Embed Size (px)
Citation preview

Pediatric Otolaryngology for Anesthetistsfollowed by the delightful
Airway Disorders in Infants and Children
Andrew M. Shapiro, MDPrivate Practice, Pediatric Otolaryngology
Clinical Associate Professor of SurgeryPennsylvania State University College of Medicine

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
What does a pediatric otolaryngologist do?
Inflammatory, congenital and neoplastic disorders involving the head and neck
Simple surgeries in fairly healthy kids Big surgeries in fairly healthy kidsSimple surgeries in sick kidsBig surgeries in sick kids
Ear surgeryNasal and sinus surgeryAirway surgeryPharyngeal surgeryCraniofacial surgeryTumors and congenital anomalies of the head and neck

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
OrganizationEmphasize that there are distinct qualities required when caring for childrenUnderstand the anesthetic implications of otolaryngologic surgeryUnderstand special situations and patient circumstancesReview significant ENT airway conditions

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Characteristics of pediatric anesthesia
Laryngospasm, bronchospasm, concurrent illnessesPhysiologic differences
Higher metabolic rate↑O2 requirementTemperature management
↓Chest wall complianceHigh closing volumes
Evolving psychological status must be appreciated from neonates to adolescentsDental

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Characteristics of Pediatric Otolaryngology Patients
“Healthy” PedENT patients are often “sick” on the day of surgery
Congestion, runny nose, cough“a case cancelled is not a case done”
“Sick PedENT patients tend to have chronic lung disease from prematurity, aspiration, cystic fibrosis, or reactive airway disease

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Points of convergenceThe surgeon and the anesthetist are a TEAM (and I’m not just saying that!)Maintain good surgical access while preserving the ability to sustain ventilation (or vice versa)

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Otologic CasesMyringotomy and tube insertions
Most common procedure under GA Mask anesthetic
Older children may benefit from IV/LMAPremed? Narcotic?
Tympanoplasty/tympanomastoidectomyNo muscle relaxant during procedureNo nitrous oxideSecure tubes and IV’s; lots of “turning” during case

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Nasal and Paranasal sinus surgeryExpect secretions and bloodExpect a generous helping of vasoconstrictors
Control blood pressureExpect a “touchy airway”

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Anatomic ClassificationSupraglottic
NoseChoanal atresiaNOWCA
Craniofacial DysmorphologyPierre Robin SyndromeTreacher collinsApertsCrouzonsMoebius
MacroglossiaBeckwith WiedemannSyndromeDown’s Syndrome
TumorsHemangiomaNeuroblastoma
Laryngomalacia Glottic
Vocal cord paralysisTumors and cysts
• Laryngoceles• Papillomatosis• Cystic hygroma• Laryngoceles
AtresiaWebs
SubglotticStenosisWebsAtresiaTumors
HemangiomaCystic HygromaCysts
TracheaTracheomalaciaStenosisCystAtresia
ExtrinsicGoiterVascular RingHemangiomaCystic hygromaTeratomaMediastinal masses

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
IntroductionThe Pediatric Airway
AnatomyNasal/Pharyngeal
Obligate Nosebreathing
LaryngealSupraglottisGlottisSubglottis
• Cricoid
Upper trachea

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
The Nose and PharynxAnatomy
Nasal Cavities Pharynx
NasopharynxOropharynxHypopharynx

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Obligate Nosebreathing

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Obstruction at the Pharyngeal LevelStertor (vs. stridor)Often worst when asleepOften improved by positioning
Neck extension, sniffing position

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Tonsils and adenoidsChronic tonsillitisTonsillar hyperplasia
OSA 2% incidence. 10%SDBPeaks 2-5 years oldSecond peak in adolescenceMedical treatment
Weight lossManagement of infection
CPAPSurgical therapy
T/A, UPPPHighly effective in “normal” children

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
T & A: techniques
Tonsillectomy“Cold”
GuillotineDissection and snareMicrodebrider
“Hot”CauteryBipolar cauteryLaserCoblation
AdenoidectomyCuretteCauteryMicrodebrider
Adjunctive measuresSteroidsLocal AnestheticsAnalgesicsAntibioticsAntiemetics

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Higher risk tonsillectomy
Age < 3 yearsDocumented profound OSANeuromuscular disordersChromosomal anomaliesCraniofacial/airway disordersRecent upper respiratory infectionBleeding disorderActive infection or peritonsillar abscessSevere obesity

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Upper airway obstruction in neurologically impaired children
Hypotonia reduces predictability of T&AReasonable approach if significant adenotonsillar hypertrophy is presentUPPP? Kershner et al int J ped oto 2002
tracheotomy vs. salivary diversion, laryngeal diversion, supraglottoplasty, midfacial and maxillary advancementsBiPAP/CPAP
Increased perioperative morbidityIndividualized treatment - no reasonable studies to clearly delineate best treatment options

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Postoperative problems can be minimized by anesthetic techniques
ApneaLaryngospasmPostobstructive pulmonary edemaBleeding
Judicious narcoticsLocal anesthetic
Steroids/AntiemeticsPropofolTiming of extubationImmediate gentle positive pressure

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Now, the real reason I’m here…

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
IntroductionThe Pediatric Airway
AnatomyNasal/Pharyngeal
Obligate Nosebreathing
LaryngealSupraglottisGlottisSubglottis
• Cricoid
Upper trachea

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
StridorDefinition
Distinguish from stertorCauses
LaryngomalaciaVocal cord paralysisSubglottis stenosis

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
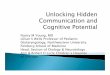
Cross Sectional Airway Diameter
Adult1mm edema = 81% of normal area
Term Newborn1mm edema = 44% of normal area
20mm
5mm

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Clinical presentationFailed extubation attempts in NICUStridorRecurrent croupProgressive respiratory failure with stridorFeeding difficultiesFailure to thrivePersistent coughTracheotomy

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
EvaluationHistory
Details of extubation attemptsPresence, absence, and characteristics of stridor
Onset/Progression Impact of position
Nature of cryFeeding abnormalitiesPrior airway interventionsCardiopulmonary statusTerm or prematureApgarBirth weight/weight gainOther medical problems
Physical examinationImagingEndoscopy

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
EvaluationHistory
Physical examinationComplete head and neck examination
Craniofacial disorders, retrognathia, nasal obstruction, laryngomalacia, vocal cord paralysis
Body HabitusDegree of dyspneaQuality of stridor
Changes with position, activityCry/VoiceAuscultation of chest
ImagingEndoscopy

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
EvaluationHistoryPhysical examination
ImagingHi KV AP and Lateral plain filmsAirway flouroscopy/Barium SwallowMRI in patients with suspected vascular/mediastinal pathologyEndoscopy

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
EvaluationHistoryPhysical examinationImaging
EndoscopyFlexible
Need for sedation and inability to control airway and ventilation Useful for proximal airway evaluation at bedside or as outpatientDistal airway evaluation in intubated patients
RigidSpontaneous ventilationMicrolaryngoscopy
• Webs, glottic scarring, interarytenoid adhesions, fixation or paralysisSubglottis
• Size, maturity, length, stomal siteRemainder of tracheobronchial treeSizing of airway

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Airway Endoscopy-Stages1. Preparation and
Communication a) Equipmentb) Monitoring
2. Induction3. Diagnostic Laryngoscopy and
topical anesthetic4. Diagnostic Suspension
laryngoscopyControlled airway for microscopy or bronchoscopy
and Diagnostic Bronchoscopy5. Therapeutic intervention

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Anesthesia for airway endoscopyClear communication essentialAvoid jet in young childrenTechniques
Apneic techniqueSpontaneous ventilation in young children
Topical anesthetic?In older children (5 -10 years) relaxant with controlled ventilation
NEVER ABOLISH SPONTANEOUS RESPIRATION UNLESS AN ALTERNATIVE AIRWAY IS ASSURED

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Anesthesia for Laser EndoscopyAssure patient and staff protection
Have a fire “plan of action”Minimize FiO2Avoid adding fuel to the fire when possible
Endotracheal tubes/packsApneic ventilation
Relaxant extends working time, accuracy

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Anatomic ClassificationSupraglottic
NoseChoanal atresiaNOWCA
Craniofacial DysmorphologyPierre Robin SyndromeTreacher collinsApertsCrouzonsMoebius
MacroglossiaBeckwith Wiedemann SyndromeDown’s Syndrome
TumorsHemangiomaNeuroblastoma
Laryngomalacia Glottic
Vocal cord paralysisTumors and cysts
• Laryngoceles• Papillomatosis• Cystic hygroma• Laryngoceles
AtresiaWebs
SubglotticStenosisWebsAtresiaTumors
HemangiomaCystic HygromaCysts
TracheaTracheomalaciaStenosisCystAtresia
ExtrinsicGoiterVascular RingHemangiomaCystic hygromaTeratomaMediastinal masses

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Nasal DisordersChoanal Atresia
Obstruction in posterior nasal cavity90% bony, 10% membraneousBilateral in 40%; other congenital anomalies in 50%Failure to pass #6 catheterUnilateral- observeBilateral
Oral airway; gavage; repair; tracheostomy

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Nasal DisordersPyriform Aperture StenosisHairy polypEncephalocele/Glioma

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Craniofacial disordersPierre Robin Syndrome
Micrognathia, cleft palate, glossoptosisRespiratory distress worst with feedingNasopharyngeal airwayImprovement with mandibular growth
Distraction osteogenesis

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Craniofacial DisordersTreacher Collins Sydrome
Autosomal DominantFindings
Antimongoloid slantlower lid colobomaauricular malformationMalar/mandibular hypoplasia

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Craniofacial DisordersCrouzon’s Syndrome
Midfacial hypoplasiaGlossoptosis, posterior pharyngeal compromise

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Break time!

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Laryngeal Disorders

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
LaryngomalaciaMost common cause of stridor in neonateEtiology: collapse of supraglottic structures into airway lumen, creating turbulent flow and obstructionIdiopathic--Anatomy vs. innervationGERD relationship (suck swallow dyscoordination)Coarse, non musical inspiratory stridor during first few weeks of life
Accentuated by supine position, feedingCry is normal
Evaluation: Flexible laryngoscopy, airway flouro, BSTreatment
Spontaneous resolution by 2 years in vast majority of patientsEpiglottoplastyTracheostomy

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Vocal Cord Paralysis2nd most common cause of congenital stridorBilateral
EtiologyIdiopathic, CNS lesions, birth trauma
PresentationProgressive stridor, voice may be normalHigh risk for aspiration
UnilateralEtiology
Mediastinal anomalies, idiopathic(heart, TEF surgery), trauma
PresentationHoarse cry,feeding difficulties, aspiration
EvaluationEndoscopyImaging
MR or CT of Brain, Neck and MediastinumLaryngeal EMG
ManagementTracheotomy: spontaneous recovery in >50% within 2 yearsVocal cord lateralization: arytenoidectomyvs. transverse cordotomy

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Congenital laryngeal websIncomplete recanalization of laryngotrachealanlageSx: Mild dysphonia to airway obstruction
1/3 have associated anomalies, most often subglottic stenosisChromosome 22q11.2 deletion (VCFS)
Rx: Observation-> surgery->tracheotomyLaryngeal Atresia
Acute airway obstructionTE fistula may allow some ventilationTracheostomy is lifesavingPolyhydramnios may provide a clue, allow for preoperative preparation

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Laryngeal CystCongenital saccular cyst
25% of laryngeal cystsObstruction of sacculewith accumulation of mucus
Vallecular cystSubglottic cyst

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Subglottic hemangioma1.5% of congenital airway anomalies
Female 2:1 Male. ½ with cutaneoushemangiomataUsually asymptomatic at birth, rapid growth after 2 months through 12 monthsSymptoms mimic recurrent croup
Treatment optionsObservation, tracheostomy, steroids (systemic and local), interferon, surgical excision

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Recurrent Respiratory PapillomatosisHPV 6,11Entire respiratory tractInfancy through adultNo cureSurgical therapy, medical adjunctVaccine holds promise

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Subglottic stenosisCongenital
RareIncomplete recanalizationMore mild
Elliptical cricoid
AcquiredMost common1-8% of intubated neonatesOther causes
TraumaBurns NeoplasmsInfectionCollagen vascular disorders

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Pathogenesis of acquired subglottic stenosisintubation
Pressure injury
Mucosal edemaUlcerationPerichondrial injuryCartilage necrosis
Fibroblasts& Granulation tissue
Circumferential scarring

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Subglottic Stenosis – the recipeCongenital subglottic stenosisGERDInfectionNasogastric tubeETT size and propertiesMovement of ETTReintubationsDuration?

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
StagingClassification from to
Grade I No obstruction
50%
Grade II 51% 70%
Grade III 71% 99%
Grade IV No lumen

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Evaluation:GER/GERD, GLPR/GLPRD
GER is common in children with subglottic stenosis and usually asymptomatic
GER/GLPR likely exacerbates SGS and compromises repair No gold standard to differentiate GER and GERDDual pH probe:
50% of candidates have upper probe pH<4 more than 1% of the timeMajority had no symptoms

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Evaluation: Swallowing Dysfunction Increased risk of aspiration postoperativelyRely on history
Videoflouroscopic examinationLimited in patients with food aversion or congenital aerodigestive anomalies
FEES

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
ManagementObservationTracheostomyEndoscopic techniquesCricoid splitAugmentation LaryngoplastyPartial cricotracheal resection

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
ObservationNon tracheotomized Grade I or mild grade II
Occasional symptoms – infrequent hospitalizationsNo retractionsNo feeding difficulties
Tracheotomized patients reactive larynxAge/weight/pulmonary status/neurologic disease/aspiration potential/craniofacial or systemic abnormalities

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Endoscopic ManagementMild SGS
May be required following open repair techniquesTechniques
DilationCO2 laser
wedge resections

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
TracheotomyTemporizing measure
Allows for growth prior to definitiveprocedure
Time for improvement of BPDFacilitates dischargeGold Standard?
Mortality rate varies with degree of obstruction above stomaImpairment of speech and language skillsNursing/childcare issues

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
History of airway reconstruction 193O’s
Chevalier Jackson recognizes that many children with laryngeal stenosis do not outgrow their obstruction –permanent tracheotomy was treatment of choice
1960’sMcDonald and Stocks: long term intubation for the management of prolonged ventilatory support in newbornsGreater survival potential of premature newbornsShift of subglottic stenosis from older children and adults to premature infants

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
History of airway reconstructionIncreased incidence of subglottic stenosis recognizedTreatment consisted of repeated dilations
Dogma was “never divide the larynx” to avoid growth disturbance1956 Rethi Expansion of larynx and trachea with long term stent1970’s Fearon and Cotton: Pedicled thyroid cartilage grafts1980’s Free cartilage grafts allow for posterior and anterior grafting1993 First series of successful cricotracheal resections reported

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Cricoid SplitOverviewIndications
Acquired subglottic stenosis in neonate (>1500g) without significant coincidental airway or pulmonary disease<30%FiO2, <35mm Pressure, no vent support
Surgical techniqueOutcomeComplications

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Augmentation LaryngotracheoplastyOverviewIndicationsSurgical technique
Single stage vs. 2 stageSource of donor cartilageAutologous materials
OutcomeComplications

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Single Stage LTR Uses cartilage grafts for expansion and a short phase of stenting with ETTStoma is grafted and closedPostoperatively
0-14 days of intubation in ICU+/-Paralysis and sedationBronchoscopy and downsize prior to extubation

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Results>90% success rates in most seriesSuccess is dependent upon degree of stenosis
<50% in severe grade III and IV stenosis

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Partial Cricotracheal resectionOverviewIndicationsSurgical techniqueOutcome
Complications

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Adjunctive measuresStenting
Useful for areas of stenosis beyond subglottis (posterior glottic stenosis)result in addition granulation tissue and scarring,
Mitomycin CAntineoplastic antibiotic inhibits fibroblast formation
Fibrin glueHolds mucosal flaps, produces an airtight seal

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Postoperative carePICUIntubation for 0 – 14 days for single stage
Sedation – minimal paralysisBronchoscopy/downsizing/extubation

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Complications of Airway ReconstructionIntraoperative
HypoxiaPneumothoraxPneumomediastinumVocal cord paralysis
Early PostoperativeSQ emphysemaSeromaHematomaSingle Stage
ETT obstructionUnplanned extubationNarcotic withdrawlPulmonary problemsNasal alar ulcerationFailed extubation
Intermediate postoperativeGranulationsRestenosisGraft displacementGraft resorptionChonditisSuprastomal/ posterior glottic stenosis
Late PostoperativeVoice problemsEpiglottic/arytenoid collapseWebTracheocutaneous fistula

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Tracheal AnomaliesTracheomalacia
Abnormal flaccidity of trachea leading to collapse on expiration
Collapse of greater than 20% on endoscopy (spontaneous ventilation)Primary vs secondary
MRIRarely occurs with laryngomalacia
Rx: Mild- typically improves within 1-2 yearsReflux therapySevere – tracheostomy with PPVSurgical correction varying success
Stent placement (internal or external)Segmental resectionCartilage grafting

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Tracheal DisordersTracheal Stenosis
Congenital vs. acquiredSymptoms depend upon severity and lengthComplete tracheal ringsBiphasic or expiratory stridor, wheezing, failure to thrive, bronchiolitis, cough recurrent croupVery gentle endoscopy!Rx:
conservative for mild cases; resolution with growthSevere cases: segmental resection vs. anterior split with perichondrial grafting vs slide tracheoplasty or homograft tracheal transplantation
Complications: granulation tissue at anastamotic site

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
Tracheal DisordersVascular Compression
3% of population with anomalies of great vessels
Rarely result in airway obstructionRings vs slingsDouble aortic arch most common ringInnominate artery most common slingRight aortic arch with aberrant left subclavianBarium swallow and MR are essential

0ct 06 Airway Disorders in Neonates Andrew Shapiro, MD, FAAP
ConclusionsDiagnosis of airway disorders in the neonate requires a comprehensive and systematic approachStridor is not a diagnosis, but a symptom: the characteristics will help localize the sourceTwenty five years ago – once a trach, always a trach
Now, almost all tracheotomy dependent children with airway obstruction can eventually be decannulated
Important to have a bag of tricks, as different approach works in different patientslist of options for restoration of the pediatric airway continues to expand