Embed Size (px)
Citation preview
DOI: 10.1051/odfen/2013508 J Dentofacial Anom Orthod 2014;17:203� RODF / EDP Sciences
1
Article received: 21-2013.Accepted for publication: 05-2013.
Orofacial rare diseases: specificitiesof the collaboration between orthodontistand pediatric dentist
C. Ravinet1, P. Garrec2
1 AHU-PH - Odontologie pediatrique, Universite Paris-Diderot, Paris 7
2 MCU-PH - Orthopedie dento-faciale, Universite Paris-Diderot, Paris 7
ABSTRACT
Pediatric dentistry plays an important part in the orthodontic treatment ofpatients with rare orofacial diseases. Interactions between these twodisciplines are numerous and particularly noteworthy in the followingpathologies:– cleft lip and palate;– ectodermal dysplasia;– amelogenesis imperfecta;– dentinogenesis imperfecta.
After reviewing the main characteristics of these pathologies, we willhighlight the fundamental role of pediatric dentistry in the early diagnosis, theprevention and the dental care throughout the orthodontic treatment.A close cooperation between the orthodontist and the pediatric dentist is akey factor to a successful treatment.
KEY WORDS
Orthodontics preventive interceptive corrective treatmentpediatric dentistry interdisciplinary approach ectodermal dysplasiadentinogenesis imperfecta amelogenesis imperfecta cleft lipcleft palate
INTRODUCTION
Orthodontic treatment for patients whopresent with malformations of the face andoral cavity caused by rare diseases is car-ried out by a multidisciplinary team.
A pediatric dentist (PD) is one of the ma-jor components of this team.
Orthodontic treatments increase the riskof the development of caries37. In addition
Address for correspondence:
P. GarrecCentre de reference des malformations rares de laface et de la cavite buccale (MAFACE),Hopital Rothschild AP-HP, Pole d’odontologie, [email protected] available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2013508
to this inherent risk factor, there areother particularities of these patientsthat will have to be taken into ac-count:• clinical context:– periodontal fragility (epidermolysis
bullosa...);– weakness of the enamel (amelo-
genesis imperfecta);– specific physiological bone weak-
ness and bone loss;• general context:– psychological factors (related to the
handicap or to esthetics);– oral hygiene habits necessary to
learn to control plaque.These atypical patients require the
specialized clinical services of referralcenters (centers for comprehensivecare and diagnosis) but there are fewof them and this limits the accessthat remote and rural populationshave to care. One of the proposedsolutions is the creation of city net-works that draw from all the medicalspecialists, who then must learn tocommunicate and work together.
A recent study33 showed that82.9% of orthodontists refused totreat patients who presented orofa-cial abnormalities in their offices.
The most commonly mentionedreasons for refusing treatment werethe following:– limited experience with this type of
treatment;– lack of expertise;– lack of a multidisciplinary team.
Other reasons (the financial aspect,length of the treatment and lack ofinterest) were considered less impor-tant.
The authors conclude that addi-tional time should be allocated in uni-versity and hospital curricula totraining for these diseases.
Drawing from examples of patholo-gies encountered at the referral cen-ter, we will demonstrate how anorthodontist and pediatric dentist col-laborate with one another.
ECTODERMIC DYSPLASIA (ED)
Characteristics
Ectodermic dysplasia is a geneticdisease that affects the skin, hair,teeth and may be associated withvarious other syndromes.
From a dental perspective, it ischaracterized by total anodontia oroligodontia and existing teeth are fre-quently cone-shaped.Therapeutic objectives34:
– preserve the existing teeth;– improve esthetics;
– establish normal eating;– improve pronunciation;– enhance the psychological, social
and emotional well being of thechild and the family.Esthetic and functional improve-
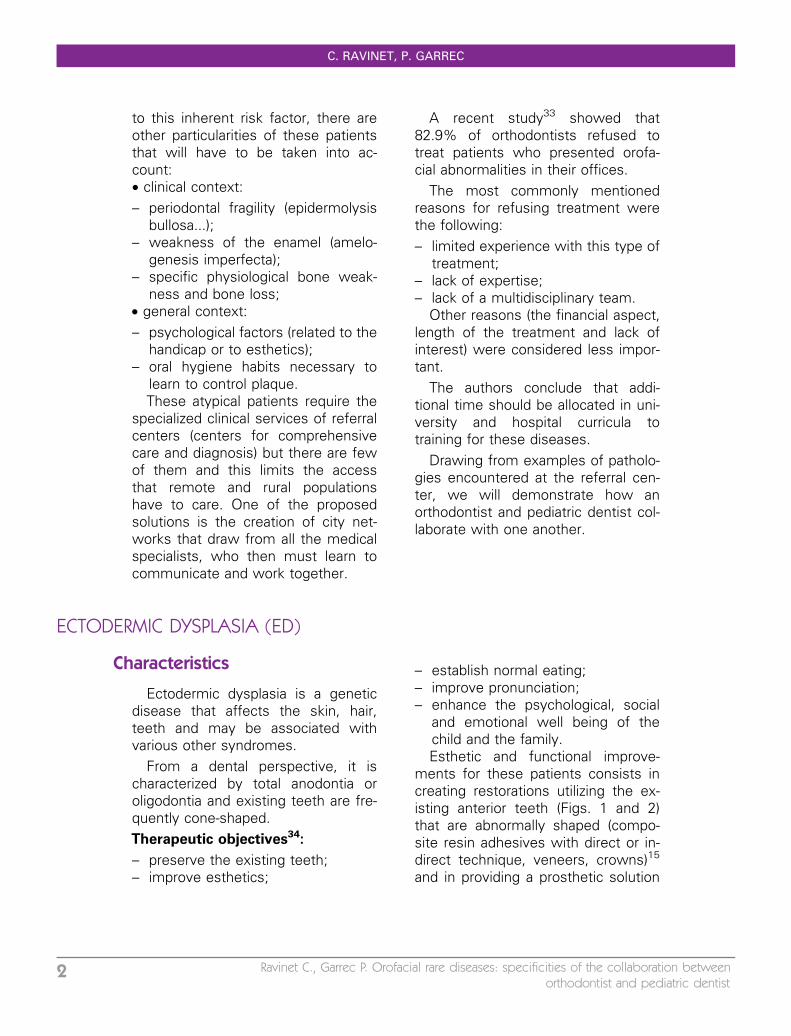
ments for these patients consists increating restorations utilizing the ex-isting anterior teeth (Figs. 1 and 2)that are abnormally shaped (compo-site resin adhesives with direct or in-direct technique, veneers, crowns)15
and in providing a prosthetic solution
C. RAVINET, P. GARREC
2 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
whether permanently attached or re-movable (+/- supported and retainedby symphyseal implants)22.
Role of the pediatric dentist
Diagnosis
An early diagnosis allows the prac-titioner to more effectively manage
the treatment plan in the long term,and to restore confidence in patientsby improving their self-image thatcan also be sometimes medically de-cisive: ectodermal dysplasia may alsobe part of a syndrome that involves alife-threatening diagnosis29.
Early detection of the presence ofagenesis is of the utmost importance
Figure 1Patient who benefitted from simplified DFO treatment and restoration using composite bonding carried out at alaboratory (Dr Garrec/Dr De La Dure Molla) (MAFACE photos).
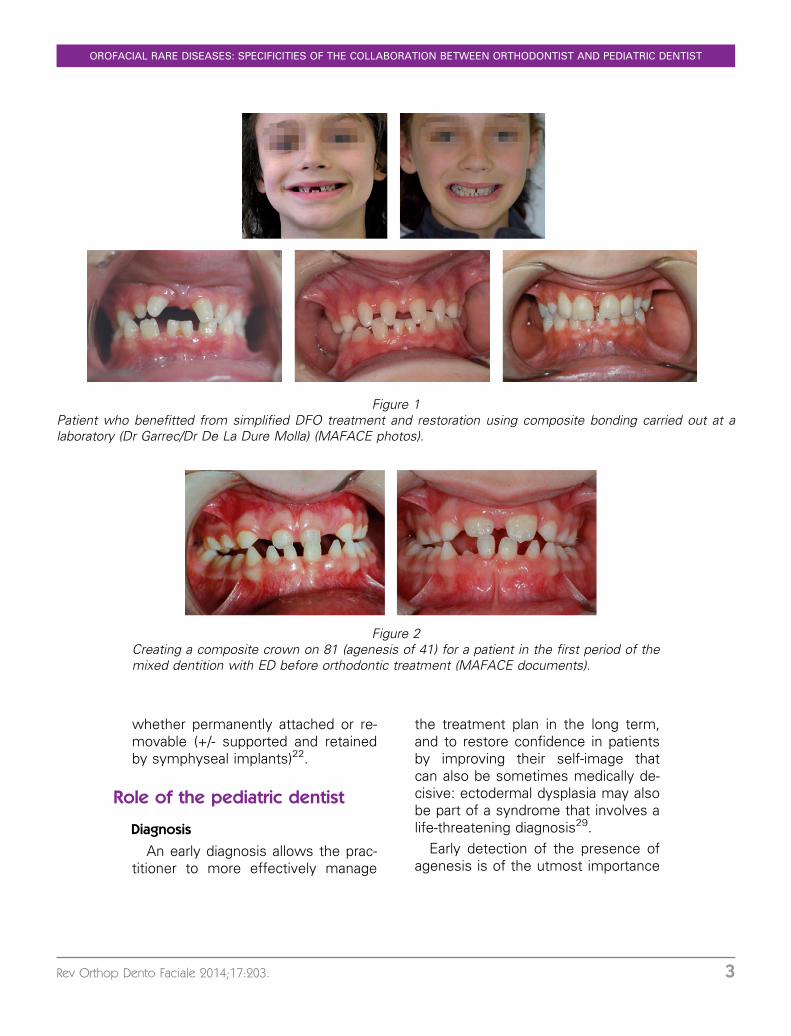
Figure 2Creating a composite crown on 81 (agenesis of 41) for a patient in the first period of themixed dentition with ED before orthodontic treatment (MAFACE documents).
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 3
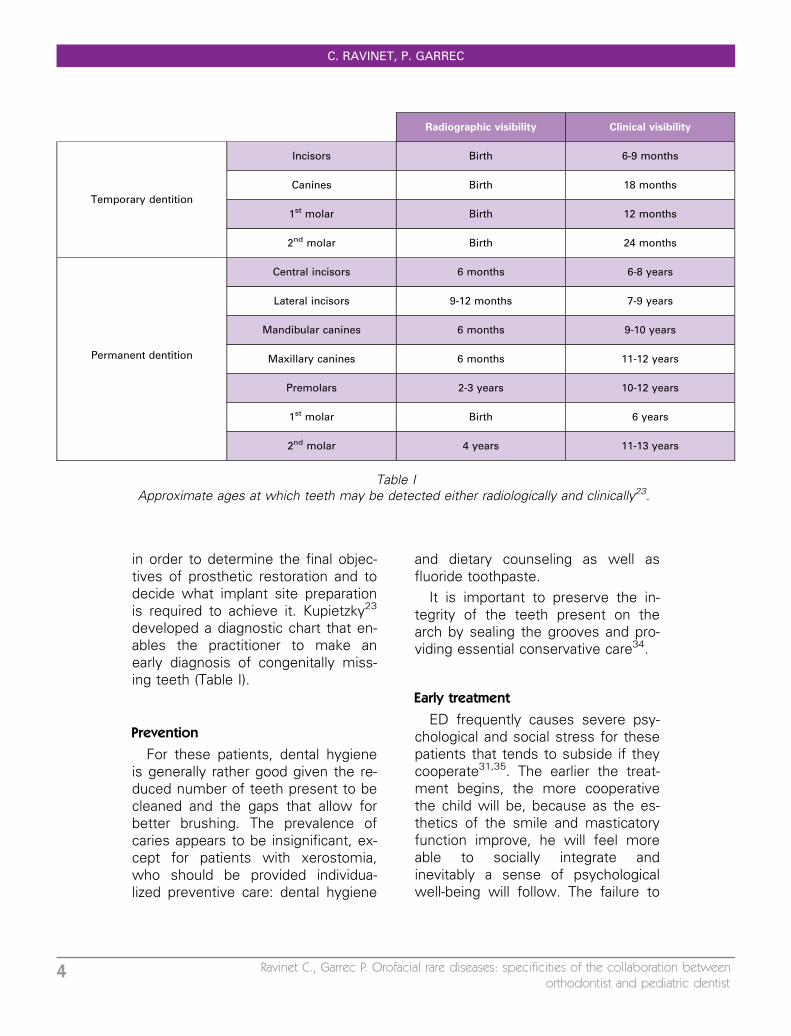
in order to determine the final objec-tives of prosthetic restoration and todecide what implant site preparationis required to achieve it. Kupietzky23
developed a diagnostic chart that en-ables the practitioner to make anearly diagnosis of congenitally miss-ing teeth (Table I).
Prevention
For these patients, dental hygieneis generally rather good given the re-duced number of teeth present to becleaned and the gaps that allow forbetter brushing. The prevalence ofcaries appears to be insignificant, ex-cept for patients with xerostomia,who should be provided individua-lized preventive care: dental hygiene
and dietary counseling as well asfluoride toothpaste.
It is important to preserve the in-tegrity of the teeth present on thearch by sealing the grooves and pro-viding essential conservative care34.
Early treatment
ED frequently causes severe psy-chological and social stress for thesepatients that tends to subside if theycooperate31,35. The earlier the treat-ment begins, the more cooperativethe child will be, because as the es-thetics of the smile and masticatoryfunction improve, he will feel moreable to socially integrate andinevitably a sense of psychologicalwell-being will follow. The failure to
Radiographic visibility Clinical visibility
Temporary dentition
Incisors Birth 6-9 months
Canines Birth 18 months
1st molar Birth 12 months
2nd molar Birth 24 months
Permanent dentition
Central incisors 6 months 6-8 years
Lateral incisors 9-12 months 7-9 years
Mandibular canines 6 months 9-10 years
Maxillary canines 6 months 11-12 years
Premolars 2-3 years 10-12 years
1st molar Birth 6 years
2nd molar 4 years 11-13 years
Table IApproximate ages at which teeth may be detected either radiologically and clinically23.
C. RAVINET, P. GARREC
4 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
provide early treatment will have aharmful effect on the adolescent withphysical, psychological and social ra-mifications43.
A lack of alveolar bone follows theabsence of tooth buds and causes asignificant loss of vertical height. Anearly prosthetic restoration will makeit possible to maintain the height ofthe lower third of the face. The pros-thesis will therefore need to be reas-sessed throughout the growth phase.
Role of the orthodontist
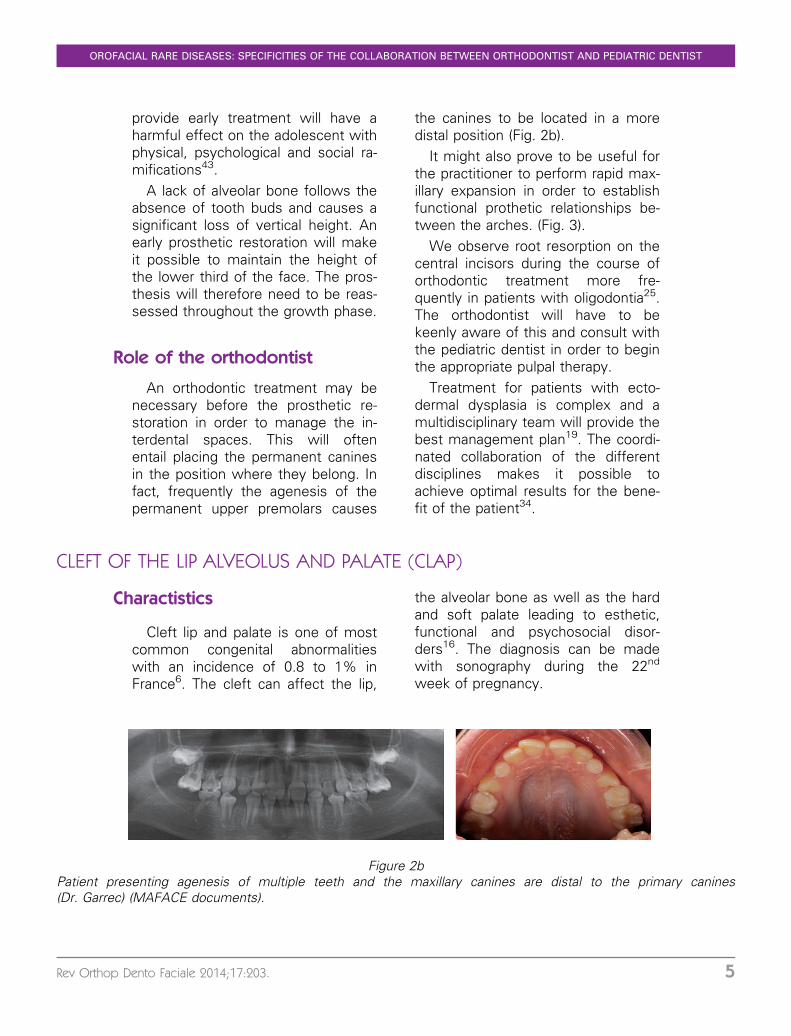
An orthodontic treatment may benecessary before the prosthetic re-storation in order to manage the in-terdental spaces. This will oftenentail placing the permanent caninesin the position where they belong. Infact, frequently the agenesis of thepermanent upper premolars causes
the canines to be located in a moredistal position (Fig. 2b).
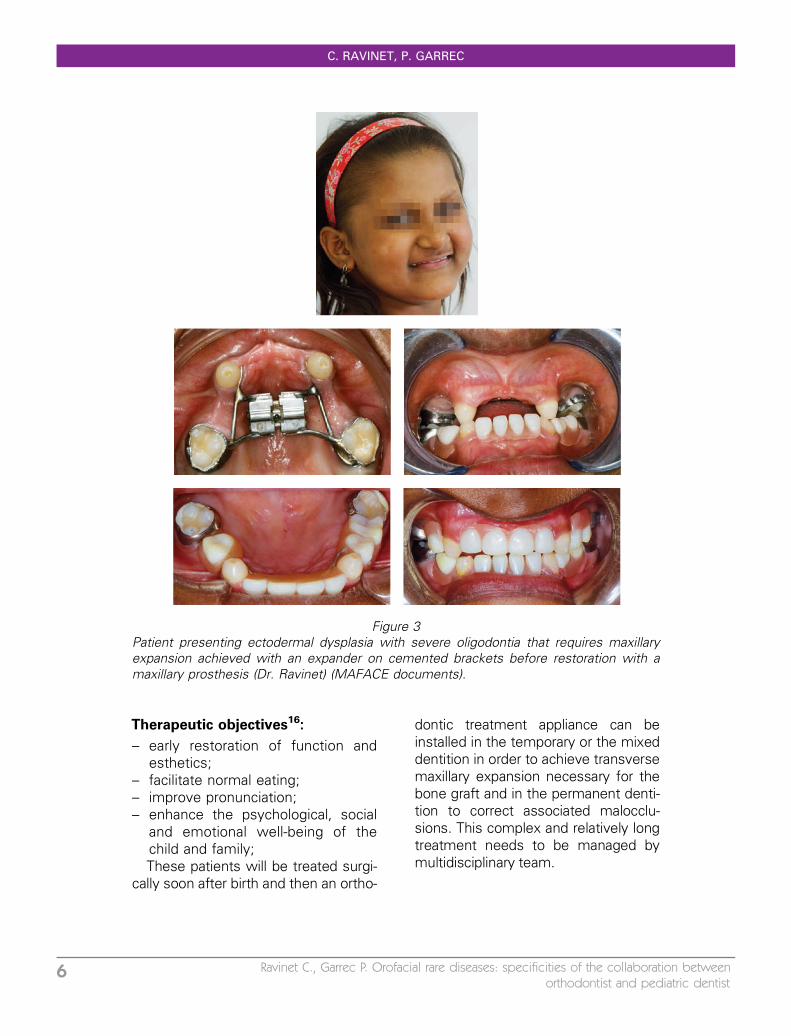
It might also prove to be useful forthe practitioner to perform rapid max-illary expansion in order to establishfunctional prothetic relationships be-tween the arches. (Fig. 3).
We observe root resorption on thecentral incisors during the course oforthodontic treatment more fre-quently in patients with oligodontia25.The orthodontist will have to bekeenly aware of this and consult withthe pediatric dentist in order to beginthe appropriate pulpal therapy.
Treatment for patients with ecto-dermal dysplasia is complex and amultidisciplinary team will provide thebest management plan19. The coordi-nated collaboration of the differentdisciplines makes it possible toachieve optimal results for the bene-fit of the patient34.
CLEFT OF THE LIP ALVEOLUS AND PALATE (CLAP)
Charactistics
Cleft lip and palate is one of mostcommon congenital abnormalitieswith an incidence of 0.8 to 1% inFrance6. The cleft can affect the lip,
the alveolar bone as well as the hardand soft palate leading to esthetic,functional and psychosocial disor-ders16. The diagnosis can be madewith sonography during the 22nd
week of pregnancy.
Figure 2bPatient presenting agenesis of multiple teeth and the maxillary canines are distal to the primary canines(Dr. Garrec) (MAFACE documents).
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 5
Therapeutic objectives16:
– early restoration of function andesthetics;
– facilitate normal eating;– improve pronunciation;– enhance the psychological, social
and emotional well-being of thechild and family;These patients will be treated surgi-
cally soon after birth and then an ortho-
dontic treatment appliance can beinstalled in the temporary or the mixeddentition in order to achieve transversemaxillary expansion necessary for thebone graft and in the permanent denti-tion to correct associated malocclu-sions. This complex and relatively longtreatment needs to be managed bymultidisciplinary team.
Figure 3Patient presenting ectodermal dysplasia with severe oligodontia that requires maxillaryexpansion achieved with an expander on cemented brackets before restoration with amaxillary prosthesis (Dr. Ravinet) (MAFACE documents).
C. RAVINET, P. GARREC
6 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
Role of pediatric dentistry16
Prevention
Shortly after birth, counselorsshould encourage breastfeeding eventhough these new mothers may bereticent46. In spite of the problemsthat may be encountered and basedon the type of cleft, breastfeeding isrecommended for optimal craniofacialgrowth7. But when this is not possi-ble, the practitioner should recom-mend latex orthodontic nipples(silicone nipples are less flexible andcreate ulcerations in the area of thecleft), with a 0.8 to 1 mm hole thatmakes it harder to extract milk there-fore stimulating the orofacial muscu-lature.
Bottlefeeding encourages the earlyintroduction of sugar into the diet ofinfants. It is frequently introduced topromote weight gain that determinesthe timing for surgical intervention.Ideally, the first contact with sugarshould be delayed as long as possi-ble46.
Neonatal teeth are frequently ob-served in the area of the cleft16 andit is important to extract them assoon as possible. These teeth areusually mobile and therefore placesthe infant at higher risk of inhalationgiven that there is communi-cation between the oral and nasalcavities8.
Studies are inconsistent about therisk of caries for these patients. Ac-cording to Nivoloni Tannure31,32,there is no significant difference forthe risk of caries compared with thegeneral population, but Johnsen21
provides evidence showing a highrisk of caries in the temporary denti-tion as does Dahllof14 who found that
patients with clefts had a highersignificant caries index (sci) at 5½years.
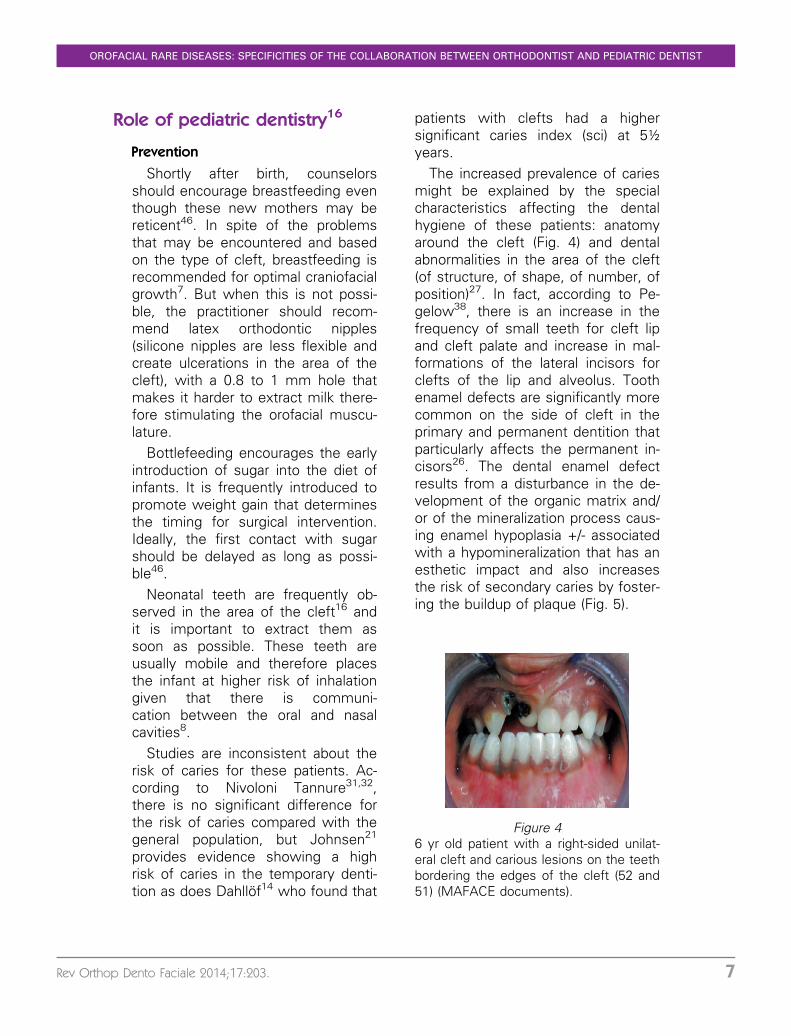
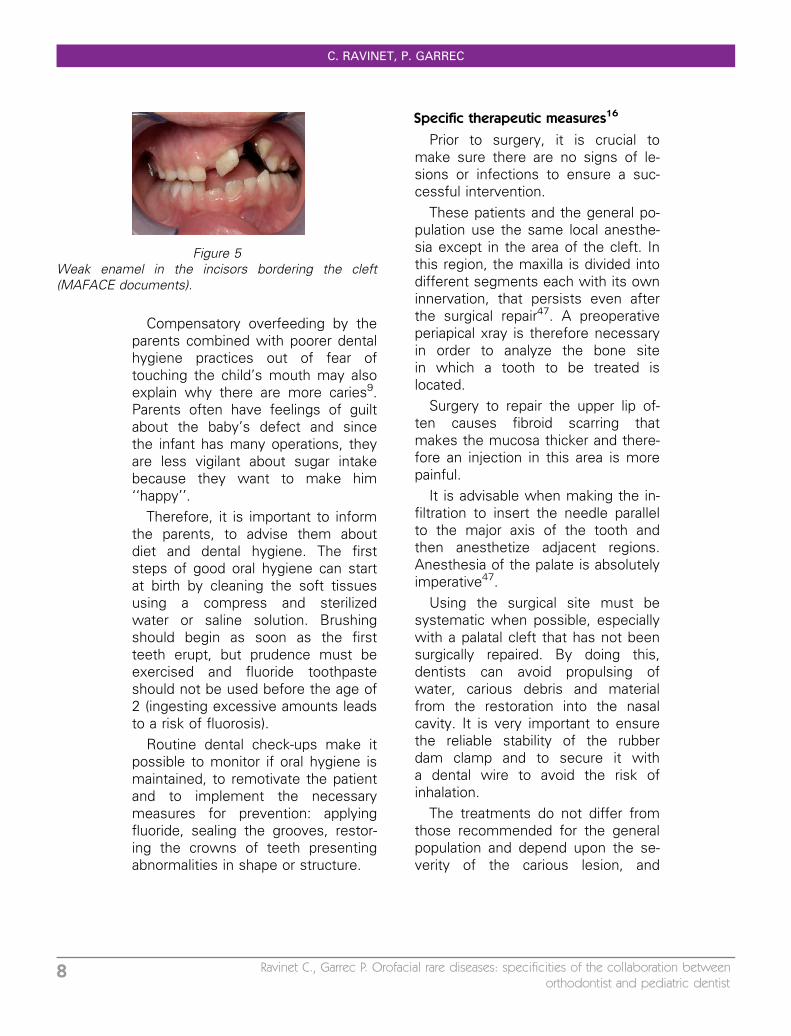
The increased prevalence of cariesmight be explained by the specialcharacteristics affecting the dentalhygiene of these patients: anatomyaround the cleft (Fig. 4) and dentalabnormalities in the area of the cleft(of structure, of shape, of number, ofposition)27. In fact, according to Pe-gelow38, there is an increase in thefrequency of small teeth for cleft lipand cleft palate and increase in mal-formations of the lateral incisors forclefts of the lip and alveolus. Toothenamel defects are significantly morecommon on the side of cleft in theprimary and permanent dentition thatparticularly affects the permanent in-cisors26. The dental enamel defectresults from a disturbance in the de-velopment of the organic matrix and/or of the mineralization process caus-ing enamel hypoplasia +/- associatedwith a hypomineralization that has anesthetic impact and also increasesthe risk of secondary caries by foster-ing the buildup of plaque (Fig. 5).
Figure 46 yr old patient with a right-sided unilat-eral cleft and carious lesions on the teethbordering the edges of the cleft (52 and51) (MAFACE documents).
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 7
Compensatory overfeeding by theparents combined with poorer dentalhygiene practices out of fear oftouching the child’s mouth may alsoexplain why there are more caries9.Parents often have feelings of guiltabout the baby’s defect and sincethe infant has many operations, theyare less vigilant about sugar intakebecause they want to make him‘‘happy’’.
Therefore, it is important to informthe parents, to advise them aboutdiet and dental hygiene. The firststeps of good oral hygiene can startat birth by cleaning the soft tissuesusing a compress and sterilizedwater or saline solution. Brushingshould begin as soon as the firstteeth erupt, but prudence must beexercised and fluoride toothpasteshould not be used before the age of2 (ingesting excessive amounts leadsto a risk of fluorosis).
Routine dental check-ups make itpossible to monitor if oral hygiene ismaintained, to remotivate the patientand to implement the necessarymeasures for prevention: applyingfluoride, sealing the grooves, restor-ing the crowns of teeth presentingabnormalities in shape or structure.
Specific therapeutic measures16
Prior to surgery, it is crucial tomake sure there are no signs of le-sions or infections to ensure a suc-cessful intervention.
These patients and the general po-pulation use the same local anesthe-sia except in the area of the cleft. Inthis region, the maxilla is divided intodifferent segments each with its owninnervation, that persists even afterthe surgical repair47. A preoperativeperiapical xray is therefore necessaryin order to analyze the bone sitein which a tooth to be treated islocated.
Surgery to repair the upper lip of-ten causes fibroid scarring thatmakes the mucosa thicker and there-fore an injection in this area is morepainful.
It is advisable when making the in-filtration to insert the needle parallelto the major axis of the tooth andthen anesthetize adjacent regions.Anesthesia of the palate is absolutelyimperative47.
Using the surgical site must besystematic when possible, especiallywith a palatal cleft that has not beensurgically repaired. By doing this,dentists can avoid propulsing ofwater, carious debris and materialfrom the restoration into the nasalcavity. It is very important to ensurethe reliable stability of the rubberdam clamp and to secure it witha dental wire to avoid the risk ofinhalation.
The treatments do not differ fromthose recommended for the generalpopulation and depend upon the se-verity of the carious lesion, and
Figure 5Weak enamel in the incisors bordering the cleft(MAFACE documents).
C. RAVINET, P. GARREC
8 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
pulpal as well as periodontal involve-ment.
It is advisable to preserve thesupernumerary primary teeth or teethincorrectly positioned in the area ofthe cleft as long as possible in orderto preserve as much bone mass aspossible in this region.
Role of the orthodontist
(refer to the article of BrigitteVi-Fane in this same issue)
Throughout treatment, the ortho-dontist should remain vigilant andshould require that parents maintaina proper diet and good dental hy-giene for the patient. The orthodon-tist should recommend regularfollow-up with a pediatric dentist andshould refer the patient if there isany hint of a carious lesion. The pa-tient will benefit from their close col-laboration.
HEREDITARY DENTINOGENESIS IMPERFECTA (HDI)
Characteristics
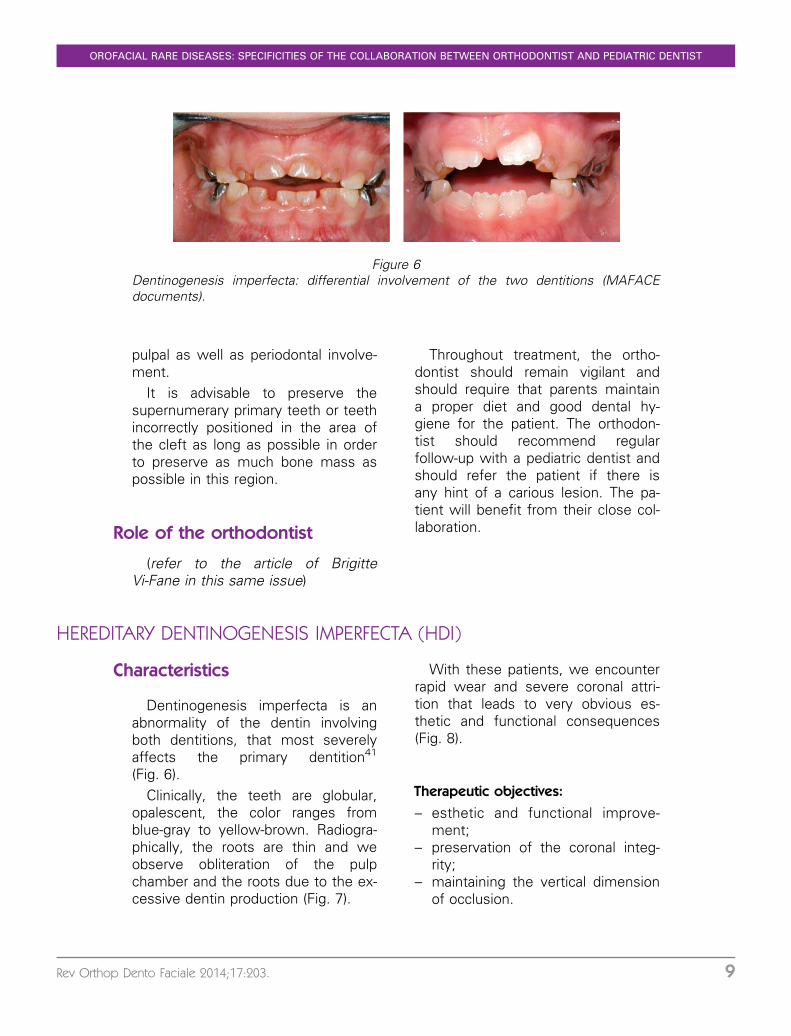
Dentinogenesis imperfecta is anabnormality of the dentin involvingboth dentitions, that most severelyaffects the primary dentition41
(Fig. 6).Clinically, the teeth are globular,
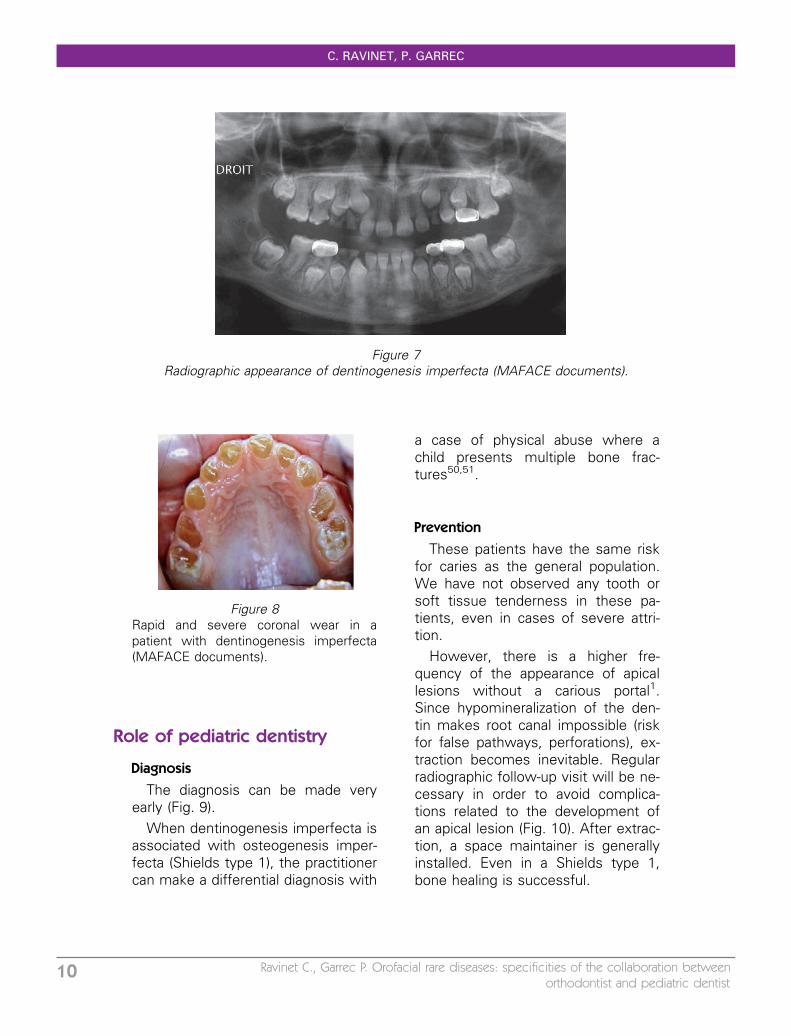
opalescent, the color ranges fromblue-gray to yellow-brown. Radiogra-phically, the roots are thin and weobserve obliteration of the pulpchamber and the roots due to the ex-cessive dentin production (Fig. 7).
With these patients, we encounterrapid wear and severe coronal attri-tion that leads to very obvious es-thetic and functional consequences(Fig. 8).
Therapeutic objectives:
– esthetic and functional improve-ment;
– preservation of the coronal integ-rity;
– maintaining the vertical dimensionof occlusion.
Figure 6Dentinogenesis imperfecta: differential involvement of the two dentitions (MAFACEdocuments).
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 9
Role of pediatric dentistry
Diagnosis
The diagnosis can be made veryearly (Fig. 9).
When dentinogenesis imperfecta isassociated with osteogenesis imper-fecta (Shields type 1), the practitionercan make a differential diagnosis with
a case of physical abuse where achild presents multiple bone frac-tures50,51.
Prevention
These patients have the same riskfor caries as the general population.We have not observed any tooth orsoft tissue tenderness in these pa-tients, even in cases of severe attri-tion.
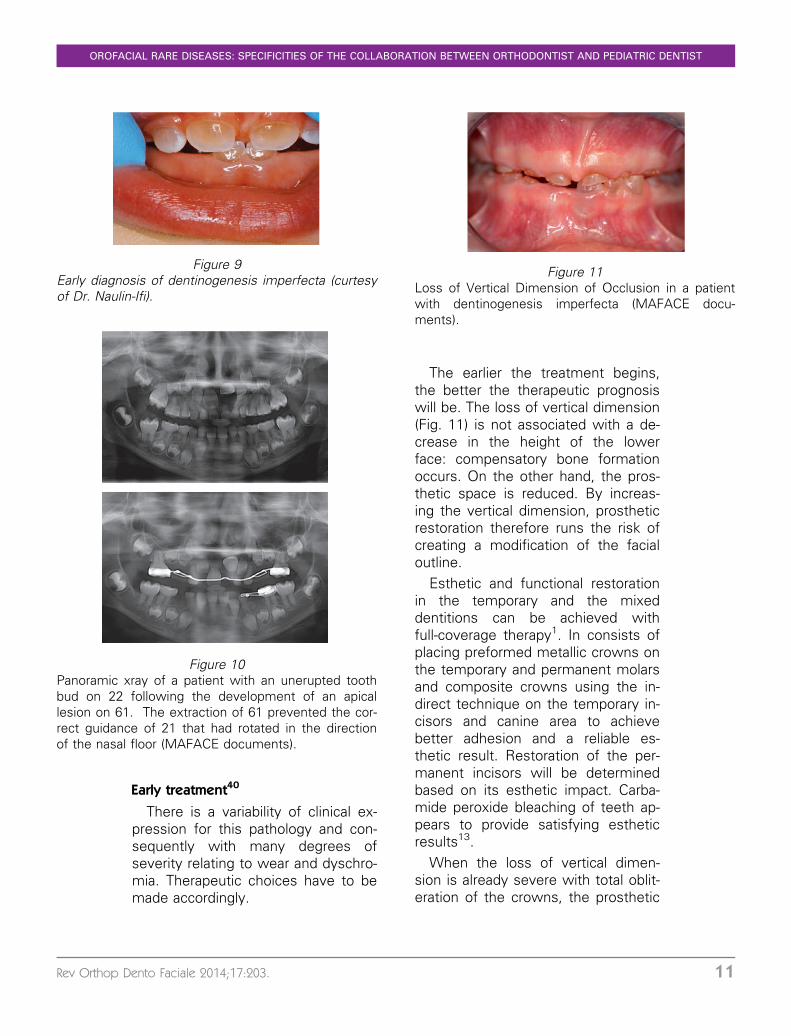
However, there is a higher fre-quency of the appearance of apicallesions without a carious portal1.Since hypomineralization of the den-tin makes root canal impossible (riskfor false pathways, perforations), ex-traction becomes inevitable. Regularradiographic follow-up visit will be ne-cessary in order to avoid complica-tions related to the development ofan apical lesion (Fig. 10). After extrac-tion, a space maintainer is generallyinstalled. Even in a Shields type 1,bone healing is successful.
Figure 7Radiographic appearance of dentinogenesis imperfecta (MAFACE documents).
Figure 8Rapid and severe coronal wear in apatient with dentinogenesis imperfecta(MAFACE documents).
C. RAVINET, P. GARREC
10 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
Early treatment40
There is a variability of clinical ex-pression for this pathology and con-sequently with many degrees ofseverity relating to wear and dyschro-mia. Therapeutic choices have to bemade accordingly.
The earlier the treatment begins,the better the therapeutic prognosiswill be. The loss of vertical dimension(Fig. 11) is not associated with a de-crease in the height of the lowerface: compensatory bone formationoccurs. On the other hand, the pros-thetic space is reduced. By increas-ing the vertical dimension, prostheticrestoration therefore runs the risk ofcreating a modification of the facialoutline.
Esthetic and functional restorationin the temporary and the mixeddentitions can be achieved withfull-coverage therapy1. In consists ofplacing preformed metallic crowns onthe temporary and permanent molarsand composite crowns using the in-direct technique on the temporary in-cisors and canine area to achievebetter adhesion and a reliable es-thetic result. Restoration of the per-manent incisors will be determinedbased on its esthetic impact. Carba-mide peroxide bleaching of teeth ap-pears to provide satisfying estheticresults13.
When the loss of vertical dimen-sion is already severe with total oblit-eration of the crowns, the prosthetic
Figure 9Early diagnosis of dentinogenesis imperfecta (curtesyof Dr. Naulin-Ifi).
Figure 10Panoramic xray of a patient with an unerupted toothbud on 22 following the development of an apicallesion on 61. The extraction of 61 prevented the cor-rect guidance of 21 that had rotated in the directionof the nasal floor (MAFACE documents).
Figure 11Loss of Vertical Dimension of Occlusion in a patientwith dentinogenesis imperfecta (MAFACE docu-ments).
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 11
restoration will consist of a singleprosthesis that overlays the completedentures1.
Role of the orthodontist
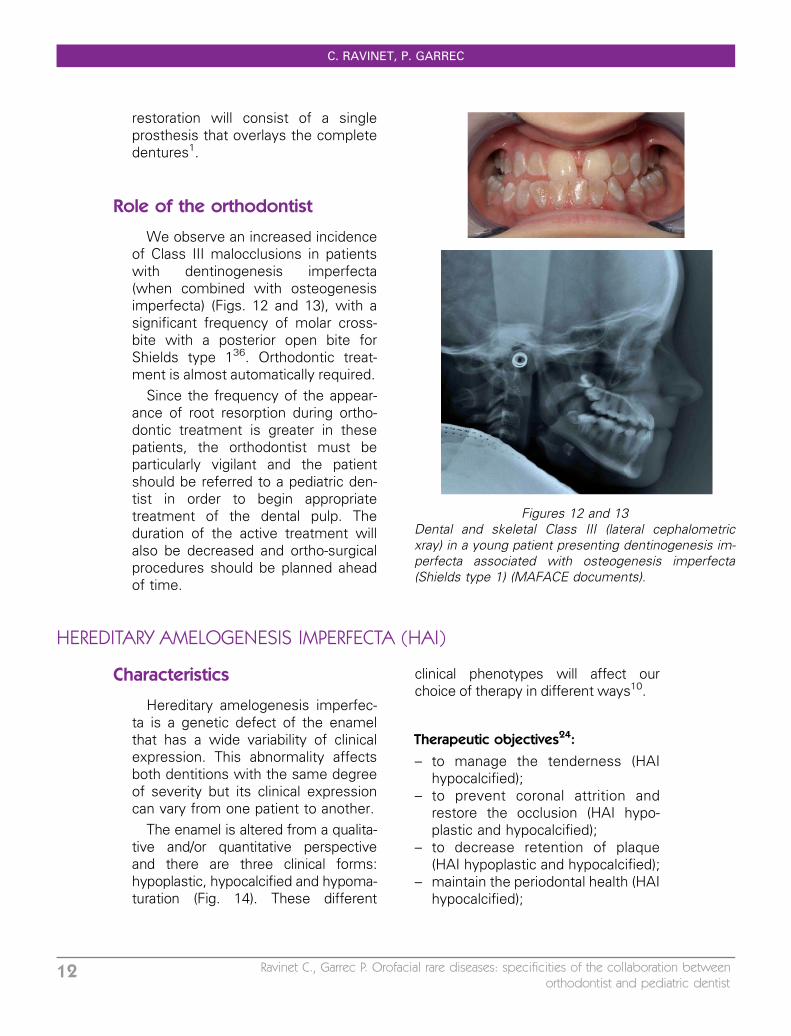
We observe an increased incidenceof Class III malocclusions in patientswith dentinogenesis imperfecta(when combined with osteogenesisimperfecta) (Figs. 12 and 13), with asignificant frequency of molar cross-bite with a posterior open bite forShields type 136. Orthodontic treat-ment is almost automatically required.
Since the frequency of the appear-ance of root resorption during ortho-dontic treatment is greater in thesepatients, the orthodontist must beparticularly vigilant and the patientshould be referred to a pediatric den-tist in order to begin appropriatetreatment of the dental pulp. Theduration of the active treatment willalso be decreased and ortho-surgicalprocedures should be planned aheadof time.
HEREDITARY AMELOGENESIS IMPERFECTA (HAI)
Characteristics
Hereditary amelogenesis imperfec-ta is a genetic defect of the enamelthat has a wide variability of clinicalexpression. This abnormality affectsboth dentitions with the same degreeof severity but its clinical expressioncan vary from one patient to another.
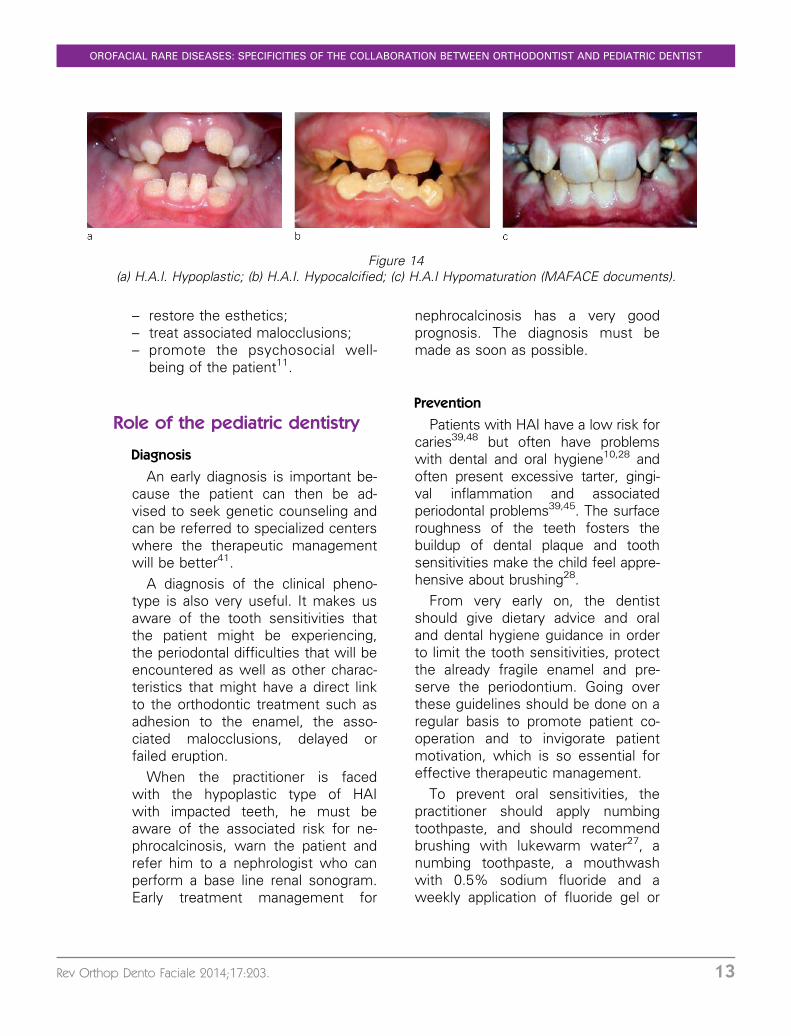
The enamel is altered from a qualita-tive and/or quantitative perspectiveand there are three clinical forms:hypoplastic, hypocalcified and hypoma-turation (Fig. 14). These different
clinical phenotypes will affect ourchoice of therapy in different ways10.
Therapeutic objectives24:
– to manage the tenderness (HAIhypocalcified);
– to prevent coronal attrition andrestore the occlusion (HAI hypo-plastic and hypocalcified);
– to decrease retention of plaque(HAI hypoplastic and hypocalcified);
– maintain the periodontal health (HAIhypocalcified);
Figures 12 and 13Dental and skeletal Class III (lateral cephalometricxray) in a young patient presenting dentinogenesis im-perfecta associated with osteogenesis imperfecta(Shields type 1) (MAFACE documents).
C. RAVINET, P. GARREC
12 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
– restore the esthetics;– treat associated malocclusions;– promote the psychosocial well-
being of the patient11.
Role of the pediatric dentistry
Diagnosis
An early diagnosis is important be-cause the patient can then be ad-vised to seek genetic counseling andcan be referred to specialized centerswhere the therapeutic managementwill be better41.
A diagnosis of the clinical pheno-type is also very useful. It makes usaware of the tooth sensitivities thatthe patient might be experiencing,the periodontal difficulties that will beencountered as well as other charac-teristics that might have a direct linkto the orthodontic treatment such asadhesion to the enamel, the asso-ciated malocclusions, delayed orfailed eruption.
When the practitioner is facedwith the hypoplastic type of HAIwith impacted teeth, he must beaware of the associated risk for ne-phrocalcinosis, warn the patient andrefer him to a nephrologist who canperform a base line renal sonogram.Early treatment management for
nephrocalcinosis has a very goodprognosis. The diagnosis must bemade as soon as possible.
Prevention
Patients with HAI have a low risk forcaries39,48 but often have problemswith dental and oral hygiene10,28 andoften present excessive tarter, gingi-val inflammation and associatedperiodontal problems39,45. The surfaceroughness of the teeth fosters thebuildup of dental plaque and toothsensitivities make the child feel appre-hensive about brushing28.
From very early on, the dentistshould give dietary advice and oraland dental hygiene guidance in orderto limit the tooth sensitivities, protectthe already fragile enamel and pre-serve the periodontium. Going overthese guidelines should be done on aregular basis to promote patient co-operation and to invigorate patientmotivation, which is so essential foreffective therapeutic management.
To prevent oral sensitivities, thepractitioner should apply numbingtoothpaste, and should recommendbrushing with lukewarm water27, anumbing toothpaste, a mouthwashwith 0.5% sodium fluoride and aweekly application of fluoride gel or
Figure 14(a) H.A.I. Hypoplastic; (b) H.A.I. Hypocalcified; (c) H.A.I Hypomaturation (MAFACE documents).
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 13

paste. These preventive measuresstrengthen resistance to deminerali-zation, significantly reduce tooth sen-sitivities, and foster enamelremineralization and post-eruptivematuration2. It should also be pointedout that a daily application ofcasein phosphopeptide combinedwith amorphous calcium phosphate(CPP-ACP) that makes it possible toaccelerate remineralization, to hardenthe enamel, to reduce enamel demi-neralization, decrease oral sensitiv-ities and to improve esthetics17.
Using a surgical dam also allowsthe surgeon to protect the non-trea-ted teeth (therefore unanesthetized)from thermal damage.
Early management of tooth sensi-tivities will provide comfort to the pa-tient but will also promote betteradhesion and more esthetically pleas-ing restorations in a healthy gingivalenvironment28,30. In addition, sensi-tivities often give rise to anxious be-havior towards treatment that canfurther complicate the managementof these patients28.
We observe rapid wear of theteeth in patients who have HAI39.Therefore, it is important to preservethe coronal integrity as soon as pos-sible in order to limit the loss of verti-cal dimension and of arch length.Coronal restorations with completecoverage are a good way to achievethis in the primary dentition and inthe immature permanent dentition,thus providing esthetic enhancementas well as a reduction in sensitiv-ities30. Moreover, these restorationsare recommended as soon as theproximal surfaces are affected41.
Esthetic and conservative treatments
In mild cases of HAI (especially forthe hypoplastic forms), a classic com-posite restoration can be fabricatedusing the direct technique. Estheticsand plaque control will both be im-proved, since the enamel surface willnow be smoother.
In cases where the damage ismore severe (especially for the hypo-mineralized forms), it is advisable toplan for total restoration with ceramiccrowns12,45 using the preformed pe-diatric composite crowns, compositecrowns by the indirect technique, apolycarbonate temporary crown,composite or ceramic veneers.
Posterior areas
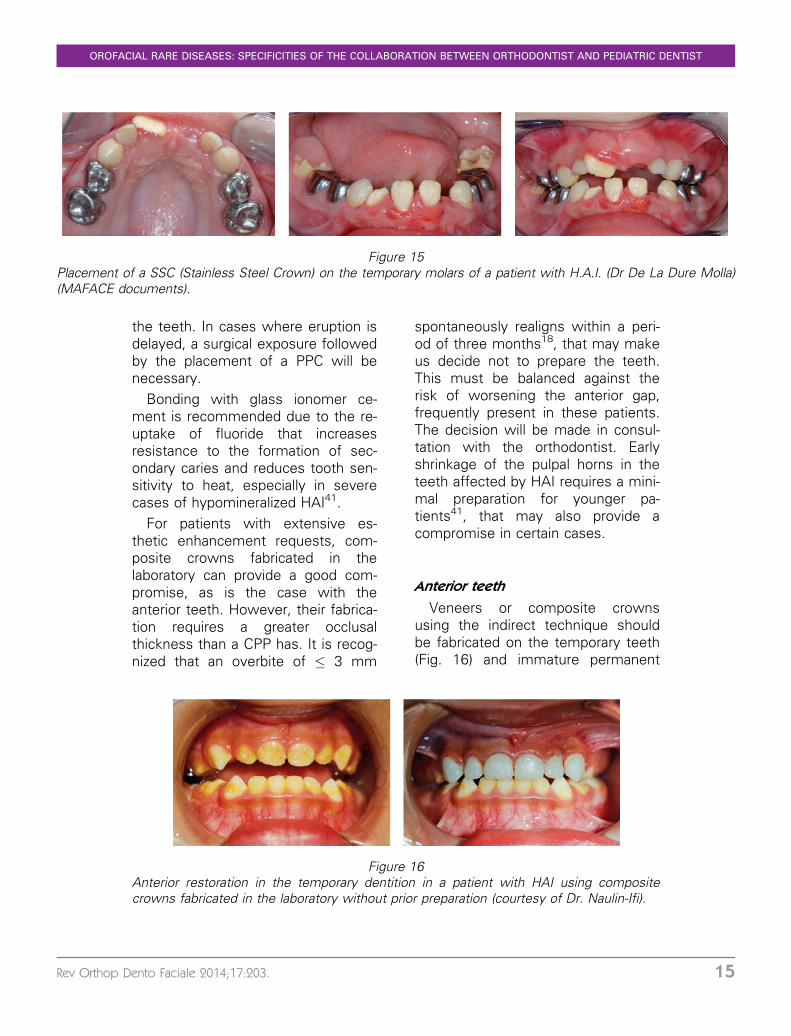
Generally, it is advisable to seal/bond the preformed pediatric crowns(PPC) on the temporary and perma-nent molars as soon as possible(Fig. 15). Placement is simple and ra-pid, their cost is still moderate andtheir long term resistance is reliableover time. They can be installed withno prior preparation of the tooth.Orthodontic separators (rings) can beplaced a few days before to avoidpreparing the proximal surfaces45.Therefore, it is possible to preservethe integrity and the vitality of thetooth by reducing tooth sensitivitiesand to foster improved oral and den-tal hygiene. The proximal and occlu-sal relationships can be correctlyestablished, the vertical dimensionand arch length are maintained andfunction is improved. Placement of aPPC also makes it easier to installorthodontic brackets with no risk to
C. RAVINET, P. GARREC
14 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
the teeth. In cases where eruption isdelayed, a surgical exposure followedby the placement of a PPC will benecessary.
Bonding with glass ionomer ce-ment is recommended due to the re-uptake of fluoride that increasesresistance to the formation of sec-ondary caries and reduces tooth sen-sitivity to heat, especially in severecases of hypomineralized HAI41.
For patients with extensive es-thetic enhancement requests, com-posite crowns fabricated in thelaboratory can provide a good com-promise, as is the case with theanterior teeth. However, their fabrica-tion requires a greater occlusalthickness than a CPP has. It is recog-nized that an overbite of � 3 mm
spontaneously realigns within a peri-od of three months18, that may makeus decide not to prepare the teeth.This must be balanced against therisk of worsening the anterior gap,frequently present in these patients.The decision will be made in consul-tation with the orthodontist. Earlyshrinkage of the pulpal horns in theteeth affected by HAI requires a mini-mal preparation for younger pa-tients41, that may also provide acompromise in certain cases.
Anterior teeth
Veneers or composite crownsusing the indirect technique shouldbe fabricated on the temporary teeth(Fig. 16) and immature permanent
Figure 15Placement of a SSC (Stainless Steel Crown) on the temporary molars of a patient with H.A.I. (Dr De La Dure Molla)(MAFACE documents).
Figure 16Anterior restoration in the temporary dentition in a patient with HAI using compositecrowns fabricated in the laboratory without prior preparation (courtesy of Dr. Naulin-Ifi).
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 15
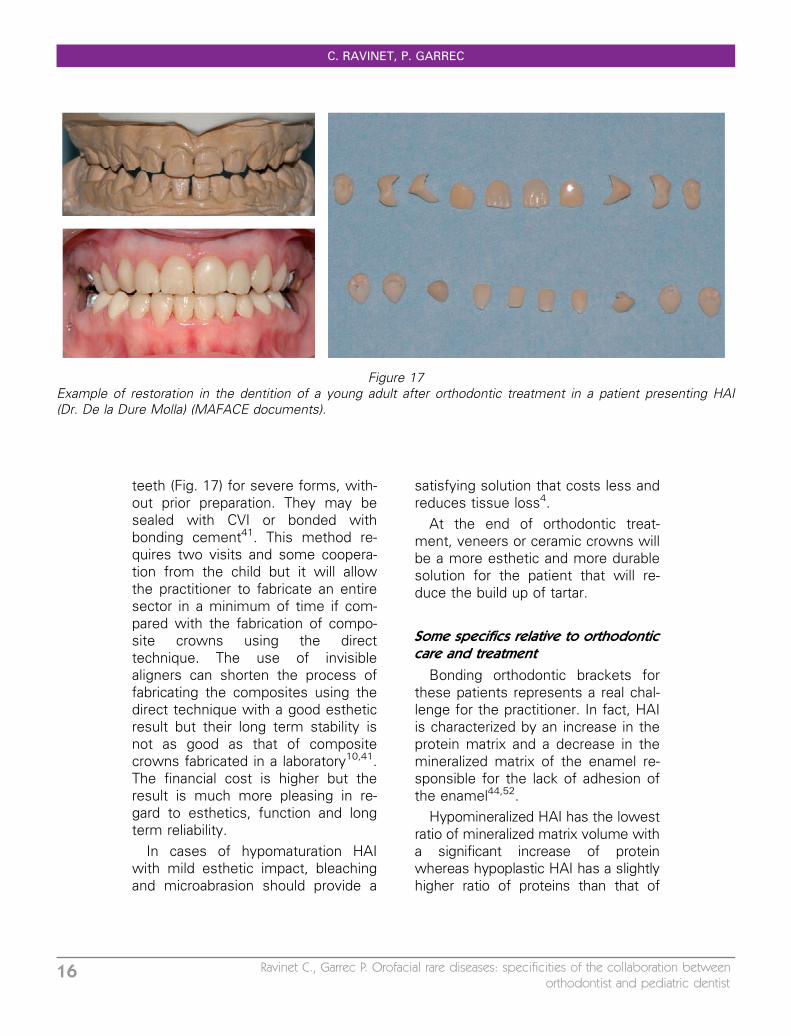
teeth (Fig. 17) for severe forms, with-out prior preparation. They may besealed with CVI or bonded withbonding cement41. This method re-quires two visits and some coopera-tion from the child but it will allowthe practitioner to fabricate an entiresector in a minimum of time if com-pared with the fabrication of compo-site crowns using the directtechnique. The use of invisiblealigners can shorten the process offabricating the composites using thedirect technique with a good estheticresult but their long term stability isnot as good as that of compositecrowns fabricated in a laboratory10,41.The financial cost is higher but theresult is much more pleasing in re-gard to esthetics, function and longterm reliability.
In cases of hypomaturation HAIwith mild esthetic impact, bleachingand microabrasion should provide a
satisfying solution that costs less andreduces tissue loss4.
At the end of orthodontic treat-ment, veneers or ceramic crowns willbe a more esthetic and more durablesolution for the patient that will re-duce the build up of tartar.
Some specifics relative to orthodonticcare and treatment
Bonding orthodontic brackets forthese patients represents a real chal-lenge for the practitioner. In fact, HAIis characterized by an increase in theprotein matrix and a decrease in themineralized matrix of the enamel re-sponsible for the lack of adhesion ofthe enamel44,52.
Hypomineralized HAI has the lowestratio of mineralized matrix volume witha significant increase of proteinwhereas hypoplastic HAI has a slightlyhigher ratio of proteins than that of
Figure 17Example of restoration in the dentition of a young adult after orthodontic treatment in a patient presenting HAI(Dr. De la Dure Molla) (MAFACE documents).
C. RAVINET, P. GARREC
16 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
healthy enamel. The adhesion of thecomposite resins on hypomineralizedenamel is significantly worse than onhealthy enamel20.
An accurate reading of an xray allowsthe practitioner to assess the thicknessof the enamel and consequently to an-ticipate problems with bonding12.
A clinical diagnosis then directly influ-ences the choice of protocol for bond-ing to the enamel for preventive careand bonding of orthodontic brackets.
A pretreatment of the enamel with5% sodium hypochlorite make it pos-sible to degrade the protein matrixand therefore enhances bond-ing42,49,53. Next, it is advisable touse self-etching adhesives ratherthan traditional etching with phospho-ric acid that causes loss of enameland is consequently responsible forinferior adhesion41.
Teeth affected by hypomineralizedHAI show a loss of post-eruptive en-amel surface (secondary hypoplasias)leading to exposed dentin. The useof dentin adhesives or placement ofglass ionomer cement before thecomposite restoration helps to mini-mize the risk of adhesion failure45.
HAI may be associated with gingi-val hyperplasia39 that requires period-ontal surgery in order to prepare theteeth for care and for bonding oforthodontic brackets.
Influence of HAI on orthodontictreatment management
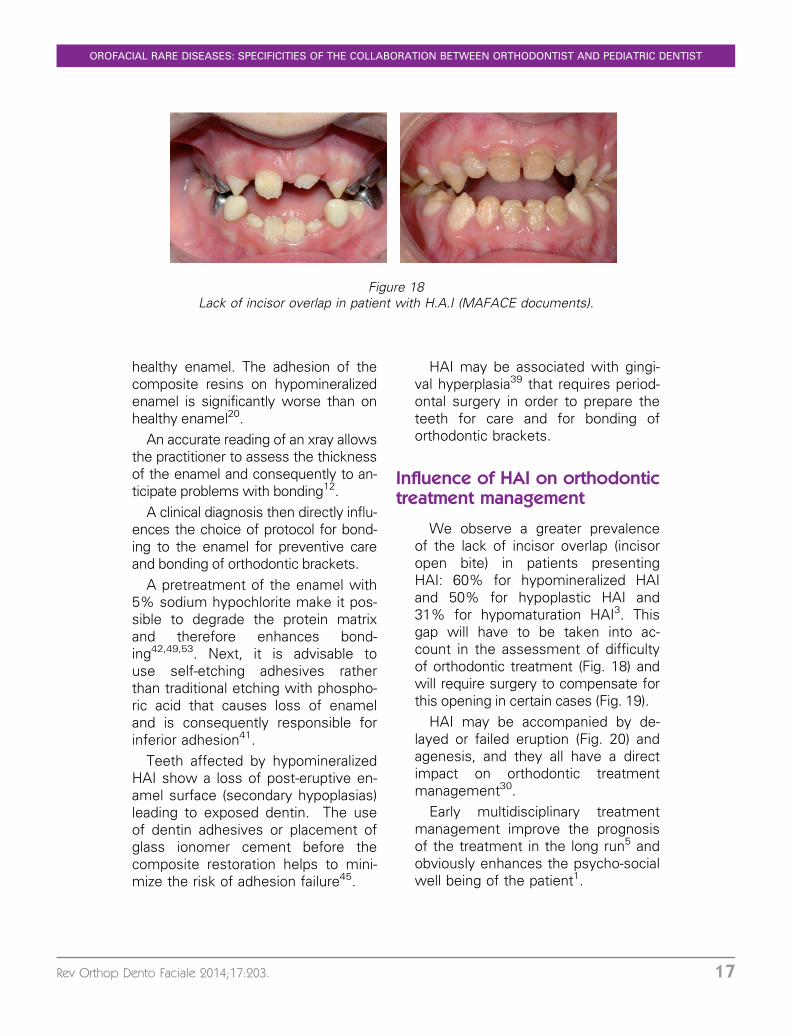
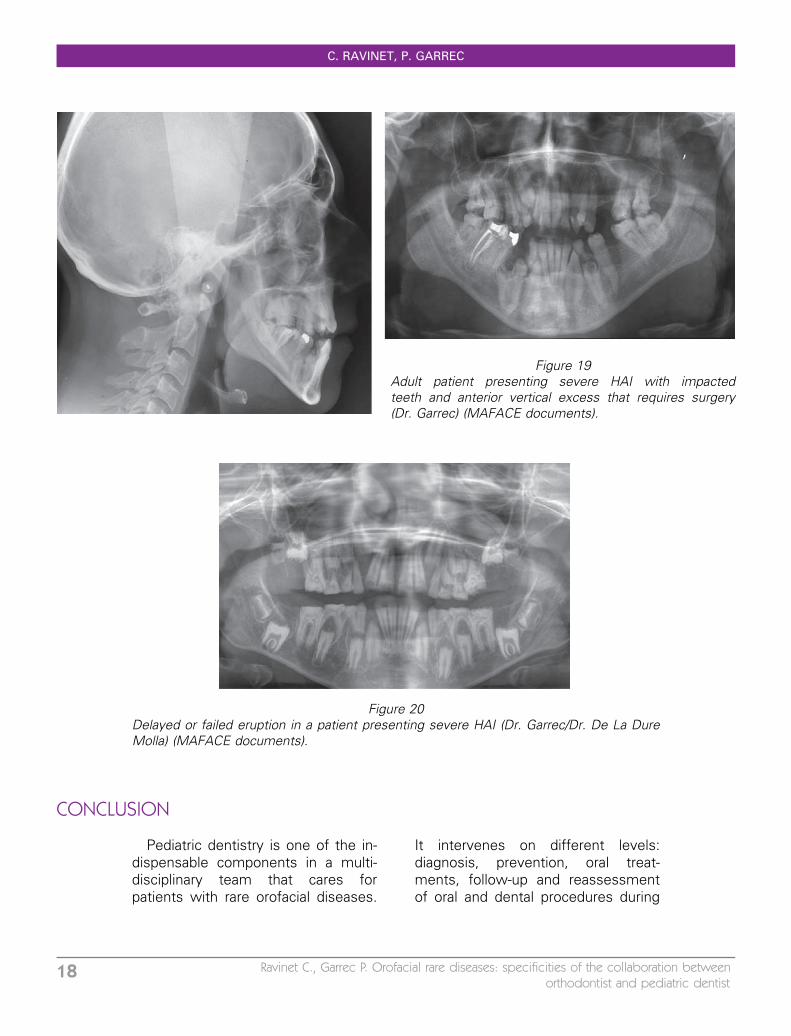
We observe a greater prevalenceof the lack of incisor overlap (incisoropen bite) in patients presentingHAI: 60% for hypomineralized HAIand 50% for hypoplastic HAI and31% for hypomaturation HAI3. Thisgap will have to be taken into ac-count in the assessment of difficultyof orthodontic treatment (Fig. 18) andwill require surgery to compensate forthis opening in certain cases (Fig. 19).
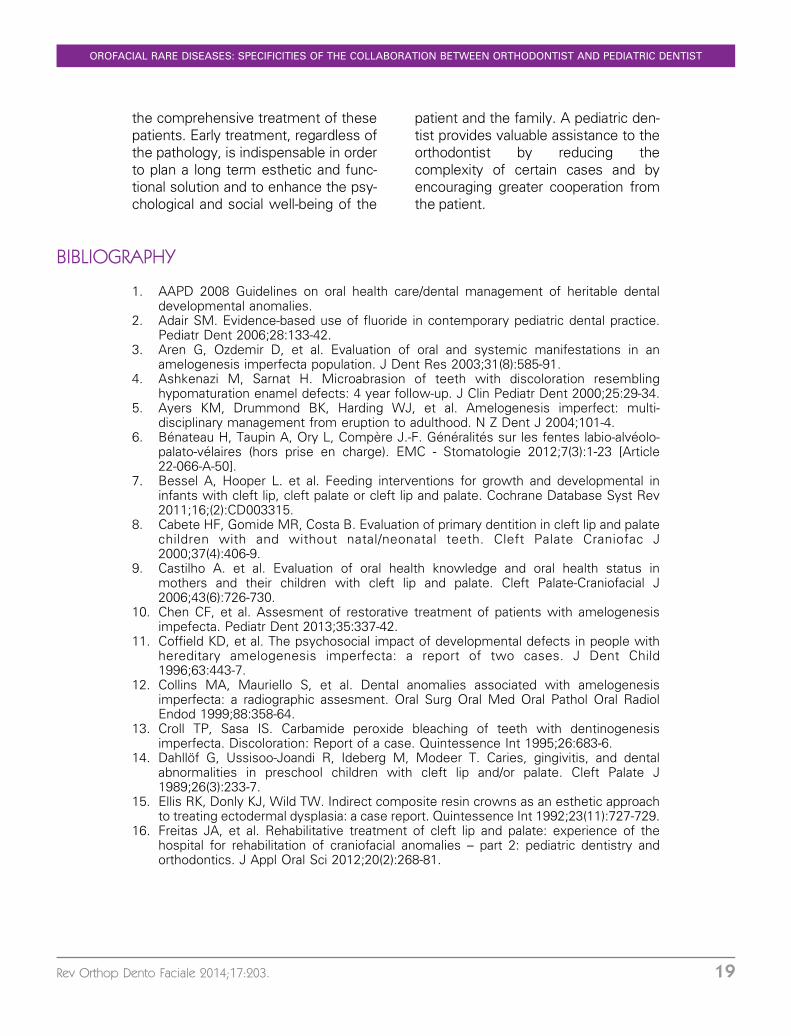
HAI may be accompanied by de-layed or failed eruption (Fig. 20) andagenesis, and they all have a directimpact on orthodontic treatmentmanagement30.
Early multidisciplinary treatmentmanagement improve the prognosisof the treatment in the long run5 andobviously enhances the psycho-socialwell being of the patient1.
Figure 18Lack of incisor overlap in patient with H.A.I (MAFACE documents).
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 17
CONCLUSION
Pediatric dentistry is one of the in-dispensable components in a multi-disciplinary team that cares forpatients with rare orofacial diseases.
It intervenes on different levels:diagnosis, prevention, oral treat-ments, follow-up and reassessmentof oral and dental procedures during
Figure 20Delayed or failed eruption in a patient presenting severe HAI (Dr. Garrec/Dr. De La DureMolla) (MAFACE documents).
Figure 19Adult patient presenting severe HAI with impactedteeth and anterior vertical excess that requires surgery(Dr. Garrec) (MAFACE documents).
C. RAVINET, P. GARREC
18 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
the comprehensive treatment of thesepatients. Early treatment, regardless ofthe pathology, is indispensable in orderto plan a long term esthetic and func-tional solution and to enhance the psy-chological and social well-being of the
patient and the family. A pediatric den-tist provides valuable assistance to theorthodontist by reducing thecomplexity of certain cases and byencouraging greater cooperation fromthe patient.
BIBLIOGRAPHY
1. AAPD 2008 Guidelines on oral health care/dental management of heritable dentaldevelopmental anomalies.
2. Adair SM. Evidence-based use of fluoride in contemporary pediatric dental practice.Pediatr Dent 2006;28:133-42.
3. Aren G, Ozdemir D, et al. Evaluation of oral and systemic manifestations in anamelogenesis imperfecta population. J Dent Res 2003;31(8):585-91.
4. Ashkenazi M, Sarnat H. Microabrasion of teeth with discoloration resemblinghypomaturation enamel defects: 4 year follow-up. J Clin Pediatr Dent 2000;25:29-34.
5. Ayers KM, Drummond BK, Harding WJ, et al. Amelogenesis imperfect: multi-disciplinary management from eruption to adulthood. N Z Dent J 2004;101-4.
6. Benateau H, Taupin A, Ory L, Compere J.-F. Generalites sur les fentes labio-alveolo-palato-velaires (hors prise en charge). EMC - Stomatologie 2012;7(3):1-23 [Article22-066-A-50].
7. Bessel A, Hooper L. et al. Feeding interventions for growth and developmental ininfants with cleft lip, cleft palate or cleft lip and palate. Cochrane Database Syst Rev2011;16;(2):CD003315.
8. Cabete HF, Gomide MR, Costa B. Evaluation of primary dentition in cleft lip and palatechildren with and without natal/neonatal teeth. Cleft Palate Craniofac J2000;37(4):406-9.
9. Castilho A. et al. Evaluation of oral health knowledge and oral health status inmothers and their children with cleft lip and palate. Cleft Palate-Craniofacial J2006;43(6):726-730.
10. Chen CF, et al. Assesment of restorative treatment of patients with amelogenesisimpefecta. Pediatr Dent 2013;35:337-42.
11. Coffield KD, et al. The psychosocial impact of developmental defects in people withhereditary amelogenesis imperfecta: a report of two cases. J Dent Child1996;63:443-7.
12. Collins MA, Mauriello S, et al. Dental anomalies associated with amelogenesisimperfecta: a radiographic assesment. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1999;88:358-64.
13. Croll TP, Sasa IS. Carbamide peroxide bleaching of teeth with dentinogenesisimperfecta. Discoloration: Report of a case. Quintessence Int 1995;26:683-6.
14. Dahllof G, Ussisoo-Joandi R, Ideberg M, Modeer T. Caries, gingivitis, and dentalabnormalities in preschool children with cleft lip and/or palate. Cleft Palate J1989;26(3):233-7.
15. Ellis RK, Donly KJ, Wild TW. Indirect composite resin crowns as an esthetic approachto treating ectodermal dysplasia: a case report. Quintessence Int 1992;23(11):727-729.
16. Freitas JA, et al. Rehabilitative treatment of cleft lip and palate: experience of thehospital for rehabilitation of craniofacial anomalies – part 2: pediatric dentistry andorthodontics. J Appl Oral Sci 2012;20(2):268-81.
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 19
17. Giniger M, MacDonald J, Ziemba S, et al. The clinical performance of professionnallydispensed bleaching gel with added amorphous calcium phosphate. J Am Dent Assoc2005;136:383-92.
18. Harley KE, Ibetson RJ. Dental anomalies: are adhesive castings the solution? Br Dent J1993;174:15-22.
19. Hobkirk JA, Nohl F, et al. The management of ectodermal dysplasia and severehypodontia. International conference statements. J Oral Rehab 2006;33:634-637.
20. Hosein I, Sheriff M, Ireland AJ. Enamel loss during bonding, debonding and clean upwith use of a self-etching primer. AM J Othod Dentofacial Orthop 2004;126:717-24.
21. Johnsen DC, Dixon M. Dental caries of primary incisors in children with cleft lip andpalate. Cleft Palate J 1984;21:104-109.
22. Kotsiomiti E, Arapostathis K, Kapari D, Konstantinidis A. Removable prosthodontictreatment for the primary and mixed dentition. J Clin Pediatr Dent 2000;24:83-89.
23. Kupietzky A, Houpt M. Hypohidrotic ectodermal dysplasia: characteristics andtreatment. Quintessence Int 1995;26:285-291.
24. Kwok-Tung L, King NM. The restorative management of amelogenesis imperfecta inthe mixed dentition. J Clin Pediatr Dent 2006;31:130-5.
25. Levander E, Malmgren O, Stenback K. Apical root resorption during orthodontictreatment of patients with multiple aplasia: a study of maxillary incisors. Eur JOrthodont 1998;20:427-434.
26. Maciel SP, Costa B, Gomide MR. Difference in the prevalence of enamel alterationsaffecting central incisors of children with complete unilateral cleft lip and palate. Cleftpalate Craniofacial J 2005;42(4):392-395.
27. McDonagh S, Pinson R, Shaw AJ. Provision of general dental care for children withcleft lip and palate—parental attitudes and experiences. Br Dent J 2000:189;432-434.
28. McDonald S, Arkutu N, et al. Managing the paediatric patient with amelogenesisimperfecta. Br Dent J 2012;212(9):425-428.
29. McLaughlin WS. Congenital absence of all primary and permanent lateral incisors in acarrier of X-linked hypohydrotic ectodermal dysplasia. Int J Paed Dent 1991;2:99-103.
30. Ng FK, Messer LB. Dental management of amelogenesis imperfecta patients: a primeron genotupe-phenotype correlations. Pediatr Dent 2009;31:20-30.
31. Nivoloni Tannure P, et al. Prevalence of dental anomalies in nonsyndromic individualswith clefts lip and palate/ A systematic review and meta-analysis. Cleft palateCraniofacial J 2012;49(2):194-200.
32. Nivoloni Tannure P, de Castro Costa M, Calvano Kuuchler E, et al. Caries experience inindividuals with cleft lip and palate. Pediatr Dent 2012;34:127-31.
33. Noble J. Motivations of orthodontics residents in Canada and the United States to treatpatients with craniofacial anomalies, cleft lip/palate, and special need. Cleft palateCraniofacial J 2012;49(5):596-600.
34. Nunn JH, Carter N, et al. The interdisciplinary management of hypodontia: backgroundand role of paediatric dentistry. Brit Dent J 2003;194(5):245-251.
35. Nussbaum B, Carrel R. The behaviour modification of a dentally disabled child. J DentChild 1976;43:255-261.
36. O’Connell A, Marini J. Evaluation of oral problems in an osteogenesis imperfectapopulation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87(2):189-96.
37. Opshal Vital S. Risque carieux et traitement orthodontique. International Orthodontics2010;8:28-45.
38. Pegelow M, Alqadi N, et al. The prevalence of various dental characteristics in theprimary and mixed dentition in patients born with non-syndromic unilateral cleft lip withor without cleft palate. Eur J Orthod 2012(34):561-570.
39. Poulsen S, Gjorup H, et al. Amelogenesis imperfecta: a systematic litterature review ofassociated dental and orofacial abnormalities and their impact on patients. ActaOdontol Scand 2008;66:193-9.
C. RAVINET, P. GARREC
20 Ravinet C., Garrec P. Orofacial rare diseases: specificities of the collaboration betweenorthodontist and pediatric dentist
40. Sapir S, Shapira Y. Dentinogenesis imperfecta: an early treatment strategy. PediatrDent 2001;23:232-7.
41. Sapir S, Shapira J. Clinical solutions for developmental defects of enamel and dentin inchildren. Pediatr Dent 2007;29:330-6.
42. Saroglu O, Aras S, Oztas D. Effect of deproteinization on composite bond strength inhypocalcified amelogenesis imperfecta. Oral Dis 2006;12:305-308.
43. Sasaki Y, Kaida C, Saitoh I, et al. Craniofacial growth and functionnal change inoligodontia with ectodermal dysplasia: a case report. J Oral Rehab 2007;34;228-235.
44. Seow WK, Amaratunge FA. The effect of acid etching on enamel from different clinicalvariants of amelogenesis imperfecta: an SEM study. Pediatr Dent 1998;30:37-42.
45. Seow WK. Clinical diagnosis and management strategies of amelogenesis imperfectavariants. Pediatr Dent 1993;15:384-93.
46. Silva Dalben G, et al. Breast-feeding and sugar intake in babies with cleft lip and palate.Cleft Palate Craniofac J 2003;40(1):84-7.
47. Silva Dalben G, et al. Dental anesthetic procedures for cleft lip and palate patients.J Clin Pediatr Dent 2000;24(3):153-8.
48. Sundell S. Hereditary amelogenesis imperfecta: an epidemiologicical, genetic, andclinical study in a Swedish child population. Swed Dent J Suppl 1986;31:1-38.
49. Venezie RD, Vadiakas G, et al. Enamel pretreatment with sodium hypochlorite toenhance bonding in hypocalcified amelogenesis imperfecta: case report and SEManalysis. Pediatr Dent 1994;16:433-436.
50. Welbury RR, Murphy JM. The dental practitionner’s role in protecting children fromabuse. 2. The orofacial signs of abuse. Br Dent J 1998;24:61-5.
51. Wright J, Thornton J. Osteogenesis imperfecta with dentinogenesis imperfecta: amistaken case of child abuse. Pediatr Dent 1983;5(3):207-9.
52. Wright JT, Deaton TC, Hall KI, et al. The mineral and protein content of enamel inamelogenesis imperfecta. Connect Tissue Res 1995;32:247-52.
53. Wright JT. The etch-bleach-seal technique for managing stained enamel defects inyoung permanent incisors. Pediatr Dent 2002;24:249-52.
OROFACIAL RARE DISEASES: SPECIFICITIES OF THE COLLABORATION BETWEEN ORTHODONTIST AND PEDIATRIC DENTIST
Rev Orthop Dento Faciale 2014;17:203. 21