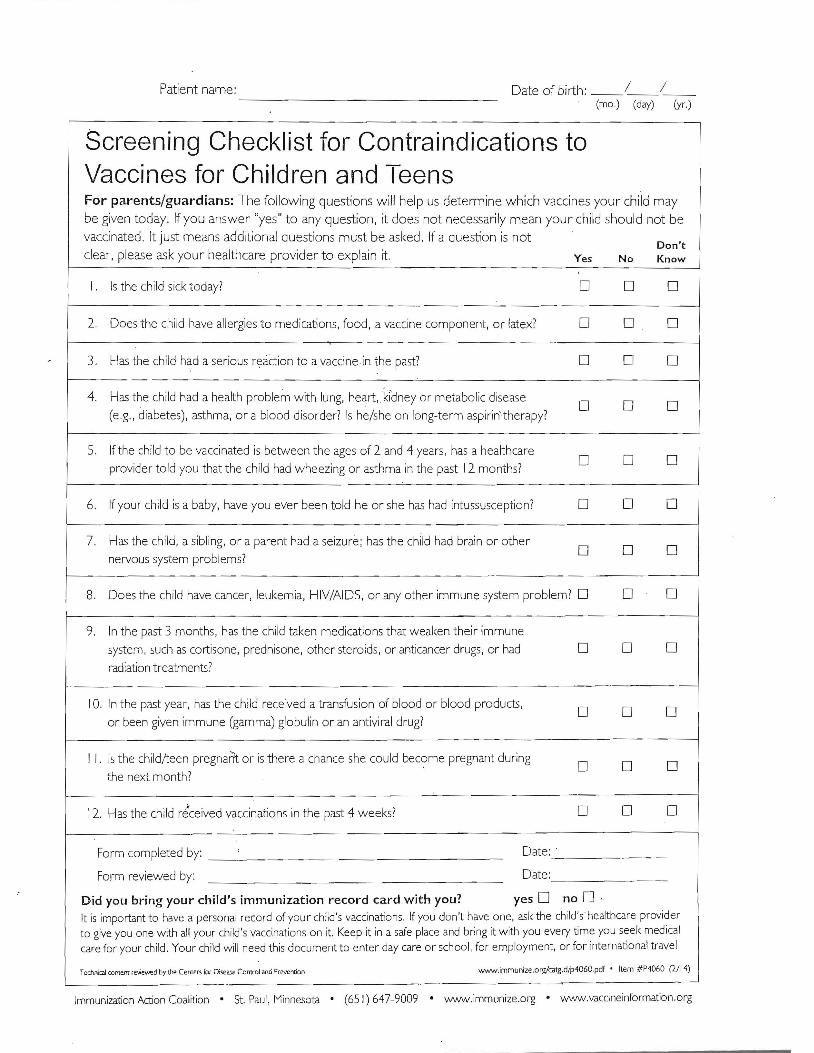
Screening Checklist for Contraindications to Vaccines for Children and Teens For parentsguardians The following questions will help us determine which vaccines your child may
be given today If you answer yes to any question it does not necessarily mean your child should not be
vaccinated It just means additional questions must be asked If a question is not Dont
clear please ask your healthcare provider to explain it Yes No Know
I Is the child sick today 0 0 0
2 Does the child have allergies to medications food a vaccine component or latex 0 0 0
3 Has the child had a serious reaCtion to a vaccine in the past 0 0 0
4 Has the child had a health problem w ith lung heart kidney or metabolic disease 0 0 0
(eg diabetes) asthma or a blood disorder Is heshe on long-term aspirintherapy
5 If the child to be vaccinated is between the ages of 2 and 4 years has a healthcare 0 0 0
providel told you that the child had wheezing or asthma in the past 12 months
6 If your child is a baby have you ever been told he or she has had intussusception 0 0 0
7 Has the child a sibling or a parent had a seizure has the child had brain or other 0 0 0
nervous system problems
B Does the child have cancer leukemia HIVAIDS or any other immune system problem 0 0 0
9 In the past 3 months has the child taken medications that weaken their immune
system such as cortisone prednisone other steroids or anticancer drugs or had 0 0 0 radiation treatments
10 In the past yeal has the child received a transfusion of blood or blood products 0 0 0
or been given immune (gamma) globulin or an antiviral drug
I I Is the childlteen pregnaiit or is there a chance she could bec~me pregnant during 0 0
the next month
12 Has the child r~ceived vaccinations in the past 4 weeks 0 0 0
Date Form completed by
Form reviewed by Date
Did you bring your childs immunization record card with you yes 0 no Dmiddot It is important to have a personal record of your chi lds vaccinations If you dont have one ask the child shealthcare provider to give you one with all your childs vaccinations on it Keep it in a safe place and bring it with you every time you seek medical care for your child Your child will need this document to enter day care or school for employment or for international travel
WWWimmunizeorgcatgdip4060pdf bull Item P4060 (214) Tecnnial content reviewed ty the Cemer for Diseae Control and Prevention
Immunization Action Coalition bull St Paul Minnesota bull (65 I) 647-9009 bull wwwimmunizeorg bull wwwvaccineinformationorg
0
STUDENT lNFORMATJON
StudentName _______________ ______ ----- shy(Last) (First) (MI) (Date of Birth)
Address Home Phone
City
Mother
Address
City State Zip Code
Phone
DOB
State
Father
Address
City State Zip Code
Phone
DOB
Zip Code
Guardian
Address
City State Zip Code
Phone
1 Does this student have a personarphysiciaD who provides medical care to himfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____ _____________ _
J Does this student have a family dentist YES NO Dentist Name _ __________
Names and ages of all Child ren in your Family Name Age DOB School
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of7lfso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________----_________________________
Billing Information Is student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company ________________ -- shy Phone Number
Policy Number GroupllD Number _________
Is srudent covered by Medicaid YES NO Medicaid Number
-
- -----------------------
(
9VorthShoreMERRILL VILLE MERRIllVillE COMMUNITY SCHOOL CORPORATION JLeallh
WtSirivcor ampdl
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the School no information is shared between the two with All information to treatment provided by NorthShore Health wil f be kept between the ParentGuardian Doctor andor Nurse Practitioner
Services NorthShore Health Center offers at the SBHC includes but nollimited to the following (Please cross off any items you your child to receive from NorthShore)
Testing for Communicable Diseases for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness orAnemia
Urinary Tract fnfection
Screenings Pregnancy Testing lmmunizations
Lead AlcohollTobaccoSubstance Abuse Counseling Or Referral
[njury Teen Parenting and Adole
Concerns scent Growth and
student services from the SBHC will be seen of age sex race social or cultural standings or health condition
student that is seen the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high nurse and attendance office
permission for my as a ParenUGuardian is necessary for your child to receive any services
receive students name)
(If your is in an acute to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time our
This permission is good for school NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND fNFORMtTION HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO
SEEK THIRD PARTY REfMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT [F APPROPRlATE ALSO IF MY INSURANCE DOES NOT PAY FOR TIDS SERVICE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
ParentlGuaniian Sienatllre - NortbSbore Health Centers SBHe
lJorthShore Heath Centers will comply with all Federa[ State and Local Laws and related to provision of and reoortinlZ to Indiana State Board of Health
Date
STUDENT [NFORMATION
__1__1_shyStudentName (First)(Las) (MI) (Da te of Birth)
Address Horne Phone
City
Mother DOB Father
State
DOB
Zip Code
Guardian
Address Address Address
City State Zip Code City State Zip Code City State Zip Code
Phone Phone Phone
1 Does this student have B personarphyslcian who provides medical care to hirnfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician ___
J D()CS this student have a family dent
Names aDd ages of all Children in your FamiName Age
ist
ly
YES NO
DOB
_________
Dentist Name
School
___
____
___
_
__
_
_
_
_
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
Drug Allergies ____ ____-----________________________
Billing Information Is student currently covered by WIC vouchers
Insurance Company _________
YES
___
NO
___ _ ___
Health Insurance
Phone Number
YES NO
Policy Number
Is student covered by Medicaid YES NO
Groupto Number
Medicaid Number
____ ____shy -_
middot(
9VorthShore~7 MrsectLlBM~1bY11ramp 9ieallh Cenlers -Zt Slrivcfor amp cdtmct
MerrillviIle Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the High School no information is shared between the two except with parent permission All information pertaining to treatment provided by NorthShbre Health Centers wil be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited (0 the fo[owing (Please cross offany items you do not ~ant your child to receive from NorthShore)
Nurritional Counseling Urinary Tract [nfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening [njury Pregnancy Testing AlcoholrrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and lmmunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a ParentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive senices above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best jUdgment)
This permission is good for school Ijfe~nless NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATIVE TO THESE SERVICES NORTHSHORE HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMElh FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIAIE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
_1_1_shyParentGuardian Signature - NorthShore Health Centers SBRC Date
iorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
----
middot(
9VorthShore~7 ~~lg~BM11bY11Tg 9-Leallh Ceniers oi SlrivcfDr ampdlcnct
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merri Ilville High School Although housed in the same location as the High School no infonnation is shared between the two except with parent permission All information pertaining to treatment provided by NorthShore Health Genters will be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited to the following (Please cross off any items you do not ~ant your child to receive from NorthShore)
Nutritional Counseling Urinary Tract fnfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening fnjury Pregnancy Testing AlcoholrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and Immunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a arentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive services above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best judgment)
This permission is good for school life unless NorthShore Health Centers is notified otherwise in writing )
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATfVE TO THESE SERVICES NORTH SHORE HEALTH CENTERS SBHC IS ALSo AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIATE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTlBLES ANDOR CO-PAY fNSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
I
ParentGuardian Signature - NorthShore Health Centers SBHC Date
-JorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number

Information for Health Professionals about the Screening Checklist for Contraindications (Children amp Teens) he you interested in knowing why we included a certain question on the screening checklist If 50 read the information below If you
want to find out even more consult the references listed at the bottom of this page
I Is the child sick today [aIvaccines] occurred within 6 weeks of a prior infiuenza vaccination vaccinate with TlV if at high
There is no evidence that acute illness reduces vaccine efftcacy or increases vaccine risk for severe infiuenza complications
adverse events (I 2) However as a precaution with moderate or severe arute illshyness all vaccines should be delayed until the illness has improved Mild illnesses (such as otitis media upper respiratory infections and diarrhea) are NOT contraindications to vaccination Do not withhold vaccination if a peron is taking antibiotics
2 Does the child have allergies to medications food a vaccine component or latex [01 vaccines]
If a person reports they have an allergy to egg ask if they can eat lightly cooked eggs (eg scrambled eggs) If they can trivalent innuenza vaccine (TIV) may be admin- istered If after eating eggs or egg-containing foods they have a reaction consisting of only hives TIV may be given and the person should be observed for at least 30 minutes If a person experiences a serious systemic or anaphylactic reaction (eg hives and either swelling of the lips or tongue arute respiratory distress or collapse) after eating eggs do not administer TlV or live attenuated influenza vaccine (LAIV) It is possible that they may be eligible to be given TIV but only after they have seen a physician with expertise in the management of aJlergic conditions If a peron has anashyphylaxis after eating gelatin do not administer LAIV measles-mumps-rubella (MMR) MMR +varicella (MMRV) or variceJla vaccine A local reaction is not a contraindication For a table of vaccines supplied in vials or syringes that contain latex go to wwwcdc govvaccinespubspinkbookJdownloadsappendicesB1atextablepdf For an extensive
table of vaccine components see reference 3
3 Has the child had a serious reaction to a vaccine in the past [01 vaccines] History of anaphyfactic reaction (see question 2) to a previous dose of vaccine or vaccine component is a contraindication for subsequent doses (I) Hisshytory of encephalopathy within 7 days following DTPJDTaP is a contraindication fOl further doses of pertussis-containing vaccine Precautions to DTaP (not T dap) include the following (a) seizure within 3 days of a dose (b) pale or limp episode or collapse within 48 hours of a dose (c) continuous crying for 3 or more hours within 48 hours of a dose and (d) fever of IOSF (40degC) within 48 hours of a previous dose There are other adverse events that might have OCCUlTed following vaccination that constitute contraindiGitions or precautions to fUture doses Under normal circumstances vacshycines are defelTed when a precaution is presenl However situations may arise when the benefrt outweighs the risk (eg during a community pertussis outbreak)
4 Has the child had a health problem with lung heart kidshyney or metabolic disease (eg diabetes) asthma or a blood disorder Is heshe on long-term aspirin therapy [LAIV]
Children with any of tl1e health conditions listed above should not be given the intranashysal live attenuated innuenza vaccine (LAIV) These children should be vaccinated with the injectable influenza vaccine
S If the child to be vaccinated is between the ages of 2 and 4 years has a healthcare provider told you that the child had wheezing or asthma in the past 12 months [lAIV]
Children who have had a wheezing episode within the past I 2 months should not be given the live attenuated infiuenza vaccine Instead these children should be given the
inactivated influenza vaccine
6 If your child is a baby have you ever been told that he or she has had intussusception [Rowvirvs]
Infants who have a history of intussusception (ie the telescoping of one portion of the intestine into another) should not be given rotavirus vaccine
h
7 Has the child a sibling or a parent had a seizure has the child had brain or other nervous system problem [OToP Td Tdop
TIV LA~I MMRV) DTaP and Tdap are contraindicated in children who have a history of encephalopathy within 7 days following DTPDT~P An unstable progressive neuroshylogic problem is a precaution to the use of DTaP and Tdap For children wi th stable neurologic disorders (induding seizures) unrelated to vaccination or for children with a family history ofseizures vaccinate as usual (exception children with a personal or family [r e parent or sibling] history of seizures generally should not be vaccinated with MMRV they should receive separate MMR and VM vaccines) A history of Guillain-Barre syndrome (GBS) is a consideration with the following I) T dT dap if GBS has OCCUlTed within 6 weeks of a tetanus-contning vaccine and decision is made to continue vaccination give age-appropriate T dap instead of T d if no history of prior Tdap to improve pertussis protection 2) Influenza vaccine (TIV or LAIV) ~ GBS has
8 Does the child have cancer leukemia HIVAIDS or any other immune system problem [lAIV MMR MMRV W vAAJ live virus vaccines (eg MMR MMRV varicella rotavirus and the intranasal live atshytenuated influenza vaccine [LAIV]) are usually contraindicated in immunocompromised children However there are exceptions For example MMR is recommended for asymptomatic HIV-infected children who do not have evidence of severe immunosupshypression Likewise varicella vaccine should be considered for HIV-infected d1ild-en with age-specific CD4+ T-Iymphocyte percentage at 15 or greater and may be considered for children age 8 years and older with CD4+ T-Iymphocyte counts of greater than or equal to 200 celisJlL Immunosuppressed children should not receive lAN I nfants who have been diagnosed with severe combined immunodenciency (SClD) should not be given a live vinus vaccine induding rotavirus (fV) vaccine For details consult the ACIP recommendabons (4 S 6)
9 In the past 3 months has the child taken medications that weaken their immune system such as cortisone prednisone other steroids or anticancer drugs or had radiation treatshyments [LAN MMR WARV VAR]
Live virus vaccines (eg MMR MIIRV varicella LAlV) should be postponed until after chemotherapy or long-terrr high-dose steroid therapy has ended For details and length of time 0 postpone consult the ACIP statemenr( I) To nnd speciAc vaccination schedules for stem cell transplant (bone marrow transplant) patients see reference 7 lAlV can be given only to healthy non-pregnant individuals age 2-49 years
10 In the past year has the child received a transfusion of blood or blood products or been given immune (gamma) globulin or an antiviral drug [lAIY NrMR MMW VAA]
Certain live virus vaccines (eg lAIV MMR MMRV varicella) may need to be defmed depending on several variables Consuk the most CUtTent ACIP feurocommendations or tl1e curshyrent Red Book for the most current information on intervals between antiviral drugs immune globulin or blood product administration and live virus vaccines (I 2)
I I Is the childteen pregnant or is there a chance she could become pregnant during the next month [lAV MMR MMRV liAR]
Live vinus vaccines (eg MMR MMRV varicella LAIV) are contraindicated one month before and dUling pregnancy because of the theoretical risk of virus transmission to the fetus ( I 6) Sexually active young women who receive a live virus vaccine should be instructed to practice careful contraception for one month following receipt of the vacshycine (5 8) On theoretical grounds inactivated poliovirus vaccine should not be given during pregnancy however it may be given if risk of disease is imminent (eg bwel to endemic areas) and immediate protection is needed Use ofTd or Tdap is not contrashyindicated in pr-egnancy At the providers discretion either- vaccine may be administered during the 2nd or 3rd trimester (9)
12 Has the child received vaccinations in the past 4 weeks [NV MJoAR MNrW VAR yellow (ever]
If the child was given either live attenuated influenza vaccine (lAIV) or an injectable live virus vaccine (eg MMR MMRV varicella yellow fever) in the past 4 veeks V1ey should wait 28 days before receiving another vaccination of this type Inactivated vacshycin~ may be given at the same time or at any spacing interval
Re(elPncps
1 CDC General recommendations on immunization at NINw cdcgovjvaccinespubsaci~listhtm
2 MP Rtd BooJc Report of he Commil1ie on Inectious Diseo-~s at AIwaJpredbookorg 3 Table ofVaccine Components wwwccJcgovfiaccinespubspinlcbookdoVJllbadsappencJices1B1
excipent-table-2pdi 4 CDC Measles mumps and rubela-vaccine u-e andstrategies forelimina1ion of motasles rubena and
congenital rubeJJa syndrome and control of mumps MMWR 1998 47 (RR-8) S CDC PrE~mjon of ~ella Recomrnendations of Lhe Advisory Commit1~e on Immunization Pracshy
tices MMWR 2007 56 (RR-I)
6 CDC Prevention and Control of innueHza-RECOmmtll(latlons of ACIP ot wWlIaJcgovnulpror~shysionaislvaccination
7 CDC Excerpl from Guidelines (or preventing opportunistic inrections among hematopoietic stem cel trgtnsplant recipients MMWR 2000 49 (AA-I 0) wwwcdcgovvlccinepubOawn-loadsm_hsa-recspdf
8 CDC floife to readers Revised ACiP reccmmendaUoll ror avoiding preglMICY arler receiving a nJbeCa-containing vaccine MMWR 200 I SO (49)
9 CDC Pre~l1Uofl ur pertu~js t~lanus antl diphheria among pregnant and postpartum vIOmen and thi infanlS Recommendations of the ACiP MMWR 2008 57 (RR-4)
Immunization Action Coalibon bull Item P4060 bull p2
Patient name Date of birth __1__ I (mo) (day) (yr)
Screening Checklist for Contraindications to Vaccines for Children and Teens For parentsguardians The following questions will help us determine which vaccines your child may
be given today If you answer yes to any question it does not necessarily mean your child should not be
vaccinated It just means additional questions must be asked If a question is not Dont
clear please ask your healthcare provider to explain it Yes No Know
I Is the child sick today 0 0 0
2 Does the child have allergies to medications food a vaccine component or latex 0 0 0
3 Has the child had a serious reaCtion to a vaccine in the past 0 0 0
4 Has the child had a health problem w ith lung heart kidney or metabolic disease 0 0 0
(eg diabetes) asthma or a blood disorder Is heshe on long-term aspirintherapy
5 If the child to be vaccinated is between the ages of 2 and 4 years has a healthcare 0 0 0
providel told you that the child had wheezing or asthma in the past 12 months
6 If your child is a baby have you ever been told he or she has had intussusception 0 0 0
7 Has the child a sibling or a parent had a seizure has the child had brain or other 0 0 0
nervous system problems
B Does the child have cancer leukemia HIVAIDS or any other immune system problem 0 0 0
9 In the past 3 months has the child taken medications that weaken their immune
system such as cortisone prednisone other steroids or anticancer drugs or had 0 0 0 radiation treatments
10 In the past yeal has the child received a transfusion of blood or blood products 0 0 0
or been given immune (gamma) globulin or an antiviral drug
I I Is the childlteen pregnaiit or is there a chance she could bec~me pregnant during 0 0
the next month
12 Has the child r~ceived vaccinations in the past 4 weeks 0 0 0
Date Form completed by
Form reviewed by Date
Did you bring your childs immunization record card with you yes 0 no Dmiddot It is important to have a personal record of your chi lds vaccinations If you dont have one ask the child shealthcare provider to give you one with all your childs vaccinations on it Keep it in a safe place and bring it with you every time you seek medical care for your child Your child will need this document to enter day care or school for employment or for international travel
WWWimmunizeorgcatgdip4060pdf bull Item P4060 (214) Tecnnial content reviewed ty the Cemer for Diseae Control and Prevention
Immunization Action Coalition bull St Paul Minnesota bull (65 I) 647-9009 bull wwwimmunizeorg bull wwwvaccineinformationorg
0
STUDENT lNFORMATJON
StudentName _______________ ______ ----- shy(Last) (First) (MI) (Date of Birth)
Address Home Phone
City
Mother
Address
City State Zip Code
Phone
DOB
State
Father
Address
City State Zip Code
Phone
DOB
Zip Code
Guardian
Address
City State Zip Code
Phone
1 Does this student have a personarphysiciaD who provides medical care to himfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____ _____________ _
J Does this student have a family dentist YES NO Dentist Name _ __________
Names and ages of all Child ren in your Family Name Age DOB School
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of7lfso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________----_________________________
Billing Information Is student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company ________________ -- shy Phone Number
Policy Number GroupllD Number _________
Is srudent covered by Medicaid YES NO Medicaid Number
-
- -----------------------
(
9VorthShoreMERRILL VILLE MERRIllVillE COMMUNITY SCHOOL CORPORATION JLeallh
WtSirivcor ampdl
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the School no information is shared between the two with All information to treatment provided by NorthShore Health wil f be kept between the ParentGuardian Doctor andor Nurse Practitioner
Services NorthShore Health Center offers at the SBHC includes but nollimited to the following (Please cross off any items you your child to receive from NorthShore)
Testing for Communicable Diseases for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness orAnemia
Urinary Tract fnfection
Screenings Pregnancy Testing lmmunizations
Lead AlcohollTobaccoSubstance Abuse Counseling Or Referral
[njury Teen Parenting and Adole
Concerns scent Growth and
student services from the SBHC will be seen of age sex race social or cultural standings or health condition
student that is seen the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high nurse and attendance office
permission for my as a ParenUGuardian is necessary for your child to receive any services
receive students name)
(If your is in an acute to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time our
This permission is good for school NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND fNFORMtTION HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO
SEEK THIRD PARTY REfMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT [F APPROPRlATE ALSO IF MY INSURANCE DOES NOT PAY FOR TIDS SERVICE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
ParentlGuaniian Sienatllre - NortbSbore Health Centers SBHe
lJorthShore Heath Centers will comply with all Federa[ State and Local Laws and related to provision of and reoortinlZ to Indiana State Board of Health
Date
STUDENT [NFORMATION
__1__1_shyStudentName (First)(Las) (MI) (Da te of Birth)
Address Horne Phone
City
Mother DOB Father
State
DOB
Zip Code
Guardian
Address Address Address
City State Zip Code City State Zip Code City State Zip Code
Phone Phone Phone
1 Does this student have B personarphyslcian who provides medical care to hirnfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician ___
J D()CS this student have a family dent
Names aDd ages of all Children in your FamiName Age
ist
ly
YES NO
DOB
_________
Dentist Name
School
___
____
___
_
__
_
_
_
_
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
Drug Allergies ____ ____-----________________________
Billing Information Is student currently covered by WIC vouchers
Insurance Company _________
YES
___
NO
___ _ ___
Health Insurance
Phone Number
YES NO
Policy Number
Is student covered by Medicaid YES NO
Groupto Number
Medicaid Number
____ ____shy -_
middot(
9VorthShore~7 MrsectLlBM~1bY11ramp 9ieallh Cenlers -Zt Slrivcfor amp cdtmct
MerrillviIle Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the High School no information is shared between the two except with parent permission All information pertaining to treatment provided by NorthShbre Health Centers wil be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited (0 the fo[owing (Please cross offany items you do not ~ant your child to receive from NorthShore)
Nurritional Counseling Urinary Tract [nfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening [njury Pregnancy Testing AlcoholrrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and lmmunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a ParentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive senices above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best jUdgment)
This permission is good for school Ijfe~nless NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATIVE TO THESE SERVICES NORTHSHORE HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMElh FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIAIE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
_1_1_shyParentGuardian Signature - NorthShore Health Centers SBRC Date
iorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
----
middot(
9VorthShore~7 ~~lg~BM11bY11Tg 9-Leallh Ceniers oi SlrivcfDr ampdlcnct
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merri Ilville High School Although housed in the same location as the High School no infonnation is shared between the two except with parent permission All information pertaining to treatment provided by NorthShore Health Genters will be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited to the following (Please cross off any items you do not ~ant your child to receive from NorthShore)
Nutritional Counseling Urinary Tract fnfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening fnjury Pregnancy Testing AlcoholrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and Immunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a arentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive services above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best judgment)
This permission is good for school life unless NorthShore Health Centers is notified otherwise in writing )
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATfVE TO THESE SERVICES NORTH SHORE HEALTH CENTERS SBHC IS ALSo AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIATE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTlBLES ANDOR CO-PAY fNSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
I
ParentGuardian Signature - NorthShore Health Centers SBHC Date
-JorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number
Patient name Date of birth __1__ I (mo) (day) (yr)
Screening Checklist for Contraindications to Vaccines for Children and Teens For parentsguardians The following questions will help us determine which vaccines your child may
be given today If you answer yes to any question it does not necessarily mean your child should not be
vaccinated It just means additional questions must be asked If a question is not Dont
clear please ask your healthcare provider to explain it Yes No Know
I Is the child sick today 0 0 0
2 Does the child have allergies to medications food a vaccine component or latex 0 0 0
3 Has the child had a serious reaCtion to a vaccine in the past 0 0 0
4 Has the child had a health problem w ith lung heart kidney or metabolic disease 0 0 0
(eg diabetes) asthma or a blood disorder Is heshe on long-term aspirintherapy
5 If the child to be vaccinated is between the ages of 2 and 4 years has a healthcare 0 0 0
providel told you that the child had wheezing or asthma in the past 12 months
6 If your child is a baby have you ever been told he or she has had intussusception 0 0 0
7 Has the child a sibling or a parent had a seizure has the child had brain or other 0 0 0
nervous system problems
B Does the child have cancer leukemia HIVAIDS or any other immune system problem 0 0 0
9 In the past 3 months has the child taken medications that weaken their immune
system such as cortisone prednisone other steroids or anticancer drugs or had 0 0 0 radiation treatments
10 In the past yeal has the child received a transfusion of blood or blood products 0 0 0
or been given immune (gamma) globulin or an antiviral drug
I I Is the childlteen pregnaiit or is there a chance she could bec~me pregnant during 0 0
the next month
12 Has the child r~ceived vaccinations in the past 4 weeks 0 0 0
Date Form completed by
Form reviewed by Date
Did you bring your childs immunization record card with you yes 0 no Dmiddot It is important to have a personal record of your chi lds vaccinations If you dont have one ask the child shealthcare provider to give you one with all your childs vaccinations on it Keep it in a safe place and bring it with you every time you seek medical care for your child Your child will need this document to enter day care or school for employment or for international travel
WWWimmunizeorgcatgdip4060pdf bull Item P4060 (214) Tecnnial content reviewed ty the Cemer for Diseae Control and Prevention
Immunization Action Coalition bull St Paul Minnesota bull (65 I) 647-9009 bull wwwimmunizeorg bull wwwvaccineinformationorg
0
STUDENT lNFORMATJON
StudentName _______________ ______ ----- shy(Last) (First) (MI) (Date of Birth)
Address Home Phone
City
Mother
Address
City State Zip Code
Phone
DOB
State
Father
Address
City State Zip Code
Phone
DOB
Zip Code
Guardian
Address
City State Zip Code
Phone
1 Does this student have a personarphysiciaD who provides medical care to himfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____ _____________ _
J Does this student have a family dentist YES NO Dentist Name _ __________
Names and ages of all Child ren in your Family Name Age DOB School
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of7lfso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________----_________________________
Billing Information Is student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company ________________ -- shy Phone Number
Policy Number GroupllD Number _________
Is srudent covered by Medicaid YES NO Medicaid Number
-
- -----------------------
(
9VorthShoreMERRILL VILLE MERRIllVillE COMMUNITY SCHOOL CORPORATION JLeallh
WtSirivcor ampdl
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the School no information is shared between the two with All information to treatment provided by NorthShore Health wil f be kept between the ParentGuardian Doctor andor Nurse Practitioner
Services NorthShore Health Center offers at the SBHC includes but nollimited to the following (Please cross off any items you your child to receive from NorthShore)
Testing for Communicable Diseases for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness orAnemia
Urinary Tract fnfection
Screenings Pregnancy Testing lmmunizations
Lead AlcohollTobaccoSubstance Abuse Counseling Or Referral
[njury Teen Parenting and Adole
Concerns scent Growth and
student services from the SBHC will be seen of age sex race social or cultural standings or health condition
student that is seen the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high nurse and attendance office
permission for my as a ParenUGuardian is necessary for your child to receive any services
receive students name)
(If your is in an acute to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time our
This permission is good for school NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND fNFORMtTION HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO
SEEK THIRD PARTY REfMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT [F APPROPRlATE ALSO IF MY INSURANCE DOES NOT PAY FOR TIDS SERVICE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
ParentlGuaniian Sienatllre - NortbSbore Health Centers SBHe
lJorthShore Heath Centers will comply with all Federa[ State and Local Laws and related to provision of and reoortinlZ to Indiana State Board of Health
Date
STUDENT [NFORMATION
__1__1_shyStudentName (First)(Las) (MI) (Da te of Birth)
Address Horne Phone
City
Mother DOB Father
State
DOB
Zip Code
Guardian
Address Address Address
City State Zip Code City State Zip Code City State Zip Code
Phone Phone Phone
1 Does this student have B personarphyslcian who provides medical care to hirnfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician ___
J D()CS this student have a family dent
Names aDd ages of all Children in your FamiName Age
ist
ly
YES NO
DOB
_________
Dentist Name
School
___
____
___
_
__
_
_
_
_
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
Drug Allergies ____ ____-----________________________
Billing Information Is student currently covered by WIC vouchers
Insurance Company _________
YES
___
NO
___ _ ___
Health Insurance
Phone Number
YES NO
Policy Number
Is student covered by Medicaid YES NO
Groupto Number
Medicaid Number
____ ____shy -_
middot(
9VorthShore~7 MrsectLlBM~1bY11ramp 9ieallh Cenlers -Zt Slrivcfor amp cdtmct
MerrillviIle Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the High School no information is shared between the two except with parent permission All information pertaining to treatment provided by NorthShbre Health Centers wil be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited (0 the fo[owing (Please cross offany items you do not ~ant your child to receive from NorthShore)
Nurritional Counseling Urinary Tract [nfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening [njury Pregnancy Testing AlcoholrrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and lmmunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a ParentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive senices above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best jUdgment)
This permission is good for school Ijfe~nless NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATIVE TO THESE SERVICES NORTHSHORE HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMElh FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIAIE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
_1_1_shyParentGuardian Signature - NorthShore Health Centers SBRC Date
iorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
----
middot(
9VorthShore~7 ~~lg~BM11bY11Tg 9-Leallh Ceniers oi SlrivcfDr ampdlcnct
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merri Ilville High School Although housed in the same location as the High School no infonnation is shared between the two except with parent permission All information pertaining to treatment provided by NorthShore Health Genters will be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited to the following (Please cross off any items you do not ~ant your child to receive from NorthShore)
Nutritional Counseling Urinary Tract fnfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening fnjury Pregnancy Testing AlcoholrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and Immunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a arentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive services above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best judgment)
This permission is good for school life unless NorthShore Health Centers is notified otherwise in writing )
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATfVE TO THESE SERVICES NORTH SHORE HEALTH CENTERS SBHC IS ALSo AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIATE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTlBLES ANDOR CO-PAY fNSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
I
ParentGuardian Signature - NorthShore Health Centers SBHC Date
-JorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number

STUDENT lNFORMATJON
StudentName _______________ ______ ----- shy(Last) (First) (MI) (Date of Birth)
Address Home Phone
City
Mother
Address
City State Zip Code
Phone
DOB
State
Father
Address
City State Zip Code
Phone
DOB
Zip Code
Guardian
Address
City State Zip Code
Phone
1 Does this student have a personarphysiciaD who provides medical care to himfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____ _____________ _
J Does this student have a family dentist YES NO Dentist Name _ __________
Names and ages of all Child ren in your Family Name Age DOB School
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of7lfso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________----_________________________
Billing Information Is student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company ________________ -- shy Phone Number
Policy Number GroupllD Number _________
Is srudent covered by Medicaid YES NO Medicaid Number
-
- -----------------------
(
9VorthShoreMERRILL VILLE MERRIllVillE COMMUNITY SCHOOL CORPORATION JLeallh
WtSirivcor ampdl
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the School no information is shared between the two with All information to treatment provided by NorthShore Health wil f be kept between the ParentGuardian Doctor andor Nurse Practitioner
Services NorthShore Health Center offers at the SBHC includes but nollimited to the following (Please cross off any items you your child to receive from NorthShore)
Testing for Communicable Diseases for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness orAnemia
Urinary Tract fnfection
Screenings Pregnancy Testing lmmunizations
Lead AlcohollTobaccoSubstance Abuse Counseling Or Referral
[njury Teen Parenting and Adole
Concerns scent Growth and
student services from the SBHC will be seen of age sex race social or cultural standings or health condition
student that is seen the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high nurse and attendance office
permission for my as a ParenUGuardian is necessary for your child to receive any services
receive students name)
(If your is in an acute to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time our
This permission is good for school NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND fNFORMtTION HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO
SEEK THIRD PARTY REfMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT [F APPROPRlATE ALSO IF MY INSURANCE DOES NOT PAY FOR TIDS SERVICE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
ParentlGuaniian Sienatllre - NortbSbore Health Centers SBHe
lJorthShore Heath Centers will comply with all Federa[ State and Local Laws and related to provision of and reoortinlZ to Indiana State Board of Health
Date
STUDENT [NFORMATION
__1__1_shyStudentName (First)(Las) (MI) (Da te of Birth)
Address Horne Phone
City
Mother DOB Father
State
DOB
Zip Code
Guardian
Address Address Address
City State Zip Code City State Zip Code City State Zip Code
Phone Phone Phone
1 Does this student have B personarphyslcian who provides medical care to hirnfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician ___
J D()CS this student have a family dent
Names aDd ages of all Children in your FamiName Age
ist
ly
YES NO
DOB
_________
Dentist Name
School
___
____
___
_
__
_
_
_
_
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
Drug Allergies ____ ____-----________________________
Billing Information Is student currently covered by WIC vouchers
Insurance Company _________
YES
___
NO
___ _ ___
Health Insurance
Phone Number
YES NO
Policy Number
Is student covered by Medicaid YES NO
Groupto Number
Medicaid Number
____ ____shy -_
middot(
9VorthShore~7 MrsectLlBM~1bY11ramp 9ieallh Cenlers -Zt Slrivcfor amp cdtmct
MerrillviIle Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the High School no information is shared between the two except with parent permission All information pertaining to treatment provided by NorthShbre Health Centers wil be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited (0 the fo[owing (Please cross offany items you do not ~ant your child to receive from NorthShore)
Nurritional Counseling Urinary Tract [nfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening [njury Pregnancy Testing AlcoholrrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and lmmunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a ParentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive senices above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best jUdgment)
This permission is good for school Ijfe~nless NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATIVE TO THESE SERVICES NORTHSHORE HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMElh FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIAIE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
_1_1_shyParentGuardian Signature - NorthShore Health Centers SBRC Date
iorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
----
middot(
9VorthShore~7 ~~lg~BM11bY11Tg 9-Leallh Ceniers oi SlrivcfDr ampdlcnct
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merri Ilville High School Although housed in the same location as the High School no infonnation is shared between the two except with parent permission All information pertaining to treatment provided by NorthShore Health Genters will be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited to the following (Please cross off any items you do not ~ant your child to receive from NorthShore)
Nutritional Counseling Urinary Tract fnfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening fnjury Pregnancy Testing AlcoholrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and Immunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a arentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive services above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best judgment)
This permission is good for school life unless NorthShore Health Centers is notified otherwise in writing )
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATfVE TO THESE SERVICES NORTH SHORE HEALTH CENTERS SBHC IS ALSo AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIATE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTlBLES ANDOR CO-PAY fNSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
I
ParentGuardian Signature - NorthShore Health Centers SBHC Date
-JorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number
- -----------------------
(
9VorthShoreMERRILL VILLE MERRIllVillE COMMUNITY SCHOOL CORPORATION JLeallh
WtSirivcor ampdl
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the School no information is shared between the two with All information to treatment provided by NorthShore Health wil f be kept between the ParentGuardian Doctor andor Nurse Practitioner
Services NorthShore Health Center offers at the SBHC includes but nollimited to the following (Please cross off any items you your child to receive from NorthShore)
Testing for Communicable Diseases for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness orAnemia
Urinary Tract fnfection
Screenings Pregnancy Testing lmmunizations
Lead AlcohollTobaccoSubstance Abuse Counseling Or Referral
[njury Teen Parenting and Adole
Concerns scent Growth and
student services from the SBHC will be seen of age sex race social or cultural standings or health condition
student that is seen the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high nurse and attendance office
permission for my as a ParenUGuardian is necessary for your child to receive any services
receive students name)
(If your is in an acute to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time our
This permission is good for school NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND fNFORMtTION HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO
SEEK THIRD PARTY REfMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT [F APPROPRlATE ALSO IF MY INSURANCE DOES NOT PAY FOR TIDS SERVICE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
ParentlGuaniian Sienatllre - NortbSbore Health Centers SBHe
lJorthShore Heath Centers will comply with all Federa[ State and Local Laws and related to provision of and reoortinlZ to Indiana State Board of Health
Date
STUDENT [NFORMATION
__1__1_shyStudentName (First)(Las) (MI) (Da te of Birth)
Address Horne Phone
City
Mother DOB Father
State
DOB
Zip Code
Guardian
Address Address Address
City State Zip Code City State Zip Code City State Zip Code
Phone Phone Phone
1 Does this student have B personarphyslcian who provides medical care to hirnfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician ___
J D()CS this student have a family dent
Names aDd ages of all Children in your FamiName Age
ist
ly
YES NO
DOB
_________
Dentist Name
School
___
____
___
_
__
_
_
_
_
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
Drug Allergies ____ ____-----________________________
Billing Information Is student currently covered by WIC vouchers
Insurance Company _________
YES
___
NO
___ _ ___
Health Insurance
Phone Number
YES NO
Policy Number
Is student covered by Medicaid YES NO
Groupto Number
Medicaid Number
____ ____shy -_
middot(
9VorthShore~7 MrsectLlBM~1bY11ramp 9ieallh Cenlers -Zt Slrivcfor amp cdtmct
MerrillviIle Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the High School no information is shared between the two except with parent permission All information pertaining to treatment provided by NorthShbre Health Centers wil be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited (0 the fo[owing (Please cross offany items you do not ~ant your child to receive from NorthShore)
Nurritional Counseling Urinary Tract [nfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening [njury Pregnancy Testing AlcoholrrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and lmmunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a ParentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive senices above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best jUdgment)
This permission is good for school Ijfe~nless NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATIVE TO THESE SERVICES NORTHSHORE HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMElh FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIAIE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
_1_1_shyParentGuardian Signature - NorthShore Health Centers SBRC Date
iorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
----
middot(
9VorthShore~7 ~~lg~BM11bY11Tg 9-Leallh Ceniers oi SlrivcfDr ampdlcnct
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merri Ilville High School Although housed in the same location as the High School no infonnation is shared between the two except with parent permission All information pertaining to treatment provided by NorthShore Health Genters will be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited to the following (Please cross off any items you do not ~ant your child to receive from NorthShore)
Nutritional Counseling Urinary Tract fnfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening fnjury Pregnancy Testing AlcoholrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and Immunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a arentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive services above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best judgment)
This permission is good for school life unless NorthShore Health Centers is notified otherwise in writing )
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATfVE TO THESE SERVICES NORTH SHORE HEALTH CENTERS SBHC IS ALSo AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIATE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTlBLES ANDOR CO-PAY fNSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
I
ParentGuardian Signature - NorthShore Health Centers SBHC Date
-JorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number

STUDENT [NFORMATION
__1__1_shyStudentName (First)(Las) (MI) (Da te of Birth)
Address Horne Phone
City
Mother DOB Father
State
DOB
Zip Code
Guardian
Address Address Address
City State Zip Code City State Zip Code City State Zip Code
Phone Phone Phone
1 Does this student have B personarphyslcian who provides medical care to hirnfher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician ___
J D()CS this student have a family dent
Names aDd ages of all Children in your FamiName Age
ist
ly
YES NO
DOB
_________
Dentist Name
School
___
____
___
_
__
_
_
_
_
I
Health Conditions Does this student have a chronic health condition which Teen Center should be aware of Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
Drug Allergies ____ ____-----________________________
Billing Information Is student currently covered by WIC vouchers
Insurance Company _________
YES
___
NO
___ _ ___
Health Insurance
Phone Number
YES NO
Policy Number
Is student covered by Medicaid YES NO
Groupto Number
Medicaid Number
____ ____shy -_
middot(
9VorthShore~7 MrsectLlBM~1bY11ramp 9ieallh Cenlers -Zt Slrivcfor amp cdtmct
MerrillviIle Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the High School no information is shared between the two except with parent permission All information pertaining to treatment provided by NorthShbre Health Centers wil be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited (0 the fo[owing (Please cross offany items you do not ~ant your child to receive from NorthShore)
Nurritional Counseling Urinary Tract [nfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening [njury Pregnancy Testing AlcoholrrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and lmmunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a ParentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive senices above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best jUdgment)
This permission is good for school Ijfe~nless NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATIVE TO THESE SERVICES NORTHSHORE HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMElh FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIAIE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
_1_1_shyParentGuardian Signature - NorthShore Health Centers SBRC Date
iorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
----
middot(
9VorthShore~7 ~~lg~BM11bY11Tg 9-Leallh Ceniers oi SlrivcfDr ampdlcnct
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merri Ilville High School Although housed in the same location as the High School no infonnation is shared between the two except with parent permission All information pertaining to treatment provided by NorthShore Health Genters will be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited to the following (Please cross off any items you do not ~ant your child to receive from NorthShore)
Nutritional Counseling Urinary Tract fnfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening fnjury Pregnancy Testing AlcoholrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and Immunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a arentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive services above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best judgment)
This permission is good for school life unless NorthShore Health Centers is notified otherwise in writing )
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATfVE TO THESE SERVICES NORTH SHORE HEALTH CENTERS SBHC IS ALSo AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIATE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTlBLES ANDOR CO-PAY fNSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
I
ParentGuardian Signature - NorthShore Health Centers SBHC Date
-JorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number

middot(
9VorthShore~7 MrsectLlBM~1bY11ramp 9ieallh Cenlers -Zt Slrivcfor amp cdtmct
MerrillviIle Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merrillville High School Although housed in the same location as the High School no information is shared between the two except with parent permission All information pertaining to treatment provided by NorthShbre Health Centers wil be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited (0 the fo[owing (Please cross offany items you do not ~ant your child to receive from NorthShore)
Nurritional Counseling Urinary Tract [nfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening [njury Pregnancy Testing AlcoholrrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and lmmunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a ParentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive senices above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best jUdgment)
This permission is good for school Ijfe~nless NorthShore Health Centers is notified otherwise in writing
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATIVE TO THESE SERVICES NORTHSHORE HEALTH CENTERS SBHC IS ALSO AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMElh FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIAIE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTIBLES ANDOR CO-PAY INSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
_1_1_shyParentGuardian Signature - NorthShore Health Centers SBRC Date
iorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
----
middot(
9VorthShore~7 ~~lg~BM11bY11Tg 9-Leallh Ceniers oi SlrivcfDr ampdlcnct
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merri Ilville High School Although housed in the same location as the High School no infonnation is shared between the two except with parent permission All information pertaining to treatment provided by NorthShore Health Genters will be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited to the following (Please cross off any items you do not ~ant your child to receive from NorthShore)
Nutritional Counseling Urinary Tract fnfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening fnjury Pregnancy Testing AlcoholrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and Immunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a arentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive services above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best judgment)
This permission is good for school life unless NorthShore Health Centers is notified otherwise in writing )
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATfVE TO THESE SERVICES NORTH SHORE HEALTH CENTERS SBHC IS ALSo AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIATE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTlBLES ANDOR CO-PAY fNSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
I
ParentGuardian Signature - NorthShore Health Centers SBHC Date
-JorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number

----
middot(
9VorthShore~7 ~~lg~BM11bY11Tg 9-Leallh Ceniers oi SlrivcfDr ampdlcnct
Merrillville Community School Corporation and NorthShore Community Health Center
Dear ParentGuardian
Merrillville Community Schools in cooperation with NorthShore Health Centers (NorthShore) has established a School Based Health Center (SBHC) located at Merri Ilville High School Although housed in the same location as the High School no infonnation is shared between the two except with parent permission All information pertaining to treatment provided by NorthShore Health Genters will be kept between the ParentGuardian Doctor andor Nurse Pnrctitioner
Services NorthShore Health Center offers at the SBHC includes but not limited to the following (Please cross off any items you do not ~ant your child to receive from NorthShore)
Nutritional Counseling Urinary Tract fnfection Testing Testing for Communicable Diseases Anemia Screening and Lab Testing for LowlHigh Blood Sugar Evaluation and Treatment of Minor Illness or Screenings Lead Screening fnjury Pregnancy Testing AlcoholrobaccoSubstance Abuse Teen Parenting and Adolescent Growth and Immunizations Counseling Or Referral Development Concerns
Any student seeking services from the SBHC will be seen regardless of age sex race income social or cultural standings or health condition
Any student that is seen by the physician andor nurse practitioner in the SBHC will be provided with an excuse for the time they were in the clinic If the Physician andor Nurse Practitioner find it necessary to send the student home there will be an excuse written and submitted to the high school nurse and attendance office
Your signature as a arentGuardian is necessary for your child to receive any of these services I give permission for my sondaughter to receive services above (please print students name)
(If your child is in an acute situation we will attempt to contact you at the number provided for 10 minutes Ifwe are unable to reach you in that time period we will treat using our best judgment)
This permission is good for school life unless NorthShore Health Centers is notified otherwise in writing )
I AUTHORIZE TREATMENT FOR SERVICES AND RELEASE OF MEDICAL AND BILLING INFORMATION RELATfVE TO THESE SERVICES NORTH SHORE HEALTH CENTERS SBHC IS ALSo AUTHORIZED TO SEEK THIRD PARTY REIMBURSEMENT FOR THESE SERVICES RENDERED TO THE DEPENDENT CHILD [F APPROPRIATE ALSO IF MY INSURANCE DOES NOT PAY FOR THIS SERVICE DUE TO DEDUCTlBLES ANDOR CO-PAY fNSURANCE I WILL NOT BE CHARGED FOR THOSE FEES
I
ParentGuardian Signature - NorthShore Health Centers SBHC Date
-JorthShore Heath Centers will comply with all Federal State and Local Laws and regulations related to provision of ervices and reporting to Indiana State Board of Health
middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number

middot STUDENT lNFORMATION
StudenlName (FIrst) ----- shy(Las) (M) (Date of Birth)
Address Home Pbone
City
Mother
Address
City Stat
Phone
e Zip Code
DOB Father
Addres~
City Stat
Phone
State
e Zip Code
DOB
Zip Code
Guardian
Address
City State
Phone
Zip Code
-
1 Does this student have a personaiphyslcian who provides medical care to himher YES NO
Name of DoctorClinic Phone Number _________
2 When was the student last seen by hisher physician _____________ _____
J Does this student have a family den tist YES NO Dentist Name __________
Names and ages of all Children in your Family Name Age DOB School
I Health Conditions Does this student have a chronic health condition which Teen Center should be aware or Ifso Please explain
Is the student taking any medicine YES NO Taking any medicine on a regular basis YES NO Name of Medicine
~
Drug Allergies _________---__________________ _____ _ _
Billing Information [s student currently covered by WIC vouchers YES NO Health Insurance YES NO
Insurance Company _______________ ___ Phone Number
Policy Number GroupID Number _________~
Is student covered by Medicaid YES NO Medicaid Number