Embed Size (px)
Citation preview
Pediatric OrthopedicsLlewellyn Mensah, MD
3/19/15
Outline Common pediatric orthopedic problems
DMD Club foot DDH
Intoeing
Common hip conditions in pediatric and adolescent population Transient synovitis SCFE Legg Calve Perthes
Osteochondroses Osteochondritis dessecans Kohler’s osteochondritis Freiberg’s osteochondrosis
Apophysitides – scoliosis, traction apophysitis, Osgood Schlatter’s, Sever’s
Benign nocturnal limb pain of childhood
Pediatric fractures
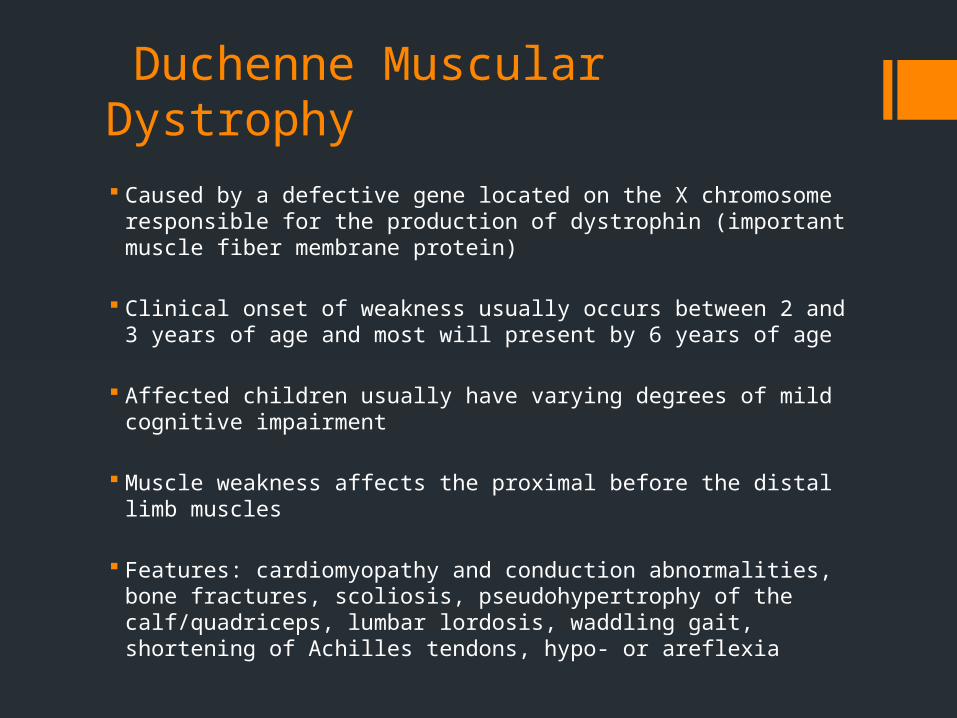
Duchenne Muscular Dystrophy Caused by a defective gene located on the X chromosome
responsible for the production of dystrophin (important muscle fiber membrane protein)
Clinical onset of weakness usually occurs between 2 and 3 years of age and most will present by 6 years of age
Affected children usually have varying degrees of mild cognitive impairment
Muscle weakness affects the proximal before the distal limb muscles
Features: cardiomyopathy and conduction abnormalities, bone fractures, scoliosis, pseudohypertrophy of the calf/quadriceps, lumbar lordosis, waddling gait, shortening of Achilles tendons, hypo- or areflexia
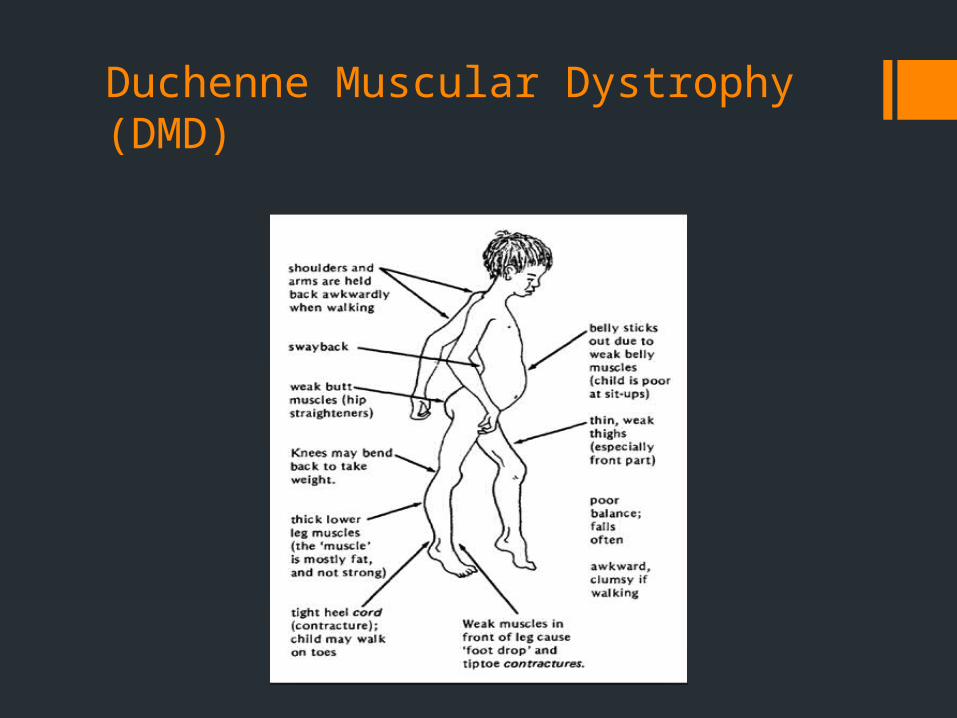
Duchenne Muscular Dystrophy (DMD)
DMD
DMD is the most common fatal disease affecting children in the United States
Patients with DMD are often confined to a wheelchair by age 12 years and die in their late teens or 20s from respiratory insufficiency or cardiomyopathy
Elevated levels of serum CK and EKG abnormalities are common
Muscle biopsy confirms the diagnosis if genetic studies are negative

DMD Treatment aims at preventing complications
Respiratory – volume recruitment / deep lung inflation, manual and mechanically assisted cough techniques, nocturnal ventilation, daytime ventilation, tracheostomy
Orthopedic interventions to prevent contractures, nutritional and weight monitoring, dietary calcium and vitamin D supplementation, exercise to prevent disuse atrophy
For boys 5 years of age and older who are no longer gaining motor skills, or whose motor skills are declining – glucocorticoids (prednisone or deflazacort)
With LVEF < 55% or LV dilation – ACEI or Β blocker
Erb’s palsy
Erb’s palsy
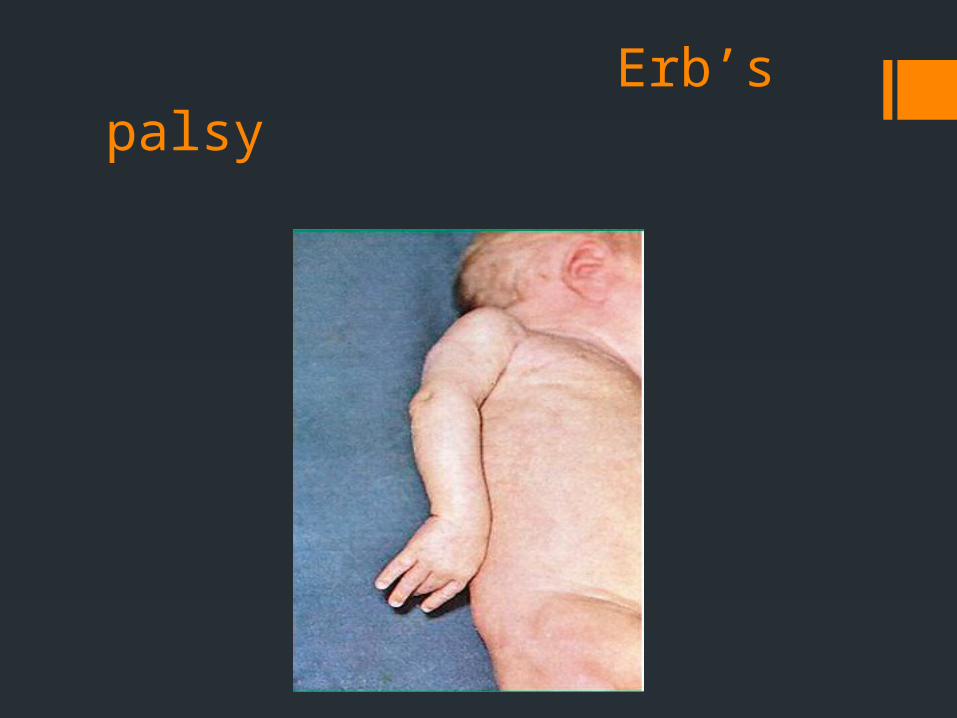
Paralysis of arm caused by injury to C5 – C6
Arises most commonly , but not exclusively, from shoulder dystocia during a difficult birth
Loss of sensation in the arm and paralysis and atrophy of the deltoid, biceps and brachialis
The arm hangs by the side and is rotated medially; the forearm is extended and pronated and there is loss of shoulder abduction, elbow flexion and supination of the forearm (waiter’s tip).
Depending on severity, the paralysis can either resolve on its own over a period of months, or necessitate rehab / surgery
Treatment: Daily PT; Serial exams for 3 – 6 mo and surgical referral if still no improvement
Club foot

Club foot
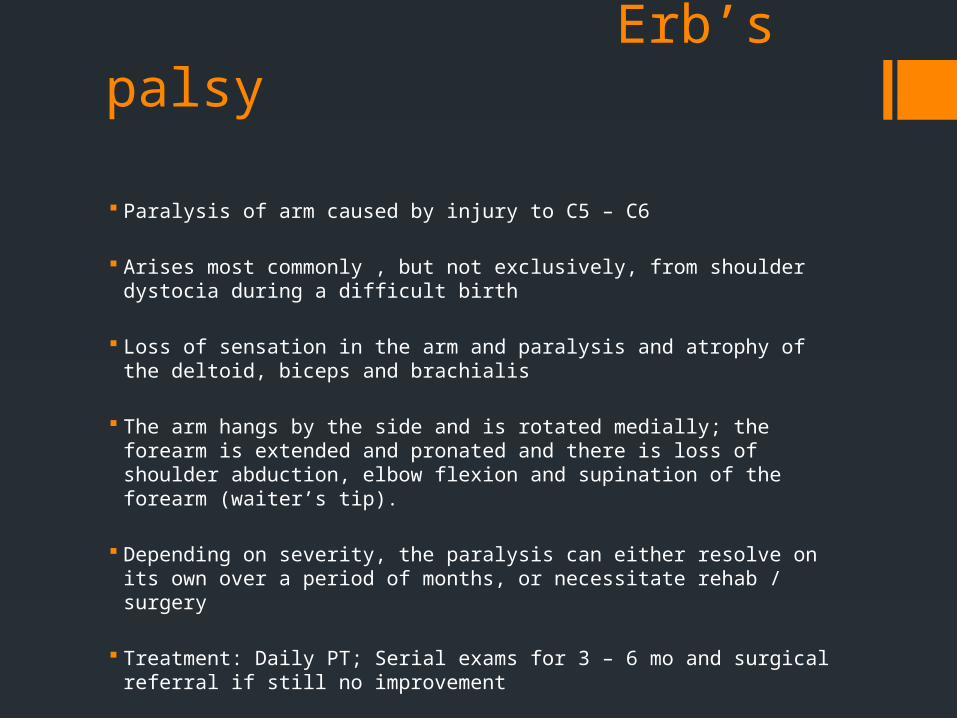
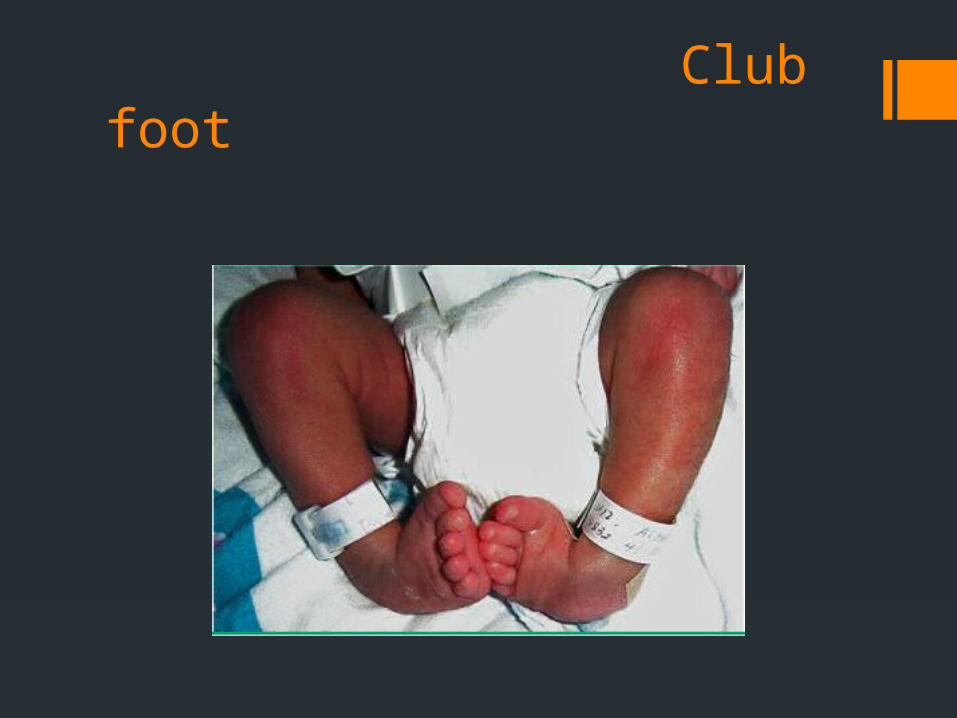
AKA talipes equinovarus – foot is excessively plantar flexed, with the forefoot swung medially and the sole facing inward
Can be diagnosed in utero by u/s; Amniocentesis for karyotype if there are associated abnormalities (syndromic clubfoot)
Hereditary predisposition; 1:1000 live births; boys > girls
For parents without clubfoot, the overall risk of recurrent isolated clubfoot depends upon the sex of the first affected child
2% after an affected male; 5% after an affected female
If both a parent and a child are affected, then the recurrence risk is as high as 25%

Club foot: Types / Therapy
Classification
Congenital (most common): isolated anomaly; - Rx: Serial casting and bracing (Ponseti method) followed by heel cord release and night time bracing x 2 years if necessary
Syndromic: associated with connective tissue, genetic, neuromuscular disorders. Rx: surgical correction at 9 – 12 mo if needed
Positional: intrauterine crowding or breech position; - easily corrects to normal position with manipulation
Developmental dysplasia of the hip
Spectrum of conditions related to the development of the hip in infants and young children – dislocation / dislocatability, subluxation / subluxability, femoral head and acetabular dysplasia
Incidence is 1 – 2 per 1000 newborn infants
Risk factors: female sex, breech presentation and other conditions associated with limited fetal mobility, family history
Hip exam should occur at birth and at every health supervision visit until the child is walking normally (usually by 2 years of age).
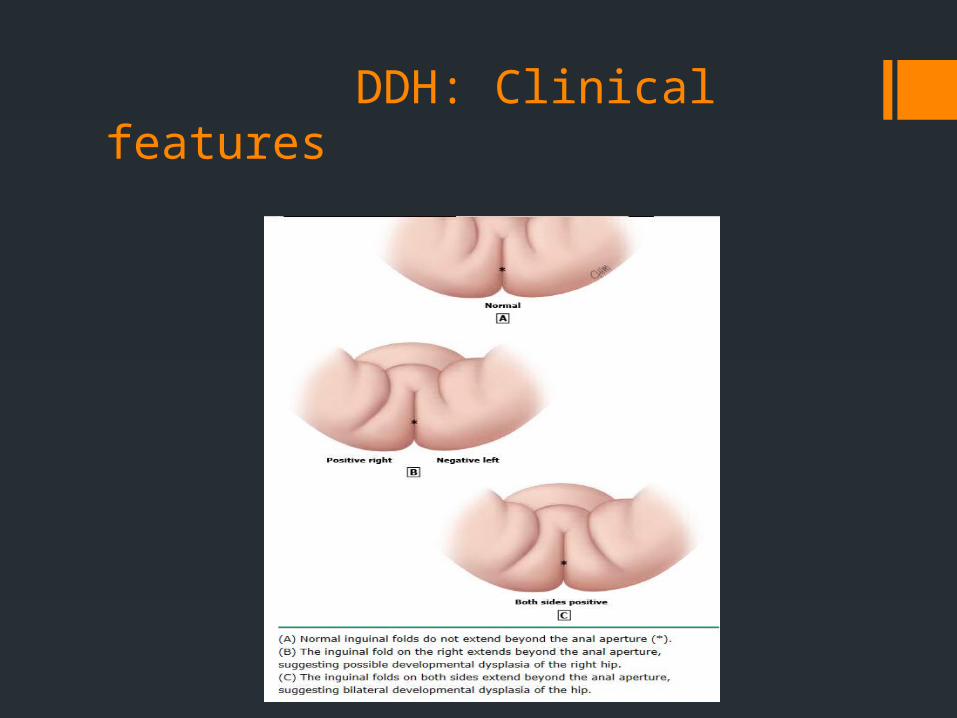
DDH: Clinical features
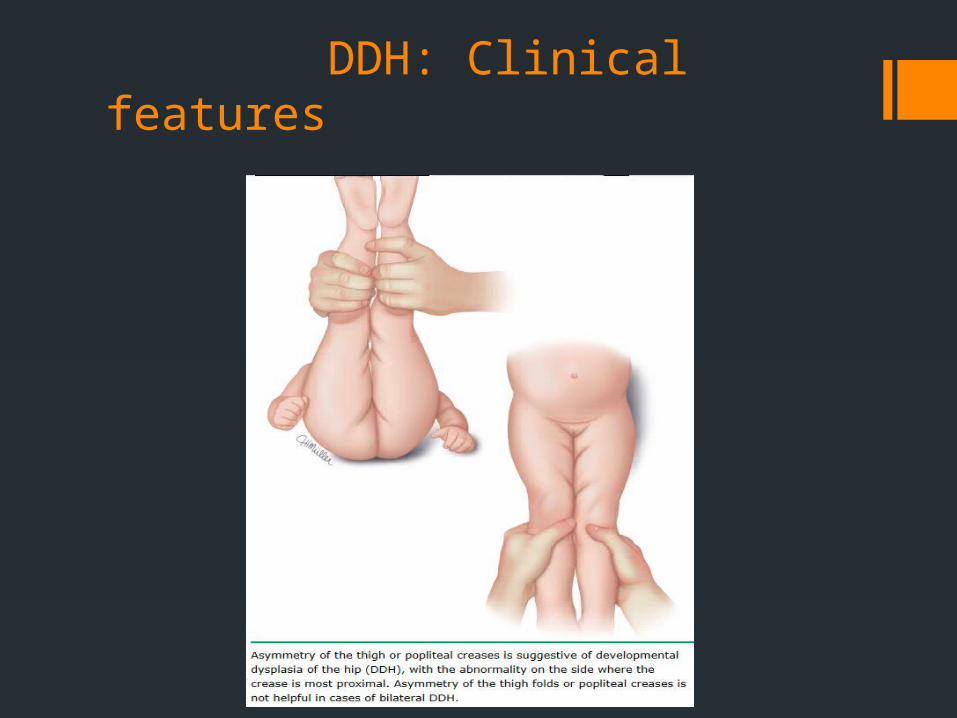
DDH: Clinical features
DDH
Detect hip instability (“jerk” or “clunk”) using adduction and posterior pressure to feel for dislocatability (Barlow’s) and abduction and elevation to feel for reducibility (Ortolani’s).
The American Academy of Pediatrics recommends ultrasound screening at 6 weeks for breech females, breech males (optional), and females with a positive family history of developmental dysplasia of the hip.
Infants and young children who have hip instability on exam (at any age) be referred to an orthopedic surgeon for further evaluation and management
DDH
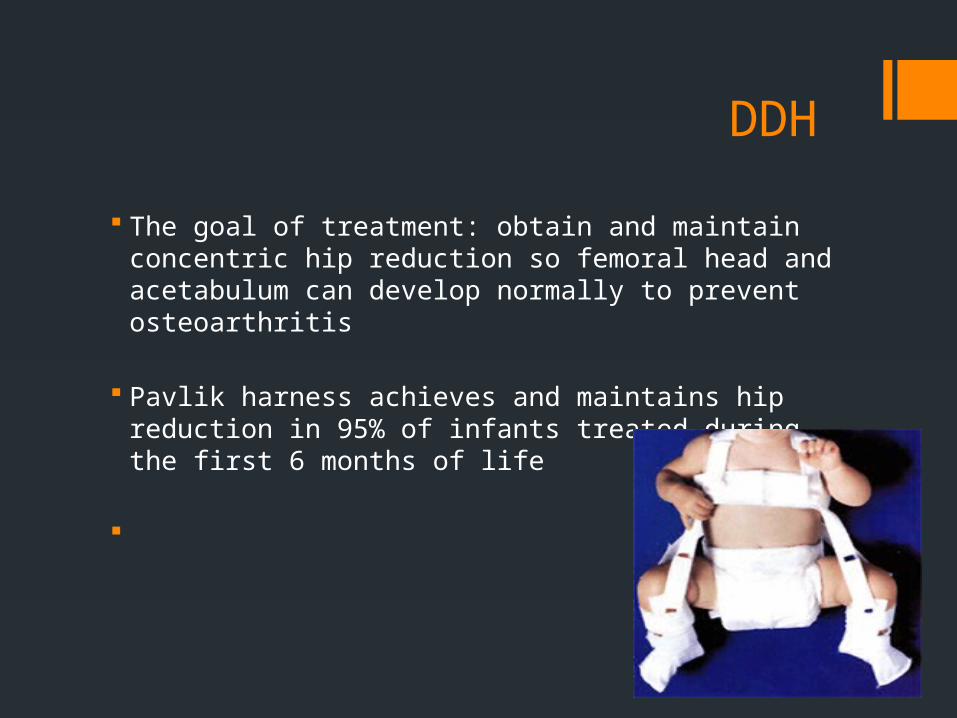
The goal of treatment: obtain and maintain concentric hip reduction so femoral head and acetabulum can develop normally to prevent osteoarthritis
Pavlik harness achieves and maintains hip reduction in 95% of infants treated during the first 6 months of life
DDH
Spica casting / Reduction under anesthesia (closed or open) is usually necessary for children who are older than 6 months of age at the time of diagnosis or initiation of therapy
Children who have been treated for DDH should be monitored with regular hip radiographs until they are skeletally mature to evaluate hip development and complications or sequelae
In toeing

In toeing
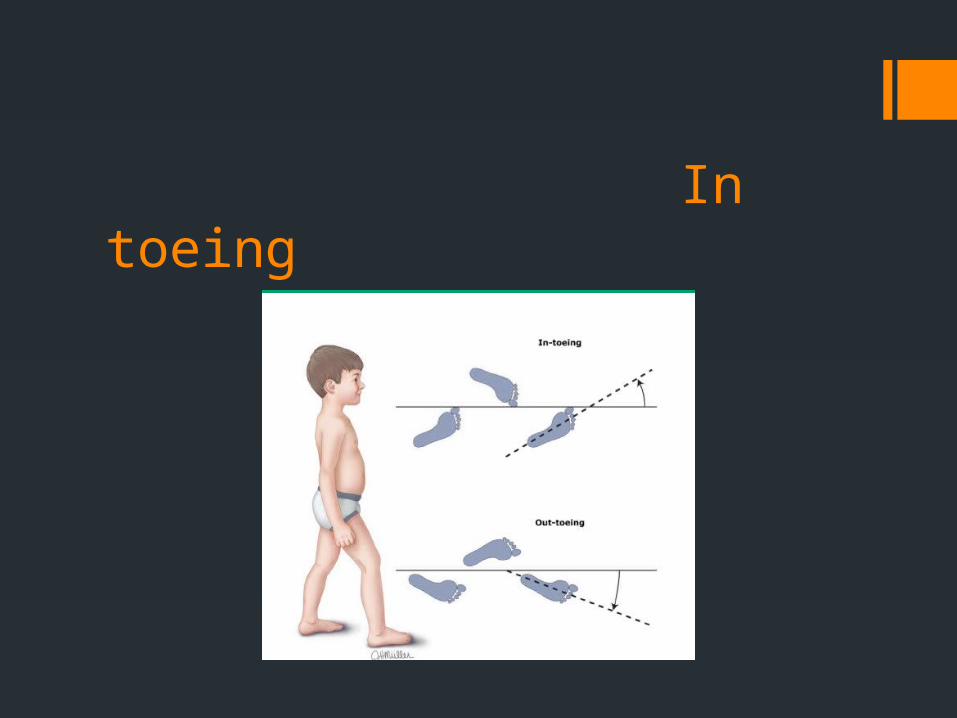
The most common causes of in – toeing in children are metatarsus adductus, internal tibial torsion, and increased femoral anteversion
These rotational variations are related to intrauterine molding and resolve spontaneously through normal growth and development
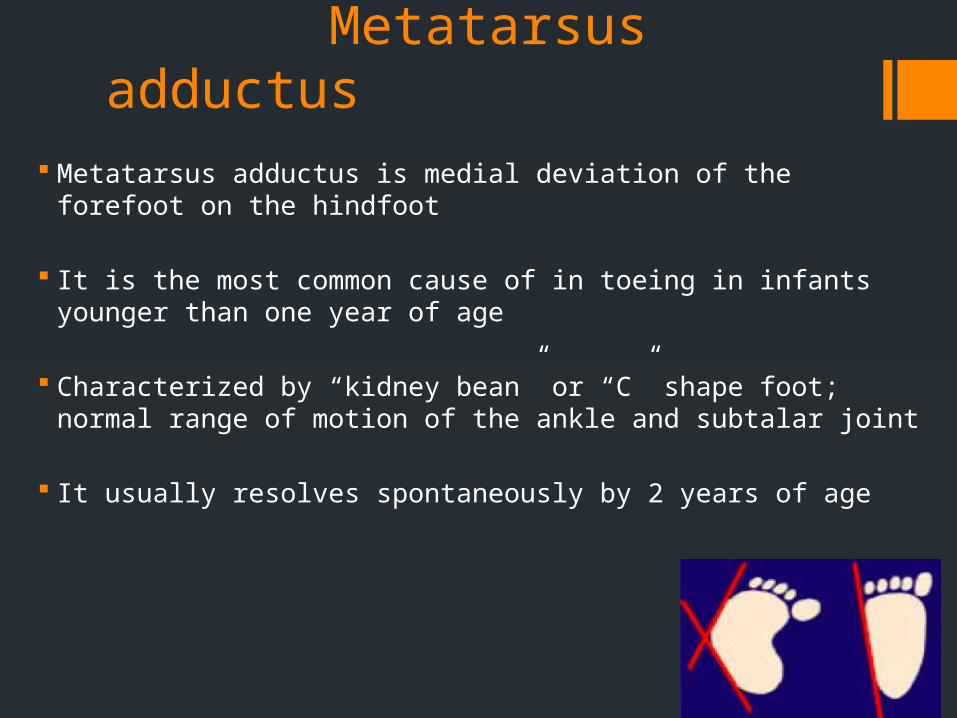
Metatarsus adductus Metatarsus adductus is medial deviation of the forefoot on the hindfoot
It is the most common cause of in toeing in infants younger than one year of age
Characterized by “kidney bean” or “C” shape foot; normal range of motion of the ankle and subtalar joint
It usually resolves spontaneously by 2 years of age
Internal tibial torsion Internal tibial torsion is internal (medial) rotation of the tibia n
relation to the transcondylar axis of the femur
It is the most common cause of in toeing in children between one and three to four years of age
Characterized by a foot that points inward when the patella faces forward
Neutral or internal thigh – foot angle
Internal tibial torsion usually resolves spontaneously by 5 years of age
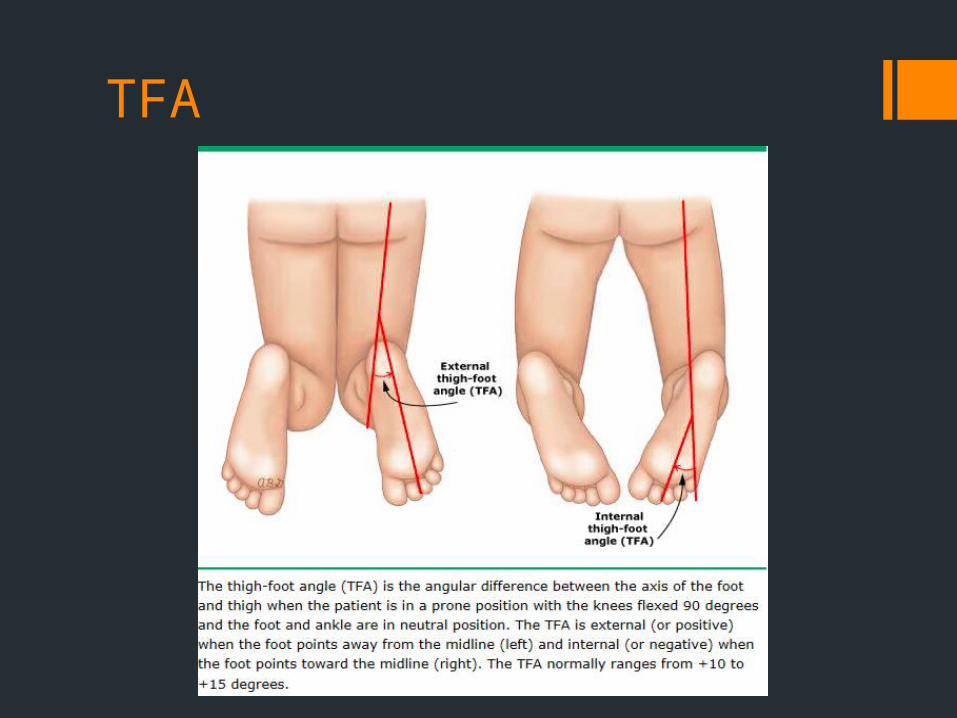
TFA
Increased femoral anteversion
Increased femoral anteversion is an increased angle of rotation of the femoral neck in relation to the transcondylar axis of the femur.
It is the most common cause of in toeing in children older than 3 years of age.
Characterized by inward facing feet and patella during walking and standing “egg – beater” pattern during runningsymmetrically increased internal rotation and decreased external
rotation of the hipspreference for sitting in the “W” position
Tends to improve spontaneously by 11 years of age
“W position” in increased femoral anteversion

In toeing
Most children with rotational variations of the lower extremity can be followed in the primary care office.
Pathologic conditions that must be considered - neuromuscular diseases eg cerebral palsy, disorders of the hip eg DDH, lower leg deformities eg skewfoot, clubfoot
The most important aspect of management of rotational causes of in toeing is parental reassurance that most “deformities” correct spontaneously and that, even in persistent cases, adverse long term sequelae are rare
In toeing Non operative interventions eg shoe inserts, braces, twister
cables, casting are ineffective in the treatment of internal tibial torsion and increased femoral anteversion.
Indications for referral include
rigid metatarsus adductus unilateral or asymmetric in toeing with findings suggestive of
cerebral palsy or developmental dysplasia / dislocation of the hip cosmetically or functionally unacceptable in toeing due to internal
tibial torsion in a child older than 8 years cosmetically or functionally unacceptable in toeing due to
femoral anteversion in a child older than 11 years in toeing that does not follow the expected clinical course
Transient synovitis
Pain and limitation of motion in the hip without clear precipitant (?post traumatic, allergic, infectious).
Relatively common (Cumulative lifetime risk of 3%)
Typically occurs in children aged 3 to 8 years, with a mean age at presentation of 6 years
Male to female ratio is slightly greater than 2:1
Symptoms affect both hips in as many as 5% of cases
Even in symptomatically unilateral disease, ultrasound can detect bilateral effusions in 25% of children
Transient synovitis
Most children have had symptoms for less than a week at the time of presentation and are generally well appearing
Fever is typically absent or low grade
Management is conservative and most children recover quickly with just NSAIDs
A small percentage may go on to develop Legg – Calve – Perthes disease with avascular necrosis of the ipsilateral femoral head
Slipped capital femoral epiphysis
Displacement of the capital femoral epiphysis from the femoral neck through the physeal plate
Mean age of presentation is 12 years in girls and 13.5 years in boys and obesity is a significant risk factor
The classic presentation is that of non radiating, dull, aching pain in the hip, groin, thigh or knee, with no history of preceding trauma
The pain is increased by physical activity and may be chronic or intermittent
There is limited internal rotation of the flexed hip on physical exam
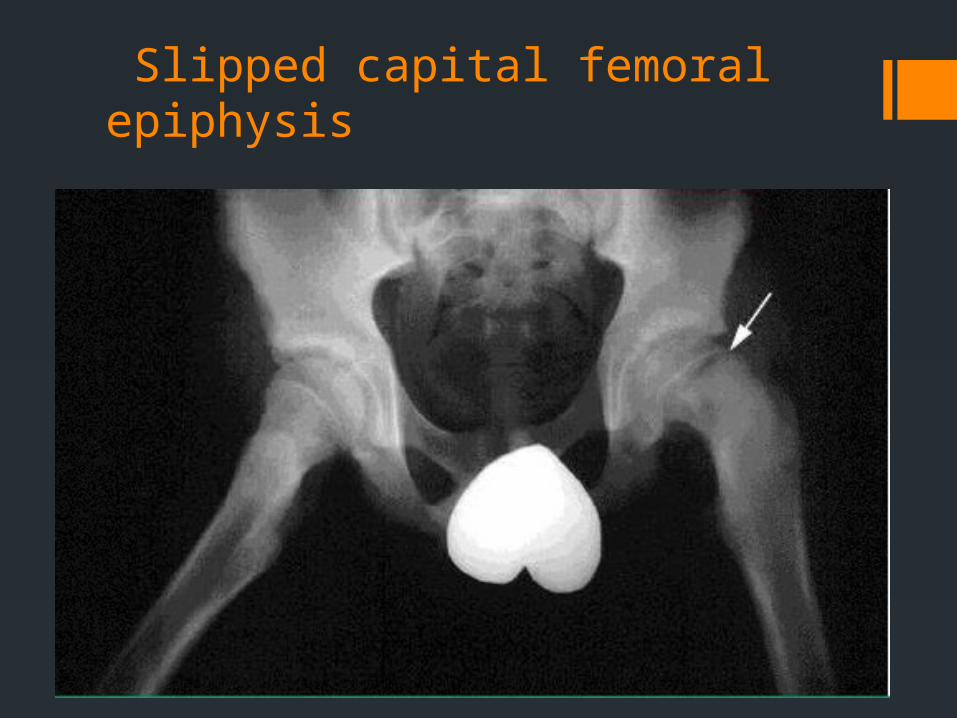
Diagnosis is usually made on plain radiograph, which reveals posterior displacement of the femoral epiphysis, like ice cream slipping off a cone
Slipped capital femoral epiphysis
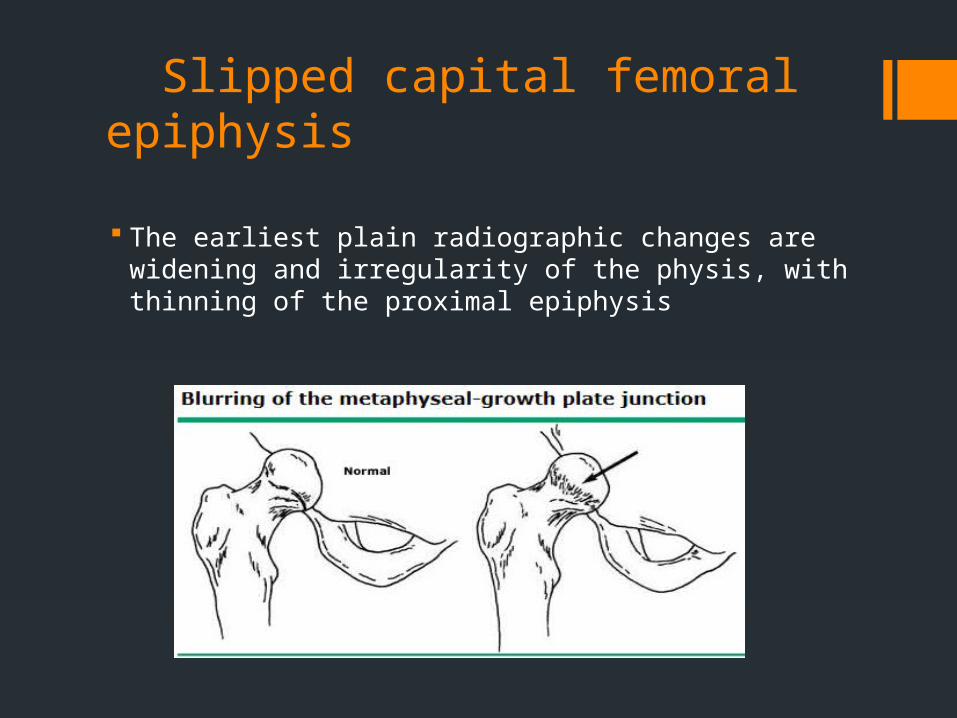
The earliest plain radiographic changes are widening and irregularity of the physis, with thinning of the proximal epiphysis
Slipped capital femoral epiphysis
Slipped capital femoral epiphysis
If the radiograph is normal but suspicion for early SCFE is high, MRI may demonstrate widening of the physis with surrounding edema
All cases of SCFE should be referred for surgical evaluation (avoid weight bearing until surgery)
Approximately 30 to 60% of patients with unilateral SCFE at presentation eventually have SCFE in the contralateral hip
To prevent delay in diagnosis of the second slip, all patients with unilateral involvement should be followed closely by an orthopedic surgeon until after the child has finished growing
The complications of SCFE include osteonecrosis of the femoral head, femoro-acetabular impingement, and chondrolysis
Legg – Calve – Perthes Disease
Syndrome of idiopathic osteonecrosis (avascular necrosis) of the hip
Typically presents as hip pain and / or limp of acute or insidious onset in children between the ages of 3 and 12 years, with peak incidence at 5 to 7 years of age
LCP is bilateral in 10 to 20% of patients; M:F of 4:1 or greater, and African Americans are rarely affected
May occur in association with underlying condition eg renal failure, glucocorticoid use, SLE, HIV, Gaucher’s disease
Legg – Calve – Perthes Disease
The etiology of LCP remains undefined – approx 10% are familial and patients often lag behind their peers in bone age and height
There is insidious onset hip pain, with limping and activity related pain
Diagnosis of LCP demands a high index of suspicion and initial radiographs are often normal
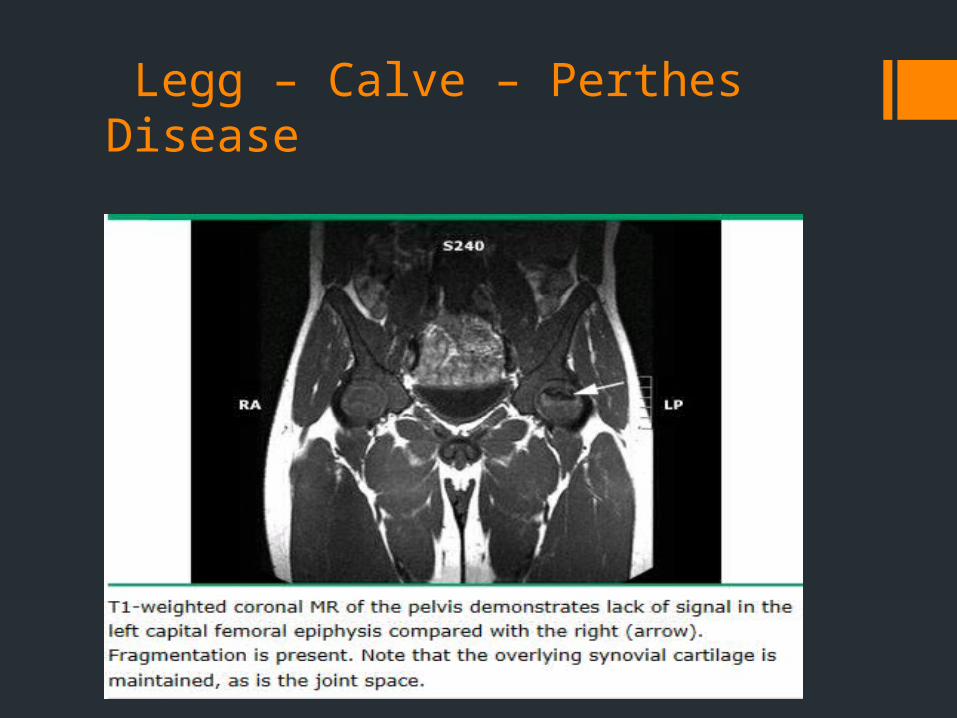
Early in the course, bone scan shows decreased perfusion to the femoral head, and MRI reveals marrow changes highly suggestive of the diagnosis
Later in the course, radiographs show fragmentation and then healing of the femoral head, often with residual deformity
Legg – Calve – Perthes Disease

Legg – Calve – Perthes Disease
Legg – Calve – Perthes Disease
Children diagnosed with LCP should be made non weight bearing and referred to an experienced pediatric orthopedist for management
Treatment focuses on containing the femoral head within the acetabulum through the use of splints or occasionally surgery
Almost all children do well in the short term; however long term outcome depends on age of onset and degree of involvement of the femoral head
Children who are younger than 6 to 8 years years have a better prognosis, perhaps because more time is permitted for femoral remodeling and because before 8 years of age the acetabulum is plastic and can mold to the deformed femoral head, maintaining congruity
Osteochondritis dessicans of the knee
Defined as osteonecrosis of subchondral bone
Specifically, a localized lesion in which a segment of subchondral bone and articular cartilage separates from the underlying bone, leaving either a stable or unstable fragment
Classified as juvenile (open physis) / adult (skeletally mature)
The need for specialty referral primarily depends upon the likelihood that the OCD lesion will not heal with nonoperative therapy
Osteochondritis dessicans of the knee
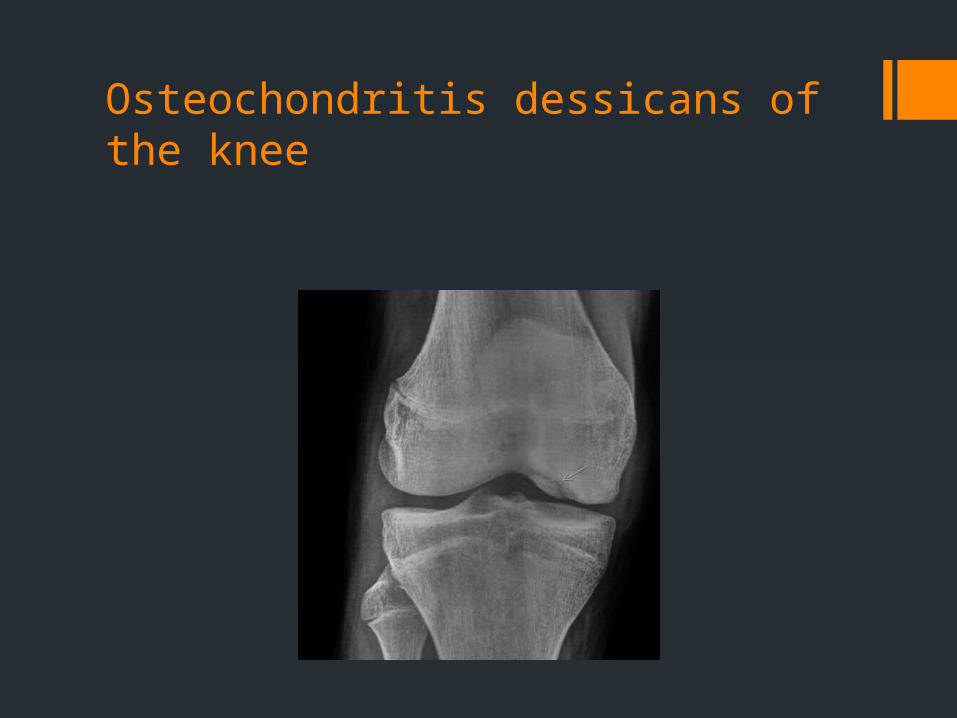
M > F, average age is 10-20 years, bilateral in 30-40%
85% in medial epicondyle & 70% at posterolateral aspect (LAME)
Radiographs as initial test; MRI can demonstrate degree of involvement
Girls < 11 y & boys < 13 y usually do well without surgery if fragment intact
Osteochondritis dessicans of the knee

Kohler’s osteochondrosis
Ages 2–8 years
Boys are 5x more commonly affected than girls
Presents with limp and midfoot pain ± dorsal foot swelling
Tender over the navicular, ± swelling/warmth
Treat in a short leg cast for 8 weeks

Kohler’s osteochondrosis
Freiberg’s osteochondrosis
Disordered ossification of the 2nd MT head
Most common in adolescent girls in dance or ballet
Causes: repetitive stress, trauma, disruption of blood supply
Bilateral in < 10% of cases
Pain, dorsal swelling; tenderness over the metatarsal head
Treat with activity modification, analgesics, ice, metatarsal pads, well-padded shoes

Freiberg’s osteochondrosis

Freiberg’s osteochondrosis
Idiopathic scoliosis
Females more commonly affected
•Prevalence of 0.5-3%
•Infantile idiopathic scoliosis is most likely to spontaneously resolve
•Juvenile idiopathic scoliosis may be considered the most malignant form of scoliosis due to high rates of progression
•Adolescent idiopathic scoliosis is most common
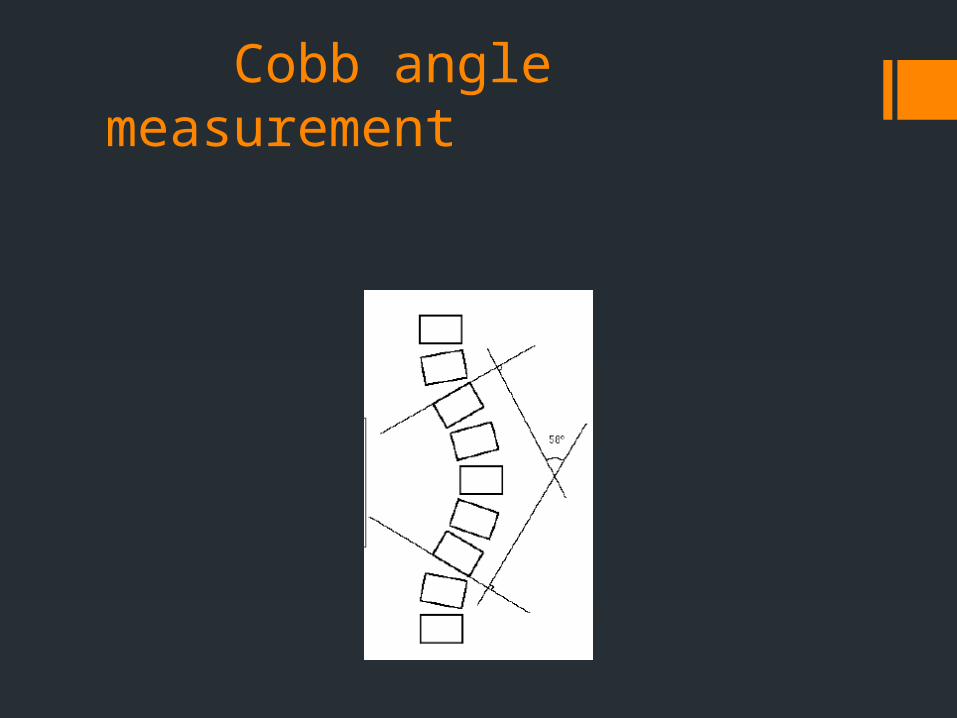
Cobb angle measurement
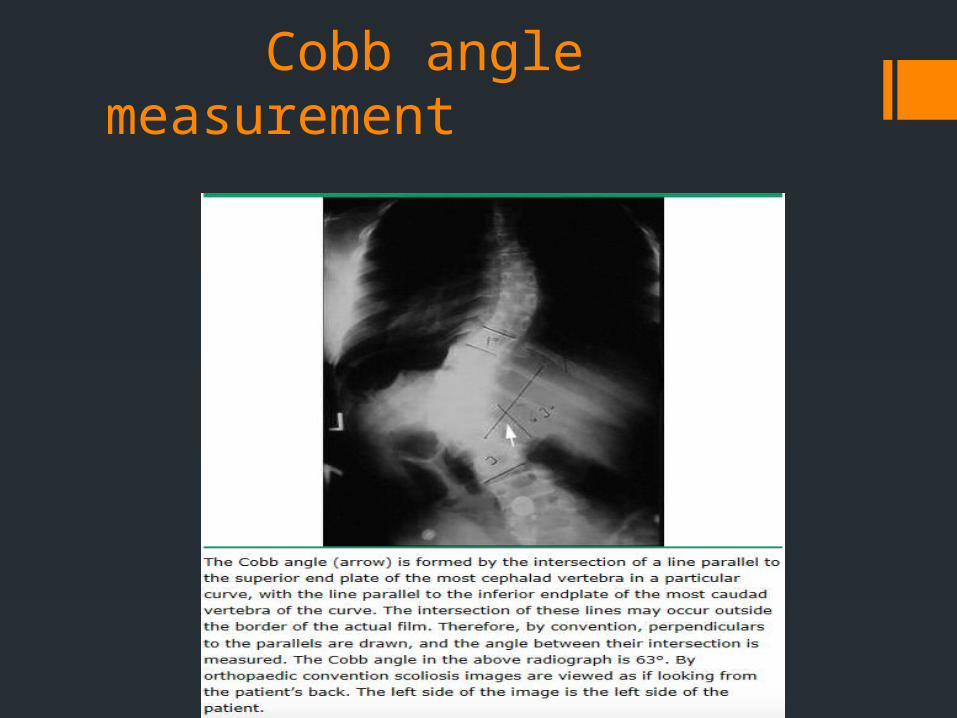
Cobb angle measurement
Adolescent idiopathic scoliosis The goal of the treatment is a curve with a Cobb angle of 40°
or less at skeletal maturity
Options for treatment include observation, bracing and surgery
Indications for referral to orthopedic surgeon may include angle of trunk rotation ≥ 7° inability to obtain a Cobb angleCobb angle between 20 and 29° in premenarcheal girls or boys
aged 12 to 14 yearsCobb angle > 30° in any patient progression of Cobb angle ≥ 5° in any patient
Adolescent idiopathic scoliosis
Surgery for patients with Cobb angle ≥ 50° at the time of presentation or later, regardless of the degree of skeletal maturity
Indications for bracing: Cobb angle 20 – 29° with substantial growth remaining and the
Cobb angle increases by ≥ 5% over a 3 to 6 month period Cobb angle 30 to 40° with substantial growth remaining
If decision is taken for just observation (Cobb angle less thsn 20°), get radiographs every 6 to 9 months (only necessary if patient is skeletally immature).
Traction apophysitis
Insidious onset that results from injury or overuse of the tendon and surrounding ossification centers
Boys are more commonly affected and symptoms generally appear between 10 to 14 years of age
Often occurs at or after growth spurt
Physical activity required
Principles of rehab include ice, stretching, and modification to activity (relative rest).
Little league elbow
Little league elbow
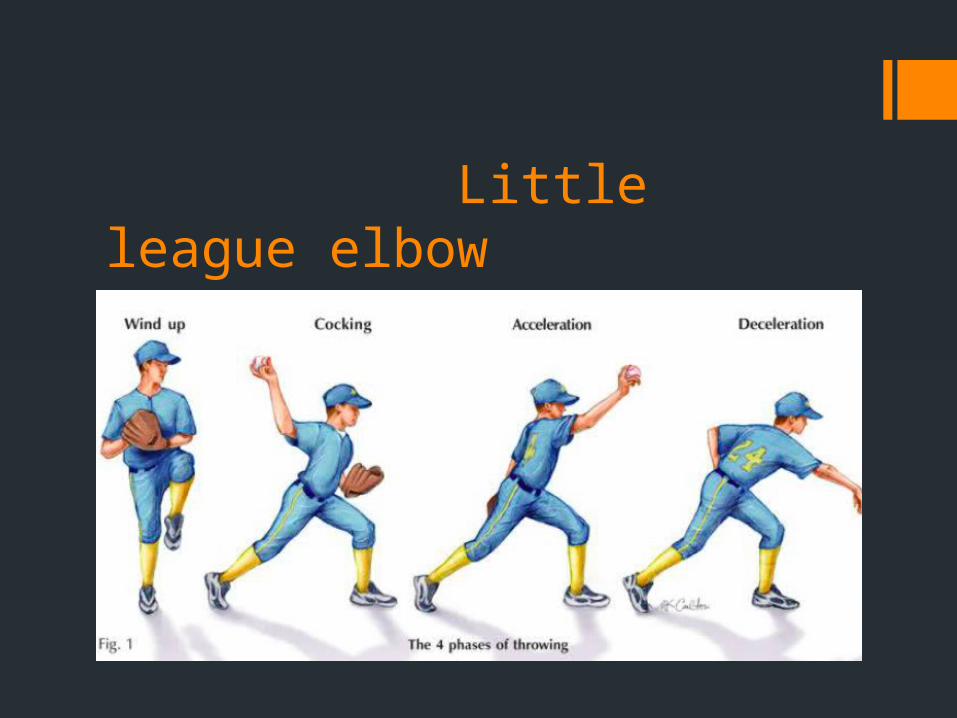
Descriptive term for a group of elbow problems related to the stress of throwing in young athletes
Throwing can cause medial symptoms as well as lateral and posterior symptoms
The medial symptoms are related to the repetitive valgus distraction forces on the medial elbow
Microtrauma from overuse or improper throwing mechanics (opening up too soon so the throwing arm trails behind the trunk rotation) can cause injury
Clinical features: Progressive medial elbow pain, diminished throwing effectiveness and decreased throwing distance
Rx: Refrain from throwing for 3 to 6 weeks until pain free and non tender then progressive return to throwing program
Ddx of heel pain in children
Osgood – Schlatter disease Sever’s calcaneal apophysitis Plantar fasciitis Painful heel pad syndrome Calcaneal apophyseal fracture or calcaneal stress fracture Calcaneal osteomyelitis Bone tumors Unicameral (simple) bone cyst Spondyloarthropathy Tarsal tunnel syndrome (specifically medial calcaneal
branch)
Osgood – Schlatter’s disease An overuse injury caused by repetitive strain and chronic
avulsion of the secondary ossification center of the tibial tubercle
Occurs most frequently in participants of sports that involve running and jumping and who have recently undergone a rapid growth spurt
The most common presenting complaint is anterior knee pain that increases gradually over time
The pain is exacerbated by direct trauma, kneeling, running, jumping, squatting, climbing stairs, or walking uphill, and is relieved by rest
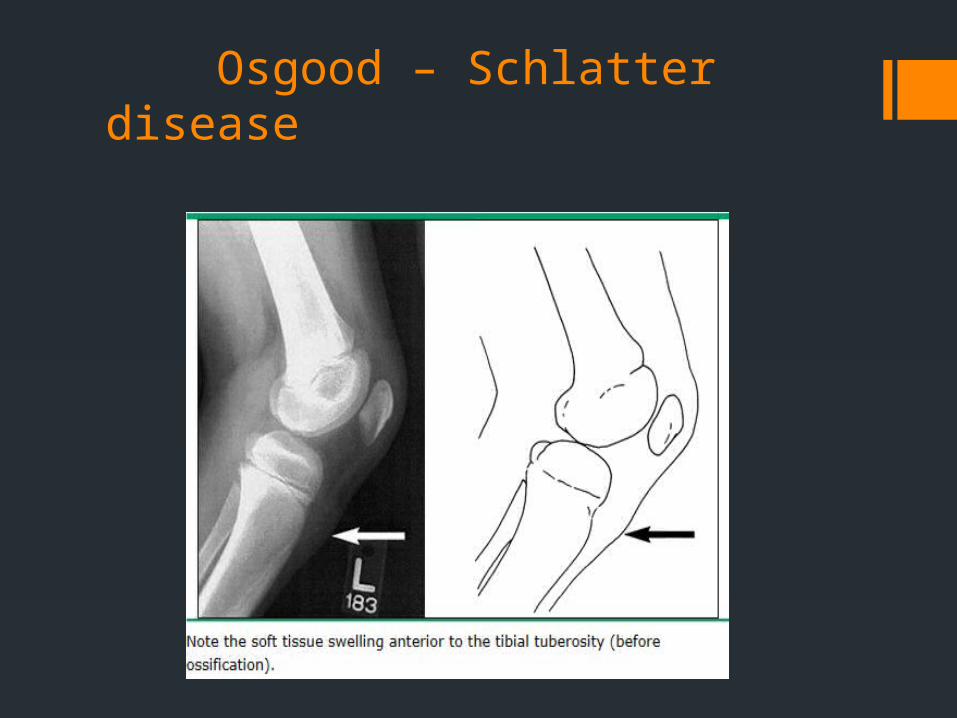
Osgood – Schlatter’s disease Diagnosis is clinical – tenderness and soft tissue or bony
prominence of the tibial tubercle in a patient with an otherwise normal examination (including ROM of the hip)
Imaging is not necessary to confirm the diagnosis but may be necessary to exclude other conditions in patients with atypical complaints, such as
pain at night rest – related pain acute onset of pain (especially after trauma) associated systemic complaints pain that is not directly over the tibial tubercle
Usually a benign and self limited condition; symptoms resolve once growth plate ossifies
Osgood – Schlatter disease
Osgood – Schlatter’s disease
Therapy is conservative – ice, NSAIDs, activity continuation, physical therapy
Patients with persistent pain that alters their ability to participate in sports for more than 3 months may benefit from injection of hyperosmolar dextrose by a sports med specialist or orthopedic surgeon
Patients who have pain that persists after closure of the proximal tibial growth plate and is related to bony or cartilaginous ossicles may benefit from surgical excision
Complications and sequelae of Osgood – Schlatter dz include persistent prominence of the tibial tubercle persistent pain (usually secondary to residual ossicle)genu recurvatum
Sever’s calcaneal apophysitis
Common cause of heel pain in young athletes, particularly those who play soccer and basketball or participate in gymnastics or track / running.
The mean age of presentation is 8 to 12 years; boys are affected more often than are girls; bilateral in 40 to 61% of cases
Inflammation of the calcaneal apophysis (growth plate at the insertion of the Achilles tendon)
The characteristic history is one of chronic heel pain related to activity and insidious in onset
Physical exam – decreased gastrocnemius – soleus flexibility; approximately 25% of patients have a flat foot or rigid foot alignment

Sever’s calcaneal apophysitis
Heel pain may be reproduced by direct digital palpation over the apophysis or the calcaneal compression test (hold affected heel in palm with the fingers enveloping the upper portion of the heel and then squeeze to compress the heel in the transverse plane)
Radiographs are not required to make the diagnosis but should be obtained to exclude other disorders if the presentation is atypical
Plain radiographs are usually normal early and may only show sclerosis and widening of the growth plate; late findings – calcaneal fragmentation
MRI is more sensitive to identify stress related changes in the calcaneal metaphysis and is only indicated in severe / chronic cases or those that do not respond to routine management
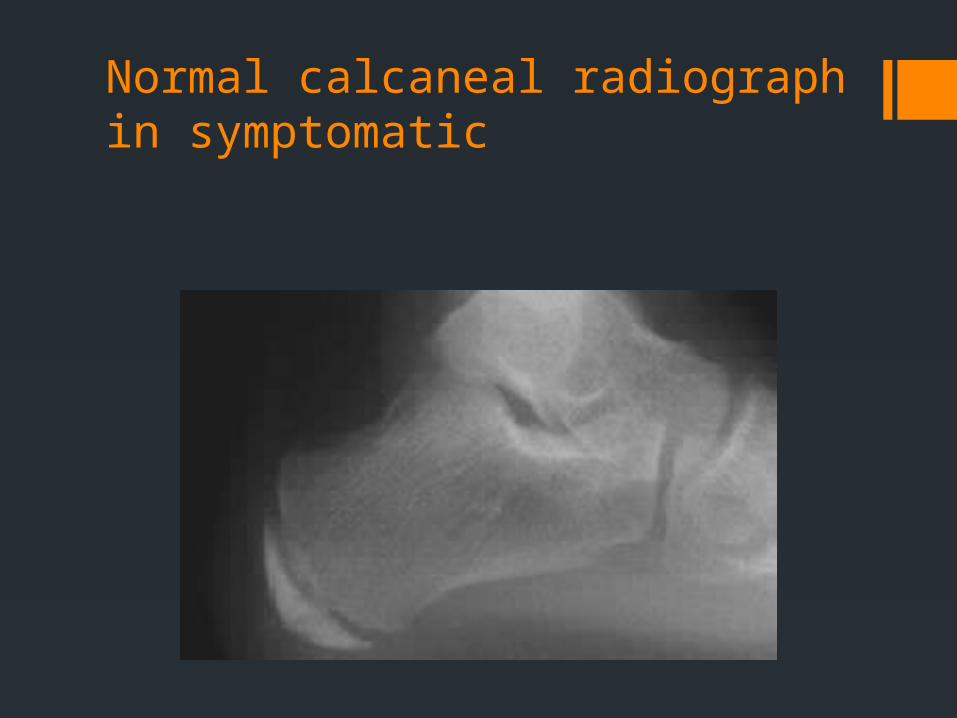
Normal calcaneal radiograph in symptomatic

Fragmentation demonstrated late in symptomatic child
Sever’s disease: Treatment
Decrease stress on the apophysis; daily icing for 20 minutes even after symptoms have began to improve
Stretch gastrocnemius – soleus complex
Use of heel cup or one fourth inch heel lift, and use of proper foot wear
NSAIDs may be helpful for pain control during early management but should not be used before exercise or to increase the amount of activity the athlete can tolerate
For the compliant patient whose symptoms fail to improve within 4 to 8 weeks, short term (3 to 4 weeks) short leg casting may help to resolve painful symptoms related to stress associated bone changes
Physical therapy and slow progressive return to activity are important to recovery
Iselin’s disease
Painful inflammatory condition of the apophysis (growth plate) of the 5th metatarsal
Seen in physically active boys and girls between the ages of 8 and 13 years of age
Most common in those that participate in soccer, basketball gymnastics and dance
An overuse injury caused by repetitive pressure and/or tension on the growth center at the base of the fifth metatarsal

Iselin’s disease
Iselin’s disease
Pain is most commonly found along the outer edge of the foot and is worsened with activity and improved with rest
A limp on the affected side may be present
The child may walk on the inside of the affected foot
The skin overlying the growth center may be swollen, red, and/or painful to touch
Diagnosis is primarily clinical
Radiographs are usually not needed to diagnose the disease, but they may prove useful in assessing for displacement of the growth center and excluding other causes of foot pain
Iselin’s disease A short period of rest from aggravating activities to reduce
inflammation and allow release of pressure on the growth center is recommended
NSAIDs / Applying ice for 10 to 15 minutes every 2 to 3 hours is helpful to reduce pain and swelling
Tension on the growth plate can be relieved by gentle stretching of the calf muscles
Proper fitting shoes and/or arch support inserts are helpful in decreasing pain
If the individual fails a trial of stretching, rest, ice, and pain medications, the affected limb may be immobilized with a walking cast or boot
Healing typically takes anywhere between 4-12 weeks
Benign nocturnal limb pain of childhood (Growing pains)
Bilateral lower extremity pain awakening a child at night (or from naps) who is otherwise without any manifestation of musculoskeletal problems
Etiology is unknown; occurs in 15% of children; Affects 35% of kids 4 to 6 years of age (may present up to age 19 years)
Workup only indicated if child appears ill, complains of pain during the day or with activity, or if pain worsens or persists
Treatment is symptomatic and must include education and reassurance;
Warm baths, heat, massage, mild exercise / analgesics prior to bed have been shown to be helpful
Fracture patterns in children
Buckle (torus) fractures
Plastic deformation
Greenstick fracture
Physeal (growth plate) fracture
Apophyseal avulsion
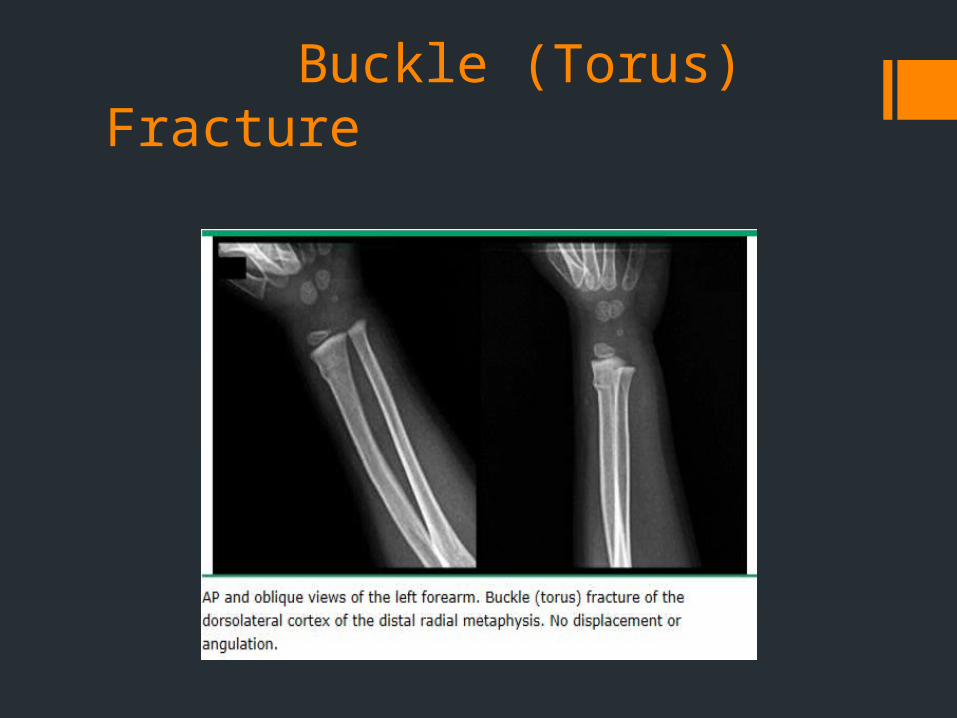
Buckle (Torus) Fracture
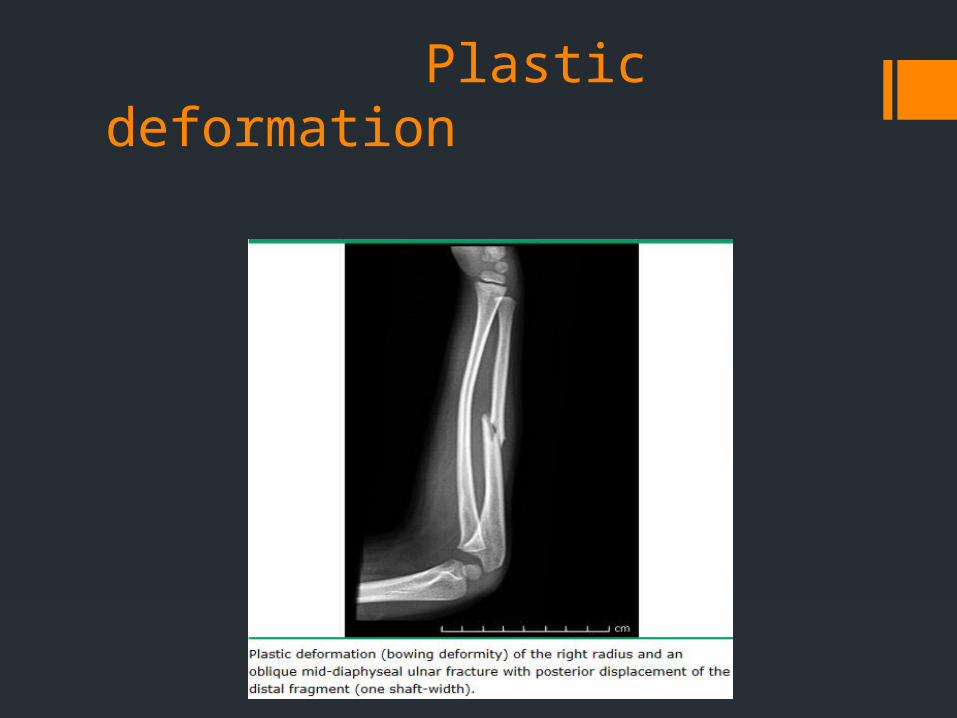
Plastic deformation

Greenstick fracture
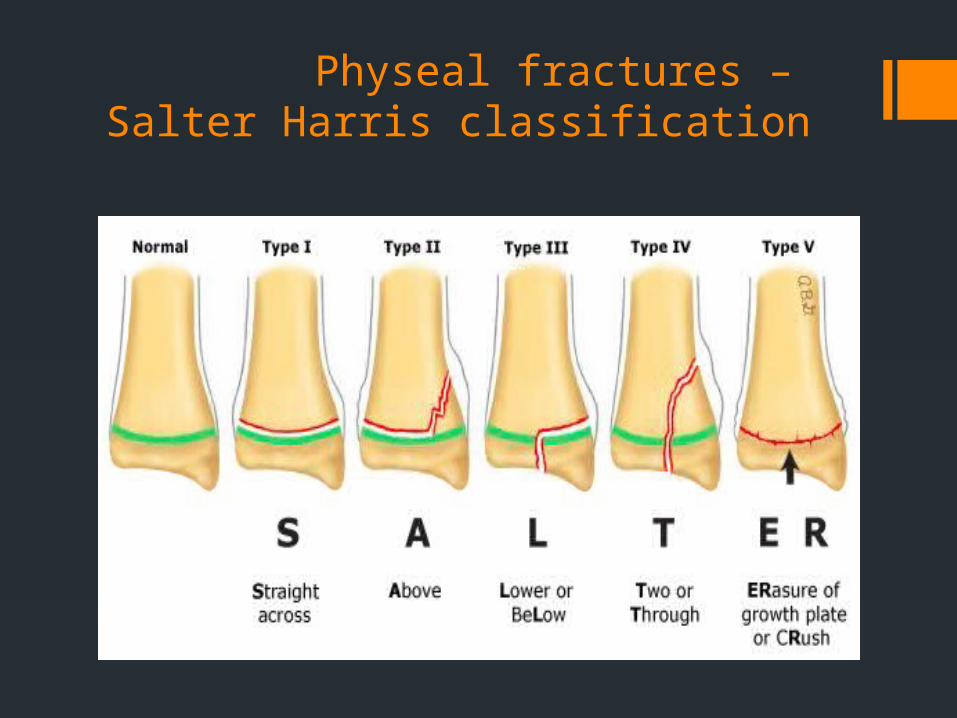
Physeal fractures – Salter Harris classification
Board Review 1/7
A 4-year-old male is brought to your office by his parents who are concerned that he is increasingly “knock-kneed.” His uncle required leg braces as a child, and the parents are worried about long-term gait abnormalities. On examination, the patient’s knees touch when he stands and there is a 15° valgus angle at the knee. He walks with a stable gait. Which one of the following should you do now?
A) Refer to orthopedics for therapeutic osteotomy B) Refer to physical therapy for customized bracing C) Prescribe quadriceps-strengthening exercises D) Provide reassurance to the patient and his family

ANSWER: D
This case is consistent with physiologic genu valgus, and the parents should be reassured. Toddlers under 2 years of age typically have a varus angle at the knee (bowlegs). This transitions to physiologic genu valgus, which gradually normalizes by around 6 years of age. As this condition is physiologic, therapies such as surgical intervention, special bracing, and exercise programs are not indicated.
Board review 2/7
A 2-week-old female is brought to the office for a well child visit. The physical examination is completely normal except for a clunking sensation and feeling of movement when adducting the hip and applying posterior pressure. Which one of the following would be the most appropriate next step?
A) Referral for orthopedic consultation B) Reassurance only, and follow-up in 2 weeks C) Triple diapering and follow-up in 2 weeks D) A radiograph of the pelvis
ANSWER: A
Developmental dysplasia of the hip encompasses both subluxation and dislocation of the newborn hip, as well as anatomic abnormalities. It is more common in firstborns, females, breech presentations, oligohydramnios, and patients with a family history of developmental dysplasia. Experts are divided as to whether hip subluxation can be merely observed during the newborn period, but if there is any question of a hip problem on examination by 2 weeks of age, the recommendation is to refer to a specialist for further testing and treatment. Studies show that these problems disappear by 1 week of age in 60% of cases, and by 2 months of age in 90% of cases. Triple diapering should not be used because it puts the hip joint in the wrong position and may aggravate the problem. Plain radiographs may be helpful after 4–6 months of age, but prior to that time the ossification centers are too immature to be seen. Because the condition can be difficult to diagnose, and can result in significant problems, the current recommendation is to treat all children with developmental dysplasia of the hip. Closed reduction and immobilization in a Pavlik harness, with ultrasonography of the hip to ensure proper positioning, is the treatment of choice until 6 months of age. The American Academy of Pediatrics recommends ultrasound screening at 6 weeks for breech females, breech males (optional), and females with a positive family history of developmental dysplasia of the hip. Other countries have recommended universal screening, but a review of the literature has not shown that the benefits of early diagnosis through universal screening outweigh the risks and potential problems of overtreating.
Board review 3/7
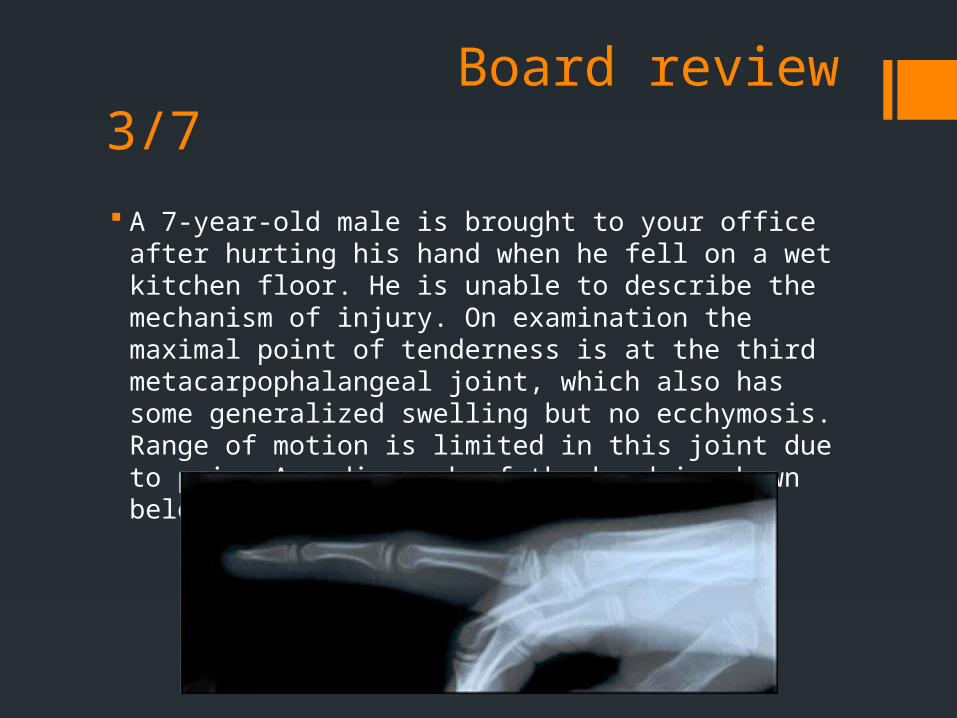
A 7-year-old male is brought to your office after hurting his hand when he fell on a wet kitchen floor. He is unable to describe the mechanism of injury. On examination the maximal point of tenderness is at the third metacarpophalangeal joint, which also has some generalized swelling but no ecchymosis. Range of motion is limited in this joint due to pain. A radiograph of the hand is shown below:
Which one of the following is the most likely diagnosis?
A) Boxer’s fracture B) Greenstick fracture C) Salter-Harris type II fracture D) Spiral fracture E) No abnormality
Board review 4/7
A 7-year-old female is brought to your office with a complaint of right hip pain and a limp with an insidious onset. There is no history of injury or repetitive use. Her vital signs are within normal limits and she has no history of fever or chills or other systemic symptoms. On examination you note that she cannot fully abduct her hip and she winces with pain on internal rotation. A FABER test is normal. Her right leg is 2 cm shorter than the left. Plain films reveal flattening and sclerosis of the proximal femur with joint space widening.
What is the most likely diagnosis in this patient? A) Iliopsoas bursitis B) Labral tear C) Legg-Calvé-Perthes disease D) Septic arthritis E) Stress fracture
ANSWER: C
Legg-Calvé-Perthes disease results from interruption of the blood supply to the still-growing femoral head. It occurs in children 2–12 years of age and presents with hip pain and an atraumatic limp. Common physical findings include leg-length discrepancies, and limited abduction and internal rotation. Radiographs reveal sclerosis of the proximal femur with joint space widening. MRI confirms osteonecrosis. Septic arthritis also causes atraumatic anterior hip pain but occurs in the acutely ill, febrile patient. A CBC, erythrocyte sedimentation rate, C-reactive protein level, and guided hip aspiration are recommended if septic arthritis is suspected. A diagnosis of stress fracture should be considered in patients with a history of overuse and weight-bearing exercise. These patients have pain that is worse with activity, and pain on active leg raising. MRI can detect fractures not seen on plain films. Iliopsoas bursitis presents with snapping or popping of the hip on extension from a flexed position. Labral tears present with sharp anterior hip pain at times, with radiation to the thigh or buttock. Usually patients will have mechanical symptoms such as clicking with activity. The FABER (flexion, abduction, external rotation) and FADIR (flexion, adduction, internal rotation) impingement tests are sensitive for labral tears.
Board review 5/7 During a preparticipation examination of a 5-year-old male for
summer soccer camp, his mother states that he frequently awakens during the night with complaints of cramping pain in both legs, and that he seems to experience this after a day of heavy physical activity. She says that she has never noticed a definite limp. A physical examination of the hips, knees, ankles, and leg musculature is entirely normal. Which one of the following would be the most appropriate next step in the evaluation and management of this patient?
A) Reassurance, with no activity restrictions or treatment B) Recommending that he not participate in running sports C) Plain films of both hips and knees D) Serum electrolyte levels E) Referral to a pediatric orthopedist
ANSWER: A
Benign nocturnal limb pains of childhood (growing pains) occur in as many as one-third of children, most often between 4 and 6 years of age. The etiology is unknown, but the course does not parallel pubescent growth, as would be expected if bone growth were the source of the pain. Pain often awakens the child within hours of falling asleep following an active day. It is generally localized around the knees, most often in the shins and calves, but also may affect the thighs and the upper extremities. A characteristic history coupled with a normal physical examination will confirm the diagnosis. Reassurance that no additional tests or treatments are necessary and that the condition is self-limiting is the most appropriate response.
Board review 6/7
A 3-year-old male is carried into the office by his mother. Yesterday evening he began complaining of pain around his right hip. Today he has a temperature of 37.6°C (99.7°F), cries when bearing weight on his right leg, and will not allow the leg to be moved in any direction. A radiograph of the hip is normal. Which one of the following would be most appropriate at this time?
A) A CBC and an erythrocyte sedimentation rate B) A serum antinuclear antibody level C) Ultrasonography of the hip D) MRI of the hip E) In-office aspiration of the hip

ANSWER: A
This presentation is typical of either transient synovitis or septic arthritis of the hip. Because the conditions have very different treatment regimens and outcomes, it is important to differentiate the two. It is recommended that after plain films, the first studies to be performed should be a CBC and an erythrocyte sedimentation rate (ESR). Studies have shown that septic arthritis should be considered highly likely in a child who has a fever >38.7°C (101.7°F), refuses to bear weight on the affected leg, has a WBC count >12,000 cells/mm3, and has an ESR >40 mm/hr. If several or all of these conditions exist, aspiration of the hip guided by ultrasonography or fluoroscopy should be performed by an experienced practitioner. MRI may be helpful when the diagnosis is unclear based on the initial evaluation, or if other etiologies need to be excluded.
Board review 7/7 A 13-year-old male presents with a 3-week history of left lower
thigh and knee pain. There is no history of a specific injury, and his past medical history is negative. He has had no fevers, night sweats, or weight loss, and the pain does not awaken him at night. He tried out for his school’s basketball team but had to quit because of the pain, which was worse when he tried to run. Which one of the following physical examination findings would be pathognomonic for slipped capital femoral epiphysis?
A) Excessive forward passive motion of the tibia with the knee flexed
B) Lateral displacement of the patella with active knee flexion C) Limited internal rotation of the flexed hip D) Reduced hip abduction with the hip flexed E) An inability to extend the hip past the neutral position
ANSWER: C
Slipped capital femoral epiphysis (SCFE) typically occurs in young adolescents during the growth spurt, when the femoral head is displaced posteriorly through the growth plate. Physical activity, obesity, and male sex are predisposing factors for the development of this condition. There is pain with physical activity, most commonly in the upper thigh anteriorly, but one-third of patients present with referred lower thigh or knee pain, which can make accurate and timely diagnosis more difficult. The hallmark of SCFE on examination is limited internal rotation of the hip. Specific to SCFE is the even greater limitation of internal rotation when the hip is flexed to 90°. No other pediatric condition has this physical finding, which makes the maneuver very useful in children with lower extremity pain. Orthopedic consultation is advised if SCFE is suspected. Hip extension and abduction are also limited in SCFE, but these findings are nonspecific. Displacement of the patella is not associated with SCFE.