-
7/29/2019 Pediatric&Minor Surgery Okt2008
1/63
BLOCK 14
SKILLS LABORATORY MANUAL
PAEDIATRIC EXAMINATION
ANDMINOR SURGERY
Faculty of Medicine
Universitas Gadjah Mada
Yogyakarta
2008
-
7/29/2019 Pediatric&Minor Surgery Okt2008
2/63
2 Block 14
Paediatric Examination & Minor Surgery
Skills Lab manual Block 14 : Pediatric Examination & Minor
Surgery
Author: Skills Laboratory
Faculty of Medicine Universitas Gadjah Mada
Contributors:
Pediatric Examination:Prof. dr. Soenarto, Sp.A(K)
dr. Amalia Setyati, Sp.A
dr. E. Suryadi, SU, PA, MHPE
dr. Santosa Budiharjo, M.Kes, PA
dr. Milana Widyasari
dr. Arum Tri Wahyuningsih
Minor Surgery
dr. Soenoko, SpB-KBTV
dr. E. Suryadi, SU, PA, MHPE
dr. Rizki Amalia Gumilang
Pre-print:
dr. Milana Widyasari, dr. Nine Luthansa, Siti Aisyah
Cover Design:
Siti Aisyah
Publisher:
Faculty of Medicine Universitas Gadjah Mada Yogyakarta
All right reserved - This book is protected by copyright
ISBN No. 979-26-1013-8
-
7/29/2019 Pediatric&Minor Surgery Okt2008
3/63
3Block 14
Paediatric Examination & Minor Surgery
CONTRIBUTORS:
Prof. dr. Soenarto, Sp.A(K)
Department of Paediatric, Faculty of Medicine,
Universitas Gadjah Mada
z
dr. Amalia Setyati, Sp.A
Department of Paediatric, Faculty of Medicine,Universitas Gadjah
Mada
z
dr. Soenoko, SpB-KBTV
Department of Surgery, Faculty of Medicine,
Universitas Gadjah Mada
z
dr. E. Suryadi, SU, PA, MHPE
Department of Anatomy, Embryology and Anthropology
Faculty of Medicine, Universitas Gadjah Mada
z
dr. Santosa Budiharjo, M.Kes, PA
Department of Anatomy, Embryology and Anthropology
Faculty of Medicine, Universitas Gadjah Madaz
dr. Milana Widyasari
Skills Laboratory, Faculty of Medicine,
Universitas Gadjah Mada
z
dr. Arum Tri Wahyuningsih
Skills Laboratory, Faculty of Medicine,
Universitas Gadjah Mada
z
dr. Rizki Amalia Gumilang
Skills Laboratory, Faculty of Medicine,
Universitas Gadjah Mada
-
7/29/2019 Pediatric&Minor Surgery Okt2008
4/63
4 Block 14
Paediatric Examination & Minor Surgery
PREFACE
It is very important for medical students to practice
clinicalskills, which are necesary for their future career as a
medical doctor.Medical schools are nowadays convinced that students
should masterthe skills before they make their contact with real
patients.Therefore, an early skills training is needed.
In the block 14, two topics of skills training are
PaediatricExamination & Minor Surgery. In this block, the
paediatricexamination only focused on heteroanamnesis.
The purpose of this book is to help students of the School
ofMedicine of Gadjah Mada University to prepare themselves for
theirclinical skills training. Particular emphasis is given to the
way aprocedure should be performed, including a step-by-step guide
onwhat students should do to be able to perform the
procedurecorrectly, though some related anatomic and physiology
issues arealso discussed briefly. A checklist is attached to help
students toassess their own performance, while also used as an
assessmentinstrument during the skills evaluation (Skills
Test).
We hope this book proves to be useful to students as well as
skills instructors who are involve in skills training.We greatly
appreciate the contribution of colleagues from various
departments for their willingness to participate in construction
ofthis book. We also express our sincere thanks to experts for
theiruseful comments and supports.
Skills Laboratory Team
-
7/29/2019 Pediatric&Minor Surgery Okt2008
5/63
5Block 14
Paediatric Examination & Minor Surgery
CONTENTS
Contributors..................................................................
3
Preface
.......................................................................
4
Contents
......................................................................
5
Pediatric examination
...................................................... 7
I.
Introduction.............................................................
7
II. The Unique of Paediatric
Examination.............................. 9
III. The Order of Examination Implementation
........................ 11
A. Anamnesis
.......................................................... 11
B. Physical Examination in Children
............................... 18
C. Physical Examination Data
....................................... 21
General
Examination.............................................. 22
Specific Examination
............................................. 28
Specific Examination in Neonates..............................
31
Appendix 1
...................................................................
34
Appendix 2
...................................................................
37
Medical
Record...............................................................
38
Simple Skin Suturing
........................................................ 42
General Objective
........................................................... 42
Specific
Objective...........................................................
42
Introduction
..................................................................
42
Required Instruments
....................................................... 43
Pincer.....................................................................
43
Needle Holder
........................................................... 44
-
7/29/2019 Pediatric&Minor Surgery Okt2008
6/63
6 Block 14
Paediatric Examination & Minor Surgery
Needle and Thread
..................................................... 45
Scissors...................................................................
47
Scalpel
....................................................................
49
Procedure for Wound Suturing
............................................ 50
Disinfecting Operation Area
.......................................... 50
Technique for Suturing Wound
....................................... 50
Making a Suturing Knot
................................................ 55
Removing the Suturing
................................................ 56
Reference
.....................................................................
58
Checklist
......................................................................
59
-
7/29/2019 Pediatric&Minor Surgery Okt2008
7/63
7Block 14
Paediatric Examination & Minor Surgery
PEDIATRIC EXAMINATION
I. INTRODUCTION
Making physical diagnose without laboratory examination,
basicallyrequires great care. The verbal and sense capabilities of
doctor areneeded to identify the manifestation of diseases by
finding the signs
and symptoms. The data that gain from history
taking/anamnesisand physical examination use to make diagnose,
therapy and prognosis
by a systematically and critical analysis.
There are two steps of activities in making physical
diagnose,that is data collecting and data analysis.
A. Data collecting
(1) Subjective Data
All information or data from patient whose seeking doctor
arenamed subjective data. Mastering in verbal capabilities
orcommunication skills and make a good rapport in the
interpersonal
relationship require to success in collecting subjective data.
The
subjective data are found and started from both
autoanamnesis/anamnesis and heteroanamnesis/alloanamnesis.
(2) Objective Data
All information or data obtained by physical examination
andlaboratory examination are called objective data. The techniques
ofphysical examination are inspection, palpation, percussion
andauscultation.
Inspection is a critical observation. To ensure accurate and
usefulinformation, doctors must approach inspection in a careful,
unhurriedmanner, pay close attention to details, and try to draw
logical
conclusions from findings.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
8/63
8 Block 14
Paediatric Examination & Minor Surgery
Palpation is test by touching. To enhance palpation
techniques,the hands can be used in different ways. The doctors can
takeadvantage of tactile sensitivity to each region of the hand.
The tipsand pads of the fingers can be distinguished texture and
shape best.The back or dorsal surface can be best feel for warmth.
The ulnarsurface, or ball of the hand (at the base of the fingers
on thepalmar) can be best feel thrills and fremitus. The thumb and
indexcan be assessed hair texture best, grasp tissues and fell for
lymphnode enlargement.
Percussion is a test using method of knocking on the surface
ofthe body using the finger to produce sounds. There is
characteristicsound produce by percussion on typical
location.Auscultation is hearing sounds from the inside of the
body. Sometimes,body sounds such as the voice, loud wheezing or
stomach growl canbe heard fairly easily, but you will need a
stethoscope to hear softerones.
At each steps of the motor activities, both in anamnesis
andphysical examinations, the doctor s mental aspect are always
neededto get involved, ex. critical and analytical thinking. How
does thecritical and analytical thinking perform? If a doctor were
in one step
to find information, this information should be thought
carefully andbecome basic information to emerge hypothesis. The
hypothesis isneeded to find for information and proved by it.
Each case has specific characteristic of the symptoms and
signsthat are different from another cases. Such as the symptoms
andsigns of fever are different from diarrhoea, confusing,
headache,paralyse, etc. Therefore, while collecting the data, the
doctor doesnot only ask many questions like filling a
questionnaire, but doingthe activity like a detective. A detective
solves a case by searchingmany relevant evidence. For example, a
rape case is directed thedetective to collect data from dirty bed
and bedcover, finger prints,loose hair, dried sperm, blood, broken
shirt or underwear; in other
-
7/29/2019 Pediatric&Minor Surgery Okt2008
9/63
9Block 14
Paediatric Examination & Minor Surgery
case, such as an engage in a gang fight, the information that
hasbeen collected are different from the rape case, so each case
needsdata that have meanings to solve the problem.
In paediatrics, especially in neonatal examinations, the
congenitaldefect should be observed critically. Such as neural tube
defect,hernia, external anogenital defect, schizis, cardiac
malformation,chromosomal malformation, etc.
B. Data Analysis
Analysis of data which done by a doctor is not only done
aftercompleting the data, but also as soon as the information
gained.Before the specific examination is done, the doctor must be
able tomake analysis and resume of the examination from data that
hasalready exist. By that, the doctor can diagnose the disease.
Only from the anamnesis and physical examinations, doctor
might
be able to define the clinical diagnosis correctly, such as
malnutrition,congenital defect, hemiplegia, paraparesis,
pharyngitis, abces, etc.Moreover, for certain diagnosis there might
be only data fromanamnesis that is needed, such as stress (caused
by fear of facingexamination, broken heart, etc) that is revealed
only by anamnesis.
The activities of collecting data and analysis involve:a. Motor
activities, such as anamnesis and examinationsb. Mental activities,
such as readiness and capabilities to make
perception of the facts found, then critically make
conclusion(temporary) and policies to step forward
c. Intellectuality capabilities about related theoretically
conceptsthat has to be mastered firstly and capability to
analyse.
II. THE UNIQUE OF PEDIATRICS EXAMINATION
The conceptual and medical techniques perpertives, to
makephysical examination in paediatrics, basically, is similar as
in adult.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
10/63
10 Block 14
Paediatric Examination & Minor Surgery
There are unique or specific techniques of paediatric
examination,such are:1. The pattern and manifestation of disease is
different from adult,
therefore, appropriate history taking and physical
examinationsare needed.
2. Sometimes in paediatrics, history taking based on
hetero-anamnesis, the child s feeling is not always same with the
parentscomplaint. Mothers have more subjective or over describing
thesigns and symptoms caused by their worry, and hope that the
doctor might gave effective drugs.3. Paediatrics examinations
need more attention, mastering in skills,
and patience.4. Children patient often uncooperative (crying,
struggle to get
loose), so many examinations can not be done, such as executethe
reflex; inspection of the conjunctivas mucosa and auscultatethe
heart sounds.
5. The order of implementation of the examination is
modified;such as the head examination is the last, usually head
examinationmake the children afraid. Auscultation of the heart
sounds isdone in the beginning.
6. The method to execute percussion is more gently and
weakly,because the wall of body cavities are thin.7. The axillar
regio is an important site in auscultating the thorax,
both right and left side, which are the lateral side of
thoracicwall.
8. The equipment of examination is fitted with body or part
ofbody size, such as the head of stethoscope (especially for
baby),size of manset (appropriate with length of upper arm),
weightbeam, stadiometer, infantometer, tape, etc.
9. There are different reference in normal range compared to
theadult normal range, both laboratory and others; such as
bloodpressure, Hb, Hmt, body part ratio.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
11/63
11Block 14
Paediatric Examination & Minor Surgery
10. Many signs or patognomonis sign are different between
childrenand adult, such as the criteria of neonatal sepsis is
specific, thatare differ with criteria in adult; in tetanus
neonatorum,contraction of masseter muscle is like fish mouth, not
as risussardonicus.
III. THE ORDER OF EXAMINATIONS IMPLEMENTATION
A. ANAMNESIS
The medical student should be practiced to take anamnesis,
notjust ask many questions to the patient or parents with the list
ofquestion (questionnaire) but how to ask patient and make
questionsso its answers become in order or in sequence on the right
trackwhich is appropriate the illness history of patient.The main
objectives of anamnesis are:a. Reconstruct the history of disease
that is suffered by patient. If
the data have obtained clearly and meaningfully, it could be
usedto analyse toward diagnosis. The knowledge of natural history
of
diseases concept is as important as prior knowledge.b. Reveal
the risk factors that relevant for diagnosis, prevention,
and prognosis.c. Knowing the efforts of treatments that already
had given by
self, doctor, alternative medicine, and how does the effects
ofits treatments. If the past therapy given by doctor or
paramedic,furthermore the information are 1) analysed and
interpretatedto know the diagnosis that already been made and also
kind ofeducational therapy.2) whether the last therapy is a
specificdrugs regimen for the disease, such as regimen for
tuberculosis,diabetes mellitus, rheumatic fever, asthma, etc. 3)
Are therespecific advise that already given, such as should regular
control,
allergic manifestation, seizure, etc.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
12/63
12 Block 14
Paediatric Examination & Minor Surgery
The content of data in paediatrics anamnesis are:1. Identity:
The patients identity: data and place of birth;
nickname, particularly for those between 2 and 10 years of
age.The parent s identity: first name of parents (and last name
ofeach, if different), their occupations, and where they may
bereached during work hours, and also the identity of someonewho
give information in anamnesis.
2. The history of the present illness, consists of:z The chief
complaint and present illness history.
- Chief complaints. These are the one or more symptomsor other
concerns for which the patient is seeking for
care or advice. Make sure whether these are concerns ofthe
patient, the parent(s) or both. In some instances athird party,
such as schoolteacher, may have expressedconcerns about the
child.
- Present illness history amplifies the chief complaints
andgives a full, clear chronological, account of how each ofthe
symptoms developed and what events were relatedto them. These are
included describing of illness, describingthe signs and symptoms,
the treatments, and the same
past illness. Should include how each member of the
familyresponds to the patients symptoms, their concerns aboutthem,
and whether the patient achieves any secondarygains from the
illness.
z The family illness and the pedigree of patient.Such congenital
and genetic disorder have social-culturalbackground or familial.
Marriage with close relative(consanguine) between the parents,
diseases present in thefamily (allergy, cardiovascular diseases,
DM, cancer, epilepsy,etc.) should be asked, in order to find the
relation withpresent illness.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
13/63
13Block 14
Paediatric Examination & Minor Surgery
z Anamnesis of the body systemSearching for the anamnesis of
body system has to be relevant
with the chief complaint and suggestion of the final
diagnosis,
including the differential diagnosis.
Basically, the systems of the human body are divided into
seven systems. These are systems of the body and symptoms
that usually accomplished by the patient according to the
system.
1. Cerebrospinal system: headache, nervous, vertigo,tremor,
etc.
2. Cardiovascular system: palpitation, weakness, cyanosis,
etc
3. Respiratory system: cough, sneezing, dyspneu, snoring,
sputum, etc
4. Gastrointestinal system: nausea, vomits, constipation,
diarrhoea, gripes (colic), puffy, etc.
5. Urogenital system: red urine, pain, pus, etc.
6. Integumentum system: white pimply, red pimply, ulcer,
swelling, etc.
7. Musculosceletal system: paralyse, pareses,
deformity,swelling, fracture, etc.
3. Personal history
z The history of intrauterine (antenatal) care, labor and
postnatal care.
Birth history is particularly important during the first 2
years
of life and for neurological and developmental problems.
Hospital records should be reviewed if preliminary
information
from the parent(s) indicates significant difficulties
before,
during or after delivery.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
14/63
14 Block 14
Paediatric Examination & Minor Surgery
- Prenatal (antenatal care):
How many times does the mother visit the doctor during
pregnancy? Minimally, the mother should visit the doctor4 times
during pregnancy; once at the first trimester
(before week 14), once at the second trimester (beforeweek 28),
and twice at the third trimester (between
week 28-36 and before week 36). Ask about the vaccinethat she
got during pregnancy, especially tetanus toxoid,
and how many times the vaccine was administered. Askabout Fe
supplement during pregnancy.
Maternal health before and during pregnancy, includingnutrition
and specific illness related to or complicated by
pregnancy; dose and duration of all drugs taken duringpregnancy;
weight gain; vaginal bleeding; duration of
pregnancy; parental attitudes concerning the pregnancyand
parenthood in general and this child in particular.
- Natal care:
The history of natal care is including date and place ofbirth,
who was taking care of the delivery, whether it
was obstetrician or midwife, delivery process(spontaneous, cunam
extraction, vacuum extraction,
caesarean section), multiple gestation, condition rightafter
delivery, and morbidity at the first day after birth.
The gestational age is also important to be asked, whetherit is
preterm, aterm, or posterm. Respiratory effort
(Apgar score) after birth is also important to be asked,whether
the baby cry spontaneously or not. Birth weight
and length are important too. Morbidity related to thedelivery
and at neonates is should be asked, including
asphyxia, delivery trauma, intrapartum infection, icterus,etc.
that might be related to the problems appear present.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
15/63
15Block 14
Paediatric Examination & Minor Surgery
- Postnatal care:Regular visit to check the mothers and neonates
conditionand where it was done (hospital, community
healthcentre).
z The history of feeding and conclusion of history in
nutritionstatus.Feeding history is particularly important during
the first 2years of life and in dealing with problems of under-
andovernutrition. In the feeding history we can ask about the
foods that has been consumed by the child before ill (shortterm)
or since infancy (long term). Then measure about thequality and the
quantity, whether it is enough or less accordingto the nutrition
value.- Infancy:
o Breastfeeding: frequency and duration of feed, use
ofcomplementary or supplementary artificial feeding,difficulties
encountered, timing and method ofweaning.
o Artificial feeding: type, concentration, amount, andfrequency
of feeds, difficulties (regurgitation, colic,
diarrhoea) encountered, timing and method ofweaning.o Solid
foods: types and amounts of baby foods given,
when introduced, infants response, introduction ofjunior and
table foods, self feeding, parental and infantresponse to feeding
process.
- Childhood:o Ask about the supplement food, the age when it
was
given first, the type, the amount, and the schedule.Parental
attitudes toward eating in general and towardthis childs under- or
overeating, parental response tofeeding problems (if present). A
diet diary kept over
-
7/29/2019 Pediatric&Minor Surgery Okt2008
16/63
16 Block 14
Paediatric Examination & Minor Surgery
7- to 14- day period may be required for an accurateassessment
of food intake in childhood feedingproblems.
z Growth and Developmental HistoryParticularly important during
infancy and childhood and indealing with problems of delayed
physical growth,psychomotor and intellectual retardation, and
behaviouraldisturbances.- Physical growth: actual (or approximate)
weight and
height at birth and at 1,2,5, and 10 years; history of anyslow
or rapid gains or losses; tooth eruption and losspattern.
- Developmental Milestone (see app. 1): for children lessthan 5
years old we have to ask about some developmentalmilestone in gross
motor, fine motor, personal-social, andadaptive-language. For the
school age, the developmentalcould be assessed grossly by
evaluating their study result,i.e. if the child is too old in its
class or fail to pass theclass for several times, it could lead us
to cognitivedevelopmental disorder. We need to ask about the
menarche and telarche (girls), also the age when pubichairs
appear. Disorder in this developmental is oftenrelated to
endocrinology disorder. In assessing thedevelopmental history, we
should ask whether there werebehavioural and emotional disorder.
These conditions areusually has background of purely emotional
(anorexianervosa in teenagers) or organic (hyperactivity in
childrensuffered from attention deficit disorders).
z The history of immunizationIt is important to ask about the
immunization status, thebasic immunization or booster, especially
BCG, DPT, Polio,Measles and Hepatitis-B, and also another
immunization, such
-
7/29/2019 Pediatric&Minor Surgery Okt2008
17/63
17Block 14
Paediatric Examination & Minor Surgery
as MMR, hepatitis-A, and Hib. Those immunizations have to
be asked in order to know the paediatric protection and also
could help to diagnose. (See app. 2)
Specific dates of administration of each vaccine should be
recorded so that an ongoing booster programs can be
maintained throughout childhood and adolescence. Any
untoward reactions to specific vaccines should also be
recorded.
z The history any kind of past illness.The past history explores
prior illness, injuries, and medical
interventions while the current health focuses on the
present
state of health and on environmental conditions, personal
habits, and health-related measures that may impinge on it.
z Social-economic and environment state.
The important things about the environmental conditions
are the house conditions, how many people leaving in the
house and with whom the child lives with, location
(downtown, suburb, or village), surroundings, the
sanitation,
etc. Is there anybody ill in the house?
There are lots of conditions that cause morbidity andmortality
related to social economic and environment, such
as malnutrition and tuberculosis.
After finishing the anamnesis and making analysis, we can
take
summary (resume anamnesis) as a base data to make
hypothesis.
The data or hypothesis from anamnesis is needed to choose or
define
priority steps of the examination or give more attention in
physical
examination.
In emergency case, while the first aid/therapy is done, the
anamnesis can be taken.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
18/63
18 Block 14
Paediatric Examination & Minor Surgery
B. PHYSICAL EXAMINATION IN CHILDRENA. General examination:
1) General condition: apparent state of health,
nutritionalstatus, level of consciousness, posture, activity, and
otheraspects that can be seen at a moment.
2) Skin and mucosa examination3) Lymph node examination4)
Musculosceletal system examination5) Vital sign examination
B. Specific examination:1) Head examination (in children, it is
usually done later)2) Thorax examination: thorax in general, heart,
lung3) Abdomen examination4) Anogenital examination5) Extremities
examination6) Neurological and reflexes examination
Physical examination in children needs more preparation
thanthose in adults, because sometimes children are not cooperative
tobe examined. In order to keep the children being cooperative
during
examination, and because the parents usually watch the
examinationprocess, we (as a doctor) have to perform a good
examination skillin an effective way. Therefore, it is very
important to master thetheoretical concepts and practice the
skills.
1. INSPECTION
Inspection means watch carefully with naked eyes or
withinstrument (loupe). Usually, this is the first step of
examination.Inspection can be done to all over the body, or just
a/severalpart(s) of body.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
19/63
19Block 14
Paediatric Examination & Minor Surgery
2. PALPATIONPalpation means a way of examination using sense of
touch(propioceptive). The most sensitive part to touch is usually
thevolair surface of fingers, with or without palm; and the
mostsensitive parts to sense the temperature are the dorsal parts
offinger II-IV.
a) With palpation we can:- feel the senseof body temperature
(with dorsum fingers),
skin surface (with volair fingers surface), skin lesions- feel
vibration (with palm or volair fingers): ictus cordis,
vocal fremitus- find intra abdominal mass (hard, springy, or
soft), the
edge and surface of liver, splenomegaly, tumor, full bladder-
find sub cutis mass and its size estimation: lipoma, position
of testis (in scrotum or in canalis inguinalis) with volairside
of finger II, III, and IV, abscess (fluctuation)
- tenderness (with volair side of finger II-III/IV),
defensemuscular (volair side of finger II-IV)
b) The technique of palpation in children is similar with those
inadults. At normal and cooperative children, abdomenpalpation can
be done easily because the abdomens wall isthin, and so do the sub
cutis tissue.
3. PERCUSSIONPercussion is a test using a method of knocking on
the bodysurface using the finger, to detect mass under the body
wall.The sounds that can be produced by percussion are:* Flatness :
indicates solid mass under the body wall (bone,
muscle; usually it is not done)* Dullness : indicates massive
mass under the body wall
(liver, solid tumor, cyst, fluid)
-
7/29/2019 Pediatric&Minor Surgery Okt2008
20/63
20 Block 14
Paediatric Examination & Minor Surgery
* Resonance : indicates aerogen mass under the body wall(normal
lung tissue)
*Hyper-resonance : over resonance sound*Tympani : indi cates air
under the body wall
(abdomen)
The technique of percussion in children is similar with those
inadult, but usually we knock gentler. Percussion can be done
by
knocking the left middle finger between phalanx II and III, with
theright middle finger. To look for the borders of heart, we have
to
identify the sound changes from resonance to relative dullness.
It issometimes difficult to find a small amount of fluid (ascites
or effusion)
by percussion.
4. AUSCULTATION
The aim of auscultation is to listen the sounds of organs
activity
(in the body), like heart, lung, and gastrointestinal
tract.Auscultation in children needs specific stethoscope with
suitable
membrane or bell size. For children, we can use bell with
diameter1 inch or membrane with diameter 1,2-1,5 inches. For
neonates,
especially for low baby birth weight, we need smaller diameterof
bell or membrane. We have to choose the suitable earpiece,
so it can completely cover the external acoustic meatal. It
issaid that stethoscope is specific for each examiner, so if
they
use different stethoscope, it will decrease the sensitivity
indetecting the sounds.
Auscultation technique in children is similar with those in
adult.Give special attention to these points:
z Chest auscultation- Perform the heart auscultation first, and
then lung
auscultation, especially for uncooperative children
-
7/29/2019 Pediatric&Minor Surgery Okt2008
21/63
21Block 14
Paediatric Examination & Minor Surgery
- Dont forget to listen vascular murmur, if there is
anindication
- Listen carefully to the sound of normal heart first, andthen
listen to the murmur. If you find murmur, listencarefully to get a
detail description. Do the same waywith lung auscultation.
z Abdomen auscultation- Do auscultation first before
percussion
C. PHYSICAL EXAMINATION DATAThe important keys of physical
examination in children compare
with those in adult are:- there is possibility to find
congenital anomaly, especially in
neonates- there is possibility to find abnormality caused by
growth disorder
that is influenced by risk factors.The abnormalities:z several
of those can be found at general examination:
- many clinical syndrome: like Down syndrome, Hurler
syndrome,hypothyroidism
- many growth disorders: like labioschizis, cretinism,
progeria,achondroplasiaz several of those can be found at specific
examination:
- anatomical abnormality/external morphology:
gnatho/palatoschizis, hernia, anus imperforates, retentio testis,
fingersabnormality, spina bifida, etc.
- internal organ abnormality: congenital heart disease,
herniadiaphragmatica, intra abdominal cyst, etc.
Several of those disorders can be found easily from history
taking(both of internal and external organs), like labioschizis,
gastroschizis,hernia, stenosis pylori, total biliary
obstruction.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
22/63
22 Block 14
Paediatric Examination & Minor Surgery
Besides, a carefully-history taking about the history of
diseasecan lead us to the diagnosis. Therefore, a carefully-history
takingsimplify us to pay attention to specific examination.
GENERAL EXAMINATIONGeneral examination lead to find data about
patient condition
generally, about anatomical-morphological and functional.
Commonly,general examination begins by enclosing entirely
inspection withoutmanipulation. This examination is important
to:
a. Ascertain the anatomy of the body generally and the
morphologyof the body.
b. Obtain trace of psychological related to patient suffering.c.
Obtain trace, even conclusion, about motorist status.
Hearing with ear and smelling with nose without
instrument(breathing sound/coughing sound and abnormal smell) have
to bepracticed, because they can give important information.Things
that need to be attended:a. General condition: in this step of
examining, identified briefly
about signs that appear immediately; those signs will be
described
specifically later in the related organ, if there are
indications.1. Ability to recognize general appearance of a patient
aboutthings that immediately recognized needs to be
practiced;sometimes this appearance often gives diagnostic
guidanceor condition, which needs immediate treatment.a) Appearance
of severe illness/suffering: this evaluation
primarily to ascertain immediate management: such aslying down
immediately, analgesic, tranquillizer,anticonvulsant, etc. If
necessary ascertain Karnofsky score
b) Breathing abnormality: dispneu, apneu, takhipneu,brakhipneu,
hiperpneu/hyperventilation, Cheyne-Stokes,Biot, stridor,
wheezing.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
23/63
23Block 14
Paediatric Examination & Minor Surgery
c) In general appearance we can estimate the abnormality ofthe
sounds (without stethoscope): crying sounds (cramping,cri du chat,
very weak cry), grunting, speech disorder(aphoni, aphasia, dumb,
hoarseness in laryngitis, nasal soundin palatum molle paralyze),
cough (pertussiform)
d) Compulsory position (orthopneu in asthma, heart
failure,appendicitis)
e) Abnormality of moving (paralysis, hemiparesys,
tremor,balismus, chorea, atetoid, hahnen Tredgang, wide base
gait,
convulsion, etc.)
b. Skin and mucosa examinationThe examinations are:1.
Inspection:
a) Pigmentation (white, yellow, chocolate, black).b) Color
alteration (pale, reddish, vitiligo, rash, bleeding):
children with high prevalence of anemia, there are lots
ofpediatric diseases with rash, petechia (and other
bleedingmanifestation) are not too common in children,
icteric,venectasia, caput medusae, telangiectasia.
c) Cyanosis (extremity, general)d) Edema (local,
general/anasarca), skin lesion (squama,lichenification, scar, skin
tumor).
e) Mucosa: pale, hyperemia, koplik spot, Bitot spots in
sclera.2. Palpation:
By palpation we can examine:a) Skin condition: temperature, skin
humidity, skin surface,
skin turgor sub dermal condition, edema, (springy,scleredema or
pitting edema), skin elasticity, tumor (hard scar; springy
lymphoma; fluctuate cyst, abces).
b) Skin sensation (Hypesthesia, normal, hyperesthesia) in
children is difficult to measure.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
24/63
24 Block 14
Paediatric Examination & Minor Surgery
Skin examination technique in pediatric is similar to the adult.
If
there is bleeding tendency, it might be needed tourniquet
test
(Rumple-Leede test). If there is skin lesions, such as red
spotting on
the skin, make sure whether it is petechia, telangiectasias,
rash in
Henoch-Schonlein syndrome, or other kind of rashes.
c. Lymph node(s)
The primary examination is palpation: enlargement (local,
general), single, multiple, size, inflammation. Examining
supraclavicular lymph nodes in children is important, because
ofthe high prevalence of pulmonal TB in children. Regional
lymphadenopathy suggests us to find another disorder (tumor,
inflammation) in the drainage regio that is connected with
the
lymph nodes.
d. Examination of muscle, bones, and joint.
1. Muscle
zzzzz Muscle development describes the nutritional status of
the
children or atrophy in flaccid paralyze.
zzzzz Muscle tonus and strength are important to measure
severe
diseases.zzzzz Contracture
2. Bone: the developmental and anatomical, fracture, tumor,
tenderness.
3. Joint: anatomical joints, position, free movement/limited
movement, intraartikular swelling
(fluctuation)/periarticular,
inflammation signs, ankylosis.
e. Vital Sign Examination1. Pulse measurement, things that
should be described: frequency,
regularity, blood vessels filling and tension, pulse type
equality,
simetricity, femoral pulse compared to radial pulse:
-
7/29/2019 Pediatric&Minor Surgery Okt2008
25/63
25Block 14
Paediatric Examination & Minor Surgery
a. If the frequency isnt normal:
zzzzz Immediately think of paroxysmal tachycardia, flutter,and
fibrillation.
zzzzz Bradycardia think about heart block (SA or NA block)b. If
there is irregularity, measure specifically:
zzzzz Regular irregularity (bigemini pulse, trigemini
pulse).
zzzzz Irregular irregularity (deficient pulse at premature
beat,escape, sinus arrest, heart block)
c. If there is abnormality in blood vessels filling:
zzzzz High filling: pulsus magnus, pulsus celer
zzzzz Very low filling: pulsus parvus (et tardus), pulsus
filiformis.
zzzzz Inequality between pulses, remember parasistole,
pulsusalternans, pulsus paradoksus think to find otherevidence.
d. If there is asymmetrical:
zzzzz Right pulse isnt equal to the left pulse blood
vesselobstruction
zzzzz Femoral artery pulse weaker than the radial artery pulse
specific in koarktasio aorta.
e. Other types of pulse: pulsus dikorot, anadikrot.
Arrhythmia isnt uncommon in children:
zzzzz Supraventricular tachycardia in severe sepsis,
severegeneral condition.
zzzzz Pulsus filiformis (thready pulse) in shock, severe
hypo-
volemia.
zzzzz Heart block as complication of diphtheria.
zzzzz Pulsus deficient.2. Respiration: we should describe:
a. Frequency: tachipneu, bradipneu, apneu.b. Types: Biot
respiration, Cheyne-Stokes, Kuszmaul/hyper-
ventilation (in children with metabolic acidosis.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
26/63
26 Block 14
Paediatric Examination & Minor Surgery
3. Blood pressure:Normal blood pressure varies according to age
(look at thelist of time interpretation of blood pressure). The
techniqueis the same as the adult. Things that should be
noticed:zzzzz The child should be calm.zzzzz Manset size should be
proper, which covers two third of
the upper arm.zzzzz Use the membrane site in order that the
korotkoff has
low tone.
zzzzz If there is arrhythmia or inequality of pulse measurethe
blood pressure more conscientious.
zzzzz If the lower extremities are pale, cold measure thefemoral
blood pressure (koarktasio aorta ?).
f. Measurement of body weight, height, and
relevantparameters.Measurement of anthropometrics parameters in
children arevery important in order to give information about
thechildrens growth, even the childrens development.
1. Body weight: measurement of body weight in baby, even
more in baby with low birth weight need to use
accuratecounterweight, whereas for children or bigger baby, thebar
counterweight is enough. The bodyweight parameteris used to
ascertain nutritional status of the children.Alteration of
bodyweight may occur rapidly so that givesimage of Protein and
Energy Malnutrition (PEM) that isntoccur in chronic time, the
abnormality of height isntoccur yet:zzzzz 90%-110% body weight of
50 per centile NCHS : normalzzzzz 80%-90% body weight of 50 per
centile NCHS : PEM Izzzzz 60%-70% body weight of 50 per centile
NCHS : PEM II
-
7/29/2019 Pediatric&Minor Surgery Okt2008
27/63
27Block 14
Paediatric Examination & Minor Surgery
zzzzz < 60% body weight of 50 per centile NCHS :
- without edema : marasmic
- with edema : marasmic kwashiorkor
2. Height: measuring the childrens height needs to ascertain
their nutritional status. PEM that occur in a long time
causing the height lower than normal.
zzzzz For children who have been able to stand up, the
height
is measured by the scale stocked to the wall or pillar;the
ankles cling to the scale.
zzzzz For babies or children who have not been able to stand
up, the height measured by scale that is stocked to
the bar (woods, light metals); one of the bar with
border on that side and a shifter that can be moved
up and down to reach the vertex. The feet must be
900 to the lower leg; the knee joints and thighs are
extension, the foot-sole stick on the border at the
tip. The shifter moved a long the bar up to the vertex.
3. Circumferences:
zzzzz Head circumference: head circumference measurementmust be
done if there is appearance oh abnormality
(micro cephalic, macro cephalic, hydrocephalus) and
or morphological abnormality (the abnormal shape of
the head should be related to the diseases such as
dolicocephalic, brachicephalic).
Measuring technique: the soft scale tape twisted around
the head passing the forehead and promontorium.
zzzzz Middle arm circumference: middle arm circumference
is one of the anthropometrics parameters to ascertain
childrens nutritional status.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
28/63
28 Block 14
Paediatric Examination & Minor Surgery
Technique: with the usual tape or specific tape,
measure the middle of the upper arm; this parameterhas value if
there is no edema.
zzzzz Abdominal circumference is a practical way to
measureascites progression, even though its not accurate.Technique:
the tape is twisted through the umbilical,so that the techniques
equal at each measurement.
SPECIFIC EXAMINATION
Specific examination including part of the body (head,
neck,chest, abdomen, anogenital, extremity) also related organ and
thefunction. For the children, scary examinations should be done in
thelast of the meeting, in example head examination using
medicalequipment (light, otoscop, tongue spatula, etc).1. Neck
Examination
Several child examinations that needs special attention:- Lymph
nodal examination: enlargement of the supraclavicular
lymph, multiple, no inflammation sign suspect primary TBof lung,
especially in under nutrition.
- If there is any enlargement in the neck, make sure that is
parotid glands (usually enlargement under the ear) orenlargement
of the lymph glands (location can be any where)- Jugular vein
pressure examination for the baby is difficult.
2. Chest Examinationa. Chest wall examination
Morphology of the thorax can describe the condition aboutchest
wall and intrathoracal organ. Watch carefully about:emphysematous,
retraction, dada corong (often in obstructiveair way), pigeon
breast, cimetricity, vausseur cardiaque,costa, cimetricity of
movements, retraction (supraclavicular,suprasternal, infrasternal,
subcostal, intercostals). Palpation
-
7/29/2019 Pediatric&Minor Surgery Okt2008
29/63
29Block 14
Paediatric Examination & Minor Surgery
on between costal is important if there area any bulging.Chest
wall on children are commonly very thick, just needssmooth
percussions.
b. Heart examinationHeart examination should be done before the
lung.Auscultation needs carefully for detect the
congenitalabnormality.
c. Lung examinationIf there is an abnormality on chest wall
inspection, lung
examination should be done more carefully because itspossible
that the etiology was from the respiration system.While do
inspection on chest cimetricity, the position of thedoctor should
be in sagital area of patient leg. Comparingchest wall right and
left on children more easy because thesize of the lungs still
little, so it makes the examinationeasier for detect abnormality of
the lung. If there is anydifferences between right and left lung in
inspection,palpation, and auscultation it show abnormality in one
ofthe lung.
In auscultation, listen carefully sound of the breath
(vesicular/
bronchial, louder/ softer), after that find additional
sound.Auscultation under armpit is often easier for detecting
theabnormality of the lung. Stiffness in the lung
(infiltrate,compressive atelectase) produce bronchial sound
(expiratorysounds are louder and inspiratory sounds are
decrease),egophony, fremitus sounds increase in the superficial
areaof lung which is stiffing (sounds produced from the vocalcord
sound higher in pitch and on palpation feel increasefremitus). By
percussion produced dullness and by palpationproduced increase
fremitus sound. By inspection there is
might be a unilateral lag (or delay) of the respiratory
movement on the stiffing lung.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
30/63
30 Block 14
Paediatric Examination & Minor Surgery
3. Abdominal ExaminationAbdominal examination begins with
inspection followed by
auscultation and so on. Inspecting the abdomen should
beperformed as the thorax examination. In neonate, dont forget
to check the umbilical cord. If it has already released, make
surethat there are no granuloma or hernia.
The abdominal wall is the best area to examine skin turgor
andelasticity. Abdominal palpation in children is usually not
difficult
if the child is cooperative. The abdominal wall that looks
enlargemight shown meteorismus, liquid (cysts, acites,
hydronephrosis),
full vesica urinaria, or hard tumors
(organo-megaly,neuroblastoma, nephroblastoma, feces accumulation in
congenital
megacolon.In the shifting dullness examination, after the border
between
the tympani with the dullness has found, incline the patient
(thefinger that becomes the percussion base should not move fromthe
borderline), after that, percuse to the opposite direction.
The ascites examination by the undulation test is not sensitive
ifthe ascites liquid is just a little. Do not forget to examine
the
inguinal hernia.
4. Anogenital ExaminationThere are some congenital and
acquisital disorder at the
anogenital, which are:a. Congenital: external genital disorder:
scrotal hernia,
hypospadia, epispadia, undecended testis, hermaphodyte,ambiguous
genitalia, imperforate hymen, imperforate anus.
b. Acquisital: hydrocele, diaper rash, infection,
phymosis,paraphymosis.
Those anomalies should be paid more attention in baby.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
31/63
31Block 14
Paediatric Examination & Minor Surgery
5. Extremity ExaminationIn short trace about extremities sizes
could illustrate the childrensgrowth. Upper extremity circumference
is used to be one ofgrowth parameter. Pseudohypertrophy of lower
leg muscle inDMD (Duchene Muscular Dystrophy). Some morphological
disorderare present in congenital anomalies (pes
equinovarus/equinovalgus, phocomelia, syndactily and other finger
disorder,simian line,etc).Active movement or walking style are
sometimes meaningfully
in diagnostic. Delay in movement ability may illustrate delay
inmotoric development or neurological disorder. There are
somespecific attitude and movement in some diseases; specific
gettingup position from sitting or laying down position in
DMD,monoparalitic gait in post polio, wide base gait in
increasedintracranial pressure, atetoid gait in cerebral palsy,
Sydenhamchorea in rheumatic fever.
6. Neurological and Reflex ExaminationThese examinations are
more difficult to be access in children,even more in uncooperative
one. Reflex examinations are often
difficult to do. In neonatal there are specific reflexes that
presentor exactly not present in this group.
SPECIFIC EXAMINATION IN NEONATESPhysical examination in neonates
needs a special attention because
there are many differences with those in children. The most
numberof items in physical examination is inspection, and then
otherexaminations with a little manipulation. Practically,
auscultation isonly done to examine the heart, although it doesnt
mean thatauscultation is not important for neonates. Neonates
examinationneeds patient, gentleness, and flexibility. In a calm
baby, we shouldauscultate the heart and abdomen after inspection,
and then palpate
-
7/29/2019 Pediatric&Minor Surgery Okt2008
32/63
32 Block 14
Paediatric Examination & Minor Surgery
the abdomen gently. After palpation, we can perform
otherexaminations. The important symptoms that are should be paid
moreattention are:- General appearance, sound of crying- Pale,
icteric, cyanotic- Level of consciousness, convulsion, twitching.-
Dyspnea, apnea, irregular breathing- Blood circulation- Birth
weight
- Many congenital anomalies, such as:zzzzz Body constitution:
Down syndrome, hypothyroidzzzzz Neural tube defect : labio
(gnato-palato-)schizis, spina bifida,
meningo(mielo)celezzzzz Specific organs anomalies: heart,
external genital,
imperforate anus.
Especially for newborn, as soon as it births, the Apgar
scoreshould be performed to assess resuscitation needs (first
minute) andto check the result of resuscitation (fifth minute). The
componentsof Apgar are:- Appearance- Pulse- Grimace- Responds to
catheter in the nasal.- Skin color
To measure gestational age while the baby born, perform the
Dubowitzscore which components are: physical and neurological
characteristics.The total score of both physical and neurological
characteristics candefinite the gestational age according to the
standard graphic (lookat the picture below).
-
7/29/2019 Pediatric&Minor Surgery Okt2008
33/63
33Block 14
Paediatric Examination & Minor Surgery
There are primitive reflects in neonates, the most important
is:- Moro reflex: asymmetric response central nervous system
disorder- Grasp reflex- Tonic neck reflex: abnormality central
nervous system disorder
Primitive reflexes are reflexes that appear and disappear
followingthe developmental period.
Implementation Procedure:1. Take the history taking of the
children patient from the
mother effectively and efficiently.2. Write the data on the
medical record and make the hypothesis
of the history taking that has been obtained.
Reference:
Bates, B.1987. A Guide to Physical Examination and History
Taking.4th edition. J.B. Lippincott Company,
Philadelphia.Matondang, CS, Wahidiyat, I, Sastroasmoro, S.2003.
Diagnosis Fisis
pada Anak. Sagung Seto, Jakarta.Saifuddin, BA, Wiknjosastro, GF,
Affandi, B, Waspodo, J. 2003. BukuPanduan Praktis Pelayanan
Kesehatan dan Neonatal. YayasanBina Pustaka Sarwono Prawirohardjo,
Jakarta.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
34/63
34 Block 14
Paediatric Examination & Minor Surgery
APPENDIX 1
Physical and Mental Development in children 0-5 years old (Gross
andFine motor, emotional, social, attitude, and language)
0-3 months Try to lift the head Following object with its eyes
Regard face and smile responsively
Respond to sounds /bell Recognize the mother by seeing,
smelling, hearing, contact Vocalize
3-6 months Head up 900 and chest up supported by their own
forearms Try to reach things/toys Put things in her/his mouth
Laughing or screaming if being asked to play with Try to find lost
things
6-9 months Able to face downward and upward by her/him self Able
to sit without help Able to creep Turn things from one hand to
another one Hold small thing with the thumb and pointing finger
Speaks meaningless word Afraid to stranger people Participate in
clapping hands or hide and seek
-
7/29/2019 Pediatric&Minor Surgery Okt2008
35/63
35Block 14
Paediatric Examination & Minor Surgery
9-12 months Able to stand up without a help Walking with guiding
by the hand Imitate speech, try to say one or two words Understand
simple command or forbidden Always eager to explore and put tings
into mouth Participate in playing games
12-18 months
Walking and explore inside the house and surrounding Able to
pile up 2 or 3 cubes Saying 5-10 words Showing jealousy and
competition
18-24 months Walking up and down the stairs Able to pile up 6
cubes Pointing to its own eyes and nose Able to compose a sentence
with 2 words Try to eat by her/him self Try to control urination
and defecation Pay attention to what the elderly do Play games with
other children
2-3 years Jumping, climbing Make a bridge with 2 cubes Able to
compose simple sentences Able to draw a circle
-
7/29/2019 Pediatric&Minor Surgery Okt2008
36/63
36 Block 14
Paediatric Examination & Minor Surgery
3-4 years Walking alone visiting the neighbour Learn to wear /
put off clothes Draw a picture of person with head and trunk
Recognize 2 or 3 colors Speaking well, mention her/his own name,
sex and age Asking how a baby given birth Recognize upper side,
down side, front side and back side Able to do simple tasks
4-5 years Jumping, dancing Draw picture of person with head,
arms and trunk Draw square and triangle Able to count fingers,
mention day in a week Complaining if prohibited what she/he likes
to do Recognize 4 colors Estimate shapes and size of things,
distinguish big and small Pay attention/imitating adult
activities
(Source: Yaumil-Mimi scale, Paediatric Psychology Department
ofIndonesian University and Social Paediatric Department of
IDAI)
-
7/29/2019 Pediatric&Minor Surgery Okt2008
37/63
37Block 14
Paediatric Examination & Minor Surgery
APPENDIX 2IMMUNISAZION SCHEDULE
Age
Months Years
Immunisation Type
0 1 2 3 4 6 9 15 18 2 6 12
PPI*
Hepatitis B I II III IV
BCG XDPT I II III IV V VI
Polio I II III IV V VI
Mumps X
Others
Act-Hib I II III IVHib
Pedvax Hib I II III
MMR
XTyphoid:
-polysaccharide
-Oral X
Varicela X
Hepatitis A XXX
Taken from Sari Pediatri, June 2000 (with simplify)
*PPI = Program Pengembangan Imunisasi Depkes RI (Immunization
DevelopmentProgramme of Health Department)
-
7/29/2019 Pediatric&Minor Surgery Okt2008
38/63
38 Block 14
Paediatric Examination & Minor Surgery
MEDICAL RECORD OF PAEDIATRICS(ANAMNESIS)
I. IDENTITYa). The child :
Name :Place/date of birth :Sex :Address :
b). The parents:Name of father : Name of the mother :
Age : Age :Address : Address :Job : Job :Education : Education
:Age when got married : Age when got married :
II. HISTORY TAKINGA. History of disease
Chief complaint:
Present Illness:
Family illness:
Pedigree:
-
7/29/2019 Pediatric&Minor Surgery Okt2008
39/63
39Block 14
Paediatric Examination & Minor Surgery
B. Personal History:
1. History of perinatal care
Pregnancy (Antenatal care):
Labor (Natal care):
Postnatal care:
Resume :
2. Eating Habit
Resume :
3. Growth and Development
Gross Motor Fine Motor Personal-Social Language
Resume:
-
7/29/2019 Pediatric&Minor Surgery Okt2008
40/63
40 Block 14
Paediatric Examination & Minor Surgery
4. Immunization
BCG
DPT
Polio
Measles
Hep. B
Other Immunization
Resume:
5. History of past disease
6. Social, economic and environment state:
Social-economic state
Environment state
Resume :
-
7/29/2019 Pediatric&Minor Surgery Okt2008
41/63
41Block 14
Paediatric Examination & Minor Surgery
7. Anamnesis of body system:
Cerebrospinal system
Cardiovascular system
Respiratiry system
Gastrointestinal system
Urogenital system
Integumentum system
Musculoskeletal system
HYPOTHESIS :
-
7/29/2019 Pediatric&Minor Surgery Okt2008
42/63
42 Block 14
Paediatric Examination & Minor Surgery
SIMPLE SKIN SUTURING
GENERAL OBJECTIVE:
1. Students understand indications for wound suturing2. Students
are able to perform wound suturing on a mannequin
SPECIFIC OBJECTIVE:
1. Students are able to provide information on wound
suturingprocedure
2. Students are able to put patient into the right position for
operation3. Students are able to perform disinfection on a
patient4. Students are able to prepare instruments for suturing a
wound5. Students are able to perform aseptic procedure6. Students
are able to use surgical instruments for suturing a wound7.
Students are able to select the appropriate needle and thread8.
Students are able to perform wound suturing9. Students are able to
make the correct knot with or without the use
of an instrument10. Students are able to apply a bandage
11. Students are able to provide information and educate patient
onpost operation care
INTRODUCTION
Wound or vulnus is a damaged or a discontinued tissue. There
maybe corpus alienum (i.e. dirt, fragment of broken glass, wood
splinter,etc) and mikroorganisme (aerob or anaerob) on the wound
which havepotential to cause suppurative infection even more
tetanus. A woundless than 8 hours (still in itsgolden period) can
be saturated by way of
asepsis. A wound that is still in its golden periodwill heal
primarily,
leaving only a slight formation of tissue scrape and good
cosmetics.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
43/63
43Block 14
Paediatric Examination & Minor Surgery
A wound that is more than 8 hours will usually have been
con-
taminated and therefore an open treatment is applied (not
sutured).
These kinds of wound will heal in a secondary manner, leaving
a
somewhat thick tissue scrape. In addition, cosmetics (and/or
func-
tion) tend to decline. Should an infection occur, then delayed
pri-
mary suturing is performed.
Wounds can be classified into two main categories; acute and
chronic. Usually, an acute wound can be treated immediately
and
may experience good anatomical restoration and its functional
in-tegrity can be restored to its original condition. On the other
hand,
chronic wound that has passed itsgolden periodwill usually heal
but
its anatomical structure and function will not be restored to
its
former condition.
Required Instruments
Instruments that are used to stitch a wound:
1.Pincer
There are 2 types of pincer;
non-serrated anatomic pincer used
to hold the tissue, and serrated
surgical pincer, to grip the skin.
Atraumatic pincers are used when
handling blood vessels and fragile
tissue. Generally, pincers are held
with the left hand similar to holding
a pen.
Figure 1. Example of pincers
-
7/29/2019 Pediatric&Minor Surgery Okt2008
44/63
44 Block 14
Paediatric Examination & Minor Surgery
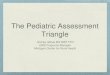
2. Needle Holder
It is held with the right hand, oneblade on the phalanx I digiti
I and theother blade on the phalanx II digiti IV.The second and
third finger is used tostabilize the holder. The needle is heldon
its 1/3 to its backend, approximately1 mm from the tip of the
holder, andthen it is fastened (figure 3).
Figure 2. Needle Holder
Figure 3. Method for fastening the needle using the needle
holder
-
7/29/2019 Pediatric&Minor Surgery Okt2008
45/63
45Block 14
Paediatric Examination & Minor Surgery
3. Needle and threadThere are several types of needles and
threads. Amongst them
are thread and needle that are on their own. Every time they
needto be used, the thread must be manually inserted through the
needle.These types of thread and needle are considered less
practical. Thethread tends to break in the middle of performing the
suturing, andthe sterility of these types of thread cannot be
ensured because thethread comes in a long roll which is kept inside
a cassette and takenaccording to needs. Furthermore, this type of
thread needle maycause extra trauma to the tissue. However, the
price is relativelycheap. A more ideal type of thread needle is the
atraumatic type,but the price can be somewhat more expensive.
Suturing needle can be categorized based on its size and
length.According to its circle, there are 2/8, 3/8, 4/8, 5/8
needles, andbased on its longitudinal section, there are triangular
needles forsuturing the skin and spherical needle to suture
internal tissue.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
46/63
46 Block 14
Paediatric Examination & Minor Surgery
Figure 4. Various types of curved needles and various types of
longitudinal
needle section
De Jong, 1997. Surgical Science Teaching Book.
A. (1) ellipse eye, (2) square eye, (3) otoumatic eye, B.
circle,
3/8 circle, circle, C. (1) needle base, (2) place to secure
needle holder,
(3) needle body or stem, (4) needle point, D. (1) spherical
needle,
(2) sharp needle, (3) spherical-sharp
-
7/29/2019 Pediatric&Minor Surgery Okt2008
47/63
47Block 14
Paediatric Examination & Minor Surgery
Figure 5. Various types of needle shape
Brown, John Stuart. 1995. Minor Surgical Atlas and Teaching
Book
Suturing thread can be categorized based on its material.
There
are biological material and synthetic material. Whilst
threads
can be categorized based on its capacity to absorb;
absorbent
and nonabsorbent thread. For absorbent threads, there are
those
that can be absorbed by the tissue in 1 week, 2 weeks or
longer,
which can be as long as 3 months. Based on their size, there
are
threads no. 2, 1, 0, 2/0, 3/0, 4/0 until the smallest size.
Based
on the number of strands, there are 1 strand (monofilamen)
and multifilament that are braded. For simple interrupted
skin
suturing, that will be removed in about 7 to 14 days, it
isrecommended to use nonabsorbent thread with the size of 3/0
or 2/0. Whilst the facial areas that requires earlier removal
of
approximately day 4, it is recommended to use monofilament
thread of the smallest size in order to give a better
cosmetic
result.
4. Scissors
The scissors are held with the right hand, similar to holding
the
needle holder (figure 7). There are thread scissors and
tissue
scissors. Tissue scissors should not be used for cutting the
thread
-
7/29/2019 Pediatric&Minor Surgery Okt2008
48/63
48 Block 14
Paediatric Examination & Minor Surgery
because it may cause the scissors to become blunt and break
easily. Tissue scissors are usually finer, very sharp, and
curved to
ensure visualization of the tissue that is being cut.
Figure 6. Types of Surgical Scissors
Figure 7. Method of holding the surgical scissors
-
7/29/2019 Pediatric&Minor Surgery Okt2008
49/63
49Block 14
Paediatric Examination & Minor Surgery
Figure 8. Scalpel and blade.
Figure 9. Method for holding the scalpel for short linear
incision
5. Scalpel
The scalpel comprises the handle and blade which can either
be
in one piece (older version) or can be separated, wherein at
the
beginning of each operation, the blade must be fastened. The
blade is very sharp, thus it is recommended to not directly
hold
it with the bare hand, but should use an instrument in order
to
prevent iatrogenic wound. To move the blade, use your thumb
and not your hand.
It is usually held by the right hand similar when holding
thekitchen knife for long linear incision. For short linear or
ellipsoidal
incision, the scalpel is held like a pen (figure 9).
-
7/29/2019 Pediatric&Minor Surgery Okt2008
50/63
50 Block 14
Paediatric Examination & Minor Surgery
PROCEDURE FOR WOUND SUTURING
To perform wound suturing that will ensure a good result,
there
are several steps that must be carefully followed; inspecting
the
wound carefully, putting the patient into a comfortable
position,
and for operators, it should be performed as ergonomical as
pos-
sible. Accordingly, all preparations should be prepared well
before
the actual operation begins.
Disinfecting the operation area
Disinfecting the operation area is performed by using
disinfect-
ing fluid such as povidone iodine.
The method for disinfecting the operation area is by
starting
from around the wound, circling the periphery area using a
disin-
fecting pincer that is long enough to prevent the operators
sterile
hands the possibility of being contaminated from the operation
area
that is still dirty. Do not forget to inform the patient in
advance that
the disinfecting fluid may cause pain when it comes into
contact
with the wound.
Disinfection is especially needed to cleanse the wound from
con-tamination such as:
Technique for Suturing Wound
After applying the disinfectant and before performing the
op-
eration, the patient may be given local anesthetics either by
way of
infiltration, nerve blocking. After that, the surgical area is
cleansed
from contamination such as:
- Corpus alienium found on the surface of the wound that can
be
easily removed / cleansed
-
7/29/2019 Pediatric&Minor Surgery Okt2008
51/63
51Block 14
Paediatric Examination & Minor Surgery
- Several corpus alienum that has entered the tissue can be
detected
by an X-ray and there are others that cannot.
- Chemical materials, toxins, snake poison etc
- Microorganism
The presence of microorganism can be decreased by cleansing
the wound with NaCl phyisiology and debridement. Microbe
aerob
can be anticipated by doing health promotive (improving the
bodys endurance: eating nutritious food and having enough
rest)
and using antibiotics prophylaksis- Anaerob Microbe especially
Clostridium tetani can be anticipated
by cleansing the wound with Hidrogen Peroksida (H2O
2) 10%,
antitetanus serum and tetanus vaksination.
The dominant hand is in a prone position. The needle, with
the
thread, is held with a needle holder at 1/3 to the back. It is
pierced
in a straight upright manner into the surface of the skin
approxi-
mately x mm from the periphery of the wound ( x = thickness of
the
sutured skin), pushed it according to the curve of the needle to
the
direction of the other side of the wound. The direction should
be
straight forward in axis to the wound, penetrating the skin as
far asx mm from the periphery of the wound (dominant hand acts
as
suspension). The tip of the protruding needle is taken by the
pincer
that is held by the non-dominant hand (similar to holding a
pen),
and then the needle is pulled out using the needle holder in
the
dominant hand after firstly releasing the needle from the
other
hand. After this, make three times knots. The periphery of
the
wound should be apposition, somewhat tightened, but should not
be
too tight as it can effect the ischemic tissue and prolong
healing
process (healing starts from the suturing area), and can
instigate
the buildup of more tissue scrape therefore disrupting
cosmetics
-
7/29/2019 Pediatric&Minor Surgery Okt2008
52/63
52 Block 14
Paediatric Examination & Minor Surgery
and function. However, if it is too loose, it may cause a dead
space
that may also disrupt the healing process and may even cause
infec-
tion. Both ends of the thread are cut using a scissors
approximately
x mm from the knot. The knot is placed at the end of the
suturing
to simplify when taking out the thread later on. This process
is
repeated until all the wound is sutured with distance between
each
suturing 2 times the thickness of the skin (x). Inspect, and if
re-
quired, restore the apposition edge of the wound and examine
the
suturing one more time, and then close the wound using
gauze.
Figure 10. Simple interrupted suture
de Jong 1997. Buku Ajar Ilmu Bedah
-
7/29/2019 Pediatric&Minor Surgery Okt2008
53/63
53Block 14
Paediatric Examination & Minor Surgery
Figure 11. Longitudinal wound and method for piercing the needle
and
performing suturing
When the needle penetrates the skin in a straight upright
manner, the outer layers of
the epidermis will convex outwards (eversion); this is the basis
for a proper healing
process (ectropion)
When the needle does not penetrate the skin in a straight
upright manner, the epidermis
surface will fold inwards and prolong the healing process
(entropion)
-
7/29/2019 Pediatric&Minor Surgery Okt2008
54/63
54 Block 14
Paediatric Examination & Minor Surgery
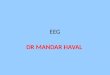
Below are various types of skin suturing:
Figure 12. Various types of skin suturing
De Jong, 1997, Buku Ajar Ilmu Bedah
A. Continuous suturing
B. Vertical Continuous suturing
C. Vertical matras suturing (Donati)
D. Horizontal matras suturing
E. Intracutaneous/subcuticuler suturing
-
7/29/2019 Pediatric&Minor Surgery Okt2008
55/63
55Block 14
Paediatric Examination & Minor Surgery
Making a suturing knot
This section will deal with practicing making a suturing knot
by
using an instrument. Type of knot that will be trained is the
square
knot or reef knot.
Making a knot using an instrument
Figure 13. Making a knot using instrument
De Jong, 1997, Buku Ajar Ilmu Bedah
-
7/29/2019 Pediatric&Minor Surgery Okt2008
56/63
56 Block 14
Paediatric Examination & Minor Surgery
After the skin suturing is completed, evaluate the suture
and
then the wound is firmly covered by gauze, the patient should
be
given information and education on caring for the wound,
which
includes diet, wound treatment such as the wound should not
come
into contact with water and should be kept clean, next schedule
for
the patient to come back and meet with the doctor who will
monitor
the wound. Usually the suture will be removed after 7 to 14
days
unless for face area where the suture will be removed in 4-5
days
due to good vascularisation in this area. If the removal of
suture isprolonged the scar will make bad cosmetic result. Should
there be
prescribed medicine, do not forget to provide explanation
about
dosage, method for using external medicine and side effects
that
may occur
Removing the suture according the schedule of removal.
a. Prior to performing the suturing, the wound and its
periphery
area should be cleansed with aseptic.
b. Tie the suturing knot with forceps, and pull the knot until
it is
fairly raised up. Cut the thread just below the knot as near
to
the skin as possible, with the prone position of 45 .
c. Pull the thread to the opposite direction from the knot so
that
the thread does not enter the tissue.
d. Apply dressing to the wound
-
7/29/2019 Pediatric&Minor Surgery Okt2008
57/63
57Block 14
Paediatric Examination & Minor Surgery
Figure 14. Method for removing suturing
De Jong,1997, Buku Ajar Ilmu Bedah
After students finish reading this manual, it is expected
that
they will follow on by practicing the acquired skills based on
the casebelow:
You are a doctor who is on duty at the emergency ward. Apatient
comes in with an open wound on his/her lower rightarm about 5 cm
long. The wound was caused by a shatteredglass and the accident
occurred 4 hours ago.
Perform a wound suturing procedure on the patient by applyingthe
simple interrupted suturing method.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
58/63
58 Block 14
Paediatric Examination & Minor Surgery
REFERENCES
Sjamsuhidajat,R., De Jong, W. (editor) 1997, Buku Ajar Ilmu
Bedah Edisi
Revisi, Jakarta: Penerbit Buku Kedokteran EGC
Schwartz, SeymourI, 1994, Principles of Surgery 2 Vol.10th ed.
New York:
Mc-Graw Hill Publishing Company.
Brown, John Stuart. 1995, Buku Ajar dan Atlas Bedah Minor.
Jakarta:
Penerbit Buku Kedokteran EGC
-
7/29/2019 Pediatric&Minor Surgery Okt2008
59/63
59Block 14
Paediatric Examination & Minor Surgery
CHECK LIST FORHETEROANAMNESIS IN PAEDIATRIC
No Criteria0
1 Able to make interpersonal relationshipwith the parents and
the patient
2 Asking the patients and parents identitycompletely
3 Asking the chief complaint
4 Able to explore present illness complainsystematically
5 Able to explore past illness history
6 Able to explore family illness history
7 Able to make pedigree of the family
8 Able to explore antenatal care history
9 Able to explore natal care history
10 Able to explore postnatal care history
11 Asking eating habits12 Asking about the patients growth
and
development since neonates to present
(gross motor, fine motor, personal-social,language)
13 Able to ask about the immunization history
14 Able to explore the social-economics andenvironmental
state
15 Able to make anamnesis of the bodysystem
16 Able to cross check unclear information
17 Able to write medical record completelyTotal score
-
7/29/2019 Pediatric&Minor Surgery Okt2008
60/63
60 Block 14
Paediatric Examination & Minor Surgery
Jogjakarta, ..............................
Instructor Observer
(.............................) (.........................)
Total ScoreFinal Score = x 100%
34
Explanation:Score 0: not performed at allScore 1: performed
unsatisfactoryScore 2: performed satisfactory
-
7/29/2019 Pediatric&Minor Surgery Okt2008
61/63
61Block 14
Paediatric Examination & Minor Surgery
CHECKLIST SIMPLE SKIN SUTURING
ScoNo. Aspects.
0 1
1. Greeting and performing emotional relationship,self
introduction
2. Performing brief physical examination needed
according to the case
3. Explaining the procedure and taking theinformed consent
4. Preparing instruments for aseptic procedure
correctly, wearing a clean short sleeves cottonsuit, caps,
googles, mask and boot.
5. Preparing minor surgery instruments in aseptic
manner
6. Performing hand washing/scrubbing andwearing the gloves
correctly
7. Sterilizing the surgery field with an antimicrobial
agent in central to peripheral direction
8. Placing sterile fenestrated linen over the surgical
field.
9. Performing local anesthesia
10. Cleaning the wound by using NaCl 0,9 % (todilute
microorganisms and foreign bodies)
11. Sterilizing the wound from anaerobic bacteria by
using Perhydrol 10% solution followed by NaCl0,9 %.
12. Placing a curved taper cut needle no. 4/8 in
needle holder, between two-third (3
2) distal and
one-third (3
1) proximal, and locking the position
13. Placing the thread no. 3/0 properly on the
curved taper cut needle
14. Lifting up the margin of the wound by usingsmooth serrated
pincer, and with wrist in prone
position, the elbow in 90o angle and shoulder
abducted, sticking the needle into the skin,straight vertically
toward wound axis.
15. Performing a penetration (x cm) from the wound
-
7/29/2019 Pediatric&Minor Surgery Okt2008
62/63
62 Block 14
Paediatric Examination & Minor Surgery
ScoreNo. Aspects.
0 1 2
16. Sticking the needle with supine wrist movement
and shoulder abduction movement, pushing the
needle according to the curved shape of the
needle
17. Piercing the needle exceeding the wound in
straight vertical direction toward wound axis.
18. Pinching the needle with needle holder after it
appears on the skin surface and pulling it out. The
distance between wound margin and where the
needle pierce the skin should match with skinthickness (x cm)
and in straight vertical direction
toward wound axis.
Pulling the thread and leaving 3-4cm from the skin
19. Holding the long thread with the left hand and
holding the needle with the right hand
20. Placing the needle holder in parallel position with
the wound axis.
22. Winding the long thread over the needle holder
23. Taking the tip of short thread by needle holder, and
pulling the short thread toward you. Meanwhile, the
long thread is pulled in opposite direction.
24. Placing the long thread over the needle holder,
winding it over the needle holder.
25. Taking the tip of short thread by needle holder, and
pull the short thread away from yourself.
Meanwhile, the long thread is pulled toward
yourself.
26. Cutting a knot by placing the scissor to the suture,
ready to cut, then placing the scissors above the
knot, turning out the scissors away from the knots
in order to be able to see the length of the thread
and cut finally. The length of the remaining thread
is about the thickness of skin (x cm).
27. Result of the suture should not be too tight or too
loose and the edge of margin should meet
properly.
-
7/29/2019 Pediatric&Minor Surgery Okt2008
63/63
63Bl k 14
Paediatric Examination & Minor Surgery
ScoreNo. Aspects.
0 1 2
28. Knot should be placed on the side of the
wound margin.
29. Checking proximity of wound margin and
performing dressing on the wound.
30. Giving educations that are needed to the
patient.
Explanation:Score 0 = Not performed at all
Score 1 = Performed imperfectly
Score 2 = Performed perfectly
Total score% coverage skills = ----------------- x 100% = %
60
Yogyakarta,
Instructor Student
Name Name