Embed Size (px)
Citation preview
Central Annals of Otolaryngology and Rhinology
Cite this article: Salturk Z, Akdağ K, Atar Y, Uyar Y, Doğan MÖ, et al. (2016) Primary Localized Amyloidosis in Nasopharynx: A rare case. Ann Otolaryngol Rhinol 3(2): 1091.
*Corresponding author
Ziya Salturk, Department of Otolaryngology, Okmeydanı Training and Research Hospital ENT Clinic, Turkey, Email:
Submitted: 30 December 2015
Accepted: 15 January 2016
Published: 03 February 2016
ISSN: 2379-948X
Copyright© 2016 Salturk et al.
OPEN ACCESS
Keywords• Nasopharynx• Amyloidosis• Surgical excision• Otitis media with effusion
Case Report
Primary Localized Amyloidosis in Nasopharynx: A rare caseZiya Salturk*, Kamil Akdağ, Yavuz Atar, Yavuz Uyar, Mehmet Önder Doğan, Muzaffer İnan, Yusuf ÖztürkçüDepartment of Otolaryngology, Okmeydanı Training and Research Hospital ENT Clinic, Turkey
Abstract
Amyloidos is defined a sex tracellular deposition of fibrillary protein material. It is generally a sytemic disease but localized form can be seen. Sinonasal region is an a typical localization for amyloidosis. We describe a 53 years old male patient who presented with unilateral middle ear effusion and diagnosed as nasopharyngeal amyloidosis. Our patient was treated by surgical excision.
INTRODUCTIONAmyloidosis is a syndrome characterized bydeposition of
insoluble proteinous material in extracellulary matrix. It can be systemicor localized [1]. Localized amyloidosis is a rare condition and larynx is the most common organ effected in head and neck region. There has been 25 cases of sinonasal amyloidosis published in literatureso far [2,3].
We present a case of localized nasopharyngeal amyloidosis which presented with unilateral hearing loss.
CASE 53 years old male patient applied to outpatient clinic with
rightsided tinnitus and hearing loss that had lasted for 6 months. He did not have any additional symptom related to upper air way structures and no history of any systemic ilness or drug usage existed. Otoscopical examination and audio logical study detected right sided otitis media with effusion. Tympanometric study concluded type B tympanograph, and pure tone audiometry comfirmed 35 decibel air-bone gap. Nasopharyngeal examination via endoscopy revealed a mass lesion filled Rosenmuller fossa fully and biopsy was taken. As the age of the patient was not young angiofibroma was excluded from differential diagnosis. Nasopharyngeal carcinoma, meta static disease, and lymphoid hyperplasia due to allergic rhinitisor local inflammation were the diagnosis assumed. Histopathological evaluation diagnosed amyloidosis. It was AA; subepithelial, extracellular, a cellular, amorphous, eosinophilic material which was dispersed randomly through out the laminapropria, sparing the over lying epithelium, and frequently demonstrated a perivascular and periglandular deposition, sometimes completely obliterating the seromucous glands by compression atrophy. A sparse in flammatory in filtrate noted in all cases was composed of lymphocytes and plasmacells with occasional histiocytes and a few giant cells, either at the peripheral margin of or enclosed with in the amyloid. In order to
asses whether it was a part of systemic disease, internal medicine and hematology consultaions were performed. Consultations revealed that there was no renal disease. It was assesed by urea creatin in levels and creatin in clearance test. Multiple myeloma was excluded by protein electrophoresis. After it was comfirmed that there was no suspicion of systemic amyloidosis, patient was treated by endoscopicalescision of the lesion and insertion of ventilation tube.
DISCUSSIONAmyloidosis is deposition of fibrillary proteinous material in
extracellulary matrix in different organs and it has 2 sub groups named AL and AA chemically [4,5]. AL is seen in primary systemic amyloidosis and AA is in secondary systemic amyloidosis [6]. Amyloidosis has systemic and localized forms clinically. Sytemic form has 3 sub groups named primary, secondary, and familial [7]. AA is the most common type seen in inflammatory and neoplastic diseases [8].
Amyloidosis is seen generally seen between 4th and 8th decades and more common in males [9]. Larynx is the most common site effected in head and neck region and followed by salivary glands, orbita, and paranasal sinuses [9,10]. In contrast to systemic forms, gender and age don’t differ in localized form [11].
Nasopharyngeal amyloidosis is a slowly progressing condition which presents by epistaxis, nasal obstruction, and hearing loss due to otitis media with effusion. As these are non spesific symptoms, endoscopical examination and radiological evaluation are crucial. Certain diagnosis is made by histopathological examination [9,12]. Typical green biref ringence is detected under a polarized light microscope followings taining by congored [13].
Surgery is the definitive treatment for locaized nasopharyngeal amyloidosis [4]. Open surgery is difficult to perform because of the location of nasopharynx. Therefore endoscopialc approach
Central
Salturk et al. (2016)Email:
Ann Otolaryngol Rhinol 3(2): 1091 (2016) 2/2
Salturk Z, Akdağ K, Atar Y, Uyar Y, Doğan MÖ, et al. (2016) Primary Localized Amyloidosis in Nasopharynx: A rare case. Ann Otolaryngol Rhinol 3(2): 1091.
Cite this article
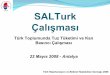
has replaced tranpalatal surgery. Bleeding is the most common and important complication of the surgery and endoscopical approach causes less bleeding [14]. We preferred endoscopical approach in our case (Figure 1).
Effects of surgery on prognosis is not known exactly and it is not certain if localized form evolved to systemic form. Regarding the high recurrence rate and risk of development of systemic disease, close followup should be performed [4,15]. This was an important case because localized amyloidosis is very rarely seen in nasopharynx and surgical treatment enabled definitive treatment in our case.
REFERENCES1. Zindanci I, Kocatürk E, Koç M, Büyükbabani N, Kavala M. A case
of biphasic amyloidosis: response to narrow band UVB. Türkiye Klinikleri J Dermatol. 2006; 16: 76-80.
2. Sadeqhipour A, Mirzaie AZ, Mohammadi SH, Nilipour Y. Primary localized amyloidosis in a child, a rarecasereport. Int J Pediatr Otorhinolaryngol. 2011; 6: 310-312.
3. Panda NK, Saravanan K, Purushotaman GP, Gurunathan RK, Mahesha V. Localized amyloidosis masquerading as nasopharyngeal tumor: a review. Am J Otolaryngol. 2007; 28: 208-211.
4. Tsikoudas A, Martin-Hirsch DP, Wood head CJ. Primary sinonasal amyloidosis. J Laryngol Otol. 2001; 115: 55-56.
5. Ünal R, Sesen T, Özdemir E, Erkilet E, Kandemir B, Süllü Y. Lingual amyloidosis. J Exp Clin Med. 2009; 26: 193-195.
6. Thompson LD, Derringer GA, Wenig BM. Amyloidosis of the larynx: a clinicopathologic study of 11 cases. Mod Pathol. 2000; 13: 528-535.
7. Simpson GT, Strong MS, Skinner M, Cohen AS. Localized amyloidosis of the head and neck and upper aerodigestive and lower respiratory tracts. Ann Otol Rhinol Laryngol. 1984; 93: 374-379.
8. Hegarty JL, Rao VM. Amyloidoma of the nasopharynx: CT and MR findings. AJNR Am J Neuroradiol. 1993; 14: 215-218.
9. Patel A, Pambuccian S, Maisel R. Nasopharyngeal amyloidosis. Am J Otolaryngol. 2002; 23: 308-311.
10. Nakayama T, Otori N, Komori M, Takayanagi H, Moriyama H. Primary localized amyloidosis of the nose. Auris Nasus Larynx. 2012; 39: 107-109.
11. Mufarrij AA, Busaba NY, Zaytoun GM, Gallo GR, Feiner HD. Primary localized amyloidosis of the nose and paranasal sinuses. A case report with immunohistochemical observations and a review of the literature. Am J Surg Pathol. 1990; 14: 379-383.
12. Pang KP, Chee LW, Busmanis I. Amyloidoma of the nose in a pediatric patient: a case report. Am J Otolaryngol. 2001; 22: 138-141.
13. Röcken C, Sletten K. Amyloid in surgical pathology. Virchows Arch. 2003; 443: 3-16.
14. Sass SMG, Pinto MC, Campos DS, Meada CAS, Mello PF. Localized nasopharyngeal amyloidosis. Int Arch Otolaryngol. 2009; 13: 207-210.
15. Lim JS, Lebowitz RA, Jacobs JB. Primary amyloidosis presenting as a nasopharyngeal mass. Am J Rhinol. 1999; 13: 209-212.
Figure 1 Endoscopical image of amyloidosis filled Rosenmuller fossa.