Embed Size (px)
Citation preview

8/3/2019 Pediatrics in Review 1993 Howie 320 3
http://slidepdf.com/reader/full/pediatrics-in-review-1993-howie-320-3 1/6
DOI: 10.1542/pir.14-8-3201993;14;320Pediatrics in Review
Virgil M. HowieOtitis Media
http://pedsinreview.aappublications.org/content/14/8/320the World Wide Web at:
The online version of this article, along with updated information and services, is located on
Print ISSN: 0191-9601.Village, Illinois, 60007. Copyright © 1993 by the American Academy of Pediatrics. All rights reserved.
trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Groveandpublication, it has been published continuously since 1979. Pediatrics in Review is owned, published,
Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on December 14, 2011http://pedsinreview.aappublications.org/ Downloaded from

8/3/2019 Pediatrics in Review 1993 Howie 320 3
http://slidepdf.com/reader/full/pediatrics-in-review-1993-howie-320-3 2/6
FOCUS Q UEST iO NS
1 . H ow can a fi rm diagnos is o f o t i t i s
m edia w ith e ffu sion b e m ad e?
2 . H ow w ell d o techn ica l procedures
su pp ort the d ia gno sis o f t i t i s
media?
3 . W hat fac tors pred i spose to fre -
qu en t or recurren t o titis m ed ia in
ch i ldren?
4. Ho w is th e occurrence o f o titis
medi a re la ted to v ira l in fec tion s?
5 Ho w Is therap y o f ot i t i s med ia
ta ilored b y Id en tifica tion o f th e
resp onsib le pa thogen?
#{149}Pr Jf t ! o r o f Pediatr i cs , D epor tm en t o f
Pediatr i cs , Th e Un ive rs ity o f Te xas M ed ica l
B ran ch at G a lv es ton , G a lv es ton , 7X .
32 0 P ed ia tr ic s i n R ev ie w VoL 14 N o. 8 Augus t 1993
ART iCLE
O titis M ed ia
V irg il M . H ow ie , M D *
Def in i t ions
W hen th e d iag no s is o f o titis m ed ia
h as b een m ade on the b as is o f sk illed
c lin ic al o bse rva tio n and the tym pan ic
m em brane is in tac t, it is p rac tic al to
a ssum e tha t an e ffus io n is p resen t.
H ow eve r, th is can be con firm ed on ly
by recov ery o f flu id from the m idd le
ea r o n tym panocen te s is on m y ringo-
tom y . S eve ral m e thods w ill con firm
the d iagnos is o f e ffus io n w ith the in -
d icated accu racy , as g en e ra lly re -
p o rted in the lite ratu re (T ab le 1 ).
A cu te O titis M ed ia
A com m on erro r in th e d iagno sis o fo tit is m ed ia w ith e ffus io n (OM E ) is
eq ua tin g an “in jected ” on “red” ear-
d rum w ith OM E . A cu te o titis m ed ia
m ay p resen t w ith an in jected drum ,
bu t th e c ritic a l fac to r is no t d rum
co lo r b u t th e p re sen ce of flu id in th e
m idd le ea r cav ity . T he drum fre-
qu en tly is su ffused and red w hen an
in fan t o r to dd ler is cry ing from e ith er
fea r o r pa in du ring th e o to sco p ic ex -
am in atio n . A bu lg ing ea rd rum , o n
the o th er h and , usu ally is rega rded as
de fin ing acu te o titis m ed ia (a lso
ca lled suppuna tiv e o r p uru len t o titism ed ia) w ith o r w ith ou t sym ptom s
(p ain , sleep le ssne ss, fev er, irritab il-
i ty ) o f sys tem ic illn ess .
E xp e rien ced c lin ic ians try to avo id
the “red ea r” erro r w ith e ith er tym -
panom e try o r acou s tic refle ct iv ity
(T ab le 1 ) on by care fu l rem ova l o f a ll
ex te rna l ea r con ten ts to v isua liz e
fu lly th e lan dm arks (eg , bo th end s of
th e m a lleo lu s) and th eir m ob ili ty w ith
th e pneum a tic o tosco pe . T h e prac tic-
in g clin ic ian w an ts to k now w heth e r
an upp er re sp ira to ry in fection , o n ig i-
n ally v ira l in m o st cases , h as b ecom e
com p licated by a b acte ria l in fec tion
w arran ting an tib io tic th e rap y .
F acto rs p ned isp os in g to OM E in-
dude prio r OM E , pro pp ed bo ttle
feed in gs , exposure to in fec tio us
g roups (eg , in day ca re sett ing s), pa -
ren ta l sm ok in g , w in te r sea son , pnes-
en ce o f sib lin gs , and fam ily h is to ry
of freq uen t OM E . C le ft p ala te and
re sp ira to ry a lle rgy a lso a re b eliev ed
to p red ispo se to m idd le ear d isea se .
Ch ro n ic O titis M ed ia
O titis m ed ia w ith pe rs is ten t pe rfo na -
tion a lw ay s has occurred m o re o ften
in m ed ica lly unde rserv ed popu la tio ns
than in popu lations h av in g good ac-
ce ss to ca re , b u t it a lso o ccurs in ra re
ins tances a s a com plica tion of ven ti-
la t ion tu be in se rtio n . R are com p lica-
tio ns o f ch ro n ic o ti tis m ed ia in clu de
m asto id itis, lab yn in th itis , an d cho le s-
te atom a . C ho le s te atom a is m an ifes ted
by chro n ic d ischa rg e th rough a p er-
s is ten t p e rfo rat ion . M asto id itis m aypre sen t a s edem a and tende rne ss o ve r
the m asto id b on e o r occu lt feve r in a
pa tien t w ho h as OM E resistan t to
the rapy . L abyn in th itis is ex trem ely
rare and is m an ifes ted by v ertigo . If
no physical signs of th ese th ree con-
d it ion s are fo und in a ca refu lly ex am -
m ed pa tien t w ho has chro n ic
pe rfo ra tio n and dra inage , add itio na l
in fo rm a tio n m ay b e ob ta ined by con -
su lting w ith an o to la ryngo log is t o r
rad io log is t. T he rad io lo g is t m ay be
ab le to iden tify an o th e rw ise h idden
cho les te a tom a or o ccu lt m asto id itis .
M asto id itis u sua lly re spond s to p ro -
lon ged the rap y w ith an appro pria te
an tib io tic , bu t m ay requ ire su rg ery .
C ho les te a tom a requ ire s su rge ry . T h e
pe rs is ten t p erfo ration of ch ron ic o ti tis
m ed ia req u ire s tym panop las ty a fte r
the ch ild ha s m atu red su ffic ien tly to
have adequ ate re s is tance to recu rren t
OME .
If th erapy w ith th e firs t an tib io tic
ag en t chosen does no t stop dra inage
in 3 to 4 days , d ra in ing flu id sh ou ld
b e cu ltu red from any p erfo ra tio n or
from the lum en o f any p aten t, d ra in -
in g tym panostom y tub es . As eudo-
m ona s in fec tio n often com plica te s
ch ro n ic OM E w ith a v en tila tio n tu be
on o the r pe rfo ra tion . T h is o rgan ism is
e rad icated m o st effec tive ly b y d aily
c lean s ing of the ex tern al and m idd le
ea r w ith suc tio n or by irriga tio n w ith
Bu row so lu tion and the ins tillatio n of
oph th alm ic g rad e an tib io tic so lu tio ns
tha t are e ffec tiv e ag ains t th e p art icu -
Ian s tra in of Pseudomonas isolated.
M ost of th ese lo ca lly in stilled an ti-
b io tic s shou ld b e d isco n tin ued a fte r 3
days h av e p assed w ith ou t m id d le ear
d ra inage becau se they w ould be tox ic
to the coch lea if in s til led in th e ab-
sen ce of m idd le ea r in flam m ation .
T ym pano cen te s is fo r cu ltu re o f th e
m idd le ear flu id in p atien ts w ho have
OM E and are se rio usly ill o r imm u-
no com p rom ised on w ho have an un-
satisfa c to ry re sponse to an tib io tic
the rap y y ie lds in fo rm a tion h e lp fu l to
th e ch o ice o f specific th e rap y . W hen
OME is sym ptom atic (ie , p ain , sleep-
lessn ess , h igh fev er) a fter 2 to 3 d ay s
o f an tib io tic th erapy , tym pano cen -
te s is o f th e in tac t d rum fo r cu ltu re
and aera tio n of the m idd le ear shou ld
be pe rfo rm ed . T h is p rocedu re w ill
iden tify the o ffend ing org an ism and
its sens itiv ity pa tte rn , so the rapy can
b e ind iv id ua liz ed . In sk illed h and s,
tym panocen te sis essen tia lly is com -
p lica tio n -free , w ith n o p ers is ten t pen-
fo ra tio ns o r m idd le ea r dam age .
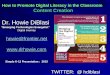
F Tab i I A ccu racy o f Tests
I To C on firm E ffus ion
T ym panocen tesis y ie ld in g flu idm idd le ea r con ten ts: 10 0%
A coustic re flec tiv ity >5 in ch ild
5 m o- 12y : 96%
F la t o r Jen gen typ e B tym panog ram :
90%
Skilled pneum atic o tosco py : 60%
90 %
N onpn eum a tic o to scop y , aud i og r ams , th e
rep o r t o f o ta lg ia , an d other metho Lc p rov ide
usefu l i n format ion but a re no t diagnos t i c of
otit is m ed ia w ith effus io n (OM E).
at Indonesia:AAP Sponsored on December 14, 2011http://pedsinreview.aappublications.org/ Downloaded from

8/3/2019 Pediatrics in Review 1993 Howie 320 3
http://slidepdf.com/reader/full/pediatrics-in-review-1993-howie-320-3 3/6
Tympanocentesis o f t h e in t a c t d r u m fo r cu lt u r e a n d a er a t io n o f
t h e m id d le ear sh ou ld b e performed when symptomati c O M E (ie ,
p a in , s leep le ssn ess , h igh fever ) con t in u e s a ft e r 2 t o 3 d a ys o fa nt ib io t ic t h er ap y.
M a n a g e m e n t
M anagement of either acute OM E on
Pediatrics in Review VoL 14 N o. 8 August 1993 3 2 1
r IN F E C T IO U S D IS E A S E
OU tis M ed ia
In c id e n c e a n d P re v a le n c e
The axiom that you find what you
look for applies to OM E. The mci-
dence of otitis media appears to in-
crease with the intensity with which
the problem is studied and the num-
ben of observations made. A study of
the incidence of OM E in 173 infantsincluded monitoring by tympanome-
try on acoustic reflectometry by
trained technicians, who made an av-
erage of 45 house calls during these
infants’ first 3 years of life. Only in
1 child of the 173 followed was no
evidence of middle ear effusion
found during this period. The per-
centage of the first 3 years of life
spent with OM E among these chil-
dren varied from 0 to 83%, despite
the ready availability of physicians,
antibiotics, and continued free moni-
toning of middle ear status at homevisits.
M ost other reported series in this
and other countries have estimated
the incidence and prevalence of OM E
primarily from observations in medi-
cal settings. In the Scandinavian
countries, selected populations were
invited for special testing (usually
tympanometry) at different consecu-
tive ages so that a cross-section of
the same populations at different ages
and in different seasons could be
viewed. Since the percentage of the
surveyed populations responding to
these invitations was very high, these
estimates of the cross-sectional mci-
dence and prevalence of OM E most
likely are reasonably accurate for the
countries studied. H owever, the mci-
dence and prevalence of OM E cannot
be generalized from one society to
another because of differences in
childrearing practices (eg, breastfeed-
ing, day cane, exposure to crowds,
parental smoking). In this article, I
w ill address primarily the manage-
ment and clinical aspects of OM E as
it occurs in the North American com-
munities with which I am familiar.
P a t h o g e n e s i s
Recent refinements in the detection
of viral infections by antigen detec-
tion, antibody response, and viral
isolation, in combination with new
epidemiologic studies, have led to
the recognition that viruses are in-
volved in about 40% of cases of
acute otitis media. A number of ani-
mal models of otitis media have been
developed, and studies involving
both viruses and bacteria are helping
to elucidate the transmission and
pathogenesis of acute and recurrent
OM E. I t is widely accepted that any
factors in the infant’ s or child’s he-
nedity, early environment, on laterenvironment that increase the chance
of contracting entenic or respiratory
viral infections also increases his on
hen risk for all types of OM E.
One prospective study in a nursery
school for A frican-American children
in N orth Carolina has shown a clear
association between viral respiratory
and entenic infections and subsequent
episodes of otitis media. The investi-
gators recorded in detail how the in-
cidence of OM E surged with
increases in the prevalence of viral
infection each year. Another group of
investigators followed in a medical
setting a fairly large cohort of white
children through the second grade in
school in the Boston area. These in-
vestigators estimated the number ofdays spent with OM E in these chil-
dren during the first 3 years of life
based on the number of episodes ob-
served during medical office visits.
W hen children with less than 30 days
of OM E were compared with those
having more than 1 10 days, a signifi-
cant difference in IQ scores, as ob-
tamed by the W ISC-R test adminis-
tered at the second-grade level, was
found. A nother investigator followed
a group of infants prospectively
through the first 2 years of life in
Cleveland and reported that the “oti-tis-pnone” infant was very likely to
have had bilateral OM E at the second
month check-up. This association be-
tween early onset and more frequent
disease has been reported by other
investigators. The peak prevalence of
OM E is from 6 to 18 months of age.
recently discovered “silent” OM E
(50% of cases are asymptom ati c)
usually involves the systemic admin-
istration of an antibiotic. Therapy
with antihistamines and deconges-
tants has been shown to be ineffec-
tive and sometimes harmful in the
management of acute OM E. The pre-dominant bacterial pathogens causing
O M E in t h is c ou n t r y co n t in u e t o b e
Streptococcus pneum o niae (30% to
40% ), nontypable H aem ophilus in/lu-
enzae (25% to 45% ) , M oraxella
catarrhalis (5% to 20%), and S py-
ogenes (2% to 3% ); less frequently,
Staphylococcus aureus and gram -neg-
ative entenic pathogens are involved.
Recent studies of acute otitis me-
dia have shown that about 40% of
subjects have an acute viral illness at
the same time as the acute OM E is
discovered. The respiratory syncytial
virus is most common, although
other respiratory and entenic viruses
also are found.
Nearly 100% of the M oraxella and
about 20% of theH aem ophilus on-ganisms isolated by tympanocentesis
are beta-lactamase producers and,
therefore, resistant to beta-lactam-
containing amoxicillin and ampicil-
lin. In 1992 and 1993, investigators
in V irginia, W ashington, DC, K en-
tucky, and Texas reported isolation
of pneumococci from ears with acute
otitis media that exhibited moderate-
to-marked penicillin resistance. Some
of these practitioner-investigators nec-
ommended new combinations of anti-
biotics to address this new develop-
ment. T he am inopenicil lins(ampicill in and amoxicillin) always
have been associated with early and-
frequent relapses, and I do not nec-
ommend them as first-line therapy in
the first 24 months of life. Sulfon-
amides given along with erythromy-
cm or penicillin G or V are less
“nelapsogenic” and, thus, are prefer-
able. Scandinavian experience has
never favored the aminopenicill ins.
In comparing the frequency of otitis
proneness (eg, 5 or more attacks) in
at Indonesia:AAP Sponsored on December 14, 2011http://pedsinreview.aappublications.org/ Downloaded from

8/3/2019 Pediatrics in Review 1993 Howie 320 3
http://slidepdf.com/reader/full/pediatrics-in-review-1993-howie-320-3 4/6
Y EARS NUMBER
ANTIB IOTIC* STUD IED T R EAT ED
Amox icillin** 1985 -1987 18 1 8(+ ) 5(+ ) 12(+) 3(+ ) 18%
13 (-) 0Amox icillin! 1988 -1989 15 1 15 0 S t 0 3%
clavulanate 1989 -1991 27 1 28 10 l8 2t 18 %
Ce f i x i me 1 9 8 5 - 1 9 8 7 4 5 1 2 6 1 4 2 8 3 1 4 %
Ce f p od ox i me 1 9 8 8 - 1 9 9 1 2 4 4 2 2 1 1 5 6 1 5 %
Cefpnoz il 1987 -1988 13 1 14 8 4 1 32%
Ce f u r o x i me 1 9 8 7 - 1 9 8 8 1 1 0 5 1 3 0 5%
Clanithromycin 1990-1991 12 0 15 12 5 1 41%
Ceftniaxone 1991 -1993 24 0 30 0 20 3 4%
* Ant ib io t i cs w ere adm inistered p.o. for 10 d ays,xce pt c eftr iaxone , w h ich wa s g iv en IM S O m g/kg o n day 0 on ly.1 On- the r apy cu l tu res usua l l y were ta ken a t 2 to 4 d ays o r nolater than 9 days a fte r s tar t o f th e ra p y.
( +) ind ica tes he to -kc tam ase positive (-) in d ica tes he to -kc tam ase nega tiv e
** O n ly am o xiciilin h ad in vivo g ro w th (failures)e la ted to h e ta -la c tam a se p rod uc tion .
322 P ed ia tr ics in Rev iew V oL 14 N o. 8 A ugu st 1993
IN FEC T IO US D ISEASE
Otitis Med i a
patients treated w ith ampic illin co rn-
pared w ith those treated w ith m ix-
tunes , w e found a 30% inc idence in
the former and 6% incidence in the
latter.
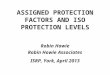
Table 2 contains a list o f antibio t-
ic s recently marketed for OME in the
USA , w ith the ir re lative e ffectivenessagainst the three most common path-
og ens. These culture results came
from tympanocentese s at 2 to 4 days
on-therapy during antibio tic trials
ov er the past 6 years . In 1985 , w e
reported sim ilar studie s on antibio tic s
currently used, but marketed earlier.
W e be lieve that the only w ay to es-
tablish antibio tic efficacy is through
the use o f on-therapy cultures of
samples from the diseased site . It is
apparent from Table 2 that most o f
the failures o f indiv idual antim icro -
bial drug s on therapy are assoc iatedw ith only one of the princ ipal patho -
gens .
Each antibio tic has its ow n pro file
o f efficacy . Remembering that 50%
o f H influenzae strains w ill disappear
after tympanocente sis alone , it is ap-
parent that ce fpro zil, c lanithromyc in,
and amoxicil lin (against be ta lac ta-
mase-positiv e strains) lack efficacy
against this o rganism in children w ho
have o titis m edia. In addition, ce fix -
ime failed to eradicate pneumoco cc i
in 12 o f 45 patients . My recommen-
dation is that antibio tic therapy thatmisse s less than 10% of the know n
princ ipal pathogens is most des irable .
Any antibio tic that misse s 30% or
more o f the principal pathogens
should be used only w hen the partic -
ular pathog en invo lved in the ear at
the tim e is know n to be sensitiv e to
that antibio tic , as demonstrated by
tympanocente s is , culture , and sensi-
tiv ity te sting . Most frequently , w e
w ill have available antibio tic s thatare only 80% effectiv e , and the anti-
bio tics that meet this requirement
change through tim e .
In a paper demonstrating the “Po l-
lyanna” effect, one investig ato r has
show n that le ss v igo rous evaluation
methods than on-therapy culture (eg ,
clinical re sponse ) are unable to show
significant differences betw een most
antibio tic s w ithout huge numbers of
subjec ts . A ntibio tic s are evaluated
best by the ir in v ivo effectiveness in
elim inating o rganism s judged to be
pathogenic in causing o titis m edia. Itw ould appear that even co rrec tion of
the failure o f am inopenic ill ins against
beta-lactamase producers (by addition
o f clavulanic ac id) w as fo llow ed by
the dev elopment of another fo rm of
res is tance , w hich appeared in the
influenzae organisms w e iso lated be-
tween 1 9 8 9 and 1991 .
Ma n a g e m e n t a n d P r e v e n t io n
o f t h e O t it is -p r o n e C o n d it io n
D espite symptomatic contro l o f acute
infections and produc tion of sterilityin middle ear fluid, a s ignificant
number of children, espec ially in-
fants, remain otitis -prone. Care ful
fo llow -up of antibio tic -treated OME
w ill show that 20% to 40% of infants
and toddlers have pers is tent middle
ear fluid for periods vary ing from 6
to 12 w eeks . Patients should be fo l-
low ed until the m iddle ear is normal
and contains air. OME is accom-
panied by up to a 40- to 50-dBdecrease in hearing acuity (av erag ing
25 dB) .
The medical community varies as
to how aggress iv ely and w ith w hat
therapy this condition should be
treated. It is fairly w ell e stablished
that breast feeding of infants de-
crease s and that attendance at nursery
schoo ls increase s the occurrence of
the otitis -pnone condition. How ever,
some authorities believ e that no pen-
manent disability comes from months
or y ears o f OME and that aggressive
therapy (such as co rtico stero idadm inistration on placement o f venti-
latory tubes) should be reserved fo r
the w orst case s. O thers , inc luding
myse lf, believ e that diminished hear-
ing and pers is tent OME should not
be to lerated at any ag e; w e advocate
the placement of pressure equaliza-
tion (PE) tubes w hen OME has per-
s is ted fo r 6 to 12 w eeks despite tw o
courses o f appropriate antibio tic then-
apy . The occurrence of three epi-
sodes of OME in 6 months on four
episodes in 12 months also should
lead to the placement o f PE tubes ,pre ferably under lo cal anesthesia w ith
appropriate sedation in the outpatient
se tting . Hearing te sts in the presence
S T R E P T O C O C C U S
P N E U M O N IA E
NUMBER
CUL TURE -
POS IT IVE t
H A E M O P H IL U S
IN F L U E N Z A E
NUMBER
NUMB E R C ULTUR E -
TR E ATE D P O S IT IVE t
M O R4Y.ELLA
CATARRHAL IS
NUMBER
NUMB E R C ULTUR E -
TREATED POS ITIVEt
K N OWN
P A T h O G E N
P E R C E N T
FA ILURES
at Indonesia:AAP Sponsored on December 14, 2011http://pedsinreview.aappublications.org/ Downloaded from

8/3/2019 Pediatrics in Review 1993 Howie 320 3
http://slidepdf.com/reader/full/pediatrics-in-review-1993-howie-320-3 5/6
Pediatrics in Review VoL 14 No. 8 August 1993 3 2 3
IN F E C T IO U S D IS E A S E
O titis M e d i a
of fluid are expected to show a m od-
enate hearing loss. PE tubes im prove
hearing im m ediately, and the im -
provem ent lasts until the tube is ex-
tnuded on until the next ear infection
occurs. M anagem ent is designed to
keep the m iddle ear air-filled w ith
norm al hearing. In 90% of patientsreceiving tubes, ear infections occur
m uch less frequently follow ing tube
placem ent than before. F unctioning
PE tubes bypass the eustachian tube
to provide m iddle ear ventilation, but
do not change the susceptibility to in-
fectious agents. W hen infection oc-
curs, the etiology is easy to ascertain
by culturing the fluid draining from
the tubes.
S u rg ic a l M an ag em en t
P rior to the advent of antibiotics,
m yningotom y frequently w as used to
alleviate pain and drain the m iddle
ear cavity w hen it w as filled w ith
purulent m aterial. Effective antibiotic
therapy can sterilize the m iddle ear
cavity, but m iddle ear effusion m ay
persist in the absence of a m iddle ear
pathogen. In the 1950s, one investi-
gaton reintroduced the insertion of
ventilation tubes through the tym -
panic m em brane to reestablish the
eardrum as a drum (m em brane w ith
air on both sides). W hen antibiotics
have not been successful in elim inat-
ing the effusion in O M E, the persist-
ent ventilation of the m iddle ear w ith
the various types of A rm strong tubes
has been practiced w idely. Their in-
sertion can be perform ed as an outpa-
tient procedure w ith local ionto-
phonesis anesthesia by using
xylocaine and epinephnine after ap-
propriate sedation. W e favor this
m o de of treatm ent in conjunction
w ith the adm inistration of prophylac-
tic doses of sulfonam ide in patients
younger than 2 years of age on 20
m g /kg of erythnom y cin or am o xicillin
in patients w ho are 2 years on olden
or w ho are allergic to one of the
other drugs.
T raditionally, adenoidectom y has
been advocated to help prevent recur-
rent acute otitis m edia; this has been
show n to be effective in olden age
groups, but not in the 6- to 18-
m onth-old infants and toddlers inw hom the incidence of O M E is high-
est. W ith general anesthesia and hos-
pitalization, this procedure entails
greaten risk and expense. T onsillec-
tom y has not been show n to be of
any benefit in controlling O M E . For
procedures that are beyond his on her
skills (eg, PE tube insertion, tym pa-
noplasty, on adenoidectom y w hen ap-
pnopniate), the prim ary care physician
can refer the patient to an otolaryn-
gologist. D iagnostic tympanocentesis
for identification of resistent patho-
gens on relief of severe pain shouldbe am o ng the pediatrician’s skills.
P r o g n o s i s
W ith persistent, conscientious pni-
m ary m edical cane, the outlook for
infants and children w ho have O M E
is generally very good. There are
very few persistent perforations, and
the incidences of m astoiditis and cho-
lesteatom a are m uch low er than prior
to the m odern era. It is hoped that
w ith the advent of effective vaccines
against respiratory syncytial virus and
som e of the other respiratory and en-
tenic viral pathogens, the precursor
viral infections that com m only lead
to O M E w ill be elim inated. W ith
better conjugated vaccines against the
com m on bacterial invaders, these
also m ay be controlled, and the
scourge of recurrent O M E m ay be
relegated to history, along w ith po-
liom y elitis, m easles, m um p s, rubella,
diphtheria, and pertussis.
S U G G E S T E D R E A D IN G
A m erican Speech-Language-H earingA ssociation. G uidelines for screening for
hearing im pairm ents and m iddle ear
disorders. ASHA. 1990;32(suppl 2):17-24
A rola M , R uuskanen 0, Ziegler T, et al.
C linical role of respiratory virus infection in
acute otitis m edia. Pediatrics. 1990;86:848-
855
A rola M , Z iegler T , R uuskanen 0. R espiratory
virus infection as a cause of prolonged
sym ptom s in acute otitis m edia.I Pedia tr .
1990116:697-701
B luestone C D . M odern m anagem ent of otitism edia. Pediatr Clin North Am. 1989;36:
1371-1378
C arlin SA , M ar chan t C D , Shu r i n PA , Johnson
C E, Super D M , R ehm us JM . H ost factors
and early therapeutic response in acute otitis
m edia. J P edi atr . 1991;118:178-183
C honm aitree T, O w en M i, H ow ie V M .
R espirato ry viru ses interfere w ith
bacteriologic response to antibiotic in
children w ith acute otitis m e dia.J I nfect
Dis. 1990;162:546-549
C honm aitree 1, O w en M J, Patel JA , H edgpeth
D , H or l i ck D , H ow ie V M . E f f ect of v i r al
respiratory tract infection on outcom e of
acute otitis m edia. J P edi atr . 1992;120:856-
862
H enderson GW , G ieb in k G S. O t i t is m ed iaam o ng children in day care: E pidem iology
and pathogenesis. Rev I nfect D is. 1986;8:
5 3 3 - 5 3 8
H ow ie V M , D illard R , Laurence B . In vivo
sensitivity test in otitis m edia: E fficacy of
antibiotics. Pediatrics. 1985;75:8-13
Lampe RM , Schwar t z RH . D iagnost i c v al ue of
acoustic reflectom e try in children w ith acute
otitis m edia. Pediatr Infect D is J. 1989;7:
59-61
M archant C D, C arlin SA , Johnson C E, Shurin
PA . M easu r in g th e com par at i ve ef f i cacy of
antibacterial ag en ts for acute o titis m edia:
T he “pollyanna phenom enon. “ I Pediatr.
1992;120:72-77
M archant C D , Shurin PA , Turczyk V A,
W asikow ski D E, Tutihasi M A , K inney SE.C ourse and outcom e of otitis m edia in early
infancy: A prospective study.J P edi atr .
1984; 104:826-831
P aradise JL . L ong-term effects of short-term
hearing loss-m enace or m yth?Pediatrics.
1983;71 :647-648
Paradise JL , R oger s K D. O n ot i t i s m ed ia,
child developm e nt, and tym p anostom y
tubes: N ew answ ers or old questions?
Pediatrics. 1 9 86 ; 7 7 : 8 8- 9 2
Sade J, Luntz M . A denoidectom y in otitis
m edia. A review . Ann Owl Rhino!
Larayngol. 1991;100:226-231
Teele D W , K lein JO , C hase C , M enyuk P.
R osner B A. O titis m edia in infancy and
intellectual ability, school achievem ent,
speech, and language at age 7 years. G reaterB oston O titis M edia Study G roup.J I nfect
Dis. 1990;162:685-694
at Indonesia:AAP Sponsored on December 14, 2011http://pedsinreview.aappublications.org/ Downloaded from

8/3/2019 Pediatrics in Review 1993 Howie 320 3
http://slidepdf.com/reader/full/pediatrics-in-review-1993-howie-320-3 6/6
DOI: 10.1542/pir.14-8-3201993;14;320Pediatrics in Review
Virgil M. HowieOtitis Media
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/14/8/320including high resolution figures, can be found at:
Permissions & Licensing
/site/misc/Permissions.xhtmlits entirety can be found online at:Information about reproducing this article in parts (figures, tables) or in
Reprints /site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at Indonesia:AAP Sponsored on December 14, 2011http://pedsinreview.aappublications.org/ Downloaded from