Embed Size (px)
Citation preview

PEDIA
TRIC
PENETR
ATIN
G
TRA
UM
A
Laura Boomer
11/18/15

PENETRATIN
G TH
ORA
CIC TRAU
MA
�Traum
a is the major cause of m
orbidity and mortality in children
�Penetrating traum
a (in general) accounts for only approximately 2%
of all pediatric traum
a
�Thoracic traum
a accounts for only 4-12% of pediatric traum
a admissions
�M
ay cause 6-10% of fatalities
�Penetrating thoracic traum
a accounts for only 10-20% of all pediatric thoracic
trauma
�Recently, w
e have seen a number of penetrating thoracic traum
a

RC
�14 yo M
handling homem
ade explosives when one w
ent off and he sustained a blow
to his chest (8/2) – trauma stat
�Patient’s m
om (w
ho is an ICU nurse) placed pressure on his axilla w
here bleeding w
as coming from
�PE: w
ound at the posterior axillary line just distal to the hairline �
Clothing blood soaked, but no active bleeding �
+ palpable distal pulses
�CTA
done: shows m
oderate axillary artery extravasation

RC

RC
�O
R: angiogram perform
ed, with exploration of right axillary fossa
�Significant hem
atoma; brachial plexus carefully retracted out of the w
ay �
Injury to axillary artery and vein – both were able to be prim
arily repaired with 6-0
prolene �
Closed over a blake drain
�A
dmitted to PICU
overnight (early am on 8/3)
�Placed on aspirin 81 m
g post-op
�Transferred to floor on 8/4
�D
rain removed and patient discharged on 8/5, aspirin x 30 days
�Seen in vascular clinic on 8/17 – som
e weakness in ulnar distribution, but w
orking w
ith PT/OT

PH
�14 yo M
, GSW
to chest, initially seen at Baptist-DeSoto (8/11)
�Believed to be self-inflicted
�Transferred as traum
a stat
�D
ecreased strength left hand grip and wrist flexion
�1 x 2 cm
wound to anterior left upper chest (3 sutures in place w
ere removed)
�2.5 x 2.5 cm
wound to upper left back
�CTA
: comm
inuted left scapula fracture �
Pulmonary contusion
�Possible 2m
m traum
atic pseudoaneurysm arising from
proximal axillary artery

PH

PH

PH
�O
R: left shoulder explored through an infraclavicular incision �
No arterial injury
�Paired vein – 1 w
as intact, 1 transected – this was ligated
�A
rteriogram perform
ed through the axillary artery – demonstrated patent subclavian
and axillary artery with flow
distal through branchial artery and its bifurcation �
Ortho w
ashed out posterior wound (open, com
minuted scapula fracture)
�N
eurosurgical evaluation of nerve trunks �
Closed over JP drain
�A
dmitted to PICU
overnight
�Transferred to floor and drain rem
oved on 8/12
�D
ischarged to inpatient psychiatric unit on 8/14 with neurosurgical follow
-up for neuro deficits

TC
�3 yo F w
ho was shot in the chest w
ith a BB gun by her brother at hom
e (8/2) – traum
a stat
�She w
as seen at an OSH
where she had a CT scan, and w
as found to have a missile
in her heart (images not available)
�PE: 4-5m
m w
ound along left sternal border
�Cardiology and CT surgery w
ere consulted in the ED
�ECH
O : foreign body lodged near the tricuspid valve, avulsed papillary m
uscle w
ith mild tricuspid regurgitation; m
oderate pericardial effusion with RV
collapse
�Taken to CV
suite for fluoroscopic and ultrasound guided evacuation of hem
opericardium and placem
ent of pericardial drain (55 ml blood)
�A
dmitted to CV
ICU

TC: 8/3/15

TC
�8/3: repeat x-ray and ECH
O perform
ed �
Echogenic mass at base of septal leaflet of tricuspid valve consistent w
ith pellet �
Trivial pericardial effusion
�8/4: no signs of tam
ponade, pellet unchanged on imaging
�Transferred to floor
�8/5: repeat ECH
O: BB
pellet in same location, avulsed papillary m
uscle with
tricuspid regurg, normal biventricular size and function
�D
ischarged home
�Cardiology clinic follow
up on 8/14: normal activity w
ithout limitations
�ECH
O: unchanged, no effusion
�Plan for repeat ECH
O and clinic visit in 6 m
onths

TC: 8/5/15

CASE 2012
�6 yo M
, presents as level 1 trauma to N
CH
�Struck in the chest by a projectile ejected from
the underside of a lawnm
ower
�Im
mediately collapsed, question of bystander CPR at the scene
�Taken to a local hospital
�H
R and BP labile on transport from O
SH to N
CH
�A
wake and com
plaining of chest pain on arrival
�Exam
: small puncture w
ound over body of sternum
�Electively intubated

CASE 2012
Pre-intubation
Post-intubation (30 minutes later)

CASE 2012
�FA
ST exam: large pericardial effusion
�Cardiology perform
ed ultrasound guided pericardiocentesis and drain placement
�150 m
l blood aspirated
�H
emodynam
ics improved
�Thoracic CT perform
ed
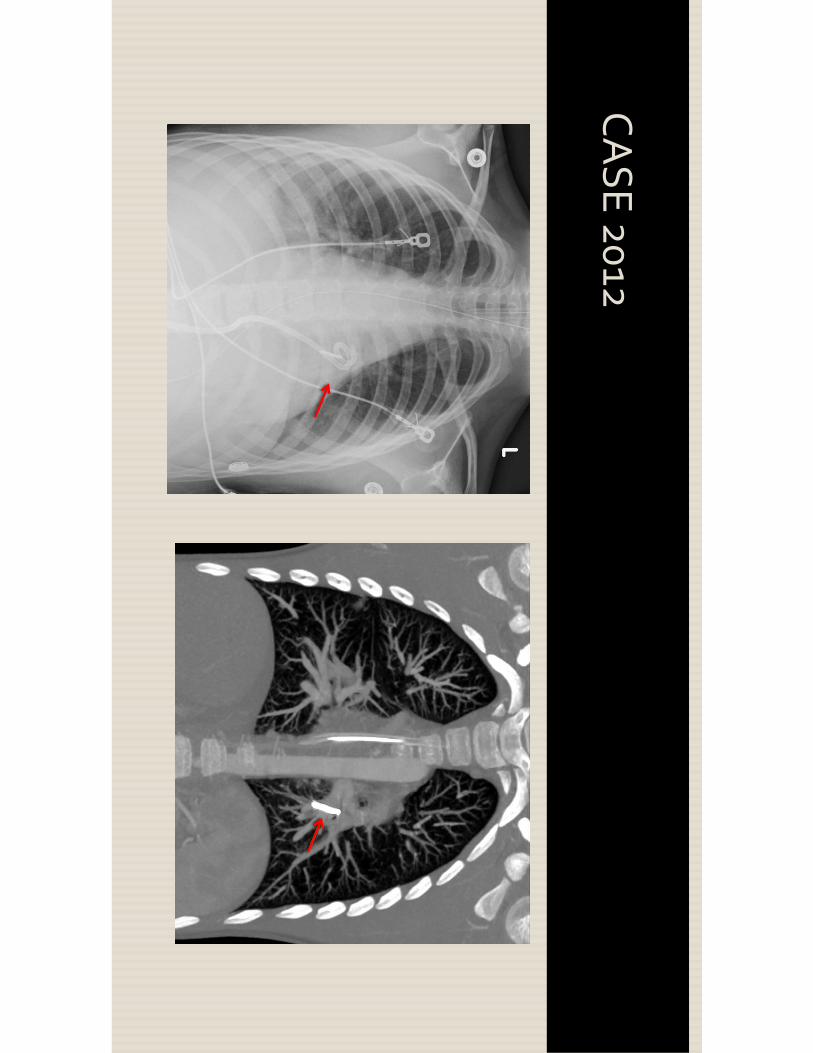
CASE 2012

CASE 2012
�A
dmitted to PICU
�Traum
a/general surgery, CT surgery, cardiology, IR
�Risks of rem
oval felt to outweigh any potential benefit
�Repeat ECH
O: no accum
ulation of fluid �
No structural or functional cardiac dam
age
�Pericardial drain rem
oved and pt extubated on HD
#2
�D
ischarged on HD
#6
�A
symptom
atic with stable CXR at follow
-up

NCH
REVIEW
�Patients extracted from
trauma registry
�10 year period (Jan 2003-D
ec 2012)
�D
ata collected �
Dem
ographics �
Mechanism
of injury �
GCS, A
IS, ISS �
Diagnoses, procedural inform
ation �
ICU days, total LO
S, ventilator days �
Outcom
e and complications

NCH
REVIEW
�65 patients w
ere found to have penetrating thoracic injuries
�These patients w
ere reviewed and categorized into 2 groupd
�H
igh velocity (GSW
) �
Low velocity (knife stab w
ound)
�There w
ere 7 total fatalities �
All w
ere high velocity wounds
�A
ll patients that underwent CPR, defibrillation or ED
thoracotomy died

NCH
DEM
OG
RAPH
ICS
ALL Low
Velocity H
igh Velocity P-value
Num
ber 65
14 (21.5%)
51 (78.5%)
Age, mean
12.16 (1.33-20) 9.53 (2.42-16)
12.89 (1.33-20) p=0.018*
Male sex
53 (81.5%)
10 (71.4%)
43 (84.3%)
p=0.271
White race
27 (41.5%)
12 (85.7%)
15 (29.4%)
p=0.002*
Private Insur. 20 (30.8%
) 5 (35.7%
) 15 (29.4%
) p=0.903

NCH
REVIEW
All Patients
Low Velocity
High Velocity
p-value
ISS 17 + 14 (1-75)
12 + 7 (1-26) 18 + 16 (1-75)
p=0.331
Total AIS 10 + 7 (1-36)
7 + 5 (1-17) 11 + 7 (1-36)
p=0.090
Initial GC
S 13 + 4 (3-15)
14 + 3 (3-15) 13 + 4 (3-15)
p=0.637
LOS (days)
6.3 + 9.0 (1-45) 3.6 + 2.2 (1-9)
7.1 + 9.9 (0-45) p=0.640
ICU
LOS (days)
1.4 + 4.5 (0-36) 0.6 + 0.7(0-2)
1.6 + 5.1 (0-36) p=0.356
Ventilator Days
0.5 + 1.6 (0-12) 0.1 + 0.4 (0-1)
0.6 + 1.8 (0-12) p=0.152

NCH
REVIEW
: INJU
RIES
�M
ajor vascular injuries occurred in 11 patients (1 low velocity)
�Cardiac injuries identified in 4 patients
�N
eurologic injuries in 7 patients
�Solid organ injuries m
ost comm
only liver, followed by renal injuries
�H
ollow viscus injuries less com
mon

NCH
REVIEW
: MO
ST COM
MO
N IN
JURIES
�H
igh velocity �
Pneumothorax (47.1%
) �
Hem
othorax (41.1%)
�Pulm
onary contusion (35.3%)
�Liver laceration (29.4%
)
�Low
velocity �
Pneumothorax (50%
) �
Liver laceration (28.6%)
�H
emothorax (21.4%
) �
Pulmonary contusion (21.4%
)

NCH
REVIEW
: PROCED
URES
ALL Low
Velocity H
igh Velocity P-value
Transfusion 8 (12.31%
) 2 (14.29%
) 6 (11.76%
) p=1.000
Chest Tube
31 (47.69%)
5 (35.71%)
26 (50.98%)
p=0.477
Intubation 19 (29.23%
) 2 (14.29%
) 17 (33.33%
) p=0.203
CPR/D
efib 7 (10.77%
) 0 (0%
) 7 (13.73%
) p=0.331
OR
ED Thorac O
R C
hest O
R Abd
OR
Other
3 (4.62%
) 10 (15.38%
) 18 (27.69%
) 11 (16.92%
)
0 (0%
) 4 (28.57%
) 2 (14.29%
) 4 (28.57%
)
3 (5.88%
) 6 (11.76%
) 16 (31.37%
) 7 (13.73%
)
p=1.000 p=0.203 p=0.316 p=0.232

PENETRATIN
G TH
ORA
CIC TRAU
MA
�Penetrating thoracic traum
a in children is rare, but on the rise
�4,500 firearm
-related deaths per year in children
�M
ost comm
on complications are from
pericardial tamponade or V
SD
�Positive pericardial blood m
ay not necessitate sternotomy
�A
s evidenced by the last 2 cases presented �
TC clearly had a cardiac injury, without a full thickness penetration (m
ost likely) of the cardiac m
uscular wall
�The case from
2012 also likely had a cardiac injury as the source of entry of the foreign body into the pulm
onary vascular system
�Both patients recovered w
ith pericardial drainage alone

PENETRATIN
G TH
ORA
CIC TRAU
MA
�There is also one institutional review
of patients undergoing either pericardial w
indow for severe chest traum
a �
3 patients with positive pericardial w
indows w
ere successfully treated without
sternotomy, and prom
pted the review (2 blunt, 1 penetrating)
�15%
of the patients had a positive pericardial window
(n=55) �
89% of w
hich (49) had sustained penetrating trauma
�38%
of those patients had non-therapeutic sternotomies
�There w
ere no differences with respect to age, m
echanism of injury, ISS, presenting lab
values, resuscitation fluids, or vital signs �
Penetrating trauma and hem
odynamic instability w
ere positive predictors of therapeutic sternotom
y
Thorson, CM, et al. Journal of Traum
a and Acute Care Surgery, 2012. 72(6): 1518-1524.

PENETRATIN
G TH
ORA
CIC TRAU
MA
�The Thorson paper is not the only one to report high rates of non-therapeutic sternotom
ies �
Has been reported to range from
0-67%
�This m
ethod not applicable to patients that present in extremis or cardiovascular
collapse �
Our patient TC, w
as clearly very stable on presentation �
A coordinated m
ulti-disciplinary effort is required when these treatm
ent modalities are
employed

EMB
OLIZATIO
N
�Foreign body em
bolization is rare
�Em
boli include needles, bullets, and other projectiles
�Risk of a bullet lodging in the vascular system
is only 0.3%
�80%
of emboli are arterial in nature
�M
any foreign bodies that embolize to the pulm
onary tree have been reported �
Many identified post-operatively (cardiac repair perform
ed, but bullet not identified intra-operatively)
�M
ost are left in place �
Most have no significant com
plications �
Biggest risk is infection, erosion, pulmonary necrosis, throm
bosis

CON
CLUSIO
NS
�Penetrating thoracic traum
a in children is rare, but may be increasing
�V
ascular injury from penetrating thoracic injury m
ay be more com
mon than
previously reported
�Cases should be considered on an individual basis, as standard treatm
ents may
not be necessary �
Patients treated non-operatively need close follow-up
�Prevention and education m
ay be the most im
portant factors to try to reduce the incidence of penetrating traum
a in pediatric patients

FUTU
RE STUD
IES
�G
iven the number of significant penetrating thoracic traum
a that presented this sum
mer alone to Le Bonheur, there m
ay be a much larger population in M
emphis
to study
�A
retrospective review m
ay lead to information that could be used for prevention
programs
�A
specific review of both blunt and penetrating vascular traum
a would likely also
yield a larger population than may have been previously reported
![BORANG BERKAITANepsmg.jkr.gov.my/images/archive/1/15/20160202011736...*Pohon rujuk Manual pH JKR untuk keterangan terperinci bagi setiap pengemukaan [JKR/pH JKR/BRG02-KB1.1] pH JKR(JKR20801-0014-15)](https://img.pdfslide.net/doc/110x75/5e5a0ea9a5d37b193b1f29d9/borang-pohon-rujuk-manual-ph-jkr-untuk-keterangan-terperinci-bagi-setiap-pengemukaan.jpg)





![arXiv:physics/9911031v1 [physics.comp-ph] 15 Nov 1999 · · 2008-02-02arXiv:physics/9911031v1 [physics.comp-ph] 15 Nov 1999 ... years [15–19], and this paper will add additional](https://img.pdfslide.net/doc/110x75/5ae045567f8b9a97518d02b1/arxivphysics9911031v1-15-nov-1999-physics9911031v1-15-nov-1999-years.jpg)
![arXiv:1811.05586v2 [quant-ph] 15 Apr 2019](https://img.pdfslide.net/doc/110x75/6206362706a4f947d167c263/arxiv181105586v2-quant-ph-15-apr-2019.jpg)



![arXiv:2107.09456v1 [physics.app-ph] 15 Jul 2021](https://img.pdfslide.net/doc/110x75/61bd422f61276e740b10f880/arxiv210709456v1-15-jul-2021.jpg)








![arXiv:2110.07974v1 [math-ph] 15 Oct 2021](https://img.pdfslide.net/doc/110x75/61bd3f0061276e740b10d4d4/arxiv211007974v1-math-ph-15-oct-2021.jpg)


![arXiv:1803.05586v1 [quant-ph] 15 Mar 2018](https://img.pdfslide.net/doc/110x75/6180509100ccf676252f2c81/arxiv180305586v1-quant-ph-15-mar-2018.jpg)
![arXiv:2005.11918v2 [quant-ph] 15 Jul 2020](https://img.pdfslide.net/doc/110x75/6210e0a520bb7c0cf64a36d6/arxiv200511918v2-quant-ph-15-jul-2020.jpg)
![arXiv:2001.05229v1 [physics.acc-ph] 15 Jan 2020](https://img.pdfslide.net/doc/110x75/61d90dacf15c5546a3113d91/arxiv200105229v1-15-jan-2020.jpg)
![arXiv:2111.08126v1 [hep-ph] 15 Nov 2021](https://img.pdfslide.net/doc/110x75/62699ebd0e5929547430dda9/arxiv211108126v1-hep-ph-15-nov-2021.jpg)

![arXiv:1301.3274v1 [quant-ph] 15 Jan 2013](https://img.pdfslide.net/doc/110x75/61da4432daa892275831f0db/arxiv13013274v1-quant-ph-15-jan-2013.jpg)
