Embed Size (px)
DESCRIPTION
jurnal
Citation preview

DOI: 10.1542/peds.2013-1737; originally published online November 18, 2013; 2013;132;e1562Pediatrics
Demmler, Ronan A. Lyons and David FoneShantini Paranjothy, Frank Dunstan, William J. Watkins, Melanie Hyatt, Joanne C.
ChildhoodGestational Age, Birth Weight, and Risk of Respiratory Hospital Admission in
http://pediatrics.aappublications.org/content/132/6/e1562.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

Gestational Age, Birth Weight, and Risk of RespiratoryHospital Admission in Childhood
WHAT’S KNOWN ON THIS SUBJECT: Preterm birth is associatedwith increased morbidity during childhood. Many studies havefocused on outcomes for preterm births before 32 weeks’gestation, but there are few follow-up data for late preterminfants (34–36 weeks’ gestation).
WHAT THIS STUDY ADDS: The risk of respiratory admissionduring childhood decreased with each successive week ingestation up to 40 to 42 weeks. The increased risk is small for latepreterm infants, but the number affected is large and has animpact on health care services.
abstractOBJECTIVE: To investigate the risk of emergency respiratory hospitaladmission during childhood associated with gestational age at birthand growth restriction in utero.
METHODS: The study included a total population electronic birth co-hort with anonymized record-linkage of multiple health andadministrative data sets. Participants were 318 613 children born inWales, United Kingdom, between May 1, 1998, and December 31, 2008.The main outcome measure was emergency respiratory hospitaladmissions.
RESULTS: The rate of admission in the first year of life ranged from 41.5per 100 child-years for infants born before 33 weeks’ gestation to 9.8per 100 child-years for infants born at 40 to 42 weeks’ gestation. Therisk of any emergency respiratory admission up to age 5 yearsincreased as gestational age decreased to ,40 weeks. Even at 39weeks’ gestation, there was an increased risk of emergency hospitaladmissions for respiratory conditions compared with infants born at40 to 42 weeks (adjusted hazard ratio 1.10; 95% confidence interval1.08–1.13). Small for gestational age (,10th centile for gestation andgender-specific birth weight) was independently associated with anincreased risk of any emergency respiratory admission to hospital(adjusted hazard ratio 1.07; 95% confidence interval 1.04–1.10).
CONCLUSIONS: The risk of emergency respiratory admission up to age5 years decreased with each successive week in gestation up to 40 to42 weeks. Although the magnitude of increased risk associated withmoderate and late preterm births is small, the number of infants af-fected is large and therefore presents a significant impact on healthcare services. Pediatrics 2013;132:e1562–e1569
AUTHORS: Shantini Paranjothy, PhD,a,b Frank Dunstan,DPhil,a William J. Watkins, PhD,c Melanie Hyatt, PhD,b
Joanne C. Demmler, PhD,d Ronan A. Lyons, MD,b,d and DavidFone, MDa,b,d
aInstitute of Primary Care and Public Health, and cDepartment ofChild Health, School of Medicine, Cardiff University, Cardiff, UnitedKingdom; and bCentre for Improvement in Population Healththrough E-records Research, and dCentre for the Developmentand Evaluation of Complex Interventions for Public HealthImprovement, Swansea University, Swansea, United Kingdom
KEY WORDSgestation, birth weight, emergency hospital admission,respiratory disease
ABBREVIATIONSCI—confidence intervalHR—hazard ratioSAIL—Secure Anonymised Information LinkageWECC—Wales Electronic Cohort for Children
Dr Paranjothy conceptualized and designed the study togetherwith Prof Dunstan and Prof Fone and drafted the initialmanuscript; Prof Dunstan contributed to the conceptualizationand design of the study, carried out the data analysis, andreviewed and revised the manuscript; Dr Watkins prepared thedata sets for analysis and carried out initial analyses, andreviewed the manuscript; Drs Hyatt and Demmler prepared thedata sets for analysis and reviewed and revised the manuscript;Prof Lyons conceptualized the Wales Electronic Cohort ofChildren and reviewed and revised the manuscript; Prof Fonecontributed to the conceptualization and design of the study andreviewed and revised the manuscript; and all authors approvedthe final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1737
doi:10.1542/peds.2013-1737
Accepted for publication Sep 19, 2013
Address correspondence to Shantini Paranjothy, PhD, Institute ofPrimary Care and Public Health, School of Medicine, CardiffUniversity, 5th Floor Neuadd Meirionnydd, Heath Park, CardiffCF14 4YS, United Kingdom. E-mail: [email protected]
(Continued on last page)
e1562 PARANJOTHY et al at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

Preterm birth is associated with ad-verse respiratory, neurodevelopmental,and educational outcomes.1–3 Pretermbirth rates have increased over the pastdecade, and the longer-term con-sequences for health are a concern forpediatricians and public health.4 A re-cent review reported that many studieshave focused on outcomes for verypreterm births (,32 weeks’ gesta-tion),5 but there are few data for latepreterm infants (34–36 weeks’ gesta-tion), who account for 6% to 7% of allbirths and up to 75% of preterminfants.6 Compared with full-terminfants, preterm infants are at risk forlong-term deficits in lung function (%forced expiratory volume in 1 second) inlater life.7 Data from a longitudinalstudy suggested that very (25–32weeks) and moderately (33–34 weeks)preterm born infants have greater def-icits in lung function during childhoodcompared with late preterm (35–36weeks) born infants.8 The inclusion ofinfants born at 32 and 34 weeks inthe very and moderately preterm cate-gories in this latter study reflectsthe classification inconsistencies in theliterature.
It is not known how reduced lungfunction translates into health careutilization, although the risk of otheradverse outcomes in childhood (suchas lower educational attainment) hasbeenshownto increasewitheveryweekreduction in gestational age from 40weeks, including within the term cate-gory of 37 to 40 weeks.3 There areno comprehensive population-basedanalyses of the risk of hospital admis-sions across the range of gestationalage and birth weight; previous studieshave grouped together broad ranges ofgestational age, making it difficult todistinguish between prematurity andthe effects of growth restriction.5,9
Such data are required to provide ac-curate information to parents, informclinical decisions, and develop care
pathways for children. We hypothe-sized that the risk of emergency re-spiratory hospital admission duringchildhood decreases with increasinggestational age at birth and is higherfor infants who were small for gesta-tional age within each category ofgestational age. We tested this hypoth-esis using data from a total populationelectronic birth cohort characterized bythe anonymized linkage of multipleroutine health and administrative datasets.
METHODS
Data Source: The Wales ElectronicCohort for Children
The Wales Electronic Cohort for Chil-dren (WECC) includes 804 290 childrenborn between January 1, 1990 andDecember 31, 2008, with a mother orchild usually residing in Wales. Eligibleparticipants are identified from theWales Demographic Service, an ad-ministrative register of all individualsliving in Wales and registered witha General Medical Practitioner. WECCanonymously record-links routinelycollected data held in health care andsocial data sets within the SecureAnonymised Information Linkage (SAIL)databank at the Health InformationResearch Unit, Swansea University,United Kingdom.10,11 For each data setwithin the SAIL databank, an individualis assigned an Anonymised LinkingField based on their National HealthService number, which is used to linkacross data sets. In this analysis, weused record-linked data from thedatabases shown in Table 1. The timeperiod for this analysis was January 1,1998 through December 31, 2008 due toavailability of data on hospital admis-sions from the Patient Episode Data-base for Wales. Data were censored formigration out of Wales (ascertained byusing the Wales Demographic Service)and death during infancy or childhood(ascertained by using the All-Wales
Perinatal Survey data set and PublicHealth mortality files).
With regard to outcome measures, wedefined each emergency hospital ad-mission for respiratory disease re-corded on Patient Episode Database forWales by using the following In-ternational Classification of Diseases,10th Revision, codes in the primarycoding position: acute upper re-spiratory tract infection (J00–J06,J10.1, J10.8, J11.1, J11.8), influenza andpneumonia (J10.0, J11.0, J12–J18),acute lower respiratory tract infec-tions (J20–22), acute bronchiolitis(J21), and asthma (J45–J46).
Definition of Exposed Groups
Gestational age was based on the bestestimate of gestation at the time ofdelivery in completed weeks, normallybased on the postmenstrual age, butthis could be modified on the basis ofantenatal ultrasound scan or from thepostnatal estimate of maturity. Wecategorized gestational age into thefollowing categories: ,33, 33 to 34, 35to 36, 37, 38, 39, and 40 to 42 weeks. Wedefined small for gestational age asbirth weight below the 10th percentile,calculated for each stratum based ongender and gestational age in weeks,using Altman’s method to model therelationship between birth weight andgestational age across the whole rangeof gestational age.12
Statistical Analysis
We calculated the child-year incidenceof emergency hospital admission forany respiratory diseaseup to age 1 yearand between ages 1 to 5 years. We usedtime to event Cox’s regression analysisto obtain crude and adjusted hazardratios (HRs) for the first emergencyhospital admission for any respiratorydisease in each gestational age cate-gory compared with the referencecategory of 40 to 42 weeks. We adjustedfor small for gestational age, maternal
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 e1563 at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

age (in 5-year bands), parity (multipa-rous vs nulliparous), quintile of so-cial deprivation (based on Townsendscore13 for social deprivation calcu-lated by using data from the 2001Census), maternal smoking duringpregnancy, caesarean delivery, gender,presence of a major or minor congen-ital anomaly as defined by the Euro-pean Congenital Anomalies Registries,14
multiple birth, seasonality of birth,breastfeeding (at birth or 6–8 weeks),Apgar score at 5 minutes, and neonataladmission to hospital (InternationalClassification of Diseases codes P00–P96). We included an interaction termbetween small for dates and each ges-tational age category to assess whetherthe effect of growth restriction in-uterowas constant across gestational ages.We also included an interaction termbetween birth by caesarean deliveryand each gestational age category,assessing interactions using likelihoodratio tests. Analyses were repeated toobtain HRs for emergency hospital ad-mission with each defined category ofrespiratory disease: (1) acute upperrespiratory tract infection, (2) influenza
and pneumonia, (3) acute lower re-spiratory tract infection, (4) acutebronchiolitis, and (5) asthma, adjustedfor the maternal and birth character-istics detailed above.
Missing Data
Breastfeeding, Apgar score, and ma-ternal smoking data were missing for20.3%, 28.6%, and 65.1% of births in thedata set, due to organizational andadministrative differences in the waythe data are collated in different hos-pitals in Wales. We used multiple im-putation to account for missing dataunder the missing at random as-sumption.15 The multiple imputationmodel included parity, presence (mi-nor or major) or absence of congenitalanomaly, gender, maternal age (in 5-yearbands), caesarean delivery, quintile ofTownsend score, multiple or single birth,and whether there was a neonatal ad-mission. We compared the results of theCox’s regression models between a com-plete case analysis and analysis of theimputed dataset and obtained consistentresults; therefore, we have presentedresults from the imputed dataset.
Ethics and Information Governance
The WECC received approval from anindependent Information GovernanceReview Panel, with membership froma range of government, regulatory, andprofessional agencies. WECC has beenassessed by the Research Ethics Com-mittee for Wales and judged to be ananonymized research database thatdoes not require ethical review in linewith National Ethics Committee guid-ance.
RESULTS
There were 318 613 children born inWales between 1998 and 2008 in theWECC cohort eligible for inclusion inthis analysis. The total length of follow-up for this cohort was 1 156 415 child-years (mean 3.63 child-years, SD 1.69child-years). Overall, 17.6% of childrenin the cohort had $1 emergency re-spiratory hospital admission. The rateof admission in the first year of life was12.2 per 100 child-years, 5.3 per 100child-years for children aged between1 and 5 years in the whole cohort, and4.8 per 100 child-years for childrenaged 1 to 5 years who were born be-tween 1998 and 2003 (ie, with follow-up for 5 years after birth to allow forthe decrease in risk of admission asage increases). The rate of emergencyhospital admission for respiratory con-ditions decreased with increasinggestational age at birth but was con-sistently higher for infants who weresmall for gestational age within eachcategory of gestational age (Table 2).The most common reasons for admis-sion in the first year of life were acuteupper respiratory tract infection (n =16 475, 45.1% of admissions) and acutebronchiolitis (n = 16 172, 44.4% ofadmissions). For children aged be-tween 1 and 5 years, the majority(57.4%, n = 26191) of emergency re-spiratory admissions were for acuteupper respiratory tract infections. Forchildren aged ,1 year, the rate of
TABLE 1 Data Sources for WECC
Data Source Description
Public Health Birth files from the Office forNational Statistics (from 2003)
Data on all births in Wales or to mothers who areusually resident in Wales
National Community Child Health Database(from 1987)
A national databaseof all children resident inWales orborn in a Welsh hospital, containing data collectedat birth such as parity, mode of delivery, gestation,birth weight, gender, breastfeeding, and ApgarScore
Public Health Mortality files from the Office forNational Statistics (from 2002)
Data on all deaths in Wales or of individuals who areusually resident in Wales
Patient Episode Dataset for Wales (from 1998) Demographicandclinicaldataonall inpatientandday-case admissions in National Health Service WaleshospitalsandallWelshresidents treated inotherUKcountries
All Wales Perinatal Survey (from 1993) A database of perinatal and infant mortality in Walesincluding infants from 20weeks’ gestation to 1 yearof age, who die in a Welsh hospital or whosemother is usually resident in Wales
Congenital Anomaly Register and InformationService (from 1998)
A population-based register of any fetus or infant whohas a congenital anomaly whose mother is usuallyresident in Wales at the time of birth; congenitalanomalies are defined by the European network ofpopulation-based registries for the epidemiologicsurveillance of congenital anomalies14
e1564 PARANJOTHY et al at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

emergency admission for specific re-spiratory conditions was 5.5 per 100child-years for acute upper respiratorytract infection, 3.0 per 100 child-yearsfor influenza and pneumonia, 5.4 per100 child-years for acute lower re-spiratory tract infections (includingbronchiolitis), 4.8 per 100 child-yearsfor bronchiolitis and 0.4 per 100 child-years for asthma. For children agedbetween 1 and 5 years the rate was 3.0per 100 child-years for acute upperrespiratory tract infection, 0.4 per 100child-years for influenza and pneu-monia, 0.6 per 100 child-years foracute lower respiratory tract infec-tions (including bronchiolitis), 0.1per 100 child-years for bronchiolitis,and 0.7 per 100 child-years forasthma.
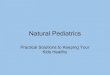
Figure 1 shows the survival functioncurves for time to the first emergencyrespiratory hospital admission accord-ing to gestational age categories. TheHR for any emergency respiratory ad-mission up to age 5 increased as ges-tational age decreased (Table 3). Smallfor gestational age was independentlyassociatedwith an increased risk of anyemergency respiratory admission tohospital (adjusted HR 1.07, 95% confi-dence interval [CI] 1.04–1.10), but therewas no strong evidence that the effect ofgrowth restriction (P = .06 for in-teraction) or caesarean delivery (P = .19for interaction) varied according togestational age. Caesarean delivery,
neonatal admission to hospital, youn-ger maternal age, and living in areasof higher social deprivation were eachindependently associated with in-creased risk of emergency respiratoryadmissions, whereas breastfeedingwas protective (adjusted HR 0.89, 95%CI 0.88–0.91). The risk of emergencyrespiratory hospital admission washigher for infants born April to June(adjusted HR 1.05, 95% CI 1.03–1.08),
July to September (adjusted HR 1.19,95% CI 1.17–1.22), and October to De-cember (adjusted HR 1.22, 95% CI1.19–1.25), compared with infants bornbetween January and March. Similarpatterns were seen when analyseswere repeated for specific types of re-spiratory admissions; the seasonalityeffects were greater for lower com-pared with upper respiratory disease(Table 4).
TABLE 2 Emergency Hospital Admissions for Respiratory Disease by Gestational Age Categories (N = 318 613)
Gestational Age % Infants With AnyERA inBefore Age 1 y
% Children With AnyERA Age 1–5 y
Mean No. of ERAsper 100 Child-YearsBefore Age 1 y
Mean No. of ERAsper 100 Child Years
Age 1–5 y
AGA SGA AGA SGA AGA SGA AGA SGA
,33 wk (AGA n = 4351/SGA n = 555) 23.6 23.4 19.4 18.4 41.5 48.0 13.5 15.033–34 (AGA n = 4580/SGA n = 480) 16.6 19.8 14.4 17.7 23.7 30.5 8.0 9.435–36 (AGA n = 11457/SGA n = 1432) 13.5 14.5 12.6 14.4 18.8 22.5 6.9 7.937 (AGA n = 15118/SGA n = 1912) 11.8 13.9 11.9 11.9 15.6 18.8 6.2 6.138 (AGA n = 37187/SGA n = 4067) 10.2 11.2 11.1 12.1 13.2 15.4 5.5 6.539 (AGA n = 59197/SGA n = 6416) 8.9 10.5 10.0 10.8 11.5 14.1 5.1 5.440–42 (AGA n = 155110/SGA n = 16751) 7.8 9.4 9.6 10.7 9.8 12.0 4.7 5.4Overall (n = 318 613) 9.3 10.5 12.2 5.3
AGA, appropriate for gestational age; ERA, emergency respiratory admission; SGA, small for gestational age.
FIGURE 1Time to the first emergency respiratory hospital admission according to gestational age categories.
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 e1565 at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

DISCUSSION
Our results show a clear pattern ofincreased risk of emergency hospitaladmissions for respiratory conditionswith decreasing gestational age; thisrisk further increased for infants whowere small for gestational age. Even at39 weeks’ gestation, infants had a 10%increase in risk of emergency hospitaladmissions for respiratory conditionscompared with those born at 40 to 42weeks, and a further 7% increase inrisk if they were small for gestational
age. These findings add support to therecent call to redefine “full-term”pregnancy from 37 to 42 weeks toa narrower interval of 39 to 42 weeks.16
However, given the additional morbid-ity observed for infants born at 39weeks, our results suggest that termshould be defined as 40 to 42 weeks.
Intrauterine factors that adversely af-fect fetal growth are associated withincreased risk of chronic respiratorydiseases in adulthood.17 Prematurityis associated with immature lung
development and consequently di-minished lung function during child-hood,7 but the effect of growthrestriction in utero on lung functionhas not been systematically studiedacross the full range of gestationalage.5 Several studies have tried to ex-amine associations between fetalgrowth restriction, which manifests assmall for gestational age, and lungfunction during childhood but havereported conflicting findings. Somestudies of infants born small for ges-tational age reported reduced forcedexpiratory volume in 1 second and re-spiratory symptoms, possibly due tosmall airway size relative to lung size.18,19
However, others have not found thisassociation, concluding that dimin-ished lung function in small infantswas attributable to prematurity ratherthan growth restriction,20–22 but thesewere all small studies from selectedpopulations (ie, infants admitted tohospital for neonatal care). One longi-tudinal study reported that childrenborn at 33 to 34 weeks had decreasedlung function at 8 to 9 years, but thisimproved by age 14 to 17 years.23 Someused low birth weight to define theirstudy population, which does not allowfor distinguishing the effects of pre-maturity (and hence physiologic im-maturity of the lung) from growthrestriction in a physiologically matureinfant.5 A recent systematic review hasshown that compared with full-terminfants, all preterm infants are at riskfor diminished lung function duringchildhood, although it is not clear howthis may impact on health care ser-vices.7 Most previous studies have fo-cused on hospital admissions ingeneral24 or specifically for asthmaand reported an increased risk asso-ciated with prematurity or low birthweight,9,25,26 but none have investigatedacute upper respiratory tract infection,the most common reason for hospitaladmission during childhood. To ourknowledge, our study is the largest
TABLE 3 Univariate and Adjusted HRsa for Emergency Respiratory Hospital Admissions up to Age5 According to Pregnancy and Birth Characteristics (HR and 95% CI, N = 318 613)
Univariate Adjusted
HR 95% CI HR 95% CI
Gestation category (wk),33 2.82 2.68–2.96 2.18 2.06–2.3033–34 1.89 1.79–2.00 1.59 1.50–1.6835–36 1.54 1.48–1.60 1.39 1.34–1.4537 1.38 1.33–1.43 1.32 1.28–1.3738 1.22 1.19–1.25 1.19 1.16–1.2239 1.12 1.09–1.14 1.10 1.08–1.1340–42 1 1
Small for gestational age 1.13 1.10–1.16 1.07 1.04–1.10Maternal age (y),20 1.24 1.21–1.28 1.23 1.19–1.2720–24 1.16 1.13–1.19 1.14 1.11–1.1725–29 1 130–34 0.89 0.87–0.91 0.90 0.88–0.9235–39 0.85 0.82–0.87 0.84 0.82–0.87$40 0.83 0.78–0.88 0.80 0.76–0.85
Parity$1 1.01 0.98–1.03 1.09 1.07–1.11
Quintile of social deprivation1 (least deprived) 1 12 1.01 0.98–1.04 0.98 0.95–1.013 1.13 1.10–1.16 1.05 1.02–1.084 1.19 1.15–1.22 1.08 1.05–1.115 (most deprived) 1.30 1.26–1.33 1.11 1.08–1.14
GenderFemale 0.75 0.74–0.77 0.77 0.75–0.80
Breastfeeding 0.81 0.80–0.83 0.89 0.88–0.91Multiple birth 1.19 1.14–1.25 0.83 0.79–0.87Smoking 1.18 1.15–1.21 1.04 1.01–1.06Neonatal admission 1.59 1.55–1.62 1.27 1.24–1.31Apgar score at 5 min #3 1.25 1.04–1.49 1.04 0.88–1.23Apgar score at 5 min 4–6 1.33 1.21–1.45 1.01 0.91–1.11Major congenital anomaly 1.89 1.83–1.95 1.66 1.61–1.72Minor congenital anomaly 1.37 1.30–1.43 1.24 1.18–1.30Caesarean delivery 1.16 1.14–1.18 1.10 1.08–1.12Season of birthJanuary–March 1 1April–June 1.04 1.02–1.07 1.05 1.03–1.08July–September 1.18 1.15–1.21 1.19 1.17–1.22October–December 1.21 1.19–1.24 1.22 1.19–1.25
a Adjusted for all variables shown in the model.
e1566 PARANJOTHY et al at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

population-based study of the risk ofemergency hospital admissions forrespiratory disease across the rangeof gestation at birth. A previous studyof maternal and perinatal factors onhospital admissions for asthma inchildren using a record-linked study of248 612 births in the Oxford regionbetween 1970 and 1989 found thatmaternal asthma, male gender, pre-term birth, low birth weight, caesareandelivery, and maternal smoking wereindependent risk factors.9 We did nothave data on maternal asthma, but ourresults are consistent with this studyfor male gender and preterm birth.However, the Oxford study used a broadrange of gestation (24–37 weeks) todefine preterm birth and therefore didnot explore the magnitude of increasedrisk associated with weekly gestationalages.9 Algert et al studied a populationof 240 511 births between 2001 and2003 in Australia and reported that 3%of children aged 2 to 5 years had $1admission for asthma; the risk ofadmissions for asthma decreased by5% for every 1-week increase in gesta-tional age.26 More recently, Boyle et alanalyzed data from the UK MillenniumCohort Study on 18 818 births andreported an increase in the proportionof children with at least 3 hospitaladmissions between age 9 months and5 years with decreasing gestation atbirth, although hospital admission was
based on parental report.4 Consistentwith this study, we found that the in-creased risk of hospital admission washighest for infants born before 33weeks’ gestation. However, the gradientof increased risk from 33 to 40 weeksapplies to the majority (at least 75%)of infants born preterm and willtherefore have a significant impact onhealth care services. The increasedrisk of respiratory hospital admissionsin infants born in the summer monthsis consistent with known risk factors ofhospitalization for bronchioloitis.27
We also found a protective effect as-sociatedwith breastfeeding, consistentwith other studies.4,28 Despite highlevels of breastfeeding initiation in theUnited Kingdom (81%), only 22% ofmothers continue to breastfeed at 6months.29 Because breastfeeding ratesare higher among more affluent pop-ulations, effective public health inter-ventions are needed to increasebreastfeeding rates, especially in moredeprived areas.
Strengths and Limitations
The strength of this study is that it isa large whole population study usingroutinely collected data over an 11-yearperiod. Data on maternal and birthcharacteristics, including gestationalage and birth weight, used to defineexposed groups and outcome data
(hospital admissions) were collectedindependently on separate databasesand record-linked. The size of the dataset available for analysis allowed forthe exploration of hospital admissionsacross the range of respiratory causesbyeachweekofgestationalage,avoidingthe need for broader categories thatlimited previous studies.
There are some limitations. As with allanalysesof routinely collecteddatasetsthere is potential for misclassificationin the coding of diagnoses for hospitaladmissions and in the recording ofexposure variables such as gestationalage. However, this is likely to be mis-classification at random, not related toexposure or outcome variables of in-terest, because thesewere collected onseparate data sets. Another limitationwas the high percentage of missingdata on maternal smoking duringpregnancy and lack of data on smokingin the household during childhood, al-though the effect of this is likely to be toreduce the apparent effect of smok-ing on respiratory admissions. Lack ofdata meant we were unable to adjustfor pregnancy complications for themother or comorbidities in children inthe analysis nor could we explore theeffect of the duration of breastfeeding.We used a standard method of multipleimputation to account formissing data.However, a separate analysis using only
TABLE 4 Adjusted HRsa for Emergency Respiratory Admission up to Age 5 for Each Type of Respiratory Emergency Admission and Gestational AgeCategories (N = 318 613)
Gestation (wk) Acute Upper RTIs Influenza andPneumonia
Acute Lower RTIs Acute Bronchiolitis Asthma
HR 95% CI HR 95% CI HR 95% CI HR 95% CI HR 95% CI
40–42 1 1 1 1 139 1.08 1.02–1.15 1.07 1.07–1.12 1.11 1.07–1.16 1.16 1.10–1.21 1.06 0.9–1.1538 1.10 1.02–1.18 1.19 1.09–1.30 1.26 1.21–1.32 1.33 1.26–1.40 1.14 1.03–1.2637 1.12 1.01–1.24 1.27 1.12–1.44 1.54 1.45–1.63 1.59 1.49–1.71 1.16 1.01–1.3335–36 1.08 0.96–1.22 1.53 1.34–1.75 1.73 1.62–1.85 1.89 1.75–2.03 1.20 1.02–1.4033–34 1.26 1.05–1.51 1.68 1.39–2.04 2.17 1.99–2.38 2.45 2.21–2.71 1.56 1.25–1.94,33 1.33 1.08–1.63 3.00 2.55–3.53 3.47 3.20–3.76 3.89 3.55–4.25 2.58 2.13–3.13
RTIs, respiratory tract infections.a Adjusted for maternal age, parity, Townsend score quintile for social deprivation, gender, major or minor congenital anomaly, multiple birth, breastfeeding, Apgar score at 5 min, neonataladmission to hospital, and season of birth.
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 e1567 at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

the completedataonmaternal smokingresulted in similar hazard ratios for thegestational age effects, so it is unlikelythat thehighproportionofmissingdatafor this variable has biased the results.During the 11-year study period, therehave been changes in neonatal care,particularly in respiratory manage-ment, with a trend toward less invasiveand shorter duration of ventilatorysupport for the most preterm infants,andpossiblywidervariation inneonatalrespiratory management for moremature preterm infants. These changesover time might be important influ-encing factors with respect to child-hood respiratory disease, but it was notpossible to explore this within our dataset.
This secondary analysis of routine datacannot address thequestionofwhetheradmission is appropriate. It is notpossible to infer whether a high ad-mission rate represents a high need for
admission or variation in medicalpractice.30,31 Admission rates may behigher from localities with easy accessto hospital or vary with clinical andparental thresholds for admission andorganization of out of hours primarycare services.32 The rate of emergencyhospital admission for respiratoryinfections in children has increasedover the past decade in the UnitedKingdom.31 The majority were short-stay admissions,33,34 suggesting thatthese were for minor illness episodesthat could have been managed in thecommunity.33 Additional investigationis required to identify differences inhealth-seeking behavior and thresh-olds for admission, and presentation,to hospital.
CONCLUSIONS
We have demonstrated the utility ofusing large-scale record-linked data
sets to describe the epidemiology ofhealth care utilization in children,particularly focusing on gestation atbirth. Our key finding is that the gra-dient of decreasing risk of respiratoryemergency admissions with increasinggestational age extends to 40 weeks’gestation. Although the magnitude ofincreased risk appears small, largenumbers of infants are affected withsignificant implications for healthservices.
ACKNOWLEDGMENTSThis study makes use of anonymizeddata held in the SAIL system, which ispart of the national e-health records re-search infrastructure for Wales. We ac-knowledge all the data providers whomake anonymized data available for re-search. Responsibility for the interpre-tation of the information supplied byHealth Information Research Unit isthe authors’ alone.
REFERENCES
1. Costeloe KL, Hennessy EM, Haider S, StaceyF, Marlow N, Draper ES. Short term out-comes after extreme preterm birth inEngland: comparison of two birth cohortsin 1995 and 2006 (the EPICure studies).BMJ. 2012;345:e7976
2. McGowan JE, Alderdice FA, Holmes VA,Johnston L. Early childhood development oflate-preterm infants: a systematic review.Pediatrics. 2011;127;1111–1124
3. MacKay DF, Smith GC, Dobbie R, Pell JP.Gestational age at delivery and specialeducational need: retrospective cohortstudy of 407,503 schoolchildren. PLoS Med.2010;7(6):e1000289
4. Boyle EM, Poulsen G, Field DJ, et al. Effectsof gestational age at birth on health out-comes at 3 and 5 years of age: pop-ulation based cohort study. BMJ. 2012;344:e896
5. Kotecha SJ, Dunstan FD, Kotecha S. Longterm respiratory outcomes of latepreterm-born infants. Semin Fetal Neo-natal Med. 2012;17(2):77–81
6. Davidoff MJ, Dias T, Damus K, et al. Changesin the gestational age distribution amongU.S. singleton births: impact on rates of
late preterm birth, 1992 to 2002. SeminPerinatol. 2006;30(1):8–15
7. Kotecha SJ, Edwards MO, Watkins WJ, et al.Effect of preterm birth on later FEV1:a systematic review and meta-analysis.Thorax. 2013;68(8):760–766
8. Kotecha SJ, Watkins WJ, Paranjothy S,Dunstan FD, Henderson AJ, Kotecha S.Effect of late preterm birth on longitudi-nal lung spirometry in school age chil-dren and adolescents. Thorax. 2012;67(1):54–61
9. Davidson R, Roberts SE, Wotton CJ, GoldacreMJ. Influence of maternal and perinatalfactors on subsequent hospitalisation forasthma in children: evidence from the Ox-ford record linkage study. BMC Pulm Med.2010;10:14
10. Ford DV, Jones KH, Verplancke J-P, et al.The SAIL Databank: building a nationalarchitecture for e-health research andevaluation. BMC Health Serv Res. 2009;9(1):157
11. Lyons RA, Jones KH, John G, et al. The SAILdatabank: linking multiple health and so-cial care datasets. BMC Med Inform De-cision Making. 2009;9(3)
12. Altman DG. Construction of age-relatedreference centiles using absolute resid-uals. Stat Med. 1993;12(10):917–924
13. Townsend P, Phillimore P, Beattie A. Healthand Deprivation: Inequality and the North.London, UK: Routledge; 1988
14. European Surveillance of CongenitalAnomalies (Eurocat). Available at: www.eurocat-network.eu. Accessed February 13,2013
15. White IR, Royston P, Wood AM. Multiple im-putation using chained equations: issuesand guidance for practice. Stat Med. 2011;30(4):377–399
16. Marlow N. Full term; an artificial concept.Arch Dis Child Fetal Neonatal Ed. 2012;97(3):F158–F159
17. Barker DJ, Godfrey KM, Fall C, Osmond C,Winter PD, Shaheen SO. Relation of birthweight and childhood respiratory infectionto adult lung function and death fromchronic obstructive airways disease. BMJ.1991;303(6804):671–675
18. Greenough A, Yuksel B, Cheeseman P. Effectof in utero growth retardation on lungfunction at follow-up of prematurely borninfants. Eur Respir J. 2004;24(5):731–733
e1568 PARANJOTHY et al at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

19. Rona RJ, Gulliford MC, Chinn S. Effects ofprematurity and intrauterine growth onrespiratory health and lung function inchildhood. BMJ. 1993;306(6881):817–820
20. Anand D, Stevenson CJ, West CR, PharoahPOD. Lung function and respiratory healthin adolescents of very low birth weight.Arch Dis Child. 2003;88(2):135–138
21. McLeod A, Ross P, Mitchell S, et al. Re-spiratory health in a total very low birth-weight cohort and their classroomcontrols. Arch Dis Child. 1996;74(3):188–194
22. Matthes JWA, Lewis PA, Davies DP, Bethel JA.Birth weight at term and lung function inadolescence: no evidence for a pro-grammed effect. Arch Dis Child. 1995;73(3):231–234
23. Kotecha SJ, Watkins WJ, Heron J, HendersonJ, Dunstan FD, Kotecha S. Spirometric lungfunction in school-age children: effect ofintrauterine growth retardation and catch-up growth. Am J Respir Crit Care Med.2010;181(9):969–974
24. Petrou S, Mehta Z, Hockley C, Cook-MozaffariP, Henderson J, Goldacre M. The impactof preterm birth on hospital inpatientadmissions and costs during the first
5 years of life. Pediatrics. 2003;112(6 Pt 1):1290–1297
25. Jaakkola JJK, Ahmed P, Ieromnimon A,Goepfert P, Laiou E, Quansah R, JaakkolaMS. Preterm delivery and asthma: a sys-tematic review and meta-analysis. J AllergyClin Immunol. 2006;118(4):823–830
26. Algert CS, Bowen JR, Lain SL, Allen HD,Vivian-Taylor JM, Roberts CL. Pregnancyexposures and risk of childhood asthmaadmission in a population birth cohort.Pediatr Allergy Immunol. 2011;22(8):836–842
27. Pezzotti P, Mantovani J, Benincori N, Muc-chino E, Di Lallo D. Incidence and risk fac-tors of hospitalization for bronchiolitis inpreterm children: a retrospective longitu-dinal study in Italy. BMC Pediatr. 2009;9:56
28. Brown A, Raynor P, Benton D, et al. Indicesof multiple deprivation predict breastfeed-ing duration in England and Wales. Eur JPublic Health. 2010;20(2):231–235
29. National Health Service Information Center,IFF Research. Infant Feeding Survey 2010:Early results. 2011. Available at: https://catalogue.ic.nhs.uk/publications/public-health/surveys/infa-feed-serv-2010-earl-
resu/infa-seed-serv-2010-earl-resu-rep.pdf.Accessed October 11, 2013
30. Esmail A, Quayle JA, Roberts C. Assessingthe appropriateness of paediatric hospitaladmissions in the United Kingdom. J PublicHealth Med. 2000;22(2):231–238
31. MacFaul R, Glass EJ, Jones S. Appropriate-ness of paediatric admission. Arch DisChild. 1994;71(1):50–58
32. MacFaul R, Stewart M, Werneke U, Taylor-Meek J, Smith HE, Smith IJ. Parental andprofessional perception of need for emer-gency admission to hospital: prospectivequestionnaire based study. Arch Dis Child.1998;79(3):213–218
33. Gill PJ, Goldacre MJ, Mant D, et al. Increasein emergency admissions to hospital forchildren aged under 15 in England, 1999–2010: national database analysis. Arch DisChild. 2013;98(5):328–334 doi:10.1136/arch-dischil-2012-302383
34. Saxena S, Bottle A, Gilbert R, Sharland M.Increasing short-stay unplanned hospitaladmissions among children in England;time trends analysis ’97–’06. PLoS One.2009;4(10):e7484
(Continued from first page)
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by a grant from the National Institute for Social Care and Health Research (grant TRP08-006). The research was also supported by The Centrefor the Development and Evaluation of Complex Interventions for Public Health Improvement, a UK Clinical Research Collaboration Public Health Research: Centre ofExcellence and The Centre for the Improvement of Population Health through E-records Research (CIPHER). CIPHER is one of four UK e-health Informatics ResearchCentres funded by a joint investment from: Arthritis Research UK, the British Heart Foundation, Cancer Research UK, the Chief Scientist Office (Scottish GovernmentHealth Directorates), the Economic and Social Research Council, the Engineering and Physical Sciences Research Council, the Medical Research Council, theNational Institute for Health Research, the National Institute for Social Care and Health Research (Welsh Government) and the Wellcome Trust (Grant reference:MR/K006525/1). Funding from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council (grant RES-590-28-0005), Medical ResearchCouncil, the Welsh Government, and the Wellcome Trust (grant WT087640MA), under the auspices of the UK Clinical Research Collaboration, is gratefullyacknowledged.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
ARTICLE
PEDIATRICS Volume 132, Number 6, December 2013 e1569 at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2013-1737; originally published online November 18, 2013; 2013;132;e1562Pediatrics
Demmler, Ronan A. Lyons and David FoneShantini Paranjothy, Frank Dunstan, William J. Watkins, Melanie Hyatt, Joanne C.
ChildhoodGestational Age, Birth Weight, and Risk of Respiratory Hospital Admission in
ServicesUpdated Information &
htmlhttp://pediatrics.aappublications.org/content/132/6/e1562.full.including high resolution figures, can be found at:
References
html#ref-list-1http://pediatrics.aappublications.org/content/132/6/e1562.full.at:This article cites 28 articles, 16 of which can be accessed free
Subspecialty Collections
_tract_subhttp://pediatrics.aappublications.org/cgi/collection/respiratoryRespiratory Tract
gy_subhttp://pediatrics.aappublications.org/cgi/collection/pulmonoloPulmonology
gy_subhttp://pediatrics.aappublications.org/cgi/collection/neonatoloNeonatology
orn_infant_subhttp://pediatrics.aappublications.org/cgi/collection/fetus:newbFetus/Newborn Infantthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on December 15, 2013pediatrics.aappublications.orgDownloaded from