Embed Size (px)
DESCRIPTION
useful
Citation preview

NOSOCOMIAL CRYPTOSPORIDIUM INFECTION
Presented By
Dr. Keerthi Guntur Medical College
INTRODUCTION• Nosocomial infection comes from
Greek words “nosus” meaning disease and “ komeion” meaning to take care of
• Also called as HOSPITAL ACQUIRED INFECTION or HEALTHCARE-ASSOCIATED INFECTIONS(HAI).
DEFINITION
• Nosocomial infections are infections which are a result of treatment in a hospital or a healthcare service unit, but secondary to the patient's original condition.
• Infections are considered nosocomial if they first appear 48 hours or more after hospital admission or within 30 days after discharge.
Nosocomial parasitic infectionsEndoparasites1. Intestinal Protozoa -Entamoeba histolytica -Giardia lamblia -Cryptosporidium parvum2.Blood&tissue protozoa -Plasmodium spp -Toxoplasma gondii -Babesia spp -Leishmania spp -Trypanosoma spp
..contd
3.Helminths -Ascaris lumbricoides -Enterobius vermicularis -Strongyloides stercoralis -Taenia solium
Ectoparasites -Sarcoptes scabeii
Cryptosporidium parvum: an emerging pathogen
•Cryptosporidium is a coccidian protozoan parasite( Sporozoa)
•First reported in humans in 1976 in 3yr old girl.
• Increasing population of immunocompromised persons and waterborne outbreaks of cryptosporidiosis
•Little is known about the pathogenesis of the parasite
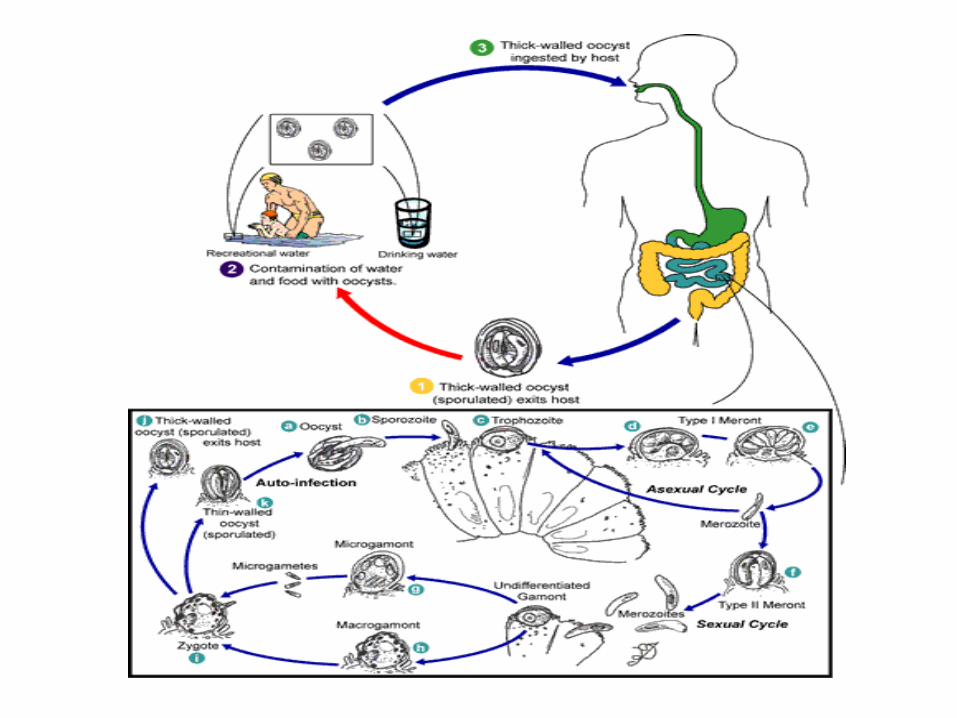
Life Cycle •Complex monoxenous life cycle--completing its entire cycle within a single host with both sexual and asexual cycles, and there are six distinct developmental stages
•Excystation of the orally ingested oocyst in the small bowel with release of the four sporozoites
•Invasion of intestinal epithelial cells initiation of the asexual intracellular multiplication stage
•Differentiation of microgametes and macrogametes
•Fertilization initiating sexual replication & Development of oocysts •The formation of new, infectious sporozoites within the oocyst, which is then excreted in the stool

Cryptosporidium parvum – Life cycle
Auto-InfectiveCycle
Thick-walled
Thin-walled
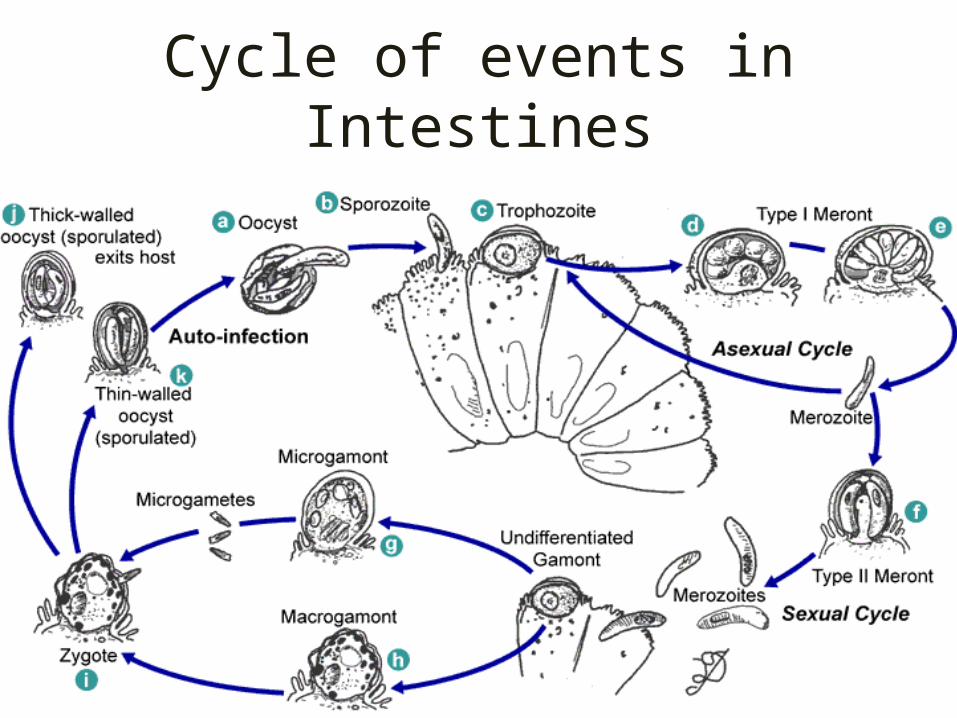
Cycle of events in Intestines
Clinical manifestationsIn immunocompetent patients
Cryptosporidiosis is an acute, yet self-limiting diarrheal illness (1-2 week duration), and symptoms include (Juranek, 1995):
Frequent, watery diarrhea Nausea Vomiting Abdominal cramps Low-grade fever
For immunocompromised persons
Illness is much more severe (Juranek, 1995):
Debilitating, cholera-like diarhoea (up to 20 liters/day) Severe abdominal cramps Malaise Low-grade fever Weight loss Anorexia
C. parvum infection has also been identified in the biliary tract (causing thickening of the gallbladder wall) and the respiratory system.
Respiratory cryptosporidiosis occurs in AIDS patients.
Transmission through surgical equipment especially ENDOSCOPES is often implicated.
Persons who have progressed from colonization to infection may represent only the “tip of iceberg” of persons carrying a particular pathogen.
50% infective dose (ID50) of C. parvum is only 132 oocysts
Epidemiology
Epidemiology Contd.
Person to person transmission through feco-oral route
Infants and younger children in Paediatric and Neonatal wards, Day care centres.
In children hospitalized for diarrhea C. parvum infection occurs most frequently in malnourished children.
Immunocompromised patients are at higher risk.
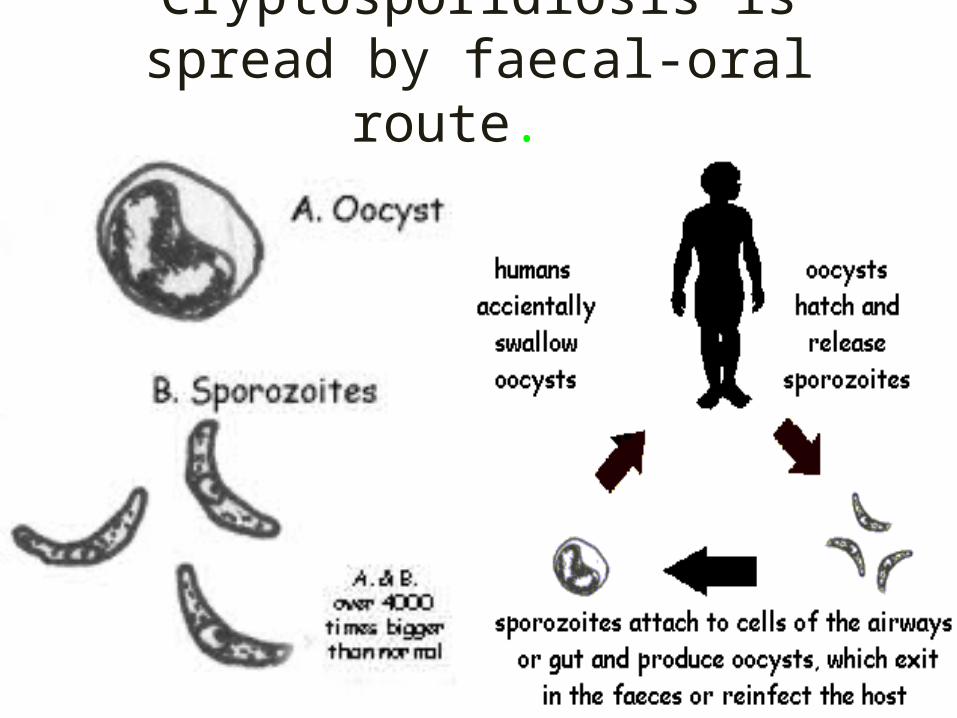
Cryptosporidiosis is spread by faecal-oral route.
MODES OF TRANSMISSION
• Droplet• Vector borne• Contact
VECTOR TRANSMISSION
Transmitted through insects and
Other invertebrates animals
such as mosquitoes and fleas.
AIR BORNE TRANSMISSION
Tiny droplet nuclei that remain (<5)
suspended in air.IN CASE OF LUNG INFECTION
AMONG IMMUNOCOMPROMISED
Direct-contact transmission
• Involves a direct body surface-to-body surface contact and physical transfer of microorganisms between a susceptible host and an infected or colonized person.
PathogenesisUpon oocyst excystation, four sporozoites are released
which adhere their apical ends to the surface of the intestinal mucosa
A sporozoite-specific lectin adherence factor has been identified
Following attachment cytokines are released from Epithelial cells which activates macrophages
Activated macrophages release histamine, serotonin, adenosine, prostaglandins, leukotrienes, and platelet-activating factor which induce loss of fluid and electrolytes

Epithelial cells are damaged
1.Cell death is a direct result of parasite invasion, multiplication, and extrusion or
2. Cell damage could occur through T cell-mediated inflammation, producing villus atrophy and crypt hyperplasia
Either model produces distortion of villus architecture results in nutrient malabsorption and diarrhea
Detection and Diagnosis
Staining methods were then developed to detect and identify the oocysts directly from stool samples.
The modified acid-fast stain is traditionally used to most reliably and specifically detect the presence of cryptosporidial oocysts
ELISA or IFA, has recently been described in diagnosis of cryptosporidiosis
PCR (Polymerase Chain Reaction) has been used for C. parvum
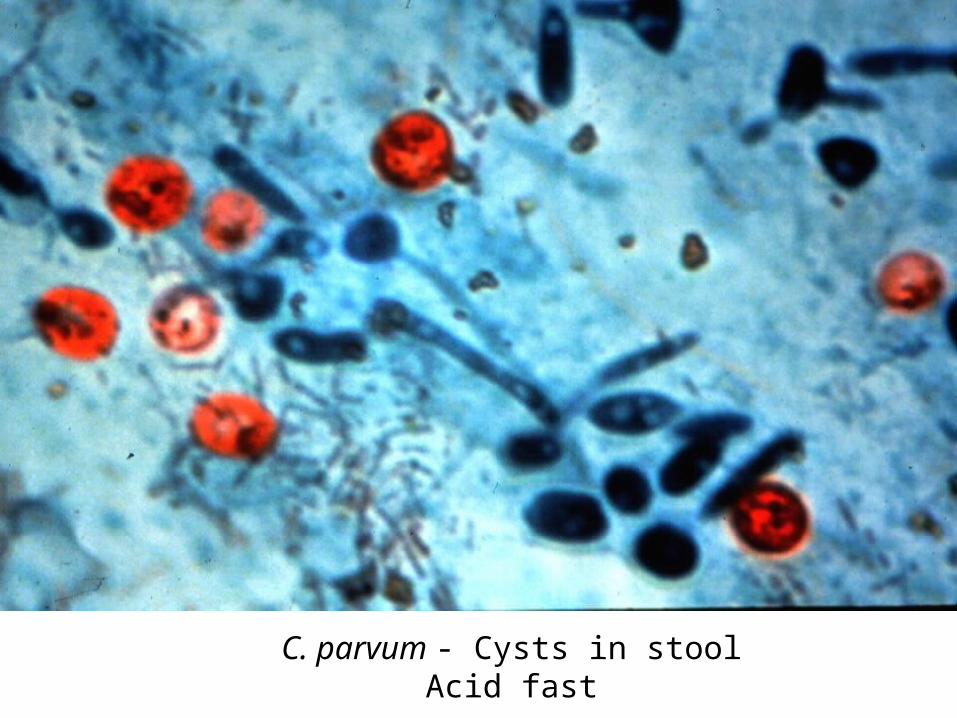
C. parvum - Cysts in stool Acid fast
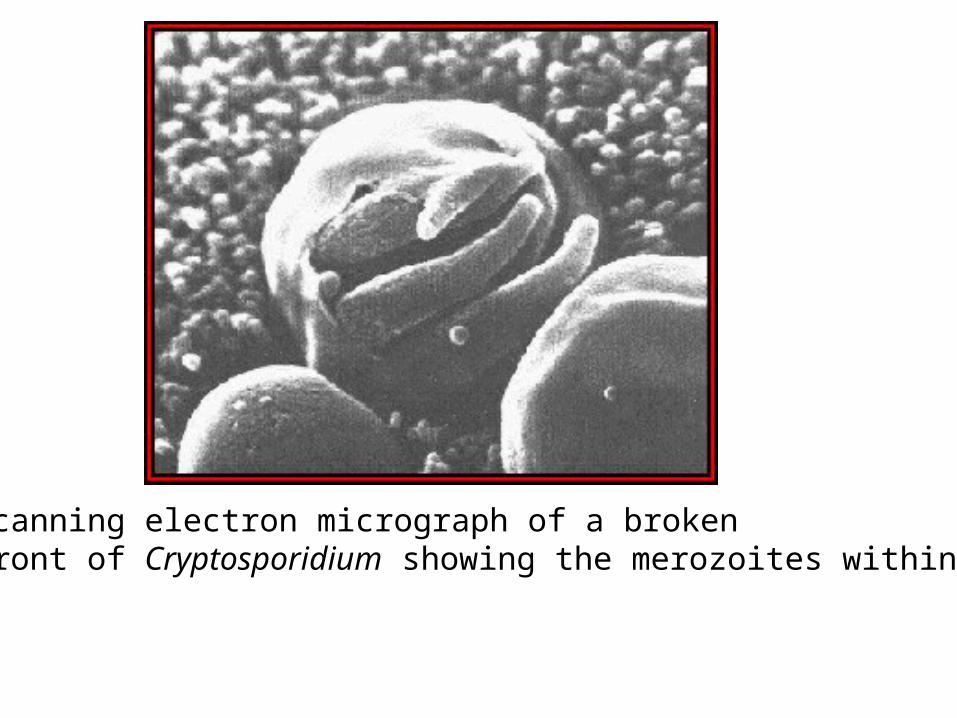
A scanning electron micrograph of a broken meront of Cryptosporidium showing the merozoites within.
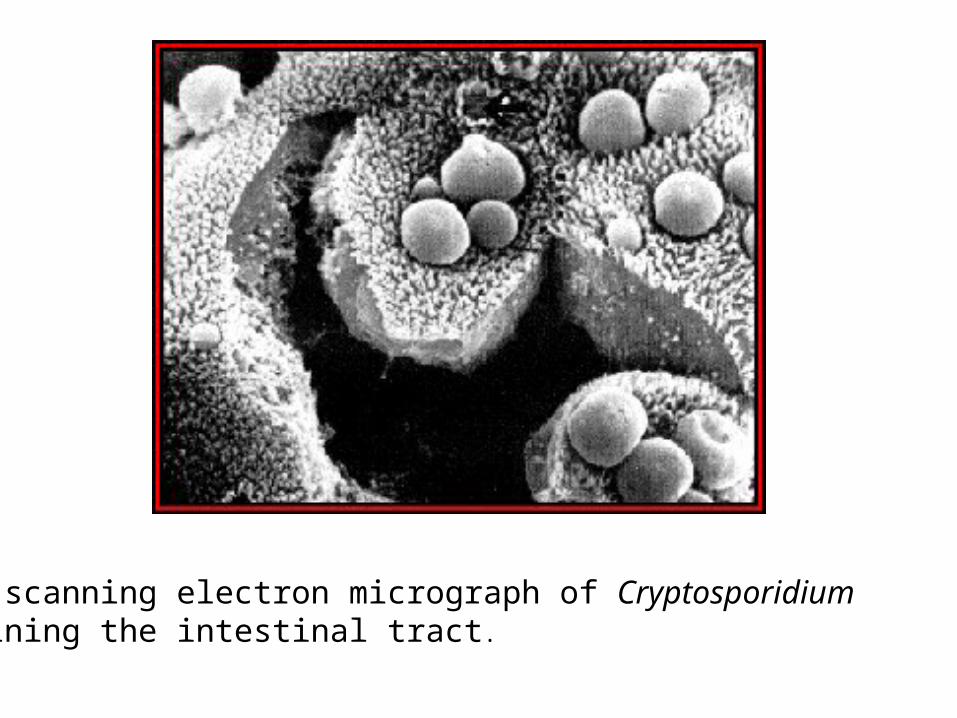
A scanning electron micrograph of Cryptosporidium lining the intestinal tract.
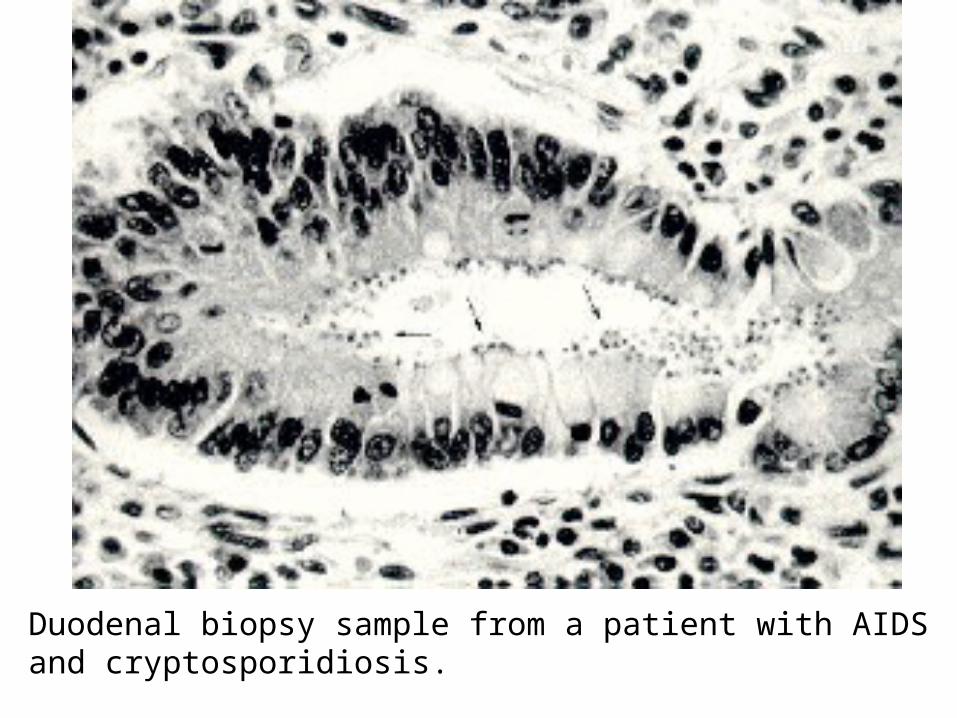
Duodenal biopsy sample from a patient with AIDS and cryptosporidiosis.
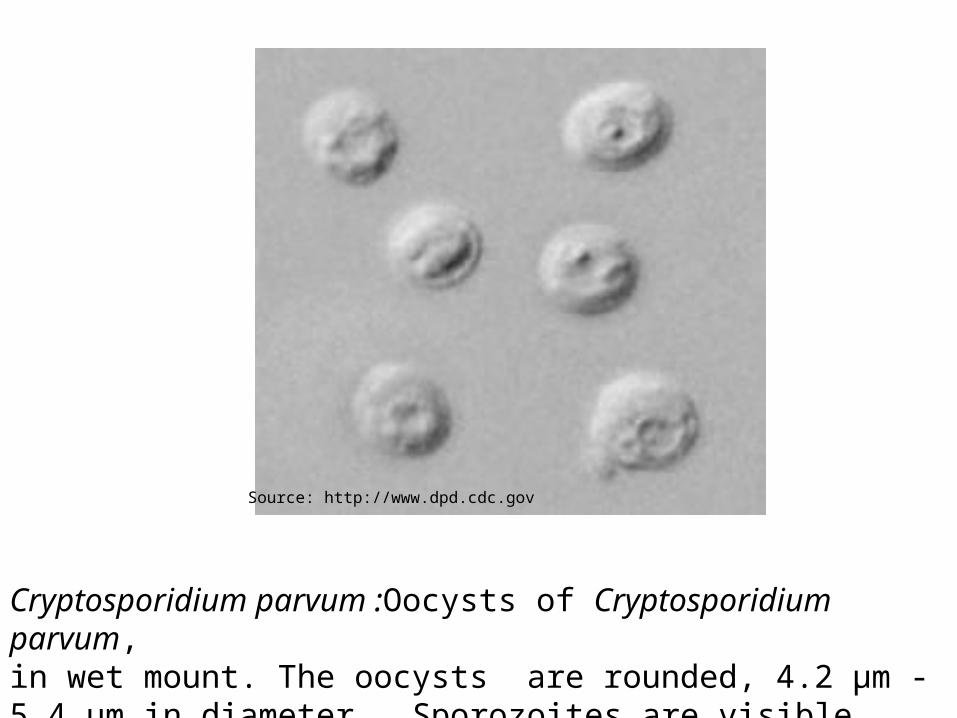
Cryptosporidium parvum :Oocysts of Cryptosporidium parvum, in wet mount. The oocysts are rounded, 4.2 µm - 5.4 µm in diameter. Sporozoites are visible inside the oocysts
Source: http://www.dpd.cdc.gov
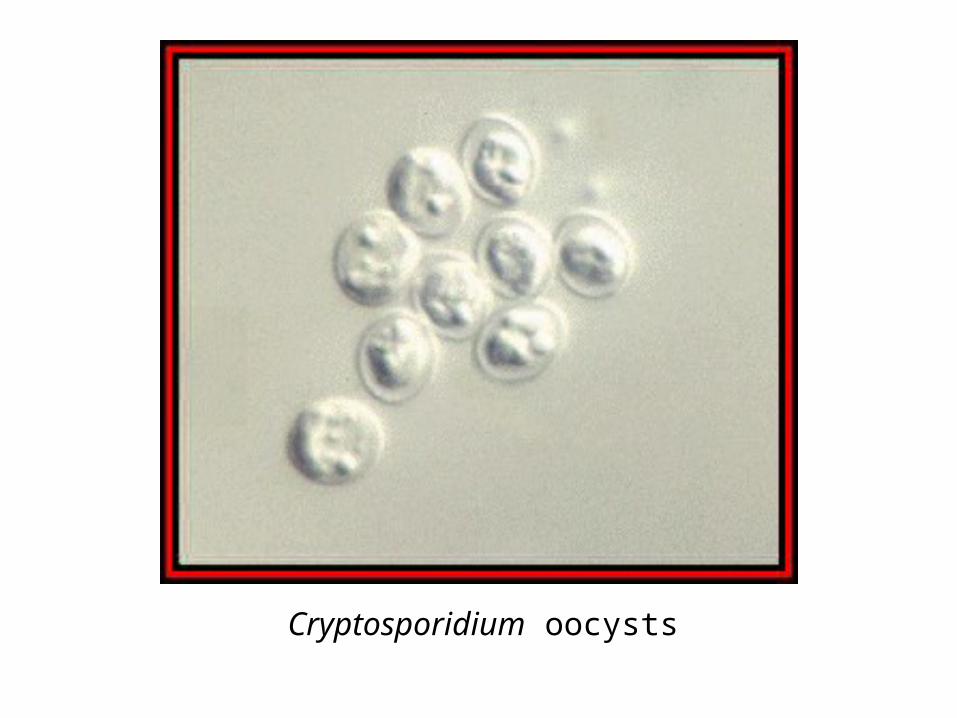
Cryptosporidium oocysts
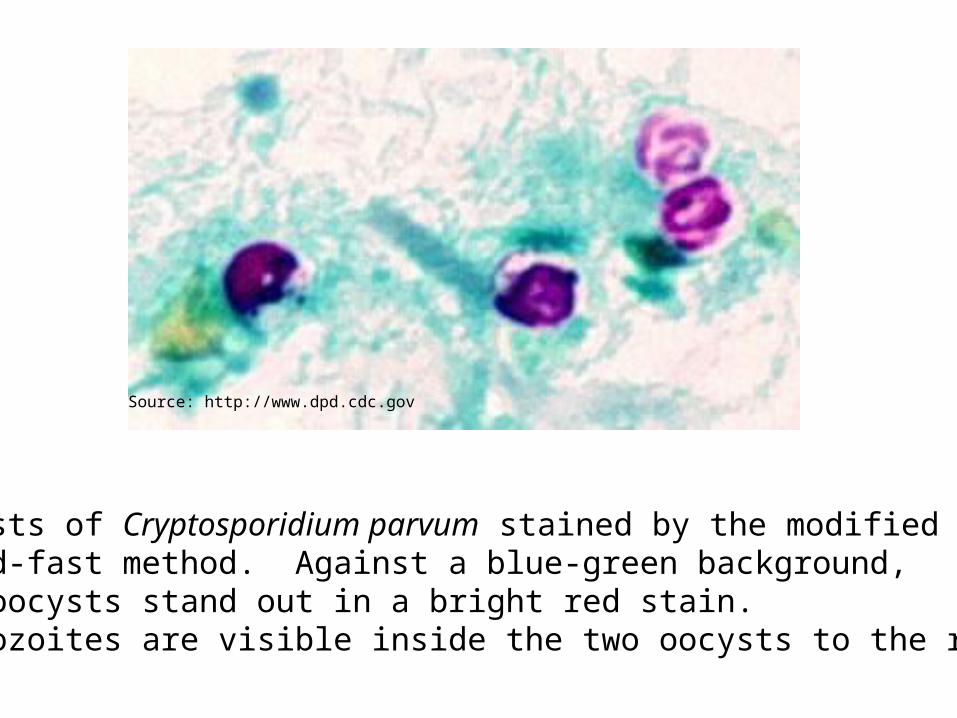
Oocysts of Cryptosporidium parvum stained by the modified acid-fast method. Against a blue-green background, the oocysts stand out in a bright red stain. Sporozoites are visible inside the two oocysts to the right.
Source: http://www.dpd.cdc.gov
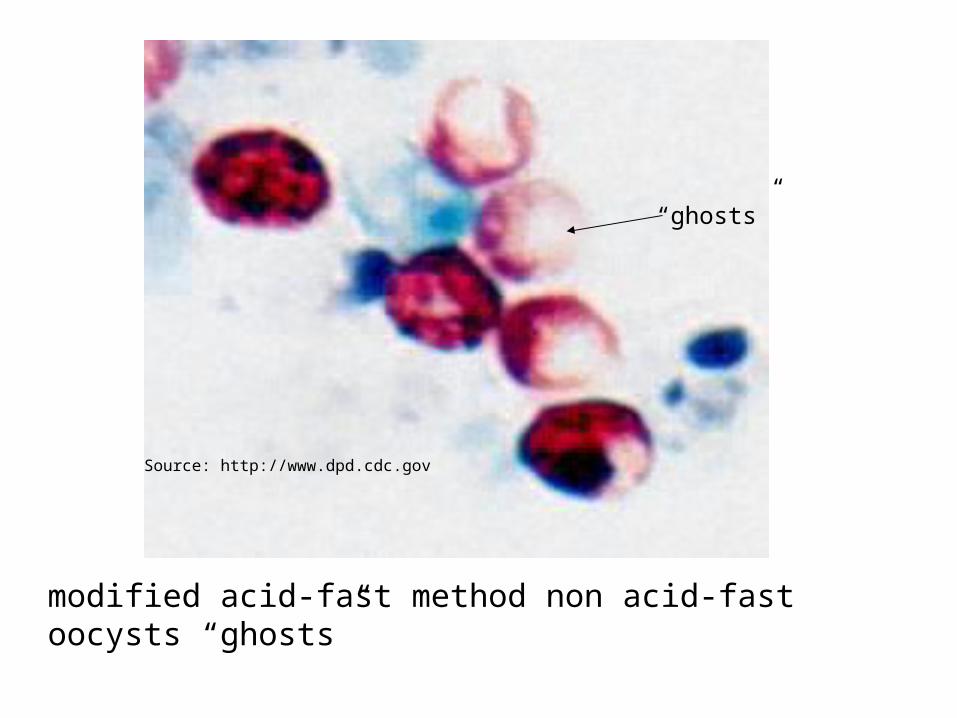
modified acid-fast method non acid-fast oocysts “ghosts”
Source: http://www.dpd.cdc.gov
“ghosts”
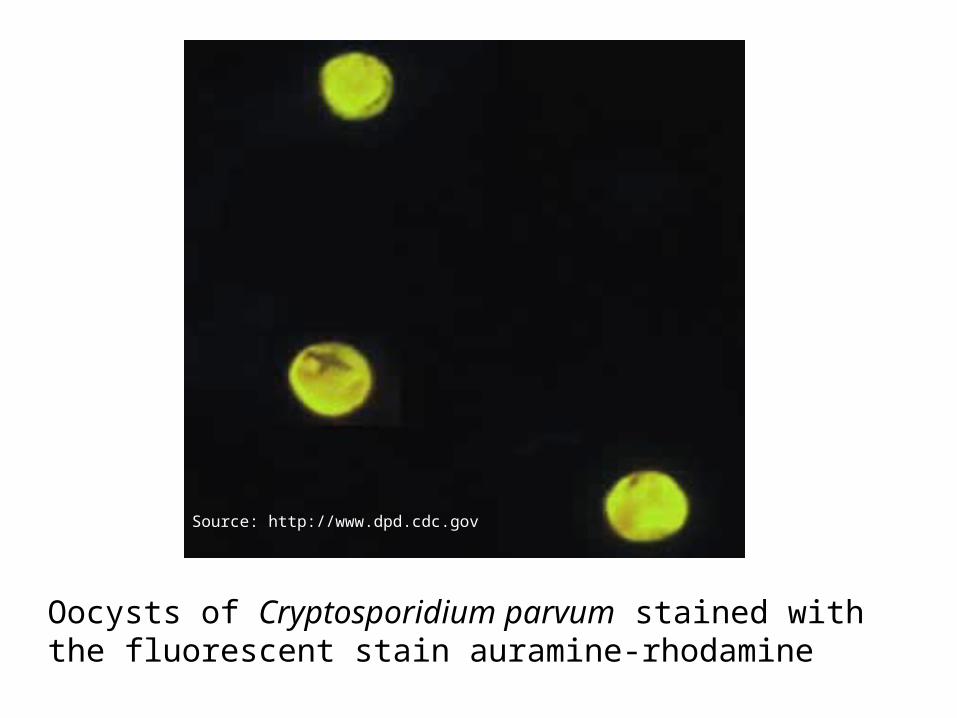
Oocysts of Cryptosporidium parvum stained with the fluorescent stain auramine-rhodamine
Source: http://www.dpd.cdc.gov
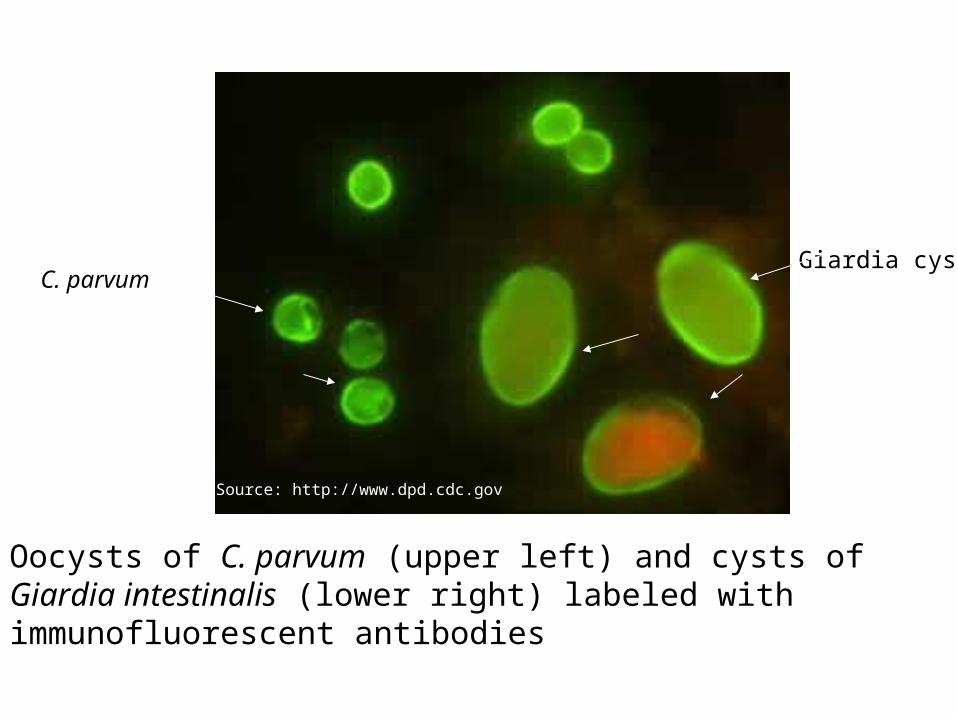
Oocysts of C. parvum (upper left) and cysts of Giardia intestinalis (lower right) labeled with immunofluorescent antibodies
Giardia cystC. parvum
Source: http://www.dpd.cdc.gov
Treatment
No safe and effective therapy for cryptosporidial enteritis has been successfully developed.
Since cryptosporidiosis is a self-limiting illness in immunocompetent individuals, general, supportive care is the only treatment for the illness.
Oral or intravenous rehydration and replacement of electrolytes may be necessary
Treatment Possibilities: Encouraging results following use of paromomycin (an aminoglycoside antibiotic) have been reported.
There is also preliminary evidence to suggest that paromomycin when used at 4 doses of 1.5 -2.0g/day has led to symptom improvement, and even eradication of the parasite.
Although Azithromycin and Lactobin-R (bovine colostrum immunoglobulin concentrate) have had some experimental success, no therapeutic agent has been clearly identified as effective
PreventionSterilization of all reusable
equipments such as ventilator,
humidifier and any device that come in
contact with the respiratory tract.
Sterilization
• 7.5% hydrogen peroxide is the only effective sterilant, while all others do not completely inactivate C.parvum.
• Other Sterilants: peracetic acid sodium hypochlorite Phenolic compounds quaternary ammonium compound 2% glutaraldehyde ortho-phthalaldehyde• RESISTANT TO CHLORINE TREATMENT
Get educatedLearn about your conditions
and treatment is the best way toprevent an error.Get involvedBe assertive about your rightsTo be a part of the decisionprocess for your medical care
The Infection Control TeamHospital EpidemiologistInfection Control Committee
ChairmanInfection Control DirectorInfection Control PractitionersGTB Healthcare Staff
YOU!!