Embed Size (px)
Citation preview
4/15/21
1
Pediatric Obesity – Assessment and Initial Management
Family Medicine Update, 4/15/2021
Dr. Julie Benard, FAAP, DABOM
Assistant Professor of Clinical Child Health
Medical Director of the Tigers on Track Clinic
1
Objectives:1. Recognize obesity as a DISEASE
2. Understand definitions for overweight and obesity in kids and understand the limitations of using these definitions.
3. Learn the epidemiology of the childhood obesity epidemic
4. Identify risk factors for obesity
5. Understand the co-morbidities associated with obesity and when to get labs
6. Know the basics of treatment with medications and potential surgical options
2
Obesity is a DISEASE, it is not…• A consequence of poor parenting
• Brought on by a lack of willpower to eat right and exercise
• As just as simple as calories in < calories out = weight loss (i.e., 500 less calories in each week does not necessarily = 1 lb weight loss weekly)
3
4/15/21
2
Obesity is COMPLEX with a lot of variables
Obesity
Genetics
EpigeneticsEnvironment
Body’s abnormal physiology
Diet
Exercise
Family dynamics
Childhood stressors
4
Obesity as a DISEASE:• Weight control is COMPLEX,
consisting of interactions between gut hormones and adipose tissue hormones and their effects on the brain to affect hunger, cognition, emotion, and behavior.
• Additionally, there are complex signal pathways within the brain that control hunger and energy expenditure
5
Effects of epigenetics on obesity development:• Both SGA and LGA can increase a
child’s risk of developing obesity
• SGA – can cause excessive postnatal weight gain– Tobacco use– Lack of adequate gestational weight
gain
• LGA– Maternal diabetes– Excessive gestational weight gain– Preconception BMI >/= 30 (? Higher
prevalence of insulin resistance)
• Low Birth-weight/Premature Birth– Stressed– May have higher level of visceral
fat– Tend to be fed higher calorie
formulas to help with growth– May have more antibiotic
exposure early in life
• Method of delivery – vaginal vs. C-section affecting microbiome?
6
4/15/21
3
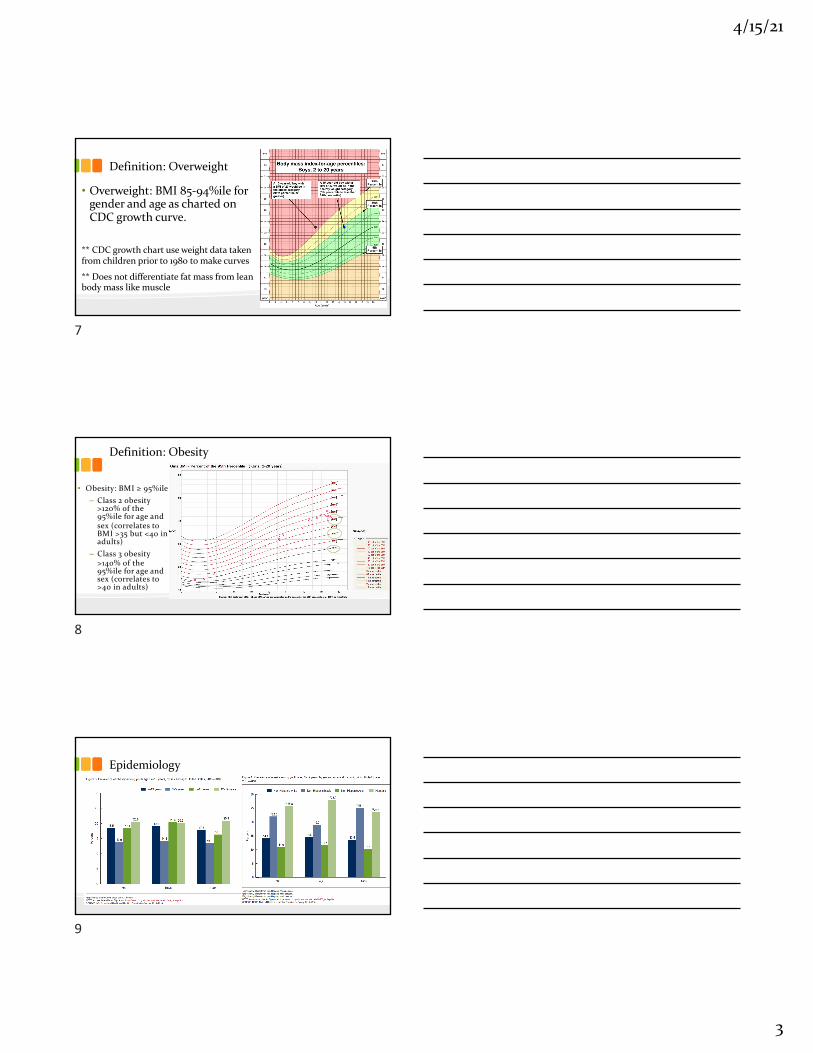
Definition: Overweight
• Overweight: BMI 85-94%ile for gender and age as charted on CDC growth curve.
** CDC growth chart use weight data taken from children prior to 1980 to make curves
** Does not differentiate fat mass from lean body mass like muscle
7
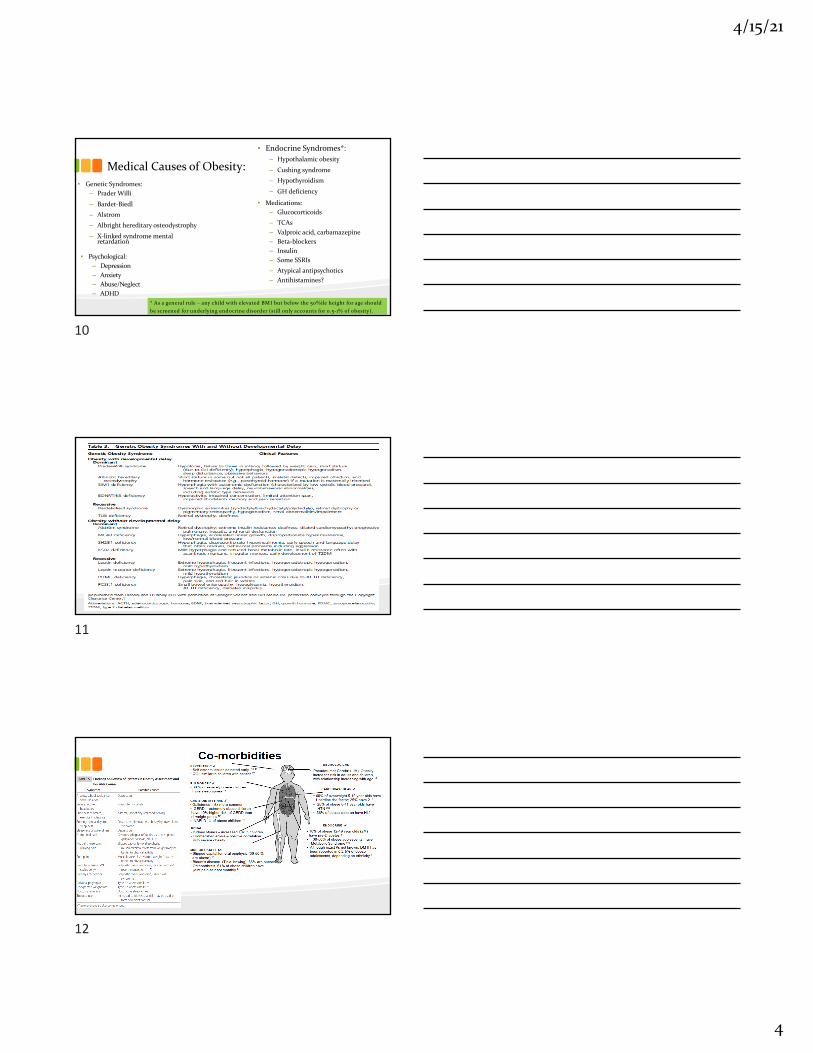
Definition: Obesity
• Obesity: BMI ≥ 95%ile– Class 2 obesity
>120% of the 95%ile for age and sex (correlates to BMI >35 but <40 in adults)
– Class 3 obesity >140% of the 95%ile for age and sex (correlates to >40 in adults)
8
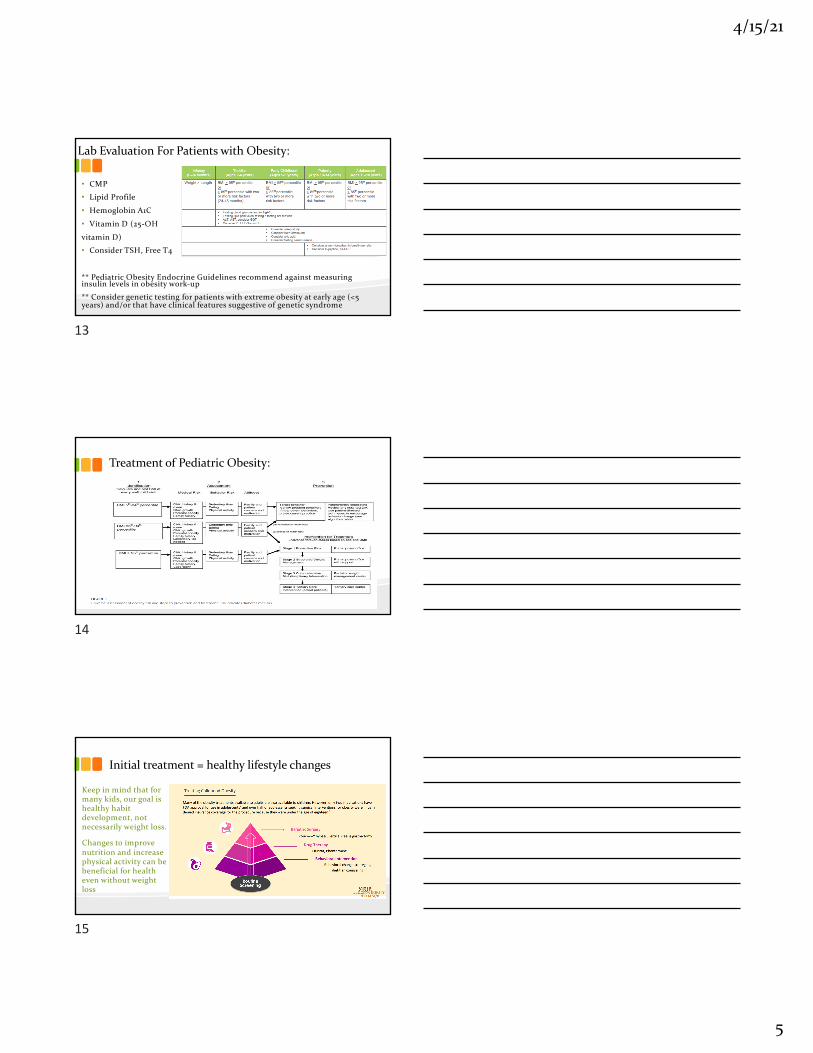
Epidemiology
9
4/15/21
4
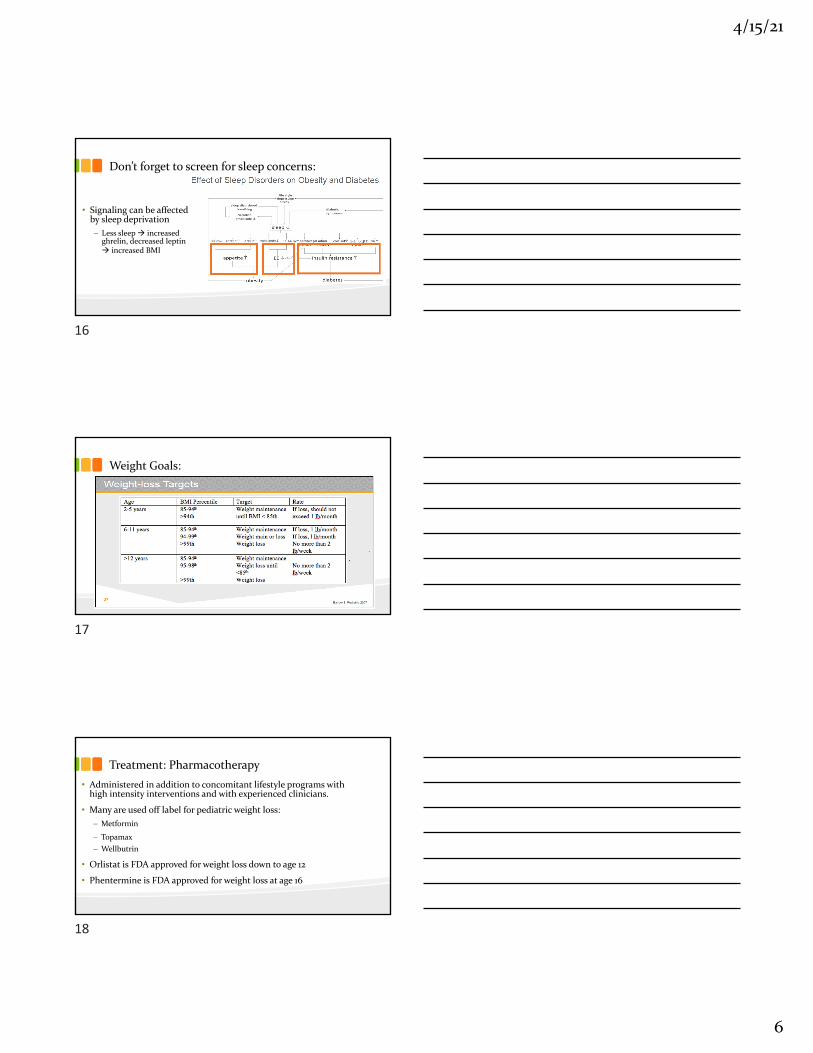
Medical Causes of Obesity:• Genetic Syndromes:
– Prader Willi
– Bardet-Biedl – Alstrom– Albright hereditary osteodystrophy
– X-linked syndrome mental retardation
• Endocrine Syndromes*:– Hypothalamic obesity
– Cushing syndrome– Hypothyroidism
– GH deficiency
• Psychological:– Depression– Anxiety– Abuse/Neglect– ADHD
• Medications:– Glucocorticoids– TCAs– Valproic acid, carbamazepine– Beta-blockers– Insulin– Some SSRIs– Atypical antipsychotics– Antihistamines?
* As a general rule – any child with elevated BMI but below the 50%ile height for age should be screened for underlying endocrine disorder (still only accounts for 0.5-1% of obesity).
10
11
12
4/15/21
5
Lab Evaluation For Patients with Obesity:
• CMP
• Lipid Profile
• Hemoglobin A1C
• Vitamin D (25-OH
vitamin D)
• Consider TSH, Free T4
** Pediatric Obesity Endocrine Guidelines recommend against measuring insulin levels in obesity work-up
** Consider genetic testing for patients with extreme obesity at early age (<5 years) and/or that have clinical features suggestive of genetic syndrome
13
Treatment of Pediatric Obesity:
14
Initial treatment = healthy lifestyle changes
Keep in mind that for many kids, our goal is healthy habit development, not necessarily weight loss.
Changes to improve nutrition and increase physical activity can be beneficial for health even without weight loss
15
4/15/21
6
Don’t forget to screen for sleep concerns:
• Signaling can be affected by sleep deprivation– Less sleep à increased
ghrelin, decreased leptin à increased BMI
16
Weight Goals:
17
Treatment: Pharmacotherapy• Administered in addition to concomitant lifestyle programs with
high intensity interventions and with experienced clinicians.
• Many are used off label for pediatric weight loss:– Metformin
– Topamax– Wellbutrin
• Orlistat is FDA approved for weight loss down to age 12
• Phentermine is FDA approved for weight loss at age 16
18
4/15/21
7
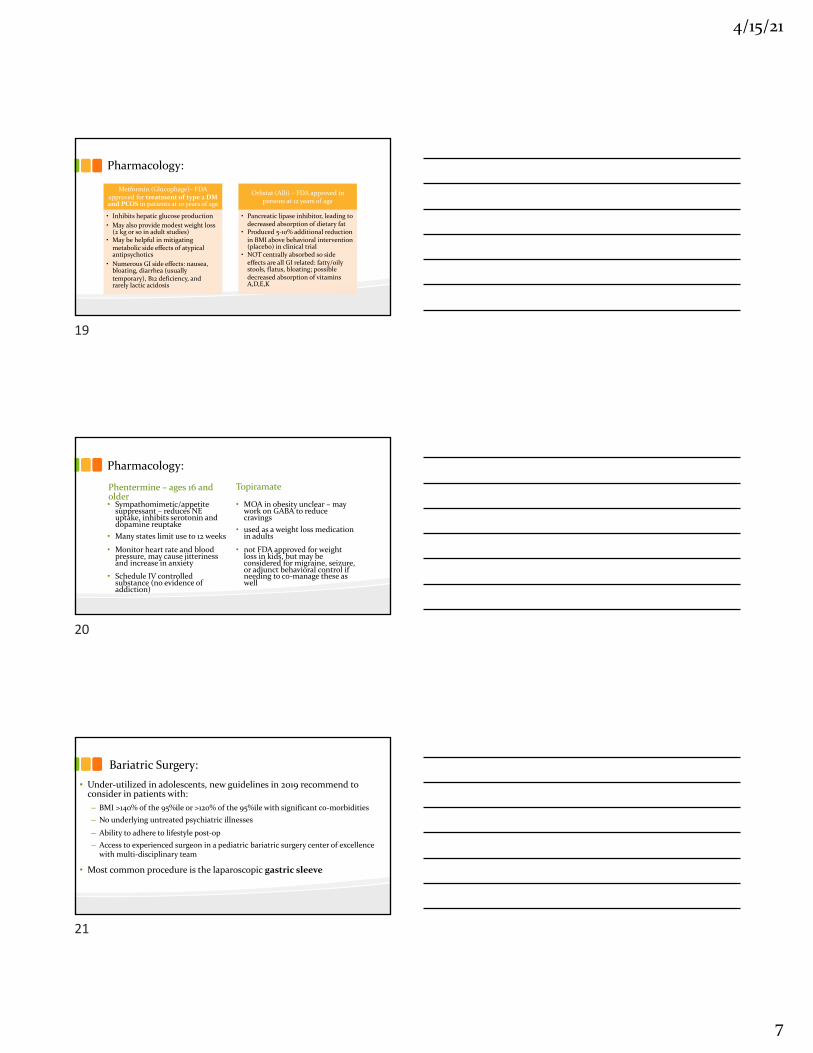
Pharmacology:
Metformin (Glucophage)– FDA approved for treatment of type 2 DM and PCOS in patients at 10 years of age
• Inhibits hepatic glucose production• May also provide modest weight loss
(2 kg or so in adult studies)• May be helpful in mitigating
metabolic side effects of atypical antipsychotics
• Numerous GI side effects: nausea, bloating, diarrhea (usually temporary), B12 deficiency, and rarely lactic acidosis
Orlistat (Alli) – FDA approved in persons at 12 years of age
• Pancreatic lipase inhibitor, leading to decreased absorption of dietary fat
• Produced 5-10% additional reduction in BMI above behavioral intervention (placebo) in clinical trial
• NOT centrally absorbed so side effects are all GI related: fatty/oily stools, flatus, bloating; possible decreased absorption of vitamins A,D,E,K
19
Pharmacology:
Phentermine – ages 16 and older• Sympathomimetic/appetite
suppressant – reduces NE uptake, inhibits serotonin and dopamine reuptake
• Many states limit use to 12 weeks
• Monitor heart rate and blood pressure, may cause jitteriness and increase in anxiety
• Schedule IV controlled substance (no evidence of addiction)
Topiramate
• MOA in obesity unclear – may work on GABA to reduce cravings
• used as a weight loss medication in adults
• not FDA approved for weight loss in kids, but may be considered for migraine, seizure, or adjunct behavioral control if needing to co-manage these as well
20
Bariatric Surgery:• Under-utilized in adolescents, new guidelines in 2019 recommend to
consider in patients with:– BMI >140% of the 95%ile or >120% of the 95%ile with significant co-morbidities– No underlying untreated psychiatric illnesses
– Ability to adhere to lifestyle post-op– Access to experienced surgeon in a pediatric bariatric surgery center of excellence
with multi-disciplinary team
• Most common procedure is the laparoscopic gastric sleeve
21
4/15/21
8
Staged Treatment Plan:https://ihcw.aap.org/resources/Documents/algorithm_brightfutures_032819.pdf
• Stage 1 treatment – elicit from patient/parent what behavior they would consider changing, make a plan to change (more for overweight category) – see back monthly if family agrees
• If not meeting goals after 3-6 months (or if BMI >95%ile), then may consider structured weight management (stage 2 treatment) (PCP guided with RD and psychological support, focus on specific lifestyle changes) – see back every 2-4 weeks if family agrees
• If not meeting goals 3-6 months, then refer to comprehensive multidisciplinary intervention at a weight management center (Tigers on Track, stage 3 treatment) –weekly for 12-26 weeks has been shown to be the most beneficial (the longer the better)
• If not meeting goals after 3-6 months, refer to tertiary care intervention (bariatric surgery consideration, Tigers on Track with collaboration with bariatric surgery team)
22
23
24
4/15/21
9
25
Your Resources at MU:• Tigers on Track Clinic– Dr. Benard, MD– Jan Todd, DNP– Dieticians: Sherly Cherian, RD; Hallee Mitchell, RD– PT: Kelsey Okruch, DPT; Sallie Fruits, DPT; Rachel Bahner, DPT– Social Worker: Jessica Peterson, MSWRefer to endocrinology and put “Tigers on Track” in the reason line.
• FitTastic Program through the MU Clinics• Dr. Benard at MU Pediatrics Clinic
26
References:• Armstrong, S.C., Bolling, C.F., Michalsky, M.P, Reichard, K.W., & Section on Obesity, Section on Surgery. Pediatric metabolic and bariatric surgery: Evidence, barriers,
and best practices. Pediatrics, 144, e20193223.
• Barlow, S. (2007). Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity. Pediatrics, 120, s164-s192.
• Bolling, C.F., Armstrong, S.C., Reichard, K.W., Michalsky, M.P & Section on Obesity, Section on Surgery. Metabolic and bariatric surgery for pediatric patients with severe obesity. Pediatrics, 114, e20193224
• Hassink, S.G. (2014). Pediatric Obesity Prevention, Intervention, and Treatment Strategies for Primary Care, 2nd ed. Illinois: American Academy of Pediatrics.
• Rome, E.S. (2011). Obesity Prevention and Treatment. Pediatrics in Review, 32, 363-373.
• Sothern M.S., Gordon, S.T., & Von Almen, T.K. (2006). Handbook of Pediatric Obesity Clinical Management. Boca Raton: CRC Taylor and Francis.
• Spear, B.A., Barlow, S.E., Ervin, C., Ludwig, D.S., Saelens, B.E., Schetzina, K.E., & Taveras, E.M. (2007). Recommendations for treatment of child and adolescent overweight and obesity. Pediatrics, 120, S254-S288.
• Styne, D.M. et al. (2017). Pediatric Obesity – Assessment, treatment, and prevention: An Endocrine Society clinical practice guidline. J. Clinical Endocrinol Metab, 102, 1-49.
• Obesity Medicine Association 2016 ABOM Board Review Series
• https://ihcw.aap.org/resources/Documents/algorithm_brightfutures_032819.pdf
• Obesity in Early Life.pdf (gwu.edu)
27