Embed Size (px)
DESCRIPTION
PEDIATRIC PROTOCOLS. Elana Pinchefsky, PGY-2 August 1 st , 2012. Outline. Protocols for: Seizures Headaches and migraines Tics and tourette syndrome Therapeutic hypothermia. Seizures. Febrile Seizures. Classification :. Febrile Seizures. Occur in 3-5% of children - PowerPoint PPT Presentation
Citation preview

PEDIATRIC PROTOCOLS
Elana Pinchefsky, PGY-2August 1st, 2012
Outline
Protocols for: Seizures Headaches and migraines Tics and tourette syndrome Therapeutic hypothermia

Seizures

Febrile Seizures
Simple Atypical/Complex (25-30%)
Generalized Focal
Brief
<15 minutes
Prolonged
>15 minutes
(status epilepticus)
Isolated
1 seizure/24 hrs
Multiple
> 1 seizure/24 hrs
Normal development & neurological exam
Abnormal neurodevelopment before seizure
Classification:
Febrile Seizures
Occur in 3-5% of children Between 6 months – 6 years
peak age 18-24 months Antipyretics make the child more comfortable, they do not prevent recurrent FS
High recurrence: 1/3 1/2 if less that 1 y.o. 10% of children experience 3 febrile seizures Factors that increase risk of recurrence:
Young age at time of first febrile seizure (<18months)
Family Hx of febrile seizures Relatively lower fever at the time of the initial seizure
Short duration of fever before the initial seizure (<1 hr)
Complex features
Febrile Seizures
Risk of developing epilepsy in general population: 1/200 If simple febrile seizures 1/100
risk of epilepsy if: Complex features Neurodevelopmental abnormality before the first seizure
Family history of afebrile seizures
Short duration (<1 hour) of fever before seizure
Risk of epilepsy increased with the presence of each atypical feature: 1 atypical feature – 3%
2 atypical features – 6%
3 atypical features – 9%
4 atypical features – 12-15%

Febrile Seizures
Febrile Seizures. BMJ. 2007
Febrile Status Epilepticus 5% of all cases of febrile seizures 25% of all childhood cases of status epilepticus More likely to have focal features Compared with afebrile SE – does Not lead to new death
or disability Association with MTS and MTLE No causal data
Treatment similar to SE, generally rapid response to Tx
Ismail et al. Saint-Justine (2012, article in press) Phenytoin is rarely effective in controlling febrile SE
Phenytoin alone was effective in treating only 14.5% of FSE (but 45% nonevaluable)
40% did not respond to Dilantin Sz duration was 2x longer when phenytoin failed (52.8 vs 109.9 min)
Sodium channel mutations (SCN1A) have been linked to atypical febrile sz may limit efficacy of Na channel blockers

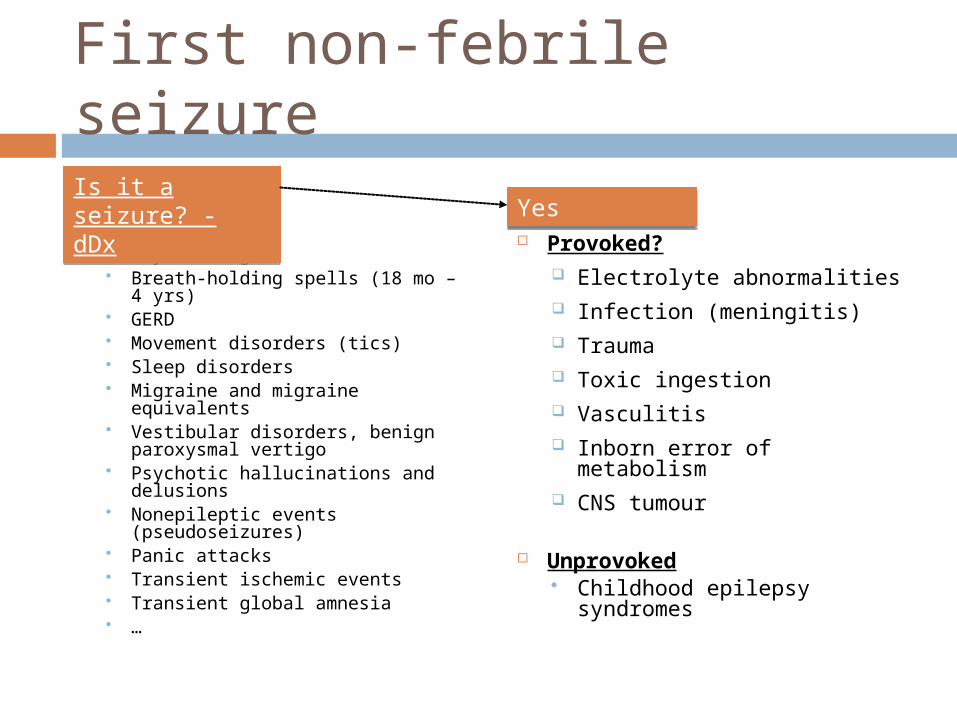
First non-febrile seizure
Syncope Daydreaming Breath-holding spells (18 mo
– 4 yrs) GERD Movement disorders (tics) Sleep disorders Migraine and migraine
equivalents Vestibular disorders, benign
paroxysmal vertigo Psychotic hallucinations and
delusions Nonepileptic events
(pseudoseizures) Panic attacks Transient ischemic events Transient global amnesia …
Provoked? Electrolyte abnormalities
Infection (meningitis) Trauma Toxic ingestion Vasculitis Inborn error of metabolism
CNS tumour
Unprovoked Childhood epilepsy syndromes
Is it a seizure? - dDx
Is it a seizure? - dDx
YesYes

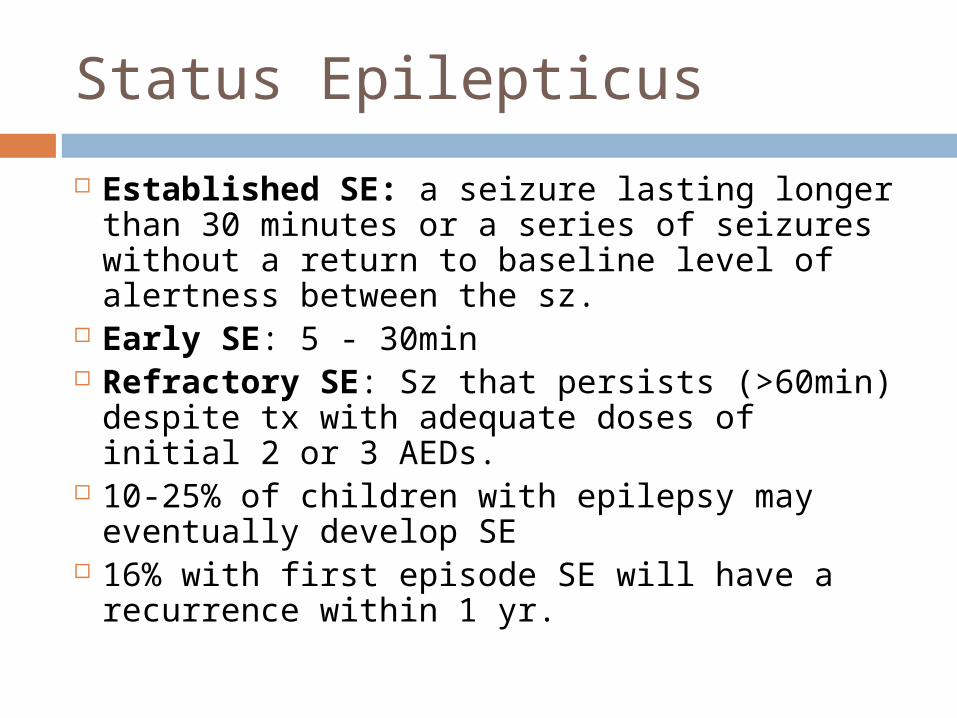
Status Epilepticus
Established SE: a seizure lasting longer than 30 minutes or a series of seizures without a return to baseline level of alertness between the sz.
Early SE: 5 - 30min Refractory SE: Sz that persists (>60min) despite tx with adequate doses of initial 2 or 3 AEDs.
10-25% of children with epilepsy may eventually develop SE
16% with first episode SE will have a recurrence within 1 yr.
Status Epilepticus
Lambrechtsen et al. (2008) Sz were terminated by a 3rd AED in 100% when administered within 60 min of the 1st AED Only 22% if >1hour after the initial AED
If 3rd AED within an hr of Tx initiation – return to baseline significantly more often than when delayed (81% vs. 0%)

Status Epilepticus
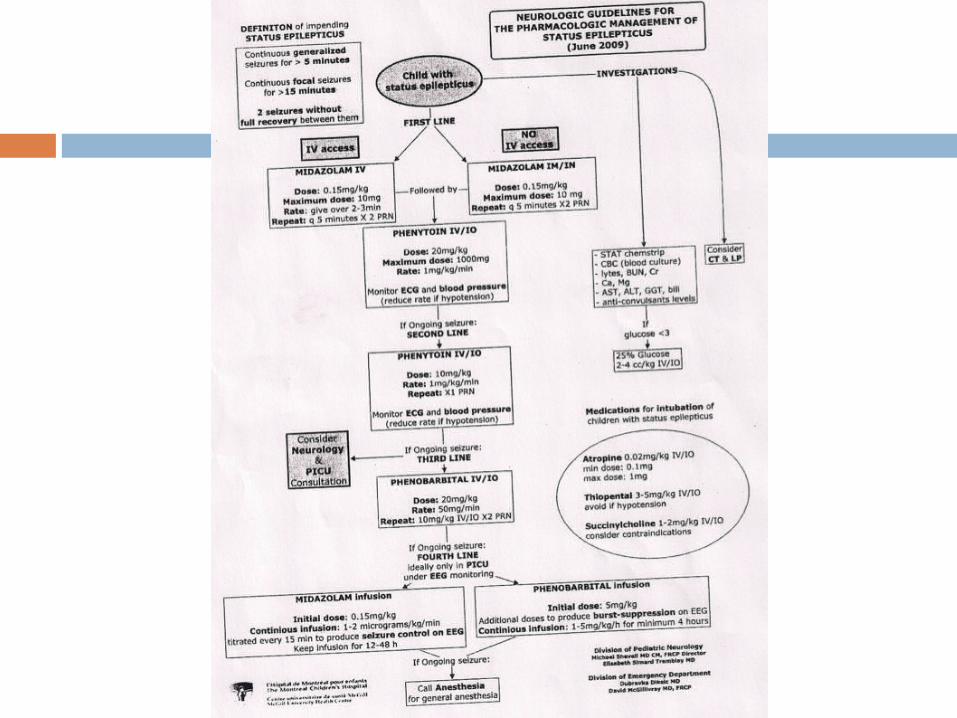
ABCs, O2, glucose, temperature, monitors, IVs, labs (CBC, CBG, electrolytes, Ca, Mg, PO4, BUN/Cr, LFTs, AED levels).
Consider toxicology, blood cultures, CT head, LP.
Initial management Benzodiazepines (effective in 30-40%)
Midazolam IV/IN/IM 0.15 mg/kg. Max 10 mg
Lorazepam IV/PR 0.1 mg/kg. Max 8 mg/12h or 0.1 mg/kg/12h IV/PR
Repeat q5 min. x 2 PRN If ongoing seizure Phenytoin 20mg/kg IV/IO. Max 1000mg
Status Epilepticus
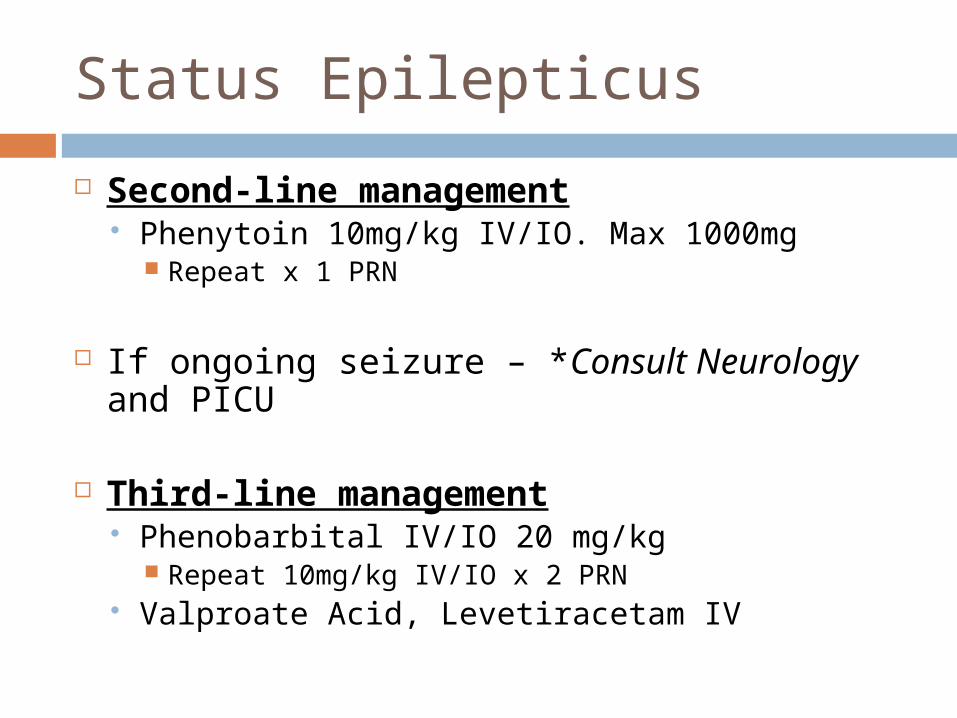
Second-line management Phenytoin 10mg/kg IV/IO. Max 1000mg
Repeat x 1 PRN
If ongoing seizure – *Consult Neurology and PICU
Third-line management Phenobarbital IV/IO 20 mg/kg
Repeat 10mg/kg IV/IO x 2 PRN Valproate Acid, Levetiracetam IV
Status Epilepticus
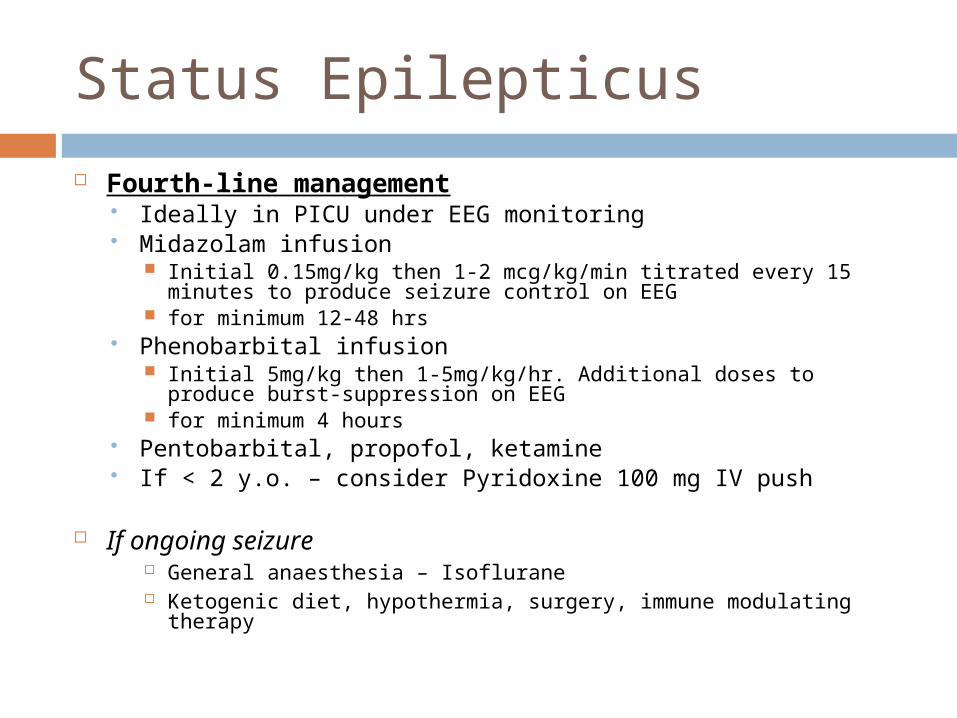
Fourth-line management Ideally in PICU under EEG monitoring Midazolam infusion
Initial 0.15mg/kg then 1-2 mcg/kg/min titrated every 15 minutes to produce seizure control on EEG
for minimum 12-48 hrs Phenobarbital infusion
Initial 5mg/kg then 1-5mg/kg/hr. Additional doses to produce burst-suppression on EEG
for minimum 4 hours Pentobarbital, propofol, ketamine If < 2 y.o. – consider Pyridoxine 100 mg IV push
If ongoing seizure General anaesthesia – Isoflurane Ketogenic diet, hypothermia, surgery, immune modulating therapy

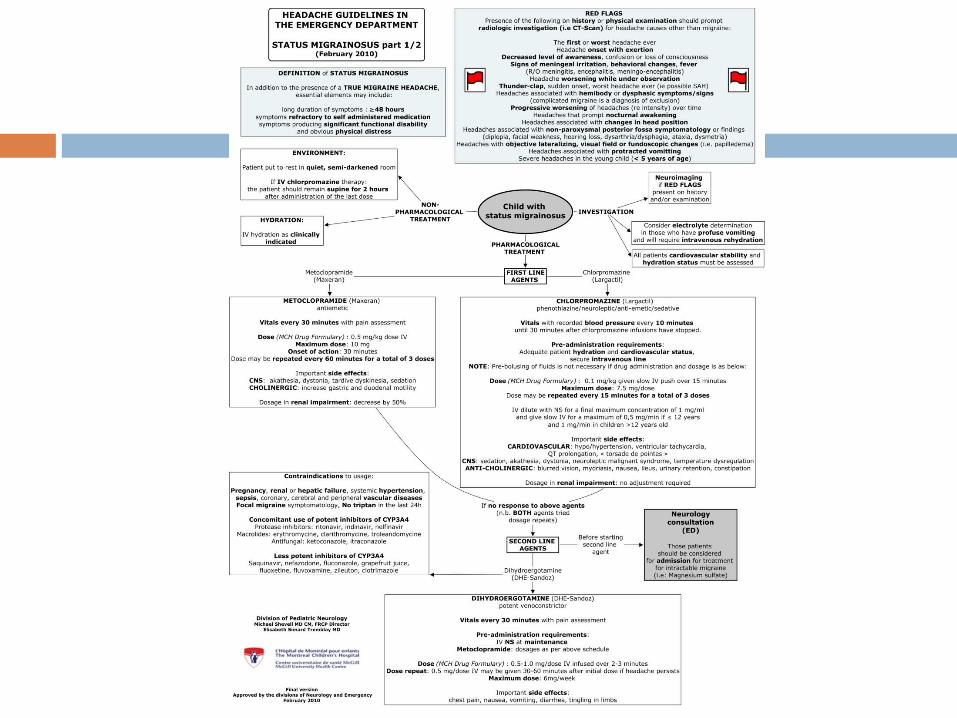
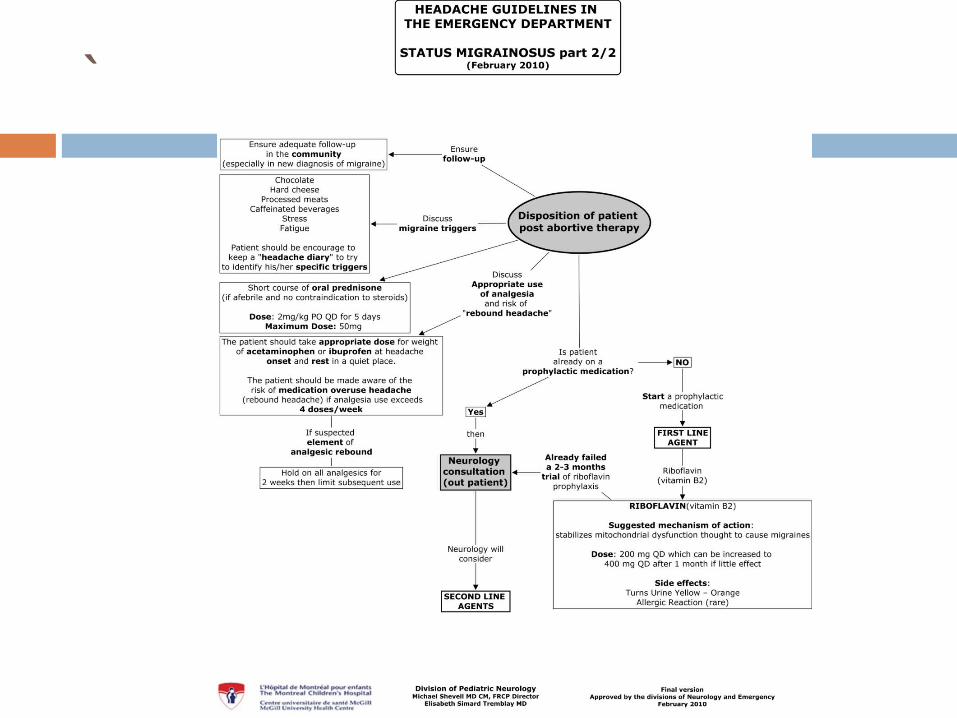
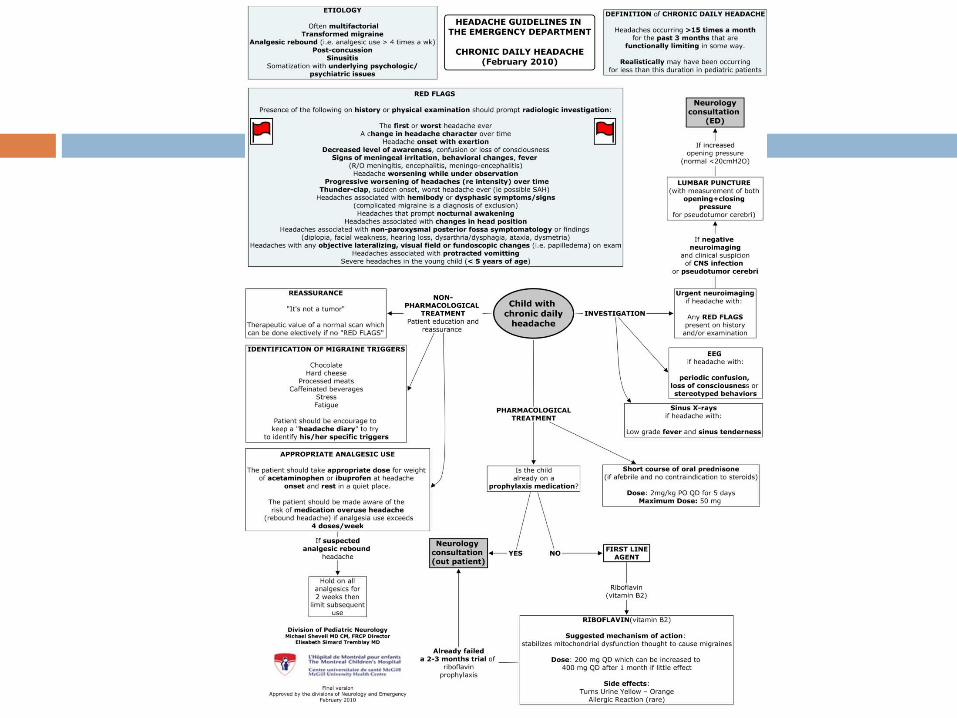
Headaches and Migraines

Migraines Prevalence:
3 to 7 years 1 to 3 % ♂ > ♀
7 to 11 years 4 to 11% ♂ = ♀
> 15 years 8 to 23% ♀ > ♂
Peak Incidence: Migraine with aura
♀: 12-13 yo (14/1000 person-yrs)
♂: 5 yo (6.6/1000 person- yrs)
Migraine without aura ♀ 14-17 yo
(19/1000 person-yrs)
♂: 10-11 yo (10/1000 person- yrs)
After age 10 ♀ > ♂(~puberty)
After age 10 ♀ > ♂(~puberty)
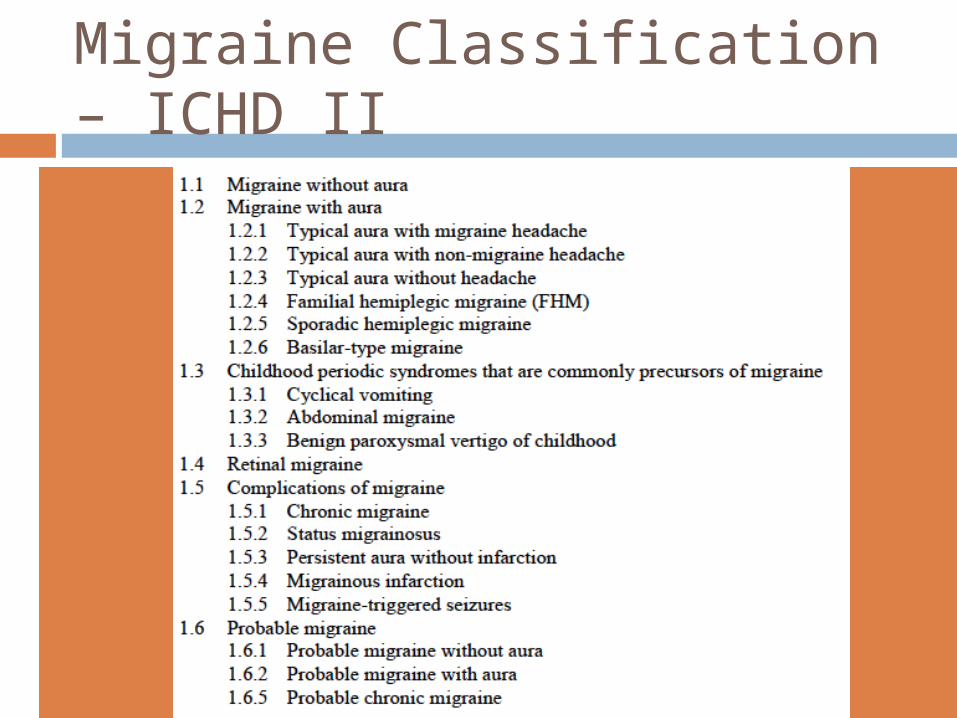
Migraine Classification – ICHD II
Migraines
Migraine without aura – (60-85%) most frequent
Migraine with aura – (15-30%) Typical aura: visual disturbances, distortions or obscuration before or as the headache begins that start gradually and last for several minutes Binocular visual impairment w/ scotoma (77%) Distortions or hallucinations (16%) Monocular visual impairment or scotoma (7%)
Sudden images and complicated visual perceptions r/o benign occipital epilepsy
Rare in children: Typical aura with nonmigraine headache Typical aura without headache

Diagnostic Criteria
Pediatric Migraine without aura – IHS 2005A) At least 5 attacks fulfilling criteria B through D
B) Lasting 1 to 72 hoursC) At least 2 of the following:
Unilateral or bilateral frontotemporal (not occipital) Pulsating quality Moderate or severe pain intensity Aggravation by or causing avoidance of routine physical activity
D) During the headache, at least 1 of the following Nausea and/or vomiting Photophobia and phonophobia, which may be inferred from behavior
E) Not attributed to another disorder

Diagnostic Criteria Pediatric Migraine with aura – IHS 2005
A) At least 2 attacks fulfilling criteria B through DB) Aura consisting of at least one of the following, but no motor weakness:
1. fully reversible visual symptoms including positive features (eg, flickering lights, spots or lines) and/or negative features (ie, loss of vision)2. fully reversible sensory symptoms including positive features (ie, pins and needles) and/or negative features (ie, numbness)3. fully reversible dysphasic speech disturbance
C) At least two of the following:1. homonymous visual symptoms and/or unilateral sensory symptoms2. at least one aura symptom develops gradually over 5 minutes and/or different aura symptoms occur in succession over 5 minutes3. each symptom lasts 5 and 60 minutes
D) Headache fulfilling criteria B-D for 1.1 Migraine without aura begins during the aura or follows aura within 60 minutesE) Not attributed to another disorder
Migraines
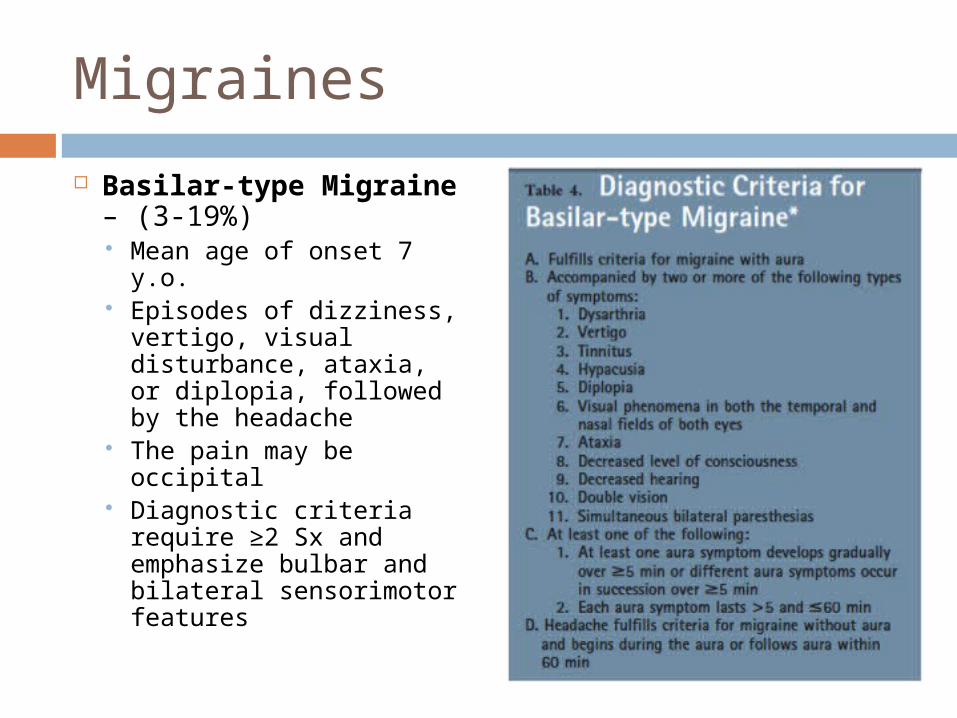
Basilar-type Migraine – (3-19%) Mean age of onset 7 y.o.
Episodes of dizziness, vertigo, visual disturbance, ataxia, or diplopia, followed by the headache
The pain may be occipital
Diagnostic criteria require ≥2 Sx and emphasize bulbar and bilateral sensorimotor features
Migraines
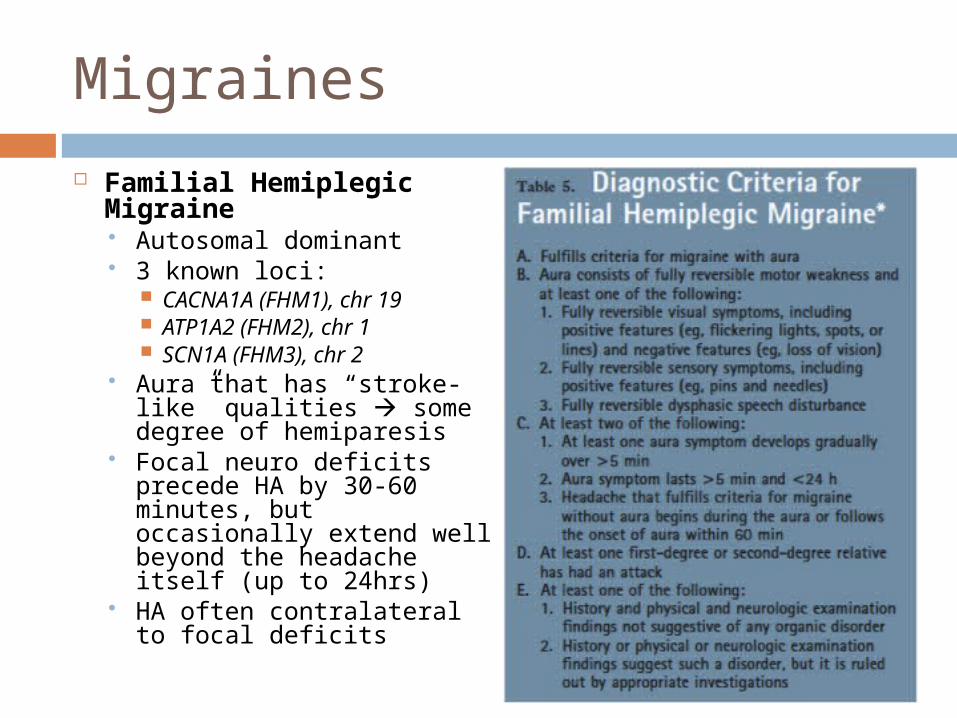
Familial Hemiplegic Migraine Autosomal dominant 3 known loci:
CACNA1A (FHM1), chr 19 ATP1A2 (FHM2), chr 1 SCN1A (FHM3), chr 2
Aura that has “stroke-like” qualities some degree of hemiparesis
Focal neuro deficits precede HA by 30-60 minutes, but occasionally extend well beyond the headache itself (up to 24hrs)
HA often contralateral to focal deficits
Migraine Equivalents – precursors of migraines
Benign paroxysmal torticollis Onset during infancy (2-8 mo.) Rare paroxysmal movement d/o or dyskinesia Attacks of head tilt alone or with V° & ataxia, lasting hrs to days Other dystonic features: truncal or pelvic posturing
Benign paraxysmal vertigo Onset in young children Abrupt and brief episodes (minutes to hrs) of unexplained unsteadiness
or ataxia Clusters that typically resolve with sleep
Cyclic vomiting syndrome Onset during childhood (~ 5 y.o.) ♂ = ♀ Recurrent episodes of intense vomiting w/ intervening wellness Recognizable by their stereotypical time of onset, duration and
symptomatology Regular q 2-4 wks, last 1-2 days, start in early morning
Abdominal migraine Onset in school-age children Episodic moderate-to-severe intensity vague, midline or periumbilical,
abdo pain lasting 1 to 72 hours associated with vasomotor symptoms (flushing, pallor) and N/V

Diagnostic Criteria


`

Tics and Tourette Syndrome
Tics and Tourette Syndrome Tics:
Stereoyped, intermittent, sudden, discrete, repetitive, nonrhythmic movements, most frequently involving head and upper body
Transient (1-12 months) or chronic (>12 mo) Transient motor tics in 25% of children
Tourette Syndrome: (1%, ♂ > ♀) Diagnostic criteria from DSM-IV-TR:
Both multiple motor and one or more vocal tics must be present at some time during the illness, although not necessarily concurrently
The tics occur many times a day (usually in bouts) nearly every day or intermittently over more than 1 year, during which time there must not have been a tic-free period of more than 3 consecutive months
The age at onset is younger than 18 years The disturbance is not due to the direct physiological
effects of a substance (eg, stimulants) or a general medical condition (eg, Huntington disease or postviral encephalitis)

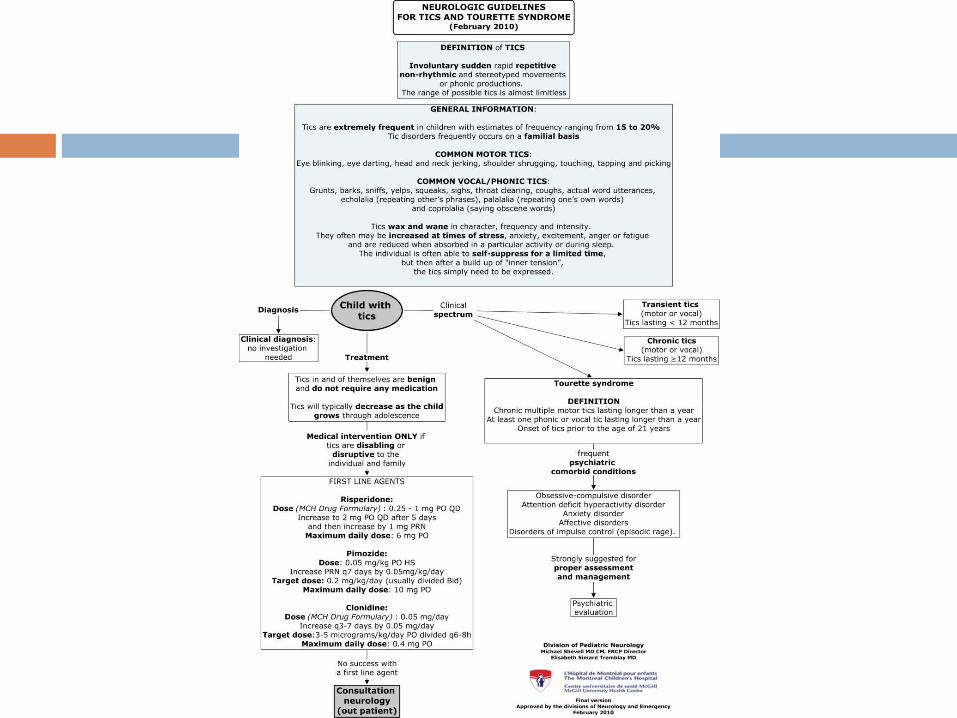
Tics and Tourette Syndrome

Tics and Tourette Syndrome

Therapeutic Hypothermia
Therapeutic Hypothermia
Standard of care for infants with moderate to severe HIE
Whole body cooling vs selective head cooling
Started before 6 hours of life - Before the secondary phase of energy failure
During 72 hours -until the end of the secondary phase of energy failure (48-72hrs)
At 33.5° (34° ± 0.5°) Amplitude-integrated EEG

Criteria for Cooling
≥36 wks and ≥1800g Cord pH ≤7.0 or base excess ≥-16mEq/L First hour of life CBG with pH ≤7.0 or base excess ≥-16mEq/L
Perinatal history of an event such as: placental abruption, cord prolapse, fetal bradycardia, shoulder dystocia…
Need for resucitation or ventilation >10 minutes after birth
Apgar ≤5 at 10 minutes Convulsions Clinical signs of HIE
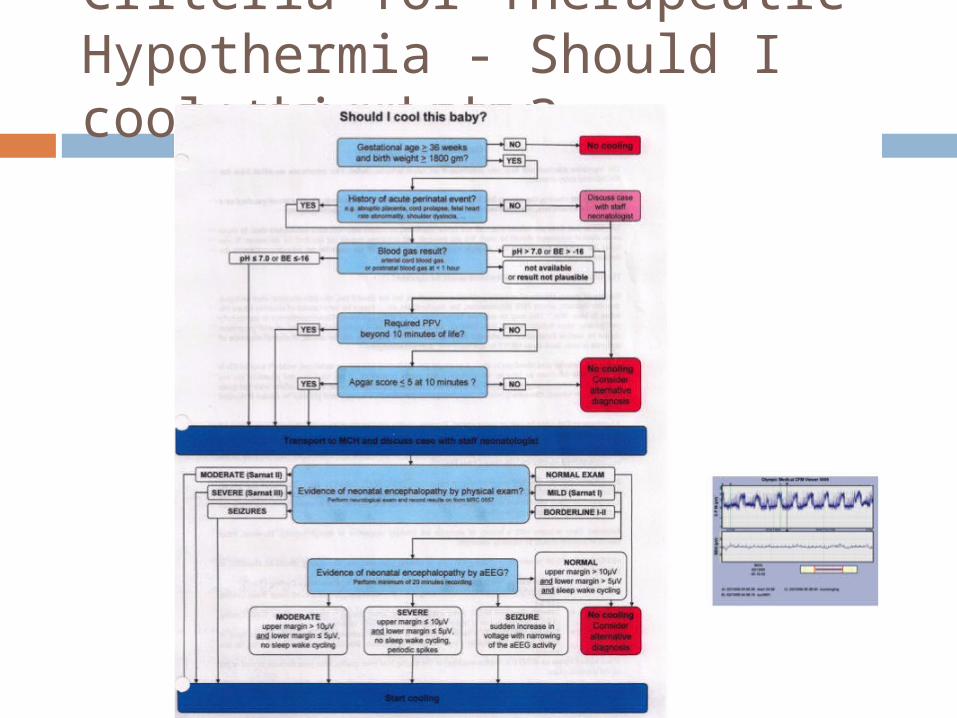
Criteria for Therapeutic Hypothermia - Should I cool this baby?

HIE clinical evaluation

Predictors of Outcome
1. Severity of the neonatal encephalopathy
2. Temporal evolution in clinical status over the first week of life
3. Presence of refractory neonatal seizures
4. Burst-suppression EEG pattern5. Qualitative impression of the severity of EEG changes
Thank You

References Ahmad et al. Febrile Status Epilepticus: Current State of Clinical and
Basic Research. Semin Pediatr Neurol. 17:150-154. 2010 Pediatrics In Review. Febrile Seizures. Vol. 18 No. 1 January 1,
1997 pp. 5 -9. Sadleir et al. Febrile seizures. BMJ. 2007 February 10; 334(7588):
307–311. Ismail et al. Lack of efficacy of phenytoin in children presenting with
febrile status epilepticus. American Journal of Emergency Medicine. 2012 article in press.
Lambrechtsen et al. Aborted and refractory status epilepticus in children: A comparative analysis. Epilepsia. Vol 49, issue 4, p. 615-625, April 2008.
Abend et al. Medical Treatment of Pediatric Status Epilepticus. Seminars in Pediatric Neurology 17:169-175. 2010.
IHS guidelines. http://www.ihs-headache.org/ihs_v3/user/code_public/guidelines_frame_access.asp?Allow=0&idSource=1
Stewart et al. Age- and Sex-specific Incidence Rates of Migraine with and without Visual Aura. Am. J. Epidemiol. (1991) 134 (10): 1111-1120.
Lewis D.W. Pediatric Migraine. Pediatrics In Review. Vol. 28 No. 2 February 1, 2007 pp. 43 -53.
H. Zinner and Jonathan W. Movement Disorders I: Tics and Stereotypies. Pediatrics in Review 2010; 31:223-233





























