Embed Size (px)
DESCRIPTION
PD prescription present 4-8-52
Citation preview
PrescriptionPrescription peritoneal dialysis peritoneal dialysis
Pantipa Tonsawan, MD
Case Case
Female , 50 yrs, ESRD Female , 50 yrs, ESRD ตั�ดสิ�นใจเลื�อก ตั�ดสิ�นใจเลื�อก PD PD
BW 50 kg , Ht 155 cm BW 50 kg , Ht 155 cm ((BSA 1.50m2, BSA 1.50m2, GFR 2ml/min =GFR 2ml/min = CCr 20L/wkCCr 20L/wk แลืะ แลืะ Kt/V = Kt/V = 0.5 /wk0.5 /wk ) ) เคยประเมิ�น เคยประเมิ�น PET PET อย��ในกลื��มิ อย��ในกลื��มิ low low average transport average transport ถ้�าตั�องการสิ��งการร�กษาถ้�าตั�องการสิ��งการร�กษาเป�นไปตัามิ เป�นไปตัามิ NKF-DOQI NKF-DOQI ((weely CCr ≥ weely CCr ≥ 60L/1.73m260L/1.73m2 ) ) จะตั�องสิ��งการร�กษาอย�างไรจะตั�องสิ��งการร�กษาอย�างไร
ESRD ??????ESRD ??????
Mode PD Vs HDMode PD Vs HD PD :CAPD or APDPD :CAPD or APD APD : CCPD, NIPD TPDAPD : CCPD, NIPD TPD Prescribe?? :Dwell time , fill volume Prescribe?? :Dwell time , fill volume
, cycle, tidal volume , cycle, tidal volume Follow up : lab, adequacyFollow up : lab, adequacy
Indication / Contraindications Indication / Contraindications of PDof PD
80% of patients have no contra-80% of patients have no contra-indication to any of the dialysis indication to any of the dialysis methods and may choose according to methods and may choose according to their life style between HD their life style between HD oror PD PD
Absolute contra-indicationsAbsolute contra-indications of PD: of PD: 1.peritoneal fibrosis and adhesions 1.peritoneal fibrosis and adhesions
following intrafollowing intra--abdominal operations abdominal operations 2.inflammatory gut diseases 2.inflammatory gut diseases
pleuro-peritoneal pleuro-peritoneal leakageleakage (Hydrothorax) (Hydrothorax)
herniahernia significant loin painsignificant loin pain big polycystic kidneys big polycystic kidneys
Relative Relative CContraontra--indications of PDindications of PD
• severe deformity arthritis • psychosis• significant decrease of lung
functions
* diverticulosis
• colostomy • obesity
• blindness
PD :Advantage PD :Advantage
Preserve residual renal functionPreserve residual renal function Control acid- baseControl acid- base HD stableHD stable No vascular accessNo vascular access Control HTControl HT No anticoagulantNo anticoagulant
Why toWhy to start with PD ?
Clinical outcomes comparable to HD, no difference
Saves vascular access Preferred for children (APD) Modality choice is a lifestyle
issue Control HT
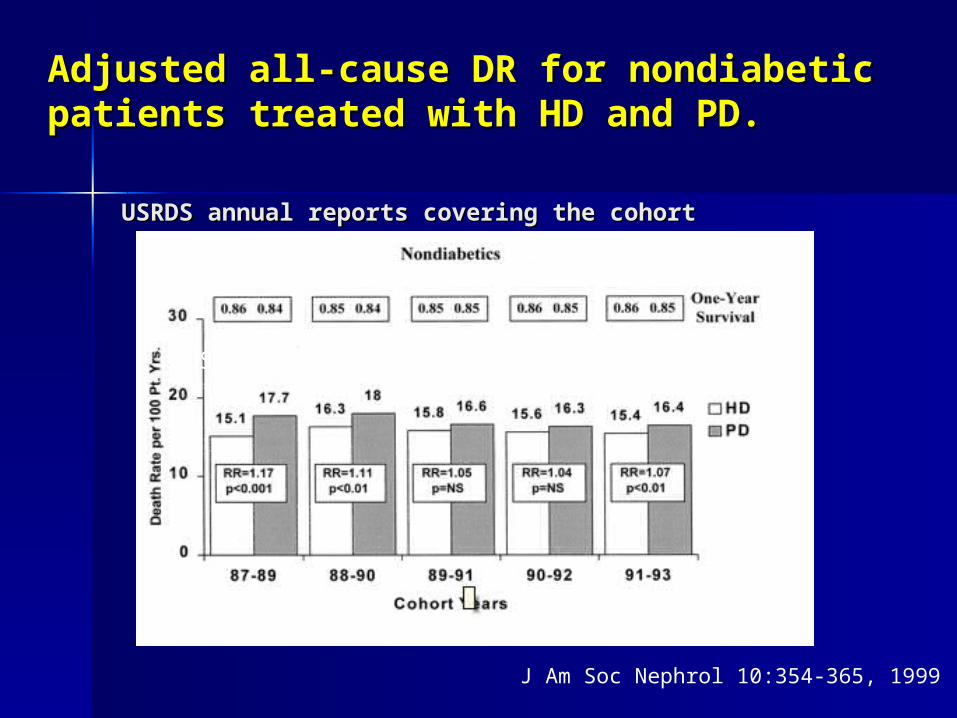
USRDS annual reports covering the cohortUSRDS annual reports covering the cohort
Adjusted allAdjusted all--cause DR for nondiabetic cause DR for nondiabetic patients treated with HD and PDpatients treated with HD and PD..
J Am Soc Nephrol 10:354-365, 1999
USRDS annual reports covering the cohort
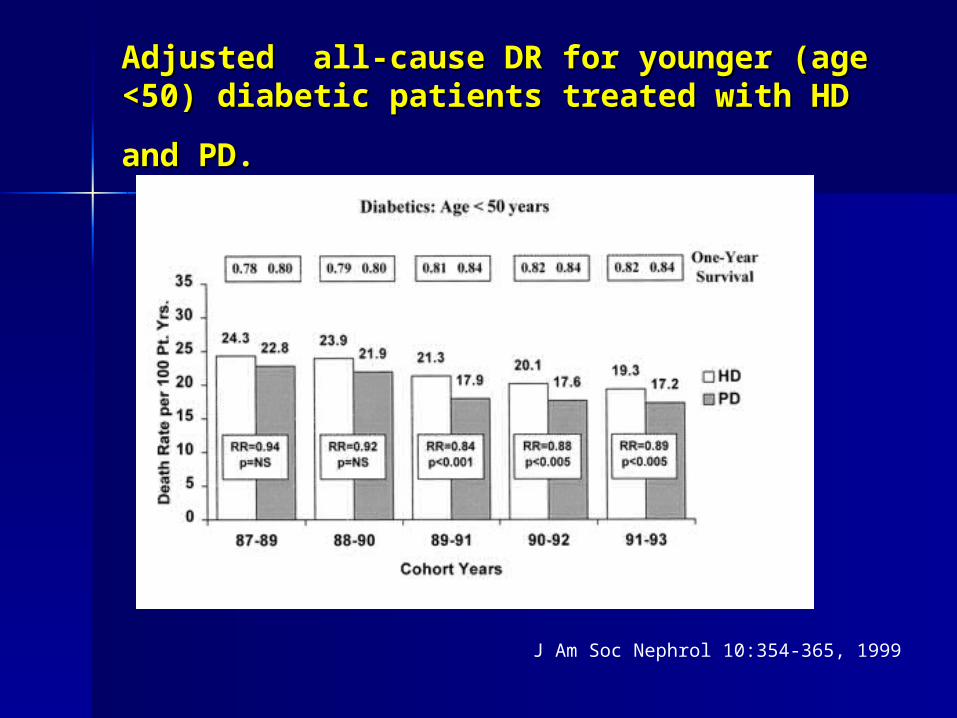
Adjusted allAdjusted all--cause DR for younger cause DR for younger ((age age <50<50 ) ) diabetic patients treated with HD diabetic patients treated with HD
and PDand PD..
J Am Soc Nephrol 10:354-365, 1999
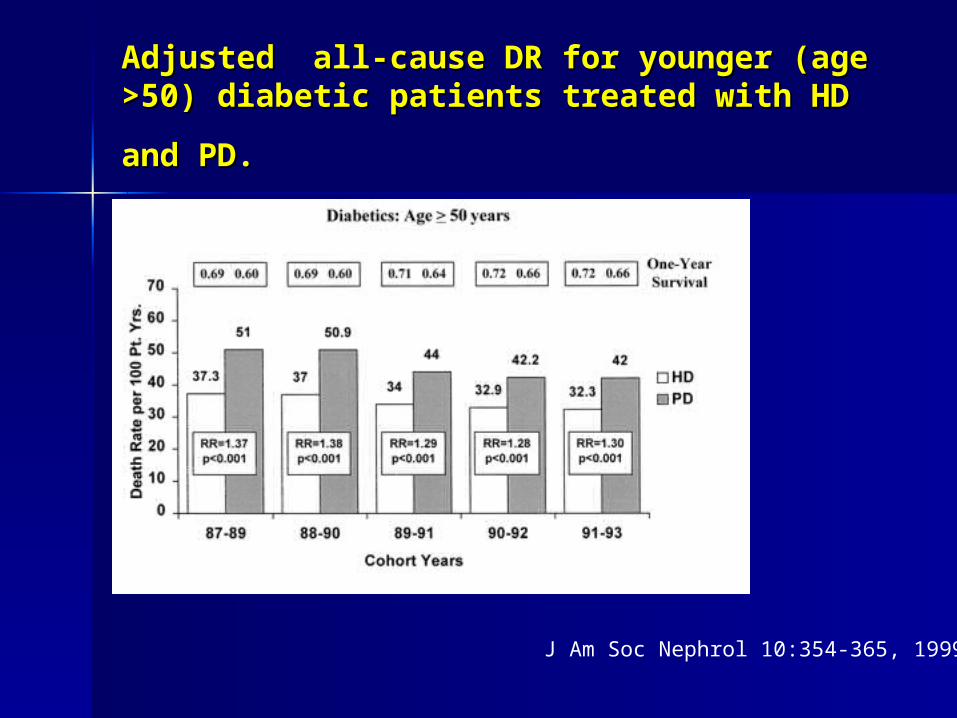
J Am Soc Nephrol 10:354-365, 1999
Adjusted allAdjusted all--cause DR for younger cause DR for younger ((age age >50>50 ) ) diabetic patients treated with HD diabetic patients treated with HD
and PDand PD..
Mortality studies comparing peritoneal Mortality studies comparing peritoneal dialysis and hemodialysisdialysis and hemodialysis : : what do they what do they
tell us?tell us? Total of six largeTotal of six large--scale registry studies & three prospective scale registry studies & three prospective
cohort studies conducted in the United States cohort studies conducted in the United States ((USUS)), Canada, , Canada, Denmark, and the Netherlands were reviewedDenmark, and the Netherlands were reviewed . .
PD PD was generally found to be associated was generally found to be associated with equal or betterwith equal or better survival among survival among nonnon--diabetic patients and younger diabeticdiabetic patients and younger diabetic patientspatients
older diabeticolder diabetic patients, patients, results variedresults varied by country by country Canadian & Danish :Canadian & Danish :no difference in survivalno difference in survival between PD & between PD &
HDHD US, HD associated with better survival for diabetics aged 45 US, HD associated with better survival for diabetics aged 45
and olderand older
Kidney Int SupplKidney Int Suppl 2006 1. Nov;( 2006 1. Nov;(-03 311):S .-03 311):S .
Conclude Conclude
overall patient survival is similar for PD overall patient survival is similar for PD & HD & HD but that important differences do exist but that important differences do exist within select subgroups of patients, within select subgroups of patients, particularly those subgroups defined by age particularly those subgroups defined by age and the presence or absence of diabetesand the presence or absence of diabetes..
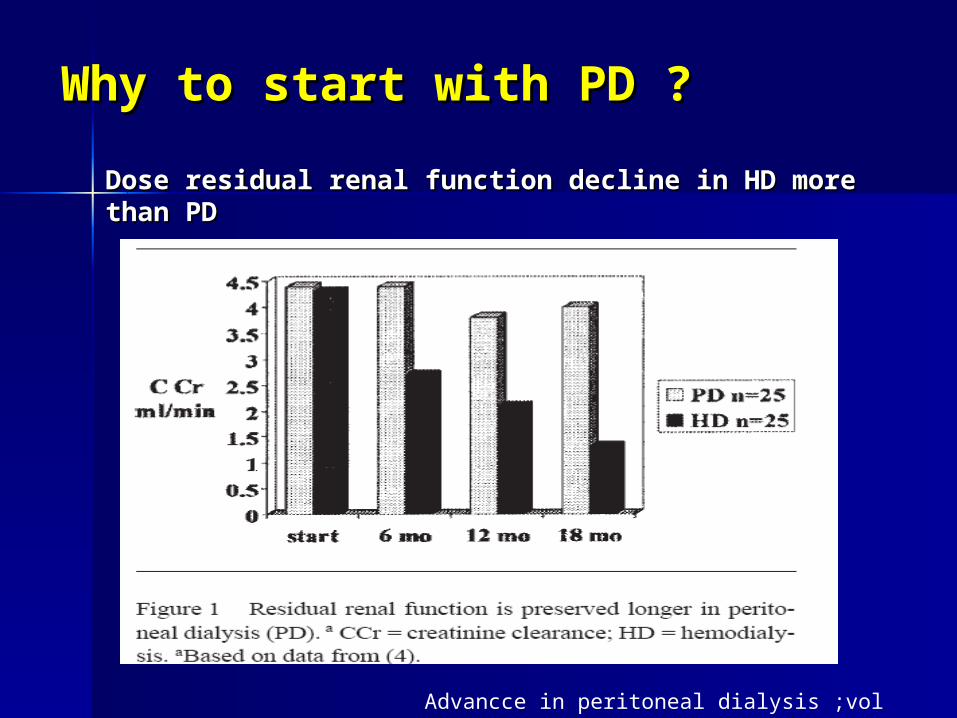
Dose residual renal function decline in HD more Dose residual renal function decline in HD more than PDthan PD
Advancce in peritoneal dialysis ;vol 20 ;2004
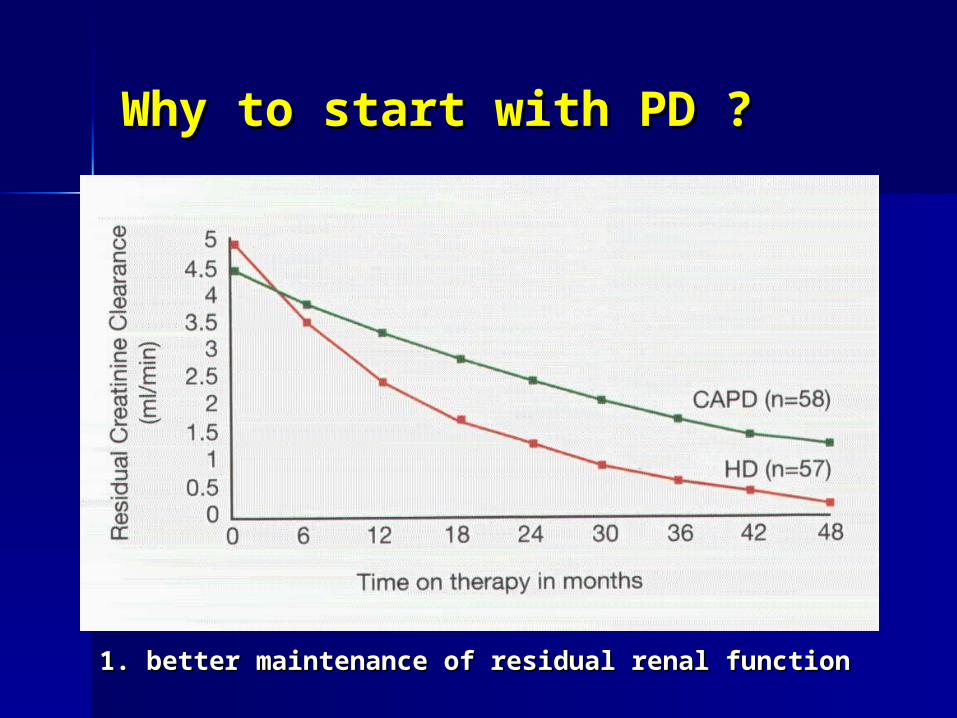
Why to start with PD ?Why to start with PD ?
Why to start with PD ?Why to start with PD ?
1. better maintenance of residual renal function1. better maintenance of residual renal function
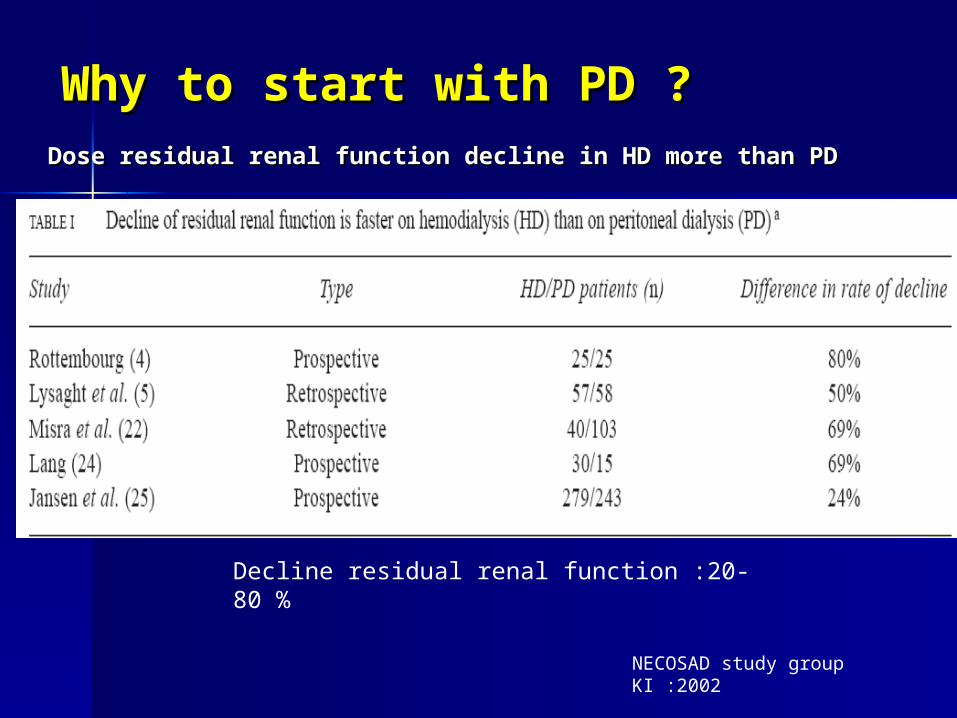
NECOSAD study group KI :2002
Why to start with PD ?Why to start with PD ?Dose residual renal function decline in HD more than PDDose residual renal function decline in HD more than PD
Decline residual renal function :20-80 %
SELECTION OF DIALYSIS MODALITYSELECTION OF DIALYSIS MODALITY
PD/HDPD/HD Indication & ContraindicationIndication & Contraindication PreferPrefer Family member, care giverFamily member, care giver Underlying disease Underlying disease Socioeconomic statusSocioeconomic status
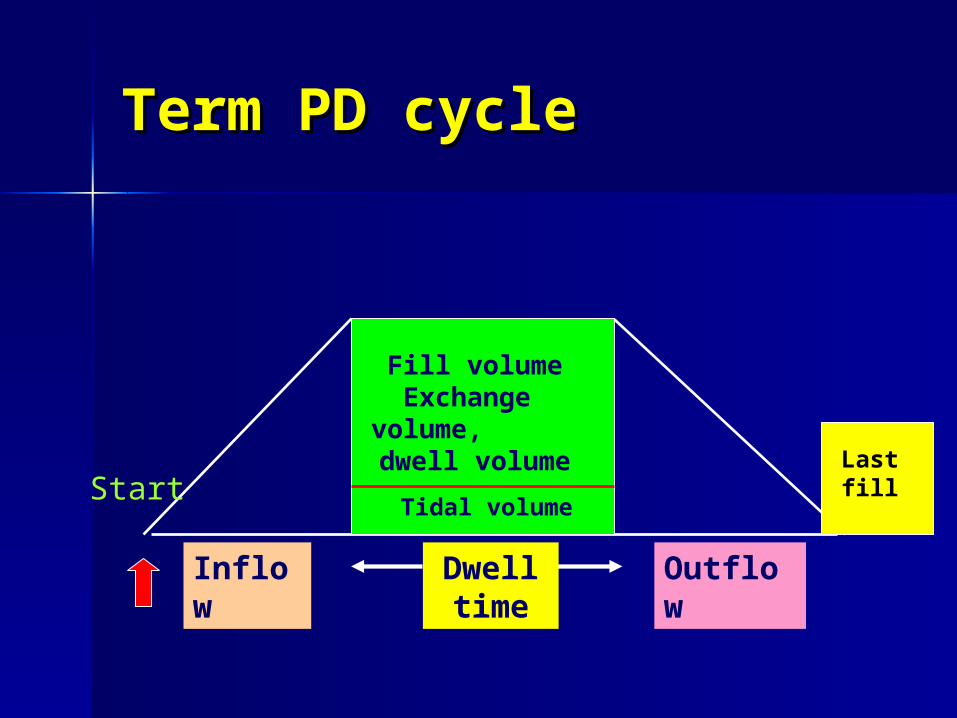
Term PD cycle Term PD cycle
Inflow
Outflow
Dwell time
Fill volume Exchange
volume, dwell volume
Tidal volumeStart
Last fill
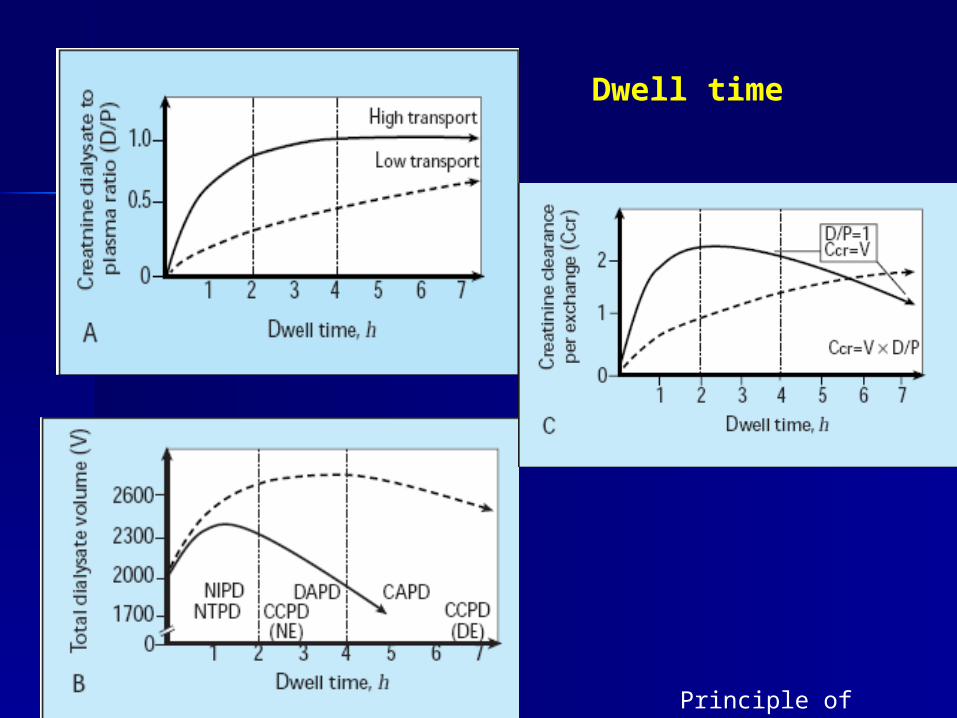
Dwell time
Principle of dialysis
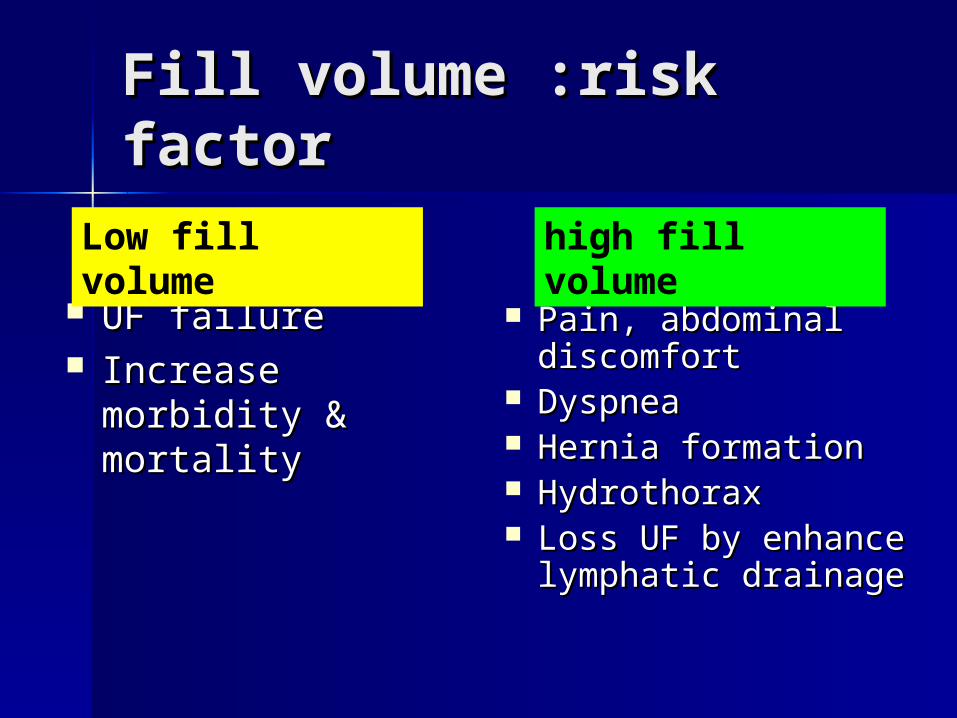
Fill volumeFill volume :risk factor:risk factor
UF failureUF failure Increase Increase
morbidity & morbidity & mortalitymortality
Pain, abdominal Pain, abdominal discomfortdiscomfort
DyspneaDyspnea Hernia formationHernia formation HydrothoraxHydrothorax Loss UF by enhance Loss UF by enhance
lymphatic drainagelymphatic drainage
Low fill volume high fill volume
Tidal volumeTidal volume
Increase amount ;diffusionIncrease amount ;diffusion Increase : toxin removalIncrease : toxin removal
Inflow + outflow: limit Inflow + outflow: limit
Depend of catheter resistant or Depend of catheter resistant or obstructionobstruction
GravityGravity Drain volumeDrain volume
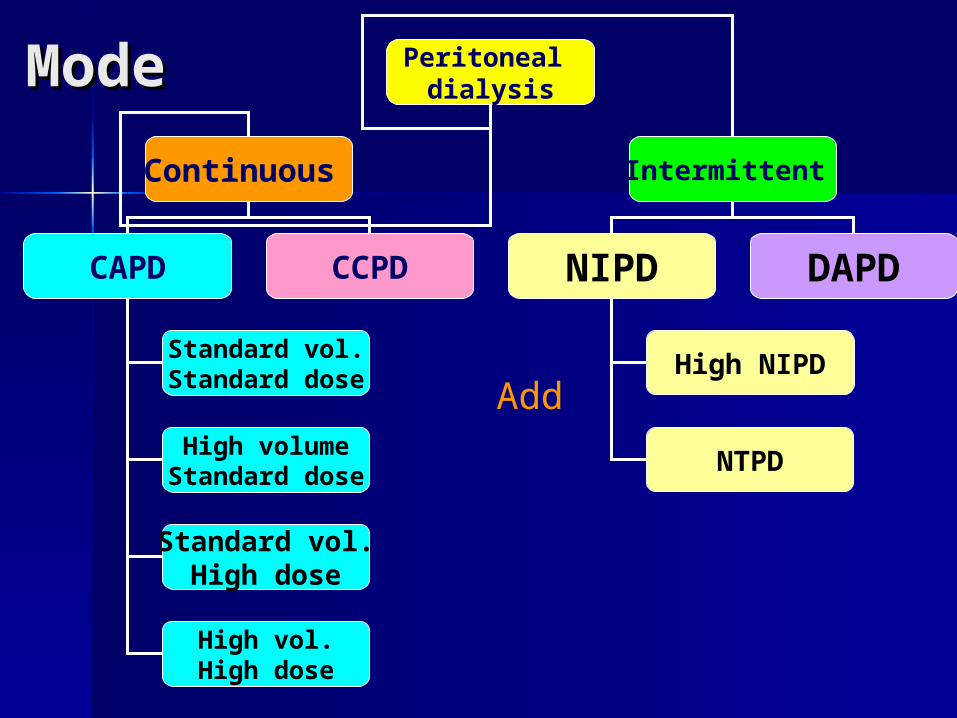
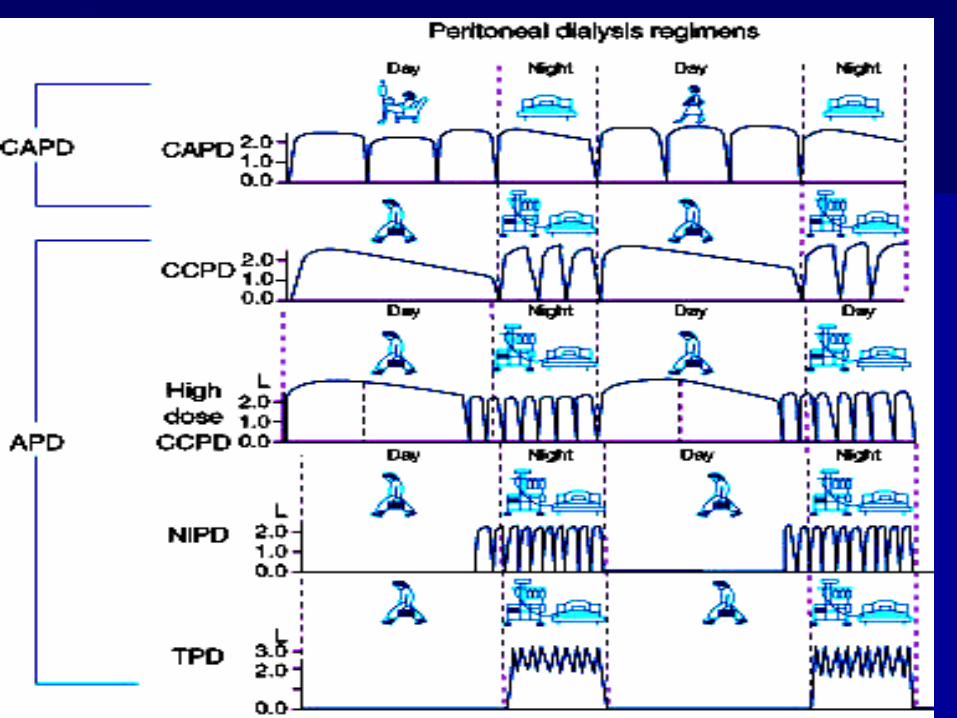
ModeMode Peritoneal dialysis
Continuous Intermittent
CAPD CCPD NIPD DAPD
Standard vol.Standard dose
High volumeStandard dose
Standard vol.High dose
High vol.High dose
High NIPD
NTPD
Add
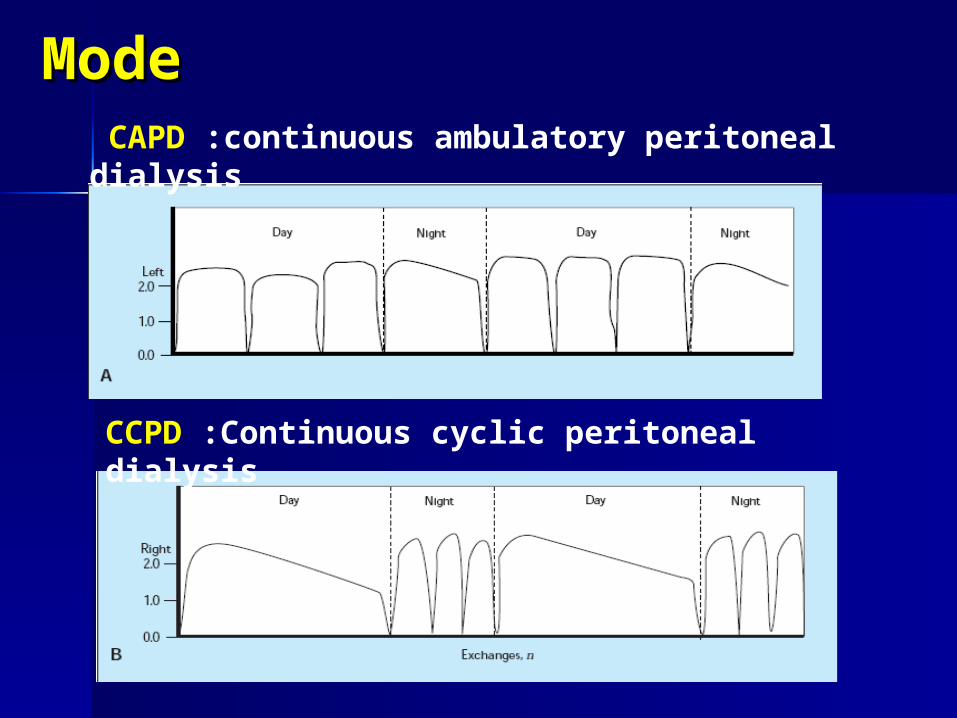
ModeMode
CCPD :Continuous cyclic peritoneal dialysis
CAPD :continuous ambulatory peritoneal dialysis
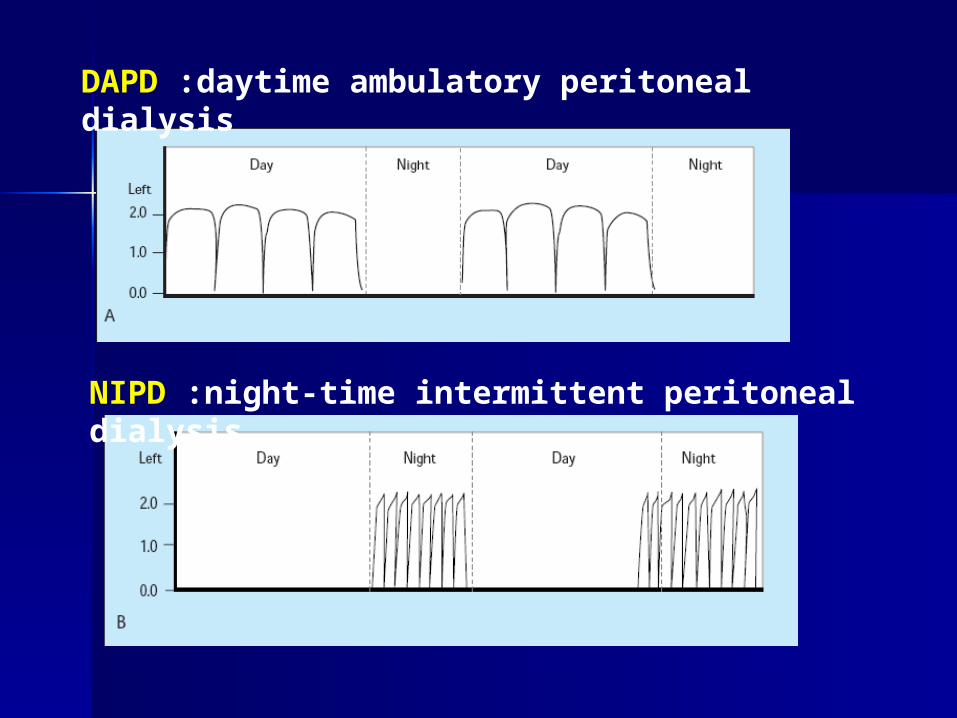
DAPD :daytime ambulatory peritoneal dialysis
NIPD :night-time intermittent peritoneal dialysis
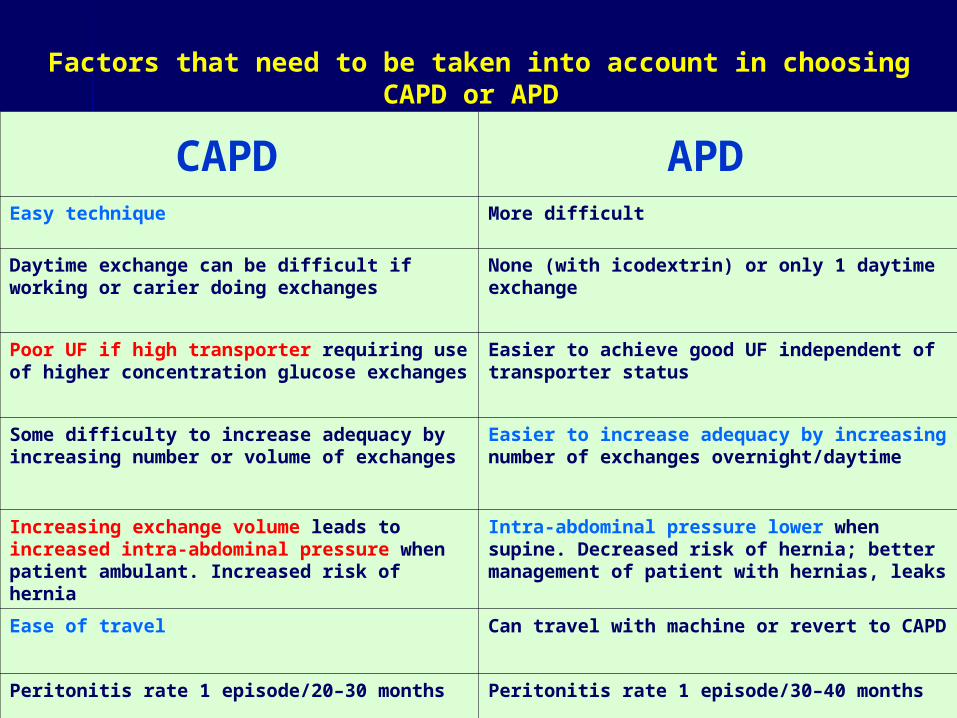
Factors that need to be taken into account in choosing CAPD or APD
CAPD APD Easy technique More difficult
Daytime exchange can be difficult if working or carier doing exchanges
None (with icodextrin) or only 1 daytime exchange
Poor UF if high transporter requiring use of higher concentration glucose exchanges
Easier to achieve good UF independent of transporter status
Some difficulty to increase adequacy by increasing number or volume of exchanges
Easier to increase adequacy by increasing number of exchanges overnight/daytime
Increasing exchange volume leads to increased intra-abdominal pressure when patient ambulant. Increased risk of hernia
Intra-abdominal pressure lower when supine. Decreased risk of hernia; better management of patient with hernias, leaks
Ease of travel Can travel with machine or revert to CAPD
Peritonitis rate 1 episode/20–30 months Peritonitis rate 1 episode/30–40 months
PD – First prescriptionPD – First prescription
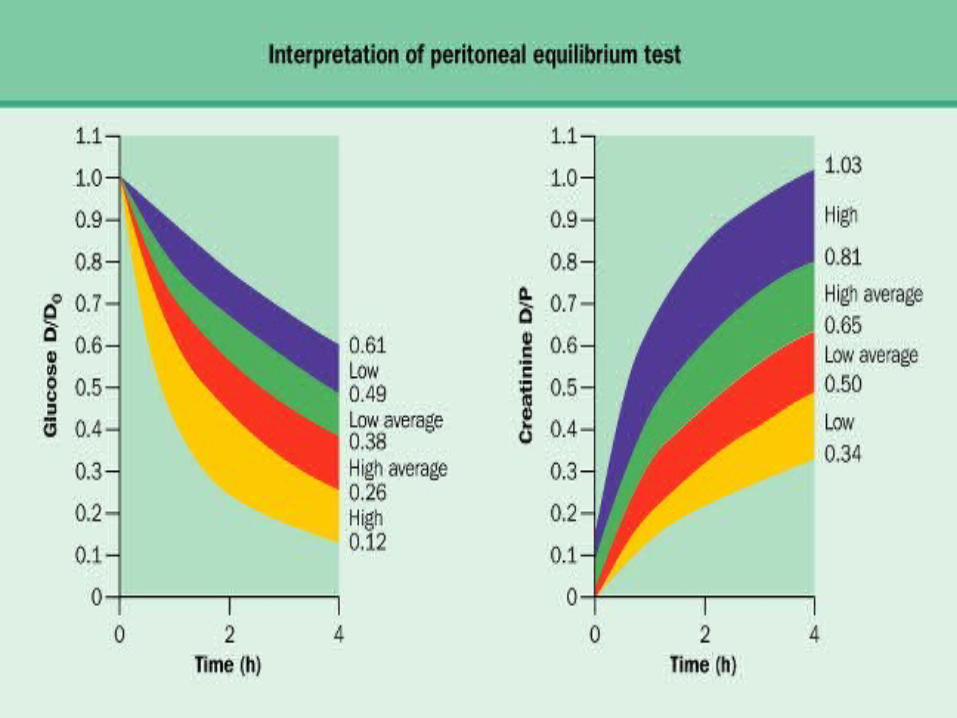
Consider;Consider;– Size – BSASize – BSA– Residual renal functionResidual renal function– PET – but only if you can PET – but only if you can tell the tell the
futurefuture– Mode :CAPD or APDMode :CAPD or APD
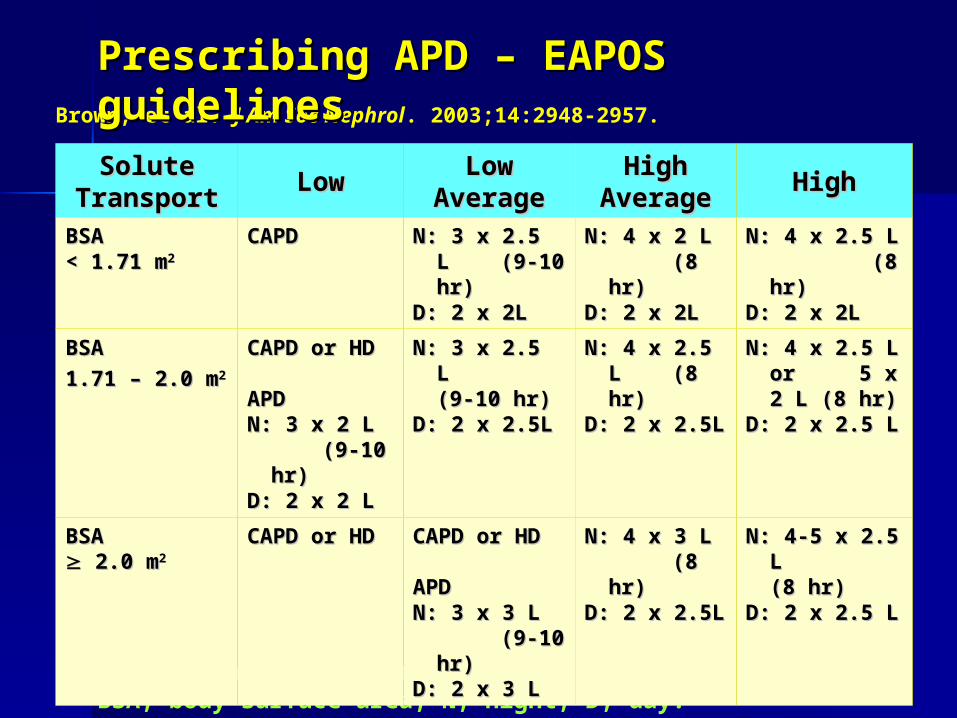
Solute transport determined by PET.BSA, body surface area; N, night; D, day.
Brown, et al. J Am Soc Nephrol. 2003;14:2948-2957.
Prescribing APD – EAPOS Prescribing APD – EAPOS guidelinesguidelinesSolute Solute
TransportTransport LowLow Low Low AverageAverage
High High AverageAverage HighHigh
BSA BSA < 1.71 m< 1.71 m22
CAPDCAPD N: 3 x 2.5 L N: 3 x 2.5 L (9-10 hr) (9-10 hr)
D: 2 x 2LD: 2 x 2L
N: 4 x 2 L N: 4 x 2 L (8 hr) (8 hr)
D: 2 x 2LD: 2 x 2L
N: 4 x 2.5 L N: 4 x 2.5 L (8 hr) (8 hr)
D: 2 x 2LD: 2 x 2L
BSA BSA
1.71 – 2.0 m1.71 – 2.0 m22
CAPD or HDCAPD or HD
APD APD N: 3 x 2 L N: 3 x 2 L
(9-10 hr) (9-10 hr)D: 2 x 2 LD: 2 x 2 L
N: 3 x 2.5 L N: 3 x 2.5 L (9-10 (9-10 hr)hr)
D: 2 x 2.5LD: 2 x 2.5L
N: 4 x 2.5 L N: 4 x 2.5 L (8 hr) (8 hr)
D: 2 x 2.5L D: 2 x 2.5L
N: 4 x 2.5 L N: 4 x 2.5 L or 5 x 2 or 5 x 2 L (8 hr)L (8 hr)
D: 2 x 2.5 LD: 2 x 2.5 L
BSA BSA 2.0 m2.0 m22
CAPD or HDCAPD or HD CAPD or HDCAPD or HD
APD APD N: 3 x 3 L N: 3 x 3 L
(9-10 hr) (9-10 hr)D: 2 x 3 L D: 2 x 3 L
N: 4 x 3 L N: 4 x 3 L (8 hr) (8 hr)
D: 2 x 2.5L D: 2 x 2.5L
N: 4-5 x 2.5 N: 4-5 x 2.5 L (8 L (8 hr)hr)
D: 2 x 2.5 L D: 2 x 2.5 L
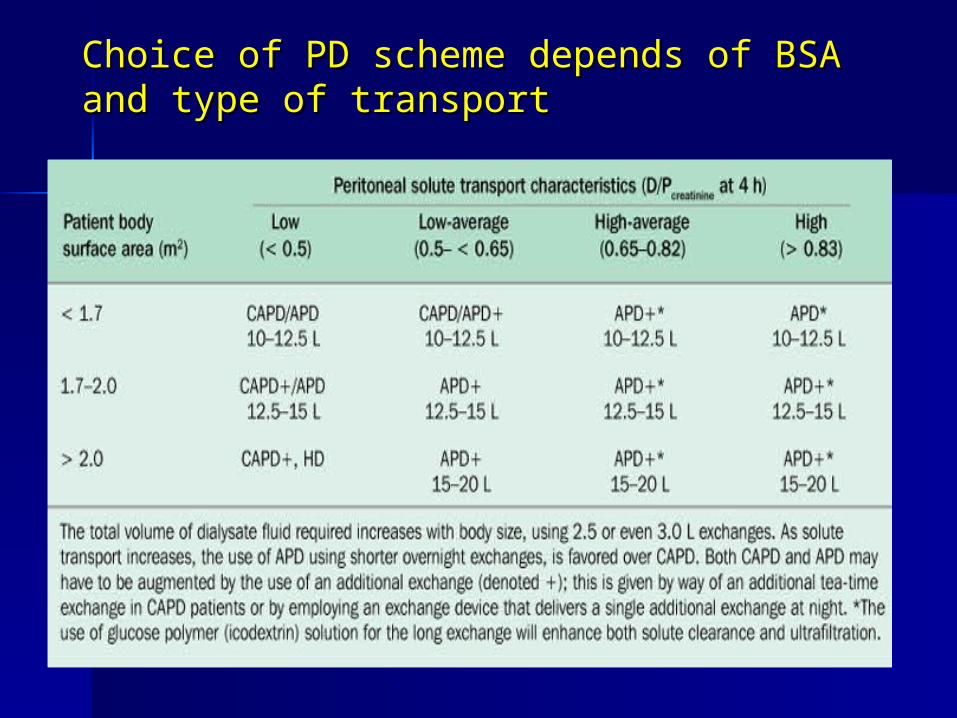
Choice of PD scheme depends of BSA and Choice of PD scheme depends of BSA and type of transporttype of transport

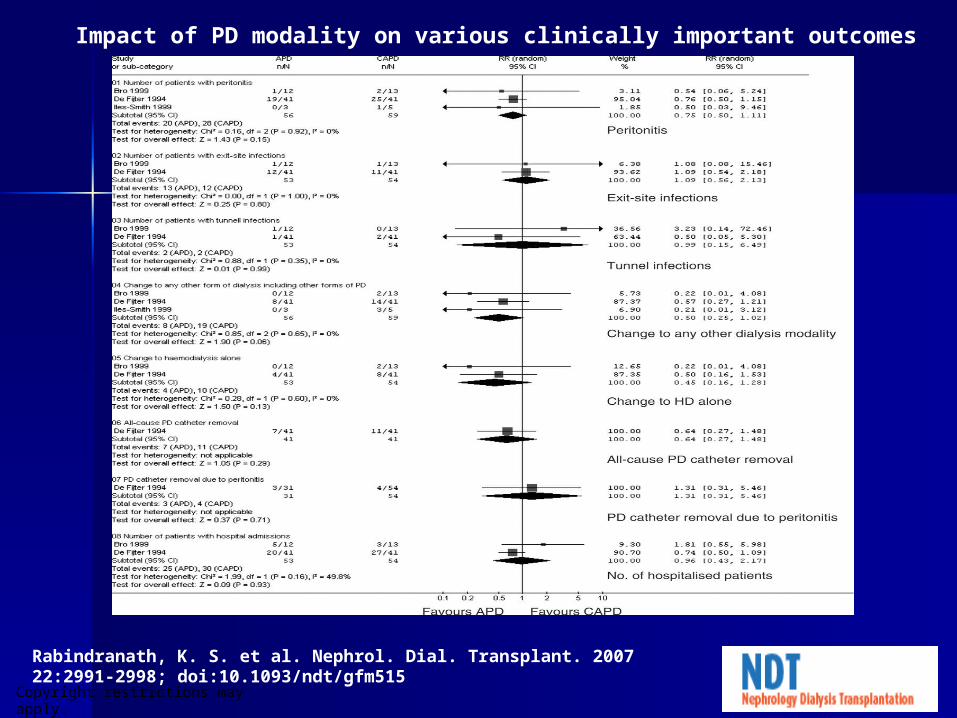
CAPD Vs APDCAPD Vs APD
Copyright restrictions may apply.
Rabindranath, K. S. et al. Nephrol. Dial. Transplant. 2007 22:2991-2998; doi:10.1093/ndt/gfm515
Impact of PD modality on various clinically important outcomes
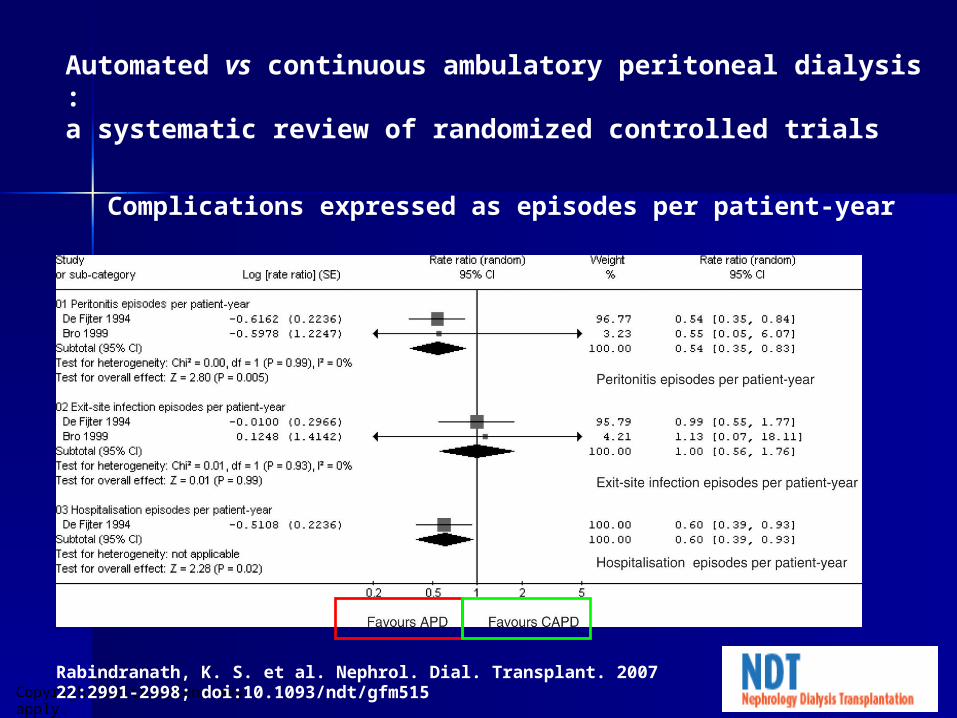
Copyright restrictions may apply.Rabindranath, K. S. et al. Nephrol. Dial. Transplant. 2007 22:2991-2998; doi:10.1093/ndt/gfm515
Complications expressed as episodes per patient-year
Automated vs continuous ambulatory peritoneal dialysis :a systematic review of randomized controlled trials
The Cochrane Collaboration, currently published in The Cochrane Database of Systematic Reviews 2009 Issue 3,
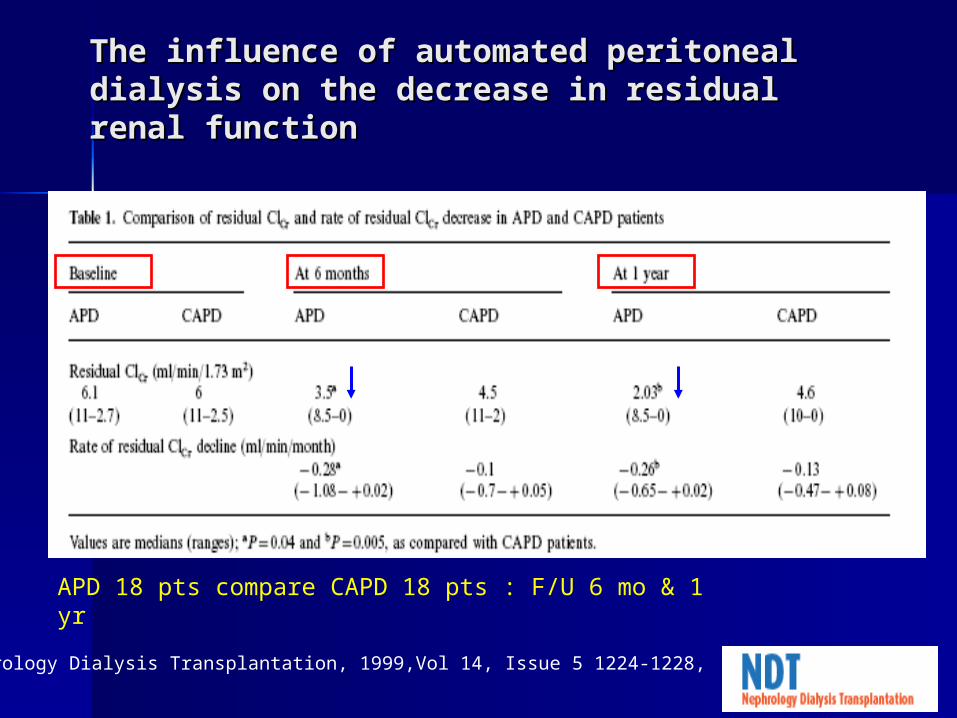
The influence of automated peritoneal The influence of automated peritoneal dialysis on the decrease in residual renal dialysis on the decrease in residual renal functionfunction
Nephrology Dialysis Transplantation, 1999,Vol 14, Issue 5 1224-1228,
APD 18 pts compare CAPD 18 pts : F/U 6 mo & 1 yr
SummarySummary
APD CAPD : peritonitisAPD CAPD : peritonitis Caution APD decline RRF > CAPDCaution APD decline RRF > CAPD Other non significantOther non significant SelectionSelection method method :1. patient :1. patient
contraindication , preference base on contraindication , preference base on life style, comfort with cycler & family life style, comfort with cycler & family + social support+ social support
2.medical requirement: 2.medical requirement: adequacyadequacy
PrescriptionPrescription
Acute peritoneal dialysisAcute peritoneal dialysis Chronic peritoneal dialysisChronic peritoneal dialysis
Acute peritoneal dialysisAcute peritoneal dialysis orderorder
Session lengthSession length: 24 hr at time: 24 hr at time Exchange volumeExchange volume :depend size of :depend size of
peritoneal cavity, tolerate 2-L peritoneal cavity, tolerate 2-L exchangeexchange
Smaller dose :pulmonary diseaseSmaller dose :pulmonary disease Prefer start :1-1.5 L :1Prefer start :1-1.5 L :1stst exchange exchange
((leakageleakage)) In large pt or hypercatabolic : 2.5- In large pt or hypercatabolic : 2.5-
3 L3 L
Acute peritoneal dialysisAcute peritoneal dialysis orderorder
Exchange timeExchange time :inflow , dwell & :inflow , dwell & draindrain
Dialysis solution Dialysis solution : depend on : depend on indicationindication
standard 1.5standard 1.5 %, high : 4.25 %%, high : 4.25 %
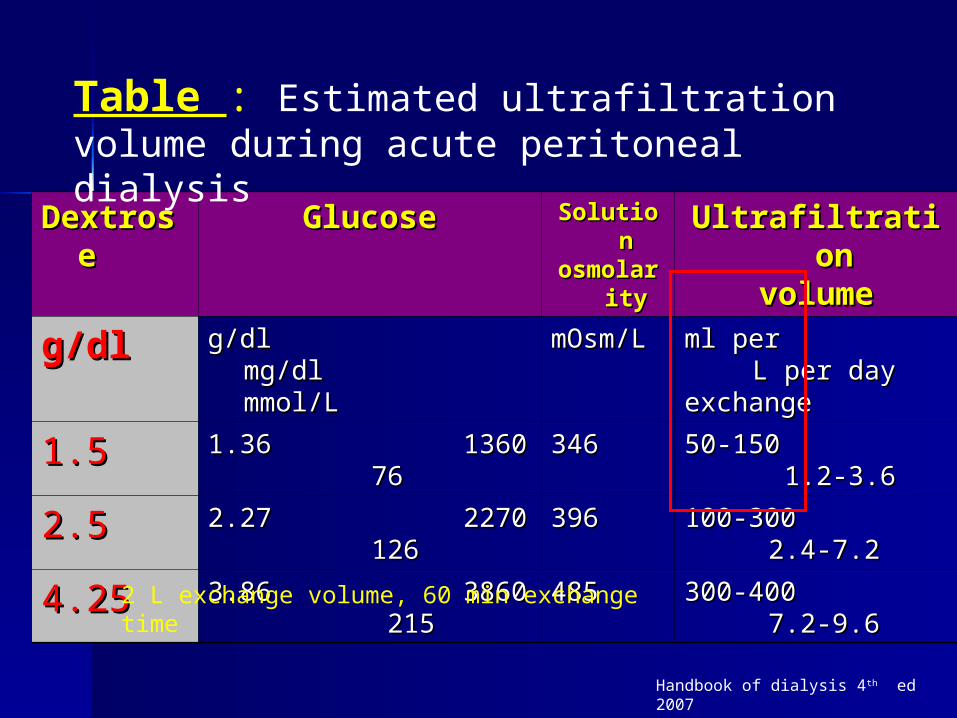
DextrosDextrosee
GlucoseGlucose SolutionSolutionosmolarityosmolarity
UltrafiltrationUltrafiltrationvolumevolume
g/dlg/dl g/dl mg/dl mmol/L g/dl mg/dl mmol/L
mOsm/LmOsm/L ml per L per dayml per L per dayexchange exchange
1.51.5 1.36 1360 761.36 1360 76 346346 50-150 1.2-3.650-150 1.2-3.6
2.52.5 2.27 2270 1262.27 2270 126 396396 100-300 2.4-7.2100-300 2.4-7.2
4.254.25 3.86 3860 2153.86 3860 215 485485 300-400 7.2-9.6300-400 7.2-9.6
Table : Estimated ultrafiltration volume during acute peritoneal dialysis
2 L exchange volume, 60 min exchange time
Handbook of dialysis 4th ed 2007
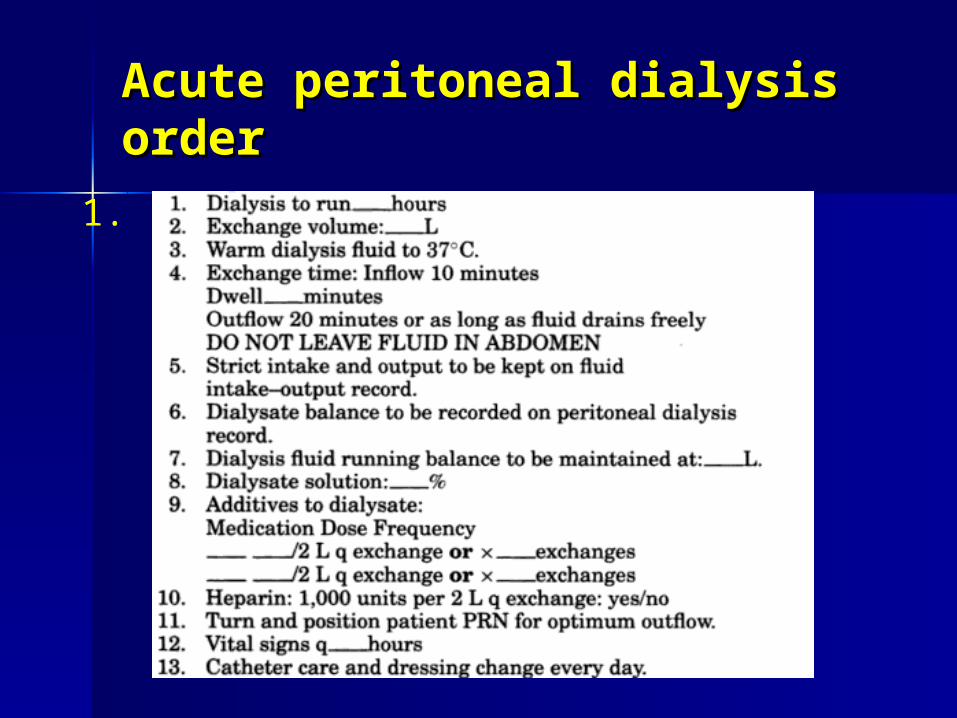
Acute peritoneal dialysis Acute peritoneal dialysis orderorder
1.
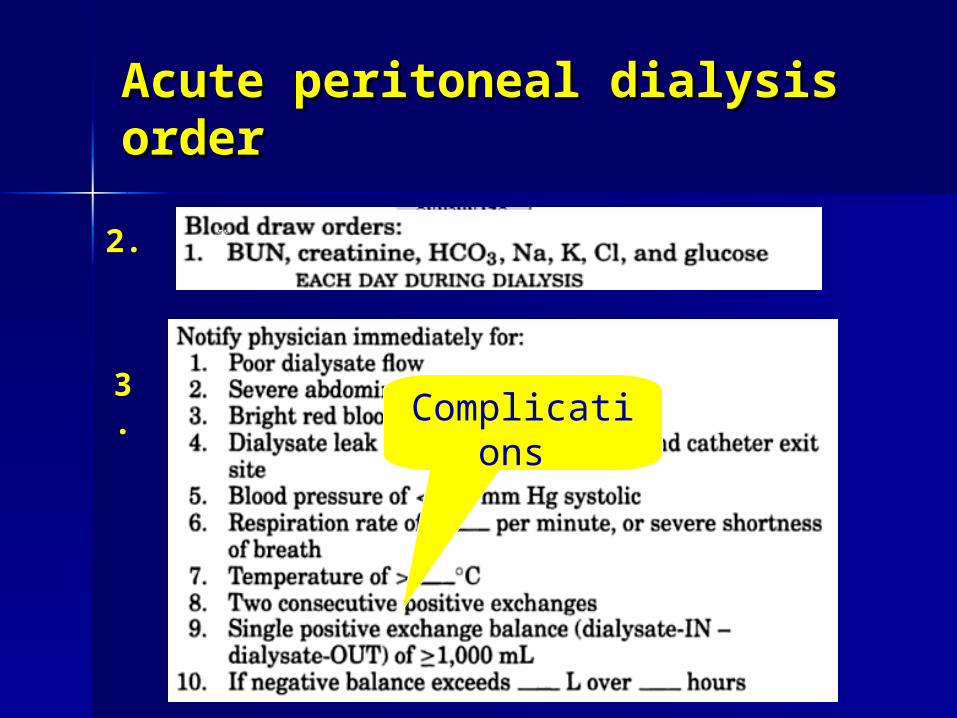
Acute peritoneal dialysis Acute peritoneal dialysis orderorder
2.
3.Complicatio
ns
Prescription of CAPDPrescription of CAPD
Dose : cycle/dayDose : cycle/day Volume : exchange volumeVolume : exchange volume Standard dose :3-4 time/dayStandard dose :3-4 time/day Standard volume :6-8 L/dayStandard volume :6-8 L/day Typical order :4* 2L dailyTypical order :4* 2L daily Dialysis solution: 1.5, 2.5 .4.25 %Dialysis solution: 1.5, 2.5 .4.25 %
Ca : low Ca , normal CaCa : low Ca , normal Ca
Augmentation UF :CAPDAugmentation UF :CAPD
Increase exchange volumeIncrease exchange volume Increase frequencyIncrease frequency Increase tonicityIncrease tonicity
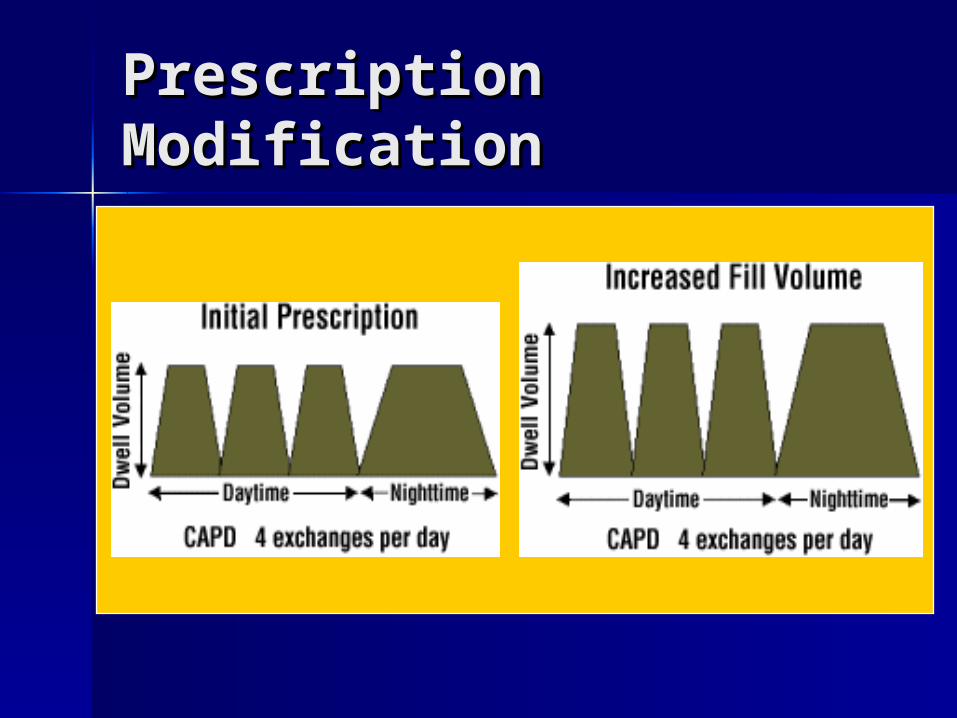
Prescription Prescription ModificationModification
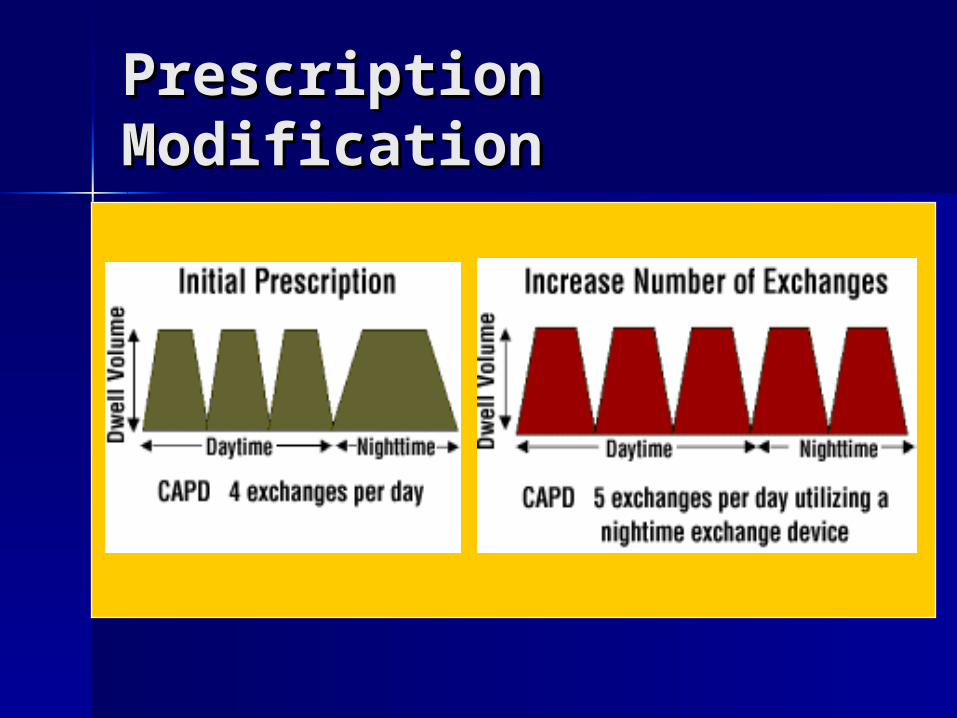
Prescription Prescription ModificationModification
Automated PD Automated PD
Mode : PET testMode : PET test Dialysis solution : glucose / CaDialysis solution : glucose / Ca Duration : dwell time, cycle, Duration : dwell time, cycle, Tidal volume :Tidal volume : Last fill volume Last fill volume :??:??
Initial APD prescriptionInitial APD prescription
Mode : NIPD Mode : NIPD Solution : 1.5%Solution : 1.5% Duration ;8-12 hrDuration ;8-12 hr Fill volume : 1.5-2.0 mlFill volume : 1.5-2.0 ml Dwell Day volume:2-L : Dwell Day volume:2-L :
caution :fluid reabsorption caution :fluid reabsorption ((if high if high transporttransport ) ) other choice : other choice : icodextrin :icodextrin : - water soluble glucose polymer- water soluble glucose polymer
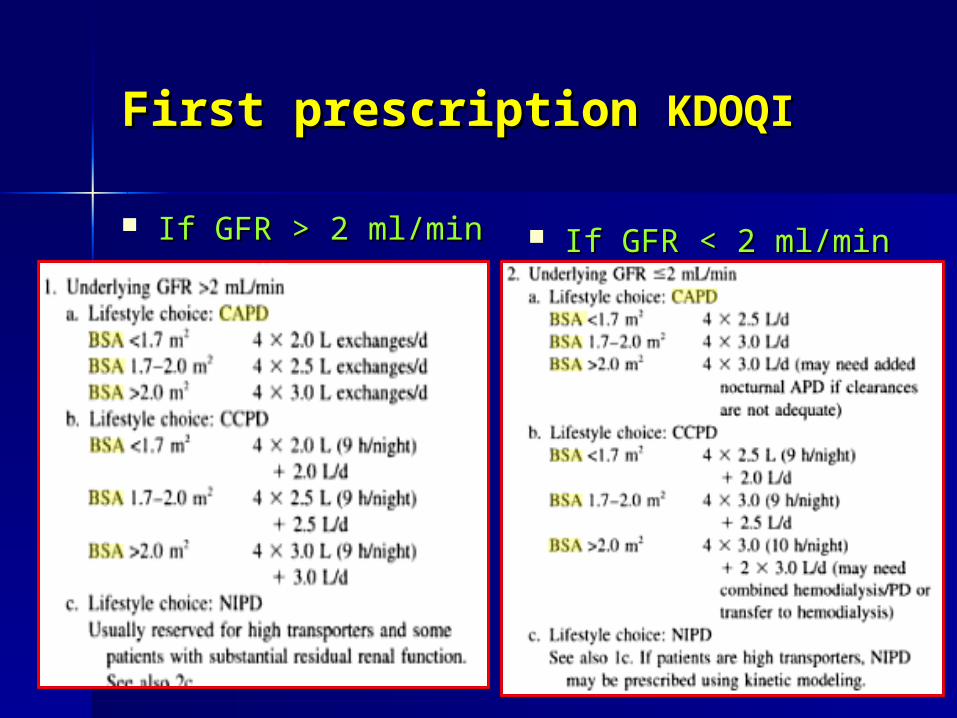
First prescription First prescription KDOQIKDOQI
If GFR > 2 ml/minIf GFR > 2 ml/min If GFR < 2 ml/minIf GFR < 2 ml/min
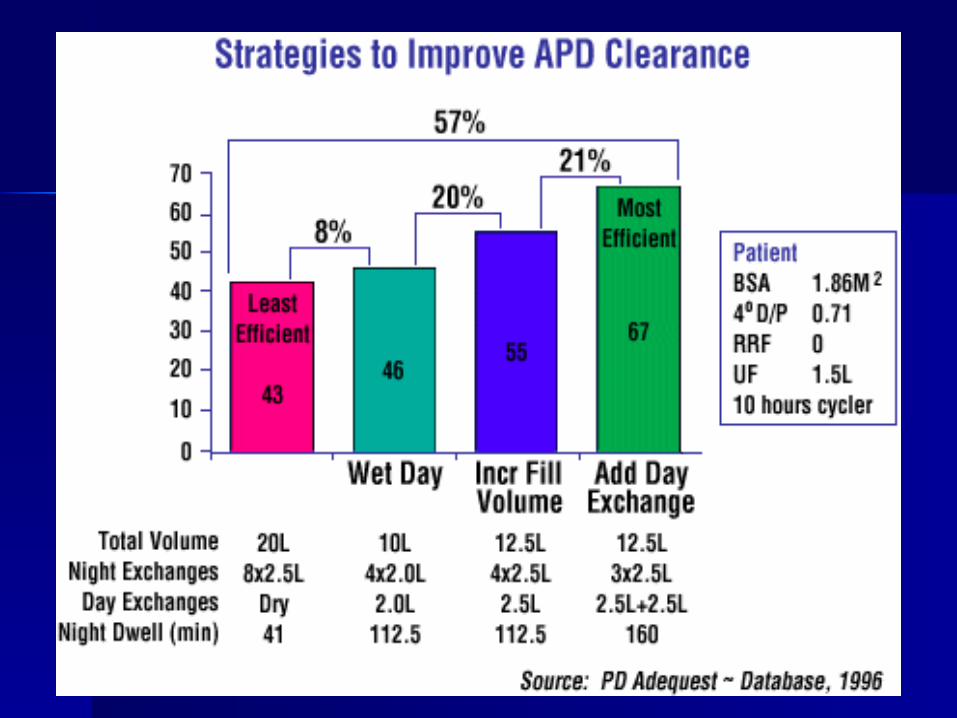
How to improved How to improved clearance in clearance in APD ????APD ????
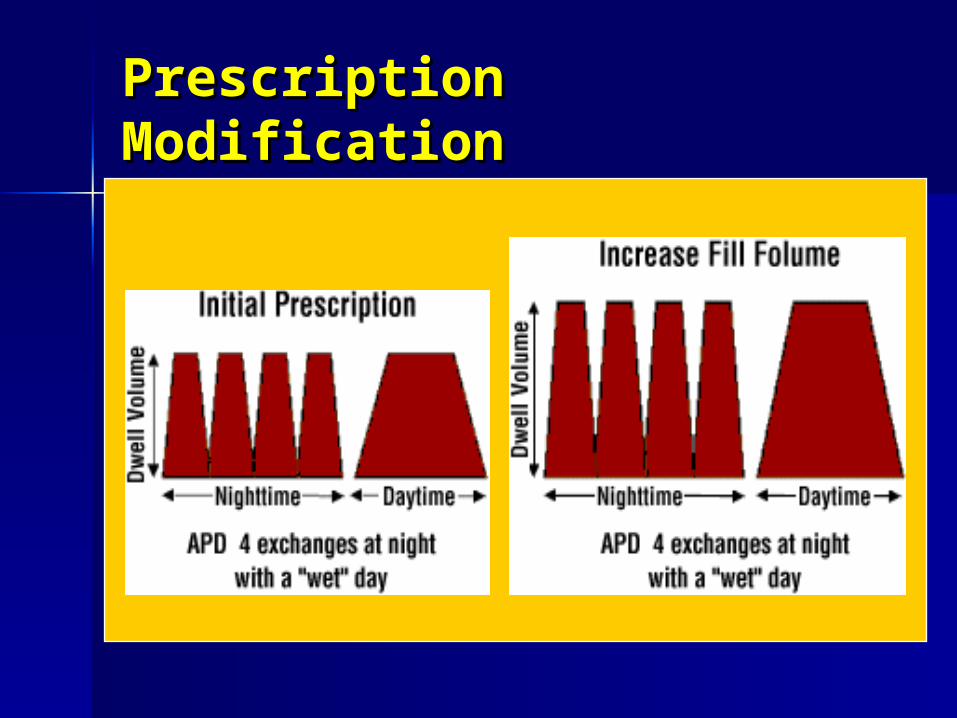
Prescription ModificationPrescription Modification
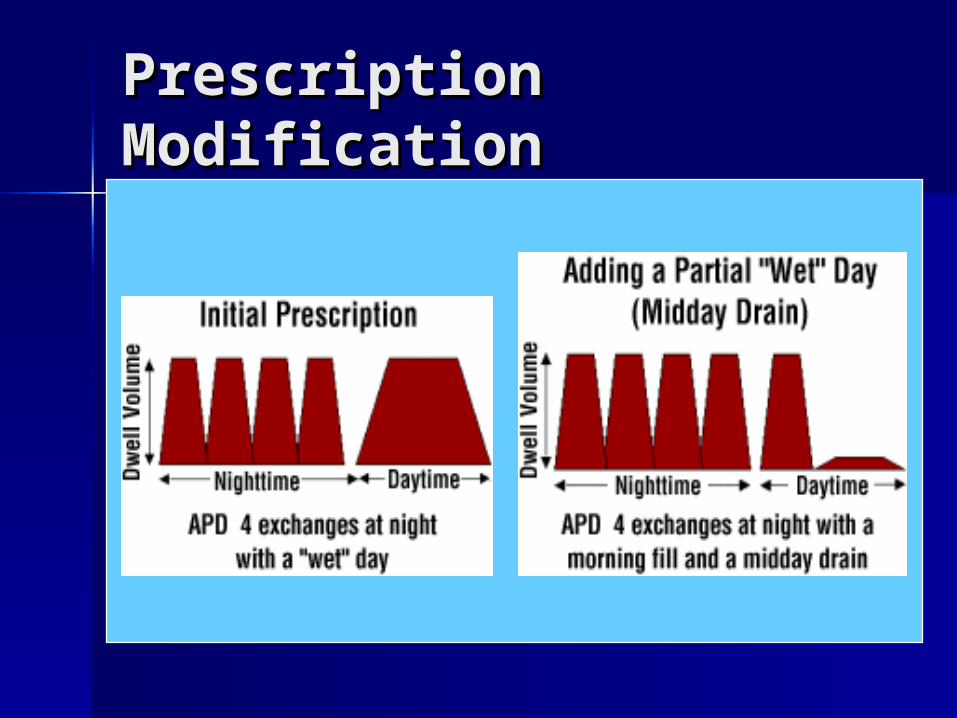
Prescription Prescription ModificationModification
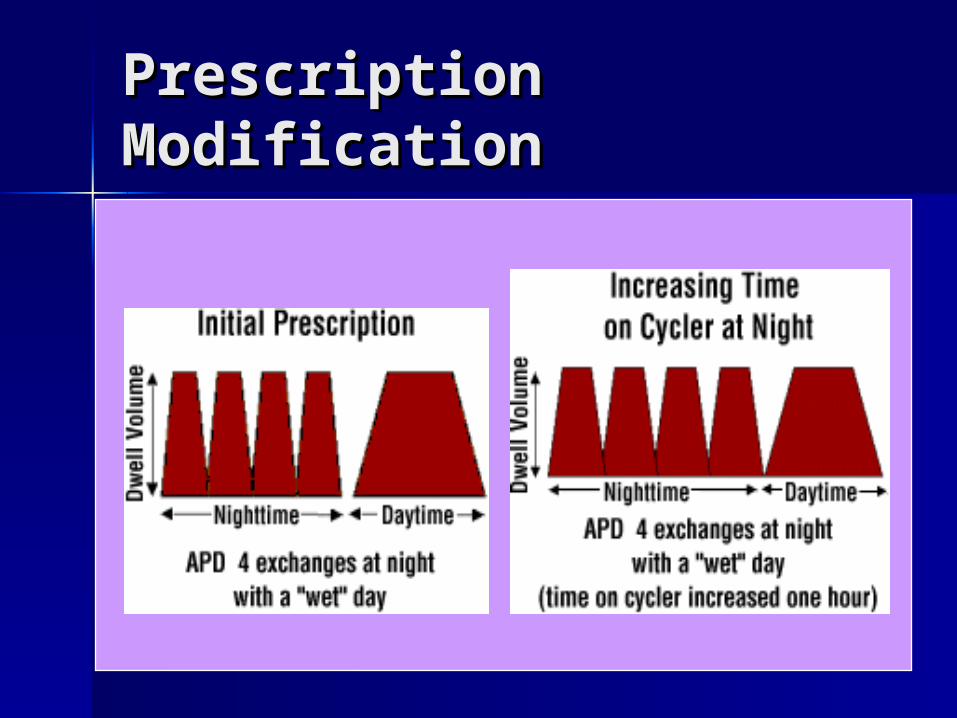
Prescription Prescription ModificationModification
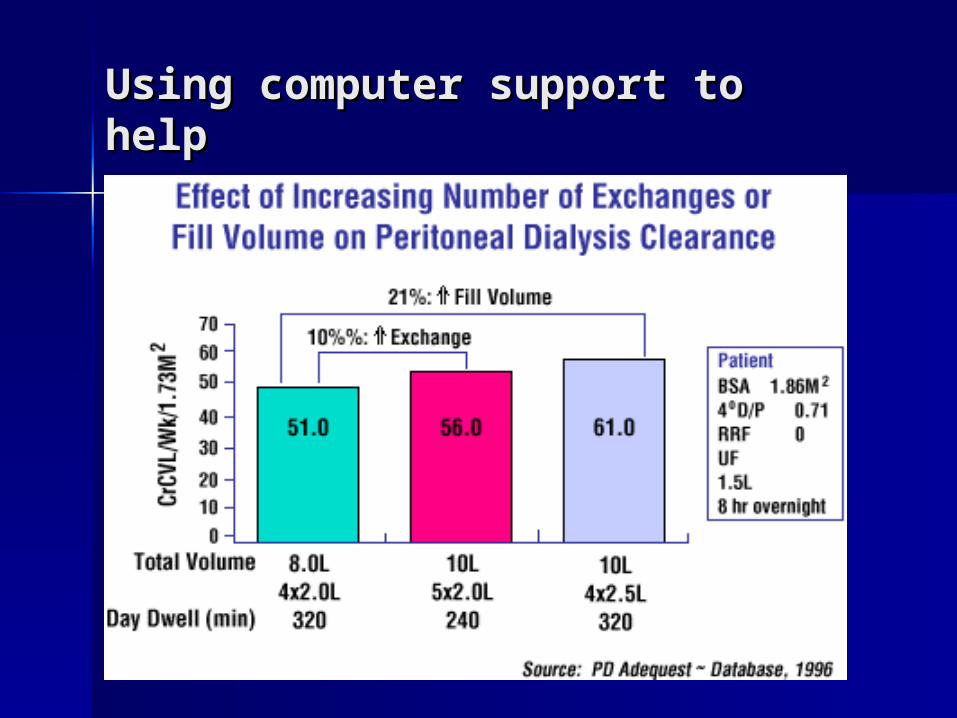
Using computer support to Using computer support to helphelp
Increase peritoneal Increase peritoneal
clearance ?clearance ?
Day dwell volumeDay dwell volume :increase Kt/V :increase Kt/V & CrCl 25-50 % & CrCl 25-50 %
Increase dwell volume on cycler Increase dwell volume on cycler Time on cyclerTime on cycler Increase frequency of cyclesIncrease frequency of cycles Increase tonicity of dialysis Increase tonicity of dialysis
solutionsolution
Prescription AIM Prescription AIM
Adequacy : Kt/VAdequacy : Kt/V EuvolemiaEuvolemia : PCWP ?: PCWP ?
== no edema : no edema : UFUF
normal BP &normal BP & minimize anti HT drugminimize anti HT drug
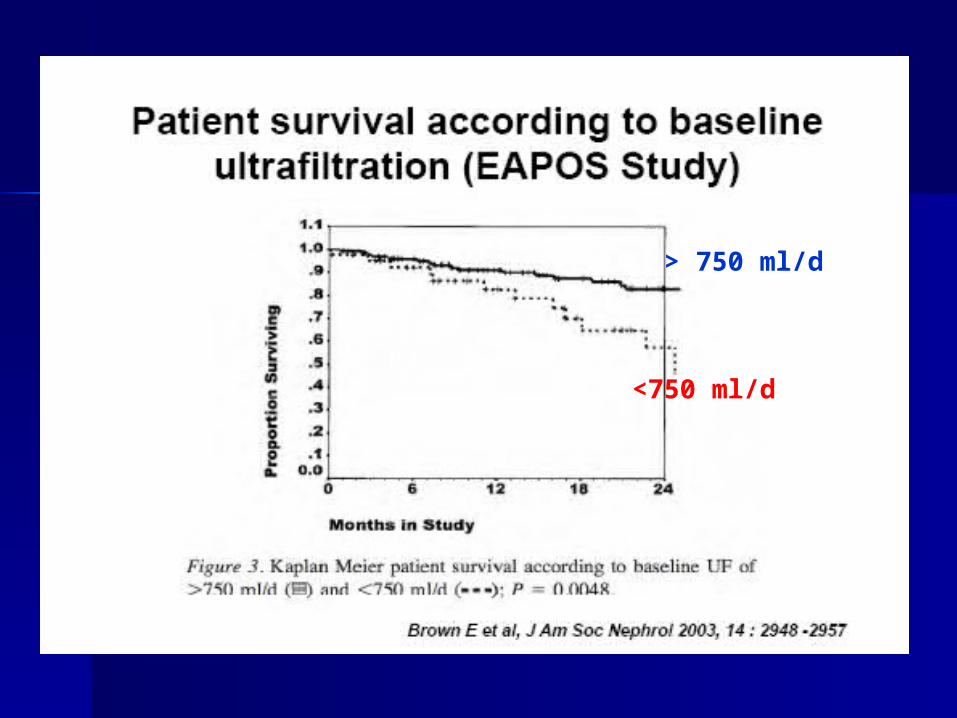
> 750 ml/d
<750 ml/d
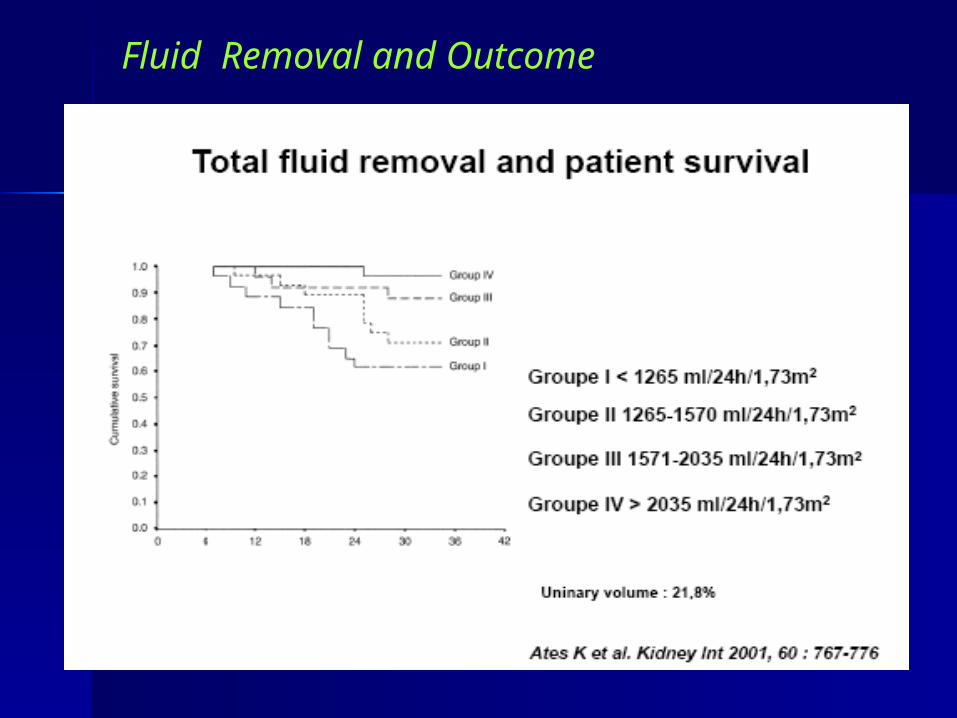
Fluid Removal and Outcome
Initiate Therapy
Measure clearanceand UF
Adjust Therapy
Managing PD adequacy & Managing PD adequacy &
prescriptionprescription
Don’t forget!
PD – getting startedPD – getting started
Measure Clearances at 2-4 weeks, then Measure Clearances at 2-4 weeks, then 2-3 times in first 6 months2-3 times in first 6 months
Thereafter every 3-4 monthsThereafter every 3-4 months Measure PET at 1 monthMeasure PET at 1 month If urine volume low – use 48hr collectionIf urine volume low – use 48hr collection Leave clearances for a month after Leave clearances for a month after
peritonitisperitonitis P creatinine – CAPD anytime, APD mid P creatinine – CAPD anytime, APD mid
daytimedaytime
Case Case
Female , 50 yrs, ESRD Female , 50 yrs, ESRD ตั�ดสิ�นใจเลื�อก ตั�ดสิ�นใจเลื�อก PD PD
BW 50 kg , Ht 155 cm BW 50 kg , Ht 155 cm ((BSA 1.50m2, BSA 1.50m2, GFR 2ml/min =GFR 2ml/min = CCr 20L/wkCCr 20L/wk แลืะ แลืะ Kt/V Kt/V = 0.5 /wk= 0.5 /wk ) ) เคยประเมิ�น เคยประเมิ�น PET PET อย��ในกลื��มิ อย��ในกลื��มิ low low average transport average transport ถ้�าตั�องการสิ��งการร�กษาถ้�าตั�องการสิ��งการร�กษาเป�นไปตัามิ เป�นไปตัามิ NKF-DOQI NKF-DOQI ((weely CCr ≥ weely CCr ≥ 60L/1.73m260L/1.73m2 ) ) จะตั�องสิ��งการร�กษาอย�างไรจะตั�องสิ��งการร�กษาอย�างไร
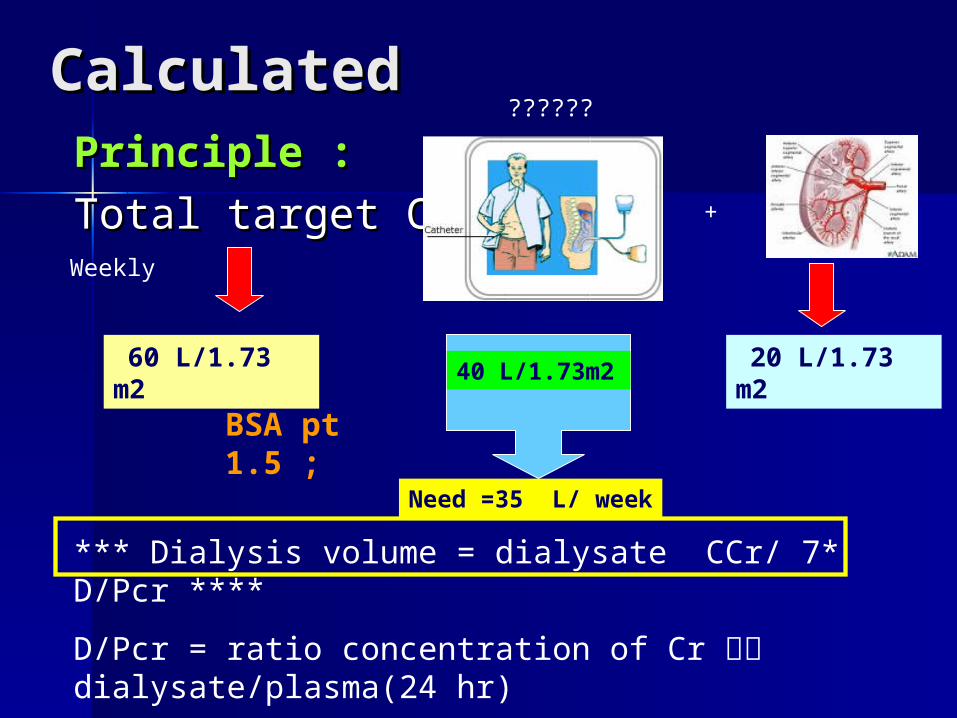
Calculated Calculated Principle :Principle :
Total target CCr = Total target CCr = +
60 L/1.73 m2
20 L/1.73 m2
40 L/1.73m2
BSA pt 1.5 ;
Need =35 L/ week
*** Dialysis volume = dialysate CCr/ 7* D/Pcr ****
D/Pcr = ratio concentration of Cr ใน dialysate/plasma(24 hr)
Or estimated PET : D/Pcr at 6 hr
Weekly
??????
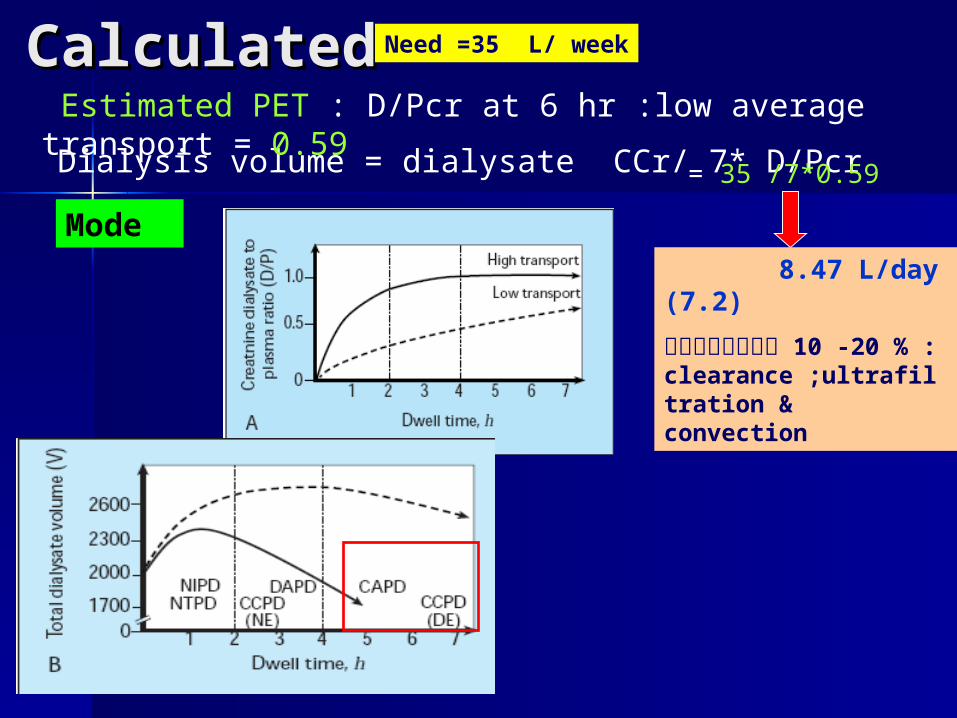
Calculated Calculated Need =35 L/ week
Dialysis volume = dialysate CCr/ 7* D/Pcr
Estimated PET : D/Pcr at 6 hr :low average transport = 0.59
= 35 /7*0.59
8.47 L/day(7.2)
ลดปริ�มาณ 10 -20 % : clearance ;ultrafiltration & convection
Mode
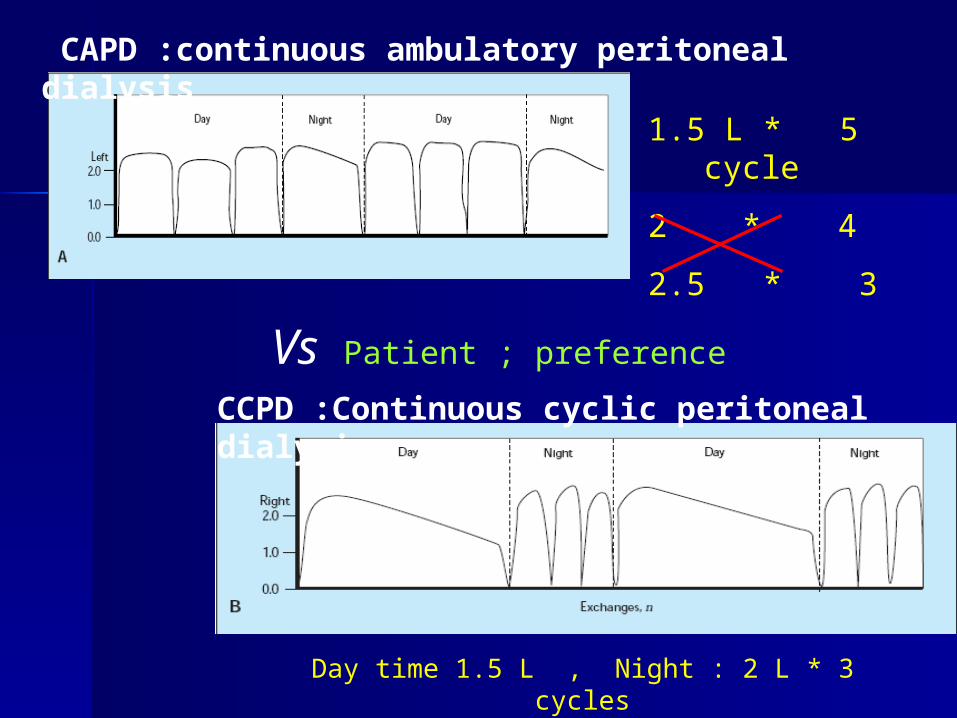
CCPD :Continuous cyclic peritoneal dialysis
CAPD :continuous ambulatory peritoneal dialysis
1.5 L * 5 cycle
2 * 4
2.5 * 3
Day time 1.5 L , Night : 2 L * 3 cycles
Vs Patient ; preference
SummarySummary Prescribing PD is important and Prescribing PD is important and
important factors includeimportant factors include– SizeSize– Transport statusTransport status– Residual renal functionResidual renal function– Other factorsOther factors
Check clinical statusCheck clinical status – supported by – supported by measurements eg UF and adequacymeasurements eg UF and adequacy





Blood pressure control in Blood pressure control in dialysis patient :HD Vs PDdialysis patient :HD Vs PD
Case Case Male , 50 yrs, ESRD with morbid obesity, BW Male , 50 yrs, ESRD with morbid obesity, BW
86 kg , Ht 155 cm 86 kg , Ht 155 cm ถ้�าตั�องการสิ��งการร�กษาเป�นไปตัามิ ถ้�าตั�องการสิ��งการร�กษาเป�นไปตัามิ NKF-DOQI NKF-DOQI ((weekly CCr ≥ weekly CCr ≥ 60L/1.73m260L/1.73m2 ) ) :prescribe?:prescribe?
Female 70 yrs, DM , HT ,ESRD & ICM BW Female 70 yrs, DM , HT ,ESRD & ICM BW 45 :prescribe?45 :prescribe?
Female , 40 years , ESRD , Hx TB peritonitis Female , 40 years , ESRD , Hx TB peritonitis * 2* 2 time on anti Tb drug complete time on anti Tb drug complete course :prescribe ?course :prescribe ?
Male 50 yrs ,ESRD, HT & alcoholic cirrhosis Male 50 yrs ,ESRD, HT & alcoholic cirrhosis child B ascites positive : child B ascites positive :
Different HD & PDDifferent HD & PD
Prefer PDPrefer PD Prefer HDPrefer HD





























