-
PEDIATRIC PROCEDURES
-
PEDIATRIC PROCEDURES PART II
Exchange Transfusion Vascular ProceduresPercutaneous Peripheral
Venous AccessUmbilical Vessel Cannulation Blood ExtractionCapillary
Blood SamplingArterial Blood Sampling
-
EXCHANGE TRANSFUSION
Term infants with levels of 20 mg/dL or higher have an increased
risk of kernicterus.Blood for exchange transfusion should be as
fresh as possible. Heparin or citrate-phosphate-dextrose-adenine
solution may be used as an anticoagulant.Blood should be gradually
warmed and maintained at a temperature between 35 and 37C
throughout the exchange transfusion.
-
EXCHANGE TRANSFUSION
The infant's stomach should be emptied before transfusion to
prevent aspirationAn assistant should be present to help monitor,
tally the volume of blood exchanged, and perform emergency
procedures.
-
EXCHANGE TRANSFUSIONPROCEDUREWith strict aseptic technique, the
umbilical vein is cannulated with a polyvinyl catheter to a
distance no greater than 7 cm in a full-term infant. When free flow
of blood is obtained, the catheter is usually in a large hepatic
vein or the inferior vena cava. Alternatively, the exchange may be
performed through peripheral arterial (drawn out) and venous
(infused in) lines
-
EXCHANGE TRANSFUSIONPROCEDUREThe exchange should be carried out
over a 4560 min period, with aspiration of 20 mL of infant blood
alternating with infusion of 20 mL of donor blood. *Smaller
aliquots (510 mL) may be indicated for sick and premature infants.
* The goal should be an isovolumetric exchange of approximately two
blood volumes of the infant (2 85 mL/kg).
-
EXCHANGE TRANSFUSIONCOMPLICATIONSAcute complications (510% of
infants)Transient bradycardia with or without calcium
infusionCyanosis Transient vasospasmThrombosisApnea with
bradycardia requiring resuscitation, and death. Infectious risks
include CMV, HIV, and hepatitis. Necrotizing enterocolitis (rare
complication of exchange transfusion).
-
After exchange transfusion, the bilirubin level must be
determined at frequent intervals (every 48 hr) because bilirubin
may rebound 4050% within hours.
-
Vascular Procedures
-
Anatomy Digital Vessels -Along lateral aspects fingers,
infiltrate easily, painful, difficult to immobilize and should be
your LAST RESORTMetacarpal Vessels -Located between joints and
metacarpal bones (act as natural splint) -Formed by union of
digital veins
Digital
-
Veins of the Upper ExtremitiesCephalic (Interns Vein) -Starts at
radial aspect of wrist -Access anywhere along entire length (BEWARE
of radial artery/nerve)
Medial Cephalic (On ramp to Cephalic Vein) -Joins the Cephalic
below the elbow bend -Accepts larger gauge catheters, but may be a
difficult angle to hit and maintain
-
Veins of the Upper ExtremitiesBasilic - Originates from the
ulner side of the metacarpal veins and runs along the medial aspect
of the arm. It is often overlooked becauses of its location on the
back of the arm, but flexing the elbow/bending the arm brings this
vein into view
Medial Basilic - Empties into the Basilic vein running parallel
to tendons, so it is not always well defined. Accepts larger gauge
catheters. - BEWARE of Brachial Artery/Nerve
-
Purposes of Vascular Access
To provide parenteral nutritionTo provide avenue for
dialysis/apheresisTo transfuse blood productsTo provide avenue for
hemodynamic monitoringTo provide avenue for diagnostic testingTo
administer fluids and medications with the ability to
rapidly/accurately change blood concentration levels by either
continuous, intermittent or IV push method.
Types of Peripheral Venous Access DevicesButterfly (winged) or
Scalp vein needles (SVN) not recommended for non compliant patient
as it can easily penetrate the vein wall causing extravasation. We
use these frequently for phlebotomySafety Over the needle catheters
(ONC)
-
Vascular ProceduresEQUIPMENT AND MATERIALSVascular Devices2
types of cannulae:1) Metal cannulae (Butterflies) - indicated for
very short term use (1-2 days) or for blood sampling - can easily
dislodged or cause inadvertent punctures.- common size: G23 or G25.
For blood extraction: G21
2)Plastic cannulae are more easily kept in place and may last
for several days if properly maintained. (size G24 or smaller for
neonates)
-
OTHER MATERIALSAntiseptic swabs, inch skin tape and a
torniquetUse of gloves is encouraged.The fluid and delivery system
should be prepared beforehand.Local anesthetic, syringes or vacuum
tube and splints may be prepared.
-
Starting a Peripheral IVTECHNIQUE
Anatomic considerations Iff an IV line is to be established, the
most distal available vein should be utilized (eg dorsum of the
hand before arm)AVOID SITES:- Angulated- Dependent- Mobile -
Contaminated
-
Starting a Peripheral IVPROCEDURE
Clean the area with antiseptic swabIf a limb is to be used,
apply a torniquet about 3-5 cms above the place where the needle
will be inserted * Placing the area in a dependent position and
local heat application will help distend the vein
Topical or local anesthetic may be used especially if a large
bore needle will be insertedThe needle bevel up is inserted into
the skin and is directed at an acute angle towards the surface or
the side of the vein
-
Starting a Peripheral IVPROCEDURE
A give may be felt or the butterfly tubing or cannula chamber
may fill by blood indicating puncture of the veinThe tornique is
removed and the previously filled intravenous tubing is attached to
the needle or cannula The needle or cannula is then taped and
secured to the skin.Proper application of fixed splints
-
COMPLICATIONS AND PRECAUTIONS
Hematoma formationExtravascular infiltration Local infection or
phlebitis
-
Infiltration/ExtravasationThe most common cause is damage to the
wall during insertion or angle of placement.
-
Phlebitis/Thrombophlebitis Chemical- Infusate chemically erodes
internal layers. Warm compresses may help while the infusate is
stopped/changed. Anti-inflammatory and analgesic medications are
often used no matter what the cause Mechanical- Caused by
irritation to internal lumen of vein during insertion of vascular
access device and usually appears shortly after insertion. The
device may need to be removed and warm compresses applied
Bacterial- Caused by introduction of bacteria into the vein. Remove
the device immediately and treat w/antibiotics. The arm will be
painful, red and warm; edema may accompany
-
Cellulitis Inflammation of loose connective tissue around
insertion site- Red swollen area spreads from insertion site
outwardly in a diffuse circular pattern- Treated w/antibiotics
-
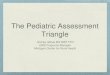
Umbilical Vessel CannulationThe umbilical vessels are accessible
generally up to only 10-14 days of life
INDICATIONS:For umbilical artery cannulation:Frequent ABG
determination in extremely low birth weight infants, preterms,
PPHN, AsphyxiaContinuous IV BP monitoring Additional Vascular
access
-
ANATOMY
-
Umbilical Vessel CannulationINDICATIONS:
For umbilical venous cannulation:Emergency volume expansion or
transfusion of blood productsExchange transfusionCentral venous
access for reliable infusion of fluids with high dextrose loads,
medicationsCVP monitoring
-
Umbilical Vessel CannulationEQUIPMENT AND MATERIALSPovidone
iodine antiseptic solutionSterile NSSSterile umbilical cannulation
setSterile glovesCord tieScalpel handle and bladeIris
scissorHemostatsNeedle holderSutures (3.0 or 4.0 silk)Umbilical
catheter (single/double/triple lumen or feding tubes (5.0 or 8
Fr)Syringes3-way stop cock2x2 gauze pads
-
Umbilical Vessel CannulationPROCEDUREImmobilize the neonate in
supine position (arms and legs are properly restrained)Provide
thermoregulationMeasure distance from the acromioclavicular (AC)
joint to a line extending laterally from the umbilicusDon a cap and
mask, Perform 3-5 mins surgical scrub. Put on sterile gown and
gloves.Open the cannulation set, check contents, flush catheters w/
NSS, attach to stopcocks, affix needle/suture to needle holder and
check all other equipment
-
Umbilical Vessel CannulationPROCEDURE6) Grasp the cord with mild
traction. Paint the cord and its base w/ povidone and iodine
solution and allow to dry.7) Apply cord tie to the umbilical base.
Cut the cord about 1-1.5 cm from the base8) Identify the umbilical
vessels (2 arteries: 1 vein) Arteries have thick muscular walls,
vein is thin-walled and bleeds more easily after cutting)
-
Umbilical Artery CannulationDIRECT TECHNIQUEGrasp the side of
the cord with a hemostat. Dilate one of the arteries, initially
with iris forceps The tip of the catheter is then introduced into
the lumen and advance with a gentle and even pressure
-
Umbilical Artery CannulationSIDE TECHNIQUEVisualize the
approximate course of one of the arteries along the side of the
cordCut partially through the cord until you transect one third to
halfway through the artery.Dilate and cannulate
-
Umbilical Artery CannulationSIDE TECHNIQUEVisualize the
approximate course of one of the arteries along the side of the
cordCut partially through the cord until you transect one third to
halfway through the artery.Dilate and cannulate
-
Umbilical Artery Cannulation
A low lying arterial catheter is generally advanced about
two-thirds the distance from the acromioclavicular joint to the
umbilical level previously measured.
-
Umbilical Vein CannulationDoes not require dilatationThe flushed
catheter is slowly advanced, initially to a level 1-2 cm beyond the
planned distance.The catheter is slowly withdrawn until a steady
backflow of blood is encountered.
-
Umbilical Vein CannulationDoes not require dilatationThe flushed
catheter is slowly advanced, initially to a level 1-2 cm beyond the
planned distance.The catheter is slowly withdrawn until a steady
backflow of blood is encountered.
-
Umbilical Vessel CannulationXray for placement verificationThe
cannulae can be taped using goalpost of H-type
-
UMBILICAL VESSEL
CANNULATIONVIDEOhttp://www.youtube.com/watch?v=UIRy3kaxoKY
-
BLOOD EXTRACTIONCAPILLARY BLOOD SAMPLINGINDICATIONSRoutine
laboratory blood tests including serial glucose
determinationCapillary blood gas sampling Difficulty obtaining
blood from a vein (preterm infants)
-
BLOOD EXTRACTIONCAPILLARY BLOOD
SAMPLINGCONTRAINDICATIONSInfection at the siteDecreased blood flow
to the area (extremities with poor perfusion) in cases of
shockEdema of the extremityPolycythemia Bleeding disorders with
prolonged bleeding time
-
BLOOD EXTRACTIONCAPILLARY BLOOD
SAMPLINGCONTRAINDICATIONSInfection at the siteDecreased blood flow
to the area (extremities with poor perfusion) in cases of
shockEdema of the extremityPolycythemia Bleeding disorders with
prolonged bleeding time
-
BLOOD EXTRACTIONCAPILLARY BLOOD SAMPLINGSITE Medial plantar
surface of the heel (lateral area is also
acceptable)EQUIPMENTSterile gloves70& alcohol swab or cotton
with alcoholGauze square LancetCapillary tubes with sealer
caps/waxMicrotainers/collecting tubes
-
BLOOD EXTRACTIONCAPILLARY BLOOD SAMPLINGTECHNIQUEWarm the heel
using a small wet towel or disposable diaper soaked in warm water.
Wring out excess water. This will increase blood flow to the
areaClean the area using alcohol swabs. Allow it to dryPosition the
heel. Grasp gently using your thumb & second or third finger to
assume a dorsiflexed position so that it will be possible to milk
the heel.
-
BLOOD EXTRACTIONCAPILLARY BLOOD SAMPLINGTECHNIQUE4) Use a lancet
to pierce the skin using one continuous stroke. Do not go deeper
than 2.5mm. If less amount of blood is needed, make a shallower
incision.5) Once the 1st drop of blood is obtained, wipe this off
using a dry gauze
-
BLOOD EXTRACTIONCAPILLARY BLOOD SAMPLINGTECHNIQUE6) Slightly
relaxed the grip on the heel to allow blood to accumulate. Gently
squeeze or milk the heel again. This step may be repeated7)
Position the collecting tube (microtainer or the capillary tube so
that it touches the drop of blood)
-
BLOOD EXTRACTIONCAPILLARY BLOOD SAMPLINGTECHNIQUE8) Place the
cap onto the containers or seal the capillary tubes using wax
3-5mm
9) Apply pressure on the puncture site for at least 2 minutes
until no bleeding at the site occurs.
-
BLOOD EXTRACTIONCOMPLICATIONS Maceration of the site from
excessive squeeze or from numerous pricks.Subcutaneous nodules at
puncture sites.Osseus spurs from hitting to the talus.Ankle
dislocation or even foot fracture from overzealous milking of the
heel
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGINDICATIONSDetermination
of arterial blood gas Blood sampling when capillary and venous
sites are found inaccessibleSpecific blood tests (e.g. ammonia
levels)
-
BLOOD EXTRACTIONARTERIAL BLOOD
SAMPLINGCONTRAINDICATIONSCompromised blood supply to the extremity
siteInfection in the affected siteSite will be used for central or
percutaneous line insertion Clotting disorders
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGSITESRadial
arteryDorsalis pedisPosterior tibial arteriesUlnar artery, temporal
& brachial arteries (alternative sites)
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGSITESAVOID FEMORAL
ARTERY!
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGEQUIPMENTSterile
GlovesGauze 23 or 25 butterfly needle for venipucture preferredTB
syringe (Heparinized syringe for blood gases)Antiseptic
solution/spraySterile gauze/ cotton ballsSterile alcohol
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGTECHNIQUE Select and
prepare the site. One that has barely been tapped is ideal.
Transillumination of the vessel may aid if pulsation from the
artery is not palpated. Apply antiseptic solution thrice and allow
it to dry
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGTECHNIQUE 2) Position the
limb. If the radial artery is chosen, extend the wrist. Do nit
hyperextend. If the dorsalis pedis artery is selected, slightly
extend the foot. If the temporal artery is used, choose the area
anterior to the tragus of the ear.
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGTECHNIQUE 3) Locate where
to puncture and position the needle at 15-25 degree angle for the
horizontal plane of the skin. At wrist, choose an area proximal to
the wrist crease
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGTECHNIQUE 4) Insert the
needle to penetrate the skin, bevel down for small premature
infants.Advance the needle very slowly to allow the blood to flow
into the needle. Avoid advancing and pulling the needle blindly
using several strokes as this can injure nerves and other
tissues.5) Apply gentle suction by applying traction on the syringe
plunger while simultaneously advancing the needle until resistance
is not felt & blood from the vessel lumen is drawn
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGTECHNIQUE Secure the
angiocatheter with Tegaderm and tape just as with any intravenous
line.Send blood specimen immediately for blood gas analysis or
ammonia level
-
BLOOD EXTRACTIONARTERIAL BLOOD
SAMPLINGCOMPLICATIONSHematomaArterial embolism, thrombosis and
fibrosis of a vesselInfection (eg abscess formation, septic emboli,
and osteomyelitis)Fibrosis of artery
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGCOMPLICATIONS5) Keloid
and hypertrophic scar formation6) Arterial spasm7) Extensor tendon
sheath injury resulting in false cortical thumb8) Nerve injury of
the median, posterior tibial or femoral nerves
-
Intraosseous infusionINDICATIONS1) Reserved for use when
attempts in establishing immediate vascular access are not
successful as in shock, status epilepticus and in cardiopulmonary
arrest.
-
Intraosseous infusionINDICATIONS2) As 1st attempt in cases of
cardiopulmonary arrest
-
Intraosseous infusionCONTRAINDICATIONSPlacement ina recently
fractured boneOsteogenesis imperfectaSoft tissue infection or
cellulitis in the area selected for intraosseous infusion
Obliterative diseases of marrow as osteopetrosis
-
INTRAOSSEUS INFUSION procedure
VIDEOhttp://www.youtube.com/watch?v=UIRy3kaxoKY
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGCOMPLICATIONS5) Keloid
and hypertrophic scar formation6) Arterial spasm7) Extensor tendon
sheath injury resulting in false cortical thumb8) Nerve injury of
the median, posterior tibial or femoral nerves
-
BLOOD EXTRACTIONARTERIAL BLOOD SAMPLINGCOMPLICATIONS5) Keloid
and hypertrophic scar formation6) Arterial spasm7) Extensor tendon
sheath injury resulting in false cortical thumb8) Nerve injury of
the median, posterior tibial or femoral nerves
-
]\
*and body temperature should be maintained and vital signs
monitored. *SET UP EXCHANGE TRANSFUSION*and body temperature should
be maintained and vital signs monitored. *and body temperature
should be maintained and vital signs monitored. *and body
temperature should be maintained and vital signs monitored. **Show
person in classWhy difficult to access elderly patientLaying
proneVeins of the lower extremities*Veins of upper
extremities****************