Embed Size (px)
Citation preview

Incorporating Trauma into PBIS & Teacher Management
Chris Dunning, Ph.D.Professor Emerita
University of [email protected]

Trauma and Learning
Children who do not feel safe live in a state of emergency. Their energy is consumed by crisis, making it impossible for them to focus on learning.
From “Too Scared to Learn” by Jenny Horsman, 2000
Who couldbe the traumastudent here?
ANSWER: Either

Implications for Learning
“Traumatized children often spend somuch time in the lower level brain in a state of fear that they consistently focus on non-verbal vs. verbal cues.”
Children who have experienced trauma also experience:
▪More school nurse visits/School absences▪Referral to school speech pathologist/support services▪More Disciplinary Actions/Suspension from school▪More aggressive or non-attentive in school▪Difficulties with peers, teachers, and staff▪Lower performance and grade point averages▪Higher drop-out rates

• “The school setting can be a battleground in which
traumatized children’s assumptions of the world as a dangerous place sabotage their ability to develop constructive relationships with nurturing adults. Unfortunately, many traumatized children adopt behavioral coping mechanisms that frustrate educators and evoke exasperated reprisals, reactions that both strengthen expectations of confrontation and danger and reinforce a negative self-image.
• Traumatized children’s behavior can be perplexing. Prompted by internal states not fully understood by the children themselves and unobservable by teachers, traumatized children can be ambivalent, unpredictable and demanding. But it is critical to underscore that traumatized children’s most demanding behavior often originates in feelings of vulnerability.”
(Helping Traumatized Children Learn, p. 32-33)

Trauma-Informed Educator Practice
The trauma-informed educator:• Understands the impact of trauma on a
child’s behavior, development, relationships, and survival strategies
• Can integrate that understanding into planning for the child and learning
• Understands his or her role in responding to child traumatic stress
5
What Can an Educator Do?• Recognize that exposure to trauma occurs to
many children, not just those in protective or foster care.
• Recognize the signs and symptoms of child traumatic stress and how they vary in different age groups.
• Recognize that children’s “bad” behavior is sometimes an adaptation to trauma.
• Understand the impact of trauma on different developmental domains.
6
What Can an Educator Do?
• Understand the impact of trauma and PTSD on learning.• Understand the cumulative effect of trauma.• Gather and document psychosocial information regarding
all traumas in the child’s life to make better-informed decisions.
• Lessen the risk of system-induced secondary trauma by serving as a protective and stress-reducing buffer for children:– Develop trust with children through listening, frequent
contacts, and honesty in order to mitigate previous traumatic stress.
– Understand that schools would do well to be proactive about trauma rather than reactive.

Trauma-Informed Educator
• Offers interventions that increase self worth,• Forms strong relationships to enhance sense of
trust, • Emphasizes the relationship consequences of
behaviors, • Build up avenues for achievement and hope,• Helps child learn both emotion management
skills and relationship skills, • Teaches how to calm biology to increase ability
to think.

Essential Elements of Trauma-Informed education
1. Maximize the child’s sense of safety.2. Assist children in reducing inappropriate
hyperarousal and/or dissociation.3. Address the impact of trauma and subsequent
changes in the child’s behavior, learning, development, and relationships.
4. Utilize comprehensive assessment of the child’s trauma experiences and their impact on the child’s development and behavior to guide services.
5. Coordinate services with other agencies. 9

• Children who have experienced trauma often exhibit extremely challenging behaviors and reactions.
• When we label these behaviors as “good” or “bad,” we forget that children’s behavior is reflective of their experience.
• Many of the most challenging behaviors are strategies that in the past may have helped the child survive in the presence of abusive or neglectful caregivers.
10
Maximizing Safety: Understanding Children’s Responses

Maintaining safety• Behavior management based on
self-regulation rather than compliance– Conflict resolution– Problem-solving– Compromise
• Create positive peer culture– Reduce or prevent isolation/bullying– Increase social competence
• Understand child’s need for containment• Providing positive behavioral supports
– Identify triggers that set child off– Consistency and structure– Involve child, especially feedback

PBIS
• Assumes that approximately 80% of students can and will behave well if – 1) there are clear behavioral expectations– 2) they are taught how to behave in effective and
ongoing manners. “Insights from Trauma-Informed Care help us to
understand that it is just as important, if not more so, to focus on students’ emotional responses as their behavioral responses. Behavior may often communicate a student’s emotional need.”
White and Dibble (2012) Wisconsin DPIUsing Positive Behavioral Interventions & Supports (PBIS) to Help Schools Become More Trauma-Sensitive

Paradigm Shift
• Understanding that trauma is not a cognitive experience, but a sensory one, dictates strategies that immediately restore, to victims, a sense of safety and renewed sense of empowerment/control in the face of fear and uncertainty generated by the incident.
• Reduction of the arousal level is critical to the restoration of pre-trauma cognitive processes, learning functions, behavior and performance.

Trauma and School• Trauma can trigger (arouse) the activation of the
autonomic nervous system to ready itself to resist or solve the real or perceived threat presented by exposure to an incident such as…..
• If the response (arousal) is not discharged or deactivated, the sustained arousal state can lead to sustained cognitive and behavioral dysfunction.
• Trauma being a sensory experience, arousal is experienced as an absence of the “sense of safety” and as a “sense of powerlessness.”
• Aggressiveness, over reactive responses and exaggerated withdrawal are survival behaviors – attempts to feel safe, in control.

What This Tells Us• As long as a student is not feeling safe and in
control, this aroused state makes it difficult to process verbal information, attend, focus, retain and recall.
• Intervention designed to deactivate the arousal state and return the student to a sense of safety and a sense of power or control, helps to restore previous cognitive and behavioral patterns.
• The most immediate, short-term and long-term intervention, therefore, must be designed to restore that sense of safety and control.

Why use the PBIS Trianglefor Traumatized Students?

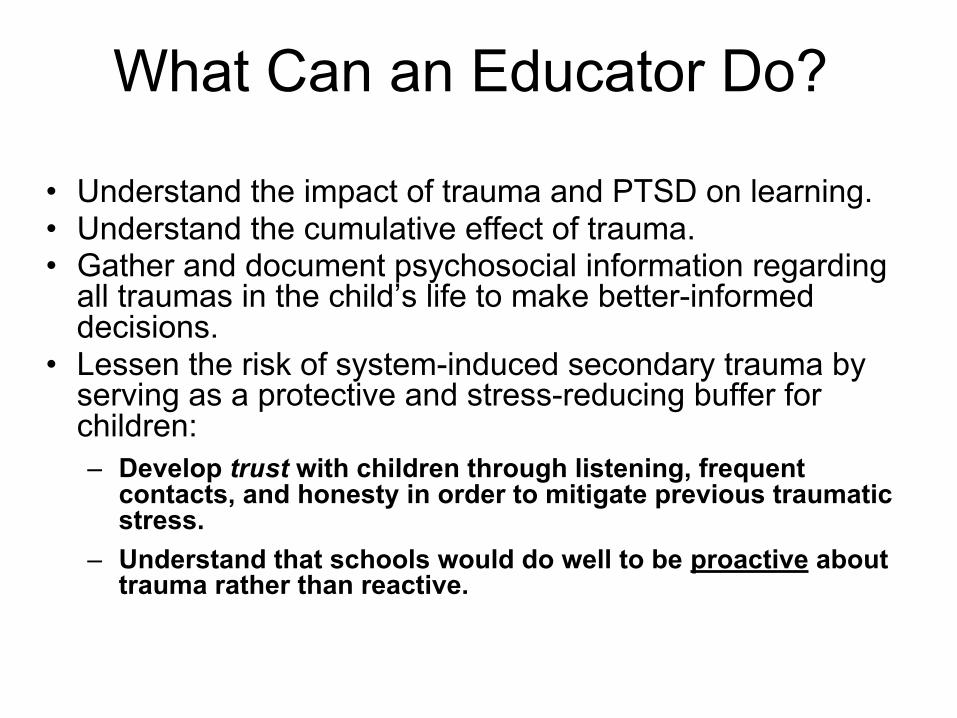
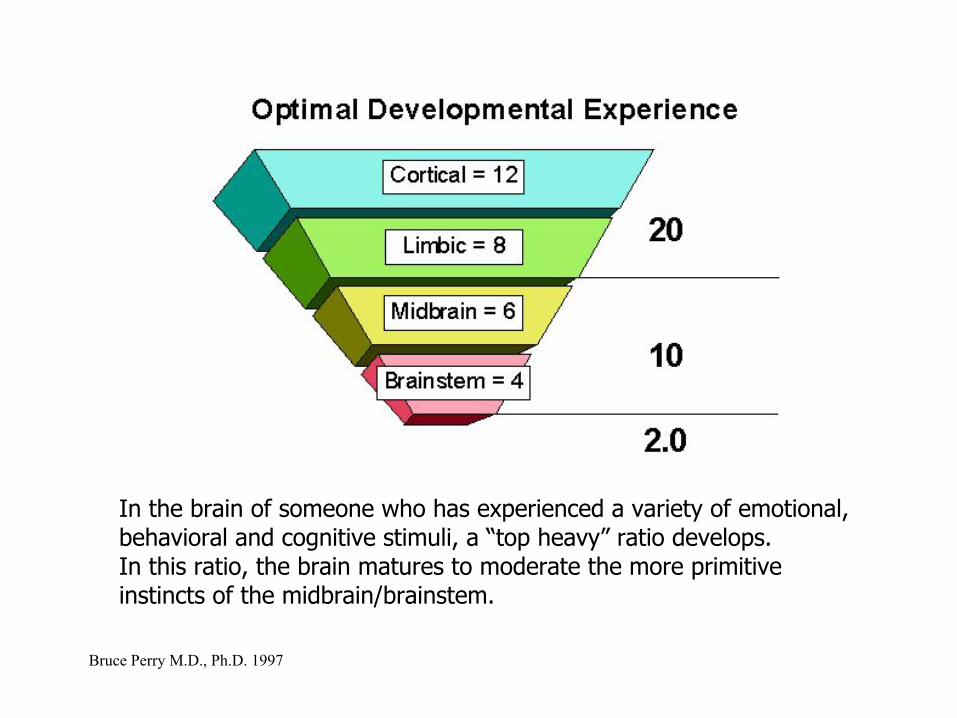
Hierarchy of Brain Function
Bruce Perry M.D., Ph.D. 1997
In the brain of someone who has experienced a variety of emotional, behavioral and cognitive stimuli, a “top heavy” ratio develops. In this ratio, the brain matures to moderate the more primitive instincts of the midbrain/brainstem.
Bruce Perry M.D., Ph.D. 1997

When key experiences (Which develop the cortical/limbic part of the brain)are absent or minimal, the “higher” to “lower” brain ratio is impaired. In this case, the ability of the brain to moderate impulsive, reactive responses and to work through frustration is diminished significantly.
Bruce Perry M.D., Ph.D. 1997

Children raised in environments characterized by domestic violence, physical abuse or other persistent trauma will develop an excessively active midbrain/brainstem. This results in an overly active and reactive stress response and a predisposition to aggression and impulsiveness.
Bruce Perry M.D., Ph.D. 1997

When the developing brain is both deprived of sensory stimuli and experiences traumatic stress, the brainstem/ midbrain to cortical/limbic ratio is profoundly altered.
Bruce Perry M.D., Ph.D. 1997

The Child’s BrainDifferences due to Psychological Trauma

MemoryNormally coordinated and cohesive
Explicit MemoryLeft Brain
• Facts• Details• Who, what,
where, when, how
• Tied to Language
Implicit MemoryRight Brain
• Emotional Memory• Senses-smells,
sounds, etc.• Tied to Fight, Flight,
Freeze Response

Memory and Traumatic Stress
I feel a certain wayand I don’t know why!!
Trauma UncouplesIntegration ofMemory

Fight/Flight/Freeze
• Overdevelopment of regions of the brain involved in anxiety and fear responses
And• Underdevelopment of regions of the brain
involved in complex thought and those necessary for learning.
Implications for Learning
• Traumatized children often spend so much time in the lower level brain in a state of persisting fear that they consistently focus on non-verbal vs. verbal cues
• May be very intelligent but can’t learn easily→must do verbal learning when calm
• •Learning needs to be more experience-based ⇒ → when traumatized children are stressed they are reactive/reflexive vs. accessing cognitive solutions

Implications for Behavior
• During early development, these traumatized children spent so much time in a low-level state of fear that they were focused primarily on non-verbal cues.
• Once out of such an environment, it is still difficult for the child's brain to interpret (relearn) these innocent looks and touches as benign.

These children are often labeled as learning disabled.
• Difficulties with cognitive organization contribute to a more primitive, less mature style of problem solving -- with violence often being employed as a "tool.“
• A traumatized child -- in a persistent state of arousal -- can sit in a classroom and not learn.
• The brain of this child has different areas activated -- different parts of the brain controlling his functioning.
• The capacity to internalize new verbal cognitive information depends upon having portions of the frontal and related cortical areas activated, which in turn requires a state of attentive calm.
• This is a state that the traumatized child rarely achieves.

Conduct Disorders
✴Behavior is the language of trauma.
✴Most children lack the language skills needed to describe how they are suffering, so they use behavior to express themselves.
✴Most behaviors used by children to express themselves are considered “negative” behaviors.

Cortical Modulation Is Age-Related
• The capacity to moderate frustration, impulsivity, aggression, and violent behavior is age-related.
• With sufficient motor, sensory, emotional, cognitive, and social experiences during infancy and childhood, the mature brain develops (in a use-dependent fashion) a mature, humane capacity to – tolerate frustration– contain impulsivity– channel aggressive urges.

Outcome
• When a child is threatened, he or she is likely to act in an "immature" fashion.
• Regression, a retreat to a less-mature style of functioning and behavior, is commonly observed in all of us when we are physically ill, sleep-deprived, hungry, fatigued, or threatened.
• When we regress -- in response to a real or perceived threat -- our behavior is mediated (primarily) by less-complex brain areas.

Baseline State of Arousal
▪ If a child has been raised in an environment of persistent threat, the child will have an altered baseline such that the internal state of calm is rarely obtained.
▪ The traumatized child will have a "sensitized" alarm response, over-reading verbal and non-verbal cues as threatening.
▪ Increased reactivity will result in dramatic changes in behavior in the face of seemingly minor provocative cues.
▪ Over-reading of threat will lead to a "fight or flight" reaction and impulsive violence.
▪ The child will view his violent actions as defensive.

Change in “thermostat”• Children exposed to significant threat will "re-set" their
baseline state of arousal such that even when no external threats or demands are present, they will be in a physiological state of persistent alarm.
• As external stressors are introduced (e.g., a complicated task at school, a disagreement with a peer) the traumatized child will be more "reactive."
• Even a relatively small stressor can instigate a state of fear or terror.
• The cognition and behavior of the child will reflect his or her state of arousal.

The Threat Recurs: Chronic Hyperarousal
▪ Traumatic Reenactment▪ Damages meaning, conscience, view of self and
others▪ Disrupted attachment – failed trust, failed
relationships▪ Problems with authority figures▪ Difficulties resolving conflicts▪ Inability to grieve▪ Addiction to stress▪ Resistance to change▪ Deterioration, alienation

Affective or Physiological Dysregulation
• Impaired developmental achievement related to arousal regulation:
�Mood�Bodily Functions�Diminished awareness of emotional
and behavioral states�Difficulty describing emotional or
bodily states

Students who have experienced complex trauma-
• Developmentally adverse interpersonal trauma for over one year, and exposure was before the age of 18.
• Subjective experiencing of: �Rage �Betrayal�Shame �Humiliation
Interconnected Framework for School Mental Health
Development of an Interconnected Systems Framework for School Mental Health February, 2012
Susan Barrett and Lucille Eber, National PBIS Center Partners; and Mark Weist, University of South Carolina University of Maryland, Center for School Mental Health)

Trauma-Sensitive School PBIS ModelTier 1

Trauma-Sensitive School PBIS ModelTier 1
✓School policies, culture & climate
✓Behavior management✓Instructional practices
& approaches✓Modeling✓Classroom consultation
TRAUMA SENSITIVESCHOOLTrauma Proofing CurriculumCompassionate SchoolEmotionally Safe SchoolPFA-Psychological First Aid

Physical Emotional(Stamina) (Resiliency /
empathy)
Intellectual
The Whole Learner
(Problem solving / creativity)
All components are interdependent

What’s “New” In The Context Of What’s “Old”?
• A trauma-sensitive school environment is characterized by respect and supports capable of “taking over” when the student’s coping skills fail.– Operationalization
• RtI• PBIS• Crisis/Disaster/Active Shooter Interventions• Violence Prevention/Bullying Programs• Character Education/Emotional Intelligence/Service
Learning• Stress Management/Yoga• Restorative Discipline/Justice

How We Become:
Office of the Superintendant of Public InstructionState of Washington

Ten Strategies of a Compassionate School
1. Focus on culture and climate in the school and community. 2. Train and support all staff regarding trauma and learning. 3. Encourage and sustain open and regular communication for
all. 4. Develop a strengths based approach in working with students
and peers. 5. Ensure discipline policies are both compassionate and
effective (Restorative Practices). 6. Weave compassionate strategies into school improvement
planning. 7. Provide tiered support for all students based on what they
need. 8. Create flexible accommodations for diverse learners. 9. Provide access, voice, and ownership for staff, students and
community. 10. Identify vulnerable students and outcomes and strategies

Domains of Compassionate Instruction
• Domain 1: Safety, Connection, and Assurance
• Domain 2 : Emotional and Behavioral Self-Regulation
• Domain 3: Competencies of Personal Agency, Social Skills, and Academic Skills

The Six Principles
1) Always Empower, Never Dis-empower2) Provide Unconditional Positive Regard3) Maintain High Expectations4) Check Assumptions, Observe, Question5) Be a Relationship Coach6) Provide Opportunities for Helpful
Participation

Another Curriculum for Traumatized Children
Connecting1 Safety2 Engaging3 Trusting
Processing4 Managing the self5 Managing feelings6 Taking responsibility
Adapting7 Developing social awareness8 Developing reflectivity9 Developing reciprocity
(Cairns, K. & Stanway, S., 2004.)

Step I - Safety First�� Stay aware of the terror�� Provide and sustain a relaxing environment�� Use self appropriately to deal with a terrified student:
voice, gestures, expression�� Use group work skills to create sense of safety�� Bring relaxation into the awareness of the child
and encourage practice�� Discourage dependence on high stimulus activities
• (Cairns, K. & Stanway, S., 2004.)

Step II - Engaging�� Provide appropriate environmental stimulation for
adults and students�� Learning about the effects of trauma is part of
good classroom management�� Stories and metaphors are powerful tools for
teaching about overwhelming events�� Encourage expression of experience and
development of emotional intelligence�� Bring dissociation into awareness, develop sense of
protector self and observer self

Step III - Trusting and Feeling�� Accept the level of trust the student has to offer�� Encourage open discussion of issues of trust�� Encourage the student to express inner states in
words, even though they will find this difficult�� Notice non-verbal signals of feelings and help student
to recognize and name what is happening�� Identify self-transcending as well as self-assertive
emotions

Step IV - Managing the Self�� Discuss and practice relaxation and soothing
activities with the student�� Avoid asking ‘why did you do that?’ Instead invite
reflection linking inner state with actions�� Encourage the student to be interested in their own
inner state with regard to their behavior�� Comment on small indicators of self-regulation�� Encourage students to build on growing capacity
for self-management

Procedures or Situations That May Trigger Prior Experiences of Trauma Include:
�Lack of control-powerlessness
�Threat or use of physical force
�Observing threats, assaults, others engaged in self-harm
�Isolation�Being in a locked room or
space�Physical restraints –or even
wristbands�Interacting with authority
figures
�Interacting with men, in general
�Lack of privacy�Removal of clothing –strip
searches, medical exams�Being touched –pat downs�Being watched �Loud noises�Fear based on lack of
information�Darkness Intrusive or
personal questions

Step V - Managing Feelings
�� Expect and contain disturbed behavior�� Encourage student to feel more in control -
space, time, activities�� Limit choices, restrict choice-making to less
stressful situations and celebrate successes�� Encourage student to recognize and
celebrate learning from mistakes

Step VI - Taking Responsibility
�� Recognize the power of traumatic identity andexpect resistance to changing identity
�� Provide choices about how they see themselves
�� Allow student to let go of excessive or inappropriate responsibilities
�� Encourage student to allow adults to be in control appropriately
�� Celebrate any evidence of the student takingappropriate responsibility for behavior

VII - Developing Social Awareness
�� Encourage friendships and social interaction�� Identify and rehearse social situations
requiring self-control in the student�� Encourage the student to broaden the range of
their social connections and to be interested in people generally
�� Promote activities motivating social accountability such as sport, drama, music

VIII - Developing Reflectivity�� Promote self-esteem; catch them doing
something good�� Provide and comment on role models of centered
people who are comfortable in their own lives�� Encourage the use of tools for reflection such as
keeping a diary�� Help students deal with feedback from a range of social
situations�� Be creative about ways to help the student become
fearlessly reflective

IX - Developing Reciprocity
• Provide and invite reflection on wide range of aesthetic experiences
• Share thoughts and feelings• Apologize when we hurt the student• Encourage the student to reflect on our
experience as well as their own• Invite the child to take our position - ‘What do
you think I should do about this?’ in response to student’s behavior
• Accept that we are a problem for the child

Trauma-Sensitive School PBIS ModelTier 2

Tier 2
✓Trauma assessment screening
DERS CPTSRI CANS CROPS/PROPS
Group Trauma Interventions TARGET SPARCS SSET
Sensory RegulationExperiential Therapies

Difficulties in Emotional Regulation Scale (DERS) (Gratz, K.L.)
• The DERS is a brief, 36-item, self-report questionnaire designed to assess multiple aspects of emotion dys-regulation.
• The measure yields a total score as well as scores on six scales derived through factor analysis: 1. Non-acceptance of emotional responses
(NONACCEPTANCE)2. Difficulties engaging in goal directed behavior (GOALS) 3. Impulse control difficulties (IMPULSE) 4. Lack of emotional awareness (AWARENESS) 5. Limited access to emotion regulation strategies
(STRATEGIES) 6. Lack of emotional clarity (CLARITY) Nearly all empirically validated treatments for child trauma seek to
make changes in the domain of emotion regulation, but there are few measures that assess this domain.

Group Interventions• Support for Students Exposed to Trauma (SSET)
Toolkit to manage stress and trauma: From National Child Traumatic Stress Network
• Structured Psychotherapy for Adolescents Responding to Chronic Stress (SPARCS)– For traumatized adolescents continually living with ongoing stress– Six domains of functioning to cope more effectively, make better
choices, and cultivate supportive relationshipsGoals:
• to help traumatized adolescents make better choices for their lives• to cultivate healthier relationships• to activate meaning making• to rouse mindful action• to teach tools for coping with current and future stressors• to promote healing

TARGET• Trauma Adaptive Recovery Group Education and Therapy
(TARGET)
• Objective: developed to help trauma survivors understand how trauma changes the body and brain’s normal stress response into a survival-oriented “alarm” reaction that can lead to posttraumatic stress disorder (PTSD).
• TARGET provides a practical skill-set that can be used by trauma survivors and family members to de-escalate and regulate extreme emotion states, to manage intrusive trauma memories, and to restore the capacity for information processing and autobiographical memory.
• TARGET teaches a sequence of seven (7) skills described as the FREEDOM steps.
• For ages 11-17
Trauma-Sensitive School PBIS ModelTier 3

Power and Control Strategies that are NOT Beneficial to a Traumatized
Student• Threats• Bribes• Control over bodily functions, like prohibiting
children from using the bathroom• Random enforcement of petty rules• Humiliation or degradation• Isolation• Corporal punishment

Tier 3Individual Trauma Interventions
TF-CBTCBITS (Child Behavioral Intervention for Trauma in SchoolsSensory Experiencing-SEADBT-SP (Adapted Dialectical Behavioral Therapy) Life Skills/Life Story SITCAP
Evidence-Based Trauma Interventions for Schools www.nctsn.org
http://www.nctsn.org/resources/topics/treatments-that-work/promising-practices

Resources
• Bluestein, J. (2001) Creating Emotionally Safe Schools: A guide for educators and parents. HCI
• Cairns, K. & Stanway, S., Learn the child - helping looked after children to learn: A good practice guide for social workers, carers and
teachers. London, England: BAAF• Coles, S. et al (2005) Helping Traumatized Children Learn: Supportive
School Environments for Children Traumatized by Violence. Boston: Massachusetts Advocates for Children / The Hale and Dorr Legal Services Center of Harvard Law School
• Craig, S. (2006) Reaching and Teaching Children Who Hurt: Strategies or your classroom. Paul Brookes Pub.
• Hart, S. and V. Hodson (2004) The Compassionate Classroom: Relationship based teaching and Learning Puddledancer Press
• Jaycox, L. et al.(2006) How Schools Can Help Students Recover from Traumatic Experiences: A Tool-Kit for Supporting Long-Term Recovery, RAND Corporation (TR-413), RAND Corp.
• Jaycox, L. (2003) CBITS: Cognitive-Behavioral Intervention for Trauma in Schools, Sopris West

Resources cont.• Levine, P. (2007) Trauma Through A Child’s Eyes: Awakening
the ordinary miracle of healing infancy to adolescence. Berkley, CA: North Atlantic Books
• Levine, P. and M. Kline (2008) Trauma-Proofing Your Kids. Berkley, CA: North Atlantic Books.
• Morrow, G. (1987) The Compassionate School: Educating abused and traumatized children. New York: Prentice-Hall.
• Wolpow, R. et al. Compassionate Schools: The heart of Learning and Teaching. Seattle: Office of the Superintendant of Public
Instruction State of Washington