Embed Size (px)
Citation preview

12-1
PCMH in the Direct Care System
Regina Julian, MHA, MBA, FACHECh, Primary Care, Access, Experience and Integration Defense Health AgencyPast Deputy Director of TMA Medical Management and Population [email protected]

12-2
Disclosures
• Presenter has no financial interests to disclose.
• This continuing education activity is managed and accredited by Professional Education Services Group in cooperation with the MedExcellence Program. PESG, and MedExcellence Staff, and accrediting organization do not support or endorse any product or service mentioned in this activity.
• PESG and MedExcellence Program staff has no financial interest to disclose.

12-3
Learning Objectives
1. Attendees will understand the reasons why governance selected the PCMH model of care and why those reasons still apply
2. Attendees will understand how performance has changed and the leading practices required to drive further improvement
3. Attendees will understand challenges and leadership priorities for both PCMH and the integrated delivery system.

12-4
Brief History Lesson The Journey What makes a successful PCMH? How do we compare to the
civilians? How Are We Doing? Service Specifics Challenges Governance Approvals Priorities and Way Ahead
Outline

12-5
Brief History Lesson
Variance Fragmented care - PCM Continuity was 30% Access issues Patients got lost - literally MHS PCMH Policy signed Sep 2009 directed
development of Army, Navy and Air Force PCMH operating instructions and implementation in all 440+ primary care clinics Common standards needed to drive consistency across all
Uniformed Services
5

12-6
The Journey
Tri-Service PCMH Advisory Board and Governance– Defense Health Agency role in leading collaboration
6

12-7
The Journey
Staffing models "Get Well" POM funding with ROI tied to common measures and
performance goals -- Enrollment per PCM-based resourcing (away from RVUs and churn)
Tri-Service Workflow forms with 18+ embedded clinical practice guidelines and prompts for preventive and other screening
Selection of NCQA industry "gold standard" to drive MHS PCMH transformation and meet Seven Core Principles through recognition
Access to Care Standards codified in law Embedded behavioral health specialist, clinical pharmacists and
physical therapists based on our most prevalent conditions Secure messaging and a 24-hour Nurse Advice Line implementation Identification and validation of new leading practices Training curricula (Service-Specific)
7

12-8
How do we compare to the civilians?
8
Measure PCPCC Reported Results Direct Care Results
ER Utilization Recapturable to Primary Care
Reduced; Multi-site/state examples range from -3.2% to -12%; Avg reduction 8.7%
Reduced 11%
Cost per ER VisitOne State Demo reported 3.5% cost
reduction per ER visit
Primary Care recapturable ER cost per visit up 2.7% (visits down, cost per visit is up);
cost per visit for true emergencies up 4.3% per visit
Recapturable ER Costs (for Primary Care reasons)
One state demo reported "reduced" ER costs
Reduced total costs 2.2% from $77M in FY13 to $75M in FY15 (we had fewer
visits but a higher cost per visit)
Patient SatisfactionMultiple State Demos reported "improved"
patient satisfactionAll Services and TROSS have either improved and/or are over 90%
Access to CareOne state demo reported 4% more
appointments
16% more primary care appointments per duty day available in Jan 16 due to Simplified
Appointing and capacity accountability by Services

12-9
How do we compare to the civilians?
9
Measure PCPCC Reported Results Direct Care Results
Inpatient Admissions per 1,000Reduced; Multi-site/state examples range from 1.7% to 25%; Avg reduction 11%
Reduced 15% from FY12 to FY15
Bed-Days per 1,000 Reduced 8% (NY) and 11% (MD) Reduced 12% from FY12 to FY15
Inpatient (IP) CostsAnthem (Multi-state demo) reduced costs
3.5%IP Claims reduced 12% FY12 to FY15
Primary Care UtilizationReduced; Multi-site/state examples range
from 2.7% to 17% reduction. One state demo had a 11% increase in utilization
Reduced 3.8%
ER Utilization (all ER visits)State demos' results range from "some
reduction" to -1.6% in Anthem multi-state demo and -22% in Oregon Medicaid demo
Total ER utilization down 7% (down 7% in direct care ER; down 5% in PSC ER)
CMS Response? “The most important, large-scale transformation….”

12-10
• Mean, median and variance all improved since MHS Review
Access to 24-Hour Appointments
10
Average Aug-14 Apr-16Change since MHS Review
Air Force 2.50 1.68 -33%Army 2.00 1.24 -38%NCR MD 2.80 1.33 -53%Navy 1.20 0.85 -29%Direct Care 2.00 1.32 -34%
August 2014 April 2016 ChangeMean in days 2.00 1.32 -34%Median in days 1.78 1.05 -41%Variance 1.42 0.74 -48%

12-11
• All ER visits for MTF enrollees decreased 11% overall since FY12
• Primary Care-sensitive/capturable network ER visits down 27% since FY12
• These visits account for 4% of all network ER visits and 2% of costs
11
ER Visits for Primary Care Reasons
12-12
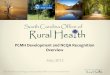
• PMCHs contributed to lower inpatient dispositions and fewer bed days per MTF enrollee through comprehensive, coordinated care
• Since FY12, inpatient dispositions 19%; 11% for diabetes-related admissions
Reducing Unnecessary Inpatient Utilization
12

12-13
• MTFs deliver 93% of MTF enrollee primary care workload• 88% in PCMH and 4% in after-hours MTF ER/UC Fast Tracks• 8% delivered in network (<.2% ER and 8% UCCs)
• Next step: Increase convenience for our patients and improve their MTF continuity by expanding extended hours and direct care UC Fast Tracks (integrated virtually PCMH through colleague to colleague secure messaging, etc.)
Primary Care Market Share
13

12-14
Leading Practices
Team-based demand management to enhance access beyond face-to-face encounters with PCM• Pre-visit planning/scrub templates - Focus on proactive, comprehensive
care (vs. fragmented, episodic)⁻ Virtual health and Telephone Visits⁻ Nurse-run walk-in clinics for common acute conditions⁻ Proactive high utilizer outreach⁻ Fully utilize embedded specialists and MM, especially for high utilizers
Simplified Appointing Guidance and First Call Resolution₋ Two appointment types₋ “When would you like to be seen” – See Today’s Patients Today₋ Match supply and demand by time of day/day of week where
economically feasible
14

12-15
What makes a successful PCMH? Engaged Leadership PCMH Management and Oversight
• Commitment to continuity• Utilization of TSWF• Robust use of team-based workflow and Nurse/Tech SSP (GS and
other performance plans rated on use of team-based workflow)• Active promotion of all team members on use of enhanced access
tools (NAL, SM, internal BH) • Adequate, standard training on processes, roles and
responsibilities as well as periodic refresher and follow-up (accountability)
• Training / Roles and Responsibilities• Full commitment to accept walk in during duty hours (including NAL
pts) Patient education / orientation Active presence on Social Media and Patient Advocate
15

12-16
Examples
Hickam- resiliency training for minor illnesses with a special card for the pharmacy
Martin ACH - Direct Care Acute Care Clinic tied to the PCMHs
NH Pensacola- specialty care booking in the primary care clinic at the time of the referral
Colorado eMSM- multidisciplinary pain team in the market showing a 60% improvement in getting patients off of narcotics, or using less narcotics
16

12-17
• Primary care annual utilization is higher than the national average in an insured population (CDC)
• 48% of enrollees have 5 or more visits per year - address utilization through team-based approach
• Develop standard processes to meet patient needs beyond a face-to-face appointment virtually via PCM phone call, T-Con, standard booking protocols for needs that do not require an appointment
• Leading practices demonstrated 40%+ reduction in high ER users through personalized intervention by embedded BH and Medical Management
“Seeing a Provider When Needed” - Challenge
17

12-18
Changing Landscapeof Healthcare
18
0.30
0.35
0.40
0.45
0.50
0.55
0.60
2.50
3.00
3.50
4.00
4.50
5.00
% A
cute
App
oint
men
ts I
n Sc
hedu
les
ED
Util
izat
ion
per
100
Enr
olle
d
ER Utilization and Acute Appointment Availability Trends
ED Utilization ED Use Target ≤ 3.7
% Acute Appointments

12-19
Challenges
Demand and public perception of MHS/access Utilization is more than double the civilian sector
Urgent Care Pilot despite recent Health Affairs study showing UCC create a new demand, and do not decrease ER demand
Staff Change fatigue Hiring and other Staffing Challenges IT system limitations … and MHS Genesis Resources Mobility of our staff and our patients NDAA 2016 (Patient Experience) and 2017
19

12-20
Recent Governance-Approved Activities (MDAG)
• PCMH is the direct care system model of primary care• TSWF to be used to document screening in all primary
care encounters• Third Next Appointment Changes• TJC to recognizes/certify PCMHs• Global NAL• Secure messaging to remain in place until MHS Genesis
portal on-line• Tri-Service standard PCMH, access and customer service
training• Specialty Appointing and Referral Policy• Codify other leading practices into Tri-Service guidance
20

12-21
New Specialty Care Access Measures
• Governance recommends two specialty care access measures to evaluate the patient experience with the specialty appointing process• Number of Days from Consult to CHCS Appointing; and • Number of Days from CHCS Appointing to Appointment (Days to
SPEC)
21
AB
A: Avg 12 daysB: Avg 14 days
12-22
Tri-Service Prioritiesand Way Ahead
• PCMH is the foundation of what we do • Integration underway to standardize patient-centered
specialty care• Tri-Service Priorities
• Optimize by implementing best practices• Training – from Leadership to staff• Improve patient experience• Increase convenience• Leverage telehealth• Focus on the health of our population• Make the Direct Care system care location “of choice”
12-23
Back Up SlidesService Initiatives
23

12-24
Medical Home Port
Navy Medicine (BSO-18) currently operates 188 primary care practices with 264 teams across 119 MTFs.
24
Practice Type MEPRS Practices
Internal Medicine BAA/BAZ 5/10Family Medicine BGZ 87Pediatrics BDZ 16Primary Care (AD Only and Training) BHA 40
Flight Medicine BJA 26Undersea Medicine BKA 4
Expanded from nine Pilot locations to 19 new MHPs last year with deployment of 17 additional MCMH and two FCMH practices.

12-25
Navy Operational Medical Home
25
Pilot FCMH Locations 2015 Implementation SitesLocation # of Teams Location # of
Teams
NAS Whidbey Island, WA 2 NAS Lemoore, CA 1
NAS North Island, CA 1 NS Bangor, WA 1
NS Gulfport, MS* 1
Pilot MCMH Locations 2015 Implementation SitesLocation # of
TeamsLocation # of
Teams
MCB Camp Lejeune, NC (French Creek)
1 MCAS Beaufort, SC 2
MCAS Cherry Point, NC 2 MCB Camp Lejeune, NC(Courthouse Bay & Hadnot Point)
2
MCB Camp Pendleton, CA (62 Area) 1 MCAS New River, NC 2
MCAS Miramar, CA 2 MCB Camp Pendleton, CA(Areas 21, 22, 33, 41, 43 & 53)
7
MCB Okinawa, JA (Hansen & Kinser) 2 MCAS Yuma, AZ 1
MCB 29 Palms, CA 2
MCB Okinawa, JA(Courtney, Foster, Futenma & Schwab)
4
MCAS Iwakuni 1
*FCMH Gulfport received NCQA PCMH Level 3 recognition in 2015, and was the first to receive recognition within the MHS

12-26
• 136 AMHs (PCMH, CBMH and SCMH)• > 44 “pure” SCMHs
• TRADOC and USASOC SCMHs in implementation phases• Nurse Advice Line (NAL)
• Tremendous growth (i.e., FT Hood and FT Bragg)• Adjunct to face-to-face encounters• Access during off-duty hours/weekends/holidays
• Telehealth initiatives• ED: FT Campbell pilot ongoing• At-Home: OPORD being drafted• Remote Monitoring (disease monitoring): JBLM pilot
implementation• Secure Messaging• Huddle Tool
AMH Status

12-27
AF Patient Centeredness
• IOM 2001 Crossing the Quality Chasm• “Care that is respectful of and responsive to individual
patient preferences, needs, and values and ensures that patient values guide all clinical decisions”
• Trusted Care CONOPS; Patient Centeredness• AFMS places the patient at the center of everything it does• AFMS defines value from the patient perspective• AFMS anticipates the patient’s expectations and excels in
every aspect of the patient experience• Patients are enabled, informed, and empowered to actively
engage in the delivery of their care and the systems that support it
• Multiple Lines of Effort/ Initiatives to launch in 2016-2017
27

12-28
Patient Activation
28
Activated and Engaged Patients are Indispensable Partners on the Road to High Reliability “Trusted Care” with Zero Harm
DoD Patient Activation Reference Guide, 2013