Embed Size (px)
Citation preview

Patient with a Right Ankle Haglund’s Deformity
Carlos Llanos, Shawn D. Felton, Jason C. CraddockFlorida Gulf Coast University, Department of Rehabilitation Sciences, Fort Myers, FL USA
Abstract
Introduction
Case Report
Rehabilitation
Discussion and Summary
ReferencesReferencesGillott, E., & Ray, P. (2013). Tuberculosis of the calcaneum masquerading as Haglund’s deformity: a rare case and brief literature review. BMJ Case Reports, 2013,
bcr2013009252. http://doi.org/10.1136/bcr-2013-009252Kang, S., Thordarson, D., Charlton, T. (2012). Insertional Achilles tendinitis and haglund’s deformity. Foot & Ankle International,33(6), 487-491.
https://doi.org/10.3113/FAI.2012.0487 Vaishya, R., Agarwal, A, Azizi, A., et al. (2016). Haglund’s syndrome: a commonly seen mysterious condition. Cureus, 8(10), e820. doi:10.7759/cureus.820Jiang, Y., Li, Y., Tao, T., Li, W., Zhang, K., Gui, J., & Ma, Y. (2016). The double-row suture technique: a better option for the treatment of haglund syndrome. BioMed Research International, 2016. http://doi.org/10.1155/2016/1895948 Stephens, M.M.(1994). Haglund's deformity and retrocalcaneal bursitis. Orthop Clin North Am. 25,41–46.Sofka, C.M., Adler, R.S., Positano, R. et al. (2006). Haglungs’ syndrome: diagnosis and treatment using sonography. HSS Journal. 2(1),27-29.
https://doi.org/10.1007/s11420- 005-0129-8 Thomas, J. L., Christensen, J. C., Kravitz, S. R., Mendicino, R. W., el al. (2010). The diagnosis and treatment of heel pain: a clinical practice guideline–revision 2010. Journal
of Foot and Ankle Surgery, 49(3), S1-s19. https://doi.org/10.1053/j.jfas.2010.01.001 Bulstra, G. H.,Rheenen,T. A., Scholtes, V. A.B. (2015). Can we measure the heel bump? radiographic evaluation of haglund's deformity. Journal of Foot and Ankle Surgery, 54(3), 338-340. https://doi.org/10.1053/j.jfas.2014.07.006 Serrano, P., Leite, F., Sousa, A., Carvalho, A., Silva, M., Costa, L., Gomes, A. (2017). Surgical treatment for Haglund's deformity. Foot and Ankle Surgery, 23(1), 133.
https://doi.org/10.1016/j.fas.2017.07.494 Bullock, M.J., Mourelatos, J., Mar, A. ((2017). Achilles impingement tendinopathy on magnetic resonance imaging. The Journal of Foot and Ankle Surgery, 56(3), 555-563.
https://doi.org/10.1053/j.jfas.2017.01.024Jung, H., Carag, J. A., Park, J., Bae, E., Lim, S., Kim, H. Osteochondroma of the calcaneus presenting as haglund's deformity. (2011) In Foot and Ankle Surgery, 17(2), e20-e22. https://doi.org/10.1016/j.fas.2010.08.007 Hunt, K. J., & Anderson, R. B. (2009). Heel pain in the athlete. Sports Health,1(5), 427-434.Lu, C., Cheng, Y., Fu, Y., Tien,Y., Chen, S., Huang, P. (2007). Angle analysis of Haglund syndrome and its relationship with osseous variations and Achilles tendon calcification. Foot & Ankle International 28(2), 181-185.Nepple, J. J., & Matava, M. J. (2009). Soft tissue injections in the athlete. Sports Health, 1(5), 396–404. http://doi.org/10.1177/1941738109343159 Bearth, L., Leumann, A., Farkas, G., Tamborrini, G. (2015). Review on Haglund-deformity: bursitis subachillea and Haglund- exostosis. Sports Orthopaedics and Traumatology 31(1), 18 – 26.
Achilles Tendon Association with Haglund’s Deformity
Haglund syndrome is an enlargement of the posterosuperior prominence of the calcaneus, which is frequently associated with insertional Achilles tendinitis, bursal projection, and Achilles bursitis. Achilles tendon disorders play a major role in sports orthopaedics. A common cause for Achilles tendon disorders is the Haglund-Exostosis in combination with Bursitis subachillea, this especially in long distance runners (Bearth, 2015).Haglund's deformity, due to bony prominence, exert repetitive mechanical irritation to the adjacent retrocalcaneal bursa and Achilles tendon that can trigger inflammatory condition secondarily developing insertional Achilles tendinopathy or retrocalcaneal bursitis. The presence of a Haglund's deformity is not pathognomonic of insertional Achilles tendinitis as illustrated by a retrospective study by Kang et al, who found Haglund's deformity was equally present in asymptomatic patients.Haglund syndrome can also induce inflammation and the degeneration of the Achilles tendon, because of the abnormal high pressure between the bursal projection of calcaneus, the Achilles tendon, and the bursal impingement of the Achilles. A majority of the insertional Achilles tendinitis patients had calcification at the tendon insertion. We believe it is possible removing the Haglund's deformity may not be necessary in the operative treatment of insertional Achilles tendinitis (Kang, 2012).
Haglund's deformity is a commonly encountered condition causing posterior heel pain, which can be difficult to evaluate and treat, due to differing terminology, anatomical discrepancies and overlapping symptoms. Haglund syndrome is characterized by chronic posterior heel pain associated with a posterosuperior calcaneal prominence.Main cause of this deformity is the tightness of the Achilles tendon due to gastrocnemius myofascial stiffness compressing on the retrocalcaneal bursa. Haglund's syndrome is a combination of soft tissue and bony abnormalities and can cause retrocalcaneal pain consisting of inflammation of the regional soft tissues, and thickening of the Achilles tendon. The following information will explain the mechanism of injury, clinical assessments, radiographic findings, diagnosis, treatment and additional information to this patients�s unique injury.
According to the literature Haglund’s syndrome can be treated conservatively or surgically. Conservative treatment includes the avoidance of rigid heel counter shoes, use of heel cushions, softer uppers or pads for elevation of the heel, insoles, activity modification, eccentric rehabilitation exercises or local block treatment. Medication includes non-steroidal anti-inflammatory drugs or corticosteroid injection into retrocalcaneal bursa are also recommended for acute cases.
A conservative approach for patients with bursitis can provide symptomatic relief but it does not resolve the deformity. However direct intra-tendinous steroid injections might weaken the tendon and cause tendon rupture (Nepple,2009).
In this case conservative treatment was implemented; emphasis on gastrocnemius myofascial release, hamstrings, gastrocnemius, soleus, and Achilles tendon dynamic and static stretches. Gastrocnemius and soleus eccentric strengthening exercises for tissue elongation.
Patient achieved successful findings post conservative treatment and exercise modification over the course of 8 weeks. Patient is asymptomatic, and able to perform pain free ADLs. Pt was able to reach to prior level of function and prior fitness level.
Background: Case report presents a female hospital nurse that was 33-years-old, 63.5 kg, 160 cm. Patient had no specific mechanism of injury to theankle, major complaint we after high impact, squatting exercises or prolongedstanding at work during long hour shifts. Patient presents with a palpablebony lump in the back of the distal Achilles tendon. Patients stated she hashad that lump for long time after many years of ballet. Patient also presentsbilateral forefoot varus and high arches. Lateral radiographs were taken andrevealed retrocalcaneal exostosis of the affected ankle. DifferentialDiagnosis: Achilles Tendon Tendinopathy, Os Trigonum, Calcific Heel Spur,Retrocalcaneal Bursitis, Calcaneal stress fracture. Treatment: According tothe recent literature Haglund's syndrome is often treated conservatively byaltering the heel height in shoewear orthosis, physical rehabilitation, and anti-inflammatory drugs, surface change for aerobic training. Conservativetreatment was implemented; emphasis on gastrocnemius myofascial release,hamstrings, gastrocnemius, soleus, and Achilles tendon dynamic and staticstretches. Gastrocnemius and soleus eccentric strengthening exercises fortissue elongation. Uniqueness: Haglund's deformity is an enlargement of theposterosuperior prominence of the calcaneus. This syndrome producesposterior impingement of the heel, which is caused by a posterosuperiorcalcaneal exostosis. Another cause of this Deformity can be tightness of theAchilles tendon due to gastrocnemius myofascial stiffness compressing onthe retrocalcaneal bursa. This case is unique because the stress on theankles and feet during ballet years growing up. Conclusions: This casereport highlighted the diagnosis and treatment of a 33-year-old femalesuffering from a right ankle Haglund’s Deformity. The case further highlightedthe various treatments options and rehabilitation protocol. Successful findingspost treatment and exercise modification over the course of 8 weeks. Patientis asymptomatic, and able to perform pain free ADLs. Pt was able to reach toprior level of function and prior fitness level.
Patient: This case presents a female hospital nurse that was 33-years-old, 63.5 kg, 160 cm. The patient’s prior medical history included right ACL grade II sprain 2 years ago, non-surgical rehabilitation performed for this injury. Patient is 6 months postpartum, with no complication during pregnancy and normal delivery.
Mechanism of Injury: Patient had no specific mechanism of injury to the ankle, major complaints were after high impact, squatting exercises or prolonged standing at work during long hour shifts.
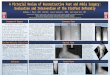
Clinical Examination: Initial evaluation revealed, tender in the area where the Achilles tendon attaches to the heel. Patient presents with a palpable bony lump in the back of the distal Achilles tendon. Patients stated she has had that lump for long time after many years of ballet. Patient had no specific mechanism of injury to the ankle, major complaints were after high impact, squatting exercises or prolonged standing at work during long hour shifts. Full ankle ROM and strength with right ankle plantar flexion, inversion, and eversion. Limited dorsiflexion compared to uninvolved side. Knee flexion and extension ROM within normal limits. Balance, coordination and sensation were intact. Patient also presents bilateral forefoot varus and high arches. (+) Silfverskiold’s Test for gastrocnemius and Achilles tendon tightness, (-) Thomson’s Test, (-) Bump Test.
Radiographic Findings: Patient was then referred to an ankle and foot specialist medical doctor where lateral radiographs were taken and revealed retrocalcaneal exostosis of the affected ankle.
Differential Diagnosis:Plantar Fasciitis, Achilles Tendon Tendinopathy, Os Trigonum, Calcific Heel Spur, Osteochondritis Dissecans, RetrocalcanealBursitis, Calcaneal stress fracture were some of the differential diagnosis associated with this case.
Case Uniqueness:This case is unique because the stress on the ankles and feet during ballet years growing up and another unique factor that can lead to this condition is the hormonal changes in the body postpartum.
Conclusions:This case report highlighted the diagnosis and treatment of a patient suffering from a right ankle Haglund’s Deformity. The case further highlighted the various treatments options and rehabilitation protocol. The patient resorted to non-surgical rehabilitation, and began treatment immediately.
The purpose of this case report was to introduce best clinical approach for a patient with a Haglund’s deformity. This case study also discusses on the conservative and surgical management of the Haglund’s syndrome or Haglund’s deformity.
Purpose
Understanding the anatomy in relation to the Haglund’s syndrome isessential in understanding the injury, presentation and clinical findings.Haglund’s deformity is a symptomatic osseous prominence of theposterosuperior corner of the calcaneus creating posterior heel pain andswelling around the insertion of the Achilles tendon (Hong-Geun Jung etal. 2010). Haglund's syndrome is a constellation of soft tissue and bonyabnormalities and represents one cause of retrocalcaneal painconsisting of inflammation of the regional soft tissues (Sofka,2016). Abony protrusion develops and the bursa becomes inflamed due to theconstant irritation of the back of the heel bone to rub against the tendon(Vaishya,2016). Another cause of Haglund’s Deformity can be a tightAchilles tendon, it causes pain by compressing the tender and theinflamed bursa.
Anatomy
Results
This case report highlighted the diagnosis and treatment of a 33-year-old female suffering from a right ankle Haglund’sDeformity. The case further highlighted the various treatments options and rehabilitation protocol. Successful findings post treatment and exercise modification over the course of 8 weeks. Patient is asymptomatic, and able to perform pain free ADLs. Pt was able to reach to prior level of function and prior fitness level.
Conclusions