Embed Size (px)
Citation preview

Cardiovascular Disease and Risk Factors in AsiaA Selected Review
Hirotsugu Ueshima, MD; Akira Sekikawa, MD; Katsuyuki Miura, MD;Tanvir Chowdhury Turin, MBBS; Naoyuki Takashima, MD; Yoshikuni Kita, PhD;
Makoto Watanabe, MD; Aya Kadota, MD; Nagako Okuda, MD; Takashi Kadowaki, MD;Yasuyuki Nakamura, MD; Tomonori Okamura, MD
Cardiovascular disease (CVD) prevention in Asia is animportant issue for world health, because half of the
world’s population lives in Asia. Asian countries and regionssuch as Japan, the Republic of Korea, the People’s Republicof China, Hong Kong, Taiwan, and the Kingdom of Thailandhave greater mortality and morbidity from stroke than fromcoronary heart disease (CHD), whereas the opposite is true inWestern countries.1 The reasons why this specific situation isobserved in countries with rapid and early-phase westerniza-tion, such as Japan and South Korea, are very interesting.
The Seven Countries Study conducted by Keys et al2 in1957 found that Japanese populations had lower fat intake,lower serum total cholesterol, and lower CHD than popula-tions in the United States and Scandinavia, in spite of highersmoking rates. The serum total cholesterol level in Japan hasincreased rapidly since World War II in accordance with anincrease in dietary fat intake from 10% of total energy intakeper capita per day to 25%.1,2 Despite this increase, thespecific characteristic of lower CHD incidence and mortalitythan that in Western countries has persisted.3,4 WhetherJapanese people and certain other Asian populations havedifferent risk factors for CHD than Western populations hasbeen a subject of discussion for quite some time.
In this article, we discuss the existence of higher strokerates and lower CHD rates in Asian countries than in Westerncountries and the respective risk factors for this on the basisof extensive reviews of cohort studies. We also discusswhether these risk factors differ from those of Westerncountries. Along with this, we examine the relationshipbetween serum total cholesterol and total stroke and itssubtypes. We also address the emerging problems and im-portant issues for CVD prevention in Asia.
An extensive article search for this review was performedwith a primary focus on cohort studies and researchers’names by country in Asia. For mortality data, statistics wereobtained from the World Health Organization.5
Mortality and Morbidity of Stroke and CHD
MortalityThe available data from the World Health Organization onage-adjusted mortality for men and women combined fromcerebrovascular disease (stroke) and CHD are shown inFigure 1.5 The left panel of Figure 1 shows age-adjustedstroke mortality for some selected Asian countries and someWestern countries, Australia, and New Zealand in 2002 forcomparison. In general, stroke mortality in Asian countriesexcept Japan and Singapore is higher than in Westerncountries; however, it is worth mentioning that Japan had thehighest stroke mortality in the world in 1965. It rapidlydecreased by �80% during the period from 1965 to 1990.1
The present stroke mortality rate in Japan is similar to that inWestern countries. Interestingly, stroke mortality trends inChina and South Korea now show similar characteristics tothe Japanese trend observed in the past. The recent age-adjusted stroke mortality rate in China is reported to bedecreasing in urban areas, whereas in rural areas, mortality isstill increasing or is stable.6 In South Korea, age-adjustedstroke mortality is also decreasing but remains at a higherlevel. Other Asian countries, including Middle Easterncountries, Central Asian countries, and South Asian coun-tries except Singapore, have higher stroke mortality thanWestern countries. Therefore, it can be concluded thatAsian countries in general have higher stroke mortalitythan Western countries.
For age-adjusted CHD mortality, it is of interest that EastAsian countries have lower mortality than other Asian coun-tries, except Thailand. As observed in the Seven CountriesStudy,2 East Asian countries still have lower CHD mortalitythan what is seen in Mediterranean countries.1,2 A largecohort study in China also confirmed that age-adjusted strokemortality was 3 times higher than CHD mortality.3 Therefore,it is a specific characteristic that East Asian countries have
From the Department of Health Science (H.U., A.S., K.M., T.C.T., N.T., Y.K., M.W., A.K., N.O., T.K., Y.N., T.O.), Shiga University of MedicalScience, Tsukinowa-cho Seta, Otsu, Shiga, Japan; Department of Epidemiology (A.S.), Graduate School of Pubic Health, University of Pittsburgh,Pittsburgh, Pa; Department of Preventive Cardiology (M.W., T.O.), National Cardiovascular Center, Suita, Osaka, Japan; and CardiovascularEpidemiology (Y.N.), Kyoto Women’s University, Kyoto, Japan.
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/cgi/content/full/118/25/2702/DC1.Correspondence to Hirotsugu Ueshima, MD, Department of Health Science, Shiga University of Medical Science, Tsukinowa-cho Seta, Otsu, Japan
520-2192. E-mail [email protected](Circulation. 2008;118:2702-2709.)© 2008 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.108.790048
2702
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
by guest on M
ay 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
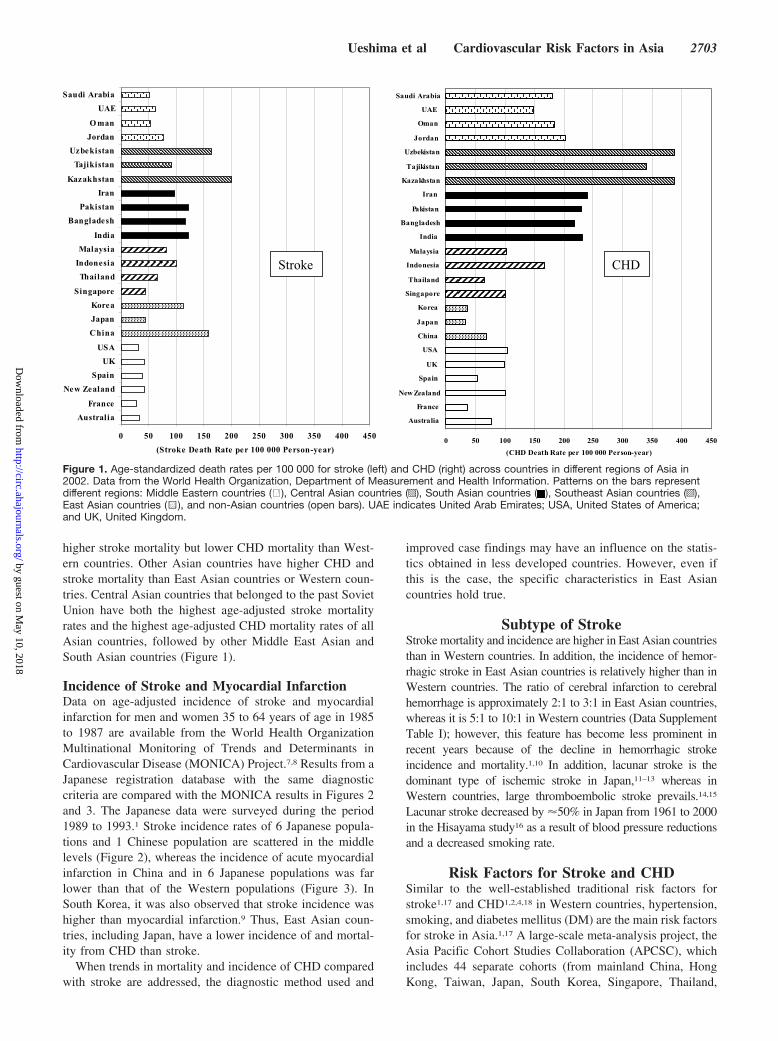
higher stroke mortality but lower CHD mortality than West-ern countries. Other Asian countries have higher CHD andstroke mortality than East Asian countries or Western coun-tries. Central Asian countries that belonged to the past SovietUnion have both the highest age-adjusted stroke mortalityrates and the highest age-adjusted CHD mortality rates of allAsian countries, followed by other Middle East Asian andSouth Asian countries (Figure 1).
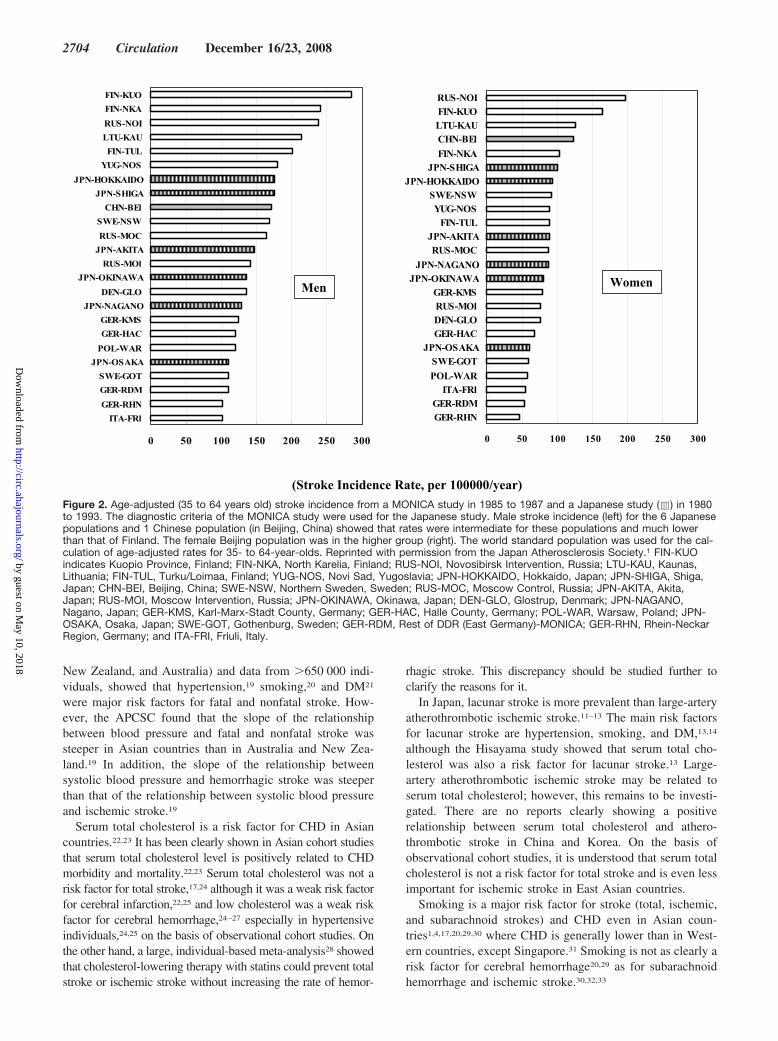
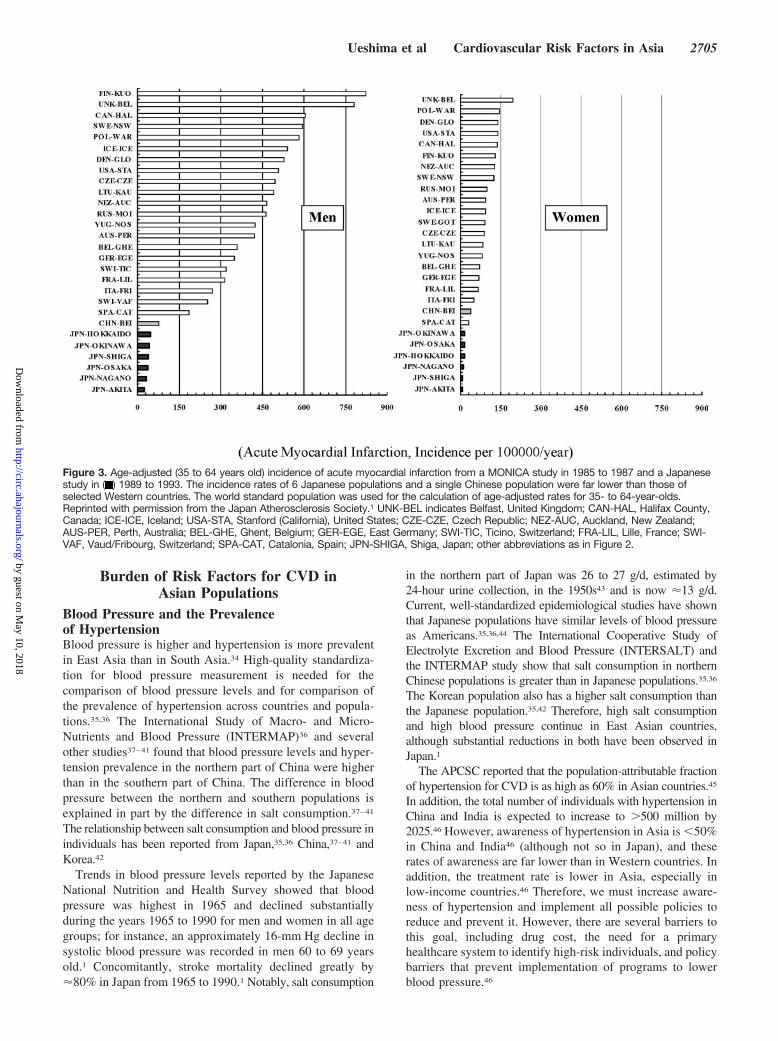
Incidence of Stroke and Myocardial InfarctionData on age-adjusted incidence of stroke and myocardialinfarction for men and women 35 to 64 years of age in 1985to 1987 are available from the World Health OrganizationMultinational Monitoring of Trends and Determinants inCardiovascular Disease (MONICA) Project.7,8 Results from aJapanese registration database with the same diagnosticcriteria are compared with the MONICA results in Figures 2and 3. The Japanese data were surveyed during the period1989 to 1993.1 Stroke incidence rates of 6 Japanese popula-tions and 1 Chinese population are scattered in the middlelevels (Figure 2), whereas the incidence of acute myocardialinfarction in China and in 6 Japanese populations was farlower than that of the Western populations (Figure 3). InSouth Korea, it was also observed that stroke incidence washigher than myocardial infarction.9 Thus, East Asian coun-tries, including Japan, have a lower incidence of and mortal-ity from CHD than stroke.
When trends in mortality and incidence of CHD comparedwith stroke are addressed, the diagnostic method used and
improved case findings may have an influence on the statis-tics obtained in less developed countries. However, even ifthis is the case, the specific characteristics in East Asiancountries hold true.
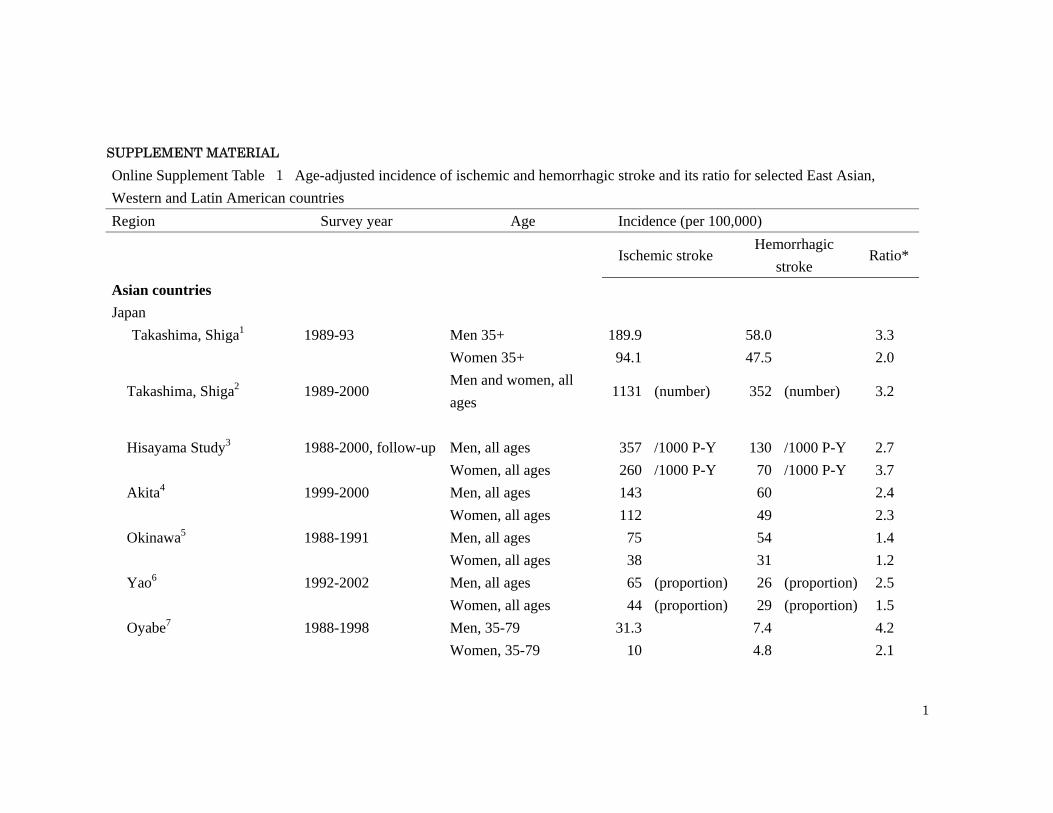
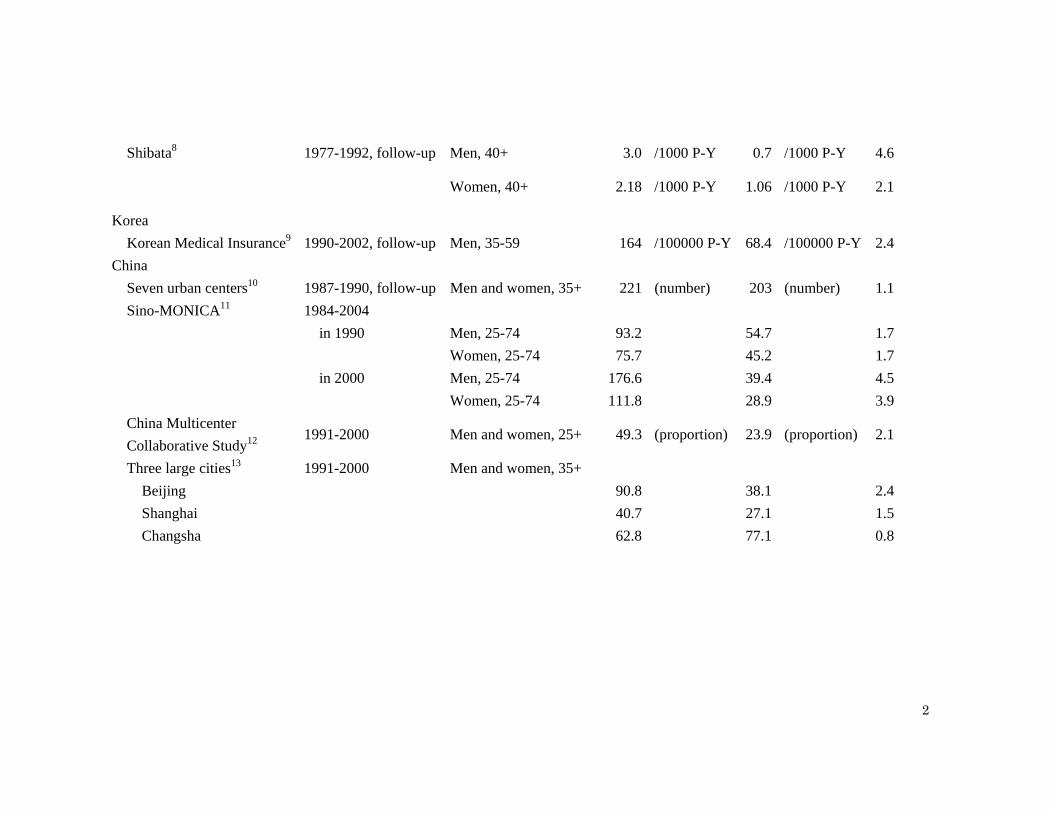
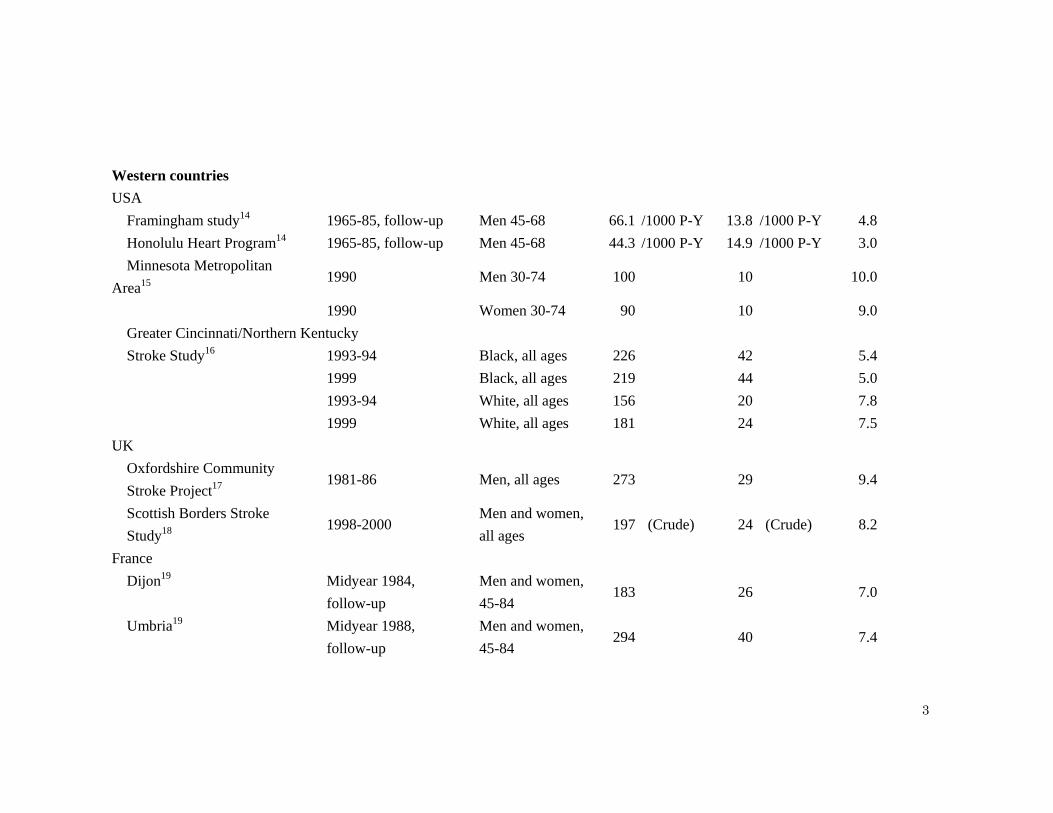
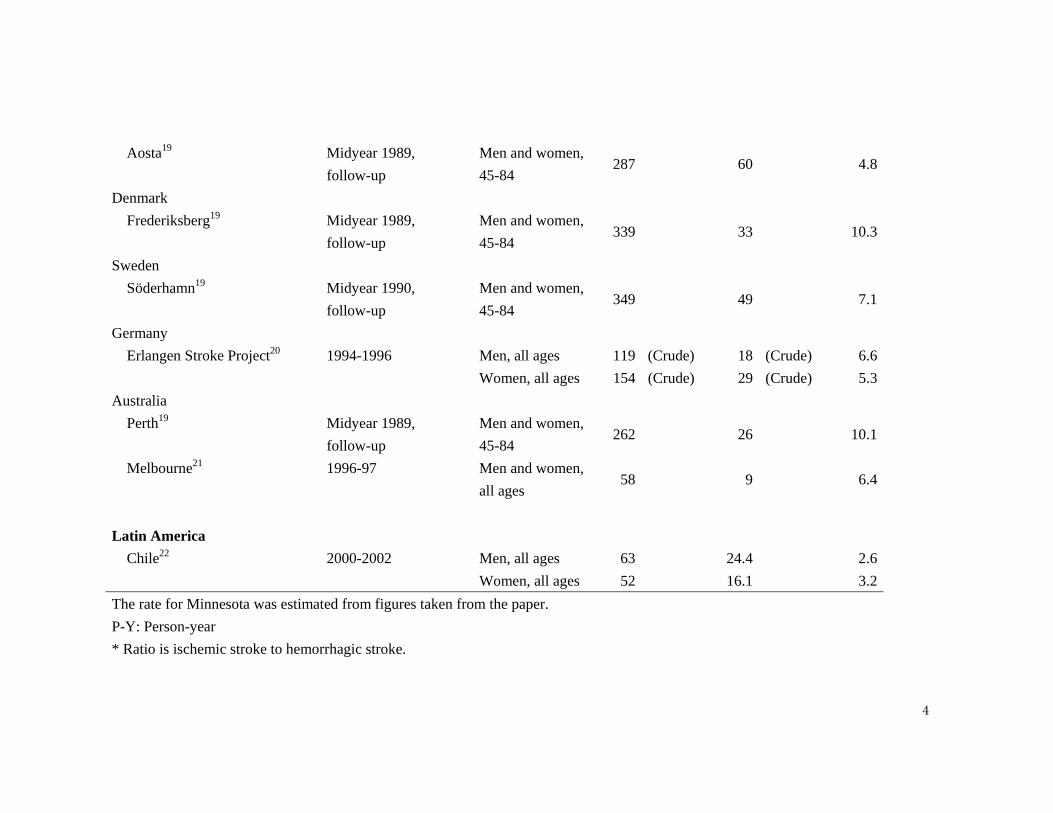
Subtype of StrokeStroke mortality and incidence are higher in East Asian countriesthan in Western countries. In addition, the incidence of hemor-rhagic stroke in East Asian countries is relatively higher than inWestern countries. The ratio of cerebral infarction to cerebralhemorrhage is approximately 2:1 to 3:1 in East Asian countries,whereas it is 5:1 to 10:1 in Western countries (Data SupplementTable I); however, this feature has become less prominent inrecent years because of the decline in hemorrhagic strokeincidence and mortality.1,10 In addition, lacunar stroke is thedominant type of ischemic stroke in Japan,11–13 whereas inWestern countries, large thromboembolic stroke prevails.14,15
Lacunar stroke decreased by �50% in Japan from 1961 to 2000in the Hisayama study16 as a result of blood pressure reductionsand a decreased smoking rate.
Risk Factors for Stroke and CHDSimilar to the well-established traditional risk factors forstroke1,17 and CHD1,2,4,18 in Western countries, hypertension,smoking, and diabetes mellitus (DM) are the main risk factorsfor stroke in Asia.1,17 A large-scale meta-analysis project, theAsia Pacific Cohort Studies Collaboration (APCSC), whichincludes 44 separate cohorts (from mainland China, HongKong, Taiwan, Japan, South Korea, Singapore, Thailand,
0 50 100 150 200 250 300 350 400 450
Australia
France
New Zealand
Spain
UK
USA
China
Japan
Korea
Singapore
Thailand
Indonesia
Malaysia
India
Bangladesh
Pakistan
Iran
Kazakhstan
Tajikistan
Uzbekistan
Jordan
O man
UAE
Saudi Arabia
(Stroke Death Rate per 100 000 Person-year)0 50 100 150 200 250 300 350 400 450
Australia
France
New Zealand
Spain
UK
USA
China
Japan
Korea
Singapore
Thailand
Indonesia
Malaysia
India
Bangladesh
Pakistan
Iran
Kazakhstan
Tajikistan
Uzbekistan
Jordan
Oman
UAE
Saudi Arabia
(CHD Death Rate per 100 000 Person-year)
Stroke CHD
Figure 1. Age-standardized death rates per 100 000 for stroke (left) and CHD (right) across countries in different regions of Asia in2002. Data from the World Health Organization, Department of Measurement and Health Information. Patterns on the bars representdifferent regions: Middle Eastern countries ( ), Central Asian countries (p), South Asian countries ( ), Southeast Asian countries (o),East Asian countries (1), and non-Asian countries (open bars). UAE indicates United Arab Emirates; USA, United States of America;and UK, United Kingdom.
Ueshima et al Cardiovascular Risk Factors in Asia 2703
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
New Zealand, and Australia) and data from �650 000 indi-viduals, showed that hypertension,19 smoking,20 and DM21
were major risk factors for fatal and nonfatal stroke. How-ever, the APCSC found that the slope of the relationshipbetween blood pressure and fatal and nonfatal stroke wassteeper in Asian countries than in Australia and New Zea-land.19 In addition, the slope of the relationship betweensystolic blood pressure and hemorrhagic stroke was steeperthan that of the relationship between systolic blood pressureand ischemic stroke.19
Serum total cholesterol is a risk factor for CHD in Asiancountries.22,23 It has been clearly shown in Asian cohort studiesthat serum total cholesterol level is positively related to CHDmorbidity and mortality.22,23 Serum total cholesterol was not arisk factor for total stroke,17,24 although it was a weak risk factorfor cerebral infarction,22,25 and low cholesterol was a weak riskfactor for cerebral hemorrhage,24–27 especially in hypertensiveindividuals,24,25 on the basis of observational cohort studies. Onthe other hand, a large, individual-based meta-analysis28 showedthat cholesterol-lowering therapy with statins could prevent totalstroke or ischemic stroke without increasing the rate of hemor-
rhagic stroke. This discrepancy should be studied further toclarify the reasons for it.
In Japan, lacunar stroke is more prevalent than large-arteryatherothrombotic ischemic stroke.11–13 The main risk factorsfor lacunar stroke are hypertension, smoking, and DM,13,14
although the Hisayama study showed that serum total cho-lesterol was also a risk factor for lacunar stroke.13 Large-artery atherothrombotic ischemic stroke may be related toserum total cholesterol; however, this remains to be investi-gated. There are no reports clearly showing a positiverelationship between serum total cholesterol and athero-thrombotic stroke in China and Korea. On the basis ofobservational cohort studies, it is understood that serum totalcholesterol is not a risk factor for total stroke and is even lessimportant for ischemic stroke in East Asian countries.
Smoking is a major risk factor for stroke (total, ischemic,and subarachnoid strokes) and CHD even in Asian coun-tries1,4,17,20,29,30 where CHD is generally lower than in West-ern countries, except Singapore.31 Smoking is not as clearly arisk factor for cerebral hemorrhage20,29 as for subarachnoidhemorrhage and ischemic stroke.30,32,33
0 50 100 150 200 250 300
ITA-FRl
GER-RHN
GER-RDM
SWE-GOT
JPN-OSAKA
POL-WAR
GER-HAC
GER-KMS
JPN-NAGANO
DEN-GLO
JPN-OKINAWA
RUS-MOl
JPN-AKITA
RUS-MOC
SWE-NSW
CHN-BEl
JPN-SHIGA
JPN-HOKKAIDO
YUG-NOS
FIN-TUL
LTU-KAU
RUS-NOI
FIN-NKA
FIN-KUO
0 50 100 150 200 250 300
GER-RHN GER-RDM
ITA-FRl POL-WAR
SWE-GOT JPN-OSAKA
GER-HAC DEN-GLO RUS-MOl GER-KMS
JPN-OKINAWAJPN-NAGANO
RUS-MOC JPN-AKITA
FIN-TUL YUG-NOS
SWE-NSW JPN-HOKKAIDO
JPN-SHIGAFIN-NKA
CHN-BEl LTU-KAU FIN-KUO RUS-NOI
(Stroke Incidence Rate, per 100000/year)
Men Women
Figure 2. Age-adjusted (35 to 64 years old) stroke incidence from a MONICA study in 1985 to 1987 and a Japanese study (d ) in 1980to 1993. The diagnostic criteria of the MONICA study were used for the Japanese study. Male stroke incidence (left) for the 6 Japanesepopulations and 1 Chinese population (in Beijing, China) showed that rates were intermediate for these populations and much lowerthan that of Finland. The female Beijing population was in the higher group (right). The world standard population was used for the cal-culation of age-adjusted rates for 35- to 64-year-olds. Reprinted with permission from the Japan Atherosclerosis Society.1 FIN-KUOindicates Kuopio Province, Finland; FIN-NKA, North Karelia, Finland; RUS-NOI, Novosibirsk Intervention, Russia; LTU-KAU, Kaunas,Lithuania; FIN-TUL, Turku/Loimaa, Finland; YUG-NOS, Novi Sad, Yugoslavia; JPN-HOKKAIDO, Hokkaido, Japan; JPN-SHIGA, Shiga,Japan; CHN-BEI, Beijing, China; SWE-NSW, Northern Sweden, Sweden; RUS-MOC, Moscow Control, Russia; JPN-AKITA, Akita,Japan; RUS-MOI, Moscow Intervention, Russia; JPN-OKINAWA, Okinawa, Japan; DEN-GLO, Glostrup, Denmark; JPN-NAGANO,Nagano, Japan; GER-KMS, Karl-Marx-Stadt County, Germany; GER-HAC, Halle County, Germany; POL-WAR, Warsaw, Poland; JPN-OSAKA, Osaka, Japan; SWE-GOT, Gothenburg, Sweden; GER-RDM, Rest of DDR (East Germany)-MONICA; GER-RHN, Rhein-NeckarRegion, Germany; and ITA-FRI, Friuli, Italy.
2704 Circulation December 16/23, 2008
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
Burden of Risk Factors for CVD inAsian Populations
Blood Pressure and the Prevalenceof HypertensionBlood pressure is higher and hypertension is more prevalentin East Asia than in South Asia.34 High-quality standardiza-tion for blood pressure measurement is needed for thecomparison of blood pressure levels and for comparison ofthe prevalence of hypertension across countries and popula-tions.35,36 The International Study of Macro- and Micro-Nutrients and Blood Pressure (INTERMAP)36 and severalother studies37–41 found that blood pressure levels and hyper-tension prevalence in the northern part of China were higherthan in the southern part of China. The difference in bloodpressure between the northern and southern populations isexplained in part by the difference in salt consumption.37–41
The relationship between salt consumption and blood pressure inindividuals has been reported from Japan,35,36 China,37–41 andKorea.42
Trends in blood pressure levels reported by the JapaneseNational Nutrition and Health Survey showed that bloodpressure was highest in 1965 and declined substantiallyduring the years 1965 to 1990 for men and women in all agegroups; for instance, an approximately 16-mm Hg decline insystolic blood pressure was recorded in men 60 to 69 yearsold.1 Concomitantly, stroke mortality declined greatly by�80% in Japan from 1965 to 1990.1 Notably, salt consumption
in the northern part of Japan was 26 to 27 g/d, estimated by24-hour urine collection, in the 1950s43 and is now �13 g/d.Current, well-standardized epidemiological studies have shownthat Japanese populations have similar levels of blood pressureas Americans.35,36,44 The International Cooperative Study ofElectrolyte Excretion and Blood Pressure (INTERSALT) andthe INTERMAP study show that salt consumption in northernChinese populations is greater than in Japanese populations.35,36
The Korean population also has a higher salt consumption thanthe Japanese population.35,42 Therefore, high salt consumptionand high blood pressure continue in East Asian countries,although substantial reductions in both have been observed inJapan.1
The APCSC reported that the population-attributable fractionof hypertension for CVD is as high as 60% in Asian countries.45
In addition, the total number of individuals with hypertension inChina and India is expected to increase to �500 million by2025.46 However, awareness of hypertension in Asia is �50%in China and India46 (although not so in Japan), and theserates of awareness are far lower than in Western countries. Inaddition, the treatment rate is lower in Asia, especially inlow-income countries.46 Therefore, we must increase aware-ness of hypertension and implement all possible policies toreduce and prevent it. However, there are several barriers tothis goal, including drug cost, the need for a primaryhealthcare system to identify high-risk individuals, and policybarriers that prevent implementation of programs to lowerblood pressure.46
Figure 3. Age-adjusted (35 to 64 years old) incidence of acute myocardial infarction from a MONICA study in 1985 to 1987 and a Japanesestudy in ( ) 1989 to 1993. The incidence rates of 6 Japanese populations and a single Chinese population were far lower than those ofselected Western countries. The world standard population was used for the calculation of age-adjusted rates for 35- to 64-year-olds.Reprinted with permission from the Japan Atherosclerosis Society.1 UNK-BEL indicates Belfast, United Kingdom; CAN-HAL, Halifax County,Canada; ICE-ICE, Iceland; USA-STA, Stanford (California), United States; CZE-CZE, Czech Republic; NEZ-AUC, Auckland, New Zealand;AUS-PER, Perth, Australia; BEL-GHE, Ghent, Belgium; GER-EGE, East Germany; SWI-TIC, Ticino, Switzerland; FRA-LIL, Lille, France; SWI-VAF, Vaud/Fribourg, Switzerland; SPA-CAT, Catalonia, Spain; JPN-SHIGA, Shiga, Japan; other abbreviations as in Figure 2.
Ueshima et al Cardiovascular Risk Factors in Asia 2705
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
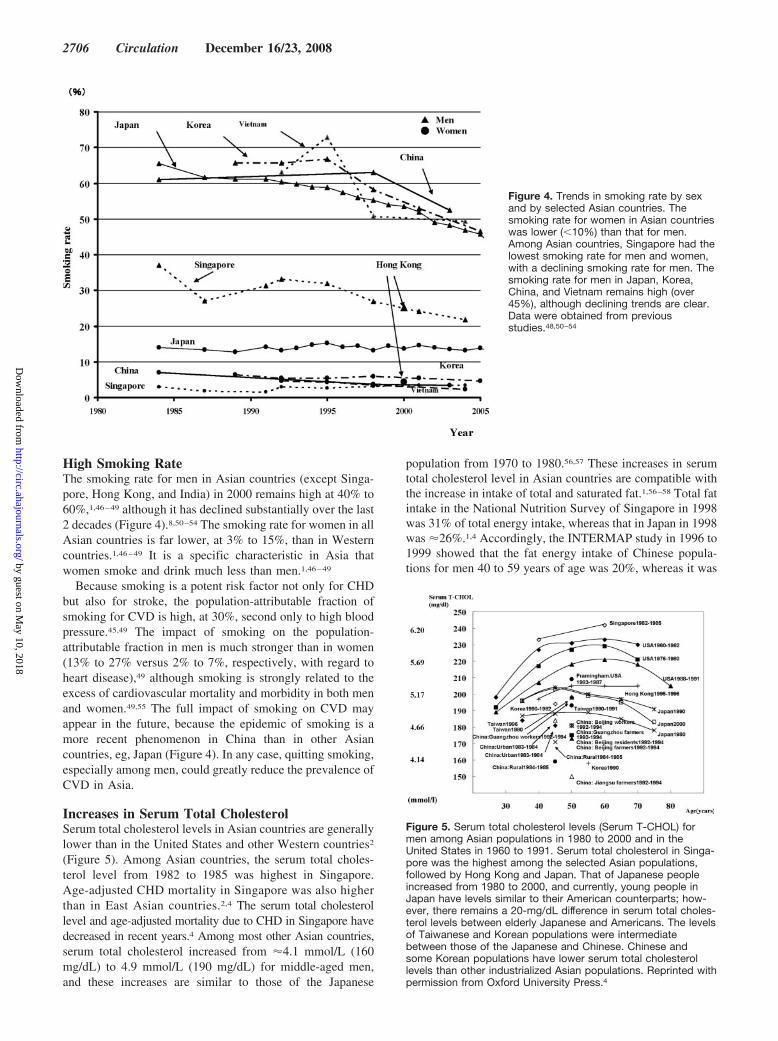
High Smoking RateThe smoking rate for men in Asian countries (except Singa-pore, Hong Kong, and India) in 2000 remains high at 40% to60%,1,46–49 although it has declined substantially over the last2 decades (Figure 4).8,50–54 The smoking rate for women in allAsian countries is far lower, at 3% to 15%, than in Westerncountries.1,46–49 It is a specific characteristic in Asia thatwomen smoke and drink much less than men.1,46–49
Because smoking is a potent risk factor not only for CHDbut also for stroke, the population-attributable fraction ofsmoking for CVD is high, at 30%, second only to high bloodpressure.45,49 The impact of smoking on the population-attributable fraction in men is much stronger than in women(13% to 27% versus 2% to 7%, respectively, with regard toheart disease),49 although smoking is strongly related to theexcess of cardiovascular mortality and morbidity in both menand women.49,55 The full impact of smoking on CVD mayappear in the future, because the epidemic of smoking is amore recent phenomenon in China than in other Asiancountries, eg, Japan (Figure 4). In any case, quitting smoking,especially among men, could greatly reduce the prevalence ofCVD in Asia.
Increases in Serum Total CholesterolSerum total cholesterol levels in Asian countries are generallylower than in the United States and other Western countries2
(Figure 5). Among Asian countries, the serum total choles-terol level from 1982 to 1985 was highest in Singapore.Age-adjusted CHD mortality in Singapore was also higherthan in East Asian countries.2,4 The serum total cholesterollevel and age-adjusted mortality due to CHD in Singapore havedecreased in recent years.4 Among most other Asian countries,serum total cholesterol increased from �4.1 mmol/L (160mg/dL) to 4.9 mmol/L (190 mg/dL) for middle-aged men,and these increases are similar to those of the Japanese
population from 1970 to 1980.56,57 These increases in serumtotal cholesterol level in Asian countries are compatible withthe increase in intake of total and saturated fat.1,56–58 Total fatintake in the National Nutrition Survey of Singapore in 1998was 31% of total energy intake, whereas that in Japan in 1998was �26%.1,4 Accordingly, the INTERMAP study in 1996 to1999 showed that the fat energy intake of Chinese popula-tions for men 40 to 59 years of age was 20%, whereas it was
Figure 4. Trends in smoking rate by sexand by selected Asian countries. Thesmoking rate for women in Asian countrieswas lower (�10%) than that for men.Among Asian countries, Singapore had thelowest smoking rate for men and women,with a declining smoking rate for men. Thesmoking rate for men in Japan, Korea,China, and Vietnam remains high (over45%), although declining trends are clear.Data were obtained from previousstudies.48,50–54
Figure 5. Serum total cholesterol levels (Serum T-CHOL) formen among Asian populations in 1980 to 2000 and in theUnited States in 1960 to 1991. Serum total cholesterol in Singa-pore was the highest among the selected Asian populations,followed by Hong Kong and Japan. That of Japanese peopleincreased from 1980 to 2000, and currently, young people inJapan have levels similar to their American counterparts; how-ever, there remains a 20-mg/dL difference in serum total choles-terol levels between elderly Japanese and Americans. The levelsof Taiwanese and Korean populations were intermediatebetween those of the Japanese and Chinese. Chinese andsome Korean populations have lower serum total cholesterollevels than other industrialized Asian populations. Reprinted withpermission from Oxford University Press.4
2706 Circulation December 16/23, 2008
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

24% for the Japanese population, 34% for the US population,and 33% for the United Kingdom population.36 The NationalNutrition Survey in South Korea58 showed that average fatintake per capita per day was 19% of total energy intake,which was lower than that in China and Japan.
Prevalence of Glucose Intolerance and DMGlucose intolerance and DM are risk factors for CHD andstroke in Asia, as in Western countries.17 However, Asianpopulations are presently less obese than Western popula-tions; the body mass index is approximately 20 to 24 kg/m2 inAsian but is 26 to 29 kg/m2 in the West.36,58 Because bodymass index is increasing in most Asian countries, the preva-lence of glucose intolerance and DM may increase further.APCSC results show that the hazard ratios of DM forischemic stroke and CHD are similar (�2) for both Asian andWestern countries.21
The prevalence of DM has been increasing throughoutAsia, and the speed of increase is much faster than in Westerncountries. The World Health Organization estimated that of171 million individuals with DM worldwide, �80 millionlived in Asia in 2000.59 The World Health Organizationprojects these numbers will double by the year 2030, with thegreatest increase in Asia. Therefore, we should carefullymonitor obesity trends in Asia that cause DM, metabolicsyndrome, or risk factor clustering for CVD.60
Migrant Studies on CVD, DM, and Atherosclerosisin Asian PopulationsMigrant studies of Asian populations to Western countriesgenerally show increases in CHD, type 2 DM, and athero-sclerosis. Migrant studies of Japanese in the United States, eg,the Honolulu Heart Program, show that Japanese Americanshave higher CHD rates than Japanese people living inJapan,61 whereas stroke rates in Japanese Americans arelower than in the Japanese in Japan and in whites.62 Likewise,migrant studies of Asian Indians show an increase in CHDamong those living in Western countries. Migrant Asianpopulations, including Chinese, Indians, and Japanese, have ahigher prevalence of type 2 DM not only when comparedwith their counterparts in their home countries but alsocompared with whites living in countries where Asians havemigrated.
A recent multiethnic study of 6700 men and women in theUnited States showed that the presence of coronary arterycalcification predicts future CHD similarly in whites andChinese Americans,63 although the latter have lower preva-lence and slower progression of coronary artery calcification.Among men in a post–World War II birth cohort, JapaneseAmericans and whites had a similarly high prevalence ofcoronary artery calcification that was significantly higherthan that in Japanese people living in Japan.64
ConclusionsIn Asian countries, stroke is more prominent than CHD. Thisis most likely due to a higher prevalence of hypertension anda lower level of serum total cholesterol in Asian countries.The population-attributable fraction of hypertension for CVDis as high as 60% in Asian countries. High blood pressure
accompanies high salt intake in East Asia, whereas low serumtotal cholesterol accompanies lower fat intake. Reduction insalt consumption in East Asian countries, including Japan, isimportant for the reduction of CVD, especially stroke. Pre-vention of smoking is also an important strategy for reducingCVD in most Asian countries, especially for men. Thepopulation-attributable fraction of smoking for CVD is�30%. Recent westernization in Asian countries has in-creased fat consumption, which has been followed by anincrease in serum total cholesterol. This may have caused theincrease in CHD in Asian countries. The prevalence ofobesity is also increasing, and this may also increase theprevalence of DM, glucose intolerance, and the metabolicsyndrome. Management of these traditional risk factors forCVD is important for the prevention of CVD in Asian andWestern countries.
AcknowledgmentsWe would like to express our appreciation to Takako Mihara andChiaki Masuda for their clerical assistance.
Sources of FundingThis research was supported by grants A 13307016 from theJapanese Ministry of Education, Culture, Sports, Science, andTechnology and R01 HL68200 and HL071561 from the NationalInstitutes of Health.
DisclosuresNone.
References1. Ueshima H. Explanation for the Japanese paradox: prevention of increase
in coronary heart disease and reduction in stroke. J Atheroscler Thromb.2007;14:278–286.
2. Coronary heart disease in Seven Countries: XVII: the diet. Circulation.1970;41(suppl I):I-162–I-183.
3. He J, Gu D, Wu X, Reynolds K, Duan X, Yao C, Wang J, Chen CS, ChenJ, Wildman RP, Klag MJ, Whelton PK. Major causes of death among menand women in China. N Engl J Med. 2005;353:1124–1134.
4. Ueshima H. Trends in Asia. In: Marmot M, Elliott P, eds. Coronary HeartDisease Epidemiology: From Aetiology to Public Health. 2nd ed. Oxford,United Kingdom: Oxford University Press; 2005:102–112.
5. WHO Statistical Information System. Causes of death: mortality andhealth status. WHO data and statistics. Available at: http://www.who.int/research/en/. Accessed February 10, 2008.
6. Zhang XH, Guan T, Mao J, Liu L. Disparity and its time trends in strokemortality between urban and rural populations in China 1987–2001:changing patterns and their implications for public health policy. Stroke.2007;38:3139–3144.
7. Thorvaldsen P, Asplund K, Kuulasmaa K, Rajakangas AM, Schroll M.Stroke incidence, case fatality, and mortality in the WHO MONICAProject. Stroke. 1995;26:361–367.
8. WHO MONICA Project. Myocardial infarction and coronary deaths inthe World Health Organization MONICA Project: registration pro-cedures, event rates, and case-fatality rates in 38 populations from 21countries in four continents. Circulation. 1994;90:583–612.
9. Jee SJ, Suh I, Kim IS, Appel LJ. Smoking and atherosclerosis cardiovas-cular disease in men with low levels of serum cholesterol: the KoreaMedical Insurance Corporation Study. JAMA. 1999;282:2149–2155.
10. Zhao D, Liu J, Wang W, Zeng Z, Cheng J, Liu J, Sun J, Wu Z.Epidemiological transition of stroke in China: twenty-one-year observa-tional study from the Sino-MONICA-Beijing Project. Stroke. 2008;39:1668–1674.
11. Kitamura A, Nakagawa Y, Sato M, Iso H, Sato S, Imano H, Kiyama M,Okada T, Iida M, Shimamoto T. Proportions of stroke subtypes amongmen and women �40 years of age in an urban Japanese city in 1992,1997, and 2002. Stroke. 2006;37:1374–1378.
Ueshima et al Cardiovascular Risk Factors in Asia 2707
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

12. Kimura K, Kazui S, Minematsu K, Ymaguchi T; for the Japan Multi-center Stroke Investigator’s Collaboration. Analysis of 16,922 patientswith acute ischemic stroke and transient ischemic attack in Japan: ahospital-based prospective registration study. Cerebrovasc Dis. 2004;18:47–56.
13. Tanizaki Y, Kiyohara Y, Kato I, Iwamoto H, Nakayama K, Shinohara N,Arima H, Tanaka K, Ibayashi S, Fujishima M. Incidence and risk factorsfor subtypes of cerebral infarction in a general population: the HisayamaStudy. Stroke. 2000;31:2616–2622.
14. Ohira T, Shahar E, Chambless LE, Rosamond WD, Mosley TH, FolsomAR. Risk factors for ischemic stroke subtypes: the Atherosclerosis Risk inCommunities Study. Stroke. 2006;37:2493–2498.
15. White H, Boden-Albala B, Wang C, Elkind MSV, Rundek T, Wright CB,Sacco RL. Ischemic stroke subtype incidence among whites, blacks, andHispanics: the Northern Manhattan Study. Circulation. 2005;111:1327–1331.
16. Kubo M, Kiyohara Y, Kato I, Tnizaki Y, Arima H, Tanaka K, NakamuraH, Okubo K, Iida M. Trends in the incidence, mortality, and survival rateof cardiovascular disease in a Japanese community: the Hisayama study.Stroke. 2003;34:2349–2354.
17. NIPPON DATA80 Research Group. Risk assessment chart for death fromcardiovascular disease based on a 19-year follow-up study of a Japaneserepresentative population. Circ J. 2006;70:1249–1255.
18. Stamler J. Established major coronary risk factors: historical overviews.In: Marmot M, Elliott P, eds. Coronary Heart Disease Epidemiology:From Aetiology to Public Health. 2nd ed. Oxford, United Kingdom:Oxford University Press; 2005:18–31.
19. Asia Pacific Cohort Studies Collaboration. Blood pressure and cardio-vascular disease in the Asia Pacific region. J Hypertens. 2003;21:707–716.
20. Asia Pacific Cohort Studies Collaboration. Smoking, quitting, and the riskof cardiovascular disease among women and men in the Asia-Pacificregion. Int J Epidemiol. 2005;34:1036–1045.
21. Asia Pacific Cohort Studies Collaboration. The effects of diabetes on therisks of major cardiovascular diseases and death in the Asia-Pacificregion. Diabetes Care. 2003;26:360–366.
22. Asia Pacific Cohort Studies Collaboration. Cholesterol, coronary heartdisease, and stroke in the Asia Pacific region. Int J Epidemiol. 2003;32:563–572.
23. Okamura T, Kadowaki T, Hayakawa T, Kita Y, Okayama A, Ueshima H;for the NIPPON DATA80 Research Group. What cause of mortality canwe predict by cholesterol screening in the Japanese general population?J Intern Med. 2003;253:169–180.
24. Prospective Studies Collaboration. Blood cholesterol and vascular mor-tality by age, sex, and blood pressure: a meta-analysis of individual datafrom 61 prospective studies with 55000 vascular deaths. Lancet. 2007;370:1829–1839.
25. Ebrahim S, Sung J, Song Y, Ferrer RL, Lawlor DA, Smith GD. Serumcholesterol, haemorrhagic stroke, ischemic stroke, and myocardialinfarction: Korean national health system prospective cohort study. BMJ.2006;333:22.
26. Ueshima H, Iida M, Shimamoto T, Konishi M, Tsujioka K, Tanigaki M,Nakanishi N, Ozawa H, Kojima S, Komachi Y. Multivariate analysis ofrisk factors for stroke: eight-year follow-up study of farming villages inAkita, Japan. Prev Med. 1980;9:722–740.
27. Okumura K, Iseki K, Wakugami K, Kimura Y, Muratani H, Ikemiya Y,Fukiyama K. Low serum cholesterol as a risk factor for hemorrhagicstroke in men: a community-based mass screening in Okinawa, Japan.Jpn Circ J. 1999;63:53–58.
28. Cholesterol Treatment Trials’ (CTT) Collaborators. Efficacy and safety ofcholesterol-lowering treatment: prospective meta-analysis of data from90056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278.
29. Ueshima H, Choudhury SR, Okayama A, Hayakawa T, Kita Y, KadowakiT, Okamura T, Minowa M, Iimura O; NIPPON DATA80 ResearchGroup. Cigarette smoking as a risk factor for stroke death in Japan:NIPPON DATA80. Stroke. 2004;35:1836–1841.
30. Iso H, Date C, Yamamoto A, Toyoshima H, Watanabe Y, Kikuchi S,Koizumi A, Wada Y, Kondo T, Inaba Y, Tamakoshi A; JACC StudyGroup. Smoking cessation and mortality from cardiovascular diseaseamong Japanese men and women: the JACC study. Am J Epidemiol.2005;161:170–179.
31. Khoo KL, Tan H, Liew YM, Janus DE. Lipid and coronary heart diseasein Asia. Atherosclerosis. 2003;169:1–10.
32. Feigen V, Prag V, Lawes CMM, Rodgers A, Suh I, Woodward M,Jamrozik K, Ueshima H; on behalf of the Asia Pacific Cohort StudiesCollaboration. Smoking and elevated blood pressure are the most importantrisk factors for subarachnoid hemorrhage in the Asia-Pacific Region: anoverview of 26 cohorts involving 306 620 participants. Circulation. 2005;36:1360–1365.
33. Mannami T, Iso H, Baba S, Sasaki S, Okada K, Konishi M, Tsugane S;for the Japan Public Health Center-Based Prospective Study on Cancerand Cardiovascular Disease Group. Cigarette smoking and risk of strokeand its subtypes among middle-aged Japanese men and women: the JPHCStudy Cohort I. Stroke. 2004;35:1248–1253.
34. Lawes CMM, Hoorn SV, Law MR, Elliott P, MacMahon S, Rodgers A.Blood pressure and the global burden of disease 2000: part 1: estimates ofblood pressure levels. J Hypertens. 2006;24:413–422.
35. INTERSALT Co-operative Research Group. Appendix tables: centre-specific results by age and sex. J Hum Hypertens. 1989;3:331–407.
36. Stamler J, Elliott P, Chan Q; for the INTERMAP Research Group.INTERMAP appendix tables. J Hum Hypertens. 2003;17:665–775.
37. Zhao L, Stamler J, Yan LL, Zhou B, Wu Y, Liu K, Daviglus ML, DennisBH, Elliott P, Ueshima H, Yang J, Zhu L, Guo D; for the INTERMAPResearch Group. Blood pressure differences between northern andsouthern Chinese: role of dietary factors: the International Study onMacronutrients and Blood Pressure. Hypertension. 2004;43:1332–1337.
38. Liu L, Mizushima S, Ikeda K, Hattori H, Miura A, Gao M, Nara Y,Yamori Y; on behalf of the China-Japan Cooperative Research Group ofthe WHO-CARDIAC Study. Comparative studies of diet-related factorsand blood pressure among Chinese and Japanese: results from theChina-Japan Cooperative Research of the WHO-CARDIAC Study.Hypertens Res. 2000;23:413–420.
39. Zhou B, Zhang X, Zhu A, Zhao L, Zhu S, Ruan L, Zhu L, Liang S. Therelationship of dietary animal protein and electrolytes to blood pressure:a study on three Chinese populations. Int J Epidemiol. 1994;23:716–722.
40. Liu LS, Xie JX, Fang WQ. Urinary cations and blood pressure: a collab-orative study of 16 districts in China. J Hypertens. 1988;6(suppl4):S587–S590.
41. Kesteloot H, Huang D, Li YL, Geboers J, Joossens JV. The relationshipbetween cations and blood pressure in the People’s Republic of China.Hypertension. 1987;9:654–659.
42. Kesteloot H, Park BC, Lee CS, Brems-Heyns E, Claessens J, Joossens JV.A comparative study of blood pressure and sodium intake in Belgium andin Korea. Eur J Cardiol. 1980;11:169–182.
43. Sasaki N. High blood pressure and salt intake of the Japanese. JpnHeart J. 1962;313–324.
44. Sekikawa A, Ueshima H, Kadowaki T, El-Saed A, Okamura T,Kashiwagi A, Edmundowicz D, Murata K, Sutton-Tyrrell K, Maegawa H,Evans RW, Kita Y, Kuller LH. Less subclinical atherosclerosis inJapanese men in Japan than in white men in the United States in thepost-World War II birth cohort. Am J Epidemiol. 2007;165:617–624.
45. Matriniuk ALC, Lee CMY, Lawes CMM, Ueshima H, Suh I, Lam TH,Gu D, Woodward M; for the Asia-Pacific Cohort Studies Collaboration.Hypertension: its prevalence and population-attributable fraction for mor-tality from cardiovascular disease in the Asia-Pacific region. J Hypertens.2007;25:73–79.
46. Perkovic V, Huxley R, Wu Y, Prabhakaran D, MacMahon S. The burdenof blood pressure-related disease: a neglected priority for global health.Hypertension. 2007;50:991–997.
47. World Health Organization. Tobacco. Available at: http://www.who.int/infobase/report.aspx?rid�112&ind�TOB. Accessed April 22, 2008.
48. Yang G, Fan L, Tan J, Qi G, Zhang Y, Samet JM, Taylor CE, Becker K,Xu J. Smoking in China: findings of the 1996 National PrevalenceSurvey. JAMA. 1999;282:1274–1253.
49. Matriniuk ALC, Lee CMY, Lam TH, Huxley R, Suh I, Jamrozik K, GuDF, Woodward M; for the Asia-Pacific Cohort Studies Collaboration.The fraction of ischaemic heart disease and stroke attributable to smokingin the WHO Western Pacific and South-East Asian regions. Tob Control.2006;15:181–188.
50. Morrow M, Barraclough S. Tobacco control and gender in south-eastAsia: part II: Singapore and Vietnam. Health Promot Int. 2003;18:373–380.
51. Yu JJ, Mattson ME, Boyd GM, Mueller MD, Shopland DR, Pechacek TF,Cullen JW. A comparison of smoking patterns in the People’s Republicof China with the United States: an impending health catastrophe in themiddle kingdom. JAMA. 1990;264:3149.
2708 Circulation December 16/23, 2008
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

52. Shi J, Liu M, Zhang Q, Lu M, Quan H. Male and female adult populationhealth status in China: a cross-sectional national survey. BMC PublicHealth. 2008;8:277.
53. Shafey O, Dolwick S, Guindon GE. Tobacco Control Country Profiles.2nd ed. Atlanta, Ga: American Cancer Society; 2003.
54. Organisation for Economic Co-operation and Development. OECDHealth Data 2008. Available at: http://www.oecd.org/document/16/0,3343,en_2649_34631_2085200_1_1_1_1,00.html. Accessed Sep-tember 1, 2008.
55. Hozawa A, Okamura T, Murakami Y, Kadota T, Nakamura K, HayakawaT, Kita Y, Nakamura Y, Abbott RD, Okayama A, Ueshima H; for theNIPPON DATA80 Research Group. Joint impact of smoking and hyper-tension on cardiovascular disease and all-cause mortality in Japan:NIPPON DATA80, a 19-year follow-up. Hypertens Res. 2007;30:1169–1175.
56. Ueshima H, Iida M, Shimamoto T, Konishi M, Tanigaki M, Doi M,Nakanishi N, Takayama Y, Ozawa H, Komachi Y. Dietary intake andserum total cholesterol level: their relationship to different lifestyles inseveral Japanese populations. Circulation. 1982;66:519–526.
57. Okayama A, Ueshima H, Marmot MG, Elliott P, Yamakawa M, Kita Y.Different trends in serum cholesterol levels among rural and urban pop-ulations aged 40–59 in Japan from 1960 to 1990. J Clin Epidemiol.1995;48:329–337.
58. Kim S, Moon S, Popkin BM. The nutrition transition in South Korea.Am J Clin Nutr. 2000;71:44–53.
59. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence ofdiabetes: estimates for the year 2000 and projections for 2030. DiabetesCare. 2004;27:1047–1053.
60. Gu D, Gupta A, Muntner P, Hu S, Duan X, Chen J, Reynolds RF,Whelton PK, He J. Prevalence of cardiovascular disease risk factorclustering among the adult population of China: results from the Inter-national Collaborative Study of Cardiovascular Disease in Asia(InterAsia). Circulation. 2005;112:658–665.
61. Yano K, Reed DM, McGee DL. Ten-year incidence of coronary heartdisease in the Honolulu Heart Program: relationship to biologic andlifestyle characteristics. Am J Epidemiol. 1984;119:653–666.
62. Kagan A, Popper JS, Rhoads GG. Factors related to stroke incidence inHawaii Japanese men: the Honolulu Heart Study. Stroke. 1980;11:14–21.
63. Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, Liu K,Shea S, Szklo M, Bluemke DA, O’Leary DH, Tracy R, Watson K, WongND, Kronmal RA. Coronary calcium as a predictor of coronary events infour racial or ethnic groups. N Engl J Med. 2008;358:1336–1345.
64. Sekikawa A, Curb JD, Ueshima H, El-Saed A, Kadowaki T, Abbott RD,Evans RW, Rodriguez BL, Okamura T, Sutton-Tyrrell K, Nakamura Y,Masaki K, Edmundowicz D, Kashiwagi A, Willcox BJ, Takamiya T,Mitsunami K, Seto TB, Murata K, White RL, Kuller LH. Marine-derivedn-3 fatty acids and atherosclerosis in Japanese, Japanese Americans, andwhites: a cross-sectional study. J Am Coll of Cardiol. 2008;52:417–424.
KEY WORDS: myocardial infarction � epidemiology � cerebrovascular disorders� stroke � risk factors
Ueshima et al Cardiovascular Risk Factors in Asia 2709
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

Kadowaki, Yasuyuki Nakamura and Tomonori OkamuraTakashima, Yoshikuni Kita, Makoto Watanabe, Aya Kadota, Nagako Okuda, Takashi
Hirotsugu Ueshima, Akira Sekikawa, Katsuyuki Miura, Tanvir Chowdhury Turin, NaoyukiCardiovascular Disease and Risk Factors in Asia: A Selected Review
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2008 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.108.790048
2008;118:2702-2709Circulation.
http://circ.ahajournals.org/content/118/25/2702World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2008/12/29/118.25.2702.DC1Data Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
1
SUPPLEMENT MATERIAL Online Supplement Table 1 Age-adjusted incidence of ischemic and hemorrhagic stroke and its ratio for selected East Asian, Western and Latin American countries Region Survey year Age Incidence (per 100,000)
Ischemic stroke Hemorrhagic
stroke Ratio*
Asian countries Japan Takashima, Shiga1 1989-93 Men 35+ 189.9 58.0 3.3
Women 35+ 94.1 47.5 2.0
Takashima, Shiga2 1989-2000 Men and women, all ages
1131 (number) 352 (number) 3.2
Hisayama Study3 1988-2000, follow-up Men, all ages 357 /1000 P-Y 130 /1000 P-Y 2.7 Women, all ages 260 /1000 P-Y 70 /1000 P-Y 3.7 Akita4 1999-2000 Men, all ages 143 60 2.4 Women, all ages 112 49 2.3 Okinawa5 1988-1991 Men, all ages 75 54 1.4 Women, all ages 38 31 1.2 Yao6 1992-2002 Men, all ages 65 (proportion) 26 (proportion) 2.5 Women, all ages 44 (proportion) 29 (proportion) 1.5 Oyabe7 1988-1998 Men, 35-79 31.3 7.4 4.2 Women, 35-79 10 4.8 2.1
2
Shibata8 1977-1992, follow-up Men, 40+ 3.0 /1000 P-Y 0.7 /1000 P-Y 4.6
Women, 40+ 2.18 /1000 P-Y 1.06 /1000 P-Y 2.1
Korea Korean Medical Insurance9 1990-2002, follow-up Men, 35-59 164 /100000 P-Y 68.4 /100000 P-Y 2.4 China Seven urban centers10 1987-1990, follow-up Men and women, 35+ 221 (number) 203 (number) 1.1 Sino-MONICA11 1984-2004 in 1990 Men, 25-74 93.2 54.7 1.7 Women, 25-74 75.7 45.2 1.7 in 2000 Men, 25-74 176.6 39.4 4.5 Women, 25-74 111.8 28.9 3.9
China Multicenter Collaborative Study12
1991-2000 Men and women, 25+ 49.3 (proportion) 23.9 (proportion) 2.1
Three large cities13 1991-2000 Men and women, 35+ Beijing 90.8 38.1 2.4 Shanghai 40.7 27.1 1.5 Changsha 62.8 77.1 0.8
3
Western countries USA Framingham study14 1965-85, follow-up Men 45-68 66.1 /1000 P-Y 13.8 /1000 P-Y 4.8 Honolulu Heart Program14 1965-85, follow-up Men 45-68 44.3 /1000 P-Y 14.9 /1000 P-Y 3.0 Minnesota Metropolitan Area15
1990 Men 30-74 100 10 10.0
1990 Women 30-74 90 10 9.0 Greater Cincinnati/Northern Kentucky Stroke Study16 1993-94 Black, all ages 226 42 5.4 1999 Black, all ages 219 44 5.0 1993-94 White, all ages 156 20 7.8 1999 White, all ages 181 24 7.5 UK Oxfordshire Community
Stroke Project17 1981-86 Men, all ages 273 29 9.4
Scottish Borders Stroke Study18
1998-2000 Men and women, all ages
197 (Crude) 24 (Crude) 8.2
France Dijon19 Midyear 1984,
follow-up Men and women, 45-84
183 26 7.0
Umbria19 Midyear 1988, follow-up
Men and women, 45-84
294 40 7.4
4
Aosta19 Midyear 1989, follow-up
Men and women, 45-84
287 60 4.8
Denmark Frederiksberg19 Midyear 1989,
follow-up Men and women, 45-84
339 33 10.3
Sweden Söderhamn19 Midyear 1990,
follow-up Men and women, 45-84
349 49 7.1
Germany Erlangen Stroke Project20 1994-1996 Men, all ages 119 (Crude) 18 (Crude) 6.6 Women, all ages 154 (Crude) 29 (Crude) 5.3 Australia Perth19 Midyear 1989,
follow-up Men and women, 45-84
262 26 10.1
Melbourne21 1996-97 Men and women, all ages
58 9 6.4
Latin America Chile22 2000-2002 Men, all ages 63 24.4 2.6 Women, all ages 52 16.1 3.2The rate for Minnesota was estimated from figures taken from the paper. P-Y: Person-year * Ratio is ischemic stroke to hemorrhagic stroke.
5
References:
1.Kita Y, Okayama A, Ueshima H, Wada M, Nozaki A, Choudhury SR, Bonita R,
Inamoto Y, Kasamatsu T. Stroke incidence and case fatality in Shiga, Japan 1989–1993.
Int J Epidemiol. 1999;28:1059–1065.
2. Turin TC, Kita Y, Murakami Y, Rumana N, Sugihara H, Morita Y, Nobuyoshi T,
Okayama A, Nakamura Y, Abbott RD, Ueshima H. Higher stroke incidence in the
spring season regardless of conventional risk factors: Takashima Stroke Registry,
Japan: 1988-2001. Stroke. 2008;39:745-752.
3. Kubo M, Kiyohara Y, Kato I, Tnizaki Y, Arima H, Tanaka K, Nakamura H, Okubo K,
Iida M. Trends in the incidence, mortality, and survival rate of cardiovascular disease
in a Japanese community: the Hisayama study. Stroke. 2003; 34:2349-54.
4. Nagura J, Suzuki K, Hayashi M, Sakamoto T, Shindo K, Oishi H, Hayashi K, Ozasa
K, Watanabe Y. Stroke subtypes and lesion sites in Akita, Japan. J Stroke Cerebrovasc
Dis. 2005; 14: 1 – 7.
5. Kimura Y, Takishita S, Muratani H, Kinjo K, Shinzato Y, Muratani A, Fukiyama K.
Demographic study of first-ever stroke and acute myocardial infarction in Okinawa,
Japan. Intern Med. 1998;37:736-745.
6. Kitamura A, Nakagawa Y, Sato M, Iso H, Sato S, Imano H, Kiyama M, Okada T,
Iida M, Shimamoto T. Proportions of stroke subtypes among men and women > or =40
6
years of age in an urban Japanese city in 1992, 1997, and 2002. Stroke. 2006;
37:1374-1378.
7. Miura K, Soyama Y, Morikawa Y, Nishijo M, Nakanishi Y, Naruse Y, Yoshita K,
Kagamimori S, Nakagawa H. Comparison of four blood pressure indexes for the
prediction of 10-year stroke risk in middle-aged and older Asians. Hypertension.
2004;44:715-20.
8. Nakayama T, Date C, Yokoyama T, Yoshiike N, Yamaguchi M, Tanaka H. A
15.5-year follow-up study of stroke in a Japanese provincial city. The Shibata Study.
Stroke. 1997;28:45-52.
9. Kim HC, Kang DR, Nam CM, Hur NW, Shim JS, Jee SH, Suh I. Elevated serum
aminotransferase level as a predictor of intracerebral hemorrhage: Korea medical
insurance corporation study. Stroke. 2005;36:1642-1647
10. Fang XH, Longstreth WT Jr, Li SC, Kronmal RA, Cheng XM, Wang WZ, Wu S,
Du XL, Dai XY. Longitudinal study of blood pressure and stroke in over 37,000 people
in China. Cerebrovasc Dis. 2001;11:225-229.
11. Zhao D, Liu J, Wang W, Zeng Z, Cheng J, Liu J, Sun J, WU Z. Epidemiological
transition of stroke in China. Twenty-one-year observational study from the
Sino-MONICA-Beijing Project. Stroke. 2008;39:1668-1674.
12. Zhang LF, Yang J, Hong Z, Yuan GG, Zhou BF, Zhao LC, Huang YN, Chen J, Wu
7
YF; Collaborative Group of China Multicenter Study of Cardiovascular Epidemiology.
Proportion of different subtypes of stroke in China. Stroke. 2003;34:2091-2096.
13. Jiang B, Wang WZ, Chen H, Hong Z, Yang QD, Wu SP, Du XL, Bao QJ. Incidence
and trends of stroke and its subtypes in China: results from three large cities. Stroke.
2006;37:63-68.
14. Rodriguez BL, D'Agostino R, Abbott RD, Kagan A, Burchfiel CM, Yano K, Ross
GW, Silbershatz H, Higgins MW, Popper J, Wolf PA, Curb JD. Risk of hospitalized
stroke in men enrolled in the Honolulu Heart Program and the Framingham Study: A
comparison of incidence and risk factor effects. Stroke. 2002;33:230-6.
15. Shahar E, McGovern PG, Pankow JS, Doliszny KM, Smith MA, Blackburn H,
Luepker RV. Stroke rates during the 1980s. The Minnesota Stroke Survey. Stroke.
1997;28:275-279.
16. Kleindorfer D, Broderick J, Khoury J, Flaherty M, Woo D, Alwell K, Moomaw CJ,
Schneider A, Miller R, Shukla R, Kissela B. The unchanging incidence and
case-fatality of stroke in the 1990s: a population-based study. Stroke.
2006;37:2473-2478.
17. Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. A prospective study of
acute cerebrovascular disease in the community: the Oxfordshire Community Stroke
Project--1981-86. 2. Incidence, case fatality rates and overall outcome at one year of
8
cerebral infarction, primary intracerebral and subarachnoid haemorrhage. J Neurol
Neurosurg Psychiatry. 1990;53:16-22.
18. Syme PD, Byrne AW, Chen R, Devenny R, Forbes JF. Community-based stroke
incidence in a Scottish population: the Scottish Borders Stroke Study. Stroke.
2005;36:1837-1843.
19. Sudlow CLM, Warlow CP. Comparable studies of the incidence of stroke and its
pathological types: results from an international collaboration. International Stroke
Incidence Collaboration. Stroke. 1997;28:491-499.
20. Kolominsky-Rabas PL, Sarti C, Heuschmann PU, Graf C, Siemonsen S,
Neundoerfer B, Katalinic A, Lang E, Gassmann KG, von Stockert TR. A prospective
community-based study of stroke in Germany--the Erlangen Stroke Project (ESPro):
incidence and case fatality at 1, 3, and 12 months. Stroke. 1998;29:2501-2506.
21. Thrift AG, Dewey HM, Macdonell RA, McNeil JJ, Donnan GA. Incidence of the
major stroke subtypes: initial findings from the North East Melbourne stroke incidence
study (NEMESIS). Stroke. 2001;32:1732-1738.
22. Lavados PM, Sacks C, Prina L, Escobar A, Tossi C, Araya F, Feuerhake W, Galvez
M, Salinas R, Alvarez G. Incidence, 30-day case-fatality rate, and prognosis of stroke
in Iquique, Chile: a 2-year community-based prospective study (PISCIS project).
Lancet. 2005;365:2206-2215.





























