Embed Size (px)
Citation preview
Pediatric Dose Selection for Monoclonal Antibodies: What Have We Learned?
Zhenhua (Michael) Xu, PhD, FCP Scientific Director/Janssen Fellow
Biologics Clinical Pharmacology, Biotechnology CoE Janssen Research & Development, LLC Jans
AAPS-NBC San Diego, May 21 2014
Outline
• Monoclonal antibodies (Fusion Proteins) with approved pediatric indications
• Comparisons of PK and doses for mAbs between adults and pediatrics
• Pediatric dose prediction and modeling & simulation • Technical considerations in using M&S for pediatric
dose selection • Pediatric dose-optimization strategy for mAbs
2
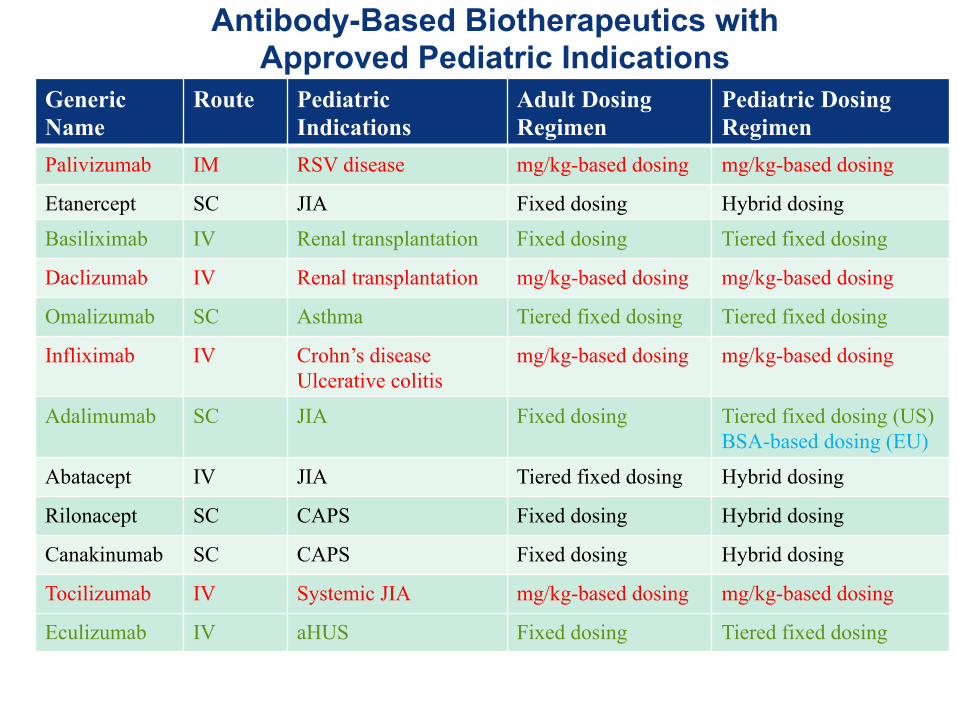
Antibody-Based Biotherapeutics with Approved Pediatric Indications
3
Generic Name
Route Pediatric Indications
Adult Dosing Regimen
Pediatric Dosing Regimen
Palivizumab IM RSV disease mg/kg-based dosing mg/kg-based dosing
Etanercept SC JIA Fixed dosing Hybrid dosing
Basiliximab IV Renal transplantation Fixed dosing Tiered fixed dosing
Daclizumab IV Renal transplantation mg/kg-based dosing mg/kg-based dosing
Omalizumab SC Asthma Tiered fixed dosing Tiered fixed dosing
Infliximab IV Crohn’s disease Ulcerative colitis
mg/kg-based dosing
mg/kg-based dosing
Adalimumab SC JIA Fixed dosing Tiered fixed dosing (US) BSA-based dosing (EU)
Abatacept IV JIA Tiered fixed dosing Hybrid dosing
Rilonacept SC CAPS Fixed dosing Hybrid dosing
Canakinumab SC CAPS Fixed dosing Hybrid dosing
Tocilizumab IV Systemic JIA mg/kg-based dosing mg/kg-based dosing
Eculizumab IV aHUS Fixed dosing Tiered fixed dosing
Janssen Research & Development
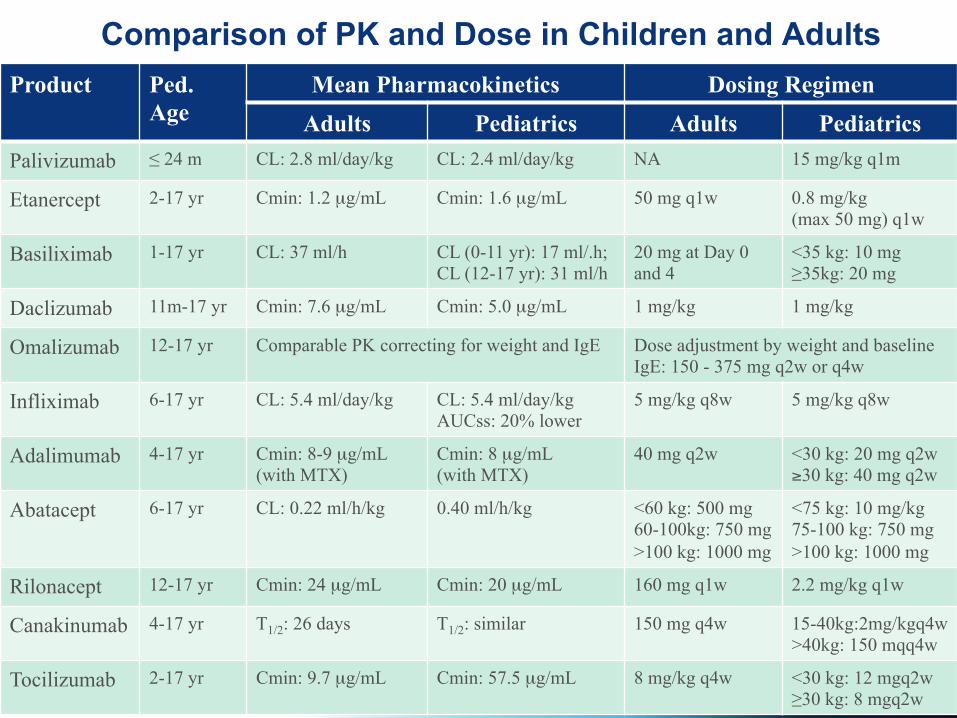
Comparison of PK and Dose in Children and Adults
4
Product Ped. Age
Mean Pharmacokinetics Dosing Regimen Adults Pediatrics Adults Pediatrics
Palivizumab ≤ 24 m CL: 2.8 ml/day/kg CL: 2.4 ml/day/kg NA 15 mg/kg q1m
Etanercept 2-17 yr Cmin: 1.2 µg/mL Cmin: 1.6 µg/mL 50 mg q1w 0.8 mg/kg (max 50 mg) q1w
Basiliximab 1-17 yr CL: 37 ml/h CL (0-11 yr): 17 ml/.h; CL (12-17 yr): 31 ml/h
20 mg at Day 0 and 4
<35 kg: 10 mg ≥35kg: 20 mg
Daclizumab 11m-17 yr Cmin: 7.6 µg/mL Cmin: 5.0 µg/mL 1 mg/kg 1 mg/kg
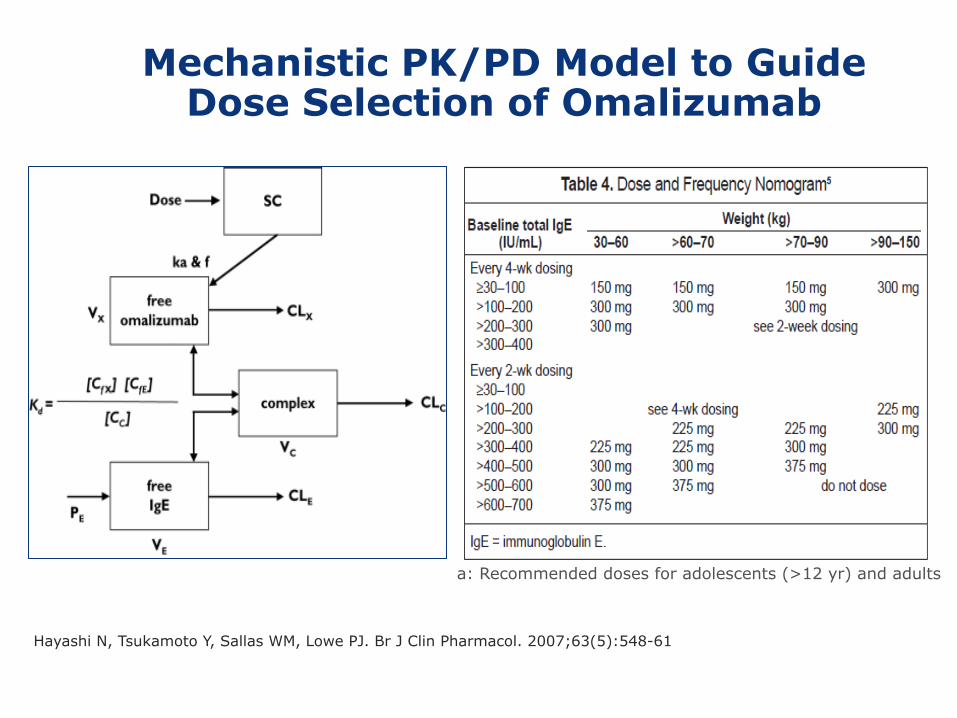
Omalizumab 12-17 yr Comparable PK correcting for weight and IgE Dose adjustment by weight and baseline IgE: 150 - 375 mg q2w or q4w
Infliximab 6-17 yr CL: 5.4 ml/day/kg CL: 5.4 ml/day/kg AUCss: 20% lower
5 mg/kg q8w 5 mg/kg q8w
Adalimumab 4-17 yr Cmin: 8-9 µg/mL (with MTX)
Cmin: 8 µg/mL (with MTX)
40 mg q2w <30 kg: 20 mg q2w ≥30 kg: 40 mg q2w
Abatacept 6-17 yr CL: 0.22 ml/h/kg 0.40 ml/h/kg <60 kg: 500 mg 60-100kg: 750 mg >100 kg: 1000 mg
<75 kg: 10 mg/kg 75-100 kg: 750 mg >100 kg: 1000 mg
Rilonacept 12-17 yr Cmin: 24 µg/mL Cmin: 20 µg/mL 160 mg q1w 2.2 mg/kg q1w
Canakinumab 4-17 yr T1/2: 26 days T1/2: similar 150 mg q4w 15-40kg:2mg/kgq4w >40kg: 150 mqq4w
Tocilizumab 2-17 yr Cmin: 9.7 µg/mL Cmin: 57.5 µg/mL 8 mg/kg q4w <30 kg: 12 mgq2w ≥30 kg: 8 mgq2w
Janssen Research & Development
Outline
• Monoclonal antibodies with approved pediatric indications
• Comparisons of PK and doses for mAbs between adults and pediatrics
• Pediatric dose prediction and modeling & simulation • Technical considerations in using M&S for pediatric
dose selection • Pediatric dose-optimization strategy for mAbs
5
Pediatric Dose Selection of mAbs: what we know?
6
• “What is the right dose in children?” is invariably a challenging question • It is equally important to leverage adult data and conduct appropriate pediatric
trials • Pediatric development of mAbs is still in its infancy. • Inconsistency in pediatric development of mAbs in Biotech/Pharm industry
Pediatric Dose
Selection
Leveraging Adult data
Extrapolation
Phase 1 PK
Phase 2 Dose-Finding
Phase 3 Efficacy/Safety
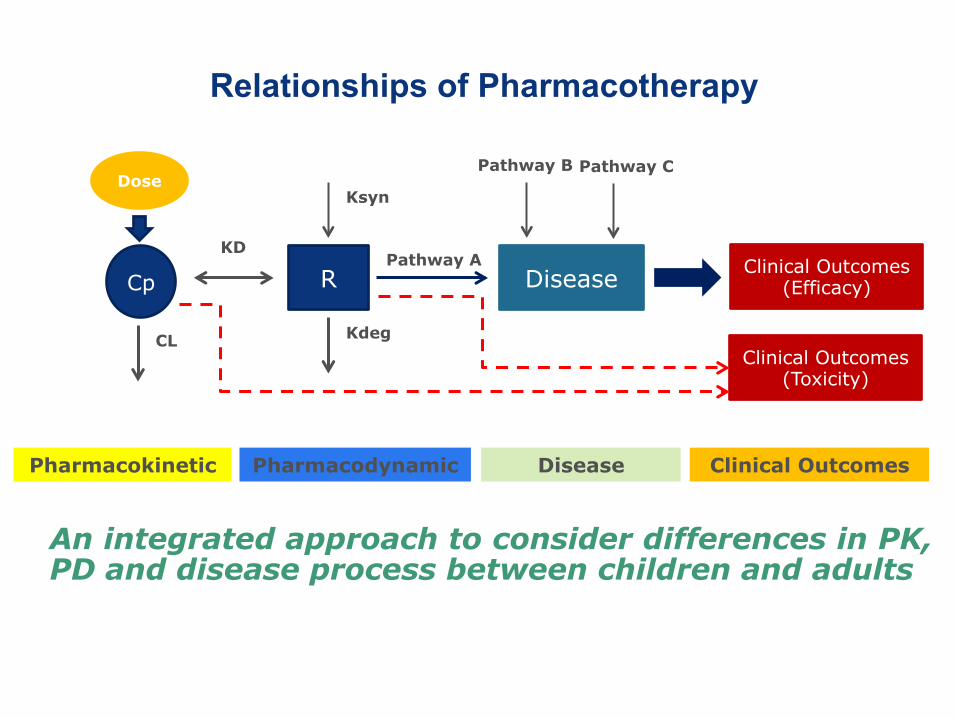
Pharmacokinetic-Pharmacodynamic-Disease Relationships of Pharmacotherapy
Cp R Disease Clinical Outcomes (Efficacy)
Ksyn
Kdeg CL
Pathway A
Pathway B Pathway C
Pharmacokinetic Pharmacodynamic Disease
Clinical Outcomes (Toxicity)
Clinical Outcomes
Dose
KD
An integrated approach to consider differences in PK, PD and disease process between children and adults
7
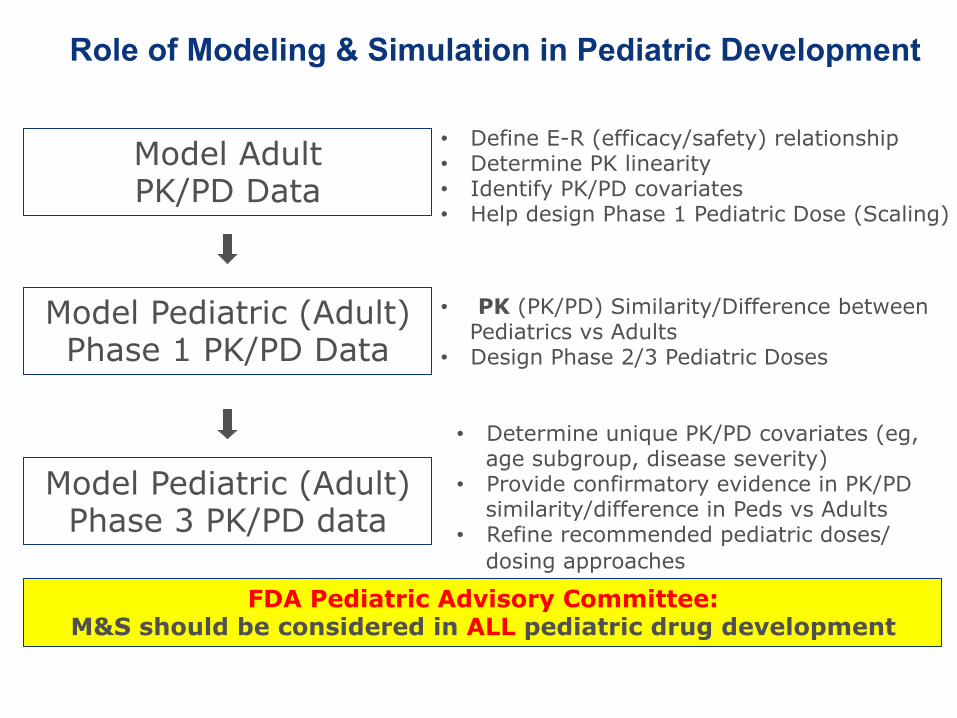
Role of Modeling & Simulation in Pediatric Development
8
FDA Pediatric Advisory Committee: M&S should be considered in ALL pediatric drug development
Model Adult PK/PD Data
Model Pediatric (Adult) Phase 1 PK/PD Data
Model Pediatric (Adult) Phase 3 PK/PD data
• Define E-R (efficacy/safety) relationship • Determine PK linearity • Identify PK/PD covariates • Help design Phase 1 Pediatric Dose (Scaling)
• PK (PK/PD) Similarity/Difference between Pediatrics vs Adults
• Design Phase 2/3 Pediatric Doses
• Determine unique PK/PD covariates (eg, age subgroup, disease severity)
• Provide confirmatory evidence in PK/PD similarity/difference in Peds vs Adults
• Refine recommended pediatric doses/dosing approaches
9
Hayashi N, Tsukamoto Y, Sallas WM, Lowe PJ. Br J Clin Pharmacol. 2007;63(5):548-61
Mechanistic PK/PD Model to Guide Dose Selection of Omalizumab
a: Recommended doses for adolescents (>12 yr) and adults
Pediatric Dose Selection Matching PK Exposure Between Ped vs Adults
Dose selection for pediatric patients based on prior PK information in adults is justified if the following requirements have been met:
1. The drug is to be used for the same indication in children and adults
2. The disease pathophysiology is similar in children and adults
3. The outcome of therapy (e.g., efficacy end point) is likely to be comparable in children and adults.
Abernethy DR and Burckart GJ (2010). Clin Pharm Ther 87:270-1. ICH E11 Clinical investigation of Medicinal Products in the Pediatric Population.
Assuming pathophysiology and pharmacodynamics in children are similar to adults
10
Covariates for mAb PK
• Body size (Weight, BSA)- a predominant determinant
• Targeted antigen levels (baseline IgE for omalizumab)
• Disease severity (C-reactive protein for golimumab)
• Concomitant medications (methotrexate on adalimumab)
• Anti-drug antibodies
• Albumin levels
11
After correcting for body-size effect, age has rarely been
identified as a significant covariate for the PK of mAbs; however,
there are limited data on the disposition of mAbs in very young
children such as neonates and infants (<2 yrs old)
Janssen Research & Development
Dosing Approaches for Correcting Body Size-Related PK Differences for mAbs
• BW-based dosing (on a mg/kg basis):
- mg dose of TP per kg of BW
- e.g., 5 mg/kg infliximab in pediatric UC or pediatric CD
• BSA-based dosing (on a mg/m2 basis):
- mg dose of TP per m2 of BSA
- e.g., 24 mg/m2 adalimumab in JIA (in EU only)
• Tiered fixed dosing:
- one fixed dose for patients in a specified BW range
- e.g., 10 mg basiliximab for BW<35 kg and 20 mg for ≥ 35 kg in pediatric subjects receiving renal transplantation
• Hybrid dosing:
- fixed dosing for older children and body size (BW or BSA)-based dosing for younger children
- e.g., 0.8 mg/kg (up to 50 mg if ≥ 63 kg) etanercept in JIA
12
Janssen Research & Development
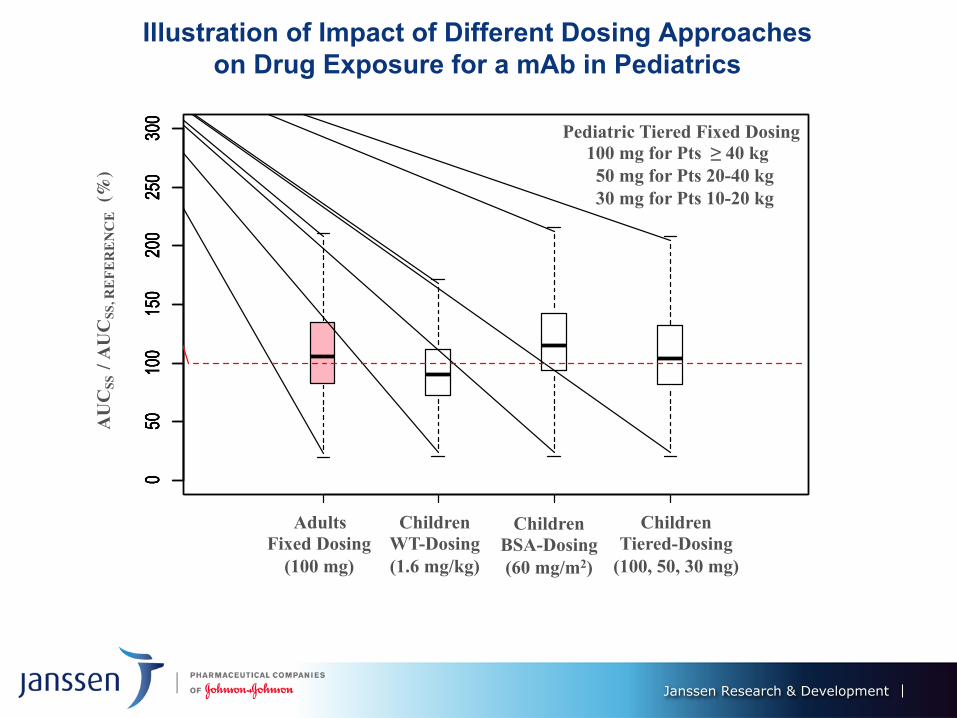
Illustration of Impact of Different Dosing Approaches on Drug Exposure for a mAb in Pediatrics
050
100
150
200
250
300
050
100
150
200
250
300
050
100
150
200
250
300
050
100
150
200
250
300
AU
CSS
/ A
UC
SS, R
EFE
RE
NC
E (
%)
Adults Fixed Dosing
(100 mg)
Children WT-Dosing (1.6 mg/kg)
Children BSA-Dosing (60 mg/m2)
Children Tiered-Dosing
(100, 50, 30 mg)
Pediatric Tiered Fixed Dosing 100 mg for Pts ≥ 40 kg 50 mg for Pts 20-40 kg 30 mg for Pts 10-20 kg
Janssen Research & Development
Outline
• Monoclonal antibodies with approved pediatric indications
• Comparisons of PK and doses for mAbs between adults and pediatrics
• Pediatric dose prediction and modeling & simulation • Technical considerations in using M&S for pediatric
dose selection • Pediatric dose-optimization strategy for mAbs
14
Janssen Research & Development
Technical Considerations in M&S for Designing Pediatric Doses of mAbs
• Data pooling for pediatric PK/PD modeling • Pediatric PK/PD model building steps
– Structural model: over-parameterization
– Covariate model: number of covariates – Use of allometry (exponent, TMDD)
• Simulation for matching drug exposure – Use of trial demographics vs growth chart – Limitation of body weight-based dosing
15
Janssen Research & Development
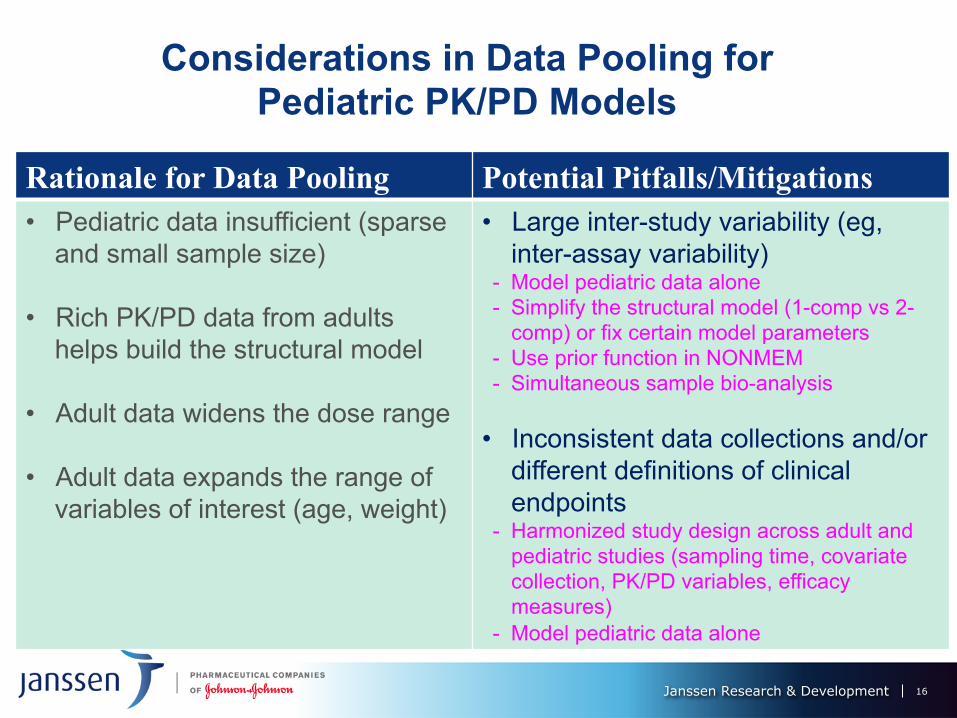
Considerations in Data Pooling for Pediatric PK/PD Models
16
Rationale for Data Pooling Potential Pitfalls/Mitigations • Pediatric data insufficient (sparse
and small sample size) • Rich PK/PD data from adults
helps build the structural model
• Adult data widens the dose range • Adult data expands the range of
variables of interest (age, weight)
• Large inter-study variability (eg, inter-assay variability)
- Model pediatric data alone - Simplify the structural model (1-comp vs 2-
comp) or fix certain model parameters - Use prior function in NONMEM - Simultaneous sample bio-analysis
• Inconsistent data collections and/or different definitions of clinical endpoints
- Harmonized study design across adult and pediatric studies (sampling time, covariate collection, PK/PD variables, efficacy measures)
- Model pediatric data alone
Janssen Research & Development
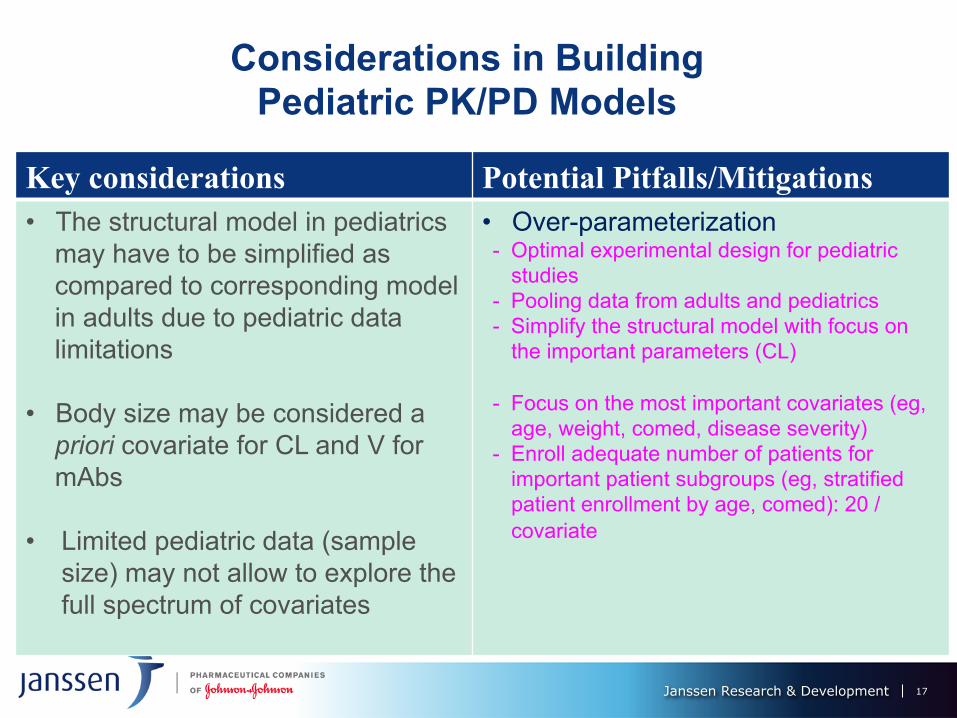
Considerations in Building Pediatric PK/PD Models
17
Key considerations Potential Pitfalls/Mitigations • The structural model in pediatrics
may have to be simplified as compared to corresponding model in adults due to pediatric data limitations
• Body size may be considered a priori covariate for CL and V for mAbs
• Limited pediatric data (sample
size) may not allow to explore the full spectrum of covariates
• Over-parameterization - Optimal experimental design for pediatric
studies - Pooling data from adults and pediatrics - Simplify the structural model with focus on
the important parameters (CL) - Focus on the most important covariates (eg,
age, weight, comed, disease severity) - Enroll adequate number of patients for
important patient subgroups (eg, stratified patient enrollment by age, comed): 20 / covariate
Anderson and Holford NHG (2008). Annu. Rev. Pharmacol. Toxicol. 48:303–32.
Most body size relations take the form
Y = a * BW b
Mathematics is all around us in the natural world
18
Considerations in Using Allometric Scaling in Pediatric Modeling Analysis for mAbs
Janssen Research & Development
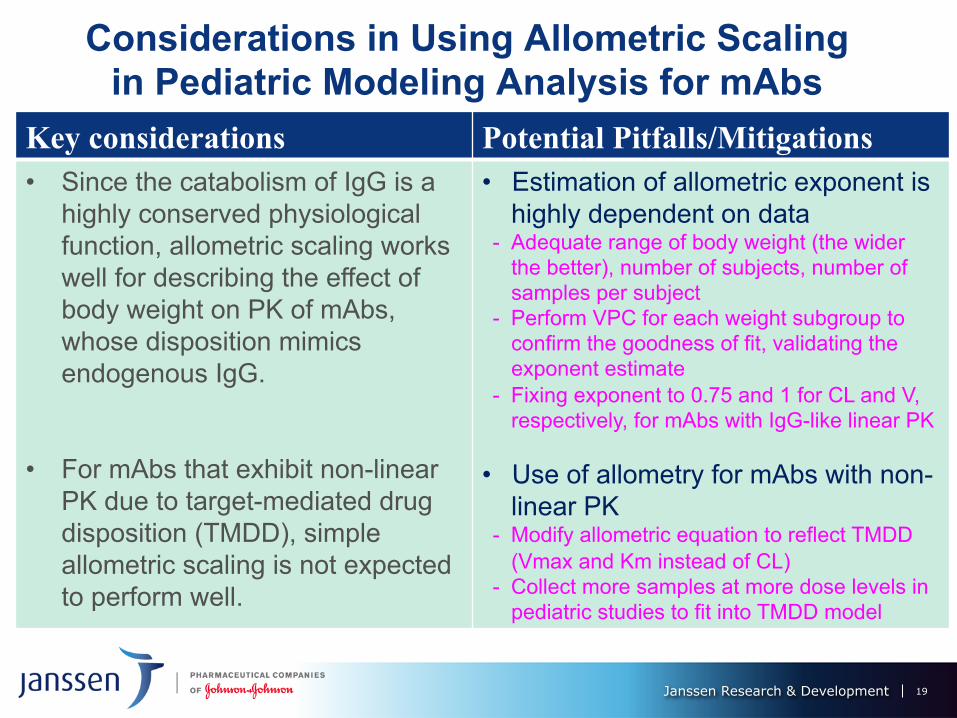
Considerations in Using Allometric Scaling in Pediatric Modeling Analysis for mAbs
19
Key considerations Potential Pitfalls/Mitigations • Since the catabolism of IgG is a
highly conserved physiological function, allometric scaling works well for describing the effect of body weight on PK of mAbs, whose disposition mimics endogenous IgG.
• For mAbs that exhibit non-linear
PK due to target-mediated drug disposition (TMDD), simple allometric scaling is not expected to perform well.
• Estimation of allometric exponent is highly dependent on data
- Adequate range of body weight (the wider the better), number of subjects, number of samples per subject
- Perform VPC for each weight subgroup to confirm the goodness of fit, validating the exponent estimate
- Fixing exponent to 0.75 and 1 for CL and V, respectively, for mAbs with IgG-like linear PK
• Use of allometry for mAbs with non-
linear PK - Modify allometric equation to reflect TMDD
(Vmax and Km instead of CL) - Collect more samples at more dose levels in
pediatric studies to fit into TMDD model
Janssen Research & Development
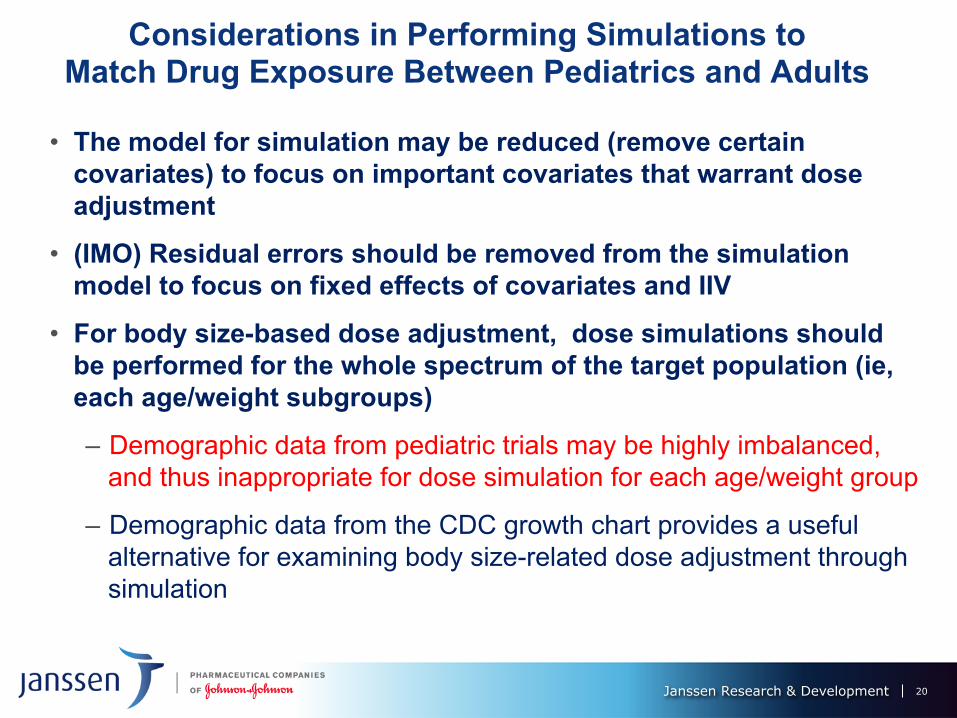
Considerations in Performing Simulations to Match Drug Exposure Between Pediatrics and Adults
• The model for simulation may be reduced (remove certain covariates) to focus on important covariates that warrant dose adjustment
• (IMO) Residual errors should be removed from the simulation model to focus on fixed effects of covariates and IIV
• For body size-based dose adjustment, dose simulations should be performed for the whole spectrum of the target population (ie, each age/weight subgroups)
– Demographic data from pediatric trials may be highly imbalanced, and thus inappropriate for dose simulation for each age/weight group
– Demographic data from the CDC growth chart provides a useful alternative for examining body size-related dose adjustment through simulation
20
Janssen Research & Development
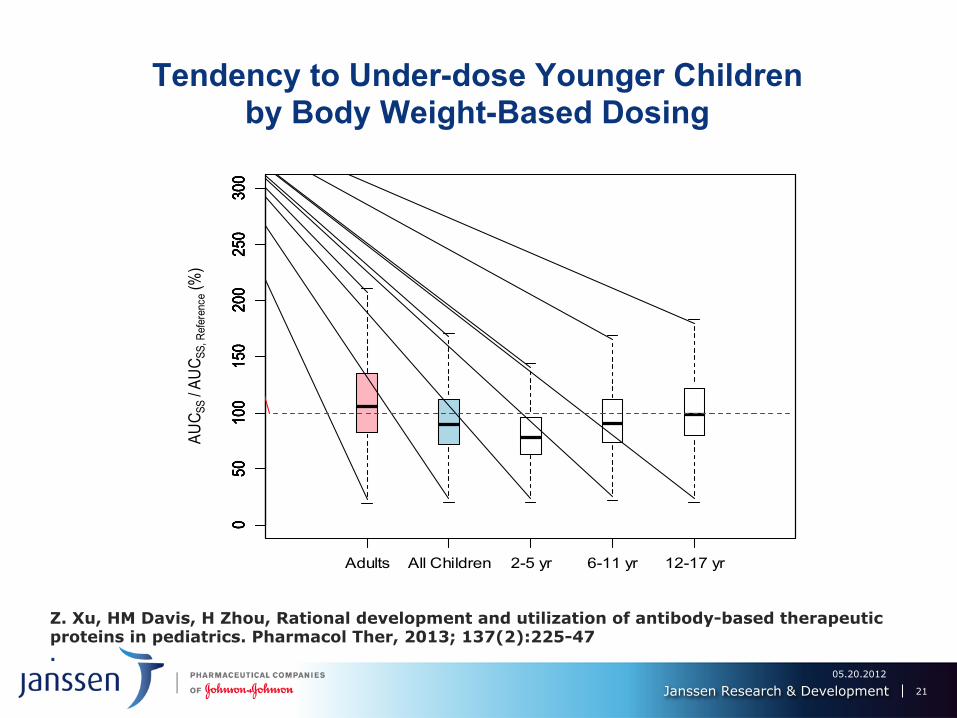
Tendency to Under-dose Younger Children by Body Weight-Based Dosing
Z. Xu, HM Davis, H Zhou, Rational development and utilization of antibody-based therapeutic proteins in pediatrics. Pharmacol Ther, 2013; 137(2):225-47 .
05.20.2012
21
050
100
150
200
250
300
AUC S
S / A
UCSS
, Ref
eren
ce (%
)
050
100
150
200
250
300
050
100
150
200
250
300
050
100
150
200
250
300
050
100
150
200
250
300
Adults All Children 2-5 yr 6-11 yr 12-17 yr
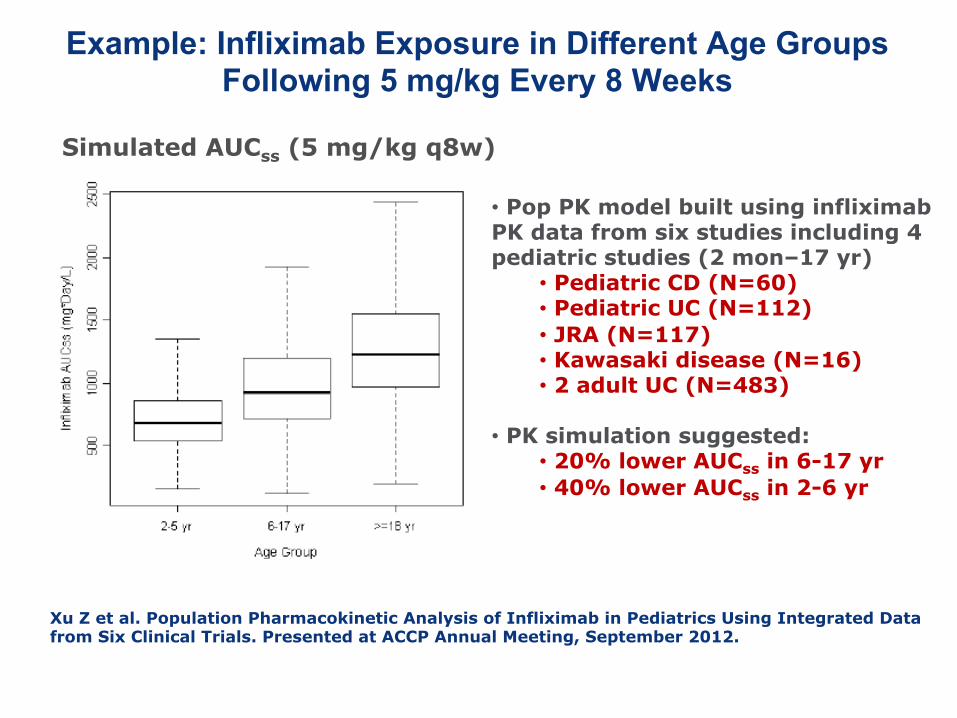
Example: Infliximab Exposure in Different Age Groups Following 5 mg/kg Every 8 Weeks
Simulated AUCss (5 mg/kg q8w)
• Pop PK model built using infliximab PK data from six studies including 4 pediatric studies (2 mon–17 yr)
• Pediatric CD (N=60) • Pediatric UC (N=112) • JRA (N=117) • Kawasaki disease (N=16) • 2 adult UC (N=483)
• PK simulation suggested: • 20% lower AUCss in 6-17 yr • 40% lower AUCss in 2-6 yr
Xu Z et al. Population Pharmacokinetic Analysis of Infliximab in Pediatrics Using Integrated Data from Six Clinical Trials. Presented at ACCP Annual Meeting, September 2012.
05.20.2012
22
Janssen Research & Development
Outline
• Monoclonal antibodies with approved pediatric indications
• Comparisons of PK and doses for mAbs between adults and pediatrics
• Pediatric dose prediction and modeling & simulation • Pitfalls in using M&S for pediatric dose selection • Pediatric dose-optimization strategy for mAbs
23
24
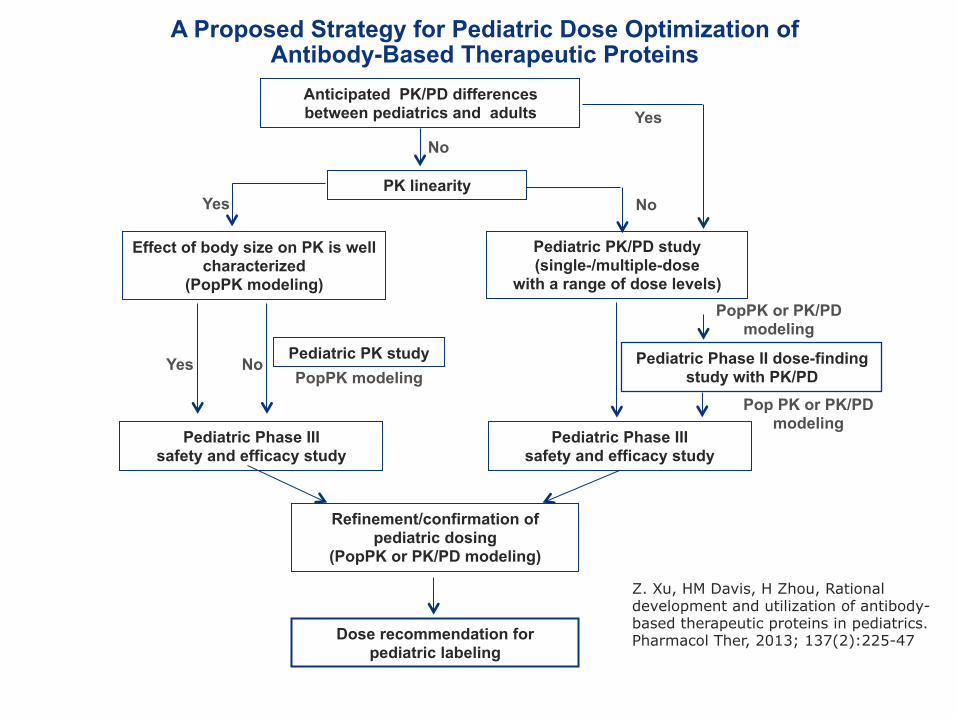
A Proposed Strategy for Pediatric Dose Optimization of Antibody-Based Therapeutic Proteins
Effect of body size on PK is well characterized
(PopPK modeling)
Pediatric PK study
Pediatric Phase III safety and efficacy study
Yes
Refinement/confirmation of pediatric dosing
(PopPK or PK/PD modeling)
No
Dose recommendation for pediatric labeling
Pediatric PK/PD study (single-/multiple-dose
with a range of dose levels)
Pediatric Phase II dose-finding study with PK/PD
Yes No
Pediatric Phase III safety and efficacy study
PopPK modeling
PopPK or PK/PD modeling
Pop PK or PK/PD modeling
PK linearity
Anticipated PK/PD differences between pediatrics and adults
No
Yes
Z. Xu, HM Davis, H Zhou, Rational development and utilization of antibody-based therapeutic proteins in pediatrics. Pharmacol Ther, 2013; 137(2):225-47
Janssen Research & Development
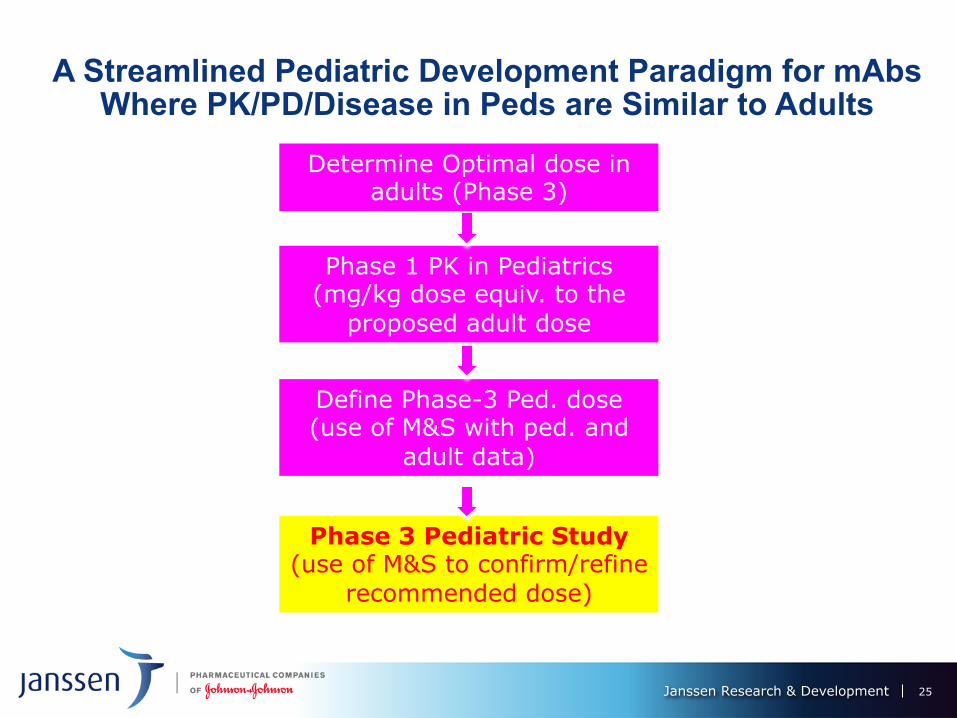
A Streamlined Pediatric Development Paradigm for mAbs Where PK/PD/Disease in Peds are Similar to Adults
25
Determine Optimal dose in adults (Phase 3)
Phase 1 PK in Pediatrics (mg/kg dose equiv. to the
proposed adult dose
Define Phase-3 Ped. dose (use of M&S with ped. and
adult data)
Phase 3 Pediatric Study (use of M&S to confirm/refine
recommended dose)
Janssen Research & Development
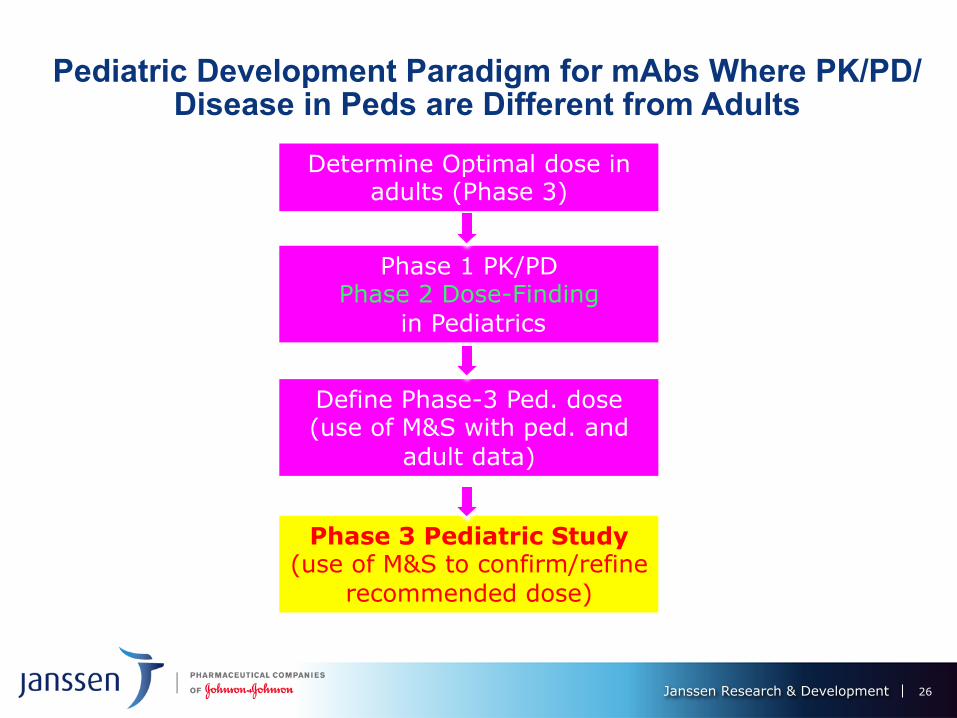
Pediatric Development Paradigm for mAbs Where PK/PD/Disease in Peds are Different from Adults
26
Determine Optimal dose in adults (Phase 3)
Phase 1 PK/PD Phase 2 Dose-Finding
in Pediatrics
Define Phase-3 Ped. dose (use of M&S with ped. and
adult data)
Phase 3 Pediatric Study (use of M&S to confirm/refine
recommended dose)
q Joseph Adedokun q Craig Comisar q Lanyi Xie q Jocelyn Leu q Yanli Zhuang q Honghui Zhou q Hugh Davis
Acknowledgement
27
Questions?
28 Biotech CoE Spring House Summit
Reference: Zhenhua Xu, Hugh Davis, Honghui Zhou, Rational Development and Utilization of Antibody-Based Therapeutic Proteins in Pediatrics, Pharmacology & Therapeutics, 2013; 137(2):225-247





























