Embed Size (px)
Citation preview

PDF hosted at the Radboud Repository of the Radboud University
Nijmegen
The following full text is a publisher's version.
For additional information about this publication click this link.
http://hdl.handle.net/2066/30190
Please be advised that this information was generated on 2020-03-15 and may be subject to
change.

Hig
h T
ibial O
steoto
my Treatm
ent o
f varus o
steoarth
ritis of th
e knee R
ob
ert D. A
. Gaasb
eek
Uitnodiging
Voor het bijwonen vande openbare verdediging
van het proefschrift
‘High tibial osteotomy.Treatment of varus osteoarthritis
of the knee’
op vrijdag 21 september 2007om 10.30 uur in de Aula Major
van de Radboud UniversiteitComeniuslaan 2 te Nijmegen.
Receptie na afloop ter plaatse
Robert GaasbeekKruisweg 16bis3513 CT Utrecht
De Paranimfen Huub van der Heide, tel: 06-43001007
[email protected] van der Gragt, tel: 06-21881485
Uitnodiging
Graag nodig ik u en uw partner uit voor het feest ter gelegenheid van
mijn promotie
zaterdag 22 september 2007 vanaf 20.00 uur
“Oranjerie Landgoed Maarsbergen” Maarnse Grindweg 30 3953 LW Maarsbergen
tel. 0343-431 [email protected]
Paranimfen:Huub van der Heide, tel: 06-43001007
[email protected] van der Gragt, tel: 06-21881485
High Tibial Osteotomy Treatment of varus osteoarthritis of the knee
Robert D. A. Gaasbeek
High Tibial Osteotomy Treatment of varus osteoarthritis of the knee
Robert D. A. Gaasbeek
High Tibial Osteotomy Treatment of varus osteoarthritis of the knee
Robert D. A. Gaasbeek

High Tibial Osteotomy Treatment of varus osteoarthritis of the knee
De valgiserende tibiakop osteotomieBehandeling van varus gonartrose
Robert D. A. Gaasbeek

High Tibial Osteotomy Treatment of varus osteoarthritis of the knee
De valgiserende tibiakop osteotomieBehandeling van varus gonartrose
een wetenschappelijke proeve op het gebied van de medische wetenschappen
Proefschrift
ter verkrijging van de graad van doctor
aan de Radboud Universiteit Nijmegen
op gezag van de Rector Magnificus prof. mr. S.C.J.J. Kortmann,
volgens het besluit van het College van Decanen
in het openbaar te verdedigen
op 21 september 2007 om 10.30 uur precies
door
Robert Dick Alexander Gaasbeek
geboren op 17 september 1969
te Zwolle
The publication of this thesis was financially supported by:
Nederlandse Orthopedische vereniging, Anna-Fonds te Leiden, Somas Chirurgische Techniek,
Bauerfeind Benelux BV, DePuy Implants, Zimmer Netherlands BV, Link Nederland,
Biomet Nederland BV, NTOC Medische Techniek, Eemland Orthopedie Techniek BV,
Mathys Orthopedics BV, Synthes BV, Hanssen Footcare, Roessingh Revalidatie Techniek BV,
Smith & Nephew BV, Janssen-Cilag BV, DJO/Aircast Benelux, Pro-Motion Medical BV Schiedam,
POM BV Nijmegen, Stryker BV.
High Tibial Osteotomy
Treatment of varus osteoarthritis of the knee
De valgiserende tibiakop osteotomie
Behandeling van varus gonarthrose
Thesis Radboud University Nijmegen Medical Centre
With summary in Dutch -136p.
© Copyright 2007 R.D.A. Gaasbeek
All rights are reserved. No part of this publication may be reproduced, stored in a retrieval system,
or transmitted in any form or by any means, mechanically, by photocopying, rcording, or otherwise,
without the written permission of the author.
ISBN/EAN: 978-90-9021884-7
Internet: http://webdoc.ubn.ru.nl/mono/g/gaasbeek _ r/hightios.pdf
Correspondence (e-mail) [email protected]
Cover: Harald Pieper
Lay-out: Harald Pieper
Print: Print Partners Ipskamp BV, Enschede, The Netherlands

Promotor:
prof. dr. A. van Kampen
Co-promotores:
dr. R.J. van Heerwaarden (Sint Maartenskliniek Nijmegen)
dr. ir. N.J.J. Verdonschot
Manuscriptcommissie:
prof. dr. A.C.H. Geurts
prof. dr. R.F.J.M. Laan
prof. dr. J.A.N. Verhaar (Erasmus Medisch Centrum Rotterdam)
Paranimfen:
drs. J.J. van der Gragt
drs. H.J.L. van der Heide
Voor mijn ouders

Contents
Chapter 1 General introduction, background and aims of the thesis
Chapter 2 Effects of valgus bracing on gait of patients with medial compartment
osteoarthritis of the knee
Gait Posture. 2007 June; 26 (1): 3-10
Chapter 3 Accuracy and initial stability of high tibial osteotomy;
A cadaveric RSA study of open versus closed wedge osteotomy
Knee Surg Sports Traumatol Arthrosc. 2005 Nov;13(8):689-94
Chapter 4 Correction accuracy and collateral laxity in open versus closed wedge
high tibial osteotomy. A one year randomized controlled study
J Bone Joint Surg Br.In revision
Chapter 5 Mechanism of incorporation of ß-TCP in patients in open wedge high
tibial osteotomy
Biomaterials. 2005 Nov;26(33):6713-9
Chapter 6 The influence of open and closed wedge high tibial osteotomy on patellar tracking
Knee Surg Sports Traumatol Arthrosc.2007 May 5; [Epub ahead of print] 2007
Chapter 7 Distal tuberosity osteotomy in open wedge high tibial osteotomy can
prevent patella infera; a new technique
Knee. 2004 Dec;11(6):457-6
Chapter 8 Summary, answers to research questions and closing remarks
Chapter 9 Samenvatting, beantwoording van de onderzoeksvragen
en afsluitende opmerkingen
Publications
Dankwoord
Curriclum Vitae
9
19
37
51
67
83
97
109
119
129
131
135

8
chapter 1General introduction, background
and aims of the thesis

10
Chapter 1
11
General introduction, background and aims of the thesis
Introduction
Osteoarthritis of the medial compartment of the knee in young active patients
represents a significant treatment challenge in orthopaedic practice. In most cases
medial compartment osteoarthritis of the knee is associated with varus leg alignment.
There is a wide range of treatment options, but the effectiveness of the different
treatments varies 1.
Non-operative treatment
Initial management for most patients should be non-operative and may include
physical therapy, bracing, orthoses, ambulatory aids, non-steroidal anti-inflammatory
medications, intra-articular steroid injections, and analgesics. Changes in habitual
activities including those related to work and recreation may also be necessary.
Obesity is a known risk factor for osteoarthritis of the knee, and weight loss has been
shown to slow the progression of the disease 1;2.
Operative treatment
Because of the progressive nature of the disease and because a varus malalignment
will lead to an ongoing unfavourable mechanical loading of the medial compartment,
many patients with medial osteoarthritis of the knee will eventually require operative
treatment. A variety of procedures have been described to treat the osteoarthritic knee,
ranging from arthroscopic lavage and debridement to total knee arthroplasty.
The choice of procedure depends on the patient’s age and activity expectations,
the severity of the disease, and the number of knee compartments involved.
One of these, high tibial osteotomy to the treat medial compartment osteoarthritis of
the knee, is the focus of this thesis.
High tibial osteotomy (HTO)
High tibial osteotomy is accepted as a valuable surgical option. Localized wear in
the knee results from a malalignment that has either produced the arthritis or has
aggravated it. For many years, the value of osteotomy was considered to be the load
transfer to the unaffected compartment of the knee which relieves symptoms and slows
disease progression. Osteotomy has been used extensively, with techniques becoming
more refined over time 3, 4. Furthermore, although the long term results of a total knee
arthroplasty are good, a significant concern remains regarding the longevity of the
prostheses which are placed, particularly in younger patients. In contrast, osteotomy
provides an alternative that preserves the knee joint, and when performed appropriately,
it should not compromise later arthroplasty if that becomes necessary. However,
although the results reported for a high tibial osteotomy vary considerably in the
literature, the procedure generally provides good pain relief and with restored function
at the 5-year follow up in approximately 80% to 90%, and at the 10-year follow up in 50%
to 65% 5-10. Most authors found that success was directly related to having achieved an
optimal alignment 6;9;11. Accurate preoperative assessment and technical precision are,
therefore, essential to achieve satisfactory outcomes. Many techniques have been
described for HTO, among them the lateral closed wedge and the medial open wedge.
Lateral closed wedge osteotomy (CWO)
The most commonly reported osteotomy for medial compartment osteoarthritis is the lateral
closed wedge osteotomy, popularized by Coventry and Insall et al. 4, 12. The goal is to
correct alignment as outlined earlier, which is achieved by removing a bone wedge from
the lateral tibia and closing the resultant defect. Many variations of this technique have
been described, but the general principle remains the same l 4;5;12;13. Traditionally,
the angular calculation is converted into the size of the wedge based on the tibial width
although newer instrument systems provide angled cutting jigs, thus eliminating the need
for this conversion. Many techniques can be used to treat the proximal tibiofibular joint,
including joint excision or disruption, fibular osteotomy, or excision of the fibular head.

12
Chapter 1
13
General introduction, background and aims of the thesis
Medial open wedge osteotomy (OWO)
While medial opening wedge osteotomy has not been as widely reported in the
English-speaking literature as the CWO technique, its use in Europe continues to
increase in popularity 14;15. The theoretical advantages of the opening wedge in
comparison to the closing wedge include restoring the anatomy by adding bone to
the diseased medial side as well as being able to achieve predictable correction in
both the coronal and sagittal planes and to adjust the correction intra-operatively.
Furthermore, only one bone cut is required and there is no proximal tibiofibular joint
disruption or invasion of the lateral compartment, and it is relatively easy to combine
with other procedures such as ACL reconstruction. However, there are also disadvantages.
These include the creation of a defect that requires bone graft with attendant harvest
morbidity, a theoretically higher risk for nonunion, and a longer postoperative period
of restricted weight-bearing. Graft choices include autograft, allograft, or preprepared
bone substitutes. Each option has its own advantages and disadvantages. Although
iliac crest autograft probably remains the current gold standard, a tricalciumphosphate
(TCP) bone substitute was used in the open wedge osteotomies we performed.
This avoids donor site morbidity and decreases surgical time.
Complications of high tibial osteotomy
Complications reported for high tibial osteotomy include recurrence of deformity (loss of
correction), peroneal nerve palsy, non-union, infection, knee stiffness or instability,
intra-articular fracture, deep venous thrombosis, compartment syndrome, patella infera,
change of tibial slope, and avascular necrosis of the proximal fragment. Some of these
complications are related to the particular osteotomy technique used, to type of fixation
chosen or the postoperative management selected. Since the introduction of more
stable implants and early postoperative mobilisation, complication rates have decreased.
Most HTO literature pertains to CWO. Complications after OWO were generally the
same, but for instance peroneal nerve problems would be unlikely to occur as no fibular
osteotomy has been performed. However, the lowering of the patella seemed to be a
more profound issue after OWO 16;17.
Background, outline and aims of this thesis
To treat patients who suffer from medial osteoarthritis of the knee, the orthopaedic
surgeon has access to a range of treatment possibilities. The choice whether non-
operative or operative procedures should be used depends on multiple factors.
The treatment strategy selected is the result of intensive dialogue between patient and
doctor and has to be based upon accurate information. New treatment options for this
patient group are continually being developed and enjoy increasing popularity.
New unloading braces have frequently been introduced as well as new operations,
using bone substitutes and stable implants. Although all these new developments are
important, it is necessary to remain critical and to compare these new alternatives to
the known forms of treatment. The author’s interest in the different treatment strategies
for patients with varus osteoarthritis of the knee formed the background of this thesis.
During the preliminary research on current developments in the treatment of medial
osteoarthritis of the knee, several aspects stood out. In the non-operative treatment
spectrum, the clinical significance of valgus brace treatment forms a recurrent topic in
the literature 18-30. Unloading valgus braces have been used as the definitive treatment
as well as during the preoperative assessment to simulate the effect of a valgus high
tibial osteotomy. A new brace was developed and one of the goals of this thesis was to
analyse the effects of such a brace on gait (Chapter 2). Many patients will eventually
need operative treatment in the form of a HTO. Since the introduction of new rigid stable
implants, the OWO is more frequently performed in recent years. Only a few comparative
studies between these two techniques have been published 15;31-33. We investigated the
differences between CWO and OWO with respect to biomechanical characteristics,
clinical outcome and histological aspects (Chapters 3-5). Cutting the bone proximally to
the tibial tuberosity with the subsequent valgus correction will change the position of
the patella, and therefore, hypothetically lead to changes in patellar tracking 16;17;31;34-46.
Therefore, another aim of this thesis was to study the patellar height and tracking
following HTO. Again the effects of CWO and OWO were compared (Chapter 6).
Finally, the question arose whether a technique could be proposed which avoids these
effects on the patella (Chapter 7).

14
Chapter 1
15
General introduction, background and aims of the thesis
The following research questions were formulated:
1. What is the effect of valgus bracing in patients with medial compartment osteoarthritis
of the knee and can this be explained by changes in gait?
2. What are the differences in accuracy and in postoperative stability between closed
and open wedge high tibial osteotomy?
3. What are the differences between closed and open wedge high tibial osteotomy in
patients with respect to correction accuracy, collateral laxity and clinical outcome?
4. Does the incorporation and remodelling of ß-TCP bone substitute in open wedge
tibial osteotomy in patients occur similarly to that in animals?
5. What are the effects of high tibial osteotomy on patellar tracking?
6. Can lowering of the patella which accompanies open wedge high tibial
osteotomy be prevented?
Reference List
1. Dabov G, Perez EA. Chapter 25: Miscellaneous Nontraumatic Disorders. In:Campbell’s Operative
Orthopaedics . Mosby , 2003;916.
2. Hanypsiak BT, Shaffer BS. Nonoperative treatment of unicompartmental arthritis of the knee.
Orthop Clin North Am 2005;36:401-411.
3. Amendola A, Panarella L. High tibial osteotomy for the treatment of unicompartmental arthritis of
the knee. Orthop Clin North Am 2005;36:497-504.
4. Coventry MB. Upper tibial osteotomy. Clin Orthop Relat Res 1984;46-52.
5. Billings A, Scott DF, Camargo MP, Hofmann AA. High tibial osteotomy with a calibrated osteotomy
guide, rigid internal fixation, and early motion - Long-term follow-up.
J Bone Joint Surg Am 2000;82A:70-79.
6. Coventry MB, Ilstrup DM, Wallrichs SL. Proximal tibial osteotomy. A critical long-term study of
eighty-seven cases. J Bone Joint Surg Am 1993;75:196-201.
7. Insall JN, Joseph DM, Msika C. High tibial osteotomy for varus gonarthrosis. A long-term follow-up
study. J Bone Joint Surg Am 1984;66:1040-1048.
8. Ivarsson I, Myrnerts R, Gillquist J. High tibial osteotomy for medial osteoarthritis of the knee.
A 5 to 7 and 11 year follow-up. J Bone Joint Surg Br 1990;72:238-244.
9. Naudie D, Bourne RB, Rorabeck CH, Bourne TJ. The Install Award. Survivorship of the high tibial
valgus osteotomy. A 10- to -22-year followup study. Clin Orthop 1999;18-27.
10. Rinonapoli E, Mancini GB, Corvaglia A, Musiello S. Tibial osteotomy for varus gonarthrosis.
A 10- to 21-year followup study. Clin Orthop 1998;185-193.
11. Yasuda K, Majima T, Tsuchida T, Kaneda K. A ten- to 15-year follow-up observation of high tibial
osteotomy in medial compartment osteoarthrosis. Clin Orthop 1992;186-195.
12. Insall J, Shoji H, Mayer V. High tibial osteotomy. A five-year evaluation.
J Bone Joint Surg Am 1974;56:1397-1405.
13. Dugdale TW, Noyes FR, Styer D. Preoperative planning for high tibial osteotomy. The effect of lateral
tibiofemoral separation and tibiofemoral length. Clin Orthop 1992;248-264.
14. Hernigou P, Medevielle D, Debeyre J, Goutallier D. Proximal tibial osteotomy for osteoarthritis with
varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354.
15. Magyar G, Ahl TL, Vibe P, Toksvig-Larsen S, Lindstrand A. Open-wedge osteotomy by hemicallotasis
or the closed-wedge technique for osteoarthritis of the knee. A randomised study of 50 operations.
J Bone Joint Surg Br 1999;81:444-448.
16. Wright JM, Heavrin B, Begg M, Sakyrd G, Sterett W. Observations on patellar height following
opening wedge proximal tibial osteotomy. Am J Knee Surg 2001;14:163-173.

16
Chapter 1
17
General introduction, background and aims of the thesis
17. Tigani D, Ferrari D, Trentani P, Barbanti-Brodano G, Trentani F. Patellar height after high tibial
osteotomy. Int Orthop 2001;24:331-334.
18. Davidson PL, Sanderson DJ, Loomer RL. Kinematics of valgus bracing for medial gonarthrosis:
technical report. Clin Biomech (Bristol , Avon ) 1998;13:414-419.
19. Draper ER, Cable JM, Sanchez-Ballester J, Hunt N, Robinson JR, Strachan RK. Improvement in
function after valgus bracing of the knee. An analysis of gait symmetry.
J Bone Joint Surg Br 2000;82:1001-1005.
20. Hewett TE, Noyes FR, Barber-Westin SD, Heckmann TP. Decrease in knee joint pain and increase in
function in patients with medial compartment arthrosis: a prospective analysis of valgus bracing.
Orthopedics 1998;21:131-138.
21. Horlick SG, Loomer BA. Valgus knee bracing for medial gonarthrosis.
Clin J Sport Med 1993;251-255.
22. Kirkley A, Webster-Bogaert S, Litchfield R et al. The effect of bracing on varus gonarthrosis.
J Bone Joint Surg Am 1999;81:539-548.
23. Komistek RD, Dennis DA, Northcut EJ, Wood A, Parker AW, Traina SM. An in vivo analysis of the
effectiveness of the osteoarthritic knee brace during heel-strike of gait. J Arthroplasty 1999;14:738-742.
24. Lindenfeld TN, Hewett TE, Andriacchi TP. Joint loading with valgus bracing in patients with varus
gonarthrosis. Clin Orthop 1997;290-297.
25. Matsuno H, Kadowaki KM, Tsuji H. Generation II knee bracing for severe medial compartment
osteoarthritis of the knee. Arch Phys Med Rehabil 1997;78:745-749.
26. Otis JC, Backus SI, Campbell DA et al. Valgus bracing for knee osteoarthritis: A biomechanical
and clinical outcome study. Gait Posture 2000;11:116-117.
27. Pollo FE, Otis JC, Wickiewicz TL, Sherryl I, Backu, Backus SI. Biomechanical analysis of valgus
bracing for the osteoarthritic knee. Arthritis Rheum 1995;241.
28. Pollo FE, Otis JC, Backus SI, Warren RF, Wickiewicz TL. Reduction of medial compartment loads
with valgus bracing of the osteoarthritic knee. Am J Sports Med 2002;30:414-421.
29. Self BP, Greenwald RM, Pflaster DS. A biomechanical analysis of a medial unloading brace for
osteoarthritis in the knee. Arthritis Care Res 2000;13:191-197.
30. van Heerwaarden RJ, Gaasbeek RD, Plitz W. A new valgus brace for medial knee osteoarthritis.
A short term patient evaluation study with the Softec OA brace.
Med-Orthopädische Technik 2005;57-65.
31. Brouwer RW, Bierma-Zeinstra SM, van Koeveringe AJ, Verhaar JA. Patellar height and the inclination
of the tibial plateau after high tibial osteotomy. The open versus the closed-wedge technique.
J Bone Joint Surg Br 2005;87:1227-1232.
32. Hoell S, Suttmoeller J, Stoll V, Fuchs S, Gosheger G. The high tibial osteotomy, open versus closed
wedge, a comparison of methods in 108 patients. Arch Orthop Trauma Surg 2005;:1-6.:1-6.
33. Magyar G, Toksvig LS, Lindstrand A. Changes in osseous correction after proximal tibial osteotomy -
Radiostereometry of closed- and open-wedge osteotomy in 33 patients.
Acta Orthop Scand 1999;70:473-477.
34. Closkey RF, Windsor RE. Alterations in the patella after a high tibial or distal femoral osteotomy.
Clin Orthop 2001;51-56.
35. Dejour H, Walch G, Nove-Josserand L, Guier C. Factors of patellar instability: an anatomic
radiographic study. Knee Surg Sports Traumatol Arthrosc 1994;2:19-26.
36. Figgie HE, III, Goldberg VM, Heiple KG, Moller HS, III, Gordon NH. The influence of tibial-
patellofemoral location on function of the knee in patients with the posterior stabilized condylar knee
prosthesis. J Bone Joint Surg Am 1986;68:1035-1040.
37. Goutallier D, Delepine G, Debeyre J. [The patello-femoral joint in osteoarthritis of the knee with genu
varum (author’s transl)]. Rev Chir Orthop Reparatrice Appar Mot 1979;65:25-31.
38. Heegaard J, Leyvraz PF, van Kampen A, Rakotomanana L, Rubin PJ, Blankevoort L. Influence of soft
structures on patellar three-dimensional tracking. Clin Orthop Relat Res 1994;235-243.
39. Hill NA, Fellows RA, MacIntyre NJ, Harrison MM, Ellis RE, Wilson DR. The effect of high tibial
osteotomy on three-dimensinal tibiofemoral and patellofemoral kinematics: an in vivi study using
magnetic resonance imaging. Proc 51st ORS Conference 2005;0481.
40. Kaper BP, Bourne RB, Rorabeck CH, Macdonald SJ. Patellar infera after high tibial osteotomy.
J Arthroplasty 2001;16:168-173.
41. Meyer SA, Brown TD, Pedersen DR, Albright JP. Retropatellar contact stress in simulated patella
infera. Am J Knee Surg 1997;10:129-138.
42. Scuderi GR, Windsor RE, Insall JN. Observations on patellar height after proximal tibial osteotomy.
J Bone Joint Surg Am 1989;71:245-248.
43. Singerman R, Davy DT, Goldberg VM. Effects of patella alta and patella infera on patellofemoral
contact forces. J Biomech 1994;27:1059-1065.
44. van Kampen A, Huiskes R. The three-dimensional tracking pattern of the human patella.
J Orthop Res 1990;8:372-382.
45. Weidenhielm L, Wykman A, Lundberg A, Brostrom LA. Knee motion after tibial osteotomy for
arthrosis. Kinematic analysis of 7 patients. Acta Orthop Scand 1993;64:317-319.
46. Windsor RE, Insall JN, Vince KG. Technical considerations of total knee arthroplasty after proximal
tibial osteotomy. J Bone Joint Surg Am 1988;70:547-555.

18
chapter 2Valgus bracing in patients with medial compartment
osteoarthritis of the knee
A gait-analysis study of a new brace
Robert D. A. Gaasbeek, Brenda E. Groen, Brieke Hampsink,
Ronald J. van Heerwaarden, Jacques Duysens
Gait Posture 2007 June 26(1):3-10

20
Chapter 2
21
Valgus bracing in patients with medial compartment osteoarthritis of the knee
Abstract
A new valgus brace was evaluated in fifteen patients with medial osteoarthritis of the
knee and a varus leg axis. Significant improvement of pain and function were found
after six weeks of brace treatment. Gait analysis showed that the brace had a tendency
of lowering the peak varus moment about the knee. This effect was more profound at
higher initial varus deformity angles of the knee. Furthermore, a small decrease of knee
extension at the end of the swing phase and an increase of walking velocity were
related to brace wearing. The working mechanisms of valgus brace treatment found with
the gait analysis in this study may be of clinical importance for future developments in
brace treatment.
Introduction
Osteoarthritis of the knee is most often located in the medial compartment 1.
A progressive varus leg axis develops as a result of the cartilage loss associated with
this unicompartmental osteoarthritis. The varus deformity causes an overload of the
medial compartment with increasing symptoms during weight bearing. Decrease of
the varus leg alignment unloads the arthritic medial compartment which results in a
decrease of symptoms. Based on this principle, functional braces have been designed
to produce a valgisation force about the knee. The general working mechanism is a
distraction of the medial compartment and a transfer of the weight bearing axis
towards the lateral compartment of the knee. In several patient studies symptoms relief
and functional improvement were found after short term and longer term treatment with
valgus knee braces 1-6.
Gait analysis studies have been used to evaluate the working mechanisms that cause
improvements with brace wear. The results range from no effect to a significant
improvement in gait symmetry and a reduction in external varus moments 2, 5, 7-10.
A study using fluoroscopy during treadmill gait demonstrated articular surface
separation at heel strike in subjects wearing valgus knee braces 11. However, it remains
unclear how these changes relate to functional gait improvements. Furthermore, most
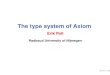
Figure 1
The SofTec OA valgus
brace. On the left:
airchamber inflation with
a bulb pump to adjust
brace valgisation force
and on the right:
schematic 3-point
mechanism producing
valgus.

22
Chapter 2
23
Valgus bracing in patients with medial compartment osteoarthritis of the knee
valgus braces offer little flexibility and there is a need for more adjustable braces.
A new valgus brace, the SofTec OA brace (Bauerfeind GmbH), has been constructed
with only a lateral hinge including an airchamber that enables adjustment of the valgus
force by the patient (Fig. 1). In the past few years, the authors used this brace in
clinical practice in the nonoperative treatment of patients with medial compartment
osteoarthritis of the knee with satisfactory results 12. No research on the effects of this
brace on pain, function scores and gait characteristics has been published. Therefore,
the present study was conducted to assess the effects of the use of this new brace
in patients with medial compartment osteoarthritis of the knee with respect to pain,
function and several gait parameters.
Materials and methods
Subjects
Fifteen consecutive patients, (12 male and 3 female) with a mean age of 52 (± 11)
years were included in the study. Inclusion criteria were an age between 18 and 70
years, unilateral medial compartment osteoarthrosis (OA) and pain localized primarily
to the medial compartment of the knee. Varus deformity of the knee was confirmed on
standing long leg X-rays (range 2 to 11° with a mean of 5.1°). Standard knee X-rays
confirmed the presence of medial compartment OA with absence of lateral and
patellofemoral compartment OA of the knee in all patients. Exclusion criteria were
health problems prohibiting full weight bearing gait, pre-existing skin problems, the
inability to apply a brace because of physical limitations and previous operative
treatment for the medial compartment OA. Informed consent was obtained. After the
subjects were fitted with the valgus brace, they were instructed to inflate the air
chamber with the bulb pump to a level at which the arthritic symptoms would subside
and asked to wear the brace for at least 6 weeks.
Data collection
Subjects were tested before fitting and wearing the brace (T0) and after wearing
the brace continuously for 6 weeks (T1). Symptoms of osteoarthritis were assessed
by the Western Ontario and McMaster Universities (WOMAC) osteoarthritis index 13.
Pain intensity, during walking was scored with a Visual Analog Scale (VAS).
Gait analysis was performed on T0 without wearing the brace and on T1 without and
with wearing the brace.
To determine the external knee moments in the frontal plane, force data and 3D
kinematic data were collected simultaneously. Forces were measured at 2400 Hz by a
force plate (Kistler) embedded in the floor. The 3D positions of reflective markers were
recorded by a six-camera motion analysis system (Primas) at 100 Hz. For the walking
trials 18 markers were attached to the left and right leg. Four frames consisting of three
markers were tied to the femur and tibia of both legs. The remaining markers were
placed on the lateral malleolus, the dorsal aspect of the calcaneus, and the lateral
aspect of the fifth metatarsal head of both feet.
Data collection started with a reference trial in standing to define the joint centres,
therefore six extra markers were used : on the greater trochanter, the lateral femoral
epicondyle (or the hinge of the brace during the brace conditions) and the medial
aspect of the first metatarsal head of both feet. Then, the extra markers were removed.
During the walking trials the subjects walked at their preferred velocity. Five trials were
collected from both feet for each of the testing conditions.
To calculate the external moment in the frontal plane, inverse dynamics were applied
on a 2D-linked segment model. The centre of the ankle joint was defined medial to the
marker on the lateral malleolus at half the ankle width. The centre of the knee joint was
defined medial to the marker on the lateral femoral epicondyle at half the knee width
The ankle and knee joint centres were determined relative to the frames on the femur
and tibia respectively. For the walking trials the positions of the joint centres were
calculated based on the position of the marker frames. The moment was calculated
with use of the mass and inertia characteristics of the foot and lower leg and force
data 14. Prior to calculations the position data were low-pass filtered by a second order
Butterworth filter with a cut-off frequency of 6Hz and the force data were resampled to
100Hz. After normalization to the stance phase duration (=100%) the peak varus
moment was derived (maximum external moment about the knee in the frontal plane)
and averaged for both the left and right foot. All moments were normalized by the
product of body weight multiplied by height and were expressed as a percentage of
that product (%BW.HT). For the calculations, programs written in Matlab (The Math
Works Inc.) were used. Finally, the preferred walking velocity was determined, using

24
Chapter 2
25
Valgus bracing in patients with medial compartment osteoarthritis of the knee
the reflective marker on the calcaneus (average of five trials).
A pressure platform (RS-scan, 0.5m x 0.4m x 0.008m) was used to determine the
foot progression angle (FPA) during walking conform to our previous studies 15.
For the definition of FPA, see figure 2. For each subject the mean FPA of each
condition of the left and right foot was determined.
Treadmill walking, to determine ankle and knee kinematics, was introduced to have the
benefit of a more consistent gait pattern at a fixed speed. During treadmill walking the
joint angles of the knee and ankle were determined with twin axis goniometers as
used by others 16, 17. To indicate the beginning (heel contact) of the each step cycle,
reflective markers were placed on the heel of both feet. The experiment started with a
period of walking to familiarize the patients to treadmill walking. A trial during standing
with the knee and ankle joints in neutral positions provided reference data. Subjects
walked at two speeds, 3 and 4 km/h for each testing condition 18. The speed of 3 km/h
corresponds with the self selected walking velocity of patients with OA and the speed
of 4 km/h with the fast velocity that was feasible for all patients 19, 20. The subjects
performed three trials of each condition at each velocity. The average of 15 sequential
cycles was calculated and normalized for gait cycle.
The knee and ankle joint angles for the walking trials were calculated with use of the
average angles of the reference data. The following variables were derived: range of
motion (ROM) in the saggital plane, maximum flexion during (early) stance, maximum
extension during (mid) stance, maximum flexion during (mid) swing, maximum
extension at the end of the swing phase. Average step frequency (steps/min) and step
length were calculated, using the heel marker position.
Statistical analysis
Paired t-tests were used to determine the effect of the brace on the VAS and WOMAC
scores and to determine differences between the affected and unaffected leg.
Multivariate analysis of variance (MANOVA) for repeated measurements with three
brace conditions (T0, T1without brace and T1with brace) were used to determine if the other
variables were affected by condition (main effect). For treadmill walking the speed
was added as between factor variable, to determine the (interaction) effects of speed
on the kinematic and spatiotemporal variables. For peak varus moment the varus
deformity was used as a covariate. Post hoc, paired t-tests were performed to
determine between which conditions the differences existed. Level of significance
was set at p=0.05 for all tests.
Results
The brace was worn 7 days a week by all patients. Following the 6 weeks of brace
wear, statistically significant improvements were found for the WOMAC and VAS-scores
(Table 1).
The effects on the moments at the knee were evaluated with inverse dynamics.
The mean group knee moment as a function of the stance phase for both the affected
and unaffected leg for all conditions are shown in figure 3. Typically the peak varus
moment was larger in the affected leg as compared with the non-affected one and the
Figure 2
Definition of the foot
progression angle (FPA)
using a plantar pressure
print. The FPA was defined
as the angle between the
direction of progression and
the foot axis defined as the
axis through the base of the
heel and MTP2. The foot
axis through the heel and
MTP2 was set manually on
the maximum pressure
image of the foot, while the
direction of progression was
in forward direction.

26
Chapter 2
27
Valgus bracing in patients with medial compartment osteoarthritis of the knee
moment was reduced after wearing the brace (Fig. 3). Figure 4a shows the group
peak varus moment of the affected and unaffected leg for all conditions. For the whole
group, the peak varus moment was significantly higher in the affected than in the
unaffected leg on T0 (p=0.021). The varus moment was also influenced by the various
brace conditions. For the affected leg, the MANOVA indicated a significant main effect
of brace condition (e.g. T0, T1without brace and T1with brace) on peak varus moment
(p=0.046). Post hoc testing showed that the peak varus moment was significantly
higher during the T1without brace condition compared to the T0 condition (p=0.019).
No significant difference was found between the braced and unbraced condition
on T1 (p=0.125). In addition, a significant interaction effect between the peak varus
moment and the varus deformity of the knee (covariate) (p=0.05) was indicated.
The interaction was significant between brace condition T1without brace and T1with brace
(p=0.010). The larger the varus deformity of the knee, the more reduction in the peak
varus moment was achieved by the brace during walking.
As shown in figure 4b, no significant differences in FPA were observed but step length
was affected.
With brace (T1with brace), the steps were shorter than without brace (T1without brace)(p=0.017
and p<0.001) (Fig. 4c). The MANOVA indicated a significant main effect of brace
condition for both affected (p=0.017) and unaffected leg (p<0.001).
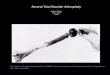
Figure 3
Group mean of the knee varus moment as a function of the stand phase for both the
unaffected and affected leg for all conditions. The moments are normalized to body weight
(BW) and height (HT) and expressed as a percentage. Note that the maximum varus moment
in this figure differs from the peak varus moments shown in figure 4a, because in the present
plot all values were averaged while in figure 4a only the peak values were averaged (due to
peak varus occurred at different times in the cycle for the various subjects).
Affected leg
T0: without braceT1: without braceT1: with brace
Valgus
Knee
mom
ent (
%BW
.HT)
% Standphase % Standphase
Knee
mom
ent (
%BW
.HT)
Valgus
VarusVarus
T0: without braceT1: without braceT1: with brace
Unaffected leg
*a
c *
** ***
*
d
b
T0: without braceT1: without braceT1: with brace
Peak
var
us m
omen
t kne
e (%
BW.H
T)
Foot
pro
gres
sion
ang
le (d
egre
es)
Step
leng
ht (c
m)
Knee
rang
e of
mot
ion
(deg
rees
)
Affected leg Unaffected leg Affected leg Unaffected leg
Affected leg Unaffected leg Affected leg Unaffected leg
Figure 4
Diagrams showing the group mean ± standard deviation of the a. Peak knee varus moment
(normalized to body weight (BW) and height (HT)), b. Foot progression angle (degrees),
c. Step length (cm) and d. Knee range of motion in the saggital plane (degrees) for both
the unaffected and affected leg at all conditions. Significant differences are indicated with
an asterisk (*).

28
Chapter 2
29
Valgus bracing in patients with medial compartment osteoarthritis of the knee
Post hoc testing showed that the patients walked with longer steps during T1without brace
than on T0 (p=0.007 and p=0.005 for the affected an unaffected leg, respectively).
The effects were independent of speed.
The shorter steps with the brace suggest that there was a limitation in ROM due to
the braces. This was confirmed by the analysis. For the affected knee ROM in the
saggital plane, the MANOVA indicated a main effect of brace condition (p=0.0045).
The ROM was significantly reduced in the braced condition (T1with brace) compared to
the unbraced condition (T1without brace) (p=0.02) independent of walking velocity
(Fig. 4d). The reduction in ROM during walking with the brace was mainly expressed
as a reduction in knee extension at end swing and end stance, as is illustrated in Fig. 5.
The MANOVA’s for ankle and knee angles indicated a main effect of brace condition
for the maximal knee extension during the end of the swing phase of the affected leg
only (p<0.001). On T1, knee extension was significantly decreased by brace wear
(p<0.001) (Fig. 5).
The three brace conditions had an effect on preferred walking velocity as well. Indeed,
the MANOVA indicated that there was a significant main effect of brace condition
(e.g. T0, T1without brace and T1with brace) on preferred walking velocity (p=0.014).
Post hoc testing showed that the patients walked faster on the second testing day
(T1 vs. T0; p=0.026). On T1, there was no significant difference between conditions
without (T1without brace) and with brace (T1with brace) (p=0.063) (Fig. 6).
Discussion
The purpose of this study was to evaluate the SofTec OA valgus brace on patients
suffering from medial compartment OA of the knee with a clinical assessment and
a gait analysis. After six weeks of bracing, improvements in pain and function scores
were observed. Although little weight can be placed on these results because of the
small number of patients and because we did not use an alternative to the brace as
a control, these findings were consistent with results presented in previous studies
with this brace 12 and other braces 1, 4, 5, 13.
As expected, the peak varus moments about the knee during the stance phase of
walking were significantly higher in the affected leg as compared with the unaffected
leg on the first testing day (before brace treatment). The values found in the present
study were within the range of those reported in literature 2, 5, 10, 21. The values for the
unaffected leg were comparable with the values for controls as reported by Goh et al.
Figure 5
The group mean knee angle as a function of the gait cycle for both the unaffected and affected
leg for all conditions during treadmill walking of 3 km/h. Note that the ROM in this figure differs
from the ROM shown in figure 4d, because in the present plot all values were averaged while in
figure 4d only the peak values were averaged (related to the maximum flexion and extension
occurring at different times in the cycle for the various subjects).
Affected leg Unaffected leg
T0: without braceT1: without braceT1: with brace
T0: without braceT1: without braceT1: with brace
Flexion
Knee
flex
ion/
exte
nsio
n (d
egre
es)
% gait cycle % gait cycle
Knee
flex
ion/
exte
nsio
n (d
egre
es)
Extension
Flexion
Extension
T0: without braceT1: without braceT1: with brace
Pref
erre
d w
alki
ng v
eloc
ity (m
/s)
Figure 6
Preferred walking velocity
(group mean ± standard
deviation) (m/s) during all
conditions. Significant
differences are indicated
with an asterisk (*).

30
Chapter 2
31
Valgus bracing in patients with medial compartment osteoarthritis of the knee
and Lindenfeld et al. 5, 22 For the affected leg, the peak varus moment about the knee
was lower during the braced condition as compared to the unbraced condition on T1
although the differences did not reach significance. The variability and the small
number of patients could explain the lack of significance. In previous brace studies a
significant reduction in peak varus moment was not found either 1, 2, 5. Pollo et al. did
not find a decrease in peak varus moment, although they observed a reduction in the
load of the medial compartment of the knee (as estimated by an analytical model) in
the brace condition 1. However, others found significant reductions in varus moments
about the knee during brace wear 5, 10. In the present study a significant interaction
effect was shown between the peak varus moment and varus deformity of the knee.
This means that patients with more varus deformity, showed more reduction of the
peak varus moment during the braced condition (p<0.05). This suggests the brace
is more effective at higher varus deformities. No other studies were found in which
the interaction effect was examined. Although reduction of the peak varus moment
was not consistently found in all patients the clinical assessment showed significant
improvement of pain and knee function in all patients. This might be due to the fact
that valgus braces do not actually change the varus alignment of the leg but might
prevent the increase in varus at mid-stance. The peak varus moments are found at
early and late stance. This raises the question whether peak varus moment analysis
is the most accurate way to study the presumed unloading effect of any brace.
The unloading of the medial compartment may be caused by other factors, especially
gait adaptations, as well.
Earlier studies observed a significant correlation between the toe angle and peak
varus moment, which suggests that the varus moment can be decreased by increa-
sing toe-out of the foot 19, 23-25. Patients with medial compartment OA could use this
compensatory mechanism to reduce the varus moment 23, 26. This was not observed in
the present group since the FPA was within normal limits 22 and showed no significant
difference between the affected and unaffected leg. Furthermore, no effect of the
brace on the FPA was observed, in agreement with others 2, 5. Hence, differences in
varus moment between the conditions found in the present study are not caused by
the rotation of the foot.
It has been speculated that these patients walk at slower velocities to reduce loading
in the medial compartment of the knee 21. The average preferred walking velocity of our
group of patients at the first testing day corresponded with values for velocity of
healthy adults and was higher than was expected on the basis of gait analysis of OA
patients 27-29. At the second testing day, after a 6 weeks period of brace wear, the
patients walked without brace with a significant faster preferred walking velocity.
This could be due to the improvement of function and reduction of pain after brace
treatment. The difference in velocity could explain the difference found in the peak
varus moment between the unbraced conditions at the first and second testing day.
However, walking with the brace did not change the walking velocity significantly on
the second testing day. Earlier studies also reported no difference between the
unbraced and braced condition after a period of brace treatment 1, 2, 5, 7. We concluded
that the tendency of peak varus moment reduction by brace wear was not due to a
reduction in walking velocity in this study.
Another adaptive mechanism that could be used to lower the adduction moment
during gait is shortening the stride or step 23. During treadmill walking on the second
testing day the patients had a significant increase of stride length as compared to the
first testing day in the unbraced situation (T1without brace). This could be due to pain
reduction. Surprisingly, the step and stride length returned to the values measured
before brace treatment in the braced condition (T1with brace). Earlier brace studies have
not found a significant difference in stride length between the unbraced and braced
conditions after a period of brace treatment 7, 9. An explanation for the reduction of
stride length after application of the brace could be a reduction of the range of motion
of the knee i.e. the brace could have altered the mobility of the knee by which the
stride and step length is affected.
The ROM of the knee in the saggital plane was similar to other studies 17, 20, 27, 30, 31.
The knee range of motion in the saggital plane was significantly reduced in the braced
condition. The knee angles at different events of the gait cycle were investigated.
The results showed that the brace prevented full extension at the end of the swing
phase. Possibly, the duration of the swing phase was decreased which could explain
the decreased step and stride length during treadmill walking with brace. These data
are consistent with the gait analysis of Davidson et al., who demonstrated that during
valgus brace wear the knee angle during the stance phase is altered 32. More specifically,
in the analysis performed full extension was prevented by the resisting valgus forces in
the coronal plane. In the present study, the kinematic parameters are obtained during

32
Chapter 2
33
Valgus bracing in patients with medial compartment osteoarthritis of the knee
treadmill walking and the peak varus moment during overground walking. Although
previous studies have indicated that the kinematics of the knee of treadmill and
overground walking are very similar 33, it is important to point out that cross-referencing
represents a minor limitation of the present study.
Whether the new hinge construction with inflatable airchamber that is applied in this
brace or a general effect of valgus producing hinged knee braces is responsible for
the changes in the gait cycle remains unclear as in the present study no comparisons
were made with other braces. In the clinical assessments no scores were found
indicating that the small decrease in range of motion was perceived by the patients.
Longer follow up of clinical assessment and gait analysis may reveal whether the
effects of brace treatment found in this study persist. The analysis of the working
mechanisms of brace treatment with gait analysis studies will enable objective evaluation
of the effects of brace treatment and may improve future brace design.
In conclusion, the SofTec OA brace significantly decreased pain and improved knee
function. The working mechanism of this new valgus brace may be explained by
reduction of the peak varus moment about the knee, this effect being more profound
at higher initial varus angles of the knee, an increased walking velocity and a small
decrease in knee ROM with prevention of full extension during gait.
Acknowledgments
The authors thank Ms Joan Evers, orthopaedic technician, for her assistance in brace
fitting and patient instruction as well as, Drs J. Hiemstra and I. Barck of Bauerfeind
Benelux and Bauerfeind GmbH for technical and administrative assistance. This study
was supported by POM, Nijmegen, The Netherlands and Bauerfeind GmbH.
Reference List
1. Pollo FE, Otis JC, Backus SI, Warren RF, Wickiewicz TL. Reduction of medial compartment
loads with valgus bracing of the osteoarthritic knee. Am J Sports Med 2002; 30: 414-421
2. Hewett TE, Noyes FR, Barber-Westin SD, Heckmann. TP Decrease in knee joint pain and increase
in function in patients with medial compartment arthrosis: a prospective analysis of valgus bracing.
Orthopedics 1998; 21: 131-138
3. Horlick SG, Loomer BA. Valgus knee bracing for medial gonarthrosis. Clin J Sport Med 1993;251-255
4. Kirkley A, Webster-Bogaert S, Litchfield R, Amendola A, MacDonald S, McCalden R, Fowler P.
The effect of bracing on varus gonarthrosis. J Bone Joint Surg Am 1999; 81: 539-548
5. Lindenfeld TN, Hewett TE, Andriacchi TP. Joint loading with valgus bracing in patients with varus
gonarthrosis. Clin Orthop 1997; 290-297
6. Matsuno H, Kadowaki KM, Tsuji H. Generation II knee bracing for severe medial compartment
osteoarthritis of the knee. Arch Phys Med Rehabil 1997; 78: 745-749
7. Otis JC, Backus SI, Campbell DA. Valgus bracing for knee osteoarthritis: A biomechanical and
clinical outcome study. Gait Posture 2000; 11: 116-117
8. Draper ER, Cable JM, Sanchez-Ballester J, Hunt N, Robinson JR, Strachan RK. Improvement in
function after valgus bracing of the knee. An analysis of gait symmetry.
J Bone Joint Surg Br 2000; 82: 1001-1005
9. Pollo FE, Otis JC, Wickiewicz TL, Sherryl I, Backu, Backus SI. Biomechanical analysis of valgus
bracing for the osteoarthritic knee. Arthritis Rheum 1995; 241
10. Self BP, Greenwald RM, Pflaster DS. A biomechanical analysis of a medial unloading brace
for osteoarthritis in the knee. Arthritis Care Res 2000; 13: 191-197
11. Komistek RD, Dennis DA, Northcut EJ, Wood A, Parker AW, Traina SM. An in vivo analysis of
the effectiveness of the osteoarthritic knee brace during heel-strike of gait.
J Arthroplasty 1999; 14: 738-742
12. Van Heerwaarden RJ, Gaasbeek RD, Plitz W. A new valgus brace for medial knee osteoarthritis.
A short term patient evaluation study with the Softec OA brace.
Med-Orthopädische Technik 2005; 57-65
13. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC:
a health status instrument for measuring clinically important patient relevant outcomes to
antirheumatic drug therapy in patients with osteoarthritis of the hip or knee.
J Rheumatol 1988; 15: 1833-1840
14. Winter DA, Patla AE, Frank JS, Walt SE. Biomechanical walking pattern changes in the fit and
healthy elderly. Phys Ther 1990; 70: 340-347

34
Chapter 2
35
Valgus bracing in patients with medial compartment osteoarthritis of the knee
15. Jaarsma RL, Ongkiehong BF, Gruneberg C, Verdonschot N, Duysens J, van Kampen A.
Compensation for rotational malalignment after intramedullary nailing for femoral shaft fractures.
An analysis by plantar pressure measurements during gait. Injury. 2004 Dec;35(12):1270-8.
16. Rowe PJ, Myles CM, Walker C, Nutton R. Knee joint kinematics in gait and other functional
activities measured using flexible electrogoniometry: how much knee motion is sufficient for normal
daily life? Gait Posture 2000; 12: 143-155
17. Myles CM, Rowe PJ, Walker CR, Nutton RW. Knee joint functional range of movement prior to
and following total knee arthroplasty measured using flexible electrogoniometry.
Gait Posture 2002; 16: 46-54
18. Kirtley C, Whittle MW, Jefferson RJ. Influence of walking speed on gait parameters.
J Biomed Eng 1985; 7: 282-288
19. Wada M, Imura S, Nagatani K, Baba H, Shimada S, Sasaki S. Relationship between gait and
clinical results after high tibial osteotomy. Clin Orthop 1998; 180-188
20. Gok H, Ergin S, Yavuzer G. Kinetic and kinematic characteristics of gait in patients with medial
knee arthrosis. Acta Orthop Scand 2002; 73: 647-652
21. Mundermann A, Dyrby CO, Hurwitz DE, Sharma L, Andriacchi TP. Potential strategies to reduce
medial compartment loading in patients with knee osteoarthritis of varying severity: reduced wal-
king speed. Arthritis Rheum 2004; 50: 1172-1178
22. Goh JC, Bose K, Khoo BC. Gait analysis study on patients with varus osteoarthrosis of the knee.
Clin Orthop 1993; 223-231
23. Wang JW, Kuo KN, Andriacchi TP, Galante JO. The influence of walking mechanics and time on
the results of proximal tibial osteotomy. J Bone Joint Surg Am 1990; 72: 905-909
24. Hurwitz DE, Ryals AB, Case JP, Block JA, Andriacchi TP. The knee adduction moment during
gait in subjects with knee osteoarthritis is more closely correlated with static alignment than
radiographic disease severity, toe out angle and pain. J Orthop Res 2002; 20: 101-107
25. Andrews M, Noyes FR, Hewett TE, Andriacchi TP. Lower limb alignment and foot angle are related
to stance phase knee adduction in normal subjects: a critical analysis of the reliability of gait
analysis data. J Orthop Res 1996; 14: 289-295
26. Torgerson WR, Jr., Kettelkamp DB, Igou RA, Jr., Leach RE. Tibial osteotomy for the treatment
of degenerative arthritis of the knee. Clin Orthop 1974; 101: 46-52
27. Al Zahrani KS, Bakheit AM. A study of the gait characteristics of patients with chronic
osteoarthritis of the knee. Disabil Rehabil 2002; 24: 275-280
28. Kaufman KR, Hughes C, Morrey BF, Morrey M, An KN. Gait characteristics of patients with
knee osteoarthritis. J Biomech 2001; 34: 907-915
29. Larsson LE, Odenrick P, Sandlund B, Weitz P, Oberg PA. The phases of the stride and their
interaction in human gait. Scand J Rehabil Med 1980; 12: 107-112
30. Baliunas AJ, Hurwitz DE, Ryals AB, Karrar A, Case JP, Block JA, Andriacchi TP. Increased
knee joint loads during walking are present in subjects with knee osteoarthritis.
Osteoarthritis Cartilage 2002; 10: 573-579
31. Messier SP, Loeser RF, Hoover JL, Semble EL, Wise CM. Osteoarthritis of the knee: effects
on gait, strength, and flexibility. Arch Phys Med Rehabil 1992; 73: 29-36
32. Davidson PL, Sanderson DJ, Loomer RL. Kinematics of valgus bracing for medial gonarthrosis:
technical report. Clin Biomech (Bristol , Avon ) 1998; 13: 414-419
33. Alton F, Baldey L, Caplan S, Morrissey MC. A kinematic comparison of overground and treadmill
walking. Clin Biomec 1998; 13: 434-440

36
chapter 3Accuracy and initial stability of open and closed
wedge high tibial osteotomy; A cadaveric RSA study
Robert D. A. Gaasbeek, Roy T. C. Welsing, Nico Verdonschot,
Willard J. Rijnberg, Corné J. M. van Loon, Albert van Kampen
Knee Surg Sports Traumatol Arthrosc. 2005 Nov;13(8):689-94

38
Chapter 3
39
Accuracy and initial stability of open and closed wedge high tibial osteotomy; a cadaveric RSA study
Abstract
We analyzed the difference in angle correction accuracy and initial stability between
open-wedge (OWO) and closed-wedge tibial valgus osteotomy (CWO). Five fresh
frozen pairs of human cadaver lower limbs were used, their bone mineral density (BMD)
was measured with DEXA and a planned 7 degree valgus osteotomy was performed,
either with an open (right knees) or closed (left knees) technique.
All osteotomies were fixed with a rigid locked plate. In OWO tricalcium phosphate
(TCP) wedges were inserted. The knees were subjected to an increasing cyclic axial
load until failure, while measuring the relative displacement of the bony
segments with roentgen stereophotogrammetric analysis. The mean postoperative
valgus correction angle was 9.5º ± 2.8º for CWO (over-correction of 2.5º) and 6.2º
± 2.0º for OWO (under-correction of 0.8º) (p = 0.08). The data of displacement under
load-bearing showed no significant differences in rotations and translations in any
direction. No significant correlation between BMD and the moment of failure was found
(p=0.27).
This study has shown that both methods gave an acceptable correction with high
variation of postoperative correction angles. There was a tendency of overcorrection
in the CWO group but no significant difference was found. There was no difference in
initial stability between CWO and OWO with a rigid locked plate fixation.
Introduction
Medial osteoarthritis of the knee is often associated with a varus deformity.
Valgus high tibial osteotomy (HTO) is the treatment for varus deformity, especially for
the younger active patient 4, 5. The goal of HTO is reduce the load on the medial
compartment by shifting the mechanical axis towards the lateral compartment with a
slight over-correction 17, 18. For good long-term clinical results the recommended post-
operative femorotibial valgus angle has to be in the region of 8 to 16 degrees 5, 7, 9, 12.
Excessive over-correction leads to poor results 10. Under-correction and loss of
correction results in a poor clinical outcome 5, 7. Hence, it is of critical importance that
the angle correction is as accurate as possible.
In some cases deterioration of the angle correction occurs after HTO because of lack
of fixation and stability 14. Therefore, adequate stability is important to maintain the
angle correction for a longer period of time. Closed-wedge osteotomy (CWO) has
been the treatment of choice for many years 5, 13, 16, 17. However, open-wedge osteotomy
(OWO) is frequently used today. OWO is a less demanding surgical procedure, without
having to perform a fibula osteotomy. It gained popularity because of the shorter
rehabilitation and sick leave periods, reduced chance of nerve and vascular damage
and the availability of stable implants 6, 15, 16.
However, at present it is unclear which of the two methods (OWO or CWO) is more
accurate in terms of angle correction and which of the two methods leads to the
strongest reconstruction.
Therefore we analyzed the accuracy and initial postoperative stability of HTO on five
pairs of human cadaver lower limbs, operated with both OWO and CWO, with roentgen
stereophotogrammetric analysis (RSA) under dynamic loading conditions.
Materials and methods
This study was conducted on 5 pairs of fresh frozen human cadaver lower limbs.
AP and lateral radiographs of the knee joint were made to exclude major degenerative

40
Chapter 3
41
Accuracy and initial stability of open and closed wedge high tibial osteotomy; a cadaveric RSA study
changes. Before preparation or testing a Dual Energy X-ray Absorptiometry scan
(DEXA) was made to measure the bone mineral density (BMD) in five different regions
of interest of the proximal tibia. All soft tissues were left in place. The femur was cut
20 cm above the knee joint and the tibia 20 cm under the knee joint and cemented
in metal sockets.
Operative technique
One surgeon performed all operations under fluoroscopic guidance. The aimed angle
of correction in all knees was 7º.
CWO: (five left knees). A standard anterolateral approach was used. An osteotomy and
2 cm resection was performed in the middle third part of the fibula. Two centimeters
below and parallel to the joint line a Kirschner wire was inserted to aim the osteotomy.
First, the proximal cut was performed and the medial cortex was preserved. Using an
aiming device the distal cut was made and the bone wedge was removed. The aiming
device we used consists of a blade which is put in the first saw cut. The second cut is
performed through a cleft in the device with a fixed angle to the blade. The defect was
closed and the osteotomy was fixed with 4 locked screws and a L-plate (Numélock 2
system, Numédic, Cholet, France).
OWO: (five right knees). A medial approach was performed, shifting the pes anserinus
and the superficial medial collateral ligament dorsally. A Kirschner wire was inserted
parallel to the joint space. Using a guide instrument a second wire was inserted just
proximal of the tuberositas in lateral cranial direction in order to obtain an equal
osteotomy angle in all knees. Along this wire the osteotomy was performed. The lateral
cortex was left intact. The gap was opened and a resorbable tricalcium phosphate
(TCP) wedge (Otis, Lourdes, France) of 7 mm (6.6º) was inserted. No fibular osteotomy
was performed. Internal fixation was performed using the Numélock 2 system,
a T-plate with 4 locked screws.
Load bearing measurement
Standardized conditions of cyclic axial load bearing were achieved by placing the
knees subsequently in a material testing system (MTS) loading machine (MTS Systems
Corporation, Minneapolis, USA). The femur was attached proximally in a position of
free movement and the tibia was fixed distally (Figure 1). A constant load of 500 N was
applied to the quadriceps tendon. A dynamic load was applied to the knees in a 1 Hz
cyclic zero-to maximal loading pattern for 10 minutes and increased in steps of 250 N
until failure occurred.
RSA
RSA was performed according to the standard procedure 2, 11. The accuracy in our
laboratory in determining the three-dimensional rotation is 0.1 degrees and for
translation about 0.05 mm. Ten tantalum markers were placed: four markers proximal
to the osteotomy in the tibial plateau, and six on the distal tibia. The bones proximal
and distal to the osteotomy were considered to represent two rigid bodies. To obtain
the most accurate data of translation we added an additional marker in the plane
of osteotomy and considered this an origin of the rigid body. The positions of the
tibial markers were reoriented to their initial position and the rotation and translation
of the markers in the tibial plateau was calculated before surgery and during loading.
Before surgery and after every load bearing step RSA recordings were obtained.
In the coordinate system we determined the postoperative tibial wedge angle (rotation
around the Z-axis), the internal and external rotation of the tibia (rotation around the
Y-axis) and the retro- and anteflexion of the tibial plateau (rotation around the X-axis).
Figure 1
Setting of the load bearing
experiment in the MTS
machine.

42
Chapter 3
43
Accuracy and initial stability of open and closed wedge high tibial osteotomy; a cadaveric RSA study
Statistics
The linear correlation between displacement of the bony segments and load bearing was
analyzed using linear regression analysis (mean and 95% CI), followed by the paired
t-test to assess whether failure loads were different. Pearson’s correlation coefficient
was used to correlate BMD and moment of failure. Postoperative correction angles were
analyzed using the non-parametric Mann-Whitney U-test. Significance was set at p<0.05
Results
The bone mineral density (BMD) in all knees showed no significant differences
(p = 0.42) between pairs. The BMD in all knees, except one, was higher in the lateral
section than in the medial section of the tibia). AP and lateral radiographs showed no
major degenerative changes and no differences between pairs.
Postoperative correction angles
The planned angle of correction was 7º of valgus. The mean postoperative tibial
wedge angle was 9.5º ± 2.8º for CWO and 6.2º ± 2.0º for OWO. Hence, there was
a tendency that the mean correction angle was smaller with the OWO as compared to
the CWO. This difference was not significant (p = 0.08). There was a high variation
in both groups. The range of tibial wedge angles for CWO was 5.1º-12.1º and for OWO
3.7º-9.2º (Figure 2). Both CWO and OWO showed postoperative retroflexion of the
tibial plateau which means an increase in posterior slope (4 of 5 knees with CWO and
3 of 5 with OWO). Furthermore there was a postoperative external rotation of the
distal tibia (3 of 5 knees with CWO and 4 of 5 with OWO). The mean retroflexion of
the tibial plateau was not significantly different (p = 0.48): -0.1º ± 4.8º for CWO
and -3.5º ± 5.5º for OWO. The mean external rotation of the tibia was 3.7º ± 4.9º
for CWO and 2.6º ± 3.2º for OWO (p = 0.65).
Stability of the reconstruction during load bearing
From the RSA data the displacement of the bony segments was calculated. The rotations
and translations of all knees were plotted in diagrams and tables (Figure 3). The data
of the measurement just before failure of the knee were not included in the calculation
of the regression analyses. Increasing rotation and translation were seen with increasing
load bearing. The means of linear regression analysis found in CWO were compared
with those found in OWO. No differences were found in internal and external rotations
of the tibia (rotation Y-axis), tibial wedge angles (rotation Z-axis), anterior-posterior
translations; medial-lateral translations and superior-inferior translations (Table 1).
Moment of failure and bone mineral density
Seven knees failed in valgus and three in varus. The moments of failure of the
reconstruction, e.g. the maximum load the knees could bear, are shown in table 2.
The difference between the means of the maximum load bearing of the CWO- and
the OWO-knees was not significant (1750 ± 586 N and 2000 ± 637 N, respectively)
(p = 0.49). We found no significant correlation between the BMD and the moment
of failure (p=0.27).
Left / CWO
Right / CWO
Angle(degrees)
Knee
Figure 2
Postoperative tibial wedge
angles in open and closed
wedge osteotomies.
Translation alongY-axis (mm)
Load bearing (N)
Figure 3
Diagram showing
translations and moment
of failure along the Y-axis
during load bearing of
all ten knees.

44
Chapter 3
45
Accuracy and initial stability of open and closed wedge high tibial osteotomy; a cadaveric RSA study
Discussion
The precision of the predicted postoperative angle of correction is an important factor
in the long-term clinical results. To avoid under-correction or extreme over-correction,
the achieved tibial wedge angle must approach the planned correction angle as much
as possible. Because we used human cadaver knees it was not possible to trace the
mechanical axis of the limb on whole leg X-ray’s. In contrast to the usual clinical
setting we had to perform osteotomies in knees without varus deformity. Therefore, we
could not determine the desired angle of over-correction and we set our goal at a 7º
tibial wedge angle. With OWO we placed a 7 mm/ 6.6º tricalcium phosphate wedge in
all right sided knees. The angle of required correction is determined by the height of
the medial opening and the length of the osteotomy 8. (Figure 4). Post-experimentally
we measured the length of the osteotomy of the knees operated with OWO.
The mean length was 60.6 ± 4.9 mm (range 55-68). Inserting a tricalcium phosphate
wedge of 7 millimeters the calculated mean tibial wedge angle was 6.6º ± 0.5º
(range 5.9º – 7.2º) (Table 3). We found a final tibial wedge with a mean angle of 6.2º.
The loss of correction of 0.4º might be the result of bone loss caused by cutting.
Billings et al. reported good clinical results with CWO, rigid internal fixation and early
motion, when using a calibrated osteotomy cutting guide 3. In our study we also used
a guide instrument for CWO. With CWO we found a higher mean post operative tibial
wedge angle compared to OWO (9.5º ± 2.8º resp. 6.2º ± 2.0º, p=0.08).
Thus, resulting in a minor under-correction of 0.8º with OWO and a major over-correction
Table 1
Mean regression analysis of rotation and translation
CWO= closed wedge osteotomy, OWO= open wedge osteotomy
Displayed are mean values (*10-3) (95% confidence intervals)
CWO OWO p-value
Rotation
X-axis -1.8 (-4.3-0.7) -0.2 (-1.5-1.1) 0.07
Y-axis 0.4 (-0.7-1.6) 0.4 (-0.1-0.8) 0.90
Z-axis -0.2 (-1.7-1.3) -0.9 (-1.8-0.1) 0.37
Translation
X-axis -0.1 (-0.7-0.5) -0.3 (-0.7-0.2) 0.45
Y-axis -0.5 (-0.9- -0.1) -0.7 (-0.9- -0.2) 0.21
Z-axis -0.5 (-1.2-0.3) -0.1 (-0.4-0.2) 0.36
Table 2
Bone Mineral Density and moment of failure
OWO= open wedge osteotomy, CWO= closed wedge osteotomy
BMD= bone mineral density
OWO CWO
BMD failure load BMD failure load
(g/cm2) (Newton) (g/cm2) (Newton)
mean lateral medial mean lateral medial
A 0,3 0,4 0,4 2250 0,3 0,4 0,3 2000
B 0,3 0,4 0,6 2000 0,3 0,5 0,3 2250
C 0,4 0,5 0,4 2250 0,5 0,6 0,4 2000
D 1,0 1,1 1,0 2750 0,7 0,7 0,8 1250
E 0,4 0,5 0,4 1000 0,4 0,5 0,4 1000
α = tan -1 ( y/x )
x
y
α
Figure 4
The angle of correction (α)
is determined by
the height of the medial
opening(Y) and the length
of the osteotomy (x).

46
Chapter 3
47
Accuracy and initial stability of open and closed wedge high tibial osteotomy; a cadaveric RSA study
of 2.5º with CWO but with high variation in the two groups. Although no statistical
difference was found , there is a tendency of overcorrection in the CWO group.
In a clinical situation an achieved tibial wedge angle larger than planned may result in
an excessive over-correction, which has poor long-term results 10. Our findings
correspond to those of Magyar et al., who used hemicallostasis osteotomy (HCO),
a different technique of OWO, and reported HCO to be more precise than CWO in the
predicted postoperative tibial wedge angle 16. OWO might be more accurate because
only one bone cut is performed. The correction angle is than merely achieved by
placing the TCP wedge. With CWO one has to perform two bone cuts, which can
introduce more loss of accuracy. Bone loss as a result of performing the osteotomies
depends on the thickness of the saw blade and surgeon skills, and will be of influence
on the achieved correction angle. With CWO, a residue of the medial top of the bony
wedge can act as a hinge when the wedge is closed. The achieved correction will be
higher than planned in this case. These might be factors in explaining the overcorrection
we found with CWO. Furthermore, in this study the absolute values of the postoperative
correction angles are the mathematical results of RSA data calculated to rotational
displacement in the frontal, transverse and sagittal plane. As can be seen from
the wide ranges and rather high standard deviations it seems that the highly sensitive
RSA reveals the truth in the three dimensional obtained correction angles.
The achieved correction angles we found in both the OWO and CWO group in this
study will probably be sufficient in clinical practice. To be more specific informed about
the clinical significance of the difference between OWO and CWO, there is need for
further randomized clinical research, which we currently perform in a two centre study.
Osseous displacement, defined as rotation and translation of the bone segments
relative to each other, started immediately after axial load bearing albeit in relatively
small amounts. A linear correlation between load magnitude and osseous displacement
could be seen until just prior to failure. This indicates that the reconstruction is stable
until the moment of gross failure. The data of osseous displacement under the influence
of load bearing showed a relative large osseous displacement just before failure.
This would bias the regression analysis and therefore we decided not to include these
last data points in our regression analyses. The regression analyses of both groups
were compared and no significant difference was found between CWO and OWO
in rotation and translation in any direction. Hence, both methods provide for a stable
situation prior to failure. This leads to the conclusion that there is no significant
difference in initial stability between CWO and OWO.
The direction of failure was probably mainly influenced by the way the knees were
positioned in the MTS. The axial loading was along the axis of the femur and the tibia
was placed in valgus, therefore the axial loading made the tibia translate laterally.
This resulted in high compression forces on the lateral tibial plateau. In the OWO-knees
this also seemed to be the most vulnerable area and longitudinal split fractures occurred
just lateral of the tips of the proximal screws. In the CWO-knees the surgical implants
withstood most of the compression forces on the lateral aspect of the tibia resulting in
different failure patterns. In one case, the screw directly distal to the osteotomy was
pulled through the plate. Because of the dependence of the position in the MTS these
failure mechanisms might not be similar to clinical practice.
Failure did not occur beneath loading of two times bodyweight, indicating a good initial
stability of the reconstruction in both CWO and OWO. In clinical practice, the stability
will further increase with bone healing and ingrowth of the TCP wedge. Considering this,
initial (partial) weight bearing might be possible.
DEXA-scans were made to be informed about the BMD of all knees and to exclude
differences between paired knees. The DEXA-scan showed in all knees, except one,
Table 3
Length of osteotomy and calculated postoperative correction angles in
open wedge osteotomy using a 7 mm wedge
Knee length osteotomy (mm) tan-1(y/x )(degrees)
Ao 68 5.9
Bo 62 6.4
Co 58 6.9
Do 55 7.2
Eo 60 6.7
Mean ± SD 60.6 ± 4.9 6.6 ± 0.5

48
Chapter 3
49
Accuracy and initial stability of open and closed wedge high tibial osteotomy; a cadaveric RSA study
a higher BMD in the lateral condyles than in the medial condyles. With DEXA-scan
measurements on condyles Akamatsu et al. reported higher BMD’s in condyles along
the mechanical axis of the leg 1. This corresponds to our findings, because we used
‘normal’ human cadaver knees and not knees with a varus deformity. We found no
significant correlation between BMD and the moment of failure (p=0.27). BMD does
not seem to be critical using this rigid locked plate fixation system. Based on the
results of this study we conclude that both methods gave an acceptable correction
with high variation of postoperative correction angles. There was a tendency of
overcorrection in the CWO group but no significant difference was found. We found no
difference in initial stability between CWO and OWO with a rigid locked plate fixation.
Although OWO seems to become more popular further clinical research has to be
performed to determine if it has major advantage over CWO or not.
References
1. Akamatsu Y, Koshino T, Saito T, Wada J (1997) Changes in osteosclerosis of the osteoarthritic knee
after high tibial osteotomy. Clin Orthop 334: 207-214
2. Aronson A S, Hoist L, Selvik G (1974) An instrument for insertion of radiopaque bone markers.
Radiology 113: 733-734
3. Billings A, Scott D F, Camargo M P, Hofmann A A (2000) High tibial osteotomy with a calibrated
osteotomy guide, rigid internal fixation, and early motion - Long-term follow-up.
J Bone Joint Surg Am 82A: 70-79
4. Closkey R F, Windsor R E (2001) Alterations in the patella after a high tibial or distal femoral
osteotomy. Clin Orthop 389: 51-56
5. Coventry M B, Ilstrup D M, Wallrichs S L (1993) Proximal tibial osteotomy. A critical long-term study
of eighty-seven cases. J Bone Joint Surg Am 75: 196-201
6. Fowler J L, Gie G A, MacEachern A G (1991) Upper tibial valgus osteotomy using a dynamic
external fixator. J Bone Joint Surg Br 73: 690-691
7. Hernigou P, Medevielle D, Debeyre J, Goutallier D (1987) Proximal tibial osteotomy for osteoarthritis
with varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am 69: 332-354
8. Hernigou P, Ovadia H, Goutallier D(1992) Mathematical modeling of open wedge tibial osteotomy
and correction tables. Rev Chir Orthop Reparatrice Appar Mot 78: 258-263
9. Insall J N, Joseph D M, Msika C(1984) High tibial osteotomy for varus gonarthrosis. A long-term
follow-up study. J Bone Joint Surg Am 66: 1040-1048
10. Ivarsson I, Myrnerts R, Gillquist J (1990) High tibial osteotomy for medial osteoarthritis of the knee.
A 5 to 7 and 11 year follow-up. J Bone Joint Surg Br 72: 238-244
11. Kärrholm J (1989) Roentgen stereophotogrammetry: Review of orthopedic applications.
Acta Orthop Scand 60: 491-503
12. Kettelkamp D B, Wenger D R, Chao E Y, Thompson C (1976) Results of proximal tibial osteotomy.
The effects of tibiofemoral angle, stance-phase flexion-extension, and medial-plateau force.
J Bone Joint Surg Am 58: 952-960
13. Koshino T, Morii T Wada J et al.(1989) High tibial osteotomy with fixation by a blade plate for medial
compartment osteoarthritis of the knee. Orthop Clin North Am 20: 227-243
14. van Loon C J, de Waal Malefijt M C, Breemans E, Veth R P(1995) Complications of high tibial
osteotomy. Orthop Int Ed 3: 484-488
15. Lobenhoffer P, Simoni C D, Staubli A E (2002) Open-wedge high tibial osteotomy with rigid plate
fixation. Techn in Knee Surgery 2: 1-11

50
Chapter 3
16. Magyar G, Toksvig-Larsen S, Lindstrand A (1998) Open wedge tibial osteotomy by callus distraction
in gonarthrosis: Operative technique and early results in 36 patients. Acta Orthop Scand 69: 147-51
17. Maquet P (1976) Valgus osteotomy for osteoarthritis of the knee. Clin Orthop 120: 143-148
18. Odenbring S, Egund N, Hagstedt B et al. (1991) Ten-year results of tibial osteotomy for medial
gonarthrosis. The influence of overcorrection. Arch Orthop Trauma Surg 110: 103-108
19. Sprenger T R, Doerzbacher J F (2003) Tibial osteotomy for the treatment of varus gonarthrosis.
Survival and failure analysis to twenty-two years. J Bone Joint Surg Am 85A: 469-474
chapter 4Correction accuracy and collateral laxity in
open versus closed wedge high tibial osteotomy
a one year randomized controlled study
R.D.A. Gaasbeek, L. Nicolaas, W.J. Rijnberg, C.J.M. van Loon, A. van Kampen
Submitted J Bone Joint Surg Br

52
Chapter 4
53
Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomyA one year randomized controlled study
Abstract
In a randomized clinical trial in 50 patients with symptomatic osteoarthritis of the
medial compartment of the knee, the clinical results of high tibial osteotomy (HTO)
according to the open wedge osteotomy (OWO) and closed wedge osteotomy (CWO)
were compared. In both groups angle stable plate fixation was used.
Clinical and radiological assessments were performed preoperative and after one year.
Postoperative hip-knee-ankle (HKA) correction angles were monitored on standing
leg X-rays. The effect of HTO on collateral laxity of the knee was measured with a
specially designed varus-valgus device. The WOMAC osteoarthritis index, the modified
knee society score (KS) and visual analogue scales (VAS) were used to assess
symptoms of osteoarthritis, function, pain and patient satisfaction.
At one year follow-up we found accurate corrections in both groups and the planned
correction angles were achieved. No loss of correction was observed. Furthermore,
the medial collateral laxity and the patellar height significantly decreased after OWO.
Significant improvements of WOMAC and KS scores were found in both groups.
All patients had significantly less pain and were significantly satisfied with the results.
Surgery time was significant longer in the CWO group, and complications were more
frequent in this group. Both techniques led to good and comparable clinical results.
The choice whether to perform an open or a closed wedge osteotomy may be based
on preoperative patellar height or concomitant collateral laxity.
Introduction
Young active patients with medial compartment osteoarthritis of the knee combined
with a varus deformity can be treated with a valgus high tibial osteotomy 1,2-4,5.
High tibial osteotomy (HTO) is performed to stop or inhibit progression of osteoarthritis
and to avoid or postpone total knee arthroplasty. In order to unload the medial
compartment, a valgus producing correction is applied by performing either a closed
wedge osteotomy (CWO), or an open wedge osteotomy (OWO). OWO is a relatively
new technique and is less involving in terms of surgical technique than CWO: only one
tibial cut needs to be made, and osteotomy of the fibula is not necessary 6.
In recent years, with the introduction of new rigid locked implants in combination with
new bone-substituting biomaterials, OWO has become more popular than CWO,
avoiding co-morbidity associated with the fibular osteotomy. Hypothetically OWO is
more accurate than CWO. However, in terms of clinical outcome these possible
advantages have not yet been thoroughly investigated in well conducted randomized
studies. Furthermore, positioning the osteotomy proximal to the tibial tuberosity and the
insertion of the medial and lateral collateral ligament will lead to potential changes in
patellar height and collateral laxity. Previous studies which compared CWO and OWO
in patients do not answer important clinical questions in terms of outcome, safety and
ligamentous stability 7-9.
The aim of the current study was to compare OWO and CWO with angle stable plate
fixation, regarding the accuracy of achievement of the planned correction, the influence
on collateral laxity and patellar height and the clinical outcome in a randomised
prospective study.
Methods and materials
Patients
Fifty consecutive patients, suffering from medial compartment osteoarthritis of the knee
were included in the study. Between January 2003 and March 2005 they visited the
Orthopaedic outpatient clinics of the Rijnstate Hospital in Arnhem or the University
Medical Centre Saint Radboud in Nijmegen, in the Netherlands. Included were active

54
Chapter 4
55
Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomyA one year randomized controlled study
patients between 18 and 70 years of age, suffering from medial osteoarthritis of the
knee with a hip-knee-ankle (HKA) varus alignment. Patients with rheumatoid arthritis or
previous osteotomy of the same knee were excluded from this study. All patients gave
their informed consent. Approval of the local Medical Ethics Committee was obtained.
Patients were randomized for their treatment according to a sealed envelopes procedure.
Primary outcome measures
Achievement of the planned correction angle of an over-correction of 4º of the
mechanical femur-tibial axis was measured on standing whole leg radiographs.
HKA angles were measured by one observer (RG). Medial and lateral collateral laxity of
the knee was measured pre- and post-operatively at one year follow-up and quantified
using a varus/valgus testing device 10. This device consisted of a base plate with a
support in which the knee could be fixed in 20º of flexion in a standardised fashion.
The foot was fixed in a mobile shoe with an attached pointer. The varus and valgus
laxity was measured by putting a load of 50 N on the leg which produced a varus or
valgus force on the knee which was quantified on a scale on the base plate (Fig 1).
Previously the intra- and inter observer reliabilities of this device were determined and
showed acceptable intra class correlation coefficients: ICC= 0.78; 95%CI=0.75-0.79
and ICC= 0.71; 95% CI= 0.69- 0.72, respectively.
Secundary outcome measures
Symptoms of osteoarthritis were assessed by the Western Ontario and McMaster
Universities (WOMAC) osteoarthritis index. A higher WOMAC score represents worse
symptom severity, with 96 points being the worst possible total score. Function was
determined using the modified Knee Society score (KS) which assesses pain, range
of movement, stability and the ability to walk and climb stairs with 200 points maximum
representing the best possible function 11;12. Pain intensity and patient-satisfaction
were scored with a 0-10 Visual Analogue Scale (VAS). A high VASknee pain score
represents more pain, whereas a low VASsatisfaction score reveals an unsatisfactory
situation for the patient.
Patellar height according to Caton’s Index (CI) was measured by one observer (RG) on
true lateral radiographic views in 30º of flexion. Furthermore, surgery time, duration of
hospital stay and complications were recorded.
Operation techniques
Closed wedge osteotomy (Fig. 2)
A standard anterolateral approach was used. An osteotomy and resection was performed
through the fibular head. Two centimetres below and parallel to the joint line a Kirschner
wire was inserted to aim the osteotomy. First, the proximal cut was performed and the
medial cortex was preserved. Using an aiming device the distal cut was made and the
bone wedge was removed. The aiming device we used consists of a blade which is
put in the first saw cut. The second cut is performed through a cleft in the device with
an adjustable angle to the blade. The defect was closed and the osteotomy was fixed
with a four hole angle stable plate (Numélock II system, Stryker, Switzerland).
Figure 1
Measuring the medial
and lateral laxity of
the knee with the varus-
valgus device.

56
Chapter 4
57
Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomyA one year randomized controlled study
Open wedge osteotomy (Fig. 3)
A medial approach was performed, shifting the pes anserinus and the superficial
medial collateral ligament dorsally. A Kirschner wire was inserted parallel to the
joint line. Using a guide instrument a second wire was inserted just proximal of the
tuberosity in lateral cranial direction in order to obtain an equal osteotomy angle in all
knees. Along this wire the osteotomy was performed. The lateral cortex was left intact.
The gap was opened gradually and the preoperatively calculated correction angle was
checked with a measuring device. After this height of the medial gap was measured
and the appropriate resorbable tricalcium phosphate (TCP) wedge (Otis, Lourdes,
France) was inserted. Internal fixation was performed using a four hole angle stable
plate (Numélock II system, Stryker, Switzerland).
All surgery was performed under fluoroscopic guidance. All patients received antibiotic
prophylaxis preoperatively and postoperative antithrombotic therapy during six weeks.
Postoperative management was equal for both groups. Mobilisation started the first post-
operative day with partial weight bearing and full range of motion exercises for six weeks.
Statistical analysis
A multivariable linear regression method was used to analyze the effect of OWO versus
CWO on HKA angles, WOMAC, KS and VAS scores, CI, medial and lateral collateral
laxity of the knee and complication rate. Age, gender, BMI, baseline values for the HKA
angle were considered as possible confounders and included in the regression model.
For statistical analysis the SPSS program was used and p<0.05 was considered
statistically significant.
Table 1 Baseline parameters
Open wedge osteotomy Closed wedge osteotomy Total group (n=25) (n=25) (n=50)
Male/female 14/11 16/9 30/20
Age (yrs) mean (SD) 47.0 (8.5) 49.8 (7.4) 48.4 (8.0)
BMI (kg/m2) mean (SD) 29.7 (4.2) 28.4 (2.9) 29.0 (3.7)
HKA varus angle(°) mean (SD) 4.3(2.2) 4.1 (2.1) 4.1 (2.4)
WOMAC (0-96) mean (SD) 51.9 (18.5) 46.5 (14.9) 49.2 (16.9)
KS (0-200) mean (SD) 111.7 (24.1) 113.6 (15.9) 112.6 (20.2)
VAS knee pain (0-10) mean (SD) 6.6 (1.7) 6.4 (1.3) 6.5 (1.5)
VAS satisfaction (0-10) 2.3 (1.8) 2.8 (1.8) 2.6 (1.8)
Medial laxity (°) mean (SD) 5.5 (1.8) 5.4 (1.2) 5.5 (1.5)
Lateral laxity (°) mean (SD) 5.2 (1.1) 5.2 (1.3) 5.2 (1.2)
Caton Index 1.0 (0.2) 1.0 (0.2) 1.0 (0.2)
Figure 2
An example of the closed
wedge high tibial osteotomy
(CWO)
Figure 3
An example of the open
wedge high tibial osteotomy
(OWO)

58
Chapter 4
59
Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomyA one year randomized controlled study
Results
No patients were lost to follow-up. 36 patients were treated in Arnhem (19 CWO and
17 OWO) and 14 patients were treated in Nijmegen (6 CWO and 8 OWO).
Table 1 shows all baseline parameters of the total study population and of each of
the treatment groups separately. In total, the group of patients consisted of 20 women
and 30 men, with an mean age of 48.4 (SD 8.0) years and a mean HKA angle of 4.1°
varus (SD 2.4). The mean BMI was 29.0 kg/m2 (SD 3.7).
Preoperatively the mean WOMAC score was 49.2 (SD 16.9) and the mean KS score
was 112.6 (SD 20.2). Furthermore, the mean VASknee pain score was 6.5 (SD 1.5) and the
mean VASsatisfaction was 2.6 (SD 1.8) before surgery. The mean medial and lateral laxity of
the knee was 5.5º (SD 1.5) and 5,2º (SD 1.2) respectively. The mean Caton Index was
1.0 (SD 0.2).
There were no statistical differences between the groups.
Primary outcome measures
Table 2 presents the results at 1- year follow-up. We found no difference between OWO
and CWO in the achieved postoperative correction angles. The mean postoperative
HKA angle was 3.8º valgus (SD 2.2) in the OWO group, and 4.4º valgus (SD 2.7) in the
CWO group (p=0.474).
The OWO group showed a mean postoperative reduction of the mean medial collateral
knee laxity to 4.5º (SD 1.5) versus 5.3º (SD 1.2) in the CWO group. This difference was
significant (p=0.041). The mean lateral collateral laxity did not change significantly:
5.3º (SD 1.1) after OWO and 5.5º (SD 1.0) after CWO (p=0.505).
Secundary outcome measures
The results are presented in table 2. The WOMAC and KS scores showed equal
effects between the groups. The mean WOMAC score decreased to 20.0 (SD 19.4)
and 16.0 (SD 15.0) after OWO respectively CWO. The mean KS score increased to
176.6 (SD 23.4) in the OWO group and 180.2 (SD 22.2) in the CWO group.
The mean VASknee pain decreased in both groups: 2.5 (SD 1.9) after OWO and 1.8
(SD 1.5) after CWO. In both groups the patients were content with the result after one
year. The mean VASsatisfaction increased to 7.8 (SD 1.8) in the OWO group and 8.7
(SD 1.4) in the CWO group. There were no significant differences between the groups.
The patellar height significantly decreased after OWO. The small increase of patellar
height following CWO was not significant. The mean CI after OWO was 0.86 (SD 0.14)
and after CWO it was 1.04 (SD 0.17). This difference was significant (p<0.001).
The mean surgery time of 54.8 min (SD 10.8) in the OWO group was significantly
shorter than the mean surgery time for the CWO of 68.0 min (SD 22.2) (p=0.010).
No difference was detected for the mean hospital stay, with 3.4 days (SD 1.8) for
the OWO group and 3.9 days (SD 1.5).
Table 2 Results at one-year follow-up
Primary outcomes
HKA valgus angle(°) mean (SD) 3.8 (2.2) 4.4 (2.7) 0.6 -0.82; 1.93 0.420
Medial laxity (°) mean (SD) 4.5 (1.5) 5.3 (1.2) 0.8 0.09;0.27 0.041*
Lateral laxity (°) mean (SD) 5.3 (1.1) 5.5 (1.0) 0.2 -0.39;0.78 0.505
Secondary outcomes
WOMAC (0-96) mean (SD) 20.0 (19.4) 16.0 (15.0) 4.0 -13.85;5.85 0.418
KS (0-200) mean (SD) 176.6 (23.4) 180.2 (22.2) 3.6 -9.36;16.56 0.579
VAS (0-10) knee pain mean (SD) 2.5 (1.9) 1.8 (1.5) 0.6 -1..60;0.38 0.221
VAS (0-10) satisfaction 7.8 (1.8) 8.7 (1.4) 0.9 -0.07; 1.78 0.07
Caton Index 0.86 (0.14) 1.04 (0.17) 0.18 0.09;0.27 <0.001*
Surgery time (min) 54.8 (10.8) 68.0 (22.2) 13.2 3.27;23.12 0.010*
Hospital stay (days) 3.4 (1.8)) 3.9 (1.5) 0.5 -0.46;1.42 0.311
*significant p-value
Open wedge
osteoto
my
mean (S
D) (n=
25)
Close
d wedge
osteoto
my
mean (S
D) (n=
25)
Mean d
iffere
nce
95% c
onfidence
inte
rval
p-valu
e

60
Chapter 4
61
Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomyA one year randomized controlled study
Complications during follow-up (Table 3)
All patients reported a local hypoesthesia on the lateral side of the lower leg as a result
of cutting branches of the infra-patellar nerve. These findings were equal for both the
OWO and CWO group. One patient in the CWO group suffered a temporary peroneal
nerve neuropathy. In the CWO group one case of deep venous thrombosis was
presented. One deep wound infection was treated in the CWO group and healed after
surgical lavage and antibiotics. In this group, two superficial wound infections were
successfully treated with antibiotics.
In the OWO group, one superficial wound infect was treated with antibiotics.
Because of pain the osteosynthesis material was removed in 2 patients in the OWO
group and in 1 patient in the CWO group.
Discussion
The purpose of this study was to compare the OWO and the CWO in a randomized
clinical setting. Randomized clinical research in this field is very limited. At the time of
design of this study, two randomized trials concerning OWO versus CWO had been
published by Magyar et al 13;14. However, neither of these studies is directly comparable
to the current project, since in both studies the OWO was performed by the
hemicallotasis technique (HCO) and the CWO was fixated with staples. They found
significant loss of correction in the CWO group and a significantly more stable fixation
with HCO. Furthermore, they found more complications in the HCO group, mainly
pin-track infections. The clinical scores were improved in both groups with no
significant difference between the groups. Hospital stay of the HCO group was
significantly shorter.
Adili et al. performed a case controlled study of HTO with the Ilizarov external fixator
versus the Coventry-type CWO. The found significantly better WOMAC scores but also
more complications in the Ilizarov group 15.
Nakamura et al. compared the HCO to the dome osteotomy (DMO) in a randomized
clinical trial. The HCO group had significantly less changes in patellar height and tibial
slope. The femur-tibia angles were not significantly different 16.
Recently, Brouwer et al. performed a prospective randomised trial in 92 patients.
At one year follow-up they concluded that CWO achieved a more accurate correction
and that both OWO and CWO reduce pain and improve function. A relevant difference
to our study is the fact that they used a non-stable implant (Puddu, Arthrex, Naples
Florida, USA) in the OWO and staples in the CWO group. Furthermore, a plaster cast
was part of the after-treatment 17.
Hoell et al. presented the clinical results of open versus closed wedge HTO techniques
in a retrospective study in 108 patients 18. They analysed the results and outcome of
OWO with a Puddu plate versus a Coventry-type CWO with staples. They observed no
differences in outcome between the two methods. Both groups showed a significant
improvement of clinical scores. Drawback of this study was the non-randomized
setting. Furthermore, the statistical analysis was not transparently reported.
Rudan and Simurda 19 found in their study that optimal clinical results were associated
with a correction of the femur-tibial angle between 6° and 14° . Under-correction was
associated with a high failure rate. Over-correction to a femur-tibial angle larger than
15° appeared to have an even better clinical outcome, but these results were
cosmetically unappealing to the patients. Other authors also recommend over-
correction of the femur-tibial angle 20;21. Hernigou on the contrary found that an
overcorrection of more than 6° is associated with progressive degeneration of the
lateral compartment and a under-correction is associated with poorer result and
reappearance of the medial compartment osteoarthritis 22. A previous cadaveric RSA
Table 3 Complications during follow-up
Open wedge osteotomy Closed wedge osteotomy (n=25) (n=25)
Peroneal nerve neuropathy 1
Deep venous thrombosis 1
Deep wound infection 1
superficial wound infections 1 2
removal of osteosynthesis material 2 1

62
Chapter 4
63
Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomyA one year randomized controlled study
study showed that both CWO and OWO gave an acceptable correction with a high
variation of postoperative correction angles. This study showed a tendency of
overcorrection in the CWO group and no difference in initial stability between CWO
and OWO with a rigid locked-plate fixation 23.
In the present clinical trial the aim was a HKA valgus angle of 4°. We found a post-
operative angle of 3.8° (SD 2.2, range 1.0-10.6) in the OWO group and 4.3° (SD 2.7,
range 1.0-12.0) in the CWO group. We observed no loss of correction after one year
follow-up. Thus, we conclude that both techniques led to an accurate and reliable
correction with the angle stable plate fixation.
In varus osteoarthritis of the knee, often a pseudo medial hyperlaxity is observed due
to the loss of medial joint space. Because the osteotomy is located proximally to the
superficial medial collateral ligament, opening the osteotomy will (re-)tighten the medial
structures. Hoell et al. investigated the influence of HTO on the medial and lateral
collateral stability. After OWO they found a shift from second degree (5-10mm) and
third degree(>10mm) to first degree (<5mm) medial instability. In their study, the level
of instability was determined by physical examination, which is not very objective 24.
We observed a significant decrease in medial collateral laxity of the knee after OWO.
The lateral and medial collateral laxity was measured with a special developed device
which enables objective reliable and reproducible varus and valgus measurements 25.
If the medial collateral ligament is tensioned excessively, e.g. in large corrections, the
pressure in the medial joint compartment may increase. To prevent this and to obtain
the desired correction the superficial medial collateral ligament should be partially
released to allow for proper opening of the osteotomy.
OWO proximal to the tibial tuberosity has been reported to cause patella baja 26,27;28.
CWO has been shown to lead to both patella baja and alta. These alterations in patellar
height have been attributed to the proximalisation (CWO) or distalisation (OWO) of the
tibial tuberosity following HTO. Furthermore, scarring, adhesions and contracture of the
patella ligament are mentioned to cause lowering of the patella in CWO 29. As expected,
we observed that the mean patellar height significantly decreased in the OWO group.
We saw no significant change in patellar height after CWO. We advice to perform a
distal tuberosity osteotomy to prevent distalisation of the tibial tuberosity with OWO in
large corrections or in case of preexistent patella baja 30.
To our knowledge, the present study is the first randomized clinical trial comparing
OWO and CWO using rigid angle stable implants and the same functional
postoperative treatment protocol in both groups. At one year follow-up we found
significant improvements of WOMAC and KS scores in both groups. Furthermore,
all patients had significantly less pain and were significantly satisfied with the treatment.
There were no differences in outcome between the groups. The medial collateral laxity
and the patellar height significantly decreased after OWO.
The authors are aware that the present study concerns only a short term follow-up.
Longer follow-up is essential to obtain information about the ongoing clinical results in
both groups. Nevertheless, this study has shown that both osteotomy techniques
led to good and comparable clinical results. Surgery time was significant longer in
the CWO group, and complications were more frequent in this group. In large OWO
corrections, the tightening of the medial collateral ligament and lowering of the patella
should be addressed by the surgeon. Along with the fact that the OWO procedure is
less demanding and that it offers the surgeon more opportunities to vary the amount of
valgus and slope correction intraoperatively, the authors prefer the OWO in their clinical
practices. In this study OWO has showed comparable results to CWO and it was a safe
and reproducible technique. Furthermore, the osteotomy of the fibula along with its
rather high co-morbidity of pain, pseudoarthrosis and peroneal nerve palsy, is not
necessary with OWO. Especially in teaching hospitals, this technique seems to be
more predictable for correcting varus deformities of the knee.

64
Chapter 4
65
Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomyA one year randomized controlled study
Reference List
1. Aglietti P, Buzzi R, Vena LM, Baldini A, Mondaini A. High tibial valgus osteotomy for medial
gonarthrosis: a 10- to 21-year study. J Knee Surg 2003;16:21-26.
2. Amendola A. Unicompartmental osteoarthritis in the active patient: the role of high tibial osteotomy.
Arthroscopy 2003;19 Suppl 1:109-116.
3. Choi HR, Hasegawa Y, Kondo S, Shimizu T, Ida K, Iwata H. High tibial osteotomy for varus
gonarthrosis: a 10- to 24-year follow-up study. J Orthop Sci 2001;6:493-497.
4. Hernigou P, Medevielle D, Debeyre J, Goutallier D. Proximal tibial osteotomy for osteoarthritis with
varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354.
5. Odenbring S, Egund N, Hagstedt B, Larsson J, Lindstrand A, Toksvig-Larsen S. Ten-year results of
tibial osteotomy for medial gonarthrosis. The influence of overcorrection.
Arch Orthop Trauma Surg 1991;110:103-108.
6. Hoell S, Suttmoeller J, Stoll V, Fuchs S, Gosheger G. The high tibial osteotomy, open versus closed
wedge, a comparison of methods in 108 patients. Arch Orthop Trauma Surg 2005;:1-6.:1-6.
7. Hoell S, Suttmoeller J, Stoll V, Fuchs S, Gosheger G. The high tibial osteotomy, open versus closed
wedge, a comparison of methods in 108 patients. Arch Orthop Trauma Surg 2005;:1-6.:1-6.
8. Magyar G, Ahl TL, Vibe P, Toksvig-Larsen S, Lindstrand A. Open-wedge osteotomy by
hemicallotasis or the closed-wedge technique for osteoarthritis of the knee. A randomised study of
50 operations. J Bone Joint Surg Br 1999;81:444-448.
9. Brouwer RW, Bierma-Zeinstra SM, van Koeveringe AJ, Verhaar JA. Patellar height and the inclination
of the tibial plateau after high tibial osteotomy. The open versus the closed-wedge technique.
J Bone Joint Surg Br 2005;87:1227-1232.
10. Rasenberg EI, Lemmens JA, van Kampen A et al. Grading medial collateral ligament injury:
comparison of MR imaging and instrumented valgus-varus laxity test-device. A prospective
double-blind patient study. Eur J Radiol 1995;21:18-24.
11. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC:
a health status instrument for measuring clinically important patient relevant outcomes to
antirheumatic drug therapy in patients with osteoarthritis of the hip or knee.
J Rheumatol 1988;15:1833-1840.
12. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system.
Clin Orthop Relat Res 1989;13-14.
13. Magyar G, Ahl TL, Vibe P, Toksvig-Larsen S, Lindstrand A. Open-wedge osteotomy by
hemicallotasis or the closed-wedge technique for osteoarthritis of the knee. A randomised study of
50 operations. J Bone Joint Surg Br 1999;81:444-448.
14. Magyar G, Toksvig LS, Lindstrand A. Changes in osseous correction after proximal tibial
osteotomy - Radiostereometry of closed- and open-wedge osteotomy in 33 patients.
Acta Orthop Scand 1999;70:473-477.
15. Adili A, Bhandari M, Giffin R, Whately C, Kwok DC. Valgus high tibial osteotomy. Comparison
between an Ilizarov and a Coventry wedge technique for the treatment of medial compartment
osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc 2002;10:169-176.
16. Nakamura E, Mizuta H, Kudo S, Takagi K, Sakamoto K. Open-wedge osteotomy of the proximal
tibia hemicallotasis. J Bone Joint Surg Br 2001;83:1111-1115.
17. Brouwer RW, Bierma-Zeinstra SM, van Raaij TM, Verhaar JA. Osteotomy for medial compartment
arthritis of the knee using a closing wedge or an opening wedge controlled by a Puddu plate:
a one-year randomised, controlled study. J Bone Joint Surg Br 2006;88:1454-1459.
18. Hoell S, Suttmoeller J, Stoll V, Fuchs S, Gosheger G. The high tibial osteotomy, open versus closed
wedge, a comparison of methods in 108 patients. Arch Orthop Trauma Surg 2005;:1-6.:1-6.
19. Rudan JF, Simurda MA. High tibial osteotomy. A prospective clinical and roentgenographic review.
Clin Orthop 1990;251-256.
20. Ivarsson I, Myrnerts R, Gillquist J. High tibial osteotomy for medial osteoarthritis of the knee.
A 5 to 7 and 11 year follow-up. J Bone Joint Surg Br 1990;72:238-244.
21. Kettelkamp DB, Wenger DR, Chao EY, Thompson C. Results of proximal tibial osteotomy.
The effects of tibiofemoral angle, stance-phase flexion-extension, and medial-plateau force.
J Bone Joint Surg Am 1976;58:952-960.
22. Hernigou P, Medevielle D, Debeyre J, Goutallier D. Proximal tibial osteotomy for osteoarthritis with
varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354.
23. Gaasbeek RD, Welsing RT, Verdonschot N, Rijnberg WJ, van Loon CJ, van Kampen A. Accuracy
and initial stability of open- and closed-wedge high tibial osteotomy: a cadaveric RSA study.
Knee Surg Sports Traumatol Arthrosc 2005;Nov;13(8):689-694.
24. Hoell S, Suttmoeller J, Stoll V, Fuchs S, Gosheger G. The high tibial osteotomy, open versus closed
wedge, a comparison of methods in 108 patients. Arch Orthop Trauma Surg 2005;:1-6.:1-6.
25. Rasenberg EI, Lemmens JA, van Kampen A et al. Grading medial collateral ligament injury:
comparison of MR imaging and instrumented valgus-varus laxity test-device. A prospective
double-blind patient study. Eur J Radiol 1995;21:18-24.
26. Brouwer RW, Bierma-Zeinstra SM, van Koeveringe AJ, Verhaar JA. Patellar height and the inclination
of the tibial plateau after high tibial osteotomy. The open versus the closed-wedge technique.
J Bone Joint Surg Br 2005;87:1227-1232.
27. Kesmezacar H, Erginer R, Ogut T, Seyahi A, Babacan M, Tenekecioglu Y. Evaluation of patellar height
and measurement methods after valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2005.

66
Chapter 4
28. Wright JM, Heavrin B, Begg M, Sakyrd G, Sterett W. Observations on patellar height following
opening wedge proximal tibial osteotomy. Am J Knee Surg 2001;14:163-173.
29. Scuderi GR, Windsor RE, Insall JN. Observations on patellar height after proximal tibial osteotomy.
J Bone Joint Surg Am 1989;71:245-248.
30. Gaasbeek RD, Sonneveld H, van Heerwaarden RJ, Jacobs WC, Wymenga AB. Distal tuberosity
osteotomy in open wedge high tibial osteotomy can prevent patella infera: a new technique.
Knee 2004;11:457-461.
chapter 5Mechanism of bone incorporation of
ß-TCP bone substitute in open wedge tibial
osteotomy in patients
Robert DA Gaasbeek, Hanneke G Toonen, Ronald J van Heerwaarden, Pieter Buma
Biomaterials. 2005 Nov;26(33):6713-9

68
Chapter 5
69
Mechanism of bone incorporation of ß-TCP bone substitute in open wedge tibial osteotomy in patients
Abstract
A histological study was performed of bone biopsies from 16 patients (17 biopsies)
treated with open wedge high tibial osteotomies for medial knee osteoarthritis.
The open wedge osteotomies were filled with a wedge of osteoconductive beta
tricalcium phosphate (ß-TCP) ceramic bone replacement. At the time of removal of
the fixation material, core biopsies of the area where the ß-TCP was located were
taken at different follow-up periods (6 to 25 months). ß-TCP resorption, bone ingrowth
and bone remodelling were studied. We hypothesized that the incorporation and
remodelling process occurs similarly as in animals.
Histology showed a good resorption of the ß-TCP with complete incorporation
and remodelling into new bone. The different phases as described in animal studies
were found. A correlation was found between histological findings and radiological
assessment.
In conclusion, ß-TCP appeared to be a bone replacement material with optimal
biocompatibility, resorption characteristics and bone conduction properties for
the clinical use.
Introduction
A valgus high tibial osteotomy (HTO) is the treatment of choice for medial knee
osteoarthritis and may be performed with a lateral closing wedge or a medial open
wedge technique 1-10. In case of a medial open wedge osteotomy, the bone gap
created during the osteotomy can be left open, or filled with autograft or allografts.
Furthermore, nonresorbable or resorbable bone substitutes can be used 1;11-15.
Autograft bone is generally considered to be the most successful bone filling material
because of its osteoconductive, osteoinductive and osteogenic properties 16-19.
Drawbacks of autograft use are increase of operation time and co-morbidity following
the bone harvesting at the iliac crest. Allografts entail the risk of virus transfer or may be
less potent to stimulate new bone formation. To encounter these problems, synthetic
bone substitutes have become more popular in the last twenty years 16;18;20.
Because of their synthetic origin, these materials cannot cause disease transmission.
It has been suggested that bone substitutes can accelerate bone growth and bone
remodelling which may lead to earlier full weight-bearing after open wedge HTO 11;17-20.
Particularly porous beta tricalcium phosphate (ß-TCP) is a very promising osteo-
conductive, ceramic bone substitute. ß-TCP has slightly different ratios of calcium
and phosphate than bone, but, in essence, the material properties are much like
the inorganic phase of bone, which constitutes 60% to 70% of human bone 18;20.
The macro-porosity of the material facilitates bone ingrowth. The resorption
characteristics depend on the mineral composition and the degree of sintering as
well as the porous structure 18;20-22. In animal studies tricalcium phosphates have
shown favourable biocompatibility, osteoconduction and resorption properties.
It appeared that the ß-TCP gradually resorbs and in the end is completely replaced
by remodelled bone 11;16-21;23-28.
The resorption of ß-TCP and its conversion into bone takes place in different phases.
In the first phase, there is some resorption of host bone, followed by apposition of
new bone on the TCP scaffold. During this phase the appearance on X-rays is that
of dense bone. In the following phase, there is further resorption of the ß-TCP and
remodelling of the bone and the density on X-rays decreases 11;17.

70
Chapter 5
71
Mechanism of bone incorporation of ß-TCP bone substitute in open wedge tibial osteotomy in patients
In patients, the incorporation was until recently assessed with standard radiographic
examination. However, it is not easy to classify bone healing and distinct between
bone and the remaining synthetic calcium phosphates on radiographs alone 16.
Based on an expected similarity of X-rays of patients with that of animals, a more
refined radiological classification system was proposed to monitor bone healing in
open wedge HTO with resorbable substitutes 11. In this classification system
(see materials and methods for details) five distinct phases can be discriminated.
So far it is not known if the resorption of ß-TCP and its conversion into bone occurs in
a similar way as in animals, but based on the similarity in x-rays we hypothesize that in
patients the same sequence of events takes place during the incorporation of the
ß-TCP scaffold as in animals. However, the only method to confirm this is histology.
This study concerns a radiological and histological follow-up examination of 16 patients
with medial osteoarthritis of the knee treated with medial open wedge high tibial osteo-
tomies (in one patient a bilateral procedure). The gap was filled with a wedge of ß-TCP.
At the time of the plate removal, a biopsy was taken through the implant site, which was
processed for histology. The process of incorporation is described and quantitative
measurements of ß-TCP resorption and new bone formation were carried out.
The histology was correlated with the radiological classification of bone healing and
related to the time frame between osteotomy and plate removal.
Materials and methods
In 16 patients (17 procedures: mean age at the time of taking the biopsy 43.6 ± 9.5 yrs),
with a medial uni-compartmental knee osteoarthritis, the open wedge osteotomy was
filled with a wedge of porous ß-TCP (Ca3(PO4)2 with 70% interconnected macropores
with a size of 100-500 µm (Fig. 1a) and micropores of 1 – 10 µm (chronOS™, Synthes
Biomaterials, Switzerland). One patient was operated on bilaterally. Preoperatively the
degree of correction was determined on a standing long-leg film. The mean knee
varus angle was 4.9 (SD ± 2.37) with a range between 2 and 11 degrees. The aim was
a correction to 3 degrees valgus creating medially based bone gaps between 5 and
14 mm. To preserve the correction, the osteotomy was fixed with a rigid angle stable
plate (TomoFix, Synthes). Postoperatively the patients were allowed partial weight
bearing of 10-15 kg for 6 weeks. Conventional AP and lateral radiographs were made
immediately after the operation, at six weeks, three months, six months, and at one
year postoperatively. The last X-ray before the removal of the fixation material was used
for the radiological classification of bone healing.
A radiological classification system to monitor bone healing in open wedge HTO with
resorbable substitutes was used 11. In Phase 0 of this classification (Table 1) no
remodelling takes place. In phase 1 there is a slight porosis of the bone. In phase 2
the ß-TCP is denser and the interface between ß-TCP and bone is blurred. In phase 3
the osteotomy is healed. In phase 4 the ß-TCP is not longer recognizable as distinct
entity, and in phase 5 the bone is normal again (complete remodelling).
Bone healing was studied histologically from bone biopsies taken during plate and
screws removal between 6 and 25 months postoperatively (mean 14.7 ± 5.82 months).
At that time, a core biopsy was taken from the medial 1/4 part of the bone region where
the ß-TCP was implanted (Fig. 1b). The biopsy was long enough to contain both sides
of the host bone. Serial non-decalcified sections along the long axis of all biopsies
were made, which were stained with HE and Goldner. A TRAP-staining was applied for
the visualization of osteoclasts. Two biopsies could not be analysed with TRAP-staining
Figure 1
A. b-TCP wedge. B. Location of biopsy.

72
Chapter 5
73
Mechanism of bone incorporation of ß-TCP bone substitute in open wedge tibial osteotomy in patients
since they were broken after taking the biopsy or not processed according to the
standard protocol. In all remaining biopsies the surface area of fibrous tissue, active
incorporation (fibrous invasion of the ß-TCP with osteoclast and osteoblast activity) and
that of newly formed trabecular bone that still contained some ß-TCP remnants at the
location of the original ß-TCP material, were estimated by two observers (HGT, PB).
In areas with new bone formation the surface area of the remaining ß-TCP and of bone
was quantified with an automated image analysis system (AnalySIS) and expressed as
percentage of the total region of interest.
Results
There were no complications during surgery or directly postoperative. Also, the
clinical healing process was without complications in all cases (i.e. normal time until
full weightbearing, no infection or non-union). Radiological follow-up showed
complete consolidation at 12 months in all cases (Fig. 2). According to the radiological
classification system all unions were classified as phase 4 or 5.
In 13 of 17 biopsy specimens, the original ß-TCP was still visible in the biopsies
(Fig. 3b, c). It had a granular appearance and in HE sections pink stained material
inside the ß-TCP indicated that material (fibrin or proteins) had penetrated into the
micropores of the ceramic (Fig.3b, c). Also small remnant areas of totally in bone
incorporated ß-TCP were present. In 6 of these 13 biopsies an also relatively larger
area of the original ß-TCP material was still present in the sections. In these biopsies
active incorporation of the ß-TCP was present. In 4 biopsies only totally remodelled
bone was found without any remnants of ß-TCP.
Particularly in the six biopsies with larger ß-TCP areas, different stages of incorporation
could be found. In the middle of the wedge, occasionally non-incorporated ß-TCP with
vascular fibrous tissue was found. More towards the osteotomy planes, the first bone
formation was found as lamellar bone apposition onto the surface of macropores in the
ß-TCP blocks (Fig. 3c). At the same locations, small mononuclear cells were found in
the pores between the ß-TCP that did not stain for TRAP (Fig. 3b). These cells were
Figure 2
Bone remodelling at different follow-up times after open wedge osteotomy filled with TCP.
A. at 6 weeks, B. at 3 months, C. at 6 months, D. at 12 months. (Adapted from van Hemert
et al. 11, with permission).
Figure 3
A. Thin section of ß-CP
material before
implantation. B. HE section
of first stage of incorpora-
tion. Fibrous tissue (FT)
has invaded the macro-
pores in the TCP blocks
and mononuclear cells
have penetrated into the
micropores of the TCP
(arrows). C. New lamellar
bone formation in macro-
pores of TCP. D. Pores of
TCP completely filled with
new bone (NB). Scale bar:
250 µm.
250 µm 250 µm
250 µm 250 µm

74
Chapter 5
75
Mechanism of bone incorporation of ß-TCP bone substitute in open wedge tibial osteotomy in patients
always associated with red or dark green material in-between the ß-TCP granules in the
goldner sections. Apparently these mononuclear cells were osteoblasts that start to
produce osteoid that subsequently mineralises the micropores in the ß-TCP material.
Occasionally, in the same locations, multinuclear TRAP positive osteoclasts penetrated
into the micropores around the ß-TCP granules and start to resorb the ß-TCP (Fig. 4a, b).
More close to the osteotomy side more bone apposition in the pores is found.
Occasionally the pores are completely filled with bone (Fig 3d). Locally abundant
osteoclast activity is present dissolving the ß-TCP remnants by surface erosion
(Fig. 4c, d). The end result of this process is normal looking bone with only sparse
remnants of ß-TCP that are completely incorporated into new vital bone (Fig. 4 e, f).
No macrophages or giant cells were found during or after the incorporation of the ß-TCP.
The mean surface area of active incorporation was 8.53% (± 12.0%) in all specimens.
The surface area of normal looking bone, which contained occasionally only sparse
remnants of ß-TCP was 77.1% (± 21.1%) of the total area of the biopsy. The remaining
tissue is fibrous tissue (13.8% ± 24.1). This means that more then 80% of the surface
area of all biopsies consisted of bone or active incorporating bone. The surface area of
remaining ß-TCP in the regions with incorporated bone was 1.20% (SD 1.98) of the total
measured area. The surface area of bone in the bone region was 22.2% ± 11.6 which
is similar to normal human bone.
Discussion
The most important aim of this study was to compare the incorporation process in
patients with that in animals. Particularly the assessment of bone substitute incorporation
is very difficult on radiographs alone since the distinction between new bone and
biomaterial cannot be made. Therefore histology is the ultimate proof for incorporation
of bone graft replacement materials. As far as we know this is the first report on the
detailed description of the incorporation of ß-TCP in patients. Optimally, evaluation of
biopsy specimens on several time points is necessary to give more insight in the
completeness of bone remodelling, the type of incorporation process and the speed
of biomaterial resorption and incorporation. In the patient population of the present
study biopsies could only be taken after healing of the osteotomy.
In various animal studies in which the incorporation of ß-TCP was studied, it was
described that the resorption of ß-TCP and conversion into bone took place in a
number of distinct phases 16;20. Initially there is some resorption of host bone,
probably due to the surgical trauma. This phase is followed by a phase in which
apposition of bone occurs and the total density of bone plus ß-TCP on X-rays is high.
After about six months, resorption and remodelling of the ß-TCP and new bone takes
place, which decreases the total density again.
Although the biopsies were taken at considerable follow up periods, different aspects
of the incorporation process were found, although not in every specimen. Apparently
the incorporation of the inserted wedge takes a variable and in some cases considerable
time. The variation may be related to patient related variables (e.g. age, smoker or not
smoker), the thickness of the biopsy and differences in local environment (vascularity,
loading). As the first biopsies in this study have only been obtained six months after the
osteotomy, the local variation in incorporation enabled us to study also the first phases
of incorporation.
Figure 4
A. and B. HE (A) and
adjacent TRAP section of
multinuclear osteocalst
penetrating into the TCP.
C. and D. HE (C) and
TRAP (D) section of
surface erosion of TCP by
osteoclasts. E. and F.
HE and Goldner stained
section of remnants of
TCP incorporated into new
bone. Scale bar: 125 µm.
125 µm 125 µm
125 µm 125 µm
125 µm 125 µm

76
Chapter 5
77
Mechanism of bone incorporation of ß-TCP bone substitute in open wedge tibial osteotomy in patients
Firstly there is invasion of fibro-vascular tissue in the large pores of the ß-TCP. Probably
simultaneous to this, there is preferential resorption of the necks linking the ß-TCP
microparticles. This might be caused by a process of chemical dissolution as suggested
by Zerbo et al.29. Next, bone apposition occurs on the inner surface of the large pores
in the ß-TCP. Simultaneously mononuclear osteoblast like cells start to mineralise the
microporous structure between the small ß-TCP agglomerates. This phase is in
animals associated with a sclerosing X-ray appearance. On the X-rays of human ß-TCP
incorporation this phenomenon is found during phase 2 of the radiological evaluation
system 11. Next multinucleated osteoclasts like cells penetrate the ß-TCP and start
resorbing it by a cellular mediated process visible as decreasing ß-TCP wedge density
in phase 3 of the radiological classification. During the whole resorption process
no macrophages or multinucleated giant cells are present confirming the good
biocompatibility of the ß-TCP. In later stages active resorption and bone apposition is
responsible for the conversion of the ß-TCP to healthy normal bone. This phase was
not abundant in our biopsy material because of timing of removal of plate and screws.
This is in general not performed before a phase 4 or 5 on the x-rays. In stage 4 some
of the ß-TCP may be present but in stage 5 the bone looks normal and indeed in the
histology the ß-TCP is then almost totally resorbed. What remains are small spots
of ß-TCP incorporated in bone at locations where no active remodelling takes place
any more.
Eggli et al. described an average incorporation of 45% in the vertebral bodies of apes
at six months and Buser et al. measured almost 70% bone matrix at six months in the
mandibles of piglets 16;23. Stoll et al. studied bone incorporation after 12 weeks into a
ß-TCP implant in a cylindrical defects of 8.5mm in the sheep tibia metaphysic and
found 10% bone ingrowth when the implant was impregnated with fresh blood and
18% when the implant was impregnated with fresh bone marrow 17. In all cases, the
expectation was that a further resorption of ß-TCP and incorporation of bone would
take place. Our study suggests that in human bone this expectation would have been
met. Although the results show a high variation, in general a good resorption of ß-TCP
is seen and after two years even 95% complete incorporation and remodelling of bone.
Concerning the quantification of bone healing used in this study and the variability of
results a few remarks can be made. First, the precise biopsy site is of interest. Because
of the wedge shaped ß-TCP-filled defect, the site where the biopsy has been removed
determines the quantity of ß-TCP and bone seen in the biopsy. Although certain criteria
are involved as to how and where the biopsy has to be taken (Fig.1), it is not possible
to obtain a biopsy from the exact same location in each patient. Also, the difference
in the amount of correction between patients may have influenced the results. A higher
number of degrees of correction means a larger defect that has to be filled and
with that a larger surface area of ß-TCP. Furthermore, the quality of the radiographs
(overexposure versus underexposure) may have influenced its classification. Finally,
smoking may have played a role in bone healing. From several studies, it has been
found that smokers have significantly poorer ( or worse) bone healing than
nonsmokers 30-35. In this study, out of 16 patients, there were 7 smokers. No difference
between smokers and non-smokers could be demonstrated. Due to the fact that this
involves a small study group, no conclusions can be drawn from this, however.
To obtain, as in animal studies, a complete and thorough overview of the process of
resorption of ß-TCP and conversion into bone, biopsies would have to be taken at
earlier points in time (six weeks, three months). In patients, however, the fixation material
can only be removed, without loss of correction, after sufficient bone consolidation.
In this study this was after at least six months and in phase 4 or 5 of the radiological
classification. Only through biopsies taken at specific intervals after the osteotomy, a
complete overview can be obtained. This would mean that the patient has to undergo
a separate intervention with the fixation material still in situ which poses medical-ethical
problems prohibiting a complete overview in the current study structure.
Conclusions
In conclusion, although in only a few biopsies the first stages of incorporation were
present, the overall conclusion is that the incorporation process of ß-TCP in patients
occurs similarly as in animals. The radiological classification system that was
developed correlates with the histological findings. Most of the ß-TCP is resorbed and
completely incorporated and remodelled into new bone. Further research will be
necessary to obtain more detailed information on the various phases incorporation
of ß-TCP in human bone though this will be difficult concerning the medical and
ethical limitations.

78
Chapter 5
79
Mechanism of bone incorporation of ß-TCP bone substitute in open wedge tibial osteotomy in patients
Acknowledgements
The authors would like to thank Thierry Stoll, Synthes Biomaterials in Bettlach,
Switzerland, for the development and preparation of the ceramic implants and the
support of the study.
References
1. Amendola A. Unicompartmental osteoarthritis in the active patient: the role of high tibial osteotomy.
Arthroscopy 2003;19 Suppl 1:109-116.
2. Gaasbeek RD, Welsing RT, Verdonschot N, Rijnberg WJ, van Loon CJ, van Kampen A. Accuracy
and initial stability of open- and closed-wedge high tibial osteotomy: a cadaveric RSA study.
Knee Surg Sports Traumatol Arthrosc 2005;Nov;13(8):689-694.
3. Scott WN, Clarke HD. The role of osteotomy 2003: defining the niche. Orthopedics 2004;27:975-976.
4. Virolainen P, Aro HT. High tibial osteotomy for the treatment of osteoarthritis of the knee: a review of
the literature and a meta-analysis of follow-up studies. Arch Orthop Trauma Surg 2004;124:258-261.
5. Aglietti P, Buzzi R, Vena LM, Baldini A, Mondaini A. High tibial valgus osteotomy for medial
gonarthrosis: a 10- to 21-year study. J Knee Surg 2003;16:21-26.
6. Hernigou P, Medevielle D, Debeyre J, Goutallier D. Proximal tibial osteotomy for osteoarthritis with
varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354.
7. Ivarsson I, Myrnerts R, Gillquist J. High tibial osteotomy for medial osteoarthritis of the knee.
A 5 to 7 and 11 year follow-up. J Bone Joint Surg Br 1990;72:238-244.
8 Magyar G, ToksvigLarsen S, Lindstrand A. Open wedge tibial osteotomy by callus distraction in
gonarthrosis: Operative technique and early results in 36 patients. Acta Orthop Scand 1998;69:147-151.
9. Brouwer R, Jakma T, Bierma-Zeinstra S, Verhagen A, Verhaar
J. Osteotomy for treating knee osteoarthritis. Cochrane Database Syst Rev 2005;CD004019.
10. Koshino T, Yoshida T, Ara Y, Saito I, Saito T. Fifteen to twenty-eight years’ follow-up results of high
tibial valgus osteotomy for osteoarthritic knee. Knee 2004;11:439-444.
11. van Hemert WL, Willems K, Anderson PG, van Heerwaarden RJ, Wymenga AB. Tricalcium
phosphate granules or rigid wedge preforms in open wedge high tibial osteotomy: a radiological
study with a new evaluation system. Knee 2004;11:451-456.
12. Amendola A, Fowler PJ, Litchfield R, Kirkley S, Clatworthy M. Opening wedge high tibial osteotomy
using a novel technique: early results and complications. J Knee Surg 2004;17:164-169.
13. Koshino T, Murase T, Saito T. Medial opening-wedge high tibial osteotomy with use of porous
hydroxyapatite to treat medial compartment osteoarthritis of the knee. J Bone Joint Surg Am
2003;85A:78-85.
14. Hernigou P, Ma W. Open wedge tibial osteotomy with acrylic bone cement as bone substitute.
Knee 2001;8:103-110.
15. Koshino T, Murase T, Takagi T, Saito T. New bone formation around porous hydroxyapatite wedge
implanted in opening wedge high tibial osteotomy in patients with osteoarthritis. Biomaterials
2001;22:1579-1582.

80
Chapter 5
81
Mechanism of bone incorporation of ß-TCP bone substitute in open wedge tibial osteotomy in patients
16. Buser D, Hoffmann B, Bernard JP, Lussi A, Mettler D, Schenk RK. Evaluation of filling materials in
membrane--protected bone defects. A comparative histomorphometric study in the mandible of
miniature pigs. Clin Oral Implants Res 1998;9:137-150.
17. Stoll T MOMTBS. New aspects in osteoinduction. Mat -wiss u Werkstofftech 2004;35:198-202.
18. LeGeros RZ. Properties of osteoconductive biomaterials: calcium phosphates. Clin Orthop 2002;81-98.
19. Eid K, Zelicof S, Perona BP, Sledge CB, Glowacki J. Tissue reactions to particles of bone-substitute
materials in intraosseous and heterotopic sites in rats: discrimination of osteoinduction,
osteocompatibility, and inflammation. J Orthop Res 2001;19:962-969.
20. Steffen T, Stoll T, Arvinte T, Schenk RK. Porous tricalcium phosphate and transforming growth factor
used for anterior spine surgery. Eur Spine J 2001;10 Suppl 2:S132-40.:S132-S140.
21. Bohner M. Calcium orthophosphates in medicine: from ceramics to calcium phosphate cements.
Injury 2000;31 Suppl 4:37-47.:37-47.
22. Bohner, M., van Lenthe, G. H., Grünenfelder, S., Hirsiger, W., Evison, R., and Müller, R. Synthesis
and characterization of porous b -tricalcium phosphate blocks. Accepted
Biomaterials March 2005. Ref Type: Generic
23. Eggli PS, Muller W, Schenk RK. Porous hydroxyapatite and tricalcium phosphate cylinders with
two different pore size ranges implanted in the cancellous bone of rabbits. A comparative
histomorphometric and histologic study of bony ingrowth and implant substitution.
Clin Orthop 1988;127-138.
24. Ogose A, Hotta T, Hatano H et al. Histological examination of beta-tricalcium phosphate graft in
human femur. J Biomed Mater Res 2002;63:601-604.
25. Chazono M, Tanaka T, Komaki H, Fujii K. Bone formation and bioresorption after implantation
of injectable beta-tricalcium phosphate granules-hyaluronate complex in rabbit bone defects.
J Biomed Mater Res 2004;70A:542-549.
26. Artzi Z, Weinreb M, Givol N et al. Biomaterial resorption rate and healing site morphology of
inorganic bovine bone and beta-tricalcium phosphate in the canine: a 24-month longitudinal
histologic study and morphometric analysis. Int J Oral Maxillofac Implants 2004;19:357-368.
27. Kovacs K, Velich N, Huszar T et al. Comparative study of beta-tricalcium phosphate mixed with
platelet-rich plasma versus beta-tricalcium phosphate, a bone substitute material in dentistry.
Acta Vet Hung 2003;51:475-484.
28. Wiltfang J, Merten HA, Schlegel KA et al. Degradation characteristics of alpha and beta
tri-calcium-phosphate (TCP) in minipigs. J Biomed Mater Res 2002;63:115-121.
29. Zerbo IR, Bronckers AL, de Lange G, Burger EH. Localisation of osteogenic and osteoclastic cells
in porous beta-tricalcium phosphate particles used for human maxillary sinus floor elevation.
Biomaterials 2005;26:1445-1451.
30. De Bruyn H, Collaert B. The effect of smoking on early implant failure.
Clin Oral Implants Res 1994;5:260-264.
31. Schwartz-Arad D, Samet N, Samet N, Mamlider A. Smoking and complications of endosseous
dental implants. J Periodontol 2002;73:153-157.
32. Wallace RH. The relationship between cigarette smoking and dental implant failure.
Eur J Prosthodont Restor Dent 2000;8:103-106.
33. Gullihorn L, Karpman R, Lippiello L. Differential effects of nicotine and smoke condensate on
bone cell metabolic activity. J Orthop Trauma 2005;19:17-22.
34. Stavropoulos A, Mardas N, Herrero F, Karring T. Smoking affects the outcome of guided tissue
regeneration with bioresorbable membranes: a retrospective analysis of intrabony defects.
J Clin Periodontol 2004;31:945-950.
35. Dahl A, Toksvig-Larsen S. Cigarette smoking delays bone healing: a prospective study of
200 patients operated on by the hemicallotasis technique. Acta Orthop Scand 2004;75:347-351.

82
chapter 6The influence of open and closed high tibial
osteotomy on dynamic patellar tracking
A biomechanical study
R. D. A. Gaasbeek, R. T. C. Welsing, M. Barink, N. Verdonschot, A. van Kampen
Knee Surg Sports Traumatol Arthrosc 2007 May 5; [Epub ahead of print].

84
Chapter 6
85
The influence of open and closed high tibial osteotomy on dynamic patellar tracking; a biomechanical study
Abstract
High tibial osteotomy (HTO) can cause alterations in patellar height, depending on
the surgical technique, the amount of correction and the postoperative management.
Alterations in patella location after HTO may lead to post-operative complications.
However, information on changes in dynamic patellar kinematics following HTO is
very limited.
We conducted a biomechanical study, to analyze the effect of open (OWO) and closed
wedge osteotomy (CWO) on patellar tracking. Using an inventive experimental set-up,
we studied the 3D dynamic patellar tracking in ten cadaver knees before and after
valgus HTO. In each specimen, corrections of 7º and 15º of valgus according to, both,
the OWO and CWO technique, were performed.
Patellar height significantly increased with CWO and decreased with OWO. Both, OWO
and CWO led to significant changes in the patellar tracking parameters tilt and rotation.
We also found significant differences between OWO and CWO. Valgus high tibial
osteotomy increased the medial patellar tilt and reduced the medial patellar rotation.
These effects were more profound after OWO. No significant differences were found
for the effect on medial-lateral patellar translation. These observations can be taken
into consideration in the decision whether to perform an OWO or a CWO in a patient
with medial compartment osteoarthritis of the knee.
Introduction
Young active patients suffering from medial compartment osteoarthritis of the knee with
a varus alignment can be treated with a high tibial osteotomy (HTO). Depending on the
surgical technique and postoperative management, alterations in patellar height can be
induced 1-7. Open wedge osteotomy (OWO) proximal to the tibial tuberosity, which is
gaining popularity in recent years, has been reported to cause patella baja 3;7. Closed
wedge osteotomy (CWO) has been shown to lead to both patella baja and alta 3;8.
These alterations in patellar height have been attributed to the proximalisation (CWO)
or distalisation (OWO) of the tibial tuberosity following HTO7. Furthermore, scarring,
adhesions and contracture of the patella ligament are mentioned to cause lowering of
the patella in CWO 5. Besides these changes in patellar height, other components of
patellar tracking may be affected by HTO. This may cause anterior knee pain, patella
locking, crepitus and limitation of knee motion. Eventually, the altered patellofemoral
congruency and contact stress may lead to patellofemoral osteoarthritis. Furthermore,
there is evidence that patellar height may affect the outcome of total knee arthroplasty
9;10. Conversely, pre-existing patellofemoral symptoms may diminish following HTO 11.
Former studies on the effect of HTO on the patellofemoral joint focus on the standard
plain radiographic measurements of patellar height at one position of knee flexion 1;8.
Furthermore, previous studies in this field restrict the dynamic patellar tracking to a
range of static measurements of the patella position in a few fixed positions of knee
flexion 12;13. As far as the authors are aware of, no study has been reported that
describes the true dynamic patellar tracking following HTO. The present study was
conducted to analyse the changes in dynamic patellar tracking after both, OWO
and CWO.
Materials and Methods
Specimens
Ten fresh frozen cadaver knees were obtained. Degenerative changes and dysplasias
were evaluated and excluded based on standard AP, lateral and patella radiographs.
The specimens were prepared for use in a knee joint motion and loading apparatus 14.

86
Chapter 6
87
The influence of open and closed high tibial osteotomy on dynamic patellar tracking; a biomechanical study
Therefore, tibia and femur were transsectioned at about 20 cm from the knee joint
centre. The ends of the bones were potted in autopolymer which guaranteed identical
positioning during the different surgeries and measurements. All soft tissues were
preserved. The quadriceps muscle was separated in three parts: rectus femoris, vastus
medialis, and vastus lateralis/intermedius. Three mounting plates were rigidly fixed to
the femur, tibia and patella, respectively, which enabled the registration of the bony
segments visible on the CT scans to the global coordinate system. Hereafter, CT scans
of all knees were obtained.
Experimental set up
A specially designed metal frame with hinges on the medial and lateral side was put
on the tibia under fluoroscopic view. This frame was designed such that the position of
the hinges coincided with the planned rotation point (the apex) of the osteotomy.
The frame allowed a free moving distal part of the tibia. In this way, different valgus
angles within the same specimen could be simulated. The tibia positions could be
set at a predetermined angle.
After this, the specimen was positioned in the loading apparatus. An electromagnetic
motion tracking system (3SPACE Fastrak, Polhemus, Colchester, VT, USA) was used to
measure the patello-femoral and tibio-femoral kinematics of the knee. Three sensors
were fixed rigidly to the mounting plates on femur, tibia and patella. The kinematics
were recorded using continuous data acquisition. The three separated parts of the
quadriceps muscle were loaded with 27 N each and an additional 50 N axial
compressive load was applied to the knee, according to an earlier published protocol 14;15.
For the first reference measurement, three flexion-extension movements were
performed manually. Next, a standard anterolateral approach was used. Two centimetres
below and parallel to the joint line a Kirschner wire was inserted to aim the osteotomy.
First, the proximal cut was performed. Using an aiming device the distal cut was made
and a 15º bony wedge was removed proximal to the tibial tuberosity. The fibula was
cut, according to the closed wedge HTO technique of Coventry 16.
The knee was put back into the loading apparatus and the measurements were
repeated in three different positions of the distal tibia: neutral (Fig. 1a), 7º and 15º
valgus (lateral closed wedge) position (Fig. 1b).
After this, a medial approach was performed, shifting the pes anserinus and the
superficial medial collateral ligament dorsally. A Kirschner wire was inserted parallel to
the joint line. Using a guide instrument a second wire was inserted just proximal of the
tuberosity in lateral cranial direction in order to obtain an equal osteotomy level in all
knees. Along this wire the osteotomy was performed.
Hereafter, flexion-extension cycles were recorded in neutral, 7º and 15º valgus (medial
open wedge) position (Fig. 1c). All correction angles were checked with an electronic
inclinometer (Cybex, EDI 320). The surgery was performed under fluoroscopic view.
Data analysis
After the recordings were made, the Fastrak motion data were analysed and combined
with the CT-scanning data. The 3D motion data, which were measured in the global
coordinate system, were transformed to anatomic coordinates. The anatomic coordinate
systems were based on bony landmarks which were retrieved from the CT scan
contours 17. In this way, a 3D dynamic model of each knee was constructed with a local
anatomic coordinate system. As the patellar kinematics are also largely dependent on
the tibial movements the tibial kinematics were also measured. The calculated patellar
tracking parameters were: patellar height, tilt, rotation, and lateral-medial translation
(For definition of parameters see fig 2). To quantify the impact of the HTO for
each of the parameters, the differences of the patellar kinematics after HTO minus the
reference patellar kinematics of the neutral measurements were calculated.
Figure 1
Schematic presentation of the tibia positioned in the specially designed frame which enabled
testing of different valgus angles within the same specimen. A. neutral, B. valgus closed
wedge(7º and 15º) and C. valgus open wedge (7º and 15º).
A B C

88
Chapter 6
89
The influence of open and closed high tibial osteotomy on dynamic patellar tracking; a biomechanical study
Statistics
The three reference measurements in neutral position were compared using a
Two-way ANOVA. The differences between the four groups, e.g. 7º and 15º lateral
closed wedge, and 7º and 15º medial open wedge, were analyzed by using a Two-way
ANOVA at every subsequent flexion step of 5º up to maximal knee flexion angle of
100º. To assess whether each group was statistically different from the non-operated
situation, we calculated whether the difference of the two measurements (intact minus
operated) was different from zero by calculating if the value zero was within the outcome
of the 95% confidence interval. Significance was set at p < 0.05.
Results
In general, the movement patterns of the patella in the non-operated knees were similar
to what clinically can be expected and is described by van Kampen and Huiskes 15.
Typical examples of the effects of HTO on patellar tilt and rotation in one of the specimen
are shown in figures 3a and b, respectively. The group results are graphically displayed
in figures 4a-d. They represent the change of patellar kinematics caused by the HTO,
not the absolute values.
Patellar height
As expected, larger tibial correction angles induced more patellar height changes
(Fig. 4a). The OWO resulted in significant lowering of the patella. Larger corrections in
the OWO group caused significant more patella lowering, whereas more correction
in the CWO group resulted in more increase in patellar height. The change of patellar
height was not related to the knee flexion. Hence, during knee flexion the position
of the patella in relation to the tibia was rather constant, which resulted in horizontal
curves. The mean decrease of patellar height following 7º OWO was 1.5 mm (range
0.7;1.7) which significantly increased to 4.2 mm (range 2.7;4.6) at 15º OWO.
The patellar height after 7º CWO increased on average with 2.2 mm (range 1.1;2.7).
At 15º CWO the mean increase was 3.0 mm (range 2.1;3.6). Figure 5 shows a schematic
presentation of the patellar height changes after open an closed wedge osteotomy.
Patellar tilt
A typical example of the effects of HTO on the patellar tilt is shown in figure 3a.
On average, OWO and CWO caused the patella to tilt more medially (Fig. 4b). A trend
was seen of more medial tilt with OWO than with CWO. Along the flexion-extension
movement we found no significant difference between CWO and OWO at 7º correction,
but during the first half of flexion significant differences were found between CWO and
Figure 2
Defenition of patellar movements.
Figure 3
Typical examples of the
effects of HTO on the
patellar tilt (a) and rotation
(b) of one specimen.
Ref : Reference curve of
neutral measurement.
Patellar Tilt
-6
-5
-4
-3
-2
-1
0
1
2
3
4
0 20 40 60 80 100
Knee Flexion (deg)
Pate
lla T
ilt (d
eg)
Medial
Lateral
Patellar Rotation
-5
-4
-3
-2
-1
0
0 20 60 80 100
Knee Flexion (deg)
Pate
lla R
otat
ion
(deg
)
Medial
Lateral40
Ref7 deg CWO15 deg CWO7 deg OWO15 deg OWO
a
b

90
Chapter 6
91
The influence of open and closed high tibial osteotomy on dynamic patellar tracking; a biomechanical study
OWO with a 15º correction. OWO caused the patella to tilt more medially in extension
and showed a decrease in additional medial tilt while the knee was brought in flexion.
With increasing flexion the difference in medial tilt between the two HTO groups
decreased. All groups showed to be significant different from zero. The mean increase
of medial tilt following 7º OWO was 1.7º (range 0.3; 4.8) which increased to 2.9º
(range 1.8; 6.2) at 15º OWO. The mean medial patellar tilt after 7º CWO increased with
0.7º (range 0.0; 0.9). At 15º CWO the mean increase was 0.5º (range -0.3; 0.7)
Patellar rotation
A typical example of the effects of HTO on the patellar rotation is shown in figure 3b.
Both, OWO and CWO reduced the normal medial rotation of the patella along the flexion
movement of the knee. In general, OWO showed significant more reduction of medial
rotation than CWO (Fig. 4c). No statistical difference between CWO and OWO with
7º correction was found around the area in the curves where the two lines cross.
At 7º OWO correction, the reduction of the medial rotation declined with increased
flexion of the knee. In full flexion this group showed a small increase of medial rotation
of the patella. Increasing the correction angle from 7º to 15º resulted in a significant
reduction of medial rotation and in some specimen lateral rotation was induced.
Figure 4
Averaged group patellar
kinematics: patellar height
(a), patellar tilt (b), patellar
rotation (c) and patellar
medial-lateral translation
(d). The data represent
the change of patellar
tracking parameters
caused by the different
HTO techniques, not the
absolute values.
Because of clarity
standard deviations are
not shown.
-10
-8
-6
-4
-2
0
2
4
6
0 20 40 60 80 100
-8
-6
-4
-2
0
2
4
0 20 40 60 80 100
-10 -8 -6 -4 -2 0 2 4 6 8
0 20 40 60 80 100
-1,5
-1
-0,5
0
0,5
1
1,5
2
2,5
3
3,5
0 20 40 60 80 100 -
Ref7 deg CWO15 deg CWO7 deg OWO15 deg OWO
Patellar Height
Knee Flexion (deg)
Pate
lla H
eigh
t (m
m)
Low
High
Patellar Tilt
Knee Flexion (deg)
Pate
llar T
ilt (d
eg)
Medial
Lateral
Patellar Rotation
Knee Flexion (deg)
Pate
llar R
otat
ion
(deg
)
Medial
Lateral
Patellar medial-lateral Translation
Knee Flexion (deg)
Med
ial-l
ater
al T
rans
latio
n (m
m)
Medial
Lateral
a
b
c
d
Figure 5
Schematic presentation of the changes in patellar height after high tibial osteotomy.
a. preoperative, b. lowering of the patella after open wedge osteotomy and c. increased
patellar height after closed wedge osteotomy.

92
Chapter 6
93
The influence of open and closed high tibial osteotomy on dynamic patellar tracking; a biomechanical study
No significant difference was found between CWO 7 and 15º. During the first half of
flexion movement the effect of CWO on the patellar rotation was not significantly
different from zero, and this was also seen for the 7ºof correction with OWO near full
extension. The mean reduction of medial rotation following 7º OWO was 1.6º
(range -0.6; 2.8) which increased to 5.2º (range 4.7; 5.5) at 15º OWO. The mean
medial rotation after 7º CWO decreased with 1.2º (range -0.1; 1.9). At 15º CWO
the mean reduction was 1.1º (range 0.0-1.9).
Patellar medial-lateral translation
We found a poor reproducibility of the differences in medial-lateral patellar translation
leading to high standard deviations. No significant differences were found between
groups in medial or lateral translation of the patella (p > 0.05). Also, all calculated
effects were not different from the reference patellar tracking pattern. (Fig. 4d).
Discussion
Previous observations of patellar height after HTO concern either the closed wedge or
the open wedge technique. To our knowledge, only three studies analyzed the effects
on patellar height in OWO versus CWO. Tigani et al. used Caton’s Index (CI) and
showed lowering of the patella more often with OWO than with CWO and a high degree
of patella proximalisation in the latter 6. Brouwer et al. found more patellar lowering after
an open wedge HTO. They applied both the Insall Salvati (ISI) and the Blackburne-Peel
Index (BPI) 1. Hoell et al. measured patellar height change with the ISI and found no
difference between OWO and CWO 18. However, this does not exclude a true change of
patellar height in relation to the joint line, as the ISI represents the length of the patellar
tendon. Furthermore, BPI and CI do not accurately measure the alteration of patellar
height after valgus HTO, because they are dependent of the tibial inclination and the
antero-posterior translation of the proximal tibia 8. The present study has the advantage
of continuous 3D monitoring of the patella movements, without the limitations of the
measurements of patellar height on plain roentgen films. We found a significant
increase in patellar height after CWO and a significant lowering of the patella after
OWO. These height changes were dependent on the amount of correction and more
profound after OWO as compared to CWO (Fig. 4a). Concerning the biomechanics of
the patella movement in relation to its anatomical position contradictory information in
literature is found. Investigations of the mechanics of patella baja have found that a
low-riding patella does not necessarily lead to an increase in patellofemoral contact
forces 19;20. However, others report an increase in patellofemoral joint reaction force as
a result of adhesions of the patella ligament 7.
During surgery we observed that the proximal translation after CWO was limited by
the medial and lateral retinaculum to such extend that the patellar tendon relaxed and
curled up. This phenomenon might well be one of the factors that lead to shortening
and adhesions of the patellar tendon that is reported after CWO 5.
Weidenhielm et al. reported on seven patients before and after CWO using kinematic
analysis with roentgen stereophotogrammetric analysis (RSA). They found no significant
change in patellar rotation and translation during knee motion, with inconsistent
changes in patella position 13. However, they were not informed about quadriceps
tension nor did they correct for relaxation or contraction of the quadriceps muscles
during the RSA measurements. This might have been a large confounder in their study.
During flexion of the knee, until the patella is well seated, its stability rests solely on
muscle tension. Hungerford et al. stated that the congruence of the patellofemoral joint
and the muscles forces provide considerable stability irrespective of restraining
ligaments 21. Because of this we applied a constant load to the quadriceps muscle
during our experiments (See Material and Methods). Hill et al. used magnetic resonance
imaging to measure patellofemoral kinematics through a range of loaded flexion before
and after CWO in 4 patients.
They found a decrease in patella flexion and internal spin (‘medial rotation’ in this
study), and an increase in medial patellar tilt and proximal translation 12. Although this
study represents a “semi-dynamic” setting, our results corroborate with their findings.
We found that valgus osteotomy increased the medial tilt and reduced the medial
patellar rotation. These effects were more profound after OWO. The increased medial
patellar tilt can be explained by the increased lateral pull on the patella. The tuberosity
is located more laterally after valgus high tibial osteotomy. The lateral patellar facet is
pressed against the lateral wall of the trochlea and the patella is forced up the lateral
groove leading to a medial tilt. As the quadriceps tendon remains to have the same
loading direction, the lateralization of the tuberosity induces lateral rotation (reduction of
medial rotation). Theoretically, the effect on the patellar medial-lateral translation is larger

94
Chapter 6
95
The influence of open and closed high tibial osteotomy on dynamic patellar tracking; a biomechanical study
near full extension of the knee. During flexion the patella enters the trochlear groove
which will enhance medial-lateral stability. Furthermore, there is a relatively high variation
in patellar position in the lower range of flexion. These phenomena may explain why no
significant differences in patellar translation could be detected. Furthermore, during our
experiments we observed that OWO, led to more tension on the patella ligament and
the retinaculi in contrast to the closed wedge osteotomies, in which we observed a
relative relaxation of the patellar tendon. This may explain why more effect of the HTO
was observed in the OWO group. It seemed that the distalisation and increased tension
following OWO, enhances the forces at the patellofemoral joint, leading to more obvious
effects on the patellar tracking. If these effects are unwanted, a different operation
technique has been described recently, to prevent the distalisation of the tibial tuberosity
with OWO by performing a distal tuberosity osteotomy 3.
To our knowledge, the current paper is the first to describe the continuous 3D patellar
tracking changes following HTO, according to both the CWO as the OWO technique.
This study clearly shows the evident influence of HTO on patellar position and the
patellofemoral movements. The effects of OWO proof to be more profound than those
following CWO, especially at larger valgus corrections of the tibia. These effects of HTO
on patellar height and patellar tracking may be of minimal clinical relevance but in
extensive open wedge corrections the effects may be quite large and lead to adverse
events with respect to the patellofemoral joint (e.g. pain, maltracking or even patellar
(sub)luxation). On the other hand, patellofemoral complaints may subside after high
tibial osteotomy.
In conclusion, the decision whether a closed or an open wedge technique is performed,
for the treatment of patients suffering from medial osteoarthritis of the knee, the
presence of patellofemoral complaints or pre-existent patella baja should be taken into
consideration. Especially in large open wedge corrections significant changes in
patellar height and tracking can be induced. In the future, the effect of the kinematic
changes in the patellofemoral joint after high tibial osteotomy in terms of clinical
presentation and radiographic changes after long term follow-up have to be determined.
Reference List
1. Brouwer RW, Bierma-Zeinstra SM, van Koeveringe AJ, Verhaar JA. Patellar height and the inclination
of the tibial plateau after high tibial osteotomy. The open versus the closed-wedge technique.
J Bone Joint Surg Br 2005;87:1227-1232.
2. Closkey RF, Windsor RE. Alterations in the patella after a high tibial or distal femoral osteotomy.
Clin Orthop 2001;51-56.
3. Gaasbeek RD, Sonneveld H, van Heerwaarden RJ, Jacobs WC, Wymenga AB. Distal tuberosity
osteotomy in open wedge high tibial osteotomy can prevent patella infera: a new technique.
Knee 2004;11:457-461.
4. Kaper BP, Bourne RB, Rorabeck CH, Macdonald SJ. Patellar infera after high tibial osteotomy.
J arthroplasty 2001;16:168-173.
5. Scuderi GR, Windsor RE, Insall JN. Observations on patellar height after proximal tibial osteotomy.
J Bone Joint Surg Am 1989;71:245-248.
6. Tigani D, Ferrari D, Trentani P, Barbanti-Brodano G, Trentani F. Patellar height after high tibial
osteotomy. Int Orthop 2001;24:331-334.
7. Wright JM, Heavrin B, Begg M, Sakyrd G, Sterett W. Observations on patellar height following
opening wedge proximal tibial osteotomy. Am J Knee Surg 2001;14:163-173.
8. Kesmezacar H, Erginer R, Ogut T, Seyahi A, Babacan M, Tenekecioglu Y. Evaluation of patellar
height and measurement methods after valgus high tibial osteotomy.
Knee Surg Sports Traumatol Arthrosc 2005.
9. Figgie HE, III, Goldberg VM, Heiple KG, Moller HS, III, Gordon NH. The influence of tibial-
patellofemoral location on function of the knee in patients with the posterior stabilized condylar
knee prosthesis. J Bone Joint Surg Am 1986;68:1035-1040.
10. Windsor RE, Insall JN, Vince KG. Technical considerations of total knee arthroplasty after proximal
tibial osteotomy. J Bone Joint Surg Am 1988;70:547-555.
11. Goutallier D, Delepine G, Debeyre J. [The patello-femoral joint in osteoarthritis of the knee with
genu varum (author’s transl)]. Rev Chir Orthop Reparatrice Appar Mot 1979;65:25-31.
12. Hill NA, Fellows RA, MacIntyre NJ, Harrison MM, Ellis RE, Wilson DR. The effect of high tibial
osteotomy on three-dimensinal tibiofemoral and patellofemoral kinematics: an in vivi study using
magnetic resonance imaging. Proc 51st ORS Conference 2005;0481.
13. Weidenhielm L, Wykman A, Lundberg A, Brostrom LA. Knee motion after tibial osteotomy for
arthrosis. Kinematic analysis of 7 patients. Acta Orthop Scand 1993;64:317-319.

96
Chapter 6
14. Van Heerwaarden, H. J. Effects of pretension in reconstructions of the anterior cruciate ligament;
clinical, biomechanical and computer model analysis. 1998. University of Nijmegen.
1998. Ref Type: Thesis/Dissertation
15. van Kampen A, Huiskes R. The three-dimensional tracking pattern of the human patella.
J Orthop Res 1990;8:372-382.
16. Coventry MB. Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee.
a preliminary report. J Bone Joint Surg Am 1965;47:984-90.:984-990.
17. Barink M, Meijerink H, Verdonschot N, van Kampen A, de Waal MM. Asymmetrical total knee
arthroplasty does not improve patella tracking: a study without patella resurfacing.
Knee Surg Sports Traumatol Arthrosc 2006.
18. Hoell S, Suttmoeller J, Stoll V, Fuchs S, Gosheger G. The high tibial osteotomy, open versus closed
wedge, a comparison of methods in 108 patients. Arch Orthop Trauma Surg 2005;125:638-643.
19. Meyer SA, Brown TD, Pedersen DR, Albright JP. Retropatellar contact stress in simulated patella
infera. Am J Knee Surg 1997;10:129-138.
20. Singerman R, Davy DT, Goldberg VM. Effects of patella alta and patella infera on patellofemoral
contact forces. J Biomech 1994;27:1059-1065.
21. Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Relat Res 1979;9-15.
chapter 7Distal tuberosity osteotomy in open wedge
high tibial osteotomy can prevent patella infera;
a new technique
R.D.A. Gaasbeek, H. Sonneveld, R.J. van Heerwaarden, W.C.H. Jacobs, A.B. Wymenga
Knee. 2004 Dec;11(6):457-6

98
Chapter 7
99
Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera; a new technique
Abstract
To prevent patella infera in open wedge high tibial osteotomy, a new operation technique
was developed. Instead of a proximal tibial tuberosity osteotomy, a distal osteotomy
was performed and the tuberosity was fixed with one screw to the tibia. First experiences
in 17 patients were evaluated and compared with results of 20 patients with open wedge
high tibial osteotomy with proximal tuberosity osteotomy. Distal tuberosity osteotomy in
open wedge high tibial osteotomy appears effective in preventing patella infera.
Introduction
In medial open wedge high tibial osteotomy (OWHTO) for valgus correction of medial
compartment osteoarthritis of the knee the patellar height may change resulting in
postoperative patella infera 1,2,3. A decrease in patellar height associated with OWHTO
has been attributed to distalisation of the tuberosity as a result of valgisation and to
shortening of the patellar ligament by scarring 1,3,4. Reduced patellar height can be the
cause of patellofemoral problems and may complicate a conversion to total knee
replacement in progressive arthritis of the knee 2,3,5,6.
A new operation technique was developed by one of the authors (AW) to prevent
distalisation of the tuberosity and subsequently prevent patellofemoral problems.
In the normal OWHTO technique the tuberosity remains attached to the distal part of
the tibia by performing a proximal tuberosity osteotomy (PTO) or by positioning the
osteotomy above the level of the tuberosity. In our newly developed technique we
perform a distal tuberosity osteotomy (DTO) so the tuberosity remains attached to
the proximal part of the tibia. Opening of the wedge will not change the position of the
tuberosity and consequently, there will be less change of patellar height. The purpose of
this report is to describe a new operation technique: a distal tuberosity osteotomy in open
wedge high tibial osteotomy and to evaluate our first experiences in clinical practice.
Figure 1
OWHTO with PTO, leading to lowering of the patella. a: before opening of the wedge,
AP-view; b: after opening of the wedge, AP-view; c: after opening, lateral view

100
Chapter 7
101
Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera; a new technique
Materials and Methods
Operation techniques:
Previous OWHTO technique with proximal tuberosity osteotomy
Through a midline incision, the tibial tuberosity and distal part of the patellar tendon is
exposed. Starting posterior to the patellar tendon insertion, a PTO is performed: an
osteotomy of the proximal tuberosity parallel to the anterior tibial cortex. After that, the
tibial osteotomy is made behind the tuberosity, which is protected by an angular blade.
Opening of the tibial osteotomy causes the tuberosity to move distally as it is attached
to the distal part of the tibia (figure 1).
New OWHTO technique with distal tuberosity osteotomy
In the new technique we perform a DTO, so the tuberosity remains attached to the
proximal part of the tibia. Therefore, the patellar height is not changed after opening of
the tibial osteotomy (figure 2). In contrast to the previous technique, first, the tibial
osteotomy is made leaving at least a 1 cm thickness of the tuberosity. After that, the
tuberosity osteotomy is performed posterior to the tuberosity. Starting from the tibial
osteotomy the tuberosity is cut distally in the frontal plane directed towards the anterior
tibial cortex. The length of the osteotomized tuberosity should be at least 2.5 cm for
small valgus corrections. In larger corrections the tuberosity length must be longer and
should be planned to at least overlap the distal tibial part for 2.0 cm after the wedge is
opened. After medial plate fixation of the tibial osteotomy, we fixate the distal part of
the tuberosity with a bicortical screw to the tibia. As a stable fixation is reached the
postoperative rehabilitation protocol for the OWHTO needs no adjustments due to the
new technique.
Figure 2
OWHTO with DTO, leaving the patellar height unchanged. a: before opening of the wedge,
AP-view; b: after opening of the wedge, AP-view; c: after opening, lateral view
Table 1
Data of patients with OWHTO with distal tuberosity osteotomy. Correction angle, pre- and
postoperative Caton index (CI) and change of CI (Δ-CI).
Nr Male/Female Age Correction Pre-CI Post-CI Δ-CI
1 m 41 9 0.78 0.82 0.03
2 m 27 10 0.72 0.72 0.00
3 m 51 15 0.74 0.68 -0.05
4 m 41 6 0.75 0.78 0.03
5 m 42 7 0.85 0.83 -0.03
6 m 46 10 0.97 0.87 -0.11
7 m 62 9 0.87 0.79 0.01
8 f 42 10 0.59 0.56 -0.03
9 m 59 10 1.00 0.97 -0.03
10 m 44 15 0.85 0.83 -0.02
11 m 64 13 0.79 0.76 -0.03
12 m 37 12 0.90 0.87 -0.03
13 f 53 14 0.67 0.64 -0.03
14 m 48 7 0.73 0.73 0.00
15 m 54 8 0.80 0.80 0.00
16 m 61 10 0.94 0.91 -0.03
17 m 48 7 0.74 0.74 0.00
Mean(SD) 48(10) 10(2.8) 0.80(0.11) 0.78(0.10) -0.02(0.03)

102
Chapter 7
103
Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera; a new technique
Patient evaluation:
Between March 2001 and October 2002, seventeen consecutive patients operated
according to the new OWHTO technique with the DTO were included for the study.
An historical control group was formed from all patients operated upon from
June 2000. The only selection criteria was presence of a suitable pre-operative lateral
radiograph in 30º of flexion. All patients in this group were operated according to
the routine operation technique, with the PTO.
The tibial osteotomy was fixed by a Tomofix plate (Mathys Medical, Bettlach) after filling
of the wedge with tri-calcium phosphate (ChronOS-Mathys Medical Ltd). The patients
in both groups suffered from medial compartment osteoarthritis of the knee and were
operated by two surgeons (AW and RVH). For details on the demographics see table 1.
Postoperative care consisted of knee flexion and extension exercises starting the day
after the operation. For the first six weeks there was restricted weight bearing (10 kg)
with two crutches and thrombosis prophylaxis with low weight high molecular heparin.
After six weeks full weight bearing was allowed.
For each patient the patellar height was measured by the Caton (-Deschamps) index 7
(CI) on pre- and six weeks postoperative lateral radiographs at 30 degrees of knee
flexion. The CI, the ratio between the distance from the inferior tip of the patella and the
antero-superior angle of the tibia and the patellar articular surface length (figure 3),
decreases with patella baja and increases with patella alta. The normal value of CI is
0.96 (SD 0.13) in males and 0.99 (SD 0.13) in females. The patella is considered low
(patella baja) when CI<0.6 and high (patella alta) when CI>1.32. In the two groups the
pre-operative and post-operative CI was measured and compared using the paired
t-test with p < 0. 05 considered significant.
Figure 3
Calculation of the Caton
(-Deschamps) Index
(CI index). PA is the length
of the articular surface
of the patella; AT is the
distance from the inferior
tip of the patella to the
antero-superior aspect of
the tibia. The CI Index is
calculated as the ratio AT/PA.
Table 2
Data of patients with OWHTO with proximal tuberosity osteotomy. Correction angle, pre- and
postoperative Caton index (CI) and change of CI (Δ-CI).
Nr Male/Female Age Correction Pre-CI Post-CI Δ-CI
18 f 23 5 1.14 1.06 -0.08
19 f 44 7 0.83 0.74 -0.09
20 f 63 10 1.03 0.76 -0.26
21 m 29 8 0.71 0.58 -0.13
22 f 51 7 0.92 0.74 -0.18
23 m 52 7 0.92 0.79 -0.13
24 m 38 3 0.84 0.79 -0.05
25 m 21 9 0.93 0.83 -0.11
26 f 59 5 0.97 0.86 -0.11
27 m 37 8 0.85 0.78 -0.08
28 m 33 9 0.93 0.84 -0.09
29 m 53 10 0.74 0.62 -0.12
30 m 43 8 0.68 0.51 -0.16
31 f 48 13 0.48 0.24 -0.23
32 m 26 6 1.03 0.97 -0.06
33 f 45 7 0.72 0.66 -0.06
34 m 50 14 0.86 0.71 -0.14
35 m 51 14 0.85 0.63 -0.23
36 m 32 12 0.95 0.82 -0.13
37 m 42 10 0.73 0.65 -0.08
Mean(SD) 42(11) 8.6(3.1) 0.86(0.15) 0.73(0.17) -0.13(0.06)

104
Chapter 7
105
Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera; a new technique
Results
Tables 1 and 2 show the calculated pre- and postoperative Caton indices (CI) of the
patients operated with the DTO and the PTO, respectively, together with the OWHTO
correction angles.
In the DTO group (table 1), the patella height was not essentially changed with a mean
preoperative CI of 0.80 (range: 0.59-1.00) and a mean postoperative CI of 0.78
(range: 0.56-0.97). The tuberosity osteotomy was radiographically healed at 6 weeks
postoperative in all but 2 patients. In one patient the tuberosity was fractured during
the tuberosity osteotomy due to a tibial osteotomy leaving less than 1 cm thickness
of the tuberosity. In another patient the tuberosity fixation screw was positioned too
proximal and slightly upward ending posteriorly in the opened wedge. At 6 weeks no
consolidation was found and the screw was repositioned more distally with uneventful
bone healing in 6 weeks. In none of the patients a secondary dislocation of the
tuberosity or the proximal tibia was found after the start of full weight bearing.
In the PTO group (table 2), the patella height decreased significantly (p< 0.001) with
a mean preoperative CI of 0.86 (range: 0.48-1.14) and a mean postoperative CI of 0.73
(range: 0.24-1.06). Bone healing of the tuberosity osteotomy was uneventful and
complete at 6 weeks follow-up in all patients.
In figure 4 the relation between the angle of correction of the OWHTO and the difference
between pre- and post-operative CI (Δ-CI) for both groups is displayed. The mean
correction angle was slightly larger in the DTO group as compared to the PTO group
(10 vs. 8.6 degrees). In the PTO group correction angle and patellar height were found
to be related: the larger the correction angle of the OWHTO the lower the postoperative
patellar height resulting in an increase of Δ-CI with increasing correction angles (figure 4).
Discussion
Open wedge high tibial osteotomy in medial osteoarthritis of the knee has gained a
lot of popularity in recent years. However, the traditional open wedge technique results
in a decrease of patellar height, which may lead to patella infera 2,3,4. Patella infera
following OWHTO causes anterior knee pain, patellar locking, crepitus and limitation of
knee motion. Eventually, the altered patellofemoral congruency and contact stress can
lead to patellofemoral osteoarthritis 8. The new distal tuberosity osteotomy technique
described in this paper encounters this problem. In addition specific difficulties with
conversion of failed HTO with patella infera to total knee arthroplasty 3,5,6 can be prevented.
Decrease of patellar height following OWHTO is mainly caused by the distalisation of
the tuberosity when a PTO is used or the tibial osteotomy is made proximal to the tibial
tuberosity. In those situations a decrease of patellar height is inevitable as was already
shown by Goutallier 8 in a mathematical model. Opening of the osteotomy causes a
distalisation and lateralisation of the tuberosity and the patella. With the OWHTO technique
with a DTO, the tibial tuberosity remains attached to the proximal tibia and opening the
osteotomy will leave patellar height unchanged. Hernigou 4 uses another strategy
to avoid patellar height decrease after OWHTO: positioning of a cement wedge
between the posterior tibial cortices and no wedge anteriorly which results in almost no
heightening of the anterior margin of the osteotomy. However, this technique will likely
lead to unwanted additional tibial slope correction, especially in large valgus corrections.
Furthermore, the decrease of patellar height can be the result of shortening of the
patellar ligament by scarring with adherence of the patellar tendon to the tibia proximal
of the tuberosity insertion 1,3,4. Methods used to avoid scarring of the patellar ligament
include meticulous surgical techniques avoiding large postoperative haematoma’s,
anti-inflammatory medication 9, continuous passive motion with flexion-extension
Figure 4
The relation between
change of Caton index
(Δ-CI) and correction
angles in PTO and DTO,
showing a decrease in CI
at higher correction angles
in the PTO group.
Δ-CI
Correction
DTO
DTO

106
Chapter 7
107
Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera; a new technique
exercises preventing immobilisation 4, and daily manual patella mobilization exercises 3.
Small decreases of the Caton index in the DTO group in individual patients were
within the measurement error and not related to the amount of OWHTO-correction.
This might also be attributed to scarring of the patellar tendon, despite the postoperative
immediate motion protocol that was used.
In this study we found that a distal tuberosity osteotomy during OWHTO prevents a
decrease of patellar height measured with the Caton Index. Wright et al. 3 used the
Blackburne-Peel ratio and the Insall-Salvati ratio as a measure of patellar height and
found patella infera in 64% of their patients after OWHTO and no significant change in
patellar ligament length. Tigani et al. 2 found a significant reduction of the Caton index
after OWHTO similar to the results that were found in the patients with the PTO in the
present study. In the PTO group, all patients showed lowering of the patella after the
OWHTO and a direct relation was found between the change in patellar height and the
amount of correction of the OWHTO. Small corrections in patients with normal patellar
height will not likely lead to symptomatic patella infera. However, based on the results
of this study, we advise to use the DTO-technique in cases in which higher valgus
corrections are indicated (>10°) and in patients with pre-existing patella infera.
We encountered two pitfalls of the DTO technique in the patients in this study:
a fracture of the tibial tuberosity due to a tuberosity thickness of less than 1 cm and
imprecise screw fixation with positioning of the tuberosity screw in the opened wedge
of the HTO. Another pitfall is the length of the saw cut, which should leave enough
room for distal screw fixation after the wedge of the HTO is opened. With meticulous
surgical technique and preoperative planning, these complications can easily
be prevented.
A weak point in our study is the formation of the experimental and the control group.
The choice for the control patients is based on availability of preoperative radiographs.
These patients might differ from those which did not require a lateral image in 30º
for diagnostics. The only way to scientifically show that the distal tuberosity osteotomy
technique leads to a more normal patella height is with a randomised controlled trial.
We conclude that the distal tuberosity osteotomy is a safe technique and that it can
prevent lowering of the patella following OWHTO, especially in patients who need a
high degree of valgus correction for medial compartment osteoarthritis of the knee.
References
1. Scuderi GR, Windsor RE, Insall JN Observations on patellar height after proximal tibial osteotomy.
J Bone Joint Surg [Am] 1989; 71A(2): 245-248
2. Tigani D, Ferrari D, Trentani P, Barbanti-Brodano G, Trentani F Patellar height after high tibial
osteotomy. Int Orthop 2001; 24(6): 331-334
3. Wright JM, Heavrin B, Begg M, Sakyrd G, Sterett W Observations on patellar height following
opening wedge proximal tibial osteotomy. Am J Knee Surg 2001; 14(3):163-73
4. Hernigou P, Ma W Open wedge tibial osteotomy with acrylic bone cement as bone substitute.
The Knee 2001; 8: 103-110
5. Figgie HE 3rd, Goldberg VM, Heiple KG, Moller HS 3rd, Gordon NH The influence of tibial-
patellofemoral location on function of the knee in patients with the posterior stabilized condylar
knee prosthesis. J Bone Joint Surg [Am] 1986; 68A(7):1035-1040
6. Windsor RE, Insall JN, Vince KG Technical considerations of total knee arthroplasty after proximal
tibial osteotomy. J Bone Joint Surg [Am] 1988; 70A(4):547-555
7. Dejour H, Walch G, Nove-Josserand L, Guier C Factors of patellar instability: an anatomical
radiographic study. Knee Surg Sports traumatol Arthrosc 1994; 2(1):19-26
8. Goutallier D, Delepine G, Debeyre J The patello-femoral joint in osteoarthritis of the knee with
genu varus. Revue de Chirurgic Orthopedique 1979; 65(1):25-31
9. Leuthof D, Tobian F, Perka C High tibial osteotomy for valgus and varus deformities of the knee.
Int. Orthop 2001; 25: 93-96

108
chapter 8Summary, answers to research questions,
and closing remarks

110
Chapter 8
111
Summary, answers to research questions, and closing remarks
Summary and answers to research questions
In chapter 1, six questions concerning the treatment of patients suffering medial
osteoarthritis of the knee in combination with varus alignment, were formulated.
In this chapter, the previous chapters are summarized and an attempt is made to
answer the research questions.
In chapter 1, a general introduction, background and aims of the thesis are formulated.
The treatment of medial osteoarthritis of the knee includes a wide spectrum of
approaches, e.g. pharmaceutical, physiotherapy, bracing, and surgical treatment.
Many of these treatments relieve pain and increase function. However, not all of them
change the course of the disease. Because of the progressive nature of the disease
and because a varus malalignment will lead to an ongoing unfavourable mechanical
loading of the medial compartment, re-aligning the knee joint is important to obtain
significant relief from the complaints. Bracing to unload the medial compartment and
high tibial osteotomy are treatments to obtain this realignment. In this thesis several
aspects of these treatments for patients with medial osteoarthritis of the knee and
varus deformity have been studied.
1. What is the effect of valgus bracing in patients with medial compartment
osteoarthritis of the knee and can this be explained by changes in gait?
In chapter 2 a new valgus brace was evaluated in fifteen patients with medial
osteoarthritis of the knee and a varus leg axis. Significant improvements of pain and
function were found after six weeks of brace treatment. Because of the small number of
patients and because we did not use an alternative to the brace as a control, these
results should be interpreted cautiously. However, these findings were consistent with
results presented in previous studies with this and other braces. Gait analysis showed
that the brace has a tendency to lower the peak varus moment about the knee.
This effect was more profound at higher initial varus angles of the knee. Furthermore,
a small decrease of knee extension at the end of the swing phase and an increase
of walking velocity occurred when the brace was worn. Whether the new hinge
construction introducing an inflatable air chamber that has been incorporated in
this brace is responsible for the changes in the gait cycle or whether this is a general
effect of valgus producing hinged knee braces remains unclear because in the present
study no comparisons were made with other braces. Longer follow up of clinical
assessment and gait analysis are necessary to reveal whether the effects of
brace treatment found in this study persist. Using gait analysis studies to assess
the working mechanisms of brace treatment will enable objective evaluation of brace
treatment and should permit improved brace design.
2. What are the differences in accuracy and in postoperative stability between
closed and open wedge high tibial osteotomy?
In chapter 3 we analyzed the difference in angle correction accuracy and initial stability
between open-wedge and closed-wedge tibial valgus osteotomy in a cadaver study.
A correction of 7º was planned. After performing high tibial osteotomies on five, fresh
frozen pairs of human cadaver lower limbs (one limb received a CWO, the other an
OWO) were subjected to an increasing cyclic axial load until failure during which
the relative displacement of the bony segments was determined with roentgen stereo-
photogrammetric analysis (RSA). No significant differences in rotations and translations
in any direction were found in the displacement data. Further, no significant correlation
between bone mineral density (BMD) and the moment of failure was found.
This study revealed that both methods gave an acceptable correction within the wide
variation of postoperative correction angles. There was a tendency for overcorrection
in the closed wedge osteotomy group but no significant difference was found.
There was no difference in initial stability between the closed and the open wedge
osteotomy with a rigid locked plate fixation. Part of the relatively wide variation in
correction angle found in this study may be due to the fact that the angle for the
required correction is determined by the height of the medial opening and the length
of the osteotomy. The highly sensitive RSA which is extremely precise can determine
the correction angles in three dimensions obtained by the high tibial osteotomy and
revealed that the desired correction angle was not always obtained.
The use of angle stable implants in both groups lead to perfect postoperative stability.
However, this study concerned a small number of knees, and the results showed a
wide variation (large standard deviation). Furthermore, the outcomes may have been
the result of the biomechanical in vitro set-up, and therefore, the results can not be
unconditionally extrapolated to a clinical practice.

112
Chapter 8
113
Summary, answers to research questions, and closing remarks
The correction angles we found for each group in this study will probably be sufficient
in clinical practice. However, to obtain certainty about the clinical significance of
differences between the closed and open wedge osteotomy, a randomized clinical
needed to be conducted.
3. What are the differences between closed and open wedge high tibial
osteotomy in patients with respect to correction accuracy, collateral laxity
and clinical outcome?
In chapter 4 the results of a randomized clinical trial are presented. In 50 patients with
symptomatic osteoarthritis of the medial compartment of the knee were randomised
between an open and a closed wedge osteotomy. In both groups angle stable plate
fixation was used. The clinical results of high tibial osteotomy according to the open
wedge osteotomy and closed wedge osteotomy were compared.
Clinical and radiological assessments were performed preoperative and after one year.
Postoperative hip-knee-ankle (HKA) correction angles were monitored on standing leg
X-rays. The effect of high tibial osteotomy on collateral laxity of the knee was measured
with a specially designed varus-valgus device. The WOMAC osteoarthritis index, the
modified knee society score (KS) and visual analogue scales (VAS) were used to
assess symptoms of osteoarthritis, function, pain and patient satisfaction.
At one year follow-up we found accurate corrections in both groups and the planned
correction angles had been achieved. No loss of correction was observed.
Furthermore, the medial collateral laxity and the patellar height significantly decreased
after the open wedge osteotomy. Significant improvements of WOMAC and KS scores
were found in both groups. All patients had significantly less pain and were significantly
satisfied with the results. The duration of the surgery was significant longer in the
closed wedge group, and complications were more frequent in this group.
Both techniques led to good and comparable clinical results. In conclusion, the choice
whether to perform an open or a closed wedge osteotomy may be made on the basis
of preoperative patellar height or concomitant collateral laxity.
Longer follow-up is essential to obtain information about the ongoing clinical results in
both groups.
4. Does the incorporation and remodelling of ß-TCP bone substitute in open
wedge tibial osteotomy in patients occur similarly to that in animals?
In chapter 5, a histological study is described which reports on the bone biopsies from
16 patients (17 biopsies) treated with open wedge high tibial osteotomies for medial
knee osteoarthritis. The open wedge osteotomies were filled with a wedge of
osteoconductive beta tricalcium phosphate (ß-TCP) ceramic bone replacement.
Biopties were taken at time of removal of osteosynthesis material at follow-up times
ranging between 6-25 months. The null-hypothesis was that the incorporation and
remodelling process occurs similarly as to that in animals. The histological analysis
showed a good resorption of the ß-TCP with complete incorporation and remodelling
into new bone. The different phases as described in animal studies were found.
A correlation was found between histological findings and radiological assessment.
ß-TCP appeared to be a bone replacement material with optimal biocompatibility,
resorption characteristics and bone conduction properties for the clinical use. However,
to make a thorough comparison to animal studies, biopsies would have to be taken
earlier during the healing process In patients the fixation material can only be removed
after sufficient bone consolidation, otherwise possible loss of correction might occur.
Further research will be necessary to obtain more detailed information on the various
phases of incorporation of ß-TCP in human bone though this will be difficult because of
the medical and ethical limitations.
5. What are the effects of high tibial osteotomy on patellar tracking?
Chapter 6 describes an in vitro biomechanical study to analyze the effect of open and
closed wedge osteotomy on patellar tracking. Using an inventive experimental set-up, we
studied the 3D dynamic patellar tracking in ten cadaver knees before and after valgus
high tibial osteotomy. In each specimen, following a protocol it was possible to perform
corrections of 7º and 15º of valgus with an CWO and then 7° and 15° with a OWO.
Patellar height increased significantly after the CWO and decreased after the OWO.
Both open and closed wedge osteotomy resulted in significant changes in the tilt and
rotation of the patellar tracking when compared to the initial condition. We also found
significant differences between the two techniques. Valgus high tibial osteotomy
increased the medial patellar tilt and reduced the medial patellar rotation. These effects
were more profound after the OWO. No significant differences were found for

114
Chapter 8
115
Summary, answers to research questions, and closing remarks
medial-lateral patellar translation. These observations can be taken into consideration
when deciding which technique to perform in a patient with medial compartment
osteoarthritis of the knee. In the future, the effect of the kinematic changes in the
patellofemoral joint after high tibial osteotomy in terms of clinical presentation and
radiographic changes after long term follow-up have to be determined.
6. Can lowering of the patella which accompanies open wedge high tibial
osteotomy be prevented?
To prevent patella infera in open wedge high tibial osteotomy, a new operation technique
was developed. This is presented in chapter 7. Instead of a proximal tibial tuberosity
osteotomy (PTO), a distal osteotomy (DTO) was performed with the tuberosity being
fixed with one screw to the tibia. The results of two case series were compared.
The first 17 patients receiving a DTO were evaluated and compared to results of
20 patients with open wedge high tibial osteotomy with the standard proximal tuberosity
osteotomy. Distal tuberosity osteotomy in open wedge high tibial osteotomy appears
to be effective in preventing patella infera. A weak point in our study is the formation of
the experimental and the control group. The control patients were selected based on
the availability of the appropriate preoperative radiographs. Results from a randomised
controlled trial are required to ascertain whether the difference between the two groups
can be attributed to the operation technique. However, based on the results of
this study, we advise the use of the distal tuberosity osteotomy technique for those
patients for which higher valgus corrections are indicated (>10°) and for patients with
pre-existing patella infera.
Closing remarks and future directions
Medial osteoarthritis of the knee combined with varus deformity is a frequently
encountered medical problem in daily orthopaedic practice. For patients the progressive
course of this disease will have significant consequences in their socio-economical,
recreational and sports activities.
The treatment of varus deformity by re-aligning the knee can be obtained by means of
a valgus brace or high tibial osteotomy. Unloading braces come in all shapes and
sizes. Patient-compliance forms a recurrent problem with brace treatment. Especially
the more rigid unloading braces have been poorly accepted by the patients because
of discomfort, adverse effects or little effect at all. In the future, well conducted controlled
trials with long term follow-up to investigate the working mechanism of unloading braces
and underlying gait changes will be necessary. Only after such studies can clinical
questions about the actual effectiveness be answered. This will clarify proper treatment
decisions. Gait analysis research methods as described in this thesis can be utilised
when performing further research. For example, different types of braces could be
compared. Furthermore, it would be interesting to compare gait analysis before and
after high tibial osteotomy in patients who have been treated pre-operatively with an
unloading brace.
Surgical interventions, including joint replacement and osteotomy, reverse the progress
of osteoarthritis and provide long-term improved function and pain relief.
During the last few years the open wedge high tibial osteotomy has gained in popularity
over the closed wedge technique. While the results are dependent of the
preoperative diagnosis and the surgeon’s skill and experience, the clinical results
of both techniques seem to be generally the same.
Both techniques have advantages and disadvantages. The closed wedge technique
has the benefit of primary stability and progressive bone healing. However, it may lead
to deformity of the tibial head with potential problems for future total knee placement.
The osteotomy of the fibula and its co-morbidity form another disadvantage.
The open wedge osteotomy is a more straightforward technique which does not involve
the fibula. Often the proximal medial tibial head is deformed in varus knees.
With the open wedge osteotomy, the shape of the medial tibial head is restored.
As the clinical results of high tibial osteotomy depend largely on the correction angle
which has been obtained, the use of angle stable implants should be mandatory,
especially for open wedge high tibial osteotomy. In this thesis, angle stable fixation
showed no loss of correction in either closed or open wedge high tibial osteotomies.
In future comparative study designs, it is essential to use the same fixation material
in both groups. Furthermore, randomized clinical trials are necessary to investigate
the differences in long-term clinical outcome, using total knee arthroplasty as the
end-point.

116
Chapter 8
117
Summary, answers to research questions, and closing remarks
Further research should also compare high tibial osteotomy with a knee athroplasty
using the unicompartmental knee prosthesis. And last but not least, it is essential that
clear patient criteria be established so that the most beneficial clinical outcome can
be obtained.
The recent evolutions in cartilage repair procedures are promising and will possibly
prove to be useful in the treatment of osteoarthritis of the knee. However, at present
no conclusive long-term data support this premise. Furthermore, when malalignment
is present, it is probably beneficial to combine cartilage repair with high tibial osteotomy
to unload the repaired joint surface.
With the revival of the open wedge technique, the high tibial osteotomy seems to have
reclaimed its position in the spectrum for treatment of varus osteoarthritis of the knee.
The large numbers of open wedge procedures recently performed worldwide contain
valuable information on clinical outcome, possible adverse events and pitfalls.
The biomechanical set-ups which were designed for the research reported in this thesis,
are extremely suitable for further future osteotomy research. For example, correction
accuracy, stability and effects on patellofemoral kinematics of supracondylar femur
osteotomies can be studied using these methods.
The results found in studies reported in this thesis clearly show the effects of high
tibial osteotomy on patellar height and tracking. While these effects may be of minimal
clinical relevance, for extensive open wedge corrections the effects may be quite
large and lead to adverse events with respect to the patellofemoral joint (e.g. pain,
maltracking or even patellar (sub)luxation). On the other hand, patellofemoral
complaints may subside after high tibial osteotomy. Furthermore, the (re-) tensioning
of the medial collateral ligament after open wedge osteotomy may lead to unfavourable
higher contact pressures in the medial compartment of the knee. Even so, pre-existent
medial instability can be reduced by tensioning the medial collateral ligament.
Surgeons should be aware and understand these effects in their choice for one of the
high tibial osteotomy techniques.
Finally, the straightforward surgical technique and the possibility of intra-operative
variation of the amount of valgus and slope correction are big advantages of the open
wedge osteotomy. Moreover, the potential treatment of medial collateral (pseudo-)
laxity can be beneficial. Furthermore, the possibility of preventing patellar height
and tracking changes by combining the open wedge with the distal tuberosity
osteotomy technique is another advantage. These aspects make the open wedge
high tibial osteotomy with angle stable internal fixation a very powerful treatment option
for patients with medial osteoarthritis of the knee.

118
chapter 9Samenvatting, beantwoording van de
onderzoeksvragen en afsluitende opmerkingen

120
Chapter 9
121
Samenvatting, beantwoording van de onderzoeksvragen en afsluitende opmerkingen
Samenvatting en beantwoording van de onderzoeksvragen
In de vorm van zes onderzoeksvragen betreffende de behandeling van patiënten met
varus gonarthrose, zijn de doelstellingen van dit proefschrift geformuleerd in hoofdstuk 1.
In deze samenvatting worden de verschillende hoofdstukken samengevat en zal er
getracht worden deze vragen te beantwoorden.
Hoofdstuk 1 bevat een algemene introductie, de achtergronden en de doelstellingen
van dit proefschrift. De behandeling van gonarthrose behelst een breed spectrum aan
mogelijkheden, e.g. medicamenten, fysiotherapie, brace behandeling en chirurgische
interventies. Deze behandelingen verlichten veelal de pijn en verbeteren de functie,
maar zullen niet allen het voortschrijden van de artrose voorkomen. Herstellen van het
alignement van de knie is belangrijk voor significante vermindering van klachten.
Behandelingen in de vorm van een ontlastende valgiserende brace of de valgiserende
tibiakop osteotomie hebben dit als doel. In dit proefschrift worden verschillende aspecten
van deze behandelingen van patiënten met varus gonarthrose nader bestudeerd.
1. Wat is het effect van behandeling met een valgus brace bij patiënten met
artrose van het mediale compartiment van de knie en kan dit verklaard worden
op grond van veranderingen in het looppatroon ?
Patiënten met arthrose van het mediale compartiment van de knie kunnen conservatief
behandeld worden met een valgiserende brace. Om de goede klinische ervaringen
met een nieuwe valgiserende knie brace nader te onderzoeken is een prospectieve
ganganalyse studie uitgevoerd naar de effecten van de Softec OA brace (Bauerfeind).
Deze studie staat beschreven in hoofdstuk 2. Vijftien patiënten, met een varus beenas
en mediale gonarthrose, werden geïncludeerd in de studie. Voor en na brace
behandeling gedurende zes weken, werden de WOMAC arthrose index en VAS
pijnscores afgenomen. Daarnaast werd een ganganalyse verricht voor aanmeten en
dragen van de brace en na het dragen van de brace gedurende zes weken.
De ganganalyse bestond uit het simultaan meten van de externe knie momenten in
het frontale vlak, krachten data en 3D kinematische data. De grondreactie krachten
werden gemeten met een in de vloer gelegen krachten platform. De 3D posities van
de reflecterende markers werd geregistreerd met behulp van een 6-camera motion
analysis system. Voor de plantaire druk metingen en de “foot progression angle” (FPA)
werd gebruik gemaakt van een drukplatform. De lopende band werd gebruikt om
gewrichtshoeken en range of motion (ROM) te meten met behulp van goniometers.
Verder zijn staplengte en stapfrequentie gemeten.
De klinische resultaten lieten een significante verbetering zien van de klinische scores
na zes weken de brace gedragen te hebben. Deze resultaten zijn echter gebaseerd op
een korte follow-up en bij een relatief kleine groep zonder dat er een controle brace is
gebruikt. Ganganalyse liet zien dat de brace een tendens vertoonde in het verlagen
van het peak varus moment rond de knie en dat dit effect meer uitgesproken was bij
een grotere varus deformiteit. Verder was er een kleine afname van de eindstrekking
van de knie aan het einde van de swingfase en een toename van de loopsnelheid
gerelateerd aan het dragen van de brace. Van belang is de vraag of een valgiserende
knie brace daadwerkelijk het varus alignement van het been vermindert of dat de brace
een toename in varus tijdens de mid-standfase verhindert. Aangezien het peak varus
moment zich juist aan het begin en aan het einde van de standfase bevindt, is het
maar de vraag of dit de juiste parameter is om te meten om het effect van valgiserende
braces aan te tonen. Mogelijk spelen ook andere factoren, zoals gang-adaptaties, een
rol bij het ontlasten van het mediale compartiment. Langere follow up van klinische
resultaten en ganganalyse moet aantonen of deze effecten persisteren. De analyse van
de werkingsmechanismen van brace behandeling met ganganalyse studies maakt
objective evaluatie van de effecten van brace behandeling mogelijk en kan toekomstige
brace ontwerpen verbeteren.
2. Wat is het verschil in nauwkeurigheid en postoperatieve stabiliteit tussen de
gesloten en open wig tibiakop osteotomie?
De valgiserende tibiakop osteotomie bij varus gonarthrosis kan bestaan uit een lateraal
gesloten wig osteotomie of een mediaal open wig osteotomie. In een biomechanische
kadaver RSA studie zijn beide operatiemethoden vergeleken voor wat betreft de
nauwkeurigheid in correctie hoek en initiële postoperatieve stabiliteit. Deze studie staat
beschreven in hoofdstuk 3. Vijf paar vers bevroren humane kadaver knieën werden
gebruikt en 7º correctie osteotomieën werden verricht. Er werd gebruik gemaakt van
de open en de gesloten techniek. De osteotomieën werden gefixeerd met hoekstabiele
interne fixatie. Vervolgens werden de knieën onderworpen aan een toenemende

122
Chapter 9
123
Samenvatting, beantwoording van de onderzoeksvragen en afsluitende opmerkingen
dynamische belasting waarbij de relatieve verplaatsing van de botstukken werd gemeten
met röntgen stereophotogrammetrische analyse (RSA).
Er werden geen verschillen gevonden in vlakken van rotatie en translatie. De RSA data
betreffende de verplaatsing van de botstukken onder invloed van de belasting lieten
geen statistische verschillen zien tussen de gesloten en de open wig osteotomie.
Middels DEXA metingen werd de botdichtheid van alle preparaten bepaald, maar er
werd geen significante correlatie gevonden tussen botdichtheid en verplaatsing van de
botstukken of het moment van falen.
Beide technieken gaven een acceptabele correctie geven met een hoge variatie van
postoperatieve correctie hoeken. Er is een tendens naar overcorrectie van de geplande
wig hoek bij de gesloten wig osteotomie, maar geen significant verschil kon worden
aangetoond. Er is geen verschil in initiële stabiliteit tussen gesloten wig en open wig
osteotomie met hoekstabiele implantaten. Dit onderzoek betrof een klein aantal knieën
en de resultaten hadden een grote variatie en grote standaard deviaties. Daarnaast zijn
de uitkomsten grotendeels afhankelijk van de biomechanische in vitro setting.
Daarom kunnen de resultaten niet eenvoudig worden geëxtrapoleerd naar de klinische
praktijk. De bereikte correctie hoeken bij zowel de gesloten als de open wig groep in
deze studie zijn waarschijnlijk toereikend in de klinische praktijk. Er is behoefte aan
gerandomiseerd klinisch onderzoek naar het verschil tussen beide osteotomie technieken.
3. Wat zijn de verschillen tussen de gesloten en open wig tibiakop osteotomie
voor wat betreft de correctie nauwkeurigheid, de collaterale stabiliteit en de
klinische resultaten?
Hoofdstuk 4 beschrijft een prospectieve gerandomiseerde klinische trial die is uitgevoerd
in twee ziekenhuizen. De patiënten werden gerandomiseerd voor een van de twee
operatie technieken: de lateraal gesloten wig en de mediaal open wig valgiserende
tibiakop osteotomie. Vijftig patiënten met symptomatische mediale gonarthrose werden
geïncludeerd en gerandomiseerd voor een van beide behandelingen zodat twee
groepen van 25 patiënten ontstonden. In beide technieken is een hoekstabiele
plaat gebruikt voor de fixatie van de osteotomie. Bij de open wiggen is een tricalcium-
phosphaat (TCP) wig geplaatst. In beide gevallen bestond de nabehandeling uit
aantippend belast mobiliseren met krukken en onbelast oefenen.
Uitkomstmaten waren nauwkeurigheid van correctie en het effect op de collaterale
stabiliteit van de knie. Daarnaast is vergeleken voor wat betreft klinische resultaten
(WOMAC en VAS pijnscores) operatieduur en complicaties. Na 1 jaar follow-up is de
geplande en de bereikte correctie vergelijkbaar voor beide technieken. Er werd geen
correctie verlies gezien. Bij de open wig osteotomie werd een afname gevonden van
de mediale collaterale laxiteit van de knie, waarschijnlijk als gevolg van het opspannen
van de mediale structuren. Daarnaast trad er een significante distalisatie op van de
patella bij de open wig osteotomie. Verder was er sprake van een vergelijkbare
significante verbetering van de klinische scores voor beide technieken. De operatie
duur van de gesloten wig osteotomie was significant langer, evenals de complicatie
frequentie. Beide technieken leiden tot goede en vergelijkbare klinische resultaten.
De keuze voor een open of een gesloten wig osteotomie zou gebaseerd kunnen zijn
op de preoperatieve patella hoogte of bijkomende collaterale laxiteit. Langere follow-up
is noodzakelijk om aan te tonen of verschillen optreden tussen beide technieken wat
betreft klinische scores en late complicaties.
4. Verloopt de bot-incorporatie en remodelering van ß-TCP botvervanger bij de
open wig tibiakop osteotomie bij patiënten het zelfde als in proefdieren?
In patiënten is het niet gemakkelijk de incorporatie en botgenezing te beoordelen op
standaard röntgenfoto’s. In eerder onderzoek werd een radiologische classificatie
ontwikkeld die de verschillende stadia van incorporatie en remodelering van ß-TCP
beschrijft. Histologische data zijn echter niet bekend. Een histologische studie
werd verricht naar de incorporatie, resorptie en remodeling van ß-TCP. Hiertoe zijn
16 patiënten (17 osteotomieën) geïncludeerd. Deze studie staat beschreven in hoofd-
stuk 5. Deze patiënten hadden allemaal mediale compartiments gonarthrose, waarvoor
zij een open wig tibiakop osteotomie ondergingen. De geopende osteotomie werd
opgevuld met een ß-TCP wig. Ten tijde van het verwijderen van het osteosynthese
materiaal na verschillende follow-up duur (6-25 maanden) werden biopten genomen
van de tibiakop ter plaatse van de ß-TCP wig. De biopten werden onderzocht op
resorptie, incorporatie en bot remodelering van de ß-TCP wig. De hypothese van de
studie was dat de incorporatie en remodelering hetzelfde patroon zouden laten zien als
in proefdieren. Histologie toonde een goede resorptie van de ß-TCP met een complete
incorporatie en remodelering in nieuw bot. De verschillende fases zoals beschreven in
proefdierstudies werden gevonden. Een correlatie tussen de histologische bevindingen

124
Chapter 9
125
Samenvatting, beantwoording van de onderzoeksvragen en afsluitende opmerkingen
en de radiologische classificatie bleek te bestaan. Concluderend, de ß-TCP wig blijkt
een botvervanger met optimale biocompatibiliteit, goede resorptie en osteoconductieve
eigenschappen voor klinisch gebruik. Medisch ethische bezwaren maken het nemen
van biopten in eerdere fasen van de incorporatie onmogelijk.
5. Wat zijn de effecten van de tibiakop osteotomie op het de patella-sporing?
De valgiserende tibiakop osteotomie kan veranderingen in patella hoogte veroorzaken,
afhankelijk van de operatie techniek, de grootte van de correctie en het postoperatieve
beleid. Veranderingen in patella hoogte kunnen leiden tot postoperatieve complicaties,
maar er is weinig informatie over de effecten op de dynamische patella kinematica na
een tibiakop osteotomie. Daarom is er een biomechanische kadaver studie uitgevoerd
naar het effect van de open en gesloten wig osteotomie op de patella sporing.
Deze studie staat beschreven in hoofdstuk 6. In deze studie is de 3D dynamische
patella sporing bestudeerd, in tien kadaver knieën, voor en na een valgiserende
tibiakop osteotomie. Met behulp van een speciaal ontwikkeld frame, konden in elke
kadaver knie, correcties worden verricht van 7º en 15º valgus volgens zowel de open
als de gesloten wig techniek. Zowel de open als de gesloten wig osteotomie gaven
significante veranderingen van de patella sporings parameters tilt en rotatie.
We vonden significante verschillen tussen de open en gesloten wig osteotomie.
De valgiserende tibiakop osteotomie gaf een toename van de mediale patella tilt en
een afname van de mediale patella rotatie. Door de verplaatsing van de tuberositas
treedt een verandering op in de trekkrachten van de patellapees en dientengevolge de
beschreven veranderingen in de stand en sporing van de patella. Deze effecten waren
meer uitgesproken bij open wig techniek. Er werden geen verschillen gevonden in het
effect op de mediale-laterale translatie. De patella hoogte nam significant toe bij de
gesloten wig osteotomie. Bij de open wig osteotomie trad een significante laagstand
van de patella op. Van belang is het de observaties uit deze studie in het achterhoofd
te houden bij de keuze voor een open of een gesloten wig osteotomie.
Toekomstig onderzoek moet uitwijzen wat de klinische en radiologische implicaties zijn
van deze effecten op de patella sporing op langere termijn na een open of gesloten
wig valgiserende tibiakop osteotomie.
6. Kan de patella laagstand die optreedt na een open wig tibiakop osteotomie
worden voorkomen?
Bij de valgiserende mediaal open wig osteotomie ter behandeling van mediale
compartiments gonarthrose zal een distalisatie optreden van de tuberositas tibiae.
Laagstand van de patella na mediaal open wig tibiakop osteotomie kan leiden tot
patellofemorale klachten en moeilijkheden bij een eventuele totale knie prothese
plaatsing in de toekomst. Ter voorkoming van distalisatie van de patella, werd een
nieuwe techniek ontwikkeld. Dit staat beschreven in hoofdstuk 7. In plaats van een
proximale tuberositas osteotomie (PTO), is gebruik gemaakt van een distale
tuberositas osteotomie (DTO). Hierbij wordt de tuberositas tibiae losgezaagd naar
distaal. Bij openen van de wig blijft de tuberositas nu op zijn oorspronkelijke plaats,
zodat geen distalisatie van de patella optreedt. De tuberositas wordt gefixeerd met een
schroef. De eerste ervaringen met de DTO bij 17 patiënten zijn geëvalueerd en
vergeleken met een groep van 20 patiënten waarbij een PTO werd verricht.
Ter bepaling van de patella-hoogte werd bij alle patiënten de Caton index (CI) gemeten
op de pre- en zes weken postoperatieve laterale knie röntgenfoto’s. In beide groepen
werden de pre- en postoperatieve CI vergeleken met de gepaarde t-toets. In de PTO
groep trad een significante vermindering op van de patella-hoogte. In de DTO groep
was er geen essentiële verandering van de patella-hoogte. Er werd een relatie
gevonden tussen de correctiehoek en de mate van vermindering van de CI bij PTO.
Er gingen twee pitfalls gepaard met deze nieuwe techniek: een fractuur van de
tuberositas als gevolg van onvoldoende dikte van het fragment en verkeerde
schroefplaatsing in de osteotomie. De lengte van de osteotomie is ook van belang
om voldoende overlap en ruimte voor de schroef te bewerkstelligen, voornamelijk bij
de grotere correcties. De distale tuberositas osteotomie kan laagstand van de patella
voorkomen en wordt geadviseerd bij open wig valgiserende tibiakop osteotomieën
met een correctie van meer dan 10º, of bij preëxistente patella infera.

126
Chapter 9
127
Samenvatting, beantwoording van de onderzoeksvragen en afsluitende opmerkingen
Afsluitende opmerkingen en toekomstig onderzoek
Mediale compartiments arhrose van de knie in combinatie met een varus malalignement
is een veel voorkomend probleem in de dagelijkse orthopedische praktijk. Voor de
patiënt zal de progressief verlopende aandoening aanzienlijke consequenties hebben
voor zijn of haar activiteiten tijdens werk, recreatie en sport.
De behandeling van de varus stand kan plaatsvinden door middel van een valgiserende
brace of een tibiakoposteotomie. Unloader braces zijn er in alle soorten en maten.
Therapie trouwheid vormt een probleem bij brace behandeling. Vooral de meer rigide
valgiserende braces worden matig verdragen door de patiënt vanwege te weinig
draagcomfort, drukplekken of beperkt effect. In toekomstig onderzoek is er behoefte
aan goed opgezette gecontroleerde studies met lange termijn follow-up om de
werkingsmechanismen en de gangadaptaties van deze braces nader te onderzoeken.
Dit moet er toe leiden dat klinische vragen betreffende de effectiviteit beantwoordt
worden en dat behandel-indicaties duidelijker worden. De ganganalyse onderzoeks-
methode zoals beschreven in dit proefschrift is zeer geschikt voor verder toekomstig
onderzoek. Bijvoorbeeld om verschillende braces met elkaar te vergelijken. Verder zou
het interessant zijn om ganganalyse voor en na een tibiakop osteotomie te vergelijken
met ganganalyse bij dezelfde patiënten met pre-operatief brace gebruik.
Chirurgische ingrepen, inclusief gewrichtsvervangende behandeling en osteotomie,
stoppen de progressie van arthrose en leiden tot verbeterde functie en pijn verlichting
op lange termijn. Op dit moment is er een tendens te zien van een groeiende
populariteit van de open wig tibiakop osteotomie ten opzichte van de gesloten wig
osteotomie. Afhankelijk van de indicatiestelling, de chirurgische vaardigheden en
ervaring, lijken de klinische resultaten van beide technieken vergelijkbaar te zijn.
Beide technieken hebben hun voor- en nadelen. De gesloten wig osteotomie heeft het
voordeel van stabiel direct bot-op-bot contact, met een gunstige uitgangssituatie voor
de bot heling. De eventuele plaatsing van een totale knieprothese in de toekomst kan
echter bemoeilijkt worden door de opgetreden deformiteit en het botverlies van de
tibiakop. Daarnaast vormt de met mogelijke co-morbiditeit gepaard gaande fibula
osteotomie een nadeel van de gesloten wig osteotomie. De open wig osteotomie is
een betrekkelijk eenvoudige operatie zonder de nadelen van een fibula osteotomie.
Omdat de klinische resultaten van de tibiakoposteotomie voor een groot deel
afhankelijk zijn van de bereikte correctie, zou het gebruik van hoekstabiele implantaten
de gouden standaard moeten zijn, voornamelijk bij de open wig osteotomie. Bij zowel
de gesloten als de open tibiakoposteotomie werd geen correctieverlies gezien met
hoekstabiele plaatfixatie. Het is daarom essentieel dat in toekomstige vergelijkende
studies in beide groepen de zelfde hoekstabiele plaat wordt gebruikt. In de toekomst
zijn gerandomiseerde klinische trials nodig om de onderlinge verschillen verder te
onderzoeken evenals de klinische uitkomsten op de lange termijn met de totale
knieprothese als eindpunt.
Toekomstig onderzoek is ook nodig voor de vergelijking van de tibiakop osteotomie
met de hemi-knieprothese. Er is nog altijd behoefte aan heldere criteria voor een zo
goed mogelijk klinisch resultaat.
De recente ontwikkelingen in kraakbeen chirurgie zijn veelbelovend en mogelijk in de
toekomst een goed alternatief bij de behandeling van gonarthrose. Echter, er zijn op
dit moment geen conclusieve lange termijn data die dit ondersteunen. De tibiakop
osteotomie zal mogelijk gecombineerd dienen te worden met kraakbeen procedures
bij varus (of valgus) deformiteiten teneinde het aangedane gewrichtsoppervlak te
ontlasten.
Met de open wig osteotomie lijkt het erop dat de valgiserende tibiakop osteotomie zijn
plek heeft heroverd binnen het behandelspectrum van de varus gonarthrose.
De grote aantallen open wig osteotomieën die in de recente periode wereldwijd zijn
verricht vormen een bron van waardevolle informatie over klinische uitkomst mogelijke
complicaties en pitfalls. De biomechanische test modellen zoals beschreven in dit
proefschrift zijn zeer geschikt voor toekomstige osteotomie studies. De nauwkeurigheid
van correctie, de stabiliteit en de effecten op de patellofemorale kinematica van
bijvoorbeeld de supracondylaire femur osteotomie kunnen in deze opstellingen
bestudeerd worden.
In de recente literatuur en in dit proefschrift worden de effecten beschreven van de
tibiakoposteotomie op de hoogte en sporing van de patella. Vaak zullen deze effecten
weinig klinsche relevantie hebben, maar bij grote open wig correcties kunnen er
behoorlijke consequenties zijn voor het patellofemorale gewricht (e.g. pijn, laterale
sporing, (sub)luxatie van de patella). Aan de andere kant, patellofemorale klachten

128
Chapter 9
129
Publications
Rutten GJ, Gaasbeek RD, Franssen H.
Decrease in nerve temperature: a model for increased temporal dispersion.
Electroencephalogr Clin Neurophysiol. 1998 Feb;109(1):15-23.
Gaasbeek RDA, Sonneveld H, van Heerwaarden RJ, Jacobs WC, Wymenga AB.
Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent
patella infera: a new technique. Knee. 2004 Dec;11(6):457-61.
Gaasbeek RD, Rijnberg WJ, van Loon CJ, Meyers H, Feith R.
No local recurrence of enchondroma after curettage and plaster filling.
Arch Orthop Trauma Surg. 2005 Feb;125(1):42-5.
van Heerwaarden RJ, GaasbeekRDA, Plitz W. A new valgus brace for medial knee osteoarthritis.
A short term patient evaluation study with the Softec OA brace.
Med-Orthop Technik 2005: 57-65.
Gaasbeek RDA, Welsing RT, Verdonschot N, Rijnberg WJ, van Loon CJ, van Kampen A.
Accuracy and initial stability of open- and closed-wedge high tibial osteotomy: a cadaveric RSA study.
Knee Surg Sports Traumatol Arthrosc. 2005 Nov;13(8):689-94.
Gaasbeek RDA, Toonen HG, van Heerwaarden RJ, Buma P.
Mechanism of bone incorporation of beta-TCP bone substitute in open wedge tibial osteotomy in
patients. Biomaterials. 2005 Nov;26(33):6713-9.
Gaasbeek RD, Groen BE, Hampsink B, van Heerwaarden RJ,
Duysens JEJ. Valgus bracing in patients with medial compartment osteoarthritis of the knee.
A gait-analysis study of a new brace. Gait Posture 2007 Jun; 26(1):3-10.
Gaasbeek RD, Welsing RTC, Verdonschot N, van Kampen A.
The influence of open and closed high tibial osteotomy on dynamic patellar tracking:
a biomechanical study. Knee Surg Sports Traumatol Arthrosc. 2007 May 5; [Epub ahead of print]
kunnen ook verminderen na een tibiakoposteotomie. Daarnaast kan het opspannen
van de mediale collaterale band na een open wig osteotomie leiden tot ongewenste
verhoogde drukken in het mediale compartiment van de knie. Echter, preëxistente
mediale instabiliteit kan worden verminderd door dit zelfde mechanisme. Orthopedisch
chirurgen moeten zich bewust zijn van deze effecten bij het maken van een keuze voor
een van beide osteotomie technieken.
Tenslotte vormen de relatief eenvoudige techniek en de mogelijkheid om tijdens de ope-
ratie de valgus correctie en eventuele slope correctie te kunnen variëren, grote voordelen
van de open wig techniek. Daarnaast is er de mogelijkheid om mediale (pseudo-)laxiteit
te behandelen. De mogelijke combinatie van de open wig techniek met de distale tube-
rositas osteotomie ter preventie van patella laagstand en sporingsproblemen vormt een
ander voordeel. Deze eigenschappen maken de open wig osteotomie met hoekstabiele
fixatie tot een sterke keuze als behandeling voor patiënten met mediale gonarthrose.

130 131
Dankwoord
Dit proefschrift is het tastbare resultaat van een vruchtbare samenwerking van de
drie opleidingsziekenhuizen in regio Oost: het Rijnstate Ziekenhuis te Arnhem,
de Sint Maartenskliniek en het UMC St. Radboud te Nijmegen. Op alle drie locaties
is gewerkt aan de studies in dit boekje. Dit is het bewijs van de vele verschillende
klinische en wetenschappelijke disciplines die de assistent Orthopedie ter beschikking
staan tijdens zijn of haar opleiding in dit cluster. Vele mensen hebben een bijdrage
geleverd aan de studies in deze thesis. Enkele van hen wil ik graag in het bijzonder
bedanken:
Prof. Dr. A. van Kampen, mijn promotor. Beste Albert, toen ik je medio 2002 benaderde
betreffende de promotie mogelijkheden reageerde je gelijk enthousiast. De avondjes
met de “hele ploeg” bij jou thuis waren steeds zeer vruchtbaar en motiverend.
Tijdens mijn opleiding en ook als trauma-fellow heb ik naast wetenschappelijke ook
veel praktische vaardigheden van je geleerd. Vooral jouw onuitputtelijke drive voor het
vak, in combinatie met een gezonde dosis humor vormen voor mij een groot voorbeeld.
Dr. R.J. van Heerwaarden, mijn co-promotor. Beste Ronald, tijdens mijn opleiding in
de Sint Maartenskliniek is er een stevige basis gelegd voor dit boekje en dankzij jouw
volhardendheid en ongekende gedrevenheid is de missie geslaagd. Er waren snelle
successen en ook wat zwaardere bevallingen, maar uiteindelijk is het een mooi “kindje”
geworden. Ik hoop dat we nog veel samen zullen werken in de toekomst.
Dr. Ir. N.J.J. Verdonschot, mijn co-promotor. Beste Nico, jouw wetenschappelijk
verantwoorde input en biomechanische benadering waren van onschatbare waarde
voor deze thesis. De flexibele wijze waarop ik aanvankelijk als “buitenstaander” aan de
slag kon in het lab, en de laagdrempeligheid voor overleg heb ik zeer gewaardeerd.
Jij hebt het Orthopaedic Research Lab de laatste jaren wereldwijd op de kaart gezet,
en ik hoop dat toekomstige samenwerking mogelijk blijft.
Gaasbeek RD, Nicolaas L, Rijnberg WJ, van Loon CJM, van Kampen A.
Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomy
A one year randomizes controlled. J Bone Joint Surg Br. 2007 In revision

132 133
Dr. W.J. Rijnberg, mijn opleider. Beste Willaart, het idee om de open en de gesloten wig
tibiakop osteotomie met elkaar te vergelijken kwam uit jouw koker. Ik was een van jouw
eerste opleidings-assistenten en de wetenschappelijke trein kwam maar traag op gang.
Zoals blijkt uit dit proefschrift, heb je mij toch op het juiste spoor gezet. Hartelijk dank
voor de ruimte die mij tijdens mijn opleiding geboden is om dit onderzoek te doen.
Dr. C.J.M. van Loon. Beste Corné, als zeer efficiënte schrijver met een enorme output,
ben jij tijdens de eerste jaren van mijn opleiding, een drijvende kracht geweest.
Samen met jou heb ik het “recept” van dit boekje bedacht. Daarbij was het erg fijn dat de
nodige paden door jou al waren bewandeld. Je snelle beoordeling van de manuscripten
en je oprechte verbazing als een stuk geweigerd werd hebben mij enorm gesteund.
Dr. P. Buma. Beste Pieter, de vrij plotselinge en kortstondige samenwerking in het kader
van dit proefschrift heeft geleid tot een mooie publicatie. Ik realiseer mij terdege dat,
zonder jouw uitgemeten histologische expertise, dit nooit zover was gekomen.
Prof. Dr. J.E.J. Duysens. Beste Jaak, toen ik met mijn ganganalyse studie onder de arm
bij je langs kwam, was je gelijk enthousiast. Hartelijk dank voor de snelle en kritische
beoordeling van het manuscript en de perfecte formulering van de antwoorden voor de
reviewers.
Prof dr. A.C.H. Geurts, Prof dr. R.F.J.M. Laan, Prof dr. J.A.N. Verhaar, leden van de
manuscript-commissie, dank u voor uw tijd en de interesse.
Dhr. W.S.J. van de Wijdeven, Beste Willem, ik denk dat maar weinig mensen zich
realiseren aan hoeveel proefschriften jij je bijdrage hebt geleverd. Hartelijk dank voor je
praktische tips en tomeloze inzet bij het uitvoeren van de experimenten op het ORL.
Wilco Jacobs, Roy Welsing, Brieke Hampsink, Brenda Groen, Loes Nicolaas, medisch
studenten van het klinisch score station, alle patiënten, medewerkers van de klinieken,
poliklinieken en secretariaten, medewerkers van het ORL, allen zeer veel dank voor jullie
inspanningen. Patsy Anderson, bedankt voor de correctie van het Engels.
De onderzoeken en het grootste deel van het schrijfwerk van dit proefschrift hebben
plaatsgevonden tijdens mijn opleiding tot orthopedisch chirurg en mijn trauma
fellowship. Mijn opleiders, Dr. B.J. Dwars, Dr. A.B. Wymenga en Prof. dr. R.P.H. Veth,
Prof. dr. A. van Vugt, evenals alle stafleden van de opleidingsklinieken dank ik voor mijn
opleiding en voor de mogelijkheden om dit onderzoek voort te zetten.
Mijn paranimfen: Huub van der Heide en Jack van der Gragt. Huub, natuurlijk ben jij één
van mijn paranimfen. Dank je voor de enorme gastvrijheid tijdens de diensten in de
UMC tijd. Jack, daar staan we dan straks weer in rok, net als 16 jaar geleden. Wie weet
is er ooit tijd voor de derde keer...
Mijn schoonouders, pa en ma Mulder, jullie dank ik voor de ondersteuning en
enorme toewijding aan ons gezin. Thom en Marilou kunnen zich geen betere opa en
oma wensen!
Mijn zus, Pauline en haar mannen René, Laurens en Rutger, dank voor jullie steun
en hulp de afgelopen tijd.
Mijn ouders, pa en ma, mijn basis ligt bij jullie. Dank jullie voor de liefde en kansen
die jullie mij hebben gegeven. Aan jullie draag ik dit proefschrift op.
Lieve Anne-Marie, de zekerheid van jouw liefde en steun zijn voor mij een rustpunt
van waaruit alles mogelijk (b)lijkt. Op naar de volgende mijlpaal!
Thom en Marilou, jullie zijn de twee grootste cadeaus op aarde.
Nu is het verhaaltje uit. Maar we gaan nog lang niet slapen!

134 135
Curriculum Vitae
Robert Dick Alexander Gaasbeek werd geboren op 17 september 1969 te Zwolle.
In 1987 behaalde hij het VWO diploma aan de Thorbecke Scholengemeenschap
te Zwolle. Na een onbezorgde jeugd vertrok hij naar Utrecht. Daar werd in 1991
de studie Fysiotherapie afgerond aan de Internationale Academie voor Fysiotherapie
Thim van der Laan te Utrecht. Hierna volgde de studie Geneeskunde aan de
Universiteit van Utrecht. Tijdens deze studie was de auteur werkzaam als fysiotherapeut
en verrichtte hij wetenschappelijk onderzoek naar zenuwgeleiding bij de vakgroep
klinische neurofysiologie van het UMC Utrecht (begeleiding: Dr. H. Franssen).
Het artsexamen werd in 1997 behaald. Van 1997-1998 werkte hij als arts-assistent op
de afdeling orthopedie van het Onze Lieve Vrouwe Gasthuis te Amsterdam.
(opleider: Prof. dr. J.W. van der Eijken). In het kader van de opleiding tot orthopedisch
chirurg, werd de tweejarige vooropleiding heelkunde eind 1999 voltooid in het
Slotervaart Ziekenhuis te Amsterdam. (opleider: Dr. B.J. Dwars).
Op 1 januari 2000 werd gestart met de opleiding orthopedie in het Rijnstate Ziekenhuis
te Arnhem (opleider: W.J. Rijnberg). Van 2001 tot 2003 werden stages doorlopen in de
St. Maartenskliniek (opleider Dr. A.B. Wymenga) en in het UMC st. Radboud
(opleider: Prof. dr. R.P.H. Veth) te Nijmegen. Tijdens de opleiding werd op alle drie de
locaties gewerkt aan onderzoek dat tot dit proefschrift heeft geleid. De opleiding werd
eind 2004 afgerond.
Het jaar 2005 was hij als orthopedisch chirurg/trauma-fellow, werkzaam in het UMC
St. Radboud te Nijmegen (opleiders: Prof. Dr. A. van Kampen en Prof. dr. A.B. van Vugt).
Per 1 januari 2006 is de auteur werkzaam als orthopedisch chirurg in het Meander
Medisch Centrum te Amersfoort in associatie met J.B. van Lent, M.P.J. van der List,
H. Sonneveld, A.B. Stibbe, H.G.W. Vermeer en H.J.J Zwart. De auteur is getrouwd
met Anne-Marie en zij hebben twee kinderen: Thom en Marilou.


Hig
h T
ibial O
steoto
my Treatm
ent o
f varus o
steoarth
ritis of th
e knee R
ob
ert D. A
. Gaasb
eek
Uitnodiging
Voor het bijwonen vande openbare verdediging
van het proefschrift
‘High tibial osteotomy.Treatment of varus osteoarthritis
of the knee’
op vrijdag 21 september 2007om 10.30 uur in de Aula Major
van de Radboud UniversiteitComeniuslaan 2 te Nijmegen.
Receptie na afloop ter plaatse
Robert GaasbeekKruisweg 16bis3513 CT Utrecht
De Paranimfen Huub van der Heide, tel: 06-43001007
[email protected] van der Gragt, tel: 06-21881485
Uitnodiging
Graag nodig ik u en uw partner uit voor het feest ter gelegenheid van
mijn promotie
zaterdag 22 september 2007 vanaf 20.00 uur
“Oranjerie Landgoed Maarsbergen” Maarnse Grindweg 30 3953 LW Maarsbergen
tel. 0343-431 [email protected]
Paranimfen:Huub van der Heide, tel: 06-43001007
[email protected] van der Gragt, tel: 06-21881485
High Tibial Osteotomy Treatment of varus osteoarthritis of the knee
Robert D. A. Gaasbeek
High Tibial Osteotomy Treatment of varus osteoarthritis of the knee
Robert D. A. Gaasbeek
High Tibial Osteotomy Treatment of varus osteoarthritis of the knee
Robert D. A. Gaasbeek