Embed Size (px)
Citation preview

870
Metabolic Crises
CHAPTER 40
LEARNING OBJECTIVES Review the physiologic basis and patterns of inborn ■
errors of metabolism. Review the most common clinical and biochemical ■
presentations of children with metabolic diseases. Utilize screening laboratory tests to help guide the ■
further diagnostic work up of a child with suspected metabolic disease. Recognize potential pitfalls when analyzing the results of ■
metabolic testing. Outline initial treatment strategies for managing a child ■
during a metabolic crisis.
CHAPTER OUTLINELearning ObjectivesIntroductionGeneral Principles of Human Metabolic DiseaseHyperammonemiaAnion Gap Metabolic Acidosis
Organic AcidemiasMitochondrial DisordersDisorders of Ketolysis
HypoglycemiaDisorders of GluconeogenesisDisorders of Fatty Acid OxidationGlycogen Storage DiseasesCongenital Disorders of Glycosylation
Review QuestionsAnswersSuggested Readings
INTRODUCTION
The diagnosis and management of the acutely ill child with suspected metabolic disease can present a formidable challenge to even the most astute clinician. Metabolic disease may present in a fulminate fashion to the pediatric intensivist with profound biochemical distur-bances, encephalopathy and even cardiac failure. The diagnosis of an inborn error of metab-olism (IEM) may be delayed if a high index of suspicion is not maintained when an infant presents with critical illness. This chapter serves as a guide to the recognition of metabolic disease based on presenting signs, symptoms and screening laboratory tests. The rapid implementation of therapy for children with suspected or known metabolic disease will also be reviewed.
GENERAL PRINCIPLES OF HUMAN METABOLIC DISEASE
Children with metabolic derangements can present at various ages with a wide range of symptoms. Early detection can make a signifi cant difference in outcome. Certain presenting signs and symptoms can alert the physician to the possibility of a metabolic derangement (Table 40-1 ). A common presenting sign of metabolic crisis is acute encephalopathy. Multiple
PAUL J. BELLINO

871 C HAPTER 40 • M ETABOLIC C R IS ES
processes may mimic metabolic encephalopathy and include toxic ingestions, sepsis, central nervous system infection, endocrinopathies, and abuse including Munchausen by proxy syn-drome. The investigation of metabolic disease should never delay rapid treatment of life-threatening processes such as hypoglycemia, intracranial hypertension and shock.
The age of the child at the onset of symptoms may suggest the presence and type of meta-bolic disorder. In general, since the placenta and maternal processes of metabolism act as an effective dialyzer of fetal metabolic byproducts, the newborn infant rarely presents with symptoms at birth. Of the diagnoses encountered in the neonate, severe acidosis from either glutaric acidemia type II or pyruvate carboxylase defi ciency, or hyperammonemic enceph-alopathy from transient hyperammonemia of the newborn (THAN) are most commonly encountered. Later in infancy, a much broader range of diagnoses should be considered. These include the organic acidurias, primary lactic acidemias, disorders of CNS metabo-lism, and THAN. The remainder of this chapter will be devoted to the workup of children who present with suspected metabolic crisis beyond the immediate neonatal period.
The initial laboratory assessment of a child with suspected metabolic derangement should include rapid glucose determination, serum electrolytes, lactate, pyruvate, ammonia, liver function studies and urinalysis. Calculation of the anion gap should be done routinely if any degree of acidosis is present. Although many other tests for metabolic disease are available, these screening tests are often a helpful starting point and are sensitive to detect the majority of metabolic disorders presenting in acute crisis.
Children with metabolic derangements presenting in crisis can be grouped into three major categories based on screening laboratory fi ndings:
I. Hyperammonemia II. Anion Gap Metabolic Acidosis III. Hypoglycemia
A common presenting sign of metabolic crisis is acute metabolic encephalopathy.
The initial laboratory assessment of a child with suspected meta-bolic derangement should include serum electrolytes, lactate, glucose, ammonia, urinalysis, and liver function studies.
Neurologic
Change in mental status ■
Unexplained developmental delay ■
Seizures ■
Encephalopathy ■
Inconsolability ■
Lethargy ■
Poor tone ■
Respiratory
Rapid onset of tachypnea without lung disease ■
Apnea ■
Cardiac
Congestive heart failure ■
Ischemic heart disease ■
Cardiomegaly ■
Gastrointestinal
Jaundice ■
Diarrhea ■
Vomiting ■
Abdominal pain ■
Constitutional
Failure to thrive ■
Unusual odor to the urine, breath, cerumen, or other body fl uid ■
Syndromic appearance ■
TABLE 40-1
PRESENTING SIGNS AND SYMPTOMS OF INBORN ERRORS OF METABOLISM

872 P. J. B ELLI NO
When an IEM is suspected, if clinically possible, pre-therapy blood specimens should be obtained, since some disturbances may be affected by initial therapies (such as glucose administration).
Categorization of inborn errors is inherently diffi cult due to the multiple areas of overlap in clinical and laboratory features that exists among various metabolic diseases. An initial approach to the diagnosis of an IEM based on the most prominent abnormality is presented but should be used with the understanding that a complex interplay often exists between multiple biochemical pathways.
HYPERAMMONEMIA
Ammonia is produced in the breakdown of proteins, more specifi cally by the catabolism of amino acids. Ammonia is subsequently removed through the production of urea in a series of chemical steps known as the urea cycle. A defect in any one of these steps can result in decreased ability to eliminate ammonia. Children with urea cycle defects will develop dangerously high levels of ammonia after the ingestion of a high protein containing meal, or during times of increased mus-cle catabolism as seen during starvation states, severe systemic illnesses, or prolonged exercise.
Ammonia is highly toxic to many body tissues and the central nervous system in particu-lar is extremely sensitive to its effects. Elevated levels of ammonia initially result in gastro-intestinal symptoms such as anorexia, nausea, and vomiting. Patients usually develop varying degrees of confusion, ataxia, and sleepiness, which may progress to seizures or coma. Common metabolic causes of hyperammonemia seen outside of the immediate newborn period are urea cycle defects, organic acidemias, and aminoacidopathies (Table 40-2 ). Less likely etiologies of hyperammonemia such as fulminant hepatic failure (toxin or infection induced) and Reye’s syndrome should also be considered.
Interpretation of serum ammonia levels must be undertaken with caution, since there is considerable variation with age. Newborns may exhibit levels ranging between 90–150 m g/
The more common metabolic causes of hyperammonemia seen outside of the immediate newborn period are the urea cycle defects, organic acidemias, and amino acidopathies.
Defi ciencies of the urea cycle
Carbamyl phosphate synthetase (CPS) ■
■ N -acetylglutamate synthetase (NAGS)
Ornithine transcarbamylase (OTC) ■
Arginosuccinate acid synthetase (ASA) - ■ Citrullinemia
Arginosuccinate lyase (ASL) - ■ Argininosuccinic aciduria
Arginase - ■ Argininemia
Organic acidemias
Methylmalonic acidemia ■
Isovaleric acidemia ■
Propionic acidemia ■
Multiple carboxylase defi ciency ■
Glutaric acidemia type II ■
3-hydroxy-3-methylglutaric acidemia ■
Other
Disorders of fatty acid oxidation ■
Hyperammonemia-hyperornithemia-homocitrullinemia syndrome (HHH) ■
Transient Hyperammonemia of the Newborn (THAN) ■
Congenital hyperinsulinism with hyperammonemia syndrome ■
TABLE 40-2
INBORN ERRORS OF METABOLISM RESULTING IN HYPERAMMONEMIA

873 C HAPTER 40 • M ETABOLIC C R IS ES
dL. The levels gradually decrease over several months, ultimately reaching normal adult ranges between 10–45 m g/dL. In addition to the normal age variation, several factors may contribute to spuriously elevated levels in samples. Specimens are best obtained from a free fl owing venous or arterial puncture. Use of a tourniquet, rough handling of specimens, pro-longed delay in completion of testing, and exposure to heat may result in signifi cant eleva-tions in ammonia. In most laboratories, the determination the serum ammonia level is done using a photometric analysis that indirectly measures the ammonia concentration by assess-ing the catalyzed conversion of NADPH to NADP + . While this method is less likely to pro-duce erroneous levels, some evidence exists that with some of these reagent assays, reported levels may be spuriously low if children are receiving thiopental. Other barbiturates do not seem to interfere with these tests.
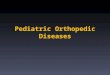
An algorithm for the evaluation of a child with hyperammonemia is depicted in Fig. 40-1 . The presence of concomitant hypoglycemia or acidosis should be quickly deter-mined. The combination of moderate hyperammonemia, acidosis and hypoglycemia with-out urine ketones is highly suggestive of a disorder of fatty acid oxidation (see fatty acid oxidation disorder section). The presence of an anion gap acidosis in the setting of hyper-ammonemia should prompt a further investigation of an organic acidemia. Urine for organic acid analysis should be obtained to help determine the exact metabolic defect (see Organic
Serum ammonia levels should be interpreted with caution as they may be spuriously elevated if not drawn from a free fl owing venous or arterial site.
Citrullinemia,Argininemia
Argininosuccinic aciduria, orHHH Syndrome
Hyperammonemia ispresent
Yes
Check urine ketones
Ketonespresent?
Is acidosispresent?
Disorders of FAoxidation
Check urineorganic acids
Organic Aciduria
Specific AAelevation?
Check serum amino acids
No
YesNoYes
OTCdeficiency
Yes
No
No
Check urineorotic acid
Check serumcitrulline
Orotic acidelevated
Check serum pHor HCO3
No
CPS or NAGS deficiency
THAN
Citrullineelevated?
FIGURE 40-1
Systematic approach to hyperammonemia ( CPS - Carbamyl phosphate synthetase NAGS - N-acetylglutamate synthetase OTC - Ornithine transcarbamylase HHH - Hyperammonemia-hyperornithemia-homocitrulline-mia THAN - transient hyperammone-mia of the newborn)

874 P. J. B ELLI NO
Acidemia section). Hyperammonemia without acidosis is the hallmark of the urea cycle defects . Ammonia may stimulate the respiratory center causing tachypnea and an initial respiratory alkalosis. Children with urea cycle defects may present with only an elevated ammonia level.
Several less common entities such as THAN and certain aminoacidopathies may present with hyperammonemia. Serum amino acid analysis should be obtained to rule out an amino-acidopathy. In some centers, the turnover time in obtaining the results of amino acid assays from a referral laboratory can exceed 1–2 weeks. Due to this delay and because the more likely diagnosis will be a urea cycle defect, urine should be analyzed for elevation of orotic acid at the same time that amino acid studies are sent. In the absence of an aminoacidopathy, an elevated urine orotic acid is clear evidence of ornithine transcarbamylase (OTC) defi -ciency. This X-linked dominant disorder is the most common of the urea cycle defects. Although males are clearly more severely affected, heterozygote females can exhibit some degree of disease. If orotic acid levels are not elevated, evaluation of the plasma citrulline level may help determine other forms of the urea cycle defects and THAN. THAN is gener-ally more common in premature infants and rarely occurs outside of the immediate neonatal period. Occasional cases have been reported in term infants who present after several days of life. Typically, these infants present with respiratory distress and have markedly elevated levels of ammonia (2,000–4,000 m M/L). Occasionally, citrulline levels may also be elevated. The etiology of THAN remains unknown. Devastating neurological outcomes and death are possible if intensive care management is not initiated promptly.
Regardless of the cause of hyperammonemia, emergent therapies should be undertaken to reduce ammonia levels while awaiting a defi nitive diagnosis. Several studies reveal that prompt recognition and management of patients in hyperammonemic states results in improved long-term outcomes. Initial management includes assuring the adequacy of gas exchange and maintenance of hemodynamics. Prevention of further catabolism of muscle is achieved by intravenous administration of hypertonic glucose containing fl uids and the administration of intravenous lipids at a starting dose of 1 g/kg/day. Minimal amount of essential amino acids should be given to prevent further protein load. The total daily pre-scribed amount of essential amino acids should not exceed 0.25 g/kg/day. When enteric feeding is possible a low protein liquid nutritional such as ProPhree® at a rate to allow 0.5–1 g/kg/day of protein should be started.
Once further catabolism is prevented, aggressive efforts to clear ammonia should be undertaken with administration of sodium benzoate and sodium phenylacetate. Both benzo-ate and phenylacetate bind ammonia byproducts thus promoting renal clearance. Within the mitochondria, excess ammonia can be converted to glycine and glutamine. Benzoate binds to glycine to produce hippurate and phenylacetate combines with glutamine to form pheny-lacetylglutamine. Both byproducts undergo rapid renal excretion thus allowing for alterna-tive pathways of ammonia elimination.
The administration of arginine may also aid in clearing excess ammonia due to urea cycle defects. Enteral administration of neomycin or lactulose can reduce ammonia production from gastrointestinal bacteria but does not produce an acute reduction in ammonia.
If the above therapies do not result in prompt clinical improvement, or if there is a signifi -cant delay in therapy due to the drug unavailability, hemodialysis or peritoneal dialysis should be undertaken to lower the plasma ammonia level. Ammonia is readily removed by either method. Hemodialysis is commonly used but peritoneal dialysis can be equally effec-tive. A signifi cant decrease in ammonia is usually seen within several hours, and ammonia levels can be reduced to normal within 1 or 2 days after initiating dialysis.
ANION GAP METABOLIC ACIDOSIS
Evaluation of the anion gap is essential and is determined by subtracting the sum of the serum chloride and bicarbonate from the sum of the serum sodium and potassium. The usual anion gap ranges from 8 to 16 mEq/L. Children with metabolic disease may present with an anion gap acidosis (anion gap >16 mEq/L). Other non metabolic etiologies of an anion gap
The presence of an anion gap acidosis in the setting of hyper-ammonemia is strongly suggestive of an organic acidemia.
Hyperammonemia without acidosis is the hallmark of the urea cycle defects.
Prompt recognition and manage-ment of patients in hyperam-monemic states results in improved long-term outcomes.
Ammonia is readily removed by both hemo dialysis and peritoneal dialysis.
Children with acidosis from metabolic disease present with an elevated anion gap.

875 C HAPTER 40 • M ETABOLIC C R IS ES
metabolic acidosis should be considered (Table 40-3 ). Non-anion gap acidosis is usually secondary to gastrointestinal or renal bicarbonate loss.
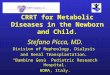
Several metabolic disorders can present with an anion gap metabolic acidosis. A stepwise evaluation can be helpful in determining an exact metabolic etiology (Fig. 40-2 ).
Detecting the presence of simple acidic byproducts of metabolism such as ketoacids and lactic acid is an important fi rst step in the evaluation of an anion gap metabolic acidosis. Initial evaluation should include urine for ketones and serum lactate level. The presence of hyperglycemia with ketonuria in the setting of a metabolic acidosis will differentiate the child with DKA from an underlying metabolic disease. Of the inborn errors of metabolism presenting with an anion gap metabolic acidosis and massive ketosis, the organic acidurias are the most common.
In the absence of ketosis, lactic acidemia is a common cause of an anion gap metabolic acidosis. It is important to note that ketosis and lactic acidosis are not exclusive of one another. Many children with organic acidemias may present with an elevated serum lactate as well as ketones in the urine. When ketones are only trace or absent, the differential includes multiple disorders of mitochondrial metabolism, disorders of gluconeogenesis or glycogen storage disease, disorders of fatty acid oxidation, and rarely D-lactic acidosis. The latter is a rare condition seen in children as a result of the production of the D isomer of lactate pro-duced by enteric bacteria. Determination of the D-lactate level will differentiate this group of children from more concerning metabolic disorders.
It is important to recognize the potential for laboratory error when assessing the serum lactate level. Erroneously elevated levels of lactate can be obtained if the specimen is not drawn as a freely fl owing venous or arterial specimen. Additionally, a delay in processing, exposure to extremes in heat, clotting, or marked hemolysis in the specimen can result in falsely elevated levels.
Important inborn errors that produce an anion gap metabolic acidosis as a prominent fi nd-ing include:
1. Organic Acidemias (a) Branched chain amino acidurias ( methylmalonic aciduria , propionic acidemia , isovaleric
acidemia , maple syrup urine disease ) (b) Multiple carboxylase defi ciencies ( holocarboxylase synthetase defi ciency , biotinidase defi -
ciency ) (c) Glutaric aciduria type I
Non-anion gap metabolic acidosis is usually due to bicarbonate loss from diarrhea or from renal tubular acidosis.
The most common inborn errors of metabolism presenting with an anion gap acidosis and massive ketosis are the organic acidurias.
Ingestions:
Methanol ■
Ethylene glycol ■
Salicylates ■
Paraldehyde ■
Uremia/chronic renal insuffi ciency
Diabetic ketoacidosis
Inborn errors of metabolism:
Aminoacidopathies ■
Organic acidurias ■
Disorders of fatty acid metabolism ■
Glycogen storage disease ■
Krebs’s cycle defects ■
Mitochondrial disorders ■
Starvation
Miscellaneous lactic acidemias
TABLE 40-3
CAUSES OF ANION GAP METABOLIC ACIDOSIS ( D ³ 16 MEQ/L)

876 P. J. B ELLI NO
Metabolic Acidosis
Non-anion Gap Acidosis Anion Gap Acidosis
Consider bicarbonate loss ordilution • Diarrhea • RTA • Hyperchloremia • Drug effect (i.e. acetazolamide
Exogenous acids • Toxins
Endogenous acids • Ketones (diabetic ketoacidosis) • Uremia • Lactic acidemia from hypoperfusion • D-Lactic acidemia from gut • Inborn Error of Metabolism
Inborn Error of Metabolism suspected as cause of anion gap acidosis – obtain:serum lactate, pyruvate, ammonia, amino acids and urine ketones and organic acids
Normal Lactate Elevated Lactate
High Ketones
AbnormalOrganic Acids
Disorders of ketolysis
Organic Acidemia* Aminoacidopathies (i.e. MSUD)
Organic Acidemia • Methylmalonic acidemia • Propionic academia • Isovaleric acidemia • MCD
* *
Elevated Pyruvate(Normal L/P ratio < 25)
Low or normal Pyruvate(High L/P ratio > 25)
NormalGlucose
LowGlucose
Pyruvate dehydrogenasedeficiency
Pyruvate carboxylasedeficiency
GSD 1
Disorder ofgluconeogenesis
MitochondrialDisorders
LowKetones
Disorder of fattyacid oxidation
Obtain muscle biopsy and ormitochondria DNA analysis fordefinitive diagnosis (i.e. MELAS,MERRF, NARP, MILS)
FIGURE 40-2
Approach to metabolic acidosis. Inborn errors should always be considered in infants presenting with unexplained anion gap acidosis. *Organic acidemias and disorders of fatty acid oxidation usually present with acidosis secondary to accumulation of abnormal organic acids and ketoacids. Lactate may be normal or elevated depending on the degree of concomitant hypoper-fusion. Hyperammonemia may also be present in organic acidemias and disorders of fatty acid oxidation. MCD- multiple carboxylase defi ciency, MSUD -maple syrup urine disease, MELAS -mitochondrial encephalopathy and stroke like syndrome, MERRF -myoclonus epilepsy with ragged-red fi bers, NARP -neuropathy, ataxia and retinitis pigmentosa, MILS -maternally inheritied Leigh syndrome

877 C HAPTER 40 • M ETABOLIC C R IS ES
(d) Disorders of fatty acid oxidation (e) Disorders of gluconeogenesis
2. Mitochondrial Disorders 3. Disorders of Ketolysis
Of note, concomitant hypoglycemia may be present in the above disorders especially in disorders of fatty acid oxidation and disorders of gluconeogenesis. Disorders of fatty acid oxidation and gluconeogenesis are discussed under metabolic conditions that have hypogly-cemia as a prominent feature.
Organic Acidemias The organic acidemias are a group of disorders that result from defects in metabolic path-ways of the amino acids, fatty acids, and carbohydrates. The metabolic defects result in accumulation of the byproducts of metabolism, the organic acids, which can be detected in the urine. The following organic acidemias produce severe anion gap metabolic acidosis:
(a) Branched chain amino acidurias ( methylmalonic aciduria , propionic acidemia , isovaleric acidemia , maple syrup urine disease )
(b) Multiple carboxylase defi ciencies ( holocarboxylase synthetase defi ciency , biotinidase defi -ciency )
Branched-Chain Amino Acidurias
Methylmalonic aciduria (MMA) has been described since the mid 1960s. There are four mutations that phenotypically result in a clinical constellation of an anion gap metabolic aci-dosis, elevated methylmalonate in the urine, and a normal serum cobalamin (B 12 ) level. Patients usually present within the fi rst several weeks of life with symptoms progressing from vomiting, dehydration, and failure to thrive to lethargy and coma. Laboratory studies fre-quently reveal ketonuria, hyperammonemia, hypoglycemia and marrow failure with leukope-nia and thrombocytopenia. Defi nitive diagnosis is made with colorimetric assay for urinary methylmalonate or gas chromatography-mass spectrometry assays for serum or urinary meth-ylmalonate. Initial treatment should include urgent correction of hyperammonemia, hypogly-cemia, and ketosis. Infusion of hypertonic dextrose in half-normal sodium bicarbonate is useful in correcting acidosis and preventing further catabolism. Initial stabilization is fol-lowed by restricted protein intake and IM administration of supplemental cyanocobalamin or hydroxocobalamin for several days. Because the administration of B 12 derivatives has mini-mal risk, they can be administered prior to a making a defi nitive diagnosis of MMA. In addi-tion, the use of L-carnitine has been found to be a useful adjunct during MMA acute crisis. Finally, metronidazole may be effective in improving neurological symptoms in children with MMA by reducing bacterial byproducts produced in the gastrointestinal tract.
Propionic acidemia is characterized by episodic metabolic ketoacidosis, protein intolerance, an elevated plasma glycine levels. Several mutations affecting the activity of propionyl-CoA carboxylase have been identifi ed that produce the clinical spectrum of the disorder. There is considerable variation in clinical severity of children with this disorder. Infants with propionic acidemia usually present within the fi rst few days of life. Later onset in childhood can occur and, interestingly, some patients never develop clinical evidence of the disease despite an almost complete lack of enzyme activity. The usual presenting signs and symptoms include dehydra-tion, vomiting, and lethargy progressing to coma. As the clinical severity can vary, propionic acidemia should be considered in children who present at a later age with a history of episodic unexplained ketoacidosis, encephalopathy, or developmental delay with seizures or cerebral atrophy. A presumptive diagnosis can be made by determination of propionic acid and its metab-olites in blood or urine. It should be noted that propionate accumulation can occur in children with MMA as well. Defi nitive diagnosis is made by studying the propionyl-CoA carboxylase activity in leukocytes or fi broblasts. Subsequent gene testing to determine the exact mutation of
Children with MMA present early in infancy with severe acidosis and progress quickly from irritability to coma.
Infusion of hypertonic dextrose to prevent further catabolism of protein is essential in manage-ment of all branched-chain aminoacidopaties.
As vitamin B 12 is not harmful, it should be administered early in any suspected case of MMA, even before confi rmatory testing is completed.

878 P. J. B ELLI NO
the enzyme is useful in helping to establish prognosis and in genetic counseling. Initial treatment is similar to that of MMA with administration of dextrose and bicarbonate to correct severe acidosis. All dietary protein should be withdrawn during an exacerbation. If hyperammonemia is present, dialysis may be indicated. In theory, since propionyl-CoA carboxylase requires biotin as a co-factor, biotin supplementation may be helpful. The clinical response to biotin administra-tion is less marked in propionic acidemia than is seen in multiple carboxylase defi ciency. L-carnitine has also been reported to be of value in the acute management of children with pro-pionic aciduria. Although no large trials have been conducted, several studies have shown that children with this disorder are relatively carnitine defi cient, and supplementation with L-carnitine can reduce the ketogenic response to fasting. Finally, as gut fl ora can contribute considerably to the body’s burden of propionic acid, metronidazole may reduce gastrointestinal bacterial pro-duction of propionic acid.
Isovaleric acidemia is caused by a defect in the enzyme isovaleryl-CoA dehydrogenase. About one-half of the children with this disorder present in the immediate neonatal period with refusal to eat, vomiting, dehydration, lethargy and coma. Tetany, seizures and tempera-ture instability are also common. Infants may exhibit a classic “sweaty feet” odor from high levels of isovaleric acid in their secretions. Laboratory assessment frequently shows severe acidosis, ketosis, mild hyperammonemia, hypocalcemia, and transient bone marrow failure manifested by thrombocytopenia and leukopenia. If not treated appropriately, infants prog-ress rapidly to cardiopulmonary failure and death.
Older patients with isovaleric acidemia may present with a chronic, intermittent form of the disease. These children usually have their fi rst metabolic crisis within the fi rst year of life. Exacerbations are typically precipitated by mild infectious illnesses or ingestion of high protein meals. Children usually present with vomiting and altered mental status that can progress to coma. Laboratory evaluation reveals an anion gap metabolic acidosis and keto-nuria. Pancytopenia and hyperglycemia may also be present. The presence of hyperglycemia and ketonuria may result in an incorrect diagnosis of diabetic ketoacidosis. It is suspected that the hyperglycemia in this disorder is due to a normal stress response, and not because of abnormal glucose metabolism. Episodic exacerbations of isovaleric acidemia are managed in a similar fashion as other branch-chained organic acidemias. Intravenous administration of dextrose and bicarbonate for severe acidosis is warranted. Prompt administration of gly-cine and L-carnitine has been shown effective in reducing the levels of toxic metabolites. In addition, reduction of dietary protein to no more than 1.5 g/kg/day is suggested.
Maple syrup urine disease is caused by the inactivity of the mitochondrial branched-chain alpha-ketoacid dehydrogenase complex. This enzyme complex is responsible for the decar-boxylation of the branched-chain amino acids: leucine, isoleucine, and valine. Decarboxylation of these amino acids is the fi rst step in their conversion to acetyl-CoA, acetoacetate, and suci-nyl CoA. As a result of the inability to utilize these amino acids, accumulation of branched-chain ketoacids occurs, leading to a strong odor of maple syrup in the urine. Children may develop progressive neurological deterioration and present in acute crisis with cerebral edema, seizures, and respiratory distress as early as the fi rst week of life. Emergent treatment requires achieving an anabolic state and ceasing the exogenous administration of offending amino acids. Rapid intravenous administration of glucose as well as volume replacement is of para-mount importance. Insulin with continuous glucose instituted early in the treatment can pre-vent further catabolism. Intravenous lipid should also be given to help prevent catabolism. Usual starting rates of 1 g/kg/day may be rapidly increased to as much as 3 g/kg/day if triglyc-eride levels permit. In addition, specifi c attention should be paid to reducing levels of branched-chain amino acids by incorporating them into new protein. This is accomplished by administration of protein solutions that are defi cient in leucine, isoleucine, and valine at a rate of 2 g/kg/day.
Multiple Carboxylase Defi ciency
Biotin is an essential B vitamin that is responsible for the activation of the four main apo-carboxylases: propionyl CoA carboxylase, pyruvate carboxylase, b -methylcrotonyl CoA carboxylase, and acetyl CoA carboxylase. These activated enzymes are essential in the
Supplementing biotin in acute attacks in patients with propionic acidemia may be helpful.
Children with isovaleric acidemia exhibit a classic odor of “sweaty feet.”
The presence of combined hyperglycemia and ketonuria in cases of isovaleric acidemia may result in an incorrect diagnosis of diabetic ketoacidosis.
Accumulation of branched-chain ketoacids in the urine leads to a strong odor of maple syrup in children with maple syrup urine disease.
Insulin administration is useful in assuring glucose utilization and reversing catabolism during a metabolic crisis.

879 C HAPTER 40 • M ETABOLIC C R IS ES
initial steps of the tri-carboxylic acid cycle, gluconeogenesis, leucine catabolism, and fatty acid synthesis respectfully. Thus, defi ciencies in biotin, or in the enzymes responsible for its utilization can have marked metabolic effects.
The two enzymes responsible for the recycling of biotin are holocarboxylase synthetase and biotinidase. Holocarboxylase synthetase is responsible for the covalent attachment of biotin to the various apocarboxylase enzymes, thus converting them to active holocarboxy-lases. Biotinidase is responsible for cleaving the biotin moiety from the holocarboxylases and thus permitting the vitamin to be recycled. Because of the broad effects of these two enzymes on several metabolic processes, defects in their function are referred to as the mul-tiple carboxylase defi ciencies.
Children with holocarboxylase synthetase defi ciency (HCSD) may develop symptoms within the fi rst several hours of life. Later onset is common, with an average age of presen-tation at 3 months. Neurological symptoms predominate and include: lethargy, irritability, vomiting, hypotonia, ataxia, and seizures. Cutaneous fi ndings such as rash and alopecia totalis can be striking. The rash of children with HCSD can vary from a severe seborrhea-like eruption to a confl uent erythematous desquamating rash over the entire body. The rash is occasionally super-infected with yeast resulting in vesicle formation. Metabolic derange-ments include marked acidosis with elevations of both lactate and ketoacids. Hyperammonemia is also common. The presence of an acidosis with elevated ammonia may result in tachypnea. Immune dysfunction and hematological abnormalities such as thrombocytopenia may be present. The diagnosis should be suspected when urine organic acids assay reveals elevation of several compounds: lactic acid, propionic acid, 3-methyl-crotonic acid, 3-methylcrotonylglycine, methylcitrate, and 3-hydroxyisovaleric acid. Defi nitive diagnosis is diffi cult and requires the demonstration of abnormal carboxylase activity in leukocytes or in cultured fi broblasts exposed to a low-biotin medium. Patients with HCSD usually exhibit improvement upon administration of biotin at a dose of 10 mg/day. Irreversible neurological injury can occur without early recognition and treatment. Since biotin has no signifi cant adverse effects, empiric treatment of any suspected case is justifi ed.
Biotinidase defi ciency can present as early as 1 week of life but more commonly presents in children between 3 and 6 months of age. Similar to HCSD, neurological symptoms and dermatological manifestations are common. Hypotonia, seizures, ataxia, lethargy, vomiting, and coma may be present in infancy. Children presenting later may have a history of devel-opmental delay, visual loss, or hearing loss. Metabolic abnormalities include lactic and ketoacidosis, and mild hyperammonemia. Tachypnea from severe acidosis and hyperam-monemia is commonly seen during an acute crisis. Cutaneous manifestations are common but may vary from those seen in HCSD. Alopecia areata is more frequently seen. Seborrhea and atopic dermatitis are common, however these children usually do not present with the severe desquamating rash seen in HCSD. Concomitant immunodefi ciency is caused by a combination of decreased leukocyte myeloperoxidase activity as well as abnormal T- and B-lymphocyte activity. Due to immune dysfunction and chronic dermatologic fi ndings, chil-dren may be misdiagnosed as having severe combined immunodefi ciency syndrome. Diagnosis is made by demonstrating abnormal biotinidase activity in whole blood which may be identifi ed during newborn screening. A urine organic acid assay reveals similar results as seen in holocarboxylase synthetase defi ciency. Treatment usually consists of biotin supplementation. Children with biotinidase defi ciency usually respond rapidly, with rash and immune functions resolving within a few days. Acute neurological symptoms may resolve quickly, however developmental, hearing, and visual changes may persist if diagnosis is delayed.
Glutaric Aciduria Type I
Glutaric aciduria type 1 is caused by a defi ciency of glutaryl-CoA dehydrogenase (GDH), resulting in abnormal lysine and tryptophan oxidation and the accumulation of glutaric and 3-hydroxyglutaric acid. The derangement in GDH also causes a secondary carnitine defi -ciency. Transmission occurs in an autosomal recessive fashion. It is more common in
Abnormalities in the cycling of biotin result in multiple carboxylase defi ciency.
Early treatment with biotin is usually effective in children with multiple carboxylase defi ciency.
Skin conditions such as alopecia and severe seborrhea are common with biotinidase defi ciency.
The combination of severe rash and an immunodefi ciency state resembles the presentation of severe combined immunodefi -ciency syndrome in children with biotinidase defi ciency.

880 P. J. B ELLI NO
isolated populations such as the Old Order Amish of Lancaster County, Pennsylvania and the Island Lake Indians of Canada. Children with this disorder are usually asymptomatic in infancy, but develop macrocephaly over the fi rst several months of life. Neuroimaging reveals bilateral frontal and basilar subdural collections as well as frontal and temporal lobe atrophy. It is believed that widening of the subdural space as a result of CNS anatomic changes causes undue tension on the bridging subdural veins resulting in tearing and sub-dural hematoma. Physicians evaluating infants for abusive head injury should rule out glu-taric aciduria type I if cerebral atrophy is present. It should be noted that extensive retinal hemorrhaging is not seen in this disorder, but single dot type hemorrhages have been rarely reported. Children develop progressive neurological fi ndings during the fi rst year of life which include epilepsy, brain atrophy, and dystonia/dyskinesia. Over time, the corpus stria-tum is permanently injured. Affected children frequently develop a metabolic crisis during an illness and may develop sudden onset of hypotonia seizures, opisthotonus, rigidity, and encephalopathy. Laboratory evaluation is variable; however most patients will demonstrate acidosis, hypoglycemia, ketonuria, hyperammonemia, and mild hepatic transaminase eleva-tions reminiscent of Reye syndrome. During acute episodes, serum amino acid assay usually demonstrates elevation of 2-aminoapidic acid, and urine amino acid assay are signifi cant for high levels of glutamine, glutamic acid, 2-aminoapidic acid, and saccharopine. Serum L-carnitine is invariably very low. Carnitine fractionation will reveal increased carnitine esters and an increase glutarylcarnitine level. Urine organic acid analysis reveals elevations of glutaric acid, 3-hydroxyglutaric acid, and glutaconic acid. CSF analysis may also demon-strate elevations of glutaric acid. Treatment of children in acute crisis is mostly supportive with special attention to supplementation with L-carnitine. Attainment of anabolism with hypertonic glucose infusions as well as administration of insulin is warranted in an acute crisis. Since pathologic evaluations of the basal ganglia of children with glutaric aciduria type 1 demonstrate low concentrations of GABA, other therapies aimed at increasing GABA levels have been attempted. These include the use of baclofen, valproic acid, and vigabatrin. Trials have been limited with variable results. Dietary restriction of protein (specifi cally lysine and tryptophan) has limited clinical effectiveness. Long-term use of L-carnitine may prevent the development acute crises in most patients.
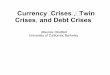
Mitochondrial Disorders The respiratory chain is a series of fi ve linked enzyme complexes that are embedded in the lipid bilayer of the mitochondria (Fig. 40-3 ). Each complex is composed of several sub-units that are derived from translation of both nuclear and mitochondrial DNA. The fi rst four complexes drive the process of oxidation, where electron transfer is used to generate an electrical gradient that ultimately converts molecular oxygen to water. The transfer of electrons from one complex to another is facilitated by two mobile carrier molecules, coen-zyme Q and cytochrome c. The fi fth complex, ATP synthase, utilizes the electrochemical gradient formed by the fi rst four enzyme complexes to develop a proton fl ux that drives the transfer of inorganic phosphate to ADP, thus forming the universal cellular energy source, ATP. This series of electrochemical reactions is governed by several feedback mechanisms, many of which are sensitive to changes in the electrical gradient along the inner mitochon-drial membrane. This complex system requires the presence of intact facilitative enzymes, carrier molecules and regulator proteins that are derived from both the nuclear and mito-chondrial genome. Mitochondrial disorders are the result of abnormalities or defi ciencies of any of the components or processes of the respiratory chain. A defect in any of the com-ponents can result in a poorly or non-functioning system, causing a wide array of cytopathology.
The respiratory chain enzymes are the product of translation of both mitochondrial DNA (mtDNA) and nuclear DNA. As such, mutations in either of these two DNA sources can result in mitochondrial disorders. Disorders resulting from nuclear DNA mutations typically follow usual Mendelian inheritance patterns. Disorders resulting from mutations of mtDNA, if not due to a spontaneous mutation, follow a pattern of maternal inheritance, as the mitochondria of all cells are directly descended from the oocyte. Since mitochondria are ubiquitous in human
Macrocephaly, cortical atrophy, and bilateral subdural hemato-mas are common in glutaric aciduria type I.
Initial presentation of glutaric aciduria type I may mimic abusive head injury.
L-carnitine should be adminis-tered to children with glutaric aciduria type I.

881 C HAPTER 40 • M ETABOLIC C R IS ES
cells, mitochondrial disorders can affect multiple organ systems simultaneously. Since acquired mutations of mtDNA are rather common, mutations during gametogenesis or post-conceptual mutations leading to populations of mutant mitochondria may occur. Consequently, cells may contain mutant as well as non-mutated mitochondria. In general, the activity of coexisting non-mutated mitochondria is usually enough to maintain cellular integrity. When populations of mutated mitochondria exceed disease specifi c tolerances, phenotypic disease becomes evi-dent. Other factors including the type of mutation and its effect on the translated proteins play a role in the phenotypic expression of mitochondrial disease. Mitochondrial disease should be considered in any patient who presents with evidence of global cytopathology with no clear underlying cause.
Mitochondrial disorders by their nature affect multiple organ systems. The CNS, particu-larly vision and hearing, are sensitive to abnormalities of mitochondrial function. Other organs commonly involved are the peripheral nervous system, heart, muscle, endocrine pan-creas, kidney, and liver in decreasing severity. Generalized developmental delay, stroke or stroke-like events, hypotonia, seizures, and oculomotor abnormalities are common in affected infants. Systemic symptoms may also include vomiting, failure to thrive, intestinal dysmotil-ity, respiratory insuffi ciency, arrhythmias and congestive heart failure. The most common laboratory abnormality found in most mitochondrial diseases is lactic acidemia with an ele-vated lactate to pyruvate ratio noted in the CSF or serum. Children are generally normogly-cemic on presentation. The diagnosis may be confi rmed on muscle biopsy fi ndings that demonstrate ragged-red fi bers (RRF’s) due to the accumulation of mitochondria along the sarcolemmal membrane. As RRF’s may not be seen in all mitochondrial disorders, specifi c mtDNA testing using PCR and Southern blot techniques or respiratory chain complex func-tional analysis may be required for defi nitive diagnosis. Recently, advanced gene sequencing techniques have been developed that can identify alterations in the mtDNA genome without the need for a muscle biopsy. The clinical fi ndings of known mitochondrial disorders are summarized in Table 40-4 .
Mitochondrial disease should be considered in any patient with evidence of global cytopathology with no clear underlying cause.
The most common laboratory abnormality found in most mitochondrial diseases is lactic acidemia with an elevated lactate to pyruvate ratio noted in the CSF.
NADH FADH2NAD+ FAD++ H2O
H+
H+H+ H+
P
Citrate
TCA Cycle
NADH
Malate
Fumarate
SuccinateSuccinyl CoA
α-ketoglutarate
Isocitrate
cis-Aconitate
NADHFADH2
NADH
Oxaloacetate
CoQ Cyt C
In oxidative phosphorylation,NADH and FADH2 derived fromthe TCA cycle are used to generate at H* gradientacross the mitochondrialmembrane. This gradient is used by complex V of therespiratory chain to convertADP and inorganic phosphateto ATP. (CoQ: Coenzyme Q;Cyt C: cytochrome c)
ATP
ADP1/2 02
Complex I Complex II Complex III Complex IV Complex V
FIGURE 40-3
Processes of oxidative phosphorylation

TAB
LE 4
0-4
MIT
OC
HO
ND
RIA
L D
ISO
RD
ERS
SEEN
IN
CH
ILD
HO
OD
SYN
DR
OM
E SY
MP
TO
MS
LAB
OR
AT
OR
Y F
IND
ING
S G
EN
ETIC
CA
US
E
Kea
rns-
Sayr
e sy
ndro
me
Ata
xia;
neu
ropat
hy;
pig
men
tary
ret
inal
ch
ange
s;
card
iom
yopat
hy
with
co
nduct
ion
ab
no
rmal
ities
; sh
ort
sta
ture
Elev
ated
CSF
pro
tein
(>10
0 m
g/dL)
; el
evat
ed s
erum
lact
ate;
el
evat
ed C
SF la
ctat
e to
pyr
uva
te r
atio
; R
RF’
s o
n m
usc
le
bio
psy
; po
sitiv
e So
uth
ern
blo
t hyb
ridiz
atio
n a
nal
ysis
of
DN
A f
rom
musc
le o
r blo
od
Spo
radic
del
etio
ns
or
duplic
a-tio
ns
of
mtD
NA
Pear
son
’s s
yndro
me
(bo
ne
mar
row
-pan
crea
s sy
ndro
me)
R
efra
cto
ry s
ider
obla
stic
an
emia
with
mar
row
fa
ilure
; exo
crin
e pan
crea
s in
suffi
cie
ncy
; m
alab
sorb
tion
; dea
th d
uri
ng
infa
ncy
Elev
ated
ser
um
lact
ate;
ele
vate
d C
SF la
ctat
e to
pyr
uva
te
ratio
; RR
F’s
on
musc
le b
iopsy
; po
sitiv
e So
uth
ern
blo
t fo
r m
tDN
A r
earr
ange
men
t in
blo
od s
pec
imen
s
Spo
radic
del
etio
ns
or
duplic
a-tio
ns
of
mtD
NA
Mito
cho
ndri
al e
nce
ph
alo
myo
pa-
thy
with
lact
ic a
cido
sis
and
stro
ke-li
ke e
pis
odes
(MEL
AS)
Rec
urr
ent
stro
ke-li
ke e
pis
odes
with
fo
cal l
esio
ns
of
the
par
ieto
-occ
ipta
l lo
bes
as
wel
l as
po
nto
cere
bel
lar
fi ber
s; d
egen
erat
ion
of
the
po
ster
ior
colu
mn
s an
d s
pin
oce
rebel
lar
trac
ts;
seiz
ure
s; v
om
itin
g; p
igm
enta
ry r
etin
opat
hy;
dea
fnes
s
Elev
ated
ser
um
lact
ate;
ele
vate
d C
SF la
ctat
e to
pyr
uva
te
ratio
; RR
F’s
on
musc
le b
iopsy
wh
ich
are
po
sitiv
e fo
r C
OX
ac
tivity
; Co
mple
x I a
nd t
o a
less
er d
egre
e C
om
ple
x IV
fu
nct
ion
dim
inis
hed
on
ass
essm
ent
of
resp
irat
ory
ch
ain
co
mple
xes;
abn
orm
al m
ole
cula
r an
alys
is o
f m
tDN
A f
rom
blo
od o
r m
usc
le
Poin
t m
uta
tion
of
mtD
NA
(3
24
3A
> G
)
Myo
clo
nic
epile
psy
with
RR
F’s
(MER
RF)
M
yocl
on
us;
epile
psy
; musc
le w
eakn
ess
and
musc
le w
astin
g; d
eafn
ess;
ata
xia;
lipo
mat
osi
s o
f th
e tr
un
k
Elev
ated
ser
um
lact
ate;
ele
vate
d C
SF la
ctat
e to
pyr
uva
te
ratio
; RR
F’s
on
musc
le b
iopsy
wh
ich
are
neg
ativ
e fo
r C
OX
ac
tivity
; Co
mple
x IV
an
d t
o a
less
er e
xten
t C
om
ple
x I
fun
ctio
n d
imin
ish
ed o
n a
sses
smen
t o
f re
spir
ato
ry c
hai
n
com
ple
xes;
abn
orm
al m
ole
cula
r an
alys
is o
f m
tDN
A f
rom
blo
od o
r m
usc
le
Poin
t m
uta
tion
of
mtD
NA
(8
34
4A
> G
)
Neu
roge
nic
wea
knes
s, a
taxi
a,
and r
etin
itis
pig
men
tosa
(N
AR
P); m
ater
nal
ly in
her
ited
leig
h s
yndro
me
(MIL
S)
Ata
xia;
pig
men
tary
ret
ino
pat
hy;
per
iph
eral
n
euro
pat
hy;
cer
ebra
l an
d c
ereb
ella
r at
rophy;
le
sio
ns
of
the
bas
al g
angl
ia
Elev
ated
ser
um
lact
ate;
ele
vate
d C
SF la
ctat
e to
pyr
uva
te
ratio
; RR
F’s
no
t se
en o
n m
usc
le b
iopsy
; Co
mple
x V
fu
nct
ion
dim
inis
hed
on
ass
essm
ent
of
resp
irat
ory
ch
ain
co
mple
xes;
abn
orm
al m
ole
cula
r an
alys
is o
f m
tDN
A f
rom
blo
od o
r m
usc
le
Poin
t m
uta
tion
of
mtD
NA
(8
99
3T >
G o
r T >
C)
Leig
h s
yndro
me
Psyc
ho
mo
tor
del
ay, p
yram
idal
sig
ns,
dys
ton
ia,
seiz
ure
s, a
pn
ea, h
yper
pn
ea, r
ecurr
ent
vom
itin
g,
occ
ulo
mo
tor
dis
turb
ance
s; f
oca
l sym
met
ric
lesi
on
s o
f th
e bra
inst
em, t
hal
amus,
an
d
po
ster
ior
colu
mn
s o
f th
e sp
inal
co
rd
Elev
ated
ser
um
lact
ate;
ele
vate
d C
SF la
ctat
e to
pyr
uva
te
ratio
; RR
F’s
no
t se
en o
n m
usc
le b
iopsy
; ass
essm
ent
of
resp
irat
ory
ch
ain
rev
eals
def
ects
of
term
inal
oxi
dat
ive
met
abo
lism
Multi
ple
cau
ses:
mtD
NA
an
d
nucl
ear
DN
A m
uta
tion
s;
auto
som
al r
eces
sive
an
d
X-li
nke
d f
orm
s
Mito
chin
dri
al
neu
ro-g
astr
oin
test
ial
ence
ph
alo
myo
pat
hy
(MN
GIE
)
Oph
thal
mo
par
esis
; per
iph
eral
neu
ropat
hy;
h
eari
ng
loss
; leu
koen
ceph
alo
pat
hy;
inte
stin
al
dysm
otil
ity; f
ailu
re t
o t
hri
ve
No
ele
vatio
n o
f la
ctat
e; R
RF’
s o
n m
usc
le b
iopsy
that
are
n
egat
ive
for
CO
X a
ctiv
ity; a
bn
orm
al t
hym
idin
e ph
osp
ho
-ry
lase
act
ivity
in b
uff
y co
at p
repar
atio
n o
f blo
od
Nucl
ear
DN
A m
uta
tion
; au
toso
mal
rec
essi
ve
mtD
NA
dep
letio
n s
yndro
me
(MD
S)
Infa
ntil
e m
yopat
hy;
ren
al f
ailu
re; h
epat
itis
lead
ing
to li
ver
failu
re; p
rogre
ssiv
e m
yopat
hy
lead
ing
to r
espir
ato
ry f
ailu
re; d
eath
by
age
3
No
ele
vatio
n o
f la
ctat
e; a
bn
orm
al li
ver
fun
ctio
n s
tudie
s; R
RF
are
pre
sen
t w
hic
h a
re n
egat
ive
for
CO
X a
ctiv
ity; a
bn
orm
al
com
par
ativ
e an
alys
is o
f m
tDN
A a
nd n
DN
A f
rom
blo
od o
r m
usc
le b
y PC
R o
r So
uth
ern
blo
t
Nucl
ear
DN
A m
uta
tion
; au
toso
mal
rec
essi
ve
Co
enzy
me
Q d
efi c
ien
cy
Fatig
abili
ty; s
low
ly p
rogre
ssiv
e w
eakn
ess
of
pro
xim
al li
mbs
and t
run
k; s
eizu
res;
men
tal
reta
rdat
ion
; ren
al f
ailu
re
Lact
ic a
cido
sis;
myo
glo
bin
uri
a; c
om
bin
ed a
citiv
ity o
f co
mple
xes
I-III a
nd I
I-III a
re r
educe
d; R
RF’
s o
n m
usc
le
bio
psy
; lip
id e
xces
s o
n m
usc
le b
iopsy
Un
kno
wn

883 C HAPTER 40 • M ETABOLIC C R IS ES
Unfortunately, there currently are no cures for most mitochondrial disorders. Supportive measures to improve nutrition, reduce acidosis, improve cardiac function and support venti-lation are often required during exacerbations. In coenzyme Q defi ciency, supplementation with oral coenzyme Q or its analogue, idebenone, has been demonstrated to halt progression, or in some cases, even reverse the deleterious effects of mitochondrial disease. Given that this coenzyme is relatively free of side effects, initiation of coenzyme Q once mitochondrial disease is suspected is reasonable. Creatine may also be benefi cial in some mitochondrial diseases. Creatine is converted to phosphocreatine, which is an energy storage compound in skeletal and heart muscle as well as the CNS.
Pyruvate carboxylase defi ciency is a rare but severe form of mitochondrial disease. Pyruvate carboxylase is a mitochondrial enzyme found primarily in the liver and kidney. It is considered to be the main regulator of gluconeogenesis. Its activity is modulated by con-centrations of acetyl CoA and unbound CoA as well as concentrations of ATP and ADP in the mitochondria. Since active pyruvate carboxylase is covalently bound to biotin, biotin defi ciency or enzyme abnormalities in the biotin cycle (holocarboxylase synthetase or bio-tinidase defi ciency) will result in a secondary pyruvate carboxylase defi ciency. Although pyruvate carboxylase is responsible for the conversion of pyruvate to oxaloacetate, the fi rst step in gluconeogenesis, children with this disorder rarely present with hypoglycemia. The more profound effect of this defi ciency is on the tricarboxyllic acid cycle, as oxaloacetate must be replenished continuously for the cycle to continue. A history of hypotonia and developmental delay is often present. Children ultimately develop seizures, tremors, spas-ticity, abnormal eye movements, and fi nally coma and death. Acute presentations are char-acterized by profound lactic acidosis. Three forms of the disorder have been described. Type B, the early onset form, presents in the immediate newborn period. This form is char-acterized by severe and continuous lactic acidosis, hepatomegaly, hyperammonemia, and excess a -ketoglutarate in the urine with elevations of alanine, citrulline, lysine, and praline noted on amino acid assay. Children with this form die early in infancy. Type A has a more variable age of onset, but usually presents by 5 months of age. These children also exhibit lactic acidosis, but it is less severe and can be corrected with medical interventions. Hyperammonemia is not usually seen. Excess a -ketoglutarate is found in the urine and amino acid assay is revealing only for an elevation of alanine. Profound developmental delay may ensue and severely affected children often succumb by 5 years of age. A third type has also been described that seems to be similar to type A but with somewhat variable enzyme activity, leading to a less severe presentation. Treatment is largely supportive. Recent case reports using triheptanoin and citrate show some promise. No large trials have been conducted.
Disorders of Ketolysis The disorders of ketolysis are a rare cause of an anion gap metabolic acidosis. These disor-ders are characterized by the presence of persisting ketoacidosis despite normal caloric intake and normal serum glucose levels. Lactate and ammonia levels are normal. Organic acid screen is also usually normal. The known enzyme defi ciencies responsible for produc-ing these disorders are succinyl Co-A transferase and acetoacetyl CoA thiolase defi ciency (Fig. 40-4 ). The diagnosis should be suspected in young children who present with unex-plained ketosis. As some children may present with marginally elevated glucose due primar-ily to a stress reaction, these children may be initially misdiagnosed as having diabetic ketoacidosis. Treatment consists of limitation of protein intake, provision of adequate calo-ries, and judicious alkaline therapy if acidosis is severe.
HYPOGLYCEMIA
Hypoglycemia may occur due to various disorders, including endocrinopathies, toxic inges-tions, starvation, sepsis, liver disease, and metabolic disorders. If possible, diagnostic labora-tory studies should be obtained to identify the exact cause prior to treatment (Fig. 40-5 ).
Although not helpful in all cases, coenzyme Q is safe to begin once the diagnosis of a mitochondrial disorder is suspected.
Biotin defi ciency or enzyme abnormalities in the biotin cycle will result in a secondary pyruvate carboxylase defi ciency.
Disorders of ketolysis are characterized by the presence of persisting ketoacidosis despite normal caloric intake and normal serum glucose levels.

884 P. J. B ELLI NO
If pre-treatment studies cannot be performed due to the patient’s critical condition, following stabilization, the patient can undergo carbohydrate deprivation in a controlled environment to delineate the exact cause of the hypoglycemia.
As described in Figure 40-5, initial laboratory studies should be completed to rule out common endocrine causes of hypoglycemia. Congenital hyperinsulinism previously referred to as nesidioblastosis, can lead to profound hypoglycemia in infancy and early childhood. Important diagnoses to exclude are isolated pancreatic adenoma, exogenous insulin adminis-tration (Munchausen by proxy), and inborn errors of metabolism. A form of hyperinsulinism that may be confused with an inborn error is the hyperinsulinism/hyperammonemia syn-drome (dominant glutamate dehydrogenase (GDH) defi ciency). In this disorder, a mutated form of GDH with loss of normal inhibitory control causes unregulated insulin secretion as well as ammonia synthesis. Children present typically during mid to late infancy with unex-plained hypoglycemia. Ammonia levels are 2-10 times normal. However, unlike children with hyperammonemia due to hepatic dysfunction or urea cycle defects, these children do not experience signifi cant obtundation or emesis. Interestingly, in this disorder, the ammonia level is not altered by protein ingestion. Hypoglycemia may be more evident after a protein rich meal. Treatment with benzoate and protein restriction as in the urea cycle defects is not effective in lowering the ammonia level. Treatment is supportive with correction of hypo-glycemia as previously described. Additionally, diazoxide is usually effective for long-term euglycemic management of these children. Regardless of the cause, the initial management of clinically signifi cant hypoglycemia entails the rapid administration of glucose followed by a continuous infusion to maintain a state of euglycemia. An initial glucose bolus of 0.5 g/kg will usually raise the blood glucose above the hypoglycemic range. Depending on the cause, continued glucose infusions may be needed for prolonged periods. A continuous glucose infusion rate of 5–15 mg/kg/min is often required to prevent further hypoglycemia.
As with many metabolic diseases, laboratory studies obtained prior to initial therapy may be the most revealing.
Some metabolic disorders may require generous and prolonged dextrose administration during crisis.
Liver
2 Acetyl CoA Acetoacetyl CoA
Acetoacetyl CoA
2 Acetyl CoA
TCA Cycle
In the liver, acetyl CoA is converted to acetoacetate through reactions mediatedby HMG CoA synthase and HMG CoA lyase. As the hepaocyte is not capable ofproducting succinyl CoA transferase, acetoacetate is delivered by the liver to thebloodstream for transport to several organs that are capable of utilizing ketonebodies (heart, kidney, CNS). In these organs, ketone bodies are re-transformedinto acetyl CoA which can react with oxaloacetate to enter the TCA cycle.
Acetoacetyl CoAThiolase
HMG-CoA Svnthase
HMG-CoA Lyase
Succinyl CoATransferase
3-Hydroxybutryate
Brain, Heart, Kidney
Acetoacetate Acetone
3-Hydroxy-3-Methylglutaryl CoA
FIGURE 40-4
Production and utilization of ketone bodies

885 C HAPTER 40 • M ETABOLIC C R IS ES
In addition to glucose administration, intravenous or intramuscular glucagon may be used to emergently increase the blood glucose. The recommended dosage of 0.025–0.1 mg/kg (not to exceed 1 mg per dose) usually raises the serum glucose level by approximately 20%. The dose may be repeated if necessary after 20 min. Failure to respond to glucagon may indicate an inability to liberate glycogen stores as seen in glycogen storage disease or a dis-order of gluconeogenesis.
Metabolic diseases that may have hypoglycemia as a prominent metabolic derangement include: 1. Disorders of Gluconeogenesis 2. Fatty Acid Oxidation Disorders 3. Glycogen Storage Diseases 4. Congenital Disorders of Glycosylation
Failure to respond to glucagon may indicate an inability to liberate glycogen stores as seen in glycogen storage disease or a disorder of gluconeogenesis.
• Branched-chain Amino acidurias MMA Propionic aciduria
• Tyrosingma type I
• Glutaric aciduria type I
Hypoglycemia
normal
elevated
low
low
normal
yes
yes
yes
no
no
no Lactateeleveted?
Growthhormone level
Insulinlevel
Cortisollevel
Ketoneselevated?
Severeacidosis?
• Disorders of gluconeogenesis• Glyoogen storeage diseases
Exclude:
• Sepsis• Liver disease• Starvation/malnutrition• Gastrointestinal loss• Toxic ingestion/overdose: Salicylates Alcohol Oral hypoglycemics Insulin Propranolol Pentamadine Quinine Disopyramide Vacor (rat poison)
Growth hormonedeficiency
• Waterhouse-Friedrickson Syndrome• Congenital adrenal hyperplasia• Glycerol kinase deficiency• Adrenoleukodystrophy• Addison’s disease
Adrenal Insufficiency:
• Islet cell adenoma• Islet cell hyperplasia• Nesidioblastosis• Beckwith-wiedemann S.• Congenital disorder of glycosolation• Disorders of KATP channel• Hyperinsulin/hyperammonia syndrome (dominant glutamate dehydrogenae hyperinsulinism)
• Carnitine deficiency• Carnitine transporter deficiency• CPT I deficiency• Translocase deficiency• VLCAD deficiency• MCAD deficiency• Multiple acyl-CoA dehydrogenase deficiency (MADD)
Disturbance of fatty acid oxidation:
Ketotichypoglycemia
FIGURE 40-5
Systematic approach to hypoglycemia

886 P. J. B ELLI NO
Disorders of Gluconeogenesis The disorders of gluconeogenesis result in the impairment of glucose formation from lactate/ pyruvate, glycerol and alanine (see Fig. 40-6 ). Four enzymes are known regulate this path-way: pyruvate carboxylase (discussed previously), phosphoenolpyruvate carboxykinase, fructose-1,6-bisphosphatase, and glucose-6-phosphatase. Mutations of each of these enzymes have been demonstrated to cause clinical disease. Biochemical analysis reveals a marked elevation in lactate with a concomitant elevation of pyruvate resulting in a normal lactate to pyruvate ratio. Defi ciencies of phosphoenolpyruvate carboxykinase , fructose - 1 , 6 - bisphos-phatase , and glucose - 6 - phosphatase all present with hypoglycemia during crisis. Pyruvate carboxylase defi ciency , despite the fact that it’s activity is responsible for the formation of oxaloacetate, the fi rst step in gluconeogenesis, rarely presents with hypoglycemia. This disor-der is further discussed in the section on mitochondrial disorders.
Treatment consists of rapid correction of hypoglycemia and acidosis. Volume expansion with isotonic saline and glucose administration will usually correct acidosis without the administration of sodium bicarbonate. Once enteral feeds are restarted, avoidance of certain carbohydrates may be recommended depending on the enzyme defi ciency.
Fructose 1 , 6 - bisphosphatase is responsible for the conversion of fructose 1,6-biphosphate to fructose 6-phosphate and inorganic phosphate. This critical step is needed for the conversion of not only fructose, but pyruvate, glycerol, and D-glycerate to glucose. Lack of this enzyme results in rapid onset of hypoglycemia during prolonged fasting. Presentation in early infancy is common. Infants present with signs and symptoms of hypoglycemia. Tachypnea is also a frequent presenting symptom due to concomitant acidosis. The majority of infants have keto-nuria, however ketones may be absent if suffi cient shunting of acetyl CoA away from the pro-cesses of b -oxidation occurs due to an excess of pyruvate. Neurological signs such as tremors, seizures, and apnea may be prominent. Mental status changes ranging from irritability to som-nolence and coma may occur. Older children may have an episodic pattern of illness consisting of acidosis and hypoglycemia occurring during periods of fast or with minor illnesses.
Disorders of gluconeogenesis should be considered in patients with marked elevation in lactate and pyruvate resulting in a normal lactate to pyruvate ratio.
Management of acute crisis centers around appropriate volume expansion and continuous dextrose administration.
Glucose
Glucose-6-phosphate
Glucose-6- phosphatase
Fructose-6-phosphate
Fructose-1, 6-bisphosphatase
Fructose-1,6-bisphosphate
Phosphoenolpyruvate
Pyruvate
Oxaloacetate
Shunt towards lactateand pyruvate productionwith disorders ofgluconeogenesis
Lactate
Phosphoenolpyruvatecarboxykinase
Glucose-1-phosphate
Glycogen
Fructose
Glycerol
FIGURE 40-6
Pathway of gluconeogenesis

887 C HAPTER 40 • M ETABOLIC C R IS ES
Examination may reveal hepatomegaly even in the early neonatal period. A presumptive diag-nosis can be made following a controlled fast where hypoglycemia usually occurs within 14–18 h and is not responsive to glucagon and worsened by the administration of fructose or glycerol. A defi nitive diagnosis is made by demonstrating reduced enzyme activity in hepatocytes after liver biopsy. Treatment requires correction of hypoglycemia and acidosis. Prolonged fasting should be avoided and fructose and sucrose intake should be minimized.
Defi ciency of phosphoenolpyruvate carboxykinase can produce hypoglycemia with an anion gap metabolic acidosis. Phosphoenolpyruvate carboxykinase plays a signifi cant role in the conversion of pyruvate to glucose by converting oxaloacetate to phosphoenolpyruvate early in the process of gluconeogenesis. Children may present at a later age with hypoglyce-mia and lactic acidosis. Common presenting signs include failure to thrive, hypotonia, and hepatomegaly. Unexplained hyperpyrexia has also been described. Recent data regarding the role of phosphoenolpyruvate carboxykinase as a major controlling enzyme in glyceroneo-genesis may explain the fi ndings of hypertriglyceridemia and hypercholesterolemia in sev-eral reported cases. Treatment during an acute metabolic attack consists of supportive care that includes rapid administration of glucose and restoration of circulating volume.
Glucose - 6 - phosphatase (G6P) is the fi nal enzyme required for gluconeogenesis. It facili-tates the conversion of glucose-6-phosphate to glucose. Phosphorylated glucose is not capa-ble of diffusion across cell membranes. Organs responsible for supplying glucose during times of fasting (liver, kidney, intestine) express G6P on the surface of the endoplasmic reticulum. Brain and muscle cells do not express G6P, which serves to prevent diffusion of phosphorylated forms of glucose out of muscle and brain tissue, ensuring maximal energy supply even in the face of marked hypoglycemia. In children with G6P defi ciency, the liver, kidney, and intestine are incapable of converting glucose-6-phosphate to free glucose and thus develop rapid intracellular accumulation of phosphorylated glucose and glycogen. Because of this, G6P defi ciency is often categorized as a storage disease, specifi cally, as Type I Glycogen Storage Disease (von Gerke’s Disease). Children may present in the early neonatal period, but more frequently come to medical attention between 2 and 4 months of age when fasting or an increased metabolic demand from an illness precipitates severe lactic acidemia and hypoglycemia.
Disorders of Fatty Acid Oxidation During times of fasting, b -oxidation of fatty acids provides metabolic energy. Fatty acids are stored in the form of triacylglycerol in the lipid bilayer of all cells and prominently in adipo-cytes. With fasting, lipase is activated to cleave triacylglycerol into its three constituent fatty acids. Fatty acids are generally categorized as short-chain, medium-chain, long-chain, and very long-chain molecules based on the number of carbon atoms they contain. Free fatty acids undergo activation by linking to a coenzyme A moiety under the direction of various acyl-CoA syntetases located on the outer surface of the mitochondrial membrane. The activated fatty acids, now fatty acyl-CoA molecules, are transported across the mitochondrial membrane to be oxidized. Short and medium-chain fatty acyl-CoA molecules can diffuse passively through this lipid bilayer, but long-chain and very long-chain fatty acyl-CoAs require the assistance of a transmembrane carrier. This carrier complex is composed of three subunits. The fi rst subunit, carnitine palmitoyl transferase I, binds the long and very long-chain fatty acyl-CoA to carnitine forming fatty acylcarnitines. These are then transported through the mitochondrial membrane by a transmembrane transporter, translocase. Once inside the mitochondria, the fatty acylcar-nitines are cleaved by carnitine palmitoyl transferase II to yield free carnitine and fatty acyl-CoA’s. The carnitine is then shuttled back out of the mitochondria by transferase.
Upon transfer into the mitochondria, fatty acyl-CoA molecules undergo the process of b -oxidation. Several acyl-CoA dehydrogenases and 3-hydroxyacyl-CoA dehydrogenases specifi c for various length fatty acids systematically and repeatedly remove two carbon sub-units from the lipid molecule, each time yielding FADH 2 and NADH which are shunted to the electron transport system to make ATP. In addition, with each two carbon removal, a molecule of acetyl-CoA is generated which is then used by the tricarboxylic acid cycle to further gener-ate FADH 2 and NADH. The acetyl-CoA can also be transported to hepatocytes where it is
The diagnosis of a disorder of gluconeogenesis should be considered in children who develop episodic hypoglycemia during minor illnesses or prolonged fasting.Fructose and sucrose can be toxic to children with fructose 1,6-bisphospatase defi ciency.

888 P. J. B ELLI NO
combined with acetoacteyl-CoA through a series of steps requiring hydroxymethyl glutaryl (HMG)-CoA synthase, HMG-CoA lyase, and D-3-hydroxybutyrate dehydrogenase to form ketone bodies that may be used as alternative energy sources for many body tissues.
Clinical disease manifests when an enzymatic abnormality exists anywhere in the process of fatty acid oxidation. Table 40-5 illustrates the more common enzyme and transport pro-tein defi ciencies that are known to result in clinical disease.
In general, fatty acid oxidation disorders (FAOD) should be suspected in any infant or child who presents with hypoglycemia, acidosis, myopathy/cardiomyopahty or myoglobinu-ria. Although hypoketotic hypoglycemia is not present in all forms of fatty acid disturbances, this combination is highly suggestive for a FAOD. It is important to note that most children will exhibit no laboratory abnormalities between episodes of metabolic crisis. It is therefore critical to have a high index of suspicion for FAODs in children presenting with unexplained hypoglycemia, acidosis or cardiomyopathy. Initial studies should include blood for glucose, pH, free fatty acids, ammonia, carnitine profi le, liver function studies, creatine kinase, lactate/pyruvate, and serum electrolytes. Further diagnostic studies may include urine for organic acids, plasma acylcarnitine profi le, and free fatty acid profi le. Fibroblast studies to analyze oxidation and specifi c enzyme activity may be obtained for defi nitive diagnosis. If death is imminent and the child has undiagnosed siblings or the parents plan further pregnancies, obtaining fi broblast studies prior to death is required to aid in genetic counseling and possible diagnosis of siblings. Provocative testing including a prolonged fast should only be done in a controlled setting in centers with metabolic expertise. For some disorders, challenge with administration of medium or long-chain triglycerides will cause enhanced excretion of a diagnostic metabolite. It should be noted, however, that administration of MCT oil to children with medium-chain acyl-coenzyme A dehydrogenase (MCAD) defi ciency can result in cata-strophic consequences. As such, MCAD defi ciency should be ruled out prior to this form of testing. Newborn screening of dried blood spots using mass spectroscopy to detect abnormal levels of acylcarnitines is available in most states. Repeat testing beyond the newborn period may yield a rapid diagnosis. Additional diagnostic clues may be gained upon subspecialty evaluation. Ophthalmologic examination may reveal pigmenatry retinitis. An echocardio-gram should be obtained given the high frequency of cardiomyopathy in these disorders.
Treatment of FAOD is supportive. Preventative measures are invaluable. In general, children with these disorders are maintained on a low fat diet with no more than 25% of daily calories from fat. MCT oil supplementation may be used to provide the daily lipid requirements in chil-dren with disturbances of long and very-long chain fatty acids. MCT oil is toxic to children with MCAD defi ciency, and should be avoided at all costs in these patients. Prevention of fasting by use of corn starch (1–2 g/kg/dose) or by use of continuous gastric feeding in infants may be nec-essary to prevent lipid catabolism. During times of metabolic stress, additional administration of carbohydrate may be needed to prevent hypoglycemia. Carnitine may be of some help for carni-tine transporter defects, but generally is of no use for other disorders. Treatment of the child who presents with severe metabolic crisis requires glucose, fl uid and electrolyte stabilization. Administration of glucose at a rate of 7–10 mg/kg/min should be adequate to control hypoglyce-mia and prevent further fat catabolism. Serum glucose should be closely monitored and the glu-cose infusion rate adjusted to prevent further hypoglycemia. Carnitine administration in extreme metabolic crisis is controversial but probably has no deleterious effects. Ribofl avin (200 mg/kg/day) may be useful in treating children with multiple acyl-CoA dehydrogenase disorder.
Glycogen Storage Diseases The glycogen storage diseases are a group of 12 disorders characterized by abnormal glycogen synthesis or catabolism. Glucose that is not needed for immediate energy consumption is stored as glycogen, therefore many of these disorders are characterized by the development of hypoglycemia and ketoacidosis during times of fasting. The two major sites for the storage of glycogen are the liver and muscle tissue, therefore hepatic and muscular (including cardiac) dysfunction is common in affected children. Table 40-6 lists the major glycogen storage diseases, the enzyme defect, and their more common symptoms. Glucose 6 phosphatase defi -ciency is discussed in detail under disorders of gluconeogenesis.
A disorder of fatty acid oxidation should be suspected in any patient with unexplained myopathy, cardiomyopathy or myoglobinuria.
The classic laboratory hallmark of disorders of fatty acid oxidation is hypoglycemia without ketosis.
Administration of medium-chained triglycerides (MCT oil) to children with MCAD defi ciency is contraindicated.
Administration of cornstarch will provide a continual carbohydrate source and may prevent unwanted fasting catabolism in children with many inborn errors.
Glycogen storage diseases are characterized by the development of hypoglycemia and ketoacidosis during times of fasting.
Hepatic and muscle disease, including myocardial dysfunction, are common in glycogen storage diseases.

TAB
LE 4
0-5
DIS
OR
DER
S O
F FA
TT
Y A
CID
OX
IDA
TIO
N
DE
FIC
IEN
CY
STA
TE
SYM
PT
OM
S LA
BO
RA
TO
RY
FIN
DIN
GS
TR
EAT
ME
NT
Car
niti
ne
tran
spo
rter
def
icie
ncy
H
ypo
glyc
emia
; dila
ted c
ardio
myo
pat
hy;
pro
gre
ssiv
e m
usc
le
wea
knes
s; m
usc
le li
pid
sto
rage
Lo
w o
r un
det
ecta
ble
pla
sma
carn
itin
e; d
iagn
osi
s co
nfir
med
by
fibro
bla
st u
pta
ke s
tudie
s fo
r ca
rniti
ne
or
mo
lecu
lar
anal
ysis
of
OC
TN
2 g
ene
Car
niti
ne
100
mg/
kg/d
CPT
I defi
cie
ncy
R
are;
see
n m
ost
ly in
Hutt
erite
India
ns
of
No
rth
ern
US
and
Can
ada;
epis
odic
spel
ls w
ith a
ltere
d m
enta
l sta
tus,
sei
zure
s,
com
a duri
ng
vira
l illn
esse
s
Epis
odic
hyp
oke
totic
hyp
ogl
ycem
ia; m
ild h
yper
-am
mo
nem
ia; n
orm
al o
r sl
igh
tly e
leva
ted
carn
itin
e w
ith a
hig
h f
ree
carn
itin
e fr
actio
n
Suppo
rtiv
e
Tran
slo
case
defi
cie
ncy
Ep
iso
dic
spel
ls w
ith a
ltere
d m
enta
l sta
tus,
sei
zure
s, c
om
a duri
ng
vira
l illn
esse
s; c
ardia
c ar
rhyt
hm
ias
and c
ardio
myo
apth
y Ep
iso
dic
hyp
oke
totic
hyp
ogl
ycem
ia; h
yper
am-
mo
nem
ia; g
ross
ly e
leva
ted a
cylc
arn
itin
e to
fre
e ca
rniti
ne
ratio
; dic
arb
oxy
llic
acid
uri
a o
n o
rgan
ic
acid
an
alys
is
Suppo
rtiv
e un
less
car
dio
myo
pta
hy
is p
rese
t (c
ardio
myo
pat
hy
may
re
spo
nd t
o c
arn
itin
e su
pple
men
tatio
n)
CPT
II d
efi c
ien
cy
Pres
ents
in la
te h
ildh
oo
d w
ith r
ecurr
ent
epis
odes
of
myo
glo
bi-
nuri
a fo
llow
ing
pro
lon
ged e
xerc
ise,
fas
ting,
fev
er, o
r em
otio
nal
str
ess;
rh
abdo
myo
lisis
may
pre
cipitat
e re
nal
fa
ilure
; pat
ien
ts w
ell b
etw
een
epis
odes
No
rmal
glu
cose
leve
ls; l
ow
to
tal p
lasm
a ca
rniti
ne
with
an
incr
ease
d a
cylc
arn
itin
e fr
actio
n;
lon
g-ch
ain
acy
lcar
niti
nes
may
be
elev
ated
; no
dic
arb
oxy
llic
acid
uri
a n
ote
d
Suppo
rtiv
e
VLC
AD
defi
cie
ncy
Ea
rly
on
set
card
iac
and s
kele
tal m
yopth
ay; c
ardia
c ar
rhyt
h-
mia
s; r
ecurr
ent
rhab
do
myo
lisis
; hep
ato
cellu
lar
failu
re
May
pre
sen
t w
ith h
ypo
keto
tic h
ypo
glyc
emia
; hyp
eram
mo
nem
ia; a
bn
orm
al li
ver
fun
ctio
n
studie
s; e
leva
ted u
rin
e dic
arb
oxy
llic
acid
Suppo
rtiv
e
MC
AD
In
term
itten
t n
euro
logic
al s
ympto
ms
ran
gin
g fr
om
agitat
ion
to
co
ma
beg
inn
ing
in t
he
seco
nd y
ear
of
life;
may
no
t pre
sen
t un
til a
do
lesc
ence
; sudden
dea
th (m
ay b
e co
nfu
sed w
ith
SID
S); h
epat
ic s
teat
osi
s; m
usc
le w
eakn
ess
No
lab a
bn
orm
aliti
es b
etw
een
epis
odes
un
less
pat
ien
t h
as h
epat
ic s
teat
osi
s; d
uri
ng
atta
cks
pat
ien
ts d
emo
nst
rate
hyp
oke
totic
hyp
ogl
y-ge
mia
, ele
vate
d d
icar
boxy
llic
acid
in u
rin
e, a
s w
ell a
s hyp
eram
mo
nem
ia
Suppo
rtiv
e
SCA
D
Neo
nat
al o
nse
t; e
pis
odes
of
rapid
ly p
rogre
ssiv
e n
euro
logic
al
det
erio
ratio
n w
ith h
yper
refl e
xia,
hyp
oto
nia
, an
d c
om
a;
failu
re t
o t
hri
ve; m
yopat
hy
Hyp
ogl
ycem
ia is
no
t co
mm
on
; hyp
eram
mo
nem
ia;
ethyl
mal
on
ic a
nd m
ethyl
succ
inic
aci
d e
leva
tion
s Su
ppo
rtiv
e
Lon
g-ch
ain
3-h
ydro
xyac
yl-
Co
A d
ehyd
roge
nas
e defi
cie
ncy
(LC
HA
D)
Car
dio
myo
pat
hy;
myo
pat
hy;
per
iph
eral
neu
ropat
hy;
rec
urr
ent
myo
glo
bin
uri
a; h
epat
oce
llula
r fa
ilure
; pig
men
tary
re
tino
pat
hy
Hyp
ogl
ycem
ia; e
leva
ted C
K; a
bn
orm
al li
ver
fun
ctio
n s
tudie
s Su
ppo
rtiv
e
Multi
ple
Acy
l-C
oA
deh
ydro
gen
ase
dis
ord
er
(MA
DD
; glu
tari
c ac
iduri
a ty
pe
II)
Neo
nat
al o
nse
t is
co
mm
on
; sev
ere
hyp
oto
nia
; fac
ial d
ysm
or-
ph
ism
s; c
ystic
kid
ney
s; s
truct
ura
l bra
in a
no
mal
ies
(age
nes
is
of
the
cere
bel
lar
verm
is, h
ypo
pla
stic
tem
po
ral l
obes
, fo
cal
dysp
lasi
a o
f th
e ce
rebra
l co
rtex
)
Elev
ated
uri
nar
y gl
uta
ric,
eth
ylm
alo
nic
, an
d a
dip
ic
acid
s ; m
etab
olic
aci
do
sis;
fas
ting
hyp
oke
totic
hyp
ogl
ycem
ia; fi
bro
bla
st d
emo
nst
rate
s en
zym
e def
ects
Som
e fo
rms
resp
on
d t
o r
ibo
fl avi
n
supple
men
tatio
n

TAB
LE 4
0-6
SUM
MA
RY
OF
GLY
CO
GEN
STO
RA
GE
DIS
EASE
S
DIS
EAS
E E
NZ
YM
E D
EFE
CT
S
IGN
S A
ND
SY
MP
TO
MS
LAB
OR
AT
OR
Y F
IND
ING
S S
PEC
IFIC
TH
ER
AP
EU
TIC
O
PT
ION
S
GSD
0
Live
r gl
yco
gen
syn
thas
e def
icie
ncy
N
eon
atal
on
set
Ket
otic
hyp
ogl
ycem
ia, p
ost
pra
ndia
l lac
tic a
cido
sis,
el
evat
ed u
ric
acid
, ele
vate
d s
erum
lipid
s, p
oo
r re
spo
nse
to
glu
cago
n
Co
rnst
arch
GSD
I (v
on
G
ierk
e’s
dis
ease
) G
luco
se-6
-ph
osp
hat
ase
defi
cie
ncy
H
epat
om
egal
y, n
eph
rom
egal
y, n
eon
atal
on
set
but
mo
re c
om
mo
nly
at
3–
4 m
on
ths
of
age,
sk
in x
anth
om
as, r
etin
al a
dip
osi
ty, n
eutr
ope-
nia
, ble
edin
g te
nden
cies
, hyp
erte
nsi
on
with
re
nal
dis
ease
Ket
otic
hyp
ogl
ycem
ia, e
lvat
ed la
ctat
e, e
leva
ted u
ric
acid
, ele
vate
d s
erum
lipid
s, p
oo
r re
spo
nse
to
gl
uca
gon
, liv
er t
ran
sam
inas
es u
sual
ly n
orm
al,
pro
lon
ged b
leed
ing
time
Co
rnst
arch
, no
cturn
al f
eeds,
al
lopuri
no
l, G
-CSF
, re
stri
ctio
n o
f fr
uct
ose
an
d
gala
cto
se in
th
e die
t
GSD
II (
Pom
pe’
s dis
ease
) Ly
soso
mal
aci
d m
alta
se
defi
cie
ncy
V
aria
ble
age
of
on
set
dep
endin
g o
n t
he
deg
ree
of
enzy
me
activ
ity (i
nfa
ncy
to
ear
ly a
dult-
ho
od),
glo
bal
hyp
oto
nia
, car
dio
myo
pat
hy,
C
HF,
hep
ato
meg
aly,
Dia
gno
sis
con
fi rm
ed b
y al
tere
d a
ctiv
ity o
f ac
id
a -g
luco
sidas
e ac
tivity
on
musc
le b
iopsy
an
d
fi bro
bla
st c
ultu
re, E
MG
rev
eals
myo
pat
hy,
ele
vate
d
CK
, LFT
’s m
ay b
e el
evat
ed, n
orm
al r
espo
nse
to
gl
uca
gon
adm
inis
trat
ion
Tria
ls o
f re
com
bin
ant
hum
an a
-glu
cosi
das
e re
pla
cem
ent
are
curr
ently
un
der
way
GSD
IIb
(Dan
no
n’s
dis
ease
) Ly
soso
me-
asso
ciat
ed
mem
bra
ne
pro
tein
2
defi
cie
ncy
(LA
MP-
2)
Proxi
mal
hyp
oto
nia
, car
dio
myo
pat
hy,
CH
F,
men
tal r
etar
dat
ion
, mal
es a
ffec
ted e
arlie
r an
d m
ore
sev
erly
th
an f
emal
es
Elev
ated
CK
, MR
I may
sh
ow
pun
ctifo
rm h
yper
den
sitie
s in
supra
ten
tori
al w
hite
mat
ter
and c
ort
ical
atr
ophy,
dia
gno
sis
con
fi rm
ed b
y ab
sen
ce o
f an
ti-LA
MP-
2
stai
nin
g o
f per
iph
eral
lym
ph
ocy
tes,
fi bro
bla
sts,
or
on
m
usc
le b
iopsy
Suppo
rtiv
e
GSD
III (l
imit
dex
trin
osi
s;
Co
ri’s
dis
ease
)
Gly
coge
n d
ebra
nch
er
defi
cie
ncy
H
epat
om
egal
y, o
nse
t in
infa
ncy
, sh
ort
sta
ture
, sp
len
om
egal
y, m
usc
le w
eakn
ess
in s
eco
nd
dec
ade
of
life
Ket
otic
hyp
ogl
ycem
ia, m
ild la
ctat
e el
evat
ion
s, m
ild
elev
atio
n o
f lip
ids,
no
res
po
nse
to
glu
cago
n if
fa
stin
g, e
leva
ted C
K, e
leva
ted R
BG
gly
coge
n
Co
rnst
arch
GSD
IV
(A
nder
sen
’s
dis
ease
)
Gly
coge
n b
ran
chin
g en
zym
e defi
cie
ncy
Pr
esen
ts in
infa
ncy
, hep
ato
meg
aly,
fai
lure
to
th
rive
, ulti
mat
ely
dev
elo
p c
irrh
osi
s, p
ort
al
hyp
erte
nsi
on
, var
ices
, dea
th b
y 5
yea
rs o
f ag
e, h
ypo
glyc
emia
is a
late
fi n
din
g, m
ay
hav
e hyp
oto
nia
an
d c
ardio
myo
pat
hy
Elev
ated
LFT
’s, h
yper
bili
rubin
emia
, liv
er b
iopsy
dem
on
stra
tes
bas
oph
ilic
incl
usi
on
s in
hep
ato
cyte
s,
defi
niti
ve d
iagn
osi
s do
ne
by
mea
suri
ng
bra
nch
ing
enzy
me
activ
ity in
hep
ato
cyte
s, m
yocy
tes,
leuko
-cy
tes,
or
fi bro
bla
sts
Live
r tr
ansp
lan
t in
appro
pri
-at
e pat
ien
ts
GSD
V (M
cArd
le’s
dis
ease
) M
usc
le p
ho
sph
ory
lase
defi
cie
ncy
Sy
mpto
ms
fi rst
no
ticea
ble
in y
oun
g ad
ulth
oo
d,
fatig
uab
ility
, dar
k uri
ne
afte
r ex
erci
se
Myo
glo
bin
uri
a, e
leva
ted C
K a
t re
st, e
lvat
ed a
mm
on
ia,
ino
sin
e, h
ypoxa
nth
ine
and u
ric
acid
aft
er e
xerc
ise,
dec
reas
ed b
loo
d la
ctat
e af
ter
exer
cise
Sucr
ose
, fru
cto
se, o
r gl
uco
se
adm
inis
trat
ion
, glu
cago
n
adm
inis
trat
ion
, vit
amin
B
6 s
upple
men
tatio
n
GSD
VI (
Her
s dis
ease
) Li
ver
ph
osp
ho
ryla
se
defi
cie
ncy
H
epat
om
egal
y, o
nse
t in
ear
ly c
hild
ho
od,
X-li
nke
d, g
row
th r
eatr
dat
ion
H
ypo
glyc
emia
, mild
ele
vatio
n o
f se
rum
lipid
s, n
orm
al
resp
on
se t
o g
luca
gon
Su
ppo
rtiv
e
GSD
VII (T
arui’s
dis
ease
) Ph
osp
ho
fruct
oki
nas
e defi
cie
ncy
Sy
mpto
ms
beg
in in
mid
-ch
ildh
oo
d, d
ark
uri
ne
with
exe
rcis
e, f
atig
uab
ility
(sim
ilar
to t
ype
V
but
earl
ier
on
set)
Dec
reas
ed a
ctiv
ity o
f ph
osp
ho
fruct
oki
nas
e in
RB
C’s
an
d m
yocy
tes,
myo
glo
bin
uri
a, e
lvat
ed b
iliru
bin
, el
evat
ed r
etic
ulo
cyte
co
un
t, hyp
eruri
cem
ia, w
ors
e ex
erci
se t
ole
ran
ce a
fter
hig
h c
arb
ohyd
rate
mea
l
No
ne,
ket
oge
nic
die
t m
ay
be
hel
pfu
l

GSD
VII
I (G
SD IX
b)
Auto
som
al li
ver
and
musc
le p
ho
sph
ory
lase
ki
nas
e defi
cie
ncy
Sym
pto
ms
beg
in e
arly
in li
fe, h
epat
om
egal
y,
gro
wth
ret
ardat
ion
, hyp
oto
nia
, fat
igab
ility
R
educe
d a
ctiv
ity o
f ph
osp
ho
ryla
se k
inas
e ac
tivity
in
musc
le a
nd li
ver
cells
N
on
e
GSD
IX
(GSD
IX
a)
X-li
nke
d li
ver
ph
osp
ho
ry-
lase
kin
ase
defi
cie
ncy
X
-lin
ked, s
ympto
ms
beg
in in
ear
ly c
hild
ho
od
(1–
5 y
ears
of
age)
, hep
ato
meg
aly,
gro
wth
re
tard
atio
n, m
ild m
oto
r del
ay
Mild
ele
vatio
n o
f ch
ole
ster
ol,
trig
lyce
rides
, an
d li
ver
tran
sam
inas
es, f
astin
g hyp
erke
tosi
s, h
ypo
glyc
emia
is
mild
with
a n
orm
al r
espo
nse
to
glu
cago
n
No
ne
is n
eeded
as
the
dis
ord
er r
eso
lves
ove
r tim
e an
d a
s ad
ults
pat
ien
ts a
re m
ost
ly
asym
pto
mat
ic
GSD
IX
c A
uto
som
al li
ver
ph
osp
ho
-ry
lase
kin
ase
defi
cie
ncy
Seve
re s
ympto
ms
beg
in e
arly
, hep
ato
meg
aly
and ja
un
din
ce, r
apid
pro
gre
ssio
n t
o c
irrh
osi
s El
evat
ed L
FT’s
, red
uce
d a
ctiv
ity o
f ph
osp
ho
ryla
se
kin
ase
activ
ity in
hep
ato
cyte
s N
on
e
GSD
IX
d
Musc
le s
pec
ifi c
ph
osp
ho
-ry
lase
kin
ase
defi
cie
ncy
Pres
ent
in a
do
lesc
ence
or
youn
g ad
ulth
oo
d,
cram
ps
and d
ark
uri
ne
on
exe
rcis
e, m
usc
le
wea
knes
s, m
usc
le a
tro
phy
Myo
glo
bin
uri
a, e
leva
ted C
K w
ith e
xerc
ise,
red
uce
d
activ
ity o
f ph
osp
ho
ryla
se k
inas
e ac
tivity
in m
yocy
tes
No
ne
GSD
IX
f Ph
osp
ho
ryla
se k
inas
e defi
cie
ncy
lim
ited t
o
hea
rt
Pres
ents
in in
fan
cy, s
ever
e co
nge
nital
ca
rdio
myo
pat
hy,
arr
hyt
hm
ias,
fai
lure
to
th
rive
, hep
ato
meg
aly,
hyp
oto
nia
Red
uce
d a
ctiv
ity o
f ph
osp
ho
ryla
se k
inas
e ac
tivity
in
card
iac
myo
cyte
s N
on
e

892 P. J. B ELLI NO
TABLE 40-7
THE CONGENITAL DISORDERS OF GLYCOSYLATION
DISEASE/ENZYME CLINICAL CHARACTERISTICS AND COMMENTS
CDG-Ia (Phosphomannomutase deficiency)
Infants exhibit abnormal eye movements, hypotonia, feeding problems; may be dysmorphic with abnormal subcutaneous fat deposits, nipple retraction; older children develop retinitis pigmentosa, epilepsy, stroke-like episodes; may go on to develop severe organ disease with acute cerebral hemor-rhage, liver failure, coagulopathy, cardiomyopathy, nephrotic syndrome, severe neurological degenera-tion; mortality is 20% in fi rst several years of life, may live to adulthood
CDG Ib (Phosphomannose isomerase defi ciency)
Symptoms usually present by 12 months; commonly develop hepatic fi brosis, protein losing enteropathy, hyperinsulinemic hypoglycemia; the only CDG that has effective treatment (oral D-mannose at doses of 100–150 mg/kg 3–6 times daily)
CDG Ic (Glucosyltransferase I defi ciency)
Mild to moderate mental and motor delay, severe axial hypotonia, epilepsy, ataxia, strabismus
CDG Id (Mannosyltransferase VI defi ciency)
In infancy develop severe motor and mental retardation and hypsarrhythmia; associated congenital fi ndings include microcephaly, optic atrophy, coloboma, and brain atrophy; case reports of hyperinsu-linemic hypoglycemia
CDG Ie (Dolichol-phosphate-mannose synthase I defi ciency)
Pronounced psychomotor delay, epilepsy, hypotonia, failure to thrive, optic atrophy; coagulopathy is common
CDG If (Mannose-P-dolichol utilization defect)
Associated with congenital dwarfi sm, congenital ichthyosis, psychomotor delay, and retinopathy; thrombosis from defi ciencies in protein C, S and antothrombin III defi ciency
CDG IIa (N-acetylglucosaminyl-transferase II defi ciency)
Congenital dysmorphic features, associated with severe mental retardation and epilepsy
CDG IIb (Glucosidase I defi ciency)
Congenital dysmorphic features; neonatal onset of epilepsy, hypoventilation, feeding problems, heaptom-egaly; death by 2 months
CDG IIc (GDP-fucose trans-porter defi ciency; leukocyte adhesion disorder II)
Congenital craniofacial dysmorphic features with microcephaly; associated with severe mental retarda-tion, hypotonia, growth failure, and recurrent infections; labs show marked leukocytosis even when not acutely infected
Galactosyltransferase defi ciency
Associated with psychomotor delay, macrocephaly, hyperlaxity of joints, hyperelastic skin, aged appear-ance (appears as a progeria-like form of Ehlers-Danlos syndrome)
EXT1/EXT2 complex defi ciency
Multiple exostoses become prominent by early childhood which ultimately cause severe deformities; may develop sarcoma in lesions; cause compression of nerves and vessels
Congenital Disorders of Glycosylation The congenital disorders of glycosylation (CDG) are a collection of inherited diseases that impair protein N-glycosylation. The clinical appearance of CDG patients is quite diverse. The clinical pathology results from depressed synthesis or remodeling of oligosaccharide moieties of glycoproteins. These defects in the biosynthesis of the oligosaccharide precursor for N-glycosylation lead to decreased occupancy of glycosylation sites. The result is the formation of abnormal glycoproteins affecting structure and metabolic functions, resulting in multiple organ dysfunctions. The most thoroughly studied subset of CDG are the type I defects affecting N-glycosylation. The broad clinical presentations of these glycosylation defects are summarized in Table 40-7 . Patients with type 1B disease do not have neurologic disease and may present with hyperinsulinemic hypoglycemia along with other features.

893 C HAPTER 40 • M ETABOLIC C R IS ES
1. The management of acute metabolic crisis due to organic aci-demias may include all the following EXCEPT: A. Dextrose infusion at 5–15 mg/kg/min B. Sodium bicarbonate C. Insulin infusion of 0.05–0.1 units/kg/h D. TPN containing more than 3 g/kg/day of protein E. L-carnitine
2. Glutaric aciduria type I may mimic abusive head injury as it may present with: A. Diffuse retinal hemorrhages B. Subdural hematoma C. Bruising D. Pathologic fractures E. Severe diaper dermatitis
3. A disorder of fatty acid oxidation should be suspected in an infant with: A. Unexplained cardiomyopathy and episodic hypoglycemia B. Hypoglycemia with an elevated lactate to pyruvate ratio C. Pronounced elevation of ketones despite euglycemia D. Obtundation with severe hyperammonemia and respiratory
alkalosis E. Hypoglycemia that does not respond to glucagon
administration
4. Children with mitochondrial disorders may present with the following symptoms: A. Profound intestinal dysmotility and delayed gastric
emptying B. Stroke-like episodes C. Generalized motor weakness D. Pigmentary retinopathy E. All of the above
5. An infant with a history of motor delay and severe seborrhea presents with progressive lethargy and vomiting. Initial labo-ratory analysis reveals marked acidosis with elevation of lac-tate and ketones as well as hyperammonemia. The most useful therapy in managing this infant is: A. Administration of 0.025–0.1 mg/kg of glucagon B. Hemodialysis C. Administration of 100 mg/kg/day of L-carnitine D. Administration of 10 mg/day of biotin E. Supplementation with ribofl avin
6. A 9 week old 4.0 kg male infant is transported to the PICU for treatment of presumed sepsis. He had presented to the emer-gency department with progressive lethargy and poor feeding. He was found to be febrile to 38.1°C, tachypneic to 64 breaths/min, tachycardic to 158 beats/min and had a blood pressure of 88/52 mmHg. He has palpable pulses and a capillary refi ll of 2 s. Blood, cerebrospinal and urine cultures are obtained. He is given broad spectrum antibiotics, a 20 mL/kg NS bolus and is transferred to the PICU due to obtundation, progressive
tachypnea and severe acidosis. He has an unremarkable chest radiograph, head CT and complete blood count. Serum chem-istries are: sodium of 145 mEq/L, chloride 98 mEq/L, glucose of 111 mg/dL and bicarbonate of 14 mEq/L. Serum lactate drawn from free fl owing arterial blood is 2.2 mMol/L, pH is 7.06, pCO 2 23 mmHg and pO 2 90 mmHg on room air. He has made 22 mL of urine since his bolus. His urine has large amount of ketones. The most appropriate assessment and care plan is: A. An organic acidemia should be suspected. Serum pyruvate,
ammonia, amino acids and urine organic acids should be obtained. Prevention of catabolism, supportive care, serial electrolyte and glucose determinations and the continuation of antibiotics are all warranted.
B. A disorder of fatty acid oxidation should be suspected. Serum pyruvate, ammonia, amino acids, urine ketones and organic acids should be obtained. Prevention of catabolism, support-ive care, serial electrolyte and glucose determinations are all warranted. Antibiotics should be discontinued.
C. A disorder of fatty acid oxidation should be suspected. Serum pyruvate, amino acids, ammonia, urine ketones and organic acids should be obtained. Prevention of catabolism, support-ive care, serial electrolyte and glucose determinations are all warranted. Antibiotics should be continued.
D. A urea cycle defect should be suspected. Serum ammonia should be obtained. Prevention of catabolism, supportive care, serial electrolyte and glucose determinations, continua-tion of antibiotics and preparation for aggressive treatment of hyperammonemia are all warranted.
E. An inborn error of metabolism is unlikely. Placement of a central venous line, measurement of mixed venous saturation and continued antibiotics are warranted
7. A 12 week old 4.2 kg male infant is transported to the PICU for treatment of presumed meningitis. He presented with vomiting, poor feeding and progressive lethargy. He is found to be febrile to 38.3°C, tachypneic to 74 breaths per minute, tachycardic to 148 beats per minute and has a blood pressure of 108/52 mmHg. He is warm, has palpable pulses and a capil-lary refi ll of 2 s. He is diffi cult to arouse, has a full fontanel and moves all extremities with stimulation. Blood, cerebrospinal and urine cultures are obtained. He is given broad spectrum antibiotics. He has an unremarkable chest radiograph, head CT, complete blood count and serum glucose. Serum chemis-tries are: sodium of 138 mEq/L, chloride 108 mEq/L, glucose of 131 mg/dL and bicarbonate of 20 mEq/L. His CSF demon-strates no cells, normal protein and glucose. Arterial lactate is 2.7 mMol/L, pH is 7.56, pCO 2 22 mmHg and pO 2 90 mmHg on room air. He has a 3 min generalized seizure that responds to lorazepam. An inborn error is suspected. The most correct assessment and care plan is: A. An organic acidemia is most likely. Serum pyruvate, amino
acids, ammonia and urine organic acids should be obtained. Pending defi nitive diagnosis, the prevention of catabolism, supportive care, serial lab testing and the continuation of antibiotics are all warranted.
REVIEW QUESTIONS

894 P. J. B ELLI NO
1. D 2. B 3. A 4. E
5. D 6. A 7. C Questions 6 and 7
ANSWERS
B. A disorder of fatty acid oxidation is most likely. Serum pyru-vate, amino acids, ammonia, urine ketones and organic acids should be obtained. Administration of glucose at a rate of 7–10 mg/kg/min should be initiated to prevent hypoglycemia and further fat catabolism
C. A urea cycle defect is most likely. Serum ammonia, pyruvate, amino acids, urine ketones and organic acids should be obtained. Aggressive treatment of hyperammonemia may be required.
D. A mitochondrial disorder is most likely. Pending defi nitive diagnosis, the prevention of catabolism, supportive care,
serial lab testing and the continuation of antibiotics are all warranted. A muscle biopsy can be delayed but Co-enzyme Q should be administered.
E. A mitochondrial disorder is most likely. Pending defi nitive diagnosis, the prevention of catabolism, supportive care, serial lab testing and the continuation of antibiotics are all warranted. A muscle biopsy should be obtained in the next 24 h.
Arad M, Maron BJ, Gorham JM, Johnson WH, Saul JP, Perez-Atayde AR. Glycogen storage diseases presenting as hypertrophic cardi-omyopathy. N Engl J Med. 2005;352:362–72.
Arid M, Benson DW, Perez-Atayde AR, et al. Constitutively active AMP kinase mutations cause glycogen storage disease mimick-ing hypertrophic cardiomyopathy. J Clin Invest. 2002;109:357–62.
Bachrach BE, Weinstein DA, Orho-Melander M, Burgess A, Wolfsdorf JI. Glycogen synthase defi ciency (Glycogen storage disease type 0) presenting with hyperglycemia and glucosuria: report of three new mutations. J Pediatr. 2002;140:781–3.
Beale EG, Hammer RE, Antoine B, Forest C. Glyceroneogenesis comes of age. FASEB J. 2002;16:1695–6.
Bodamer O. Organic acidemias. In: Rose BD, editor. UpToDate. Waltham: UpToDate; 2006.
Burton BK. Inborn errors of metabolism in infancy: a guide to diagno-sis. Pediatrics. 1998;102:1–9.
Chitkara DK, Nurko S, Shoffner JM, Buie T, Flores A. Abnormalities in gastrointestinal motility are associated with diseases of oxidative phosphorylation in children. Am J Gastroenterol. 2003;98:871–7.
Chuang DT. Maple syrup urine disease: it has come a long way. J Pediatr. 1998;132:S17–23.
Craigen WJ, Darras BT. Overview of disorders of glycogen metabo-lism. In: Rose BD, editor. UpToDate. Waltham: UpToDate; 2006.
Crone J, Möslinger D, Bodamer OA, et al. Reversibility of cirrhotic regenerative liver nodules upon NTBC treatment in a child with tyrosinemia type I. Acta Paediatr. 2003;92:625–8.
Foster JD, Nordlie RC. The biochemistry and molecular biology of the glucose-6-phosphat system. Exp Biol Med. 2002;227:601–8.
Freeze HH. Congenital disorders of glycosylation: CDG-I, CDG-II, and beyond. Curr Mol Med. 2007;7:389–96.
Garcia-Cazorla A, Rabier D, Touati G, et al. Pyrivate carboxylase defi -ciency: metabolic characteristics and new neurological aspects. Ann Neurol. 2006;59:121–7.
Gordon N. Classic diseases revisited: carbohydrate-defi cient glycopro-tein syndromes. Postgrad Med J. 2000;76:145–9.
Hartley LM, Khwaja OS, Verity CM. Glutaric aciduria type I and non-accidental head injury. Pediatrics. 2001;107:174–6.
Hoffman GF, Nyhan WL, Zschocke J, Kahler SG, Mayatepek E. Inhereted metabolic diseases. Philadelphia: Lippincott Williams and Wilkins; 2002.
Kelly A, Stanley CA. Disorders of glutamate metabolism. Ment Retard Dev Disabil Res Rev. 2001;7:287–95.
Mancuso M, Massimiliano F, Tsujino S, et al. Muscle glycogenosis and mitochondrial hepatopathy in an infant with mutations in both the myophosphorylase and deoxyguanosine kinase genes. Arch Neurol. 2003;60:1445–7.
Mochel F, DeLonlay P, Touati G, et al. Pyruvate carboxylase defi -ciency: clinical and biochemical response to anaplerotic diet therapy. Mol Genet Metab. 2005;84:305–12.
Morris AAM, Leonard JV. Early recognition of metabolic decompen-sation. Arch Dis Child. 1997;76:555–6.
Niezen-Koning KE, Wanders RJ, Ruiter JP, et al. Succinyl-CoA: ace-toacetate transferase defi ciency: identifi cation of a new patient with a neonatal onset and review of the literature. Eur J Pediatr. 1997;156:870–3.
Roe CR, Sweetman L, Roe DS, David F, Brunengraber H. Treatment of cardiomyopathy and rhabdomyolisis in long-chain fat oxida-tion disorders using an anaplerotic odd-chain triglyceride. J Clin Invest. 2002;110:259–69.
Rutledge SL, Atchison J, Boshard NU, Steinmann B. Case report: liver glycogen synthase defi ciency – a cause for ketotis hypoglycemia. Pediatrics. 2001;108:495–7.
SUGGESTED READINGS

895 C HAPTER 40 • M ETABOLIC C R IS ES
Saudubray JM, Specola JM, Middleton N, et al. Hyperketotic states due to inherited defects of ketolysis. Enzyme. 1987;38:80–90.
Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The metabolic and molecular bases of inherited disease. 8th ed. New York: McGraw Hill; 2001.
Strauss KA. Glutaric aciduria type I: a clinicians view of progress. Brain. 2005;128:697–9.
van den Berghe G. Disorders of gluconeogenesis. J Inherit Metab Dis. 1996;19:470–7.
Vockley J, Whiteman DAH. Defects of mitochondrial b -oxidation: a growing group of disorders. Neuromuscul Dis. 2002;12:235–46.
Winter SC, Buist NRM. Cardiomyopathy in childhood, mitochondrial dysfunction, and the role of L-carnitine. Am Heart J. 2000;139:S63–9.
Zeviani M, Di Donato S. Mitochondrial disorders. Brain. 2004;127:2153–72.
Zschocke J, Elfriede Q, Guldberg P, Hoffman GF. Mutation analysis in glutaric aciduria type I. J Med Genet. 2000;37:177–81.