Embed Size (px)
Citation preview

AIM
Data from 1st December 2013 to 28th February 2014 was analysed on a
site specific basis from all 50 English centres currently feed information
into the RTDS. Any treatment delivered using VMAT is coded as IMRT.
IMRT delivery within the RTDS is defined as:
The Radiotherapy Board
NATCANSAT National Clinical Analysis and
Specialised Applications Team
www.natcansat.nhs.uk
John Staffurth1, Tracey Ellison2, Chris Ball2 & Gerry Hanna3 1Institute of Cancer and Genetics, Cardiff University, Velindre Cancer Centre, Cardiff, CF14 2TL
2NATCANSAT, The Clatterbridge Cancer Centre NHS Foundation Trust, Wirral, Merseyside, CH63 4JY 3Centre for Cancer Research & Cell Biology, Queen’s University Belfast, Belfast, BT9 7BL
Patterns of IMRT delivery in England
To describe the usage of inverse planned IMRT usage across the 50
registered NHS radiotherapy centres in England during 2014 using the
National Radiotherapy Dataset, RTDS.
National guidance in 2009 from the National Radiotherapy
Implementation Group recommended that 33% of all radical radiotherapy
treatments should be delivered with IMRT and 24% with inverse planned
IMRT1. These figures were based on the treatment demographics from a
limited number of centres and expert opinion on the proportion of each
tumour sites that might benefit from IMRT. In 2011 the Commissioning for
Quality and Innovation set an incentive as part of the National Cancer
Plan2 improving cancer outcomes, to increase the uptake of IMRT.
Previous work has reported the access rates to IMRT across the UK, but
site specific data has been limited3, 4. An analysis of RTDS data was
undertaken to assess variation in global and site specific usage of IMRT
across the 50 English NHS radiotherapy centres in 2014. This has been
used to guide centres’ on their future estimation IMRT usage5.
The national usage of inverse planned IMRT is now over 36%, with only
two centres failing to meet the 24% target. Site specific targets were not
set and this may explain the wide range in usage between centres. The
variation is least for prostate and H&N cancers. These have the greatest
evidence base and there have been multi-centre IMRT trials supported by
the NCRI RTTQA group (http://ctrad.ncri.org.uk/research-support/quality-
assurance-support). IMRT trials in the other tumours are occurring, so
variations are expected to reduce.
REFERENCES
1 Intensity Modulated Radiotherapy (IMRT) A Guide for Commissioners. An NRIG Technology sub-group Report - November 2009.
http://connect.qualityincare.org/__data/assets/pdf_file/0004/554179/NHS_guidelines_on_IMRT.pdf
2 Improving Outcomes: A Strategy for Cancer DOH 2011
3 Survey of the availability and use of advanced radiotherapy technology in the UK. Mayles WPM on behalf of the Radiotherapy
Development Board. Clin Oncol (R Coll Radiol). 2010 Oct;22(8):636-642
4 Progress with intensity-modulated radiotherapy implementation in the UK. Mayles WP, Cooper T, Mackay R, Staffurth J, Williams
M. Clin Oncol (R Coll Radiol). 2012 Oct; 24(8): 543-544
5 Intensity Modulated Radiotherapy (IMRT) in the UK: Current access and predictions of future access rates. Staffurth J, Ball C,
Hanna G, Ellison T, Rowbottom C on behalf of the Radiotherapy Board.
http://www.ipem.ac.uk/Portals/0/Documents/Partners/Radiotherapy%20Board/imrt_target_revisions_recommendations_for_colleges_final2.
IMRT Delivery by
Radiotherapy Provider
Numerator: The number of (new) unique patients starting radiotherapy with inverse planned IMRT (excluding breast radiotherapy) within the specified month. Denominator: The number of (new) radical episodes starting radiotherapy including breast cancer (C50); excluding brachytherapy and patients with a diagnosis of non melanoma skin, (C44) within the specified month.
The Radiotherapy Board was set up in April 2013 and provides guidance,
oversight and support for the continuing development of high-quality
radiotherapy services for cancer patients across the 4 devolved nations.
https://www.rcr.ac.uk/clinical-oncology/faculty-structure/radiotherapy-board
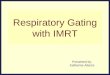
IMRT usage across
England 2012-2014: All centres/ all tumours
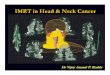
There was a marked variation in usage of IMRT between centres for
every tumour site except prostate cancer (between 0 and 100%). Usage
is highest for prostate and H&N cancer. Further details are available in
the Radiotherapy Board’s report5.
17157 radical treatments were delivered of which 6226 (36%) were
delivered by IMRT. Two centres remain below the 24% rate in Feb 2015,
compared to 4 in Feb 2014).
*
Prostate cancer; NRIG target: 80% Head and neck; NRIG target: 80%
CNS tumours; target: 60% Gynaecological; target: 20% Breast cancer; target: 0%
Lung cancer; No target Upper GI cancers; No target Rectal cancer; No target
Anal cancer; No target Bladder cancer; No target Sarcomas; No target
*Forward-planned breast IMRT is not considered as an IMRT type treatment, any inverse-
planned breast treatment or a forward planned breast IMRT plan with patient specific QA IS
included in the IMRT numbers.
BACKGROUND
METHODS
RESULTS – All tumour sites
RESULTS – Site specific usage
DISCUSSION