Embed Size (px)
Citation preview
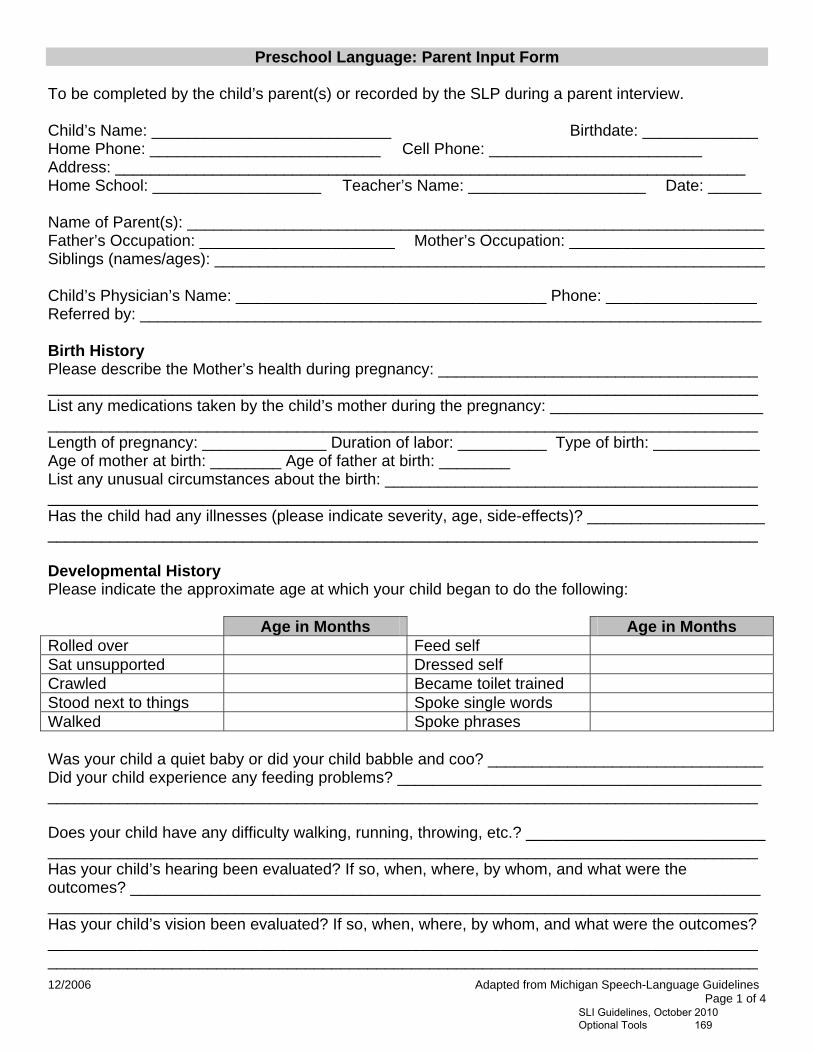
12/2006 Adapted from Michigan Speech-Language Guidelines Page 1 of 4
Preschool Language: Parent Input Form
To be completed by the child’s parent(s) or recorded by the SLP during a parent interview. Child’s Name: ___________________________ Birthdate: _____________ Home Phone: __________________________ Cell Phone: ________________________ Address: _______________________________________________________________________ Home School: ___________________ Teacher’s Name: ____________________ Date: ______ Name of Parent(s): _________________________________________________________________ Father’s Occupation: ______________________ Mother’s Occupation: ______________________Siblings (names/ages): ______________________________________________________________ Child’s Physician’s Name: ___________________________________ Phone: _________________ Referred by: ______________________________________________________________________ Birth History Please describe the Mother’s health during pregnancy: ____________________________________ ________________________________________________________________________________ List any medications taken by the child’s mother during the pregnancy: ________________________ ________________________________________________________________________________ Length of pregnancy: ______________ Duration of labor: __________ Type of birth: ____________ Age of mother at birth: ________ Age of father at birth: ________ List any unusual circumstances about the birth: __________________________________________ ________________________________________________________________________________ Has the child had any illnesses (please indicate severity, age, side-effects)? ____________________ ________________________________________________________________________________ Developmental History Please indicate the approximate age at which your child began to do the following:
Age in Months Age in Months Rolled over Feed self Sat unsupported Dressed self Crawled Became toilet trained Stood next to things Spoke single words Walked Spoke phrases Was your child a quiet baby or did your child babble and coo? _______________________________ Did your child experience any feeding problems? _________________________________________ ________________________________________________________________________________ Does your child have any difficulty walking, running, throwing, etc.? ___________________________ ________________________________________________________________________________ Has your child’s hearing been evaluated? If so, when, where, by whom, and what were the outcomes? _______________________________________________________________________ ________________________________________________________________________________ Has your child’s vision been evaluated? If so, when, where, by whom, and what were the outcomes? ________________________________________________________________________________ ________________________________________________________________________________
SLI Guidelines, October 2010 Optional Tools 169
12/2006 Adapted from Michigan Speech-Language Guidelines Page 2 of 4
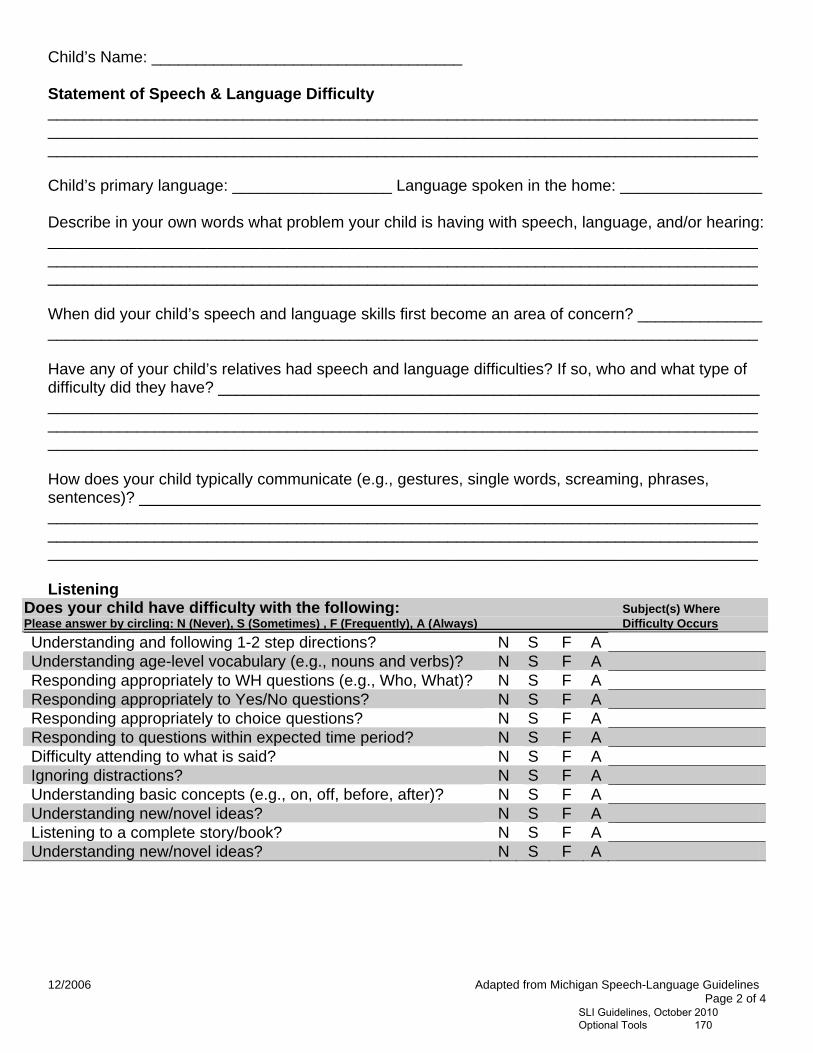
Child’s Name: ___________________________________ Statement of Speech & Language Difficulty ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ Child’s primary language: __________________ Language spoken in the home: ________________ Describe in your own words what problem your child is having with speech, language, and/or hearing: ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ When did your child’s speech and language skills first become an area of concern? ______________ ________________________________________________________________________________ Have any of your child’s relatives had speech and language difficulties? If so, who and what type of difficulty did they have? _____________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ How does your child typically communicate (e.g., gestures, single words, screaming, phrases, sentences)? ______________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ Listening
Does your child have difficulty with the following: Subject(s) Where Please answer by circling: N (Never), S (Sometimes) , F (Frequently), A (Always) Difficulty Occurs
Understanding and following 1-2 step directions? N S F A Understanding age-level vocabulary (e.g., nouns and verbs)? N S F A Responding appropriately to WH questions (e.g., Who, What)? N S F A Responding appropriately to Yes/No questions? N S F A Responding appropriately to choice questions? N S F A Responding to questions within expected time period? N S F A Difficulty attending to what is said? N S F A Ignoring distractions? N S F A Understanding basic concepts (e.g., on, off, before, after)? N S F A Understanding new/novel ideas? N S F A Listening to a complete story/book? N S F A Understanding new/novel ideas? N S F A
SLI Guidelines, October 2010 Optional Tools 170
12/2006 Adapted from Michigan Speech-Language Guidelines Page 3 of 4
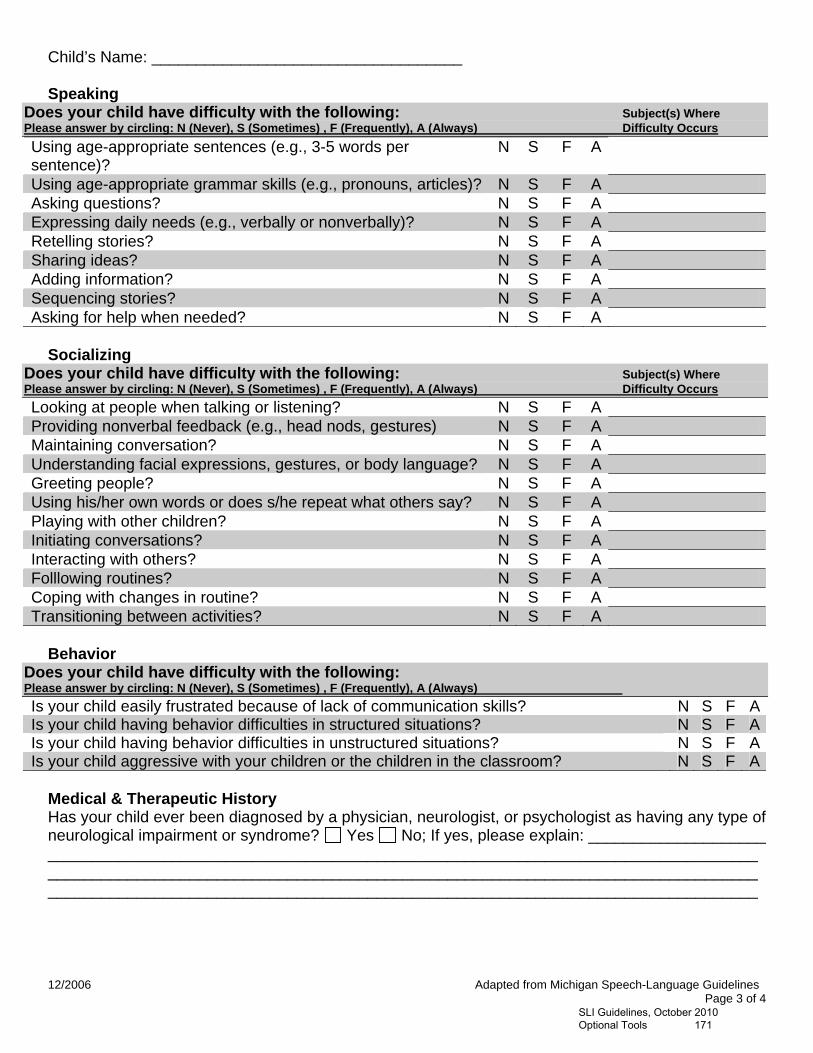
Child’s Name: ___________________________________ Speaking
Does your child have difficulty with the following: Subject(s) Where Please answer by circling: N (Never), S (Sometimes) , F (Frequently), A (Always) Difficulty Occurs
Using age-appropriate sentences (e.g., 3-5 words per sentence)?
N S F A
Using age-appropriate grammar skills (e.g., pronouns, articles)? N S F A Asking questions? N S F A Expressing daily needs (e.g., verbally or nonverbally)? N S F A Retelling stories? N S F A Sharing ideas? N S F A Adding information? N S F A Sequencing stories? N S F A Asking for help when needed? N S F A
Socializing
Does your child have difficulty with the following: Subject(s) Where Please answer by circling: N (Never), S (Sometimes) , F (Frequently), A (Always) Difficulty Occurs
Looking at people when talking or listening? N S F A Providing nonverbal feedback (e.g., head nods, gestures) N S F A Maintaining conversation? N S F A Understanding facial expressions, gestures, or body language? N S F A Greeting people? N S F A Using his/her own words or does s/he repeat what others say? N S F A Playing with other children? N S F A Initiating conversations? N S F A Interacting with others? N S F A Folllowing routines? N S F A Coping with changes in routine? N S F A Transitioning between activities? N S F A
Behavior
Does your child have difficulty with the following: Please answer by circling: N (Never), S (Sometimes) , F (Frequently), A (Always)
Is your child easily frustrated because of lack of communication skills? N S F AIs your child having behavior difficulties in structured situations? N S F AIs your child having behavior difficulties in unstructured situations? N S F AIs your child aggressive with your children or the children in the classroom? N S F A
Medical & Therapeutic History Has your child ever been diagnosed by a physician, neurologist, or psychologist as having any type of neurological impairment or syndrome? Yes No; If yes, please explain: ____________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________
SLI Guidelines, October 2010 Optional Tools 171

12/2006 Adapted from Michigan Speech-Language Guidelines Page 4 of 4
Child’s Name: ___________________________________ Please list any evaluations or therapies that your child has had and their outcomes (i.e., speech, occupational therapy, physical therapy, neurological examinations, MRI, etc.):
Evaluation/Therapy Date Started Date Ended Outcome
Please list any medications your child takes at home and/or during the school day:
Medication Amount Prescribed/ How Often (e.g., 15 mg, 2X/day)
Taken at Home/School
For what condition? (e.g., ADD, Seizures)
Does your child have any known allergies? If so, please explain: _____________________________ ________________________________________________________________________________ Additional Comments: ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ _________________________________________ __________________________ Parent Signature Date
SLI Guidelines, October 2010 Optional Tools 172





























