Embed Size (px)
DESCRIPTION
pemeriksaan ankle and foot
Citation preview


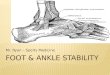
Anatomy
There are 26 bone in the foot7 tarsal , 5 metatarsal, 14 phalanges

Movements at the ankle joint are mainly dorsiflexion and plantarflexion
The foot externaly rotates with dorsiflexion and internally rotates with plantarflexion
The lower leg muscle is divided into four compartments (superficial and deep posterior, lateral, anterior)
Only one muscle on the dorsum of the foot ( digitorum brevis)

The muscle on the planter aspect of the foot are divided into four layers
The planter fascia is a very important structure that takes its origin from the heel and inserts into the bases of the proximal phalanges of the toes
Blood supply from ( anterior & posterior tibial, peroneal arteries)
Nerves (posterior tibial, saphenous, sural, superficial & deep peroneal)

1 -Club foot2 -Flat foot

- Relatively common; the incidence is 1 or 2 /1000 births
-Boys are affected twice as often as girls.
-The condition is bilateral in one-third of cases.
- Similar deformities are seen in neurological disorders, e.g. myelomeningocele, and in arthrogryposis.

- It’s mostly a problem passed from parents to children (genetic), and it may run in families
If you have one baby with clubfoot, the chance of having a second child with the condition are about one in 40 .
-Clubfoot does not have anything to do with the baby’s position during pregnancy.

The deformity is usually obvious at birth; the foot is both turned and twisted inwards so that the sole faces posteromedially.The heel is usually small and high, and deep creases appear posteriorly and medially.The infant must always be examined for associated disorders such as congenital hip dislocation and spina bifida.



In fact, doctors can see it on ultrasound images taken after about four months of pregnancy

X- rays : the tarsal bones are incompletely ossified at this age. However, the shape and position of the tarsal ossific centers are helpful in assessing progress after treatment


If the condition is not corrected early, secondary growth changes occur in the bones and these are permanent.
Relapse is common, specially in babies with associated neuromuscular disorders .
1-Conservative treatment:Should begin early, preferably within a day or two of birth.It consists of repeated manipulation and
adhesive strapping or application of plaster of Paris casts, which will maintain the correction.

2 -Operative treatment: The objectives are:
A-The complete release of joint tethers (capsular and ligamentous contractures and fibrotic bands)
B-Lengthening of tendons, so that the foot can be positioned normally without undue tension.

After operative correction, the foot is immobilized in its corrected position in a plaster cast.Kirschner wires are sometimes inserted across the intertarsal and ankle joints to augment the hold. The wires and cast are removed at 6-8 weeks.After that, hobble boots (Dennis Browne) or a customized othosis are used to maintain the correction.


Infantile Flat Foot (Congenital Vertical Talus)
Flat Foot in Children and Adolescents
Flat Foot in adults

It’s a rare neonatal condition usually affects both feet.
In appearance it is the very opposite of a club-foot; the foot is turned outwards (valgus) and the medial arch is not only flat, it actually curves the opposite way from the normal, producing the appearance of a “rocker-bottom” foot.


X-ray features are characteristic:The calcaneum is in equinus and the
talus points into the sole of the foot, with the navicular dislocated dorsally onto the neck of the talus.
Passive correction is impossibleThe only effective treatment is by
operation, ideally before the age of 2 years.


When weight-bearing, the foot is turned outwards and the medial border of the foot is in contact with the ground; the heel becomes valgus.Two forms of the condition are recognized:
1 -Flexible flat-foot2-Stiff (rigid) flat-foot

Which appears in toddlers as a normal stage in development.It usually disappears after a few years when medial arch development is complete. The arch can be restored by simply dorsiflexing the great toe.Many of the children with flexible flat-foot have ligamentous laxity and there may be a family history of both flat-feet, and joint hypermobility.

-Which cannot be corrected passively, and should alter the examiner to an underlying abnormality.
-In older children and adolescents, conditions to be considered are
1-Tarsal coalition (often a bar of bone connecting the calcaneum to the talus or the navicular)
2-Inflammatory joint condition 3-Neurological disorder.


flexible flat-foot: no symptoms, but the parents notice that the feet are flat or the shoes wear badly, the deformity becomes noticeable when the youngster stands.The first test :ask the patient to go up on tiptoes: if the heels invert, it is a flexible deformity. Then examine the foot with the child sitting or lying. Feel for localized tenderness and test the range of movement in the ankle, the subtalar and midtarsal joints. A tight Achilles tendon may induce a compensatory flat-foot deformity.

Teenagers and young adults sometimes present with a painful, rigid flat-foot.On examination, the peroneal and extensor tendons appear to be in spasm,sometimes its called “Spasmodic flat-foot”In some cases a definite cause may be found, but in many no specific cause is identified.The spine, hips, and knees should always be examined as well as, joint hypermobility and neuromuscular abnormalities.

- X-ray are unnecessary for asymptomatic, flexible flat-feet.
- For Pathological flat-feet (usually painful, and stiff), standing AP, lateral and oblique views may help to identify underlying disorders.
-CT scanning is the most reliable way of demonstrating tarsal coalitions.

Young children with flexible flat-feet require no treatment. Parents need to be reassured.If the condition is obviously due to an underlying disorder such as poliomyelitis, splintage or operative correction and muscle rebalancing may be needed.Spasmodic flat-foot is relieved by rest in a cast or a splint. If there is an abnormal tarsal bar or other bony irregularity, this may have to be removed.In late cases, if pain is intolerable, a triple arthrodesis may be necessary.

When adults present with symptomatic flat-feet the first thing to ask is whether they always had flat-feet or whether it is of recent onset.More recent deformities may be due to an underlying disorder such as rheumatoid arthritis or generalized muscular weakness,Unilateral flat-foot should make one think of tibialis posterior synovitis or rupture.Patients with painful rigid flat-feet may require more robust splintage.Those with tibialis posterior rupture can be helped by operative repair or replacement of the defective tendon