Embed Size (px)
Citation preview
CMECME
A review of proper screening, diagnosis, evaluation, and treatment
CMECME
Pediatric Hypertension
CMECME
EDUCATIONAL OBJECTIVES
• Identify children and adolescents for whom
hypertension screening is appropriate
• Implement an initial workup for pediatric
hypertension
• Develop treatment plans for children with
essential or secondary hypertension
Nicholas, a 10-year-old boy with a history of
intermit tent asthma and at tention def icit
hyperactivity disorder, is seeing you for the first
time for a well child visit. He has no complaints and
his mom has no specific questions or concerns. On
review of symptoms, Nicholas reports that he has some
chest pain when he has an asthma exacerbation. Current
medications include methylphenidate once daily and an
albuterol metered-dose inhaler as needed. His family history
reveals hypertension (HTN) in his father and paternal
grandfather, and diabetes mellitus in his paternal grandfather.
His mother and 12-year-old sister are healthy with no chronic
medical problems. On physical exam, his anthropometrics
and vital signs are as follows:
Height: 140 cm (50%)
Weight: 45 kg (95%)
Body mass index (BMI): 23 (>95%)
Temperature 37 °C
Heart rate: 85 bpm
Blood pressure (BP): 124/82 mm Hg by automated cuff
Physical exam is normal
46 www.contemporarypediatrics.com Vol. 25, No. 11
cntped1108_046.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan

TAMMY BRADY, MD, GEORGE K. SIBERRY, MD, MPH, AND BARRY SOLOMON, MD, MPH
You reference the BP tables published in the Fourth
Report by the National High Blood Pressure Education
Program Working Group on High Blood Pressure in Children
and Adolescents,1 and discover that the BP norms for
a child of this age, gender, and height percentile are as
follows:
50%: 102/61
90%: 116/76
95%: 120/80
99%: 127/88
This clinical scenario of a child found to have an
elevated initial blood pressure is not uncommon. Pediatric
hypertension, previously reported to affect only 0.3% to
1.2% of children in the 1970s and 1980s,2,3 now affects
up to 5% of all children.4 One possible explanation for
this increase may be the current growing population
of obese children.5 The prevalence of hypertension in
children increases with increasing BMI percentile,4 placing
obese children at three-times higher risk of becoming
hypertensive when compared to non-obese children.5
Regardless of the cause for this increase, a child with
hypertension can be a dilemma for many primary care
providers. It is essential for providers to understand when
to screen for hypertension, how to conduct an initial
work-up, how to manage these patients, and when to
refer them to a subspecialist.
Which children should get their blood pressure checked?
Current recommendations state that all children 3 years of
age and older should have their blood pressure measured
at all health care encounters, including both well child
care and acute care or sick visits. Certain children younger
than 3 with comorbid conditions should also have their BP
measured at each visit. This population includes children
under 3 with1:
History of prematurity
History of low birth weight or neonatal intensive
care unit (NICU) stay
Presence of congenital heart disease, kidney disease,
or genitourinary abnormality
Family history of congenital kidney disease
Recurrent urinary tract infection (UTI), hematuria,
proteinuria
Transplant of solid organ or bone marrow
Malignancy
Taking medications known to increase blood
pressure (steroids, decongestants, nonsteroidal
anti-inflammatory drugs [NSAIDs], beta-adrenergic
agonists)
Presence of systemic illness associated with hypertension
(neurofibromatosis, tuberous sclerosis)
Evidence of increased intracranial pressure
•
•
•
•
•
•
•
•
•
•
DisclosuresEditors Toby Hindin, Jeannette Mallozzi, Jeff Ryan, and John Merriman disclose that they do not have any financial relationships with any manufacturer in this area of medicine.
Manuscript reviewers disclose that they do not have any financial relationships with any manufacturer in this area of medicine.
DR. BRADY is an assistant professor of pediatric nephrology at Johns Hopkins University School of Medicine.
DR. SIBERRY is an assistant professor of pediatrics in the divisions of general pediatric and adolescent medicine and pediatric infectious diseases at Johns Hopkins Hospital.
DR. SOLOMON is an assistant professor of pediatrics in the division of general pediatrics and adolescent medicine at Johns Hopkins Hospital, and medical director of the Harriet Lane Clinic at the Johns Hopkins School of Medicine.
Accreditation
cme2 is accredited by the ACCME to provide continuing medical education for physicians.
Credit Designation
cme2 designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Target audience: Pediatricians and primary care physicians
To earn CME credit for this activityParticipants should study the article and log on to www.contemporarypediatrics.com, and click on the “Earn CME Credit” button on the left-hand side. Participants must pass a post-test and complete an online evaluation of the CME activity. After passing the post-test and completing the online evaluation, a CME certificate will be e-mailed to them. The release date for this activity is November 1, 2008. The expiration date is November 1, 2009.
The authors have nothing to disclose with regard to affiliations with, or financial interest in, any organization that may have an interest in any part of this article.
Resolution of conflict of interest
cme2 has implemented a process to resolve conflicts of interest for each continuing medical education activity, to help ensure content validity, independence, fair balance, and that the content is aligned with the interest of the public. Conflicts, if any, are resolved through a peer review process.
Unapproved/off-label use discussion
Faculty may discuss information about pharmaceutical agents, devices, or diagnostic products that are outside of FDA-approved labeling. This information is intended solely for CME and is not intended to promote off-label use of these medications. If you have questions, contact the medical affairs department of the manufacturer for the most recent prescribing information. Faculty are required to disclose any off-label discussion.
HYPERTENSIONIL
LU
ST
RA
TIO
N:J
OE
L A
ND
SH
AR
ON
HA
RR
IS/A
RT
ICU
LA
TE
GR
AP
HIC
S:
>>p.48
NOVEMBER 2008 CONTEMPORARY PEDIATRICS 47
cntped1108_047.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan
CMECME
How should blood pressure be measured in children?The proper technique for BP measurement via manual
auscultation is as follows1:
1. Ensure that the child has been resting for a minimum
of five minutes prior to measurement. The child should
be sitting with back supported, both feet on the floor and
right cubital fossa supported at heart level.
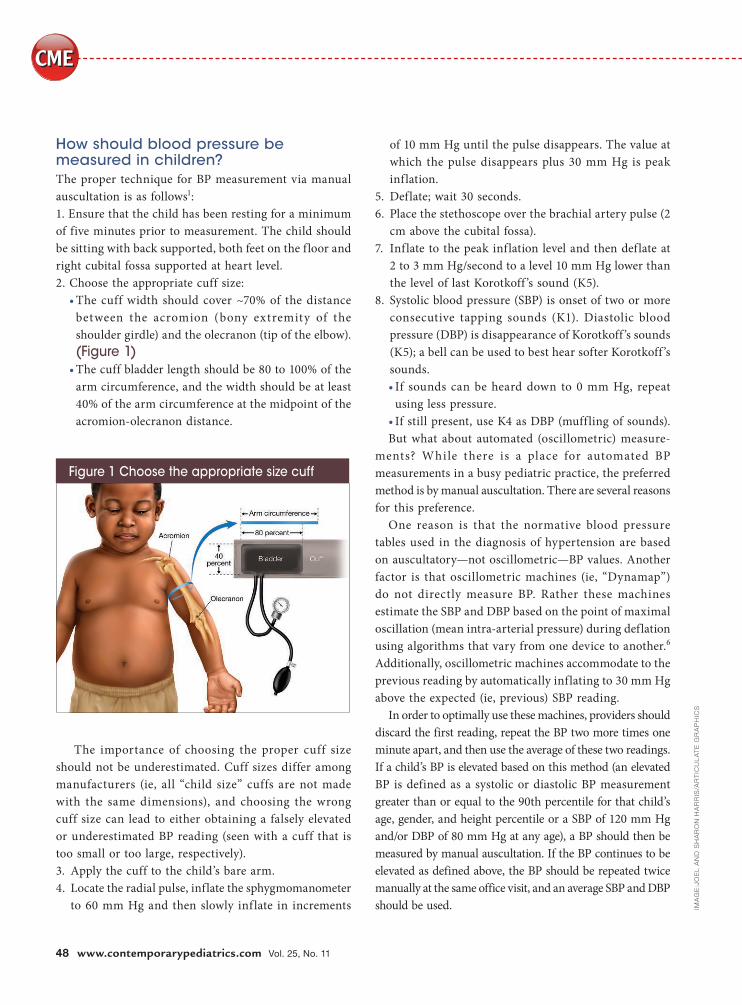
2. Choose the appropriate cuff size:
The cuff width should cover ~70% of the distance
between the acromion (bony extremity of the
shoulder girdle) and the olecranon (tip of the elbow).
(Figure 1)The cuff bladder length should be 80 to 100% of the
arm circumference, and the width should be at least
40% of the arm circumference at the midpoint of the
acromion-olecranon distance.
The importance of choosing the proper cuff size
should not be underestimated. Cuff sizes differ among
manufacturers (ie, all “child size” cuffs are not made
with the same dimensions), and choosing the wrong
cuff size can lead to either obtaining a falsely elevated
or underestimated BP reading (seen with a cuff that is
too small or too large, respectively).
3. Apply the cuff to the child’s bare arm.
4. Locate the radial pulse, inflate the sphygmomanometer
to 60 mm Hg and then slowly inf late in increments
•
•
of 10 mm Hg until the pulse disappears. The value at
which the pulse disappears plus 30 mm Hg is peak
inflation.
5. Deflate; wait 30 seconds.
6. Place the stethoscope over the brachial artery pulse (2
cm above the cubital fossa).
7. Inflate to the peak inflation level and then deflate at
2 to 3 mm Hg/second to a level 10 mm Hg lower than
the level of last Korotkoff ’s sound (K5).
8. Systolic blood pressure (SBP) is onset of two or more
consecutive tapping sounds (K1). Diastolic blood
pressure (DBP) is disappearance of Korotkoff ’s sounds
(K5); a bell can be used to best hear softer Korotkoff ’s
sounds.
If sounds can be heard down to 0 mm Hg, repeat
using less pressure.
If still present, use K4 as DBP (muffling of sounds).
But what about automated (oscillometric) measure-
ments? While there is a place for automated BP
measurements in a busy pediatric practice, the preferred
method is by manual auscultation. There are several reasons
for this preference.
One reason is that the normative blood pressure
tables used in the diagnosis of hypertension are based
on auscultatory—not oscillometric—BP values. Another
factor is that oscillometric machines (ie, “Dynamap”)
do not directly measure BP. Rather these machines
estimate the SBP and DBP based on the point of maximal
oscillation (mean intra-arterial pressure) during deflation
using algorithms that vary from one device to another.6
Additionally, oscillometric machines accommodate to the
previous reading by automatically inflating to 30 mm Hg
above the expected (ie, previous) SBP reading.
In order to optimally use these machines, providers should
discard the first reading, repeat the BP two more times one
minute apart, and then use the average of these two readings.
If a child’s BP is elevated based on this method (an elevated
BP is defined as a systolic or diastolic BP measurement
greater than or equal to the 90th percentile for that child’s
age, gender, and height percentile or a SBP of 120 mm Hg
and/or DBP of 80 mm Hg at any age), a BP should then be
measured by manual auscultation. If the BP continues to be
elevated as defined above, the BP should be repeated twice
manually at the same office visit, and an average SBP and DBP
should be used.
•
•
IMA
GE
:JO
EL
AN
D S
HA
RO
N H
AR
RIS
/AR
TIC
UL
AT
E G
RA
PH
ICS
Figure 1 Choose the appropriate size cuff
48 www.contemporarypediatrics.com Vol. 25, No. 11
cntped1108_048.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan
HYPERTENSION
Because of the inherent limitations to automated BP
readings, public blood pressure machines should be used
with caution when including them in your evaluation and
/or management of pediatric hypertension. Automated cuffs
need to be calibrated at regular intervals, and there is often
no readily available record of scheduled maintenance of
these public machines. Also, there is often only one cuff
size available, leading to false BP readings as described
above.7,8
Back to your patient
You repeat Nicholas’ BP by manual auscultation and obtain
a reading of 126/84 mm Hg; one minute later it’s 116/84 mm
Hg, giving him an average BP of 121/84. Again, referencing
the Fourth Report BP tables, you discover that Nicholas’
manual BP is between 120/80 and 132/93 (the 95th percentile
and 99th percentile plus 5 mm Hg for his age, gender and
height percentile). As he is asymptomatic (no complaints
of nausea, vomiting, epistaxis, blurry vision, or diplopia),
you have him come back weekly on two more occasions.
Manual BPs at these visits confirm he has sustained BPs
greater than or equal to the 95th percentile, and less than
the 99th percentile plus 5 mm Hg. You diagnose him with
Stage 1 Hypertension and initiate a work-up as outlined
by the Fourth Report*:
SBP or DBP percentile
When to recheck blood pressure?
Normal <90th Next health care visit
Prehypertension 90th to <95th
or
= 120/80 and
<90th percentile
Six months
Stage 1
hypertension
95th to
[99th + 5 mm Hg]
One to two weeks or
sooner if symptomatic;
if it continues to be
elevated on two or more
occasions, refer within
one month
Stage 2
hypertension
>99th + 5 mm Hg Evaluate or refer within
one week, or immediately
if symptomatic
*Adapted from the Fourth Report1
Initial work-up for pediatric hypertensionA diagnostic work-up should be conducted to rule out
secondary causes of hypertension for any child with a
confirmed diagnosis of prehypertension with comorbid
conditions (ie, African-American race, obesity, kidney
disease, insulin resistance or diabetes mellitus, history
of umbilical lines or recurrent urinary tract infections,
family history of HTN).
While primary (or “essential”) HTN is on the rise
in children, it should still be considered a diagnosis of
exclusion. Secondary hypertension is more common in
children than in adults, and is more likely the younger the
child and the higher the blood pressure at presentation.1,11
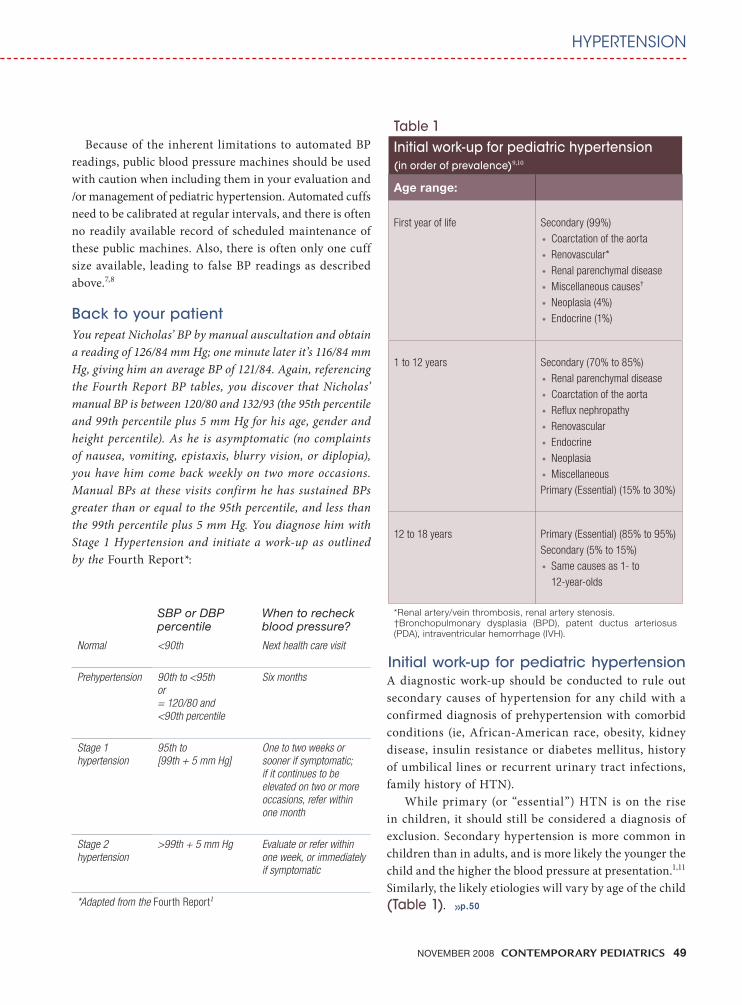
Similarly, the likely etiologies will vary by age of the child
(Table 1).
Table 1
Initial work-up for pediatric hypertension(in order of prevalence)9,10
Age range:
First year of life Secondary (99%)
Coarctation of the aorta
Renovascular*
Renal parenchymal disease
Miscellaneous causes†
Neoplasia (4%)
Endocrine (1%)
•
•
•
•
•
•
1 to 12 years Secondary (70% to 85%)
Renal parenchymal disease
Coarctation of the aorta
Reflux nephropathy
Renovascular
Endocrine
Neoplasia
Miscellaneous
Primary (Essential) (15% to 30%)
•
•
•
•
•
•
•
12 to 18 years Primary (Essential) (85% to 95%)
Secondary (5% to 15%)
Same causes as 1- to
12-year-olds
•
*Renal artery/vein thrombosis, renal artery stenosis.†Bronchopulmonary dysplasia (BPD), patent ductus arteriosus (PDA), intraventricular hemorrhage (IVH).
>>p.50
NOVEMBER 2008 CONTEMPORARY PEDIATRICS 49
cntped1108_049.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan
CMECME
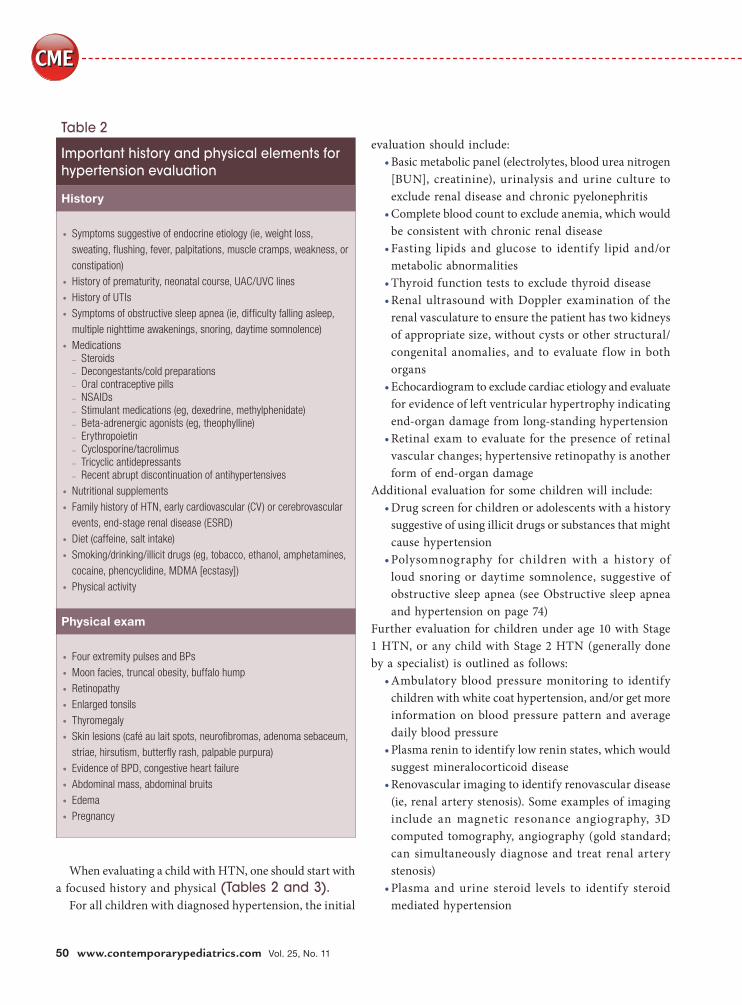
When evaluating a child with HTN, one should start with
a focused history and physical (Tables 2 and 3). For all children with diagnosed hypertension, the initial
evaluation should include:
Basic metabolic panel (electrolytes, blood urea nitrogen
[BUN], creatinine), urinalysis and urine culture to
exclude renal disease and chronic pyelonephritis
Complete blood count to exclude anemia, which would
be consistent with chronic renal disease
Fasting lipids and glucose to identify lipid and/or
metabolic abnormalities
Thyroid function tests to exclude thyroid disease
Renal ultrasound with Doppler examination of the
renal vasculature to ensure the patient has two kidneys
of appropriate size, without cysts or other structural/
congenital anomalies, and to evaluate f low in both
organs
Echocardiogram to exclude cardiac etiology and evaluate
for evidence of left ventricular hypertrophy indicating
end-organ damage from long-standing hypertension
Retinal exam to evaluate for the presence of retinal
vascular changes; hypertensive retinopathy is another
form of end-organ damage
Additional evaluation for some children will include:
Drug screen for children or adolescents with a history
suggestive of using illicit drugs or substances that might
cause hypertension
Polysomnography for children with a history of
loud snoring or daytime somnolence, suggestive of
obstructive sleep apnea (see Obstructive sleep apnea
and hypertension on page 74)
Further evaluation for children under age 10 with Stage
1 HTN, or any child with Stage 2 HTN (generally done
by a specialist) is outlined as follows:
Ambulatory blood pressure monitoring to identify
children with white coat hypertension, and/or get more
information on blood pressure pattern and average
daily blood pressure
Plasma renin to identify low renin states, which would
suggest mineralocorticoid disease
Renovascular imaging to identify renovascular disease
(ie, renal artery stenosis). Some examples of imaging
include an magnetic resonance angiography, 3D
computed tomography, angiography (gold standard;
can simultaneously diagnose and treat renal artery
stenosis)
Plasma and urine steroid levels to identify steroid
mediated hypertension
•
•
•
•
•
•
•
•
•
•
•
•
•
Table 2
Important history and physical elements for hypertension evaluation
History
Symptoms suggestive of endocrine etiology (ie, weight loss,
sweating, flushing, fever, palpitations, muscle cramps, weakness, or
constipation)
History of prematurity, neonatal course, UAC/UVC lines
History of UTIs
Symptoms of obstructive sleep apnea (ie, difficulty falling asleep,
multiple nighttime awakenings, snoring, daytime somnolence)
MedicationsSteroidsDecongestants/cold preparations Oral contraceptive pillsNSAIDsStimulant medications (eg, dexedrine, methylphenidate)Beta-adrenergic agonists (eg, theophylline)ErythropoietinCyclosporine/tacrolimusTricyclic antidepressantsRecent abrupt discontinuation of antihypertensives
Nutritional supplements
Family history of HTN, early cardiovascular (CV) or cerebrovascular
events, end-stage renal disease (ESRD)
Diet (caffeine, salt intake)
Smoking/drinking/illicit drugs (eg, tobacco, ethanol, amphetamines,
cocaine, phencyclidine, MDMA [ecstasy])
Physical activity
•
•
•
•
•
–
–
–
–
–
–
–
–
–
–
•
•
•
•
•
Physical exam
Four extremity pulses and BPs
Moon facies, truncal obesity, buffalo hump
Retinopathy
Enlarged tonsils
Thyromegaly
Skin lesions (café au lait spots, neurofibromas, adenoma sebaceum,
striae, hirsutism, butterfly rash, palpable purpura)
Evidence of BPD, congestive heart failure
Abdominal mass, abdominal bruits
Edema
Pregnancy
•
•
•
•
•
•
•
•
•
•
50 www.contemporarypediatrics.com Vol. 25, No. 11
cntped1108_050.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan
HYPERTENSION
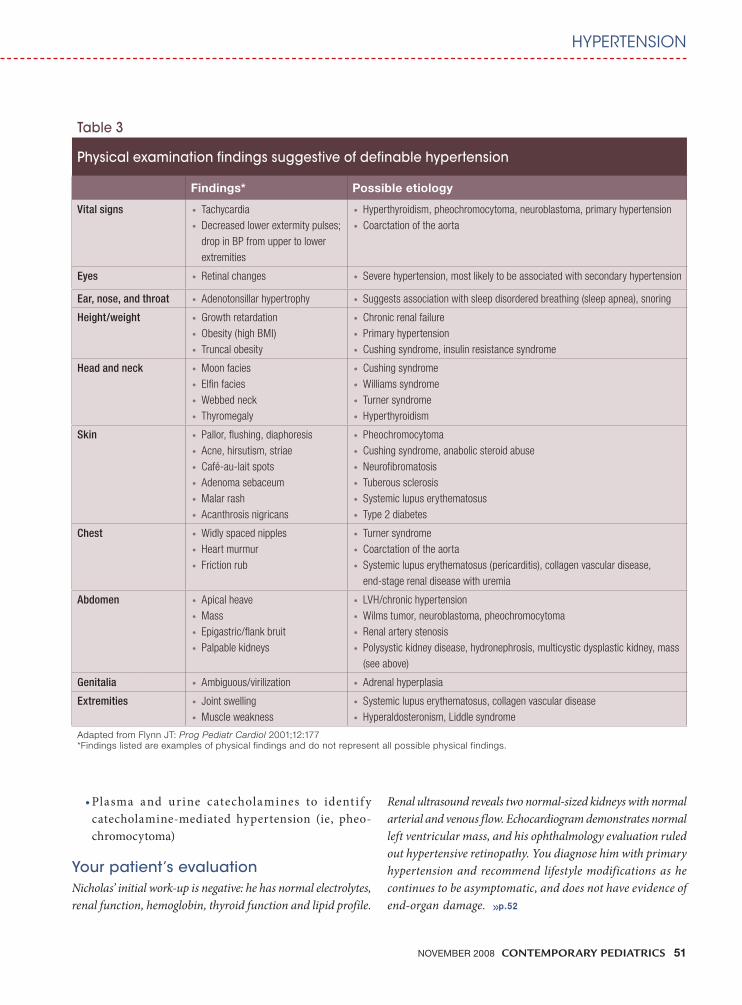
Plasma and urine catecholamines to ident i f y
catecholamine-mediated hypertension (ie, pheo-
chromocytoma)
Your patient’s evaluation
Nicholas’ initial work-up is negative: he has normal electrolytes,
renal function, hemoglobin, thyroid function and lipid profile.
• Renal ultrasound reveals two normal-sized kidneys with normal
arterial and venous flow. Echocardiogram demonstrates normal
left ventricular mass, and his ophthalmology evaluation ruled
out hypertensive retinopathy. You diagnose him with primary
hypertension and recommend lifestyle modifications as he
continues to be asymptomatic, and does not have evidence of
end-organ damage.
Table 3
Physical examination findings suggestive of definable hypertension
Findings* Possible etiology
Vital signs Tachycardia
Decreased lower extermity pulses;
drop in BP from upper to lower
extremities
•
•
Hyperthyroidism, pheochromocytoma, neuroblastoma, primary hypertension
Coarctation of the aorta
•
•
Eyes Retinal changes• Severe hypertension, most likely to be associated with secondary hypertension•
Ear, nose, and throat Adenotonsillar hypertrophy• Suggests association with sleep disordered breathing (sleep apnea), snoring•
Height/weight Growth retardation
Obesity (high BMI)
Truncal obesity
•
•
•
Chronic renal failure
Primary hypertension
Cushing syndrome, insulin resistance syndrome
•
•
•
Head and neck Moon facies
Elfin facies
Webbed neck
Thyromegaly
•
•
•
•
Cushing syndrome
Williams syndrome
Turner syndrome
Hyperthyroidism
•
•
•
•
Skin Pallor, flushing, diaphoresis
Acne, hirsutism, striae
Café-au-lait spots
Adenoma sebaceum
Malar rash
Acanthrosis nigricans
•
•
•
•
•
•
Pheochromocytoma
Cushing syndrome, anabolic steroid abuse
Neurofibromatosis
Tuberous sclerosis
Systemic lupus erythematosus
Type 2 diabetes
•
•
•
•
•
•
Chest Widly spaced nipples
Heart murmur
Friction rub
•
•
•
Turner syndrome
Coarctation of the aorta
Systemic lupus erythematosus (pericarditis), collagen vascular disease,
end-stage renal disease with uremia
•
•
•
Abdomen Apical heave
Mass
Epigastric/flank bruit
Palpable kidneys
•
•
•
•
LVH/chronic hypertension
Wilms tumor, neuroblastoma, pheochromocytoma
Renal artery stenosis
Polysystic kidney disease, hydronephrosis, multicystic dysplastic kidney, mass
(see above)
•
•
•
•
Genitalia Ambiguous/virilization• Adrenal hyperplasia•
Extremities Joint swelling
Muscle weakness
•
•
Systemic lupus erythematosus, collagen vascular disease
Hyperaldosteronism, Liddle syndrome
•
•
Adapted from Flynn JT: Prog Pediatr Cardiol 2001;12:177*Findings listed are examples of physical findings and do not represent all possible physical findings.
>>p.52
NOVEMBER 2008 CONTEMPORARY PEDIATRICS 51
cntped1108_051.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan

CMECME
Primary hypertension
Once a comprehensive work-up looking for secondary
causes of hypertension has been completed and found
to be negative, a diagnosis of primary (or “essential”)
hypertension can be made. This diagnosis, while still
considered to be a diagnosis of exclusion, is more frequently
found in post-pubertal and African American children, and
in children with BP on the lower end of the hypertensive
spectrum (ie, just above the 95th percentile). It is also more
frequently found in children with a positive family history
of HTN, and in those who are overweight or obese.12
The role of obesity in this diagnosis should not be
overlooked. The number of children with primary
hypertension is on the rise concomitant with the rise in
childhood obesity.4,5,13,14 Several studies have demonstrated
the increased risk of hypertension that exists among obese
children. For example, for each one unit increase in BMI
z-score, children 8 to 17 years of age have been shown to
have twice the risk of having a BP greater than the 95th
percentile.13 Even children as young as 2 to 5 years of age
are not immune to these effects of obesity and overweight;
their SBP and DBP have also been shown to increase with
increasing BMI.15
Obesity and hypertension both separately and together put
children at increased cardiovascular risk.16 Obese children
are more likely to have clustering of cardiovascular risk
factors in addition to hypertension, such as hyperlipidemia,
insulin resistance, type 2 diabetes mellitus and left
ventricular hypertrophy.5 Autopsy studies of children reveal
that even early in life there is evidence of coronary artery
pathology, associated with BMI, dyslipidemia, and systolic
and diastolic BP.17
The link between OSA and hypertension
The mechanism by which obstructive sleep apnea (OSA) leads to hypertension is still
not well understood. One study has found a linear relationship between the severity
of OSA symptoms, and the incidence of newly diagnosed HTN, independent of body
mass, age, gender, or baseline BP and cigarette and alcohol consumption.1
It is likely that the hypoxemia and hypercapnea experienced by individuals with
OSA leads to an increase in sympathetic nervous system activity, which then leads to
an increase in peripheral vascular resistance. Hypoxia has been shown to increase
levels of endothelin-1, a known potent and long-acting vasoconstrictor, as well as
other circulating vasoconstrictors.
Because appropriate treatment of OSA has been shown to decrease daytime and
nighttime mean systolic and diastolic blood pressures by up to 10 mm Hg,2 screening
for OSA should be included in a clinician’s work-up of a child with hypertension.
Reference
1. Peppard PE, Young T, Palta M, et al: Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342:13782. Becker HF, Jerrentrup A, Ploch T, et al: Effect of nasal continuous positive airway pressure treatment on blood pressure in patients with obstructive sleep apnea. Circulation 2003;107:68
IMA
GE
: G
ET
TY
IM
AG
ES
/ME
DIO
IMA
GE
S/P
HO
TO
DIS
C
52 www.contemporarypediatrics.com Vol. 25, No. 11
cntped1108_052.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan

HYPERTENSION
Additionally, obesity and hypertension in childhood places
these children at higher risk for obesity and hypertension
as adults,20 with increased risk for CV morbidity and
mortality.21 Blood pressure tracking from childhood to
adulthood is much more likely to occur with increasing
BMI.22 Because of this BP tracking from childhood to
adulthood, lifestyle changes should be emphasized for all
hypertensive children, but should also particularly be aimed
at obese children with primary hypertension.
Management of pediatric hypertension
Who gets treated?
Once a child is diagnosed with HTN and is appropriately
staged and evaluated, treatment should be initiated and
aimed at the underlying etiology. Children with pre-
hypertension or asymptomatic, Stage 1 Primary HTN who
do not have evidence of end-organ damage or diabetes,
should be “prescribed” lifestyle modifications (Table 4)
and be re-evaluated in six months. Children with persistent
hypertension after six months—despite attempts at lifestyle
modification—should be started on an anti-hypertensive
medication. Similarly, any child with symptomatic HTN,
Stage 2 HTN, secondary HTN, diabetes or evidence of end-
organ damage should be started on an anti-hypertensive
medication.
Even after deciding to treat with an anti-hypertensive,
nonpharmacologic lifestyle interventions should continue to
be emphasized at each visit, particularly in overweight or
obese children. It has been shown that weight loss by itself
can decrease blood pressure,23 and other associated CV
risk factors should also be expected to regress or improve
with weight loss.24 Additionally, increased physical activity
and fitness has been shown to be associated with lower
childhood BP and a reduced risk of HTN 16 to 50 years
later.25 Obese children are also more likely to be salt sensitive,
and thus more likely to respond to dietary restriction of
sodium, and improved intake of potassium. The insulin
resistance often seen in obese children leads to salt and
water retention,26 and preliminary studies have indicated
that adipocytes may secrete factors leading to increased
serum aldosterone, which then leads to increased renal
sodium reabsorption.27-29
Often implementing these changes for all family
members is necessary before any appreciable benefit can
be achieved.
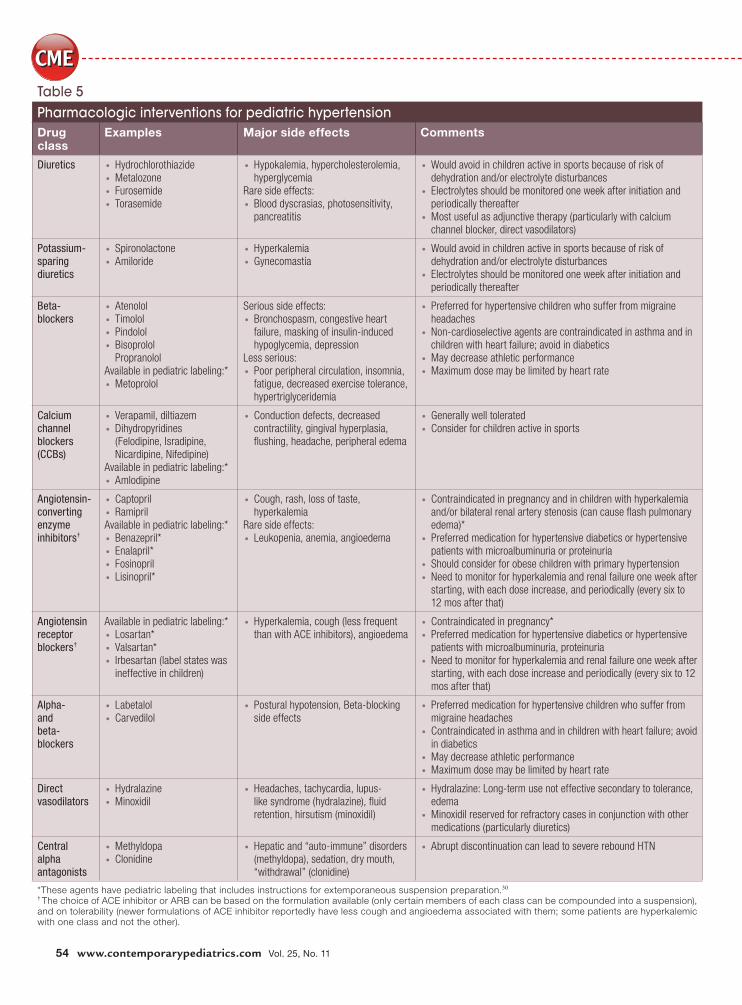
How should I treat?
There are multiple medications available to treat hypertension
in children, for which pediatric dosing is now available
(Table 5). The particular agent
chosen shou ld be a imed at
treating the underlying etiology,
with particular attention being
paid to co-morbid conditions
such as diabetes, asthma, and
migraines.
Af ter a fu l l eva luation to
determine etiology is completed
(and any interventions are under-
taken to treat the underlying
disease process), initial antihyper-
tensive therapy for a child who
continues to be hypertensive
should include either a calcium
channel blocker (CCB) or an
angiotensin converting enzyme
(ACE) inhibitor, unless there is a
compelling reason to use an agent
from another class. Both CCBs and
ACE inhibitors are generally well tolerated with a minimal
side effect profile, and can be dosed once daily.
Obese children with primary hypertension may
particularly benefit from ACE inhibitors or angiotensin-
Weight loss by
itself can
decrease blood
pressure, and
other associated
CV risk factors
should also
be expected
to regress or
improve with
weight loss.
Point
Taken
Table 4
Non-pharmacologic interventions1
Aerobic exercise: 30 to 45 minutes “most days” of the week
Limit sedentary activities to less than two hours per day
Weight reduction if overweight
Increased intake of fresh vegetables, fruits, and low-fat dairy (the
Dietary Approaches to Stop Hypertension (DASH) Study eating
plan)18
Salt restriction*
Adequate intake of potassium and calcium (both shown to have
antihypertensive effects)19
Cessation of smoking
•
•
•
•
•
•
•
*Can start with recommending “no added salt” with ultimate goal of achieving the current recommendation of 1.2 grams/day total for 4- to 8-year-olds and 1.5 grams/day for children 9 years and older.1
NOVEMBER 2008 CONTEMPORARY PEDIATRICS 53
cntped1108_053.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan
CMECME
Table 5
Pharmacologic interventions for pediatric hypertension
Drug class
Examples Major side effects Comments
Diuretics Hydrochlorothiazide
Metalozone
Furosemide
Torasemide
•
•
•
•
Hypokalemia, hypercholesterolemia,
hyperglycemia
Rare side effects:
Blood dyscrasias, photosensitivity,
pancreatitis
•
•
Would avoid in children active in sports because of risk of
dehydration and/or electrolyte disturbances
Electrolytes should be monitored one week after initiation and
periodically thereafter
Most useful as adjunctive therapy (particularly with calcium
channel blocker, direct vasodilators)
•
•
•
Potassium-
sparing
diuretics
Spironolactone
Amiloride
•
•
Hyperkalemia
Gynecomastia
•
•
Would avoid in children active in sports because of risk of
dehydration and/or electrolyte disturbances
Electrolytes should be monitored one week after initiation and
periodically thereafter
•
•
Beta-
blockers
Atenolol
Timolol
Pindolol
Bisoprolol
Propranolol
Available in pediatric labeling:*
Metoprolol
•
•
•
•
•
Serious side effects:
Bronchospasm, congestive heart
failure, masking of insulin-induced
hypoglycemia, depression
Less serious:
Poor peripheral circulation, insomnia,
fatigue, decreased exercise tolerance,
hypertriglyceridemia
•
•
Preferred for hypertensive children who suffer from migraine
headaches
Non-cardioselective agents are contraindicated in asthma and in
children with heart failure; avoid in diabetics
May decrease athletic performance
Maximum dose may be limited by heart rate
•
•
•
•
Calcium
channel
blockers
(CCBs)
Verapamil, diltiazem
Dihydropyridines
(Felodipine, Isradipine,
Nicardipine, Nifedipine)
Available in pediatric labeling:*
Amlodipine
•
•
•
Conduction defects, decreased
contractility, gingival hyperplasia,
flushing, headache, peripheral edema
• Generally well tolerated
Consider for children active in sports
•
•
Angiotensin-
converting
enzyme
inhibitors†
Captopril
Ramipril
Available in pediatric labeling:*
Benazepril*
Enalapril*
Fosinopril
Lisinopril*
•
•
•
•
•
•
Cough, rash, loss of taste,
hyperkalemia
Rare side effects:
Leukopenia, anemia, angioedema
•
•
Contraindicated in pregnancy and in children with hyperkalemia
and/or bilateral renal artery stenosis (can cause flash pulmonary
edema)*
Preferred medication for hypertensive diabetics or hypertensive
patients with microalbuminuria or proteinuria
Should consider for obese children with primary hypertension
Need to monitor for hyperkalemia and renal failure one week after
starting, with each dose increase, and periodically (every six to
12 mos after that)
•
•
•
•
Angiotensin
receptor
blockers†
Available in pediatric labeling:*
Losartan*
Valsartan*
Irbesartan (label states was
ineffective in children)
•
•
•
Hyperkalemia, cough (less frequent
than with ACE inhibitors), angioedema
• Contraindicated in pregnancy*
Preferred medication for hypertensive diabetics or hypertensive
patients with microalbuminuria, proteinuria
Need to monitor for hyperkalemia and renal failure one week after
starting, with each dose increase and periodically (every six to 12
mos after that)
•
•
•
Alpha-
and
beta-
blockers
Labetalol
Carvedilol
•
•
Postural hypotension, Beta-blocking
side effects
• Preferred medication for hypertensive children who suffer from
migraine headaches
Contraindicated in asthma and in children with heart failure; avoid
in diabetics
May decrease athletic performance
Maximum dose may be limited by heart rate
•
•
•
•
Direct
vasodilators
Hydralazine
Minoxidil
•
•
Headaches, tachycardia, lupus-
like syndrome (hydralazine), fluid
retention, hirsutism (minoxidil)
• Hydralazine: Long-term use not effective secondary to tolerance,
edema
Minoxidil reserved for refractory cases in conjunction with other
medications (particularly diuretics)
•
•
Central
alpha
antagonists
Methyldopa
Clonidine
•
•
Hepatic and “auto-immune” disorders
(methyldopa), sedation, dry mouth,
“withdrawal” (clonidine)
• Abrupt discontinuation can lead to severe rebound HTN•
*These agents have pediatric labeling that includes instructions for extemporaneous suspension preparation.30 † The choice of ACE inhibitor or ARB can be based on the formulation available (only certain members of each class can be compounded into a suspension), and on tolerability (newer formulations of ACE inhibitor reportedly have less cough and angioedema associated with them; some patients are hyperkalemic with one class and not the other).
54 www.contemporarypediatrics.com Vol. 25, No. 11
cntped1108_054.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan

HYPERTENSION
receptor blockers (ARBs) therapy as the likely mechanism
for HTN in this group is increased sodium retention and
sympathetic nervous system (SNS) activation. Moreover,
these agents may have beneficial effects on diabetes
and dyslipidemia. Because diuretics can worsen insulin
resistance and dyslipidemia, as well as increase SNS and
renin activity, they should be avoided in obese children
with hypertension. Also, beta blockers should be avoided
in this group as they can lead to weight gain, increased
triglycerides, and decreased high-density lipoprotein
cholesterol concentrations.31,32
A word of caution: ACE inhibitors and ARBs can lead
to hyperkalemia and renal failure in certain individuals.
Therefore, lab tests should be undertaken one to two weeks
after starting either one of these medications to look for
evidence of these conditions. Additionally, flash pulmonary
edema can occur if bilateral renal artery stenosis is present,
so it would be wise to delay prescribing an ACE inhibitor or
ARB until after obtaining a renal ultrasound with Doppler
examination of the renal vessels. Lastly, as ACE inhibitors
and ARBs can also be highly teratogenic, contraception
should be discussed with females of childbearing age when
considering these classes of medications.
Once a medication is chosen, the lowest dose should
be started, with the dose increased in a step-wise fashion
to achieve normotension and regression of end-organ
damage, if present. Once the patient reaches the maximum
recommended dose of a medication, or experiences side
effects that limit reaching the maximium recommended
dose, an additional medication is initiated in the same
manner.
The goal for both non-pharmacologic and pharmacologic
therapy is to achieve BPs less than the 95th percentile
for most children, or less than the 90th percentile for
children with chronic kidney disease, diabetes, or evidence
of end-organ damage. This should be done in a manner
to maximize BP response while minimizing side effects
and maximizing probability of patient compliance. Side
effects can be minimized by prescribing the least amount of
drug necessary to effectively reduce BP. Higher degrees of
medication compliance can be achieved by being mindful of
medication side effects,
patient lifestyle, and
comorbid conditions.
Once therapy is in-
it iated, close moni-
toring for desired effect,
presence of side effects
and compliance is vitally
important. There are
no specific, published
guidelines regarding
frequency of monitoring
and fol low-up af ter
initiation of therapy,
but in the beginning it
would be reasonable to
measure a child’s blood
pressure at least weekly
and arrange for follow-
up every three months.
Weekly BP monitoring
can occur in a clinic
setting (via a nursing visit), a school setting (where the
school nurse measures manual BPs and faxes the readings
to the physician), or in a home setting either with a
properly calibrated, automated cuff or by manual measure-
ment done by a properly trained family member. As previously
mentioned, public BP cuffs are not appropriate for this monitoring
as they are likely to be inaccurate.
Once the child has achieved target BP’s on a medication
regimen, clinic follow-up can be spaced to every six months.
ACE inhibitors and
ARBs can lead to
hyperkalemia and
renal failure in certain
individuals. Therefore,
lab tests should be
undertaken one to two
weeks after starting
either one of these
medications to look
for evidence of these
conditions.
Point
Taken
>>p.56IMA
GE
: G
ET
TY
IM
AG
ES
/P
HO
TO
DIS
C/K
EIT
H B
RO
FS
KY
NOVEMBER 2008 CONTEMPORARY PEDIATRICS 55
cntped1108_055r1.pgs 11.05.2008 07:24 ADVANSTAR_PDF/X-1a blackyellowmagentacyan

CMECME
When to refer?
Depending on provider comfort level, the diagnosis, initial
work-up and treatment can be provided in the primary care
setting, or can be handled by a specialist with expertise in
pediatric hypertension. Ongoing collaboration and frequent
communication between specialists and primary care
providers is essential for successful patient management.
Once presented with refractory hypertension or with a
child very likely to have secondary hypertension, referral
to a specialist should be made for further work-up and
treatment. ◽
References
1. The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Pediatrics 2004;114:555. Available at http://pediatrics.aappublications.org/cgi/reprint/114/2/S2/555. Accessed Oct. 17, 20082. Fixler DE, Laird WP, Fitzgerald V, et al: Hypertension screening in schools: results of the Dallas study. Pediatrics 1979;63:323. Sinaiko AR, Gomez-Marin O, Prineas RJ: Prevalence of “significant” hypertension in junior high school-aged children: The children and adolescent blood pressure program. J Pediatr 1989;114:6644. Sorof JM, Lai D, Turner J, et al: Overweight, ethnicity, and the prevalence of hypertension in school-aged children. Pediatrics 2004;113:4755. Sorof J, Daniels S: Obesity hypertension in children: a problem of epidemic proportions. Hypertension 2002;40:4416. Pickering TG, Hall JE, Appel LJ, et al: Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: A statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension 2005;45:1427. Get the most out of home blood pressure monitoring. Mayo Foundation for Medical Education and Research, 2008. Available at: www.mayoclinic.com/health/high-blood-pressure/HI00016. Accessed Oct. 5, 20088. Free blood pressure machines: Are they accurate? Mayo Foundation for Medical Education and Research, 2008. Available at: www.mayoclinic.com/health/blood-pressure/AN00567. Accessed Oct. 17, 20089. Bartosh SM, Aronson AJ: Childhood hypertension: An update on etiology, diagnosis, and treatment. Pediatr Clin North Am 1999;46:23510. Flynn JT: Evaluation and management of hypertension in childhood. Prog Pediatr Cardiol 2001;12:17711. Sinaiko AR: Hypertension in children. N Engl J Med 1996;335:196812. Epidemiology, risk factors, and etiology of hypertension in children and adolescents. UpToDate, 2008. Available at: www.utdol.com/online/content/topic.do?topicKey=pedineph/19132&linkTitle=Essential%20hypertension&source=preview&selectedTitle=1~150&anchor=14#14. Accessed Oct. 17, 200813. Din-Dzietham R, Liu Y, Bielo MV, et al: High blood pressure trends in children and adolescents in national surveys, 1963 to 2002. Circulation 2007;116:148814. Muntner P, He J, Cutler JA, et al: Trends in blood pressure among children and adolescents. JAMA 2004;291:210715. Falkner B, Gidding SS, Ramirez-Garnica G, et al: The relationship of body mass index and blood pressure in primary care pediatric patients. J Pediatr 2006;148:19516. Barlow SE, Dietz WH: Obesity evaluation and treatment: Expert Committee recommendations. The Maternal and Child Health Bureau, Health Resources and
Services Administration and the Department of Health and Human Services. Pediatrics 1998;102:E29.17. Berenson GS, Srinivasan SR, Bao W, et al: Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults: The Bogalusa Heart Study. N Engl J Med 1998;338:165018. Appel LJ, Moore TJ, Obarzanek E, et al: A clinical trial of the effects of dietary patterns on blood pressure: DASH Collaborative Research Group. N Engl J Med 1997;336:111719. Flynn JT: Hypertension in adolescents. Adolesc Med Clin 2005;16:1120. Lughetti L, De Simone M, Verrotti A, et al: Thirty-year persistence of obesity after presentation to a pediatric obesity clinic. Ann Hum Biol 2008;35:43921. DiPietro L, Mossberg HO, Stunkard AJ: A 40-year history of overweight children in Stockholm: life-time overweight, morbidity, and mortality. Int J Obes Relat Metab Disord 1994;18:58522. Srinivasan SR, Myers L, Berenson GS: Changes in metabolic syndrome variables since childhood in prehypertensive and hypertensive subjects: the Bogalusa Heart Study. Hypertension 2006;48:3323. Rocchini AP, Katch V, Anderson J, et al: Blood pressure in obese adolescents: effect of weight loss. Pediatrics 1988;82:1624 . Williams CL, Hayman LL, Daniels SR, et al: Cardiovascular health in childhood: A statement for health professionals from the Committee on Atherosclerosis, Hypertension, and Obesity in the Young (AHOY) of the Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2002;106:14325. Textor SC, Townsend RR: Hypertension. NephSAP 2008;7:6326. Rocchini AP, Katch V, Kveselis D, et al: Insulin and renal sodium retention in obese adolescents. Hypertension 1989;14:36727. Goodfriend TL, Calhoun DA: Resistant hypertension, obesity, sleep apnea, and aldosterone: theory and therapy. Hypertension 2004;43:51828. Goodfriend TL, Ball DL, Gardner HW: An oxidized derivative of linoleic acid affects aldosterone secretion by adrenal cells in vitro. Prostaglandins Leukot Essent Fatty Acids 2002;67:16329. Ehrhart-Bornstein M, Lamounier-Zepter V, Schraven A, et al: Human adipocytes secrete mineralocorticoid-releasing factors. Proc Natl Acad Sci USA 2003;100:1421130. Flynn JT: Pediatric hypertension: recent trends and accomplishments, future challenges. Am J Hypertens 2008;21:60531. Mathew B, Patel SB, Reams GP, et al: Obesity-hypertension: emerging concepts in pathophysiology and treatment. Am J Med Sci 2007;334:233132. Sharma AM, Pischon T, Engeli S, et al: Choice of drug treatment for obesity-related hypertension: where is the evidence? J Hypertens 2001;19:667
IMA
GE
: G
ET
TY
IM
AG
ES
/SIE
DE
PR
EIS
/KE
ITH
BR
OF
SK
Y
56 www.contemporarypediatrics.com Vol. 25, No. 11
cntped1108_056.pgs 11.04.2008 12:44 ADVANSTAR_PDF/X-1a blackyellowmagentacyan





























