Embed Size (px)
Citation preview
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 1/121
MEIHO INSTITUTE OF TECHNOLOGY
GRADUATE SCHOOL OF HEALTH CARE
MASTERS THESIS
A CORRELATIONAL STUDY OF KNOWLEDGE, ATTITUDES AND
COMPLIANCE OF HAND HYGIENE AMONG HEALTHCARE WORKERS
A Thesis submitted to the Graduate school of Meiho Institute of Technology
in partial fulfillment of the requirements for the degree of Master of Science in Health Care
Submitted by: Bui Vu Binh
Supervisor: Yang Tsan
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 2/121
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 3/121

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 4/121
ABSTRACT
Hand hygiene (HH) is the simplest, most effective measure for preventing nosocomial
infections, but poor HH compliance among healthcare workers (HCWs) has been found in
many studies. This study had been conducted (1) to describe demographic characteristics,
knowledge and attitude as well as compliance of HH; (2) to identify major factors that
influence and affect HH compliance; (3) to explain the relationship among demographic
characteristics, knowledge and attitude toward HH compliance among HCWs. A cross-
sectional study, which uses utilized both observational form and questionnaire, was conducted
in the two hospitals in Hanoi, Vietnam. In the first phase, 578 observational periods (4862 HH
opportunities) were conducted among random patient-rooms. The second phase, 500 HCWs
include doctors, nurses, and other clinical HCWs were surveyed by using a questionnaire.
The response rate was 70.2% (358 questionnaires), among them 312 questionnaires were
analyzed. The Statistical Package for Social Sciences (SPSS) for Windows (version 11.5)
was used to analyze the data. The results showed that the knowledge score on HH of
participants was good; but some gaps remained. The knowledge score was related
significantly with equipment availability (basin, handrubs available in patient room) and age
of HCWs, while it was not associated with other demographic factors (hospital, daily working
time, patient intensity, gender, job, education, and working experience of HCWs). The
participants’ attitudes to ward HH was positive; it could be affected by some factor such as

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 5/121
Log-Linear analyses showed that multi-factors associated to HH compliance such as the
distance, handrubs availability, type of HCWs, and the risk levels of HH opportunities. These
study results provided important evidences of HH compliance and suggested that suitable
interventions could be applied to improve HH compliance in the Vietnamese context.
Keywords: hand hygiene, hand washing, infection control.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 6/121
ACKNOWLEDGEMENTS
I will never forget the two-year of study in Taiwan. It not only changed my career, but
also my life. The completion of my Masters thesis has been a difficult undertaking. I do need
to thank many people who offered their inspiration; encouragement and guidance to help me
achieved my goal. It is impossible to list all of them.
Special thanks go to Professor Hsiu-Yueh Hsu, my committee chairman, for her
guidance and wisdom in leading me throughout my academic effort. I wish to express my
sincere appreciation to my thesis committee members Professor Shu-Hui Yeh and Professor
Yang Tsan, for their guidance and support, which led to more clarity in my thinking.
Professor Yang Tsan, my supervisor has patiently stayed with me throughout this study.
I would like to thank him, very much, for his instruction, insights, and guidance during my
graduate studies. I am greatly indebted to him a lot.
I would never thank enough Dr. Yu-Chia Chen and Dr. Michael R. Black for their
support and guidance. They treated me not only like a student, but also like a family member.
I also would like to thank many other professors at Meiho Institute of Technology for helping
me in both academic and personal life. My friends, Su-Chen Huang, Hui-Ping Huang, Quang-
Trung Truong, Jui-Yun Tsao, and many others, have "stuck with me, through thick and thin."I just want to let them know that they remain in my heart.
I would like to thank my colleagues at Vietduc Hospital and National Pediatric Hospital
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 7/121
care me. Their sacrifices could not be expressed in words. I would never have completed my
degree without the support from all of my family members -- especially my lovely wife,
Nguyen Thi Thu Hien, and my son, Bui Tuan Minh. They were put at a strong disadvantage.
They are my firm rear; their support provided me with the courage to persevere throughout
my graduate education.
Last, I am grateful to the Meiho Institute of Technology for providing me with financial
support during my study period. Thanks, also, to Hanoi Medical University for its support for
my career and for my gaining knowledge.
With best regards, to All.
DEDICATION
This study is dedicated to my parents, Bui Xuan Tuong and Vu Thi Thanh, who are
always caring, loving, and supporting, every step of my way. Mom, I will never forget that
while you were afflicted with brain cancer (Glioma), you would still not allow me to quitting
my studies. Dad, you have taken care of Mom even better than many trained health care
workers. I lean a lot from you.
To my lovely wife, Nguyen Thi Thu Hien and my dear son Bui Tuan Minh, who
sacrificed, a lot, during my period of study. They had to face many difficulties while I was outof the country. You are a treasure in my heart.
To my brother, Bui Vu An and his family, and to my sister, Bui Kim Anh. To my
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 8/121
CONTENTS
PageAbstract………………………………………………………………………………… i
Acknowledgement……………………………………………………………………… iii
Dedication ……………………………………………………………………………... iv
Contents………………………………………………………………………………… v
List of Tables…………………………………………………………………………… viiiList of Figures …………………………………………………………………………. ix
List of Abbreviations…………………………………………………………………… x
Chapter 1: Introduction 1
1.1. Statement of the Problem………………………………………………………… 1
1.2. Problem: Background and Significance………………………………………….. 21.3. Statement of Purpose……………………………………………………………… 3
1.4. Summary…………………………………………………………………………… 3
Chapter 2: Literature Review 4
2.1. Review of Relevant Literature……………………………………………………... 4
2.1.1. Theoretical Review…………………………………………………………. 42.1.2. The Relationship of Demographic Factors to Hand Hygiene Behavior……. 8
2.1.3. Knowledge and Attitudes of Hand Hygiene as Related to Hand Hygiene
Compliance…………………………………………………………………. 11
2.2. Theoretical Framework……………………………………………………………. 19
2.3. Summary…………………………………………………………………………… 22Chapter 3: Conceptual Framework 23
3.1. Framework Development………………………………………………………….. 23
3.1.1. The Framework……………………………………………………………. 23
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 9/121
4.4.1. Training the Observers…………………………………………………. 30
4.4.2. Pilot study…………………………………………………………….... 30
4.4.3. Validity and Reliability…………………………………………………. 30
4.4.4. Data Collection ………………………………………………………… 32
4.5. Data Analysis………………………………………………………………………. 33
4.5.1. Data Screening and Recoding ………………………………………….. 34
4.5.2. Analyses………………………………………………………………… 35
4.6. Ethical Consideration……………………………………………………………… 35
4.7. Summary…………………………………………………………………………… 36
Chapter 5: Findings 37
5.1. Analyze Questionnaire data ……………………………………………………….. 37
5.1.1. Descriptive Profiles ……………………………………………………. 37
5.1.2. Knowledge, Attitude of Hand Hygiene relate to Demographic
characteristics………………………………………………………….. 41
5.1.3. Hand Hygiene Compliance by Self-report……………………………… 52
5.2. Analyze Observational data………………………………………………………... 55
5.2.1. Descriptive Profiles……………………………………………………... 55
5.2.2. Relationship of Hand Hygiene Compliance and Demographic
characteristics…………….…………………………………………..
58
5.2.3. Log-Linear Model analyses…………………………………………….. 65
5.3. Other findings……………………………………………………………………… 75
5.4. Summary…………………………………………………………………………… 76
Chapter 6: Discussions 77
6.1. General discussion…………………………………………………………………. 77
6.2. Main finding in context of references……………………………………………… 79
6 3 Suggested Model 84
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 10/121
Appendixes
Appendix 1: The questionnaire of Hand hygiene practice…………………………. 94
Appendix 2: Hand hygiene observational form…………………………………….. 100
Appendix 3:Translated version of the questionnaire (Vietnamese version)……… 101
Appendix 4: Translated version of the Observational form (Vietnamese version)… 107

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 11/121
LIST OF TABLES
Page
Table1: Reliability analyses: Cronbach’s alpha…………………………………………… 32
Table 2: Profile of the two hospitals by questionnaire……………………………………. 39
Table 3: Profile of the participants by questionnaire………………………………………. 40
Table 4: Hand hygiene knowledge score………………………………………………….. 42
Table 5: Hand hygiene knowledge divides in groups……………………………………… 42
Table 6: Statement of each knowledge answer……………………………………………. 43
Table 7: Hand hygiene attitude score……………………………………………………… 46
Table 8: Hand hygiene attitude score divides in groups…………………………………… 46
Table 9: Statement of each attitude answer………………………………………………... 47
Table 10: Relationship between knowledge, attitude and each characteristic of the
hospitals…………………………………………………………….………… 50
Table 11: Relationship between knowledge, attitude and each characteristic of the
participants …………………………………………………………………… 52
Table 12: Association between knowledge and attitude toward hand hygiene…………… 53
Table 13: Correlation between knowledge and attitude…………………………………… 53Table 14: Hand hygiene compliance by self report………………………………………... 54
Table 15: Frequencies of the observational data…………………………………………... 57
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 12/121
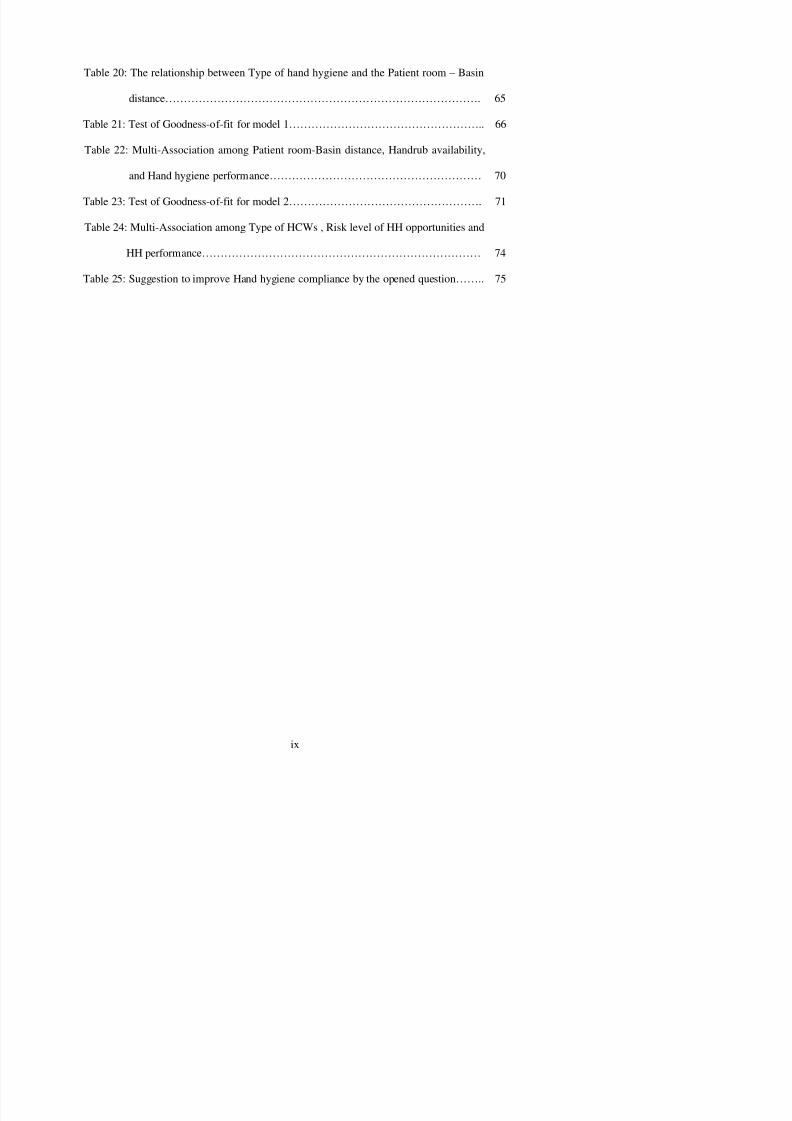
Table 20: The relationship between Type of hand hygiene and the Patient room – Basin
distance…………………………………………………………………………. 65
Table 21: Test of Goodness-of-fit for model 1…………………………………………….. 66
Table 22: Multi-Association among Patient room-Basin distance, Handrub availability,
and Hand hygiene performance………………………………………………… 70
Table 23: Test of Goodness-of-fit for model 2……………………………………………. 71
Table 24: Multi-Association among Type of HCWs , Risk level of HH opportunities and
HH performance………………………………………………………………… 74
Table 25: Suggestion to improve Hand hygiene compliance by the opened question…….. 75
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 13/121
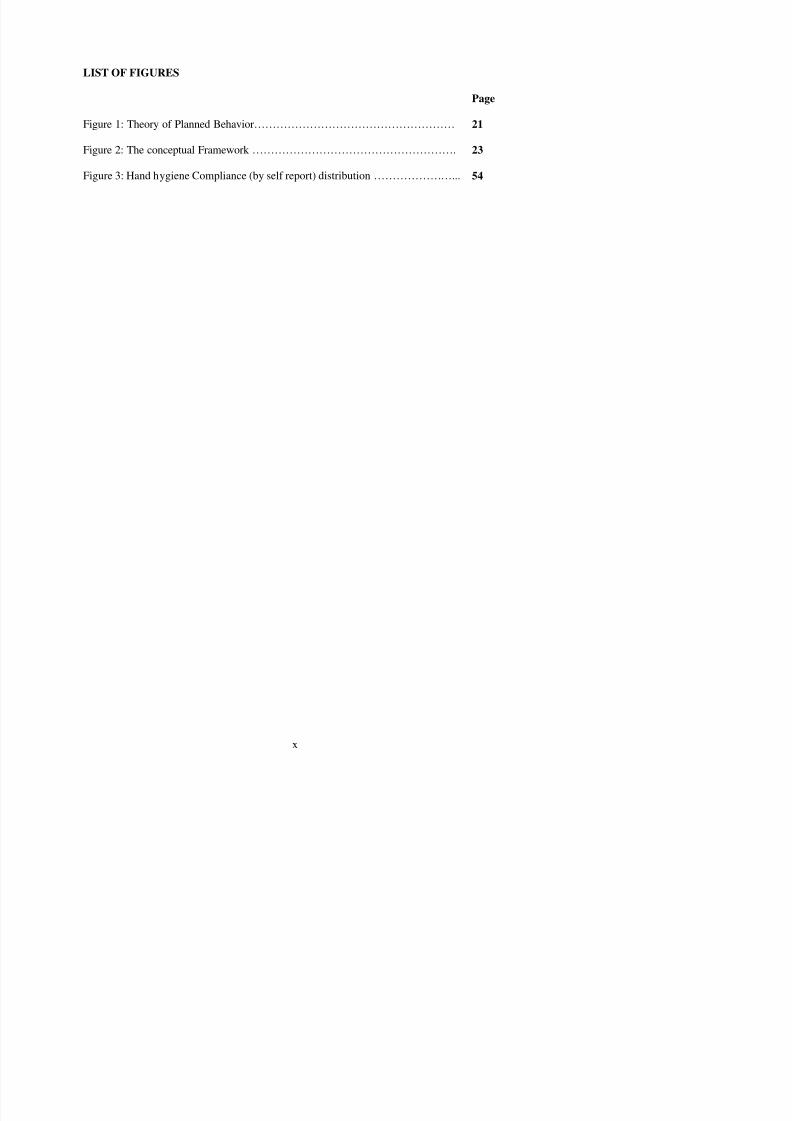
LIST OF FIGURES
Page
Figure 1: Theory of Planned Behavior……………………………………………… 21
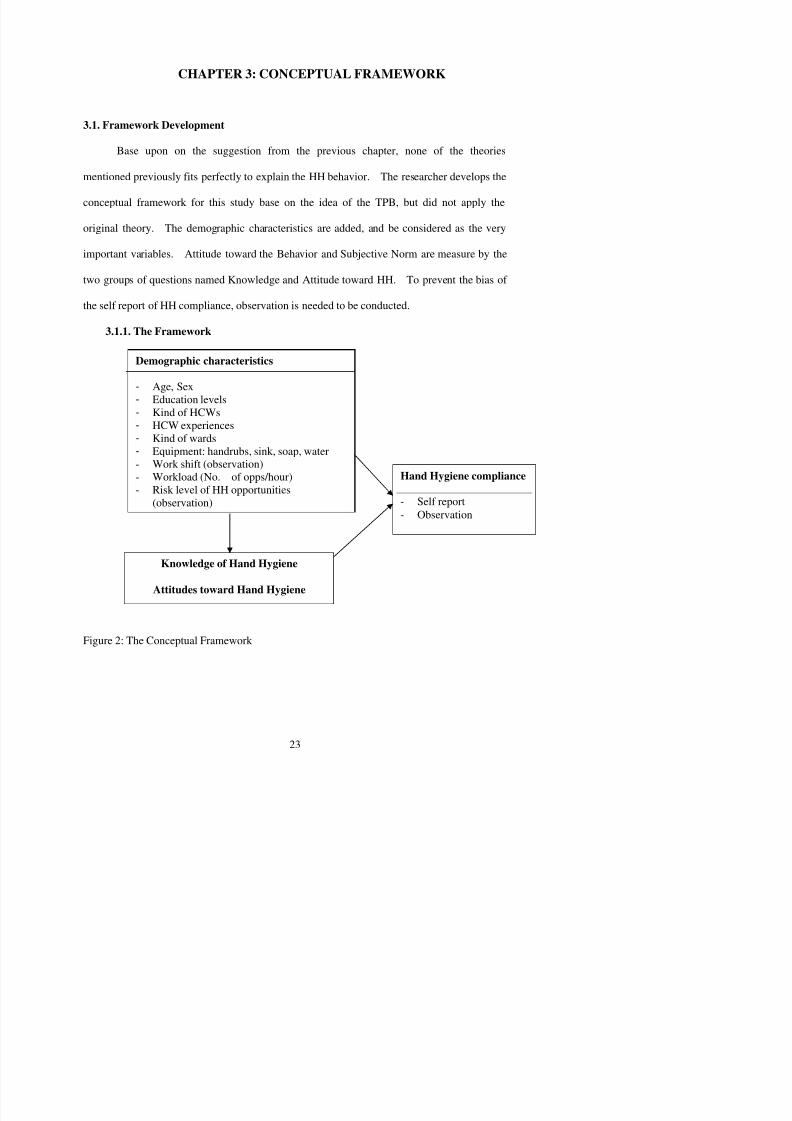
Figure 2: The conceptual Framework ………………………………………………. 23
Figure 3: Hand hygiene Compliance (by self report) distribution …………………... 54
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 14/121
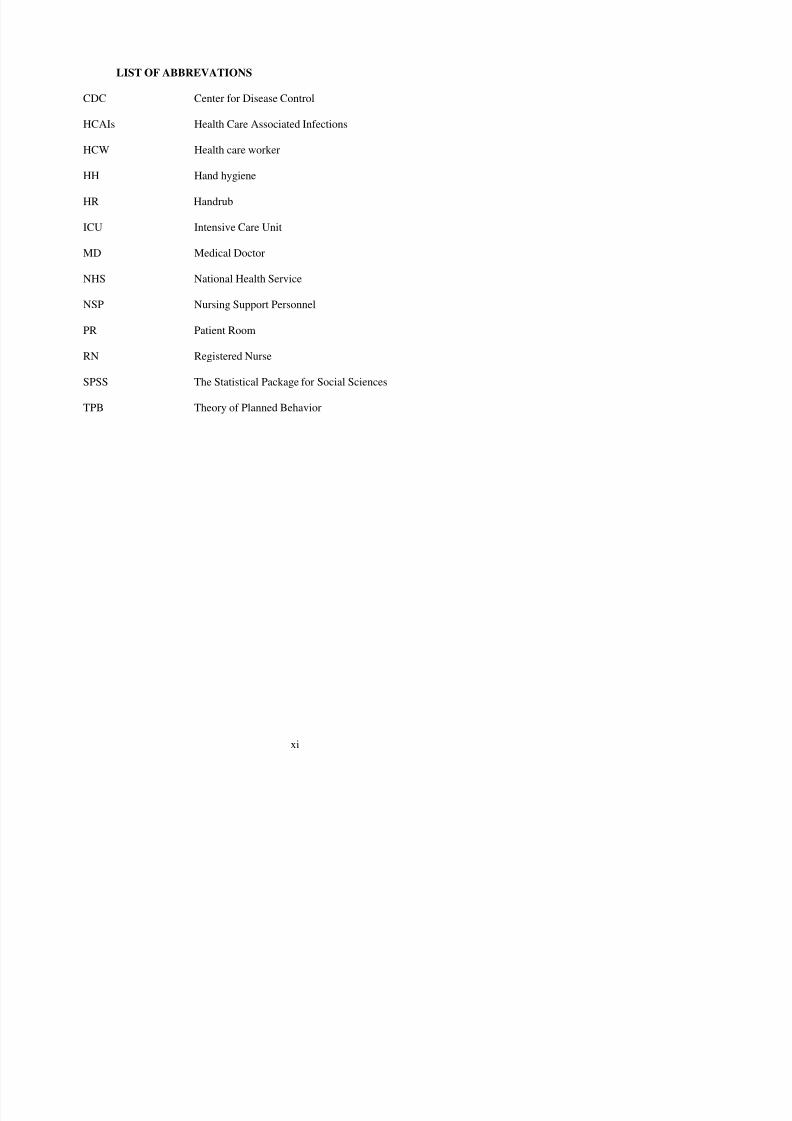
LIST OF ABBREVATIONS
CDC Center for Disease Control
HCAIs Health Care Associated Infections
HCW Health care worker
HH Hand hygiene
HR Handrub
ICU Intensive Care Unit
MD Medical Doctor
NHS National Health Service
NSP Nursing Support Personnel
PR Patient Room
RN Registered Nurse
SPSS The Statistical Package for Social Sciences
TPB Theory of Planned Behavior
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 15/121
CHAPTER 1: INTRODUCTION
1.1. Statement of the Problem
There are nearly two centuries since Ignaz Semmelweis (1818-1861) demonstrated the
hazard of contaminated hands in the transmission of disease in a health care setting (Carter,
1981). Today, HH decontamination is considered as the most effective means of preventing
and controlling nosocomial infection. However, HH compliance rate among HCWs was low
in many different studies. Many hospitals still have the problem to persuade medical staffs
to comply with the simple procedure of HH. (O’Boyce & Pittet, 2002; Carter, 1981)
From 1975 to now, many guidelines for HH have been published by Centers for
Disease control (CDC) (in 1975, 1985, and 2002), and some other organizations. In 1988, and
1995, Association for Professionals in Infection Control (APIC) announced its own
recommendation. In 1995 and 1996, the Healthcare Infection Controls Advisory Committee
(HICPAC) recommended that either antimicrobial soap or waterless antiseptic agents be used
for cleaning hands upon leaving the rooms of patients with multi-drug resistant pathogens.
Those recommendations become well understood by HCWs, but the compliance rate
improves slowly and maintains difficultly at high rate.
In a review of literature from 1977 tot 1995, Larson (1999) indicated a temporal
relation between HH practice and the rates of nosocomial infection rates. Despite this
established relationship, compliance with HW among HCWs remains low (Doebbeling et al.,
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 16/121
2003 and January 2004. Therefore, it was calling for a campaign on hand washing. It knew
that some of these infections are avoidable and the present situation is obviously unacceptable
in a twenty first century health service. Consequently, The National Patient Safety Agency
has undertaken a major body of work to tackle healthcare associated infection in the shape of
“the clean your hands campaign”. It was designed to help NHS organizations improve HH
and reduce the spread of infections. (The National Patient Safety Agency, 2004).
1.2. Problem: Background and Significance
The idea of using HH to prevent the spread of nosocomial infection is not a new
concept. The study results showed (Conly, et al., 1989) HH was the single most important
procedure in the prevention of nosocomial infections and yet it remains the most violation of
all infection control procedures. With a sequential intervention study in an intensive care unit,
the authors had demonstrated that poor HH practices were associated with a high nosocomial
infection rate, whereas good HH practices were associated with a low nosocomial infection
rate
At the time of starting this study, the researcher could not find any study on HH in
Vietnam published in international journals. Inside the country, the number of studies on HH
behavior was not many; most of their finding focused on the relationship between HH and
nosocomial infection or the effectiveness of some specific handrubs (Nguyen, Vuong, & Le,
2002; Nguyen, Nguyen, Truong, & Doan, 2007), few of them paid attention on finding the
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 17/121
the effect of HH on nosocomial infection. Some hospitals in Vietnam are trying to apply their
best effort to improve hand washing adherence among their staffs. Assessing the results of
those activities could help us realize the achievement of our work, and find out the gap in
practicing this activity. Hopefully, this study could demonstrate some correlation between
factors and compliance of hand washing, then we could give more suitable interventions to
improve the situation.
The researcher conducted the study in the two hospitals in Hanoi, Vietnam. Those
hospitals were not only the leading national hospital but also cooperated with Hanoi Medical
University in training students. Thus, besides serving patients, they also were the places
where students could learn their professional. Improving hand washing compliance there, not
only could help decrease the nosocomial infection in hospitals, but also help students learn
good habits.
1.3. Statement of the Purpose
The purposes of this study are
(1) to explore demographic characteristics, knowledge and attitude as well as compliance
of HH;
(2) to identify major factors that influence and affect HH compliance;
(3) to explain the relationship among demographic characteristics, knowledge and
attitude toward HH compliance.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 18/121
CHAPTER 2: LITERATURE REVIEW
2.1. Review of Relevant Literature
For generations, HH with soap and water was considered a measure of personal hygiene.
By the early 19th century, very soon after the discovery of an antiseptic agent, HH became
accepted as one of the most important measures for preventing transmission of pathogens in
health-care facilities. Up to now, there has been much research conducted on this topic. These
not only focused on the clinical field, but also in many other fields. These research findings
connected HH to various parts of life. Here, the researcher simply investigates the roles of HH
in the clinical field.
2.1.1. Theoretical Review
HH compliance is special behavior, which can be explained by many behavioral
theories. Six main theories were found when reviewing literature about HH compliance.
They were: (1) Biomedical Model; (2) Operant Behavior and Social Learning; (3) Diffusion
of Innovations; (4) Role Theory; (5) Theory of Planned Behavior; and (6) Precede Theory.
Each of these theoretical orientations viewed HH compliance from a different perspective.
In 1999, a group of authors in Japan did a study to ascertain the hand washing
compliance of all personnel and visitors to the ICU (Nishimura, Kagehira, Kono, Nishimura,
& Taenaka, 1999). During the study, a guideline was posted on the entrance door to the unit,
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 19/121
the invasion of foreign agents, genetic factors or the natural breakdown of the body’s parts or
processes. In this study, the recommendation of the expert (foreign agents) could affect to the
hand washing compliance (disease).
Operant and Social Learning Behavioral Models evolved from learning theories
developed by psychologists such as Pavlov, Skinner, Hull and Tolmen. The models payed
attention to the stimuli or cues that elicit behavior, the rewards that reinforce behavior, the
gradual shaping or patterning of behavior and its automation after sufficient repetition. The
models also could explain the HH compliance of HCWs. Following is an example. Hand
washing compliance was significantly different at a baseline (43%) and during a promotional
program (80%) (Won et al., 2004). In these open trial studies, the reinforcements were
financial incentives, and regular group feedback. The study findings suggested that we could
use reinforcements as an effective method to improve HH compliance.
In an attempt to further understand the low compliance with hand washing guidelines,
the author did a study for his thesis to apply the theory, Diffusion of Innovations (Abouselof,
1999). The theory maintains that any idea perceived as new to an individual is termed
innovation and the spread of the innovation is termed diffusion. Within this theory is the
innovation-decision process of which there are five stages: knowledge, persuasion, decision,
implementation and confirmation. The results showed significantly lower perceptions of
adoption for alcohol based hand rubs than for hand washing. When comparing units, the acute
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 20/121
HH opportunities in an old hospital (417 opportunities), and in a new hospital (304
opportunities). The average HH compliance was 35.7%, and it was better in the old hospital
(53%) rather than was in the new hospital (23%) ( p< .001). The results showed the better HH
compliance after HH opportunities (35.7%) than before HH opportunities (8.5%) ( p< .001).
A key finding of the study was that when a higher ranking person in the room did not perform
HH, other HCWs were significantly less likely to wash their hands (OR, .2; 95%CI, .1 to .5).
After adjustment for factors correlated to HH compliance, the authors, again, found that HCW
present in the room with a higher ranking person who did not perform HH were significantly
were, themselves, less likely to wash their hands (OR, .4; 95%CI, .2 to .6). Along with that,
some other factors were found significant (i.e.: using gloves, performing an invasive
procedure, working at the old hospital, performing HH on room entry, and having patient
contact.) The results suggest that HCW’s HH compliance was influenced significantly by the
behavior of other HCWs.
Another group of authors conducted a study to test an explanation model for
adherence to HH guidelines based on the Theory of Planned Behavior (TPB) (Boyle, Henly,
&Larson, 2001). As part of the study, HH adherence was estimated, the relationships among
motivational factors, adherence, and intensity were, also, described. The authors used a
longitudinal observational design to collect data from 120 RNs. The results showed the rate of
adherence to recommendations was 70% (a range of 61% to 74%). Correlations among the

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 21/121
remains an enigma to be explained. Actual HH behavior may be more sensitive to the
intensity of work activity in the clinical setting than to internal motivational factors.Another study based upon the TPB was also conducted to identify beliefs and
perceptions associated with intention to comply with HH (Pessoa-Silva et al., 2005). There,
61 questionnaires were analyzed. Most of respondents (41 of 61) believed that they could
improve their own compliance with HH, and 74% (45 of 61) believed that at least half of
health care associated infections are associated with microbiological contamination of HCWs’
hands. Around 43% of the respondents claimed to have never attended specific training
sections, yet most of them acknowledged their exposure to posters promoting HH at least
once a week. A positive intention to comply with HH was 61%, and most of them considered
it useful to perform HH before and after every direct contact with patient (53% to 89%).
However, some factors of non adherence with HH were mentioned --“contact with different
body sites in the same patient” (49%), “after glove removal” (31%), and “after contact with
equipment linked to the neonate” (43%). The mean score for intention to perform HH was 6.5
(SD = .7). Only a perceived control over the difficulty to perform HH (OR, 3.1; 95%CI, 1.1 to
8.7) and a positive perception of superiors toward HH (OR, 2.9; 95%CI, 1.1 to 7.8) were
independently associated with intention to HH compliance. Some other reasons for difficulty
to perform HH were skin irritation, using gloves, and failure to remember.
The interventional program relied heavily on the Precede model and aimed to
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 22/121
relation to HCWs’ attitudes, beliefs and knowledge ( p< .05).
2.1.2. The Relationship of Demography Factors to Hand Hygiene Behavior
In 1999, Pittet, Mourouga, Perneger et al. published an article in the journal of
Annals of Internal Medicine. This study aimed to identify predictors of noncompliance with
handwashing during routine patient care in the teaching hospital in Geneva. The findings
showed that, among 2834 handwashing opportunities, the handwashing compliance was 48%
(with soap was 34% in instances and with hand antiseptic was 14%). In detail, the nurses
washed hands more often than doctors, nurse assistants, and others (in sequence, 52% vs. 30%,
47%, and 11%). The HCWs tended to clean their hands less often during morning shift (45%),
and on the weekdays (46%). Workload played the important role in compliance with
handwashing; the more the number of opportunities per hour, the worse the compliance.
Among the wards, the lowest compliance rate (36%) was found in ICUs, while the highest
rate (59%) was observed in Pediatric units. In addition, the compliance with handwashing was
lower among high-risk opportunities, rather than among low-risk opportunities.
In 2001, Lipsett, and Swoboda published a study to determine whether handwashing
behavior was affected by the health care professional status and patient interaction. The
authors observed a surgical intermediate care unit in a university teaching hospital. The
results showed the handwashing compliance was lowest among doctors (MD, 15%), it was
better among nursing support personnel (NSP, 37%), and highest among nurses (RN, 50%). In
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 23/121
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 24/121
study period, the authors observed 3143 patients’ activitie, including 1091 hand-cleansing
opportunities at high or medium-risk, among 187 patients. The results showed that, thecompliance with hand-cleansing was 19.6%, in which, the HCWs washed hands with soap
and water 19% of chances, and with alcohol based products in 71% of chances. In detail, the
study found that the predictor for noncompliance included caring for patient older than 65
year-old (OR, 2.23; 95%CI, 1.40-3.57) and those recovering from clean-contaminated-surgery
(OR, 2.27; 95%CI, 1.11-4.76), as well as high intensity of patient care (OR, 1.01 per patient
care activity; 95%CI, 1.0-1.02). It would be said that, the higher the workload, the higher the
number of indications for hand-cleansing and the lower the compliance. In addition, the
compliance with hand-cleansing was lower among contact with patients already admitted to
the postanesthesia unit (12.5%).
Wendt, Knautz, and Baum (2004) observed HH behavior of the HCWs in the
University Hospital of Heidelberg. During nine months observation, they observed 2138 HH
opportunities, divided in 15 groups based on the Fulkerson scale, 31.7% of the opportunities
was made by physician, and the rest 68.3% was made by nurses. The lowest frequency of
handrub use was observed after contact with material that had had no patient contact (12.4%).
After contact with feces, antiseptic handrub was used in nearly all (97.3%) of the observations.
When contacting with infectious material directly or indirectly, the compliance ranged from
78.6% to 85.1%. Nurses complied with rubbing hands more frequently than did physicians
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 25/121
pathogens, and wearing gloves was not considered a mean of obviating HH.
2.1.3. The Knowledge and Attitudes of Hand Hygiene as Related to Hand Hygiene
Compliance
This section not only presented about the effects of knowledge and attitudes toward
HH compliance, but also kept mentioning the effects of demographic characteristics.
The group of researchers from Li-Shin Hospital in Taiwan conducted a study to assess
the knowledge and attitude toward HH compliance among nurses (Lim, Yeh, Jao, & Huang,
2001). The participants of the study were 166 nurses with working-experience less than two
years, and the measurement was the questionnaire. The results showed the mean test score of
the correct answers was 79.5 in possible of 90 score. The nurses in the Out patient
Department tended to have lower knowledge score than the nurses did in ICU (82.8) and other
wards (80.6). The wrong answers were found mostly in following issues: handwashing is the
simplest effective method to prevent nosocomial infection; handwashing is not necessary after
touching patient, contact the medical instrument which patient uses, or contact with medical
records; no need to take off rings or hand watch before handwashing. Handwashing was done
mostly after manipulation of patients’ secretions and excretions, as well as after the toilet and
patient contact. The seasons of do not washing hands included: “too busy” (88.6%), the sink
is too far from the patients’ bed” (45%), and “the cleansing product is too irritating to the
skin” (31.3%).
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 26/121
patient” (61.58%), “handwashing mainly removed transient flora on hand” (72.88%), and
“Gloves should be changed even they are not visibly contaminated during patient care”(79.66%). Knowledge of HH was different significantly among departments (F =5.643, p
= .004), the worse knowledge score was found among nurses worked in Surgery department
(mean= 17.91; SD= 2.48) compared to the nurses worked in Internal department (mean=
19.01; SD= 1.94) and the nurses worked in Emergency &ICU (mean= 19.03; SD=1.70).
Two most frequent self-reported factors of incompliance with HH were “Skin irritation and
dryness caused by hand antiseptics” (73.44%), and “busy workload” (65.53%).
The questionnaire had been used to assess the knowledge, beliefs and practices
regarding nosocomial infection, central venous catheter care and HH of HCWs worked in
neonatal ICU (Kennedy, Elward, & Fraser, 2004). The findings showed some gaps in HCWs’
knowledge, such as only 31% of HCWs knew the recommended duration of handwashing,
35% knew that bacterial hand counts are higher when rings are worn. Similarly, only 30%
knew that long fingernails (30%) and artificial fingernails are associated with higher gram-
negative contamination of HCWs’ hands. As the result, the low rate of participants believed
that ring (40%), artificial fingernails (61%), or long fingernails (48%) played a role in
nosocomial infection. Conversely, some other beliefs toward HH were good, most of
participants believed gloves (91%), and handwashing (99%) could prevent nosocomial
infection, and 74% agreed that they would voluntarily remove artificial fingernails or cut long
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 27/121
directly about HH and gloves use. The results showed the good knowledge of HH in context
of precautions. The most frequent reasons of noncompliance were “lack of knowledge” (47%),“lack of time” (42%), “forgetfulness” (28%). The authors found the better knowledge and
attitudes of HCWs correlated with previous training courses.
Nobile, Montuori, Diaco, and Villary (2002) mailed 620 questionnaires to HCWs
working in 31 ICUs, in Italy; the responded rate was 66% (after sending the questionnaires
three times). The findings of the study showed that participants knew well about the definition
of hospital acquired Infection (HAI) (90%), and were aware that inadequately decontaminated
instruments and hands of HCWs increases the risk. Most of them (93.2%) recognized the role
of compliance with infection control protocols. Whereas, lack of knowledge regarding
decontamination procedures was encountered in 38.9%. A total agreement with the correct
responses to the questions on knowledge was 53.2% of participants. The knowledge was
higher in neonatal (OR, 2.39; 95%CI, 1.18-4.88), and medicine surgery (OR, 3.47; 95% CI,
1.79-6.71) compared with the coronary ICUs. The larger the ICUs’ patient bed, the better the
HCWs’ knowledge score. Most of them agreed that HH reduces the risk of infection in
patients (96.8%) and personnel (86.2%), and that the guidelines should be used and
maintained (93%). However, 41,2% of participants believed that routine hand
decontamination can cause skin irritation. The positive attitude was significantly higher
among older and female HCWs and those who had better knowledge. The self-report HH
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 28/121
continuing education courses, 36.4% of them relied on scientific journals, and 11.5% leant
from colleagues. More than half (55.5%) felt they needed additional information.Pittet et al. (2004) conducted a study to identify risk factors for nonadherence and
assess beliefs and perceptions associated with HH among physicians. The authors observed
163 participants, and then gave them the questionnaire to ask them about beliefs and
perceptions. The findings showed the general HH adherence was 57%, and varied markedly
across medical specialties. The highest HH adherence was found among internists (87%), and
the lowest HH compliance was found among anesthesiologists (23%). There was 73% of
participants (N=111) answered that they knew about the observation, and results showed that
these participants had higher HH compliance (61%) than did physicians who did not know
about the observation (44%). The higher workload and opportunities for HH related to high
risk for cross-transmission were associated with reduced adherence. Analyzing the
questionnaires, the group of authors found some highlights. Most of the participants (85%)
were aware of the risk for cross-transmission to the patient resulting from nonadherence.
There were 77% of them intended to adhere to HH, and that they were motivated to improve
their adherence level (74%). However, less than 30% had a positive attitude toward HH after
taking off gloves. Although 65% of the respondents had a good knowledge of indications,
67% perceived HH as a difficult task, and only 35% considered that they knew the
recommended guidelines on HH. Some positive beliefs or perceptions affected to HH
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 29/121
those, therefore, many studies were conducted to report the result, as well as explored the
relationship between HH compliance and the factors. Herein, some of them would bementioned.
The prospective observational study was conducted in the Virginia Hospital with six-
month long in 1997 (Bischoff, Reynolds, Sessler, Edmond, & Wenzel, 2000). The authors
observed 1575 HH opportunities in the two ICUs to investigate the efficient of an education,
feedback, patient awareness and alcohol based handrub toward HH compliance. Fist
intervention were education/feedback program, and patient awareness program; followed by
increasingly accessible handrubs, initially available at ratio of one dispenser for four patients,
and subsequently one for each patient. The low HH compliance at the baseline was surveyed,
and found among HCWs in the medical ICU (MICU) (10% before patient care, and 22% after
patient care), and in the Cardiac surgery ICU (CSICU) (3% before patient care, and 13% after
patient care). After the education/feedback intervention sessions, the handwashing compliance
in the MICU was 16% (before patient care) and 25% (after patient care), and in the CSICU
7% (before patient care) and 14% (after patient care). These compliances did not increase
significantly. The next intervention, increasing accessible handrubs, brought the significant
changing of HH compliance. With one alcohol dispenser available for every four beds, the
handwashing rate was 19% prior to patient contact and 41% afterward. Still higher rates were
noted with a dispenser-bed ratio of 1:1—23% before patient contact and 48% afterward.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 30/121
improved progressively from 48% in 1994, to 66% in 1997 ( p<.001). The findings showed
that the rate of washing hands with soap and water was stable (around 30%), yet the rate ofusing handrub increased (13.6% to 37.0%, p< .001) made the change in general compliance.
The compliance was lower with high-risk opportunities than the medium and low-risk
opportunities; this result was unchanged during study progress. Remarkably, although it
increased among nurses and nursing assistants ( p<0.001), average compliance remained low
among doctors and other HCWs (31.1% [SD 5.3] and 39.5 [6.2], respectively) with no
significant trends over time (linear trends, p=0.92 and p=0.54, respectively). During the study
period, overall nosocomial infection decreased (prevalence of 16.9% in 1994 to 9.9% in 1998;
p=0.04), Meticillin-resistant Staphylococcus aureus transmission rates decreased (2.16 to
0.93 episodes per 10 000 patient-days; p<0.001), and the consumption of alcohol-based
handrub solution increased from 3.5 to 15.4 liters per 1000 patient-days between 1993 and
1998 ( p<0.001). Shortly, the hospital-wide program made the increasing of HH compliance
and reducing the nosocomial infection; and some most important factors were handrubs, type
of HCWs.
An observational study was conducted in Argentina to measure the effect of two
interventions: education alone and education plus performance feedback toward HH
compliance (Rosenthal, McCormick, Guzman, Villamayor, & Orellano, 2003). The baseline
(phase 1) survey was conducted followed by education alone program (phase 2), and
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 31/121
unit, 54%; and non-ICUs, 56%), work shift (morning, 47%; afternoon, 49%; and night,64%),
and type of HCWs (nurses, 55%; physicians, 37%; and ancillary staff, 33%). Shortly, HH
compliance rate was affected by varies demographic characteristics such as knowledge (made
by education), and attitudes (increasing by feedback).
In a prospective open trial Rosenthal, Guzman, and Safdar (2004) evaluated the effect
of education and performance feedback regarding catheter care measures and handwashing
compliance in the two ICUs in Argentina. During nearly three years of the study progress, the
authors observed 7347 catheter-days (1779 catheter-days during baseline period, and 5568
catheter-days during intervention period). The results showed the compliance with
handwashing (from 23.1% to 65.2%; RR, 2.82; CI95, 2.49 to 3.20; p < .0001). Catheter-
associated urinary tract infection (UTI) rates decreased significantly from 21.3 to 12.39 per
1,000 catheter-days ( RR, 0.58; CI95, 0.39 to 0.86; p = .006). These meant implementing
education and performance feedback increased the hand washing compliance; and that
associated with reduction of UTI rates.
The literature reviewing of O’Boyce (2001) summarized the changing of Antiseptic
technology. The study showed the current trend of using antiseptic method, and the reasons
why it was changing. The accessibility of HH facilities (such as sink, soap, water, towels,
alcohol based antiseptics, etc.) was the important factor. The HCWs needed to spend 62
seconds for a handwashing (go to the sink, wash, and go back), thus HH become very difficult
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 32/121
antiseptics would be offset by cost savings. The acceptance of HH products by HCWs was
needed to encourage HCWs comply with the recommendations. The references showed that
not all HH products are equally acceptable to personnel. Most considered issues related to
hand skin condition, such as skin dryness, cracking, redness, or itching. There were many
HCWs believed that rubbing hand with hand antiseptics causes more skin problem rather than
washing hand with soap and water, while many studies showed opposite. This suggested the
important role of education to promote personnel’s knowledge and attitude.
In 2002, O’Boyce, & Pittet reviewed 423 published-articles to construct a guideline
for HH in the Infect Control Hosp Epidemiol journal. It became the formal recommendations
for HCWs of CDC and was accepted worldwide. The Guideline for HH in Health-Care
Settings provided a review regarding handwashing and hand antisepsis in health-care settings.
In addition, it provided specific recommendations to promote improved hand-hygiene
practices and reduced transmission of pathogenic microorganisms to patients and personnel in
health-care settings. This report reviewed studies published since the “1985 CDC guideline”
and the “1995 APIC guideline” was issued. It provided an in-depth review of HH practices of
HCWs, levels of adherence of personnel to recommended HH practices, and factors adversely
affecting adherence. New studies of the in-vivo efficacy of alcohol-based hand rubs and the
low incidence of dermatitis associated with their use were reviewed. Herein, recent studies
demonstrating the value of multidisciplinary HH promotion programs and the potential role of
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 33/121
population) had been signed on to the Global Patient Safety Challenge in October 2005. A
year after that, on last November 13 more countries pledged commitment to the initiative, and
seven countries and regions reported on their first year of achievements. The report also
emphasized that the infection acquired in hospital was 5% to 10% of patient in developed
countries, and it was around 15% in some developing countries. Many countries had already
substantially improved HH practice that could be good example for joining the program.
The WHO world Alliance for Patient Safety called the others to join “Clean care is Safer care”.
In most of recent studies, the results indicated that handwashing compliance was
strong related to nosocomial infection (Pittet et al., 2000; Rosenthan et al., 2004; Won et al.,
2004). Although, handwashing was the simple technique, yet it was difficult to explain and
control. There were many behavioral theories were applied, but none of them were really
fitted to explain the behavior. The result turning back from self-report and the observed result
were quite different. Many factors related to the handwashing compliance, therefore, non
single-intervention can improve handwashing compliance much (Pittet, 2001). The improving
of HH compliance was usually motivated by HH campaigns which included some interventions.
As the previous review, the researcher found varies demographic factors could affect
to HH compliance. Some most important demographic factors were sex, workload,
professional status, the department, and so on. Knowledge and attitudes toward HH played the
different perspective in explanation HH behavior. Some most frequent issues were using
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 34/121
could explain the behavior well? The researcher found that HH was the special social
behavior., of course, could be explained by many behavioral theories (this would be presented
on the literature review section). However, not all of them could explain the behavior well.
HCWs’ behavior related to HH is a complex phenomenon; it is not easily understood or
explained by a single variable or a cluster of variables from one domain. HCWs interaction
with their environments affects HH behaviors. Among the theories, the Theory of Planned
Behavior (TPB) seemed fitter than some others did.
Some main characteristics of the theory would be presented herein.
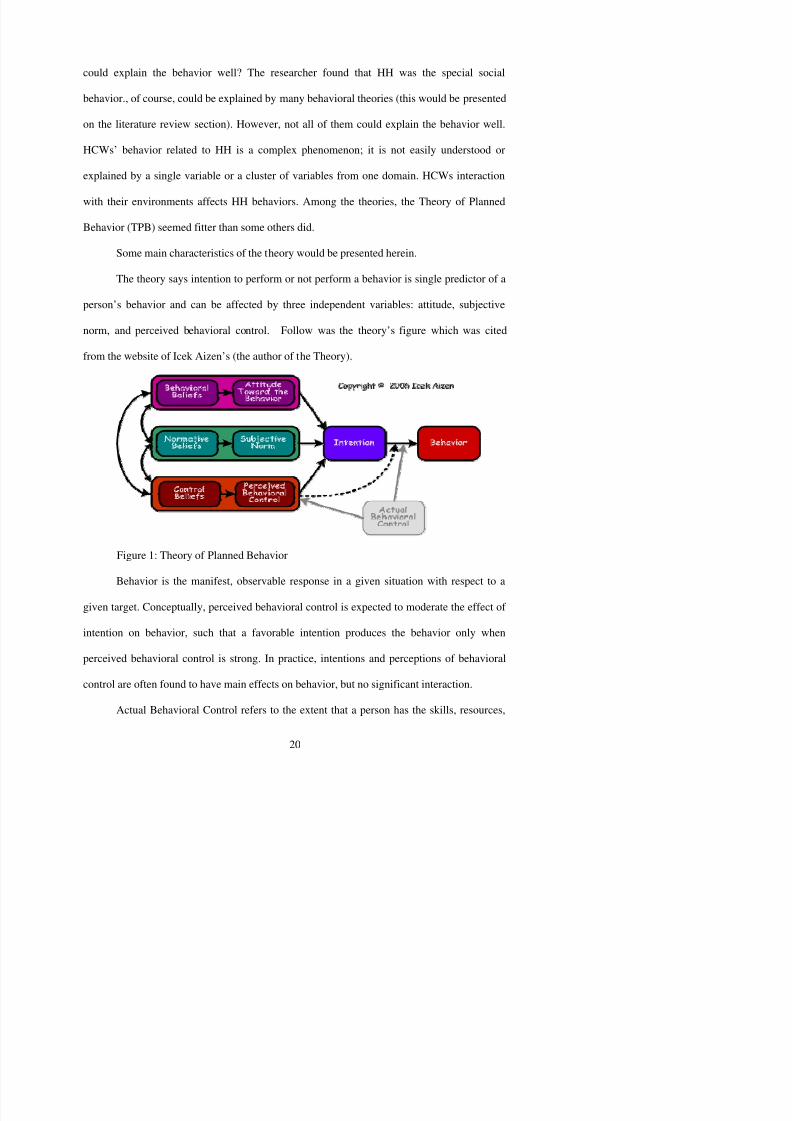
The theory says intention to perform or not perform a behavior is single predictor of a
person’s behavior and can be affected by three independent variables: attitude, subjective
norm, and perceived behavioral control. Follow was the theory’s figure which was cited
from the website of Icek Aizen’s (the author of the Theory).
Figure 1: Theory of Planned Behavior
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 35/121
and other prerequisites needed to perform a given behavior. Successful performance of the
behavior depends not only on a favorable intention but also on a sufficient level of behavioral
control. To the extent that perceived behavioral control is accurate, it can serve as a proxy of
actual control and can be used for the prediction of behavior.
Intention is an indication of a person's readiness to perform a given behavior, and it is
considered to be the immediate antecedent of behavior. The intention is based on attitude
toward the behavior, subjective norm, and perceived behavioral control, with each predictor
weighted for its importance in relation to the behavior and population of interest.
Attitude toward the behavior is the degree to which performance of the behavior is
positively or negatively valued. According to the expectancy-- value model, attitude toward a
behavior is determined by the total set of accessible behavioral beliefs linking the behavior to
various outcomes and other attributes.
Hive norm is the perceived social pressure to engage or not to engage in a behavior.
Drawing an analogy for the expectancy-value model of attitude, it is assumed that subjective
norm is determined by the total set of accessible normative beliefs concerning the
expectations of important referents. Specifically, the strength of each normative belief (n) is
weighted by motivation to comply (m) with the referent in question, and the products are
aggregated.
Subjective norm is the perceived social pressure to engage or not to engage in a
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 36/121
al., 2001), though some other author did not totally agree with that. In a doctoral dissertation,
the researcher did not found the relationship existed between TPB and HH behaviors (Hassan,
2005). However, the author still believed that the theory could explain the HH behavior if it
was modified. The author added some items such as Age, Gender, Year of Experience,
Nurse/patient ratio and Skin condition.
2.3. Summary
The chapter has been reviewed many literatures related to HH behavior. It supports
the researcher the overview of the HH picture; through it shows that HH behavior in general
and HH compliance in particular is still need to be explored more. There are many factors
relate to HH compliance, however they are different among studies. In addition, the
framework of the study should be developed base on TPB, which means the researcher can
not apply the original one.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 37/121
Demographic characteristics
- Age, Sex
- Education levels- Kind of HCWs- HCW experiences- Kind of wards- Equipment: handrubs, sink, soap, water- Work shift (observation)- Workload (No. of opps/hour)- Risk level of HH opportunities
(observation)
CHAPTER 3: CONCEPTUAL FRAMEWORK
3.1. Framework Development
Base upon on the suggestion from the previous chapter, none of the theories
mentioned previously fits perfectly to explain the HH behavior. The researcher develops the
conceptual framework for this study base on the idea of the TPB, but did not apply the
original theory. The demographic characteristics are added, and be considered as the very
important variables. Attitude toward the Behavior and Subjective Norm are measure by the
two groups of questions named Knowledge and Attitude toward HH. To prevent the bias of
the self report of HH compliance, observation is needed to be conducted.
3.1.1. The Framework
Hand Hygiene compliance
- Self report- Observation
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 38/121
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 39/121
HH opportunity happens after patient’s contact/care or after contacting with body fluids.
“Low risk” indicates that the HH performance while doing hospital maintenance, and
during indirect patient’s contact.
Visibly soiled hands were hands showing visible dirt or visibly contaminated with
proteinaceous material, blood, or other body fluids (e.g., fecal material or urine).
Working shifts are divided in three groups, morning, afternoon, and evening base
on the rule of daily working time.
Workload (patient intensity) refers to the number of HH opportunities which occur
in a unit of time (opportunities/hour).
Waterless antiseptic agent referred to an antiseptic agent that does not require use
of exogenous water. After applying such an agent, the hands are rubbed together until
the agent has dried.
3.2. Research hypotheses
1. Different demographic characteristics would result in significantly different in hand
hygiene compliance.
2. Difference knowledge score lead hand hygiene compliance different.
3. Attitudes correlate to handwashing compliances.
4. Multi-factors associate with handwashing compliance.
3 3 S
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 40/121
CHAPTER 4: MATERIAL AND METHODS
4.1. Research design
There were many studies had done in HH subject, those studies followed various study
designs. To explore HH compliance and factors toward HH compliance some authors used
Review literature method (Pittet, 2001; Larson, 2001). Some others used cross-sectional
design with mailed questionnaire (Nobile et al., 2002), or directed questionnaire (Pessoa-Silva
et al., 2005). In order to find out more about the difference between self-reported and
observational result, some studies used cross-sectional design with both observation and
questionnaire (Pittet, Simon et al., 2004). Longitudinal observation was used as the study
design of some researches (O'Boyle, Henly et al., 2001). A quasi-experimental design - open
trial design, which has more advantages itself compared with some other kinds of study
methods were used in some published papers (Creedon, 2005; Won et al., 2004). Choosing
suitable study design is very important when conducting a research. Each kind of design has
its own advantages and disadvantages.
The differences about HH compliance among countries were found in the previous
chapters, therefore conducting studies to find out the actual situation in the context of each
country or hospital was needed. In Vietnam, there were few studies had been done on the
topic as mentioned in Literature Review Chapter; however none of them were recognized by
international journals. Therefore, description of HH compliance was very important to choose
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 41/121
4.2. Sampling and Setting
Setting
The study was conducted in the Vietduc teaching Hospital (the Vietduc Hospital) and
in the National Hospital of Pediatric (the Pediatric Hospital) in Hanoi, Vietnam. These
hospitals were the teaching hospitals supporting for Hanoi Medical University (HMU).
Therefore, they played the important role not only in taking care patient but also in training
the HCWs.
The Vietduc Hospital was the biggest surgical hospital in Vietnam. At that time, it had
more than 500 patient beds, 18 modern specialty surgical rooms, and the high quality human
resource. There were more than 800 staffs in this hospital, 500 of them are HCWs. It
responded in serving 60,000 in-patients each year, and trained many medical and nursing
undergraduate, graduate, and PhD students from Hanoi Medical University and HCWs from
other hospitals in Vietnam. Beside that, it also was the leading surgical research center, where
hundreds of studies had been conducted here.
The National Hospital of Pediatrics was the leading research center for pediatrics in
the country. It also collaborated with the pediatric department of Hanoi Medical University in
training medical students, specialists, sub-specialists, general practitioners, and MD-PhDs.
The Pediatric Hospital served about 40,000 in-patients and 350,000 out-patients per year.
Each year, the NHP also performed about 6000 major surgical operations. It had 22 clinical
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 42/121
The HCWs in the two hospitals’ selected wards were recruited when the study
inclusion criteria were reached. The participants were HCWs who were (1) doctors, nurses
and others HCWs including assistant nurses were working in the clinical departments; (2)
students of Hanoi Medical University (include undergraduate, graduate students) studying in
the hospital at that time. The exclusion criteria were HCWs who: (1) did not want to answer
the questionnaire; (2) did not include visiting experts, students attended short retraining
course, and guests; (3) came from the non-clinical departments (such as: administration dept,
pharmacy dept, hematology dept…).
The sample size was estimate by using the software ‘Sample size version 2.0”, which
was created by WHO. The below formula was designed for calculating sample size of the
survey study by using random sampling method.
)1()1()1(
22 / 1
2
22 / 1
PP z N d
N PP zn
−+−
−=
−
−
α
α
Where:
n: is sample size (The number of samples drawn in the study.)
N: is population size (Size of the population used in lot quality assurance sampling,
which are sampling techniques designed to ascertain whether batches of items meet specified
standards.)
P: is anticipated population proportion (Expected value of the proportion of
i di id l i l ti i i h t i ti )
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 43/121
The researcher recruited 230 HCWs from Vietduc Hospital and 270 HCWs from
Pediatric Hospital to answer the questionnaire. From each hospital, the researcher chose ten
wards randomly. On average, each ward was observed with 30 periods, which equaled 10
hours. All the HCWs worked in the wards at that time were asked to answer the
questionnaire.
4.3. Research Instruments
The researcher decided to apply both interview by questionnaire and observation.
The two instruments supported the both two together; the observation form could reduce the
limitation of the self-reported resulting on HH compliance, and the questionnaire helped
collecting the knowledge and attitudes of HCWs toward the behavior.
The questionnaire was made after reviewing literatures. Then, it was validated by
three experts. It included demographic characteristics (11 questions), knowledge (26
questions), attitudes (23 questions), skin irritation (4 questions) and HH compliance (1
question). In detail, knowledge questions were right/wrong questions; the total score
(Knowledge score) was calculated by the sum of number of correct answers. Attitudes of HH
in this study are the five-categories questions, the score of each question ranged from five to
one for the positive statements and ranged from one to five score for the negative statements.
The total score of all attitudes’ items (Attitude score) was calculated by the sum of the items’
score, it represented the score of attitude of HCWs toward HH. The theoretical score of the
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 44/121
4.4. Research Progress
4.4.1. Training the Observers
As mentioned at the literature review, there was a significant difference between
self-reported (or when the participants knew about observations) and observational
result on HH compliance. Therefore, observer training was very important and it was
taken care of very carefully. Seven observers were the freshman nurses, which had just graduated from Hanoi Medical University. The researcher collected them in the
observation training. The observers were trained about the purposes of the study, the
questionnaire, and the observational skills. The requirements after the training period
were mentioned before. The observers could explain well the questionnaire well to
participants about potential unclear points in questionnaire if it had. Then, they
practiced observing to improve observation skills. The meetings after each observation
period were arranged, thus, the observers could address their difficulties and shared
with others their experiences.
4.4.2. Pilot study
The pilot was conducted after the proposal passed. The aims of pilot study
were to re-check the questionnaire, and the observation procedures. This work had
been done for few days. The researcher did the pilot to find out how good the
questionnaire was (include translation problems); how good the observation form was;
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 45/121
The study proposal, questionnaire, and observation form were sent to the experts
to be validated. There are three experts from Meiho Institute of Technology and
School of Public Health, National Defense Medical Center, in Taiwan for asking their
opinions. After receiving back the study instruments, the researcher rewrote them
following the instruction. Finally, they were translated to Vietnamese, and were sent
to the Vietnamese expert for checking the translation validation.Reliability
The questionnaire contained demographic characteristics, knowledge questions,
attitude statements, as well as HH practice before. With the aim to check the internal
consistency, the Cronbach’s alpha was used. The technique just could deal with the
information of groups. The first group included the entire question which was used
to measure the knowledge score. This group contained the question number 12 to the
question number 37 (26 items). The second group contained 23 questions, there were
questions ranged from 38 to 40, from 42 to 53, and from 58 to 65.
The data of the pilot was inputted in the computer and analyzed about the reliability
level. The results of reliability test were showed in the table 3.1. As its showing, the
Cronbach’s alpha score of the group one was .731 and after adjustment the score based on
standardized items was higher (.809). This was acceptable when comparing it with the
common cut-off point (alpha, .70) in many other studies. It represented that the items among
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 46/121
Table 1: Reliability Statistics: Cronbach’s alpha
Groups
Cronbach's
Alpha
Cronbach's Alpha Based on
Standardized Items N of Items
1. Knowledge items .731 .809 262. Attitude items .701 .729 23
4.4.4. Data Collection
The researcher had asked for the permit from the administrative leaders of the two
hospitals. Each hospital had been received a recommendation from Hanoi Medical
University, which introduced about the researcher and the study, attached with the proposal,
as well as the instruments. Then, the researcher made appointment with hospital authorities to
explain about the study, and asked for the cooperation. This work was started right after the
observer training and pilot study, from June 30, 2006.
The study data collection started from July 16 , 2006 to September 5, 2006. The data
collection included two phases. The first phase was observation; and the second one was
interview. The two phrases were done in succession. The second phase had to wait for the
finishing of the observation phase to control the objective result. It helped solving the problem
showed in literature review: the compliance would be higher if the participants knew that they
were observing (Pittet et al., 2004).
Seven trained observers observed all the opportunities of actual performance of HH
during 20-minute observational periods. They had not to observe every period followed the
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 47/121
update the information, as well as help the observer if necessary.
The Vietduc Hospital was observed first. Ten chosen wards at this hospital were: the
Emergency and Out Patients Department, the Anesthesia and Reanimation Department, the
Neurosurgery Department, the Thoracic and Cardiovascular Surgical Department, the
Pediatric Surgical Department, the Traumatic Surgical and Orthopedics Department, the
Emergency Abdominal Surgical Department, the Septic Surgical Department, the UrologySurgical Department, the Liver and Biliary Surgical Department.
Following by the Pediatric Hospital, the observation was conducted at Pediatric
Hospital. Ten chosen clinical wards were: the Emergency Department, the Infectious
Department, the Neonatology Department, the Surgical Department, the Hematology
Department, the Respiratory Diseases Department, the Intensive Care Unit, the Oncology
Department, the Cardiology Department, the Department of Anesthesia and Resuscitation.
After finish the first phase -- observation, the questionnaire were used to ask the
participants’ about their demographic characteristics, knowledge, attitudes, and the self-report
on HH compliance. All the participants were explained about the aims of the study by the
open letter. Researcher asked to answer the anonymous questionnaires. Each questionnaire
usually needed 15 to 20 minutes to be finished. The questionnaires were returned when the
subjects finished it.
4.5. Data analysis
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 48/121
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 49/121
“strong disagree” was coded by five score. In addition, the participants did not answer
some attitudes, then those missing data were considered to replace by mean (three score).
After coding the data, the total of knowledge score and the total of attitude score were
calculated. The knowledge score, which ranged theoretically from zero to 26 scores, was
considered to divide it into four categories variable later on. The attitude score ranked
from 23 to 115, also was divided into four categories variable.
4.5.2. Analyses
The Statistical Package for Social Science software, version 11.5 was used to
analyze the data. Starting any section the descriptive analyses were conducted.
These including descriptive summary statistics such as frequencies, means, standard
deviation of demographic variables, HH knowledge score, or attitudes toward HH
compliance score. ANOVA test would be useful to compare the mean of HW
compliance among participants’ gender, education levels, work shifts, and workload,
experience, level of convenience when access HW toward HW compliance. Chi-
square test was used to analyze the associations between each demographic
characteristic and knowledge or attitude level variable. Correlative technique needed
to use to analyze correlation between participants’ knowledge and attitude of HW
toward HW compliance. Multivariate analyses (Loglinear model) had been used to test
the association among three variables or more.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 50/121
observation data would be bias. Therefore, the anonymous observation forms had used to
protect the individual’s information, while the leaders of the hospitals and wards had known
about this. The second phase, every HCWs was received the questionnaire with the opened
letter in the first page. They could refuse or accept to answer the questionnaire if they wanted
to. They were explained about the study purposes and how the researcher protected their
personal information, such as using the anonymous questionnaire and coding it. No one couldaccess the participants’ personal data, even the hospitals’ authorities.
4.7. Summary
The chapter presents the detail of the methods and material which applied for this study.
By describing the detail of the study design, setting, sampling, materials, procedure of data
collection, pilot testing, data analyses which has been applied in the study; the researcher could
explorer the picture of HH compliance among HCWs in the two hospitals. It supplies the scientific
guidelines for the study, thus guarantees for the close results.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 51/121
CHAPTER 5: RESULTS
This chapter described and summarized the statistical analyses used to evaluate the
research hypotheses. Those hypotheses were :(1) to explore demographic characteristics,
knowledge and attitude as well as compliance of HH; (2) to identify major factors that
influenced and affected HH compliance; (3) to explain the relationship among demographiccharacteristics, knowledge and attitude toward HH compliance.
Before the analyses, the data screening process had been applied to find out every
illogical data or other possible errors on the data sheet. Firstly, the researcher reported the
results of the analyze procedures applied on the questionnaire data. Secondly, the
observation data was dissected and presented. Finally, the other findings were mentioned.
5.1. Analyze Questionnaire Data
5.1.1. Descriptive Profile
Two hospitals which had been taken part in this study were Vietduc University
Hospital (Vietduc Hospital) and National Hospital of Pediatric (Pediatric Hospital).
In Vietduc Hospital, 230 questionnaires had been delivered, 270 other copies of the
questionnaire had been sent to HCWs in Pediatric Hospital. 358 of them (70.2%) had
been filled out, and 312 of them (62.4%) were good enough to be analyzed.
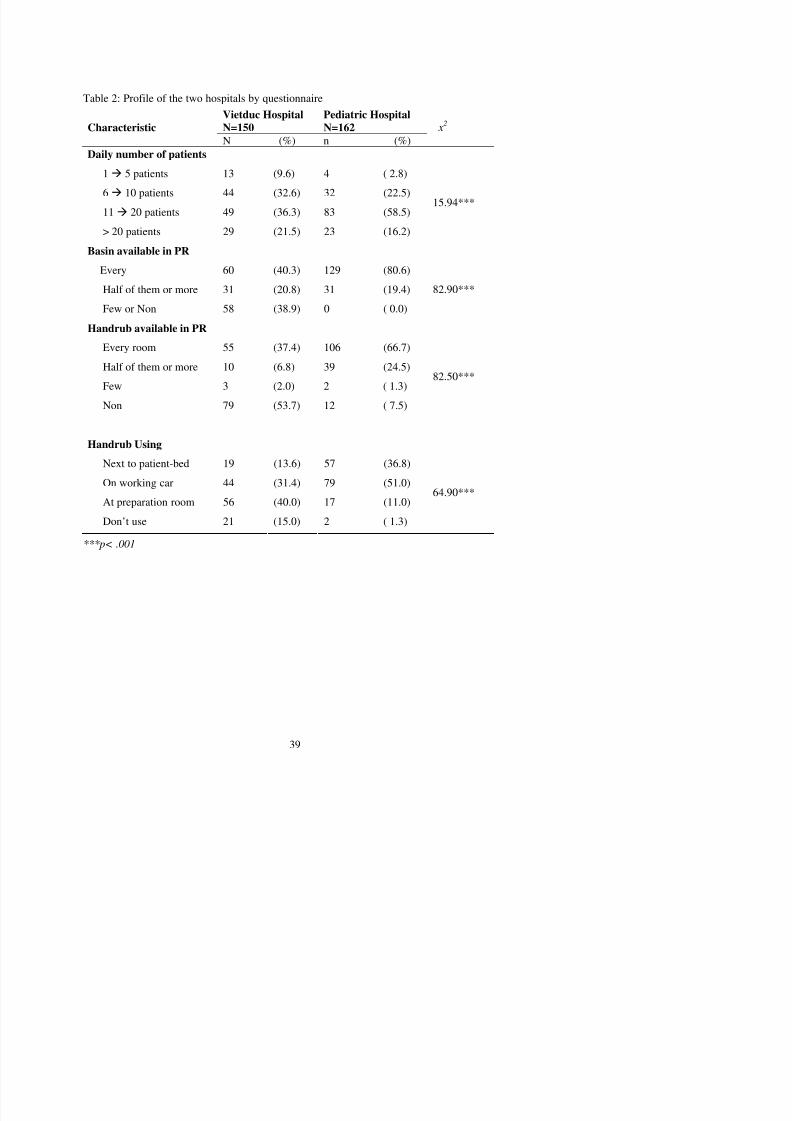
The profiles of the two hospitals were presented in Table 2. The “daily number
Th i t t d f HH ffi i t i th P di t i H it l th
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 52/121
The equipments supported for HH was sufficient in the Pediatric Hospital than
the Vietduc Hospital. Basins could be found in every patient room of the clinical ward
which was reported by 80.6% HCWs in the Pediatric Hospital, but it was only 40.3%
in the other’. In the meantime, 106 participants (66.7%) in the Pediatric Hospital
reported that handrub is available in every patient-room in their wards, but only 60
participants (40.3%) in the Vietduc Hospital had the same answer. Then, thesignificant differences were showed with the both two variables ( χ 2 = 82.9, p<.001
and χ 2 = 82.5, p < .001). The previous results linked logically to the number of
participants who usually used handrub next to patient-bed, this rate were 13.6% in the
Vietduc Hospital and 36.8% in the Pediatric Hospital. The rate of HCWs, although
people there did not use handrub, was also higher in the Vietduc Hospital (15% vs.
1.3%).
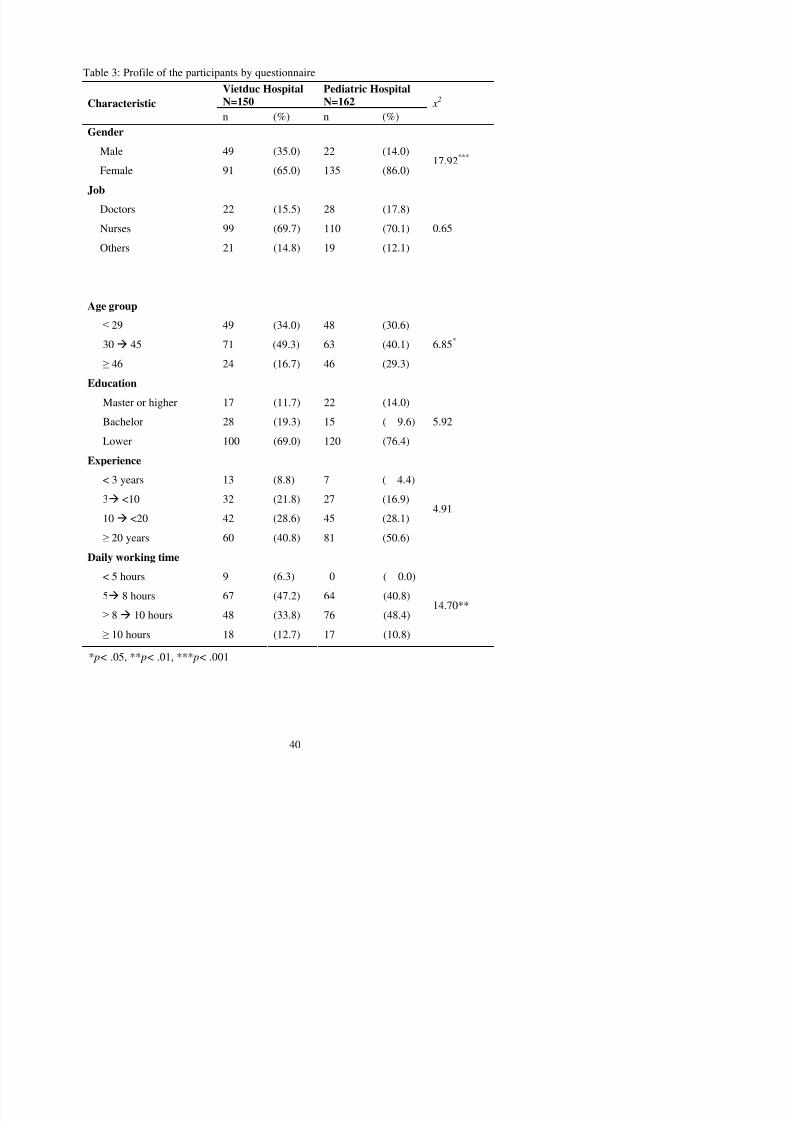
Table 3 showed the characteristics of HCWs in the two hospitals. In this table,
we recognized that the rate of male HCWs in the Vietduc Hospital was significantly
higher than it was in the Pediatric Hospital (35% vs. 14%, χ 2 = 17.92, p < .001).
However, the frequencies of the kinds of HCWs were not significantly different
between the two hospitals ( χ 2 = .65, p > .5). The HCWs in the Pediatric Hospital were
somehow older than in Vietduc Hospital, the Chi-square value was 6.85, p< .5.
Number of working experience years of participants and the education levels of
2
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 53/121
Table 2: Profile of the two hospitals by questionnaire
Vietduc HospitalN=150
Pediatric HospitalN=162Characteristic
N (%) n (%) x
2
Daily number of patients
1 5 patients 13 (9.6) 4 ( 2.8)
6 10 patients 44 (32.6) 32 (22.5)
11 20 patients 49 (36.3) 83 (58.5)
> 20 patients 29 (21.5) 23 (16.2)
15.94***
Basin available in PR
Every 60 (40.3) 129 (80.6)
Half of them or more 31 (20.8) 31 (19.4)
Few or Non 58 (38.9) 0 ( 0.0)
82.90***
Handrub available in PR
Every room 55 (37.4) 106 (66.7)
Half of them or more 10 (6.8) 39 (24.5)
Few 3 (2.0) 2 ( 1.3)
Non 79 (53.7) 12 ( 7.5)
82.50***
Handrub Using
Next to patient-bed 19 (13.6) 57 (36.8)
On working car 44 (31.4) 79 (51.0)
At preparation room 56 (40.0) 17 (11.0)Don’t use 21 (15.0) 2 ( 1.3)
64.90***
***p< .001
Table 3: Profile of the participants by questionnaire
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 54/121
Table 3: Profile of the participants by questionnaire
Vietduc HospitalN=150
Pediatric HospitalN=162Characteristic
n (%) n (%) x
2
Gender
Male 49 (35.0) 22 (14.0)
Female 91 (65.0) 135 (86.0)17.92***
Job
Doctors 22 (15.5) 28 (17.8)Nurses 99 (69.7) 110 (70.1)
Others 21 (14.8) 19 (12.1)
0.65
Age group≤ 29 49 (34.0) 48 (30.6)
30 45 71 (49.3) 63 (40.1)
≥ 46 24 (16.7) 46 (29.3)
6.85*
Education
Master or higher 17 (11.7) 22 (14.0)Bachelor 28 (19.3) 15 ( 9.6)
Lower 100 (69.0) 120 (76.4)
5.92
Experience
< 3 years 13 (8.8) 7 ( 4.4)
3 <10 32 (21.8) 27 (16.9)10 <20 42 (28.6) 45 (28.1)
≥ 20 years 60 (40.8) 81 (50.6)
4.91
D il ki ti
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 55/121
suggested us about the gaps on participants’ knowledge, and would be discussed later
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 56/121
suggested us about the gaps on participants knowledge, and would be discussed later
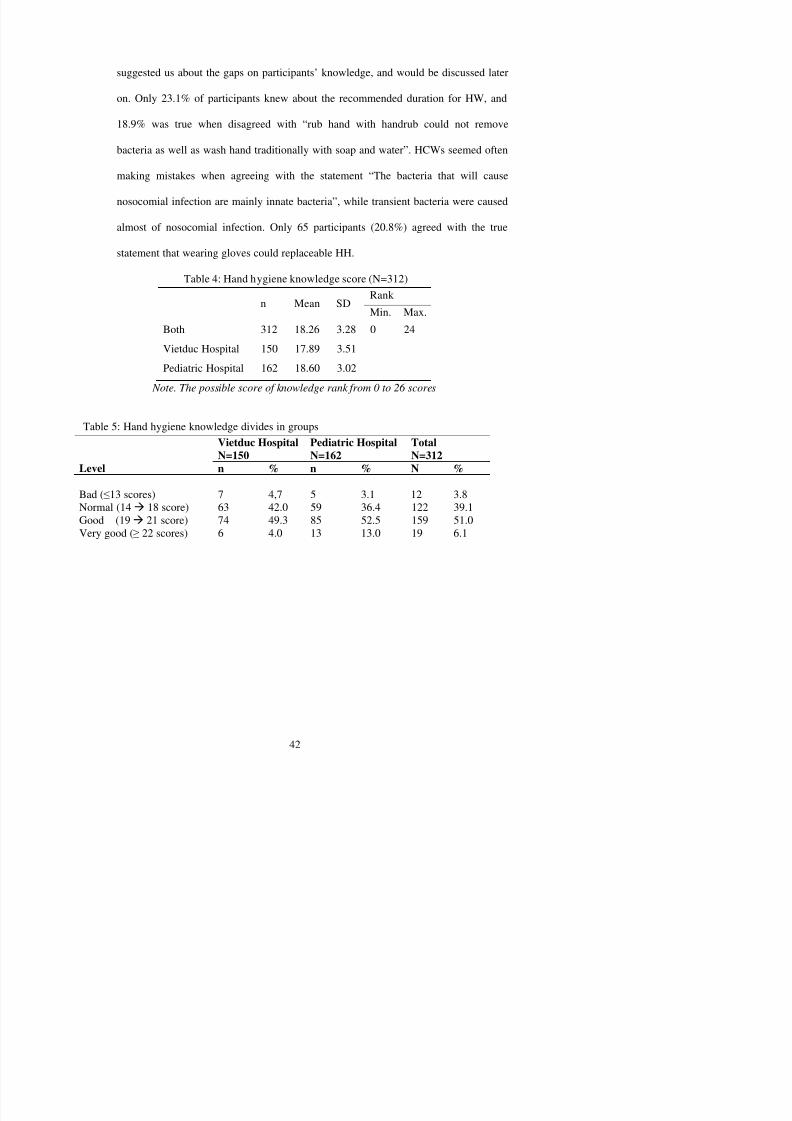
on. Only 23.1% of participants knew about the recommended duration for HW, and
18.9% was true when disagreed with “rub hand with handrub could not remove
bacteria as well as wash hand traditionally with soap and water”. HCWs seemed often
making mistakes when agreeing with the statement “The bacteria that will cause
nosocomial infection are mainly innate bacteria”, while transient bacteria were caused
almost of nosocomial infection. Only 65 participants (20.8%) agreed with the true
statement that wearing gloves could replaceable HH.
Table 4: Hand hygiene knowledge score (N=312)
Rank
n Mean SD Min. Max.
Both 312 18.26 3.28 0 24
Vietduc Hospital 150 17.89 3.51
Pediatric Hospital 162 18.60 3.02
Note. The possible score of knowledge rank from 0 to 26 scores
Table 5: Hand hygiene knowledge divides in groups
Vietduc HospitalN=150
Pediatric HospitalN=162
TotalN=312
Level n % n % N %
Bad (≤13 scores) 7 4,7 5 3.1 12 3.8Normal (14 18 score) 63 42.0 59 36.4 122 39.1Good (19 21 score) 74 49.3 85 52.5 159 51.0Very good (≥ 22 scores) 6 4.0 13 13.0 19 6.1
Table 6: Statement of each knowledge answer (N=312)

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 57/121
g ( )Correct
Ans.
Que
stion
No.
Statement of Knowledge
n (%)
12 The recommended duration for HW 72 (23.1)
13 Hands are the most important vehicles of transmission of infectious agents in
the hospital.299 (95.8)
14 Health-care instruments are the most important vehicle of transmission of
infectious agents in the hospital.243 (77.9)
15 HH is the most effective, simple and economic way to prevent nosocomial. 300 (96.2)
16 Soap and water are enough to remove up to 98% transient germs on our hands (#) 236 (75.6)
17 S. aureus is one of the transient germs on our hands. 155 (75.6)
18 S. aureus is a kind of innate bacterium on our hands.(#) 189 (60.6)
19 HCWs clean their hands to protect themselves, not the patients. (#) 253 (81.1)
20 It is not necessary to wash hands if you just touched the patients’ bodies.(#) 277 (88.8)
21 Hygiene hands immediately after caring for a patient help to protect HCWs. 273 (87.5)
22 HH need to be applied before/after using gloves. 285 (91.3)
23 If you have already worn gloves to care for a patient, taking off the gloves will
be enough; no need to clean your hands before caring other patients. (#)281 (90.1)
24 It is not necessary to clean your hands if you only touched the medical devices
that the patients have touched. (#)
290 (92.9)
25 Compare with rub hand with handrub, wash hand with soap and water is a
better way to remove the germs on our hands. (#)59 (18.9)
26 It is necessary to wash your hands if you touched the patients’ medical record. 223 (71.5)
27 The bacteria that will cause nosocomial infection are mainly innate bacteria. (#) 68 (21.8)
28 Long fingernails are associated with higher gram (-) bacterial hand contamination. 247 (79.2)
29 Fingernails shorter than fingertips are not associated with higher bacterial handcontamination. (#)
141 (45.2)
30 Wearing rings are associated with higher gram (-) bacterial hand contamination. 244 (78.2)
31 After washing your hands, dry your hands with the hand towels; throw them243 (77 9)
hands, but how you wash them.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 58/121
y
37 Washing hand might cause skin damages. 138 (44.2)
Note. # indicates an aliased negative statement.
5.1.2.2. Describe the HH attitude of HCWs
There were 23 statements had been used to ask about the attitudes of HCWs
toward HH. The score were given from one to five with the negative statements and
from five to one with the positive statements. The missing data was accepted while
calculating the frequencies of every statement in the table 7; however, those missing
data had been replaced by mean (three-score) while calculating the total attitude score
in the table 4.4a. This technique obtained justice among participants’ attitudes score; it
made every participant has the same number of answers. The theoretical score of
attitudes ranged from 23 to 115. Less than 69-score (≤ 3-score with each statement)
represented the “bad attitude” of HH and more than 92 (≥ 4-score with each statement)
represented the “very good attitude” of HH.
The table 4.4a showed that the real attitude score ranged from 62 to 99 scores.
The mean of attitudes score of whole participants was 81.82 (SD = 6.96). Therefore,
we could say that the participants had quite good attitude on HH. However, when
comparing two hospitals the researcher found that the attitudes of HCWs in the
Vietduc Hospital were better than they were in the Pediatric Hospital (82.65 vs. 81.06).
I dditi th t bl l h d th t th ttit d f th HCW i th P di t i
To understand clearly about the attitudes of HCWs on HH, the table 9 showed
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 59/121
the detail opinions of each statement. Starting with first three statements, we
recognized that, participants tended to remind their colleagues about HH much more
than they received back the reminder. There were 136 participants (50.2%) “Never” or
“Hardly ever” be reminded by their colleagues and almost of HCWs (97.8%) was not
reminded by patients. In opposite, 64.1% participants reported that they often or
usually remind their colleagues about clean hands, and only two patients (.7%) did the
same.
The next statement showed that most of HCWs had good attitudes in not
wearing rings (72.7% HCWs disagree with wearing any ring). Saying out about not
cleaning hands directly with the HCWs who forget to clean hands was found before
seem to be “a culture”. Beside that, 56.2% of HCWs reported that they do not have
any idea or disagreed to say it out with the colleagues’ superiors. These would be
considered when we wanted to do some intervention to improve HH compliance.
Another valuable finding when looking at the table was participants seemed not
to be convinced to use handrub because they worried about skin irritation. “Too busy”
and “HH products are not in a convenient location” were two reasons, which were
accepted by many participants when explaining the reasons for “not clean their hands”.
The finding showed the fact happened at these two hospitals, HCWs had overload
was helpful for administrators to make intervention plan, if they would want to
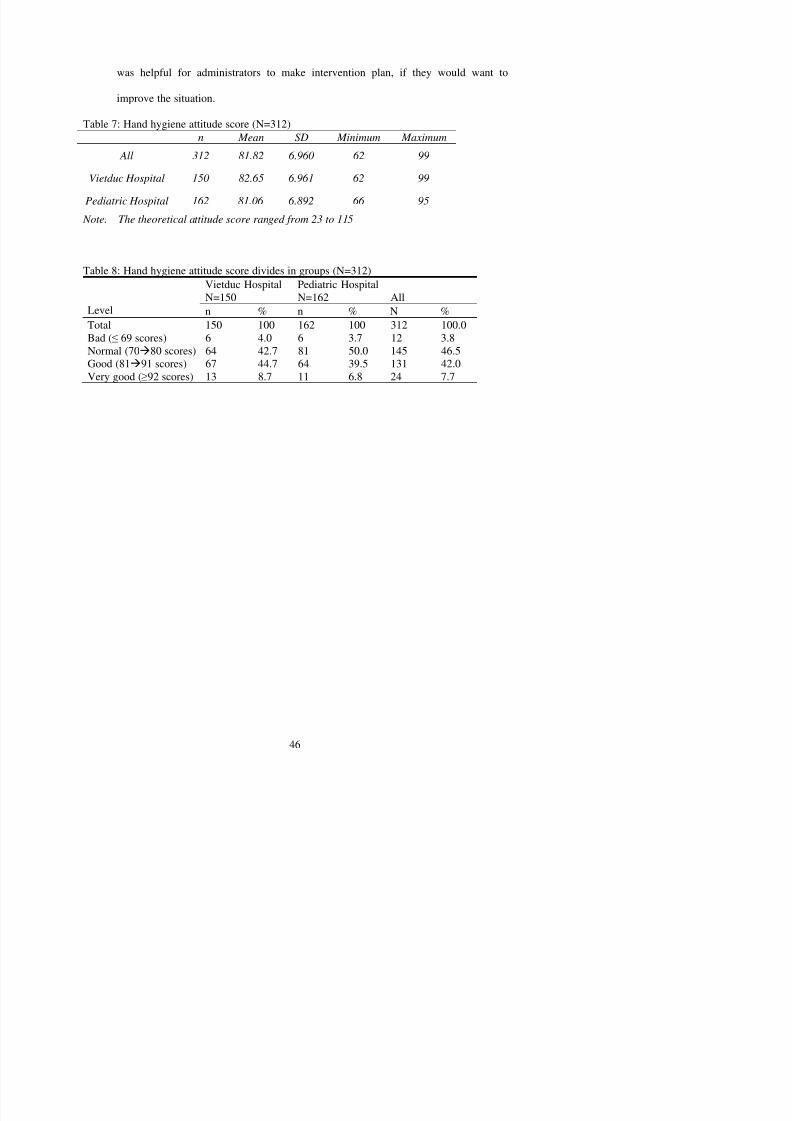
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 60/121
improve the situation.
Table 7: Hand hygiene attitude score (N=312)n Mean SD Minimum Maximum
All 312 81.82 6.960 62 99
Vietduc Hospital 150 82.65 6.961 62 99
Pediatric Hospital 162 81.06 6.892 66 95
Note. The theoretical attitude score ranged from 23 to 115
Table 8: Hand hygiene attitude score divides in groups (N=312)Vietduc HospitalN=150
Pediatric HospitalN=162 All
Level n % n % N %Total 150 100 162 100 312 100.0Bad (≤ 69 scores) 6 4.0 6 3.7 12 3.8Normal (7080 scores) 64 42.7 81 50.0 145 46.5Good (8191 scores) 67 44.7 64 39.5 131 42.0Very good (≥92 scores) 13 8.7 11 6.8 24 7.7
T bl 9 St t t f h ttit d (N 312)
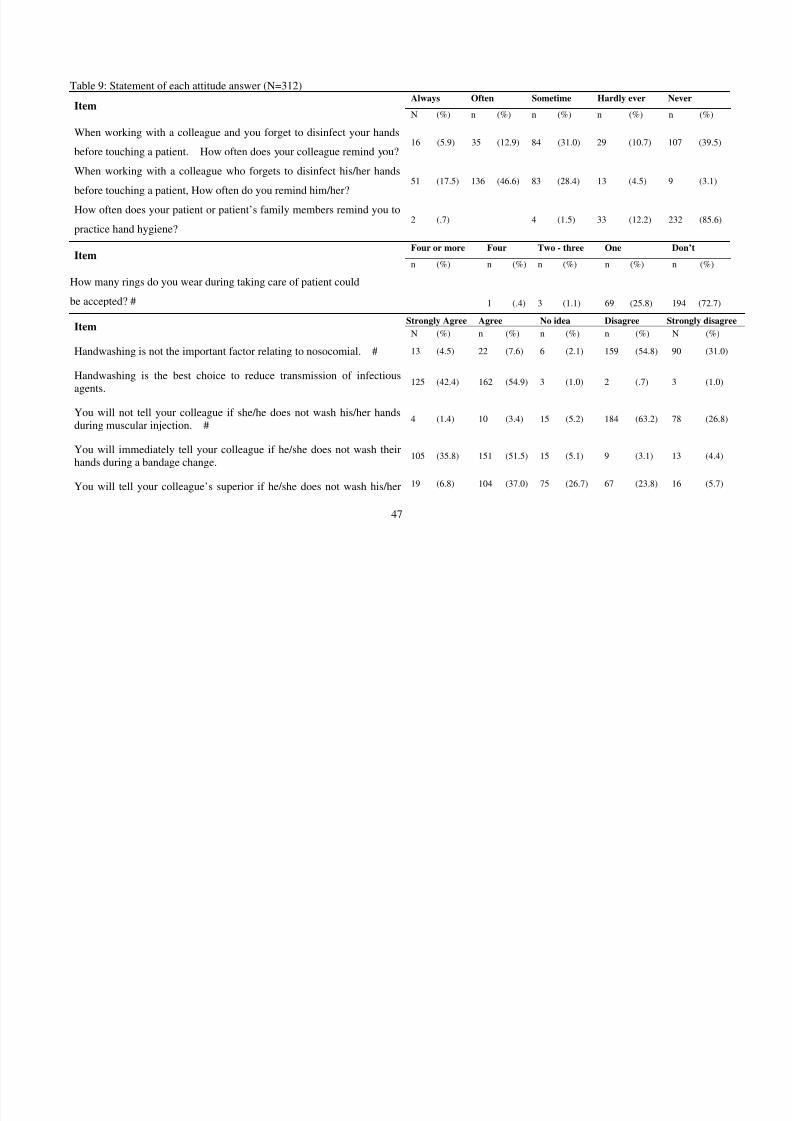
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 61/121
47
Table 9: Statement of each attitude answer (N=312)Always Often Sometime Hardly ever Never
Item N (%) n (%) n (%) n (%) n (%)
When working with a colleague and you forget to disinfect your hands
before touching a patient. How often does your colleague remind you?16 (5.9) 35 (12.9) 84 (31.0) 29 (10.7) 107 (39.5)
When working with a colleague who forgets to disinfect his/her hands
before touching a patient, How often do you remind him/her?51 (17.5) 136 (46.6) 83 (28.4) 13 (4.5) 9 (3.1)
How often does your patient or patient’s family members remind you topractice hand hygiene?
2 (.7) 4 (1.5) 33 (12.2) 232 (85.6)
Four or more Four Two - three One Don’tItem
n (%) n (%) n (%) n (%) n (%)
How many rings do you wear during taking care of patient could
be accepted? #
1 (.4) 3 (1.1) 69 (25.8) 194 (72.7)Strongly Agree Agree No idea Disagree Strongly disagree
Item N (%) n (%) n (%) n (%) N (%)
Handwashing is not the important factor relating to nosocomial. # 13 (4.5) 22 (7.6) 6 (2.1) 159 (54.8) 90 (31.0)
Handwashing is the best choice to reduce transmission of infectiousagents.
125 (42.4) 162 (54.9) 3 (1.0) 2 (.7) 3 (1.0)
You will not tell your colleague if she/he does not wash his/her handsduring muscular injection. #
4 (1.4) 10 (3.4) 15 (5.2) 184 (63.2) 78 (26.8)
You will immediately tell your colleague if he/she does not wash theirhands during a bandage change.
105 (35.8) 151 (51.5) 15 (5.1) 9 (3.1) 13 (4.4)
You will tell your colleague’s superior if he/she does not wash his/her 19 (6.8) 104 (37.0) 75 (26.7) 67 (23.8) 16 (5.7)
hands d ring a intra eno s injection
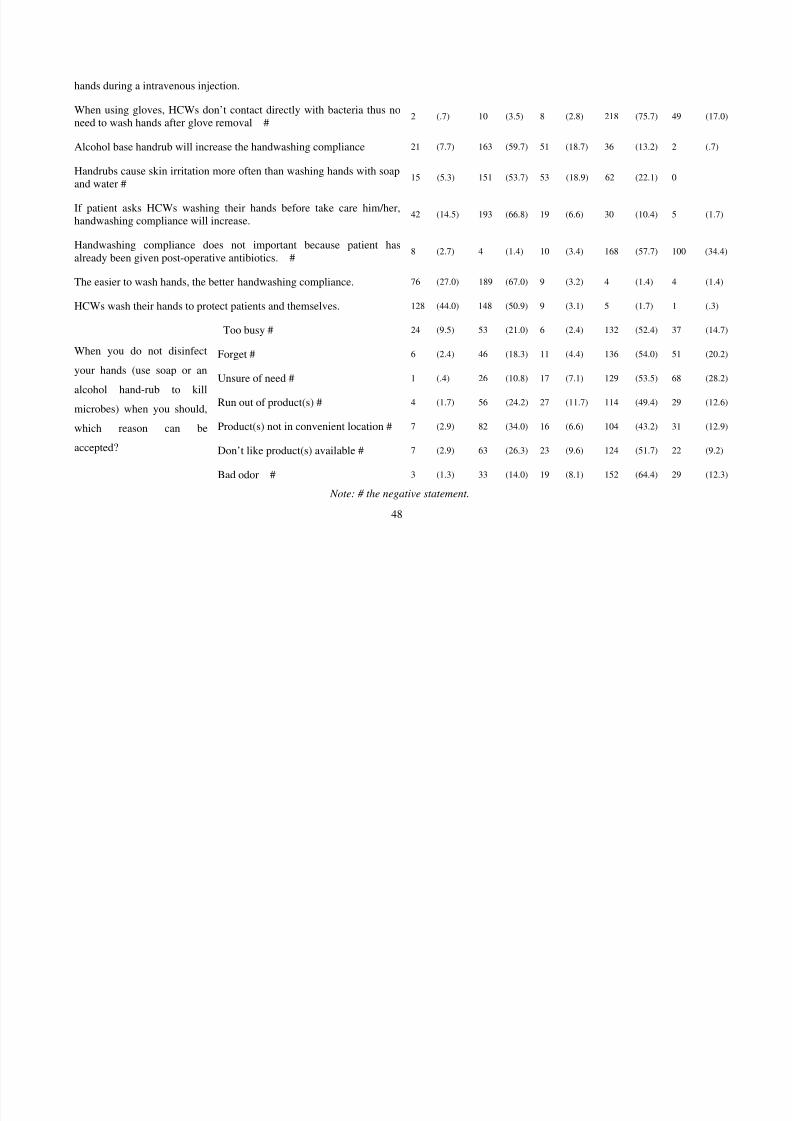
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 62/121
48
hands during a intravenous injection.
When using gloves, HCWs don’t contact directly with bacteria thus noneed to wash hands after glove removal # 2 (.7) 10 (3.5) 8 (2.8) 218 (75.7) 49 (17.0)
Alcohol base handrub will increase the handwashing compliance 21 (7.7) 163 (59.7) 51 (18.7) 36 (13.2) 2 (.7)
Handrubs cause skin irritation more often than washing hands with soapand water #
15 (5.3) 151 (53.7) 53 (18.9) 62 (22.1) 0
If patient asks HCWs washing their hands before take care him/her,handwashing compliance will increase.42 (14.5) 193 (66.8) 19 (6.6) 30 (10.4) 5 (1.7)
Handwashing compliance does not important because patient hasalready been given post-operative antibiotics. #
8 (2.7) 4 (1.4) 10 (3.4) 168 (57.7) 100 (34.4)
The easier to wash hands, the better handwashing compliance. 76 (27.0) 189 (67.0) 9 (3.2) 4 (1.4) 4 (1.4)
HCWs wash their hands to protect patients and themselves. 128 (44.0) 148 (50.9) 9 (3.1) 5 (1.7) 1 (.3)
Too busy # 24 (9.5) 53 (21.0) 6 (2.4) 132 (52.4) 37 (14.7)
Forget # 6 (2.4) 46 (18.3) 11 (4.4) 136 (54.0) 51 (20.2)
Unsure of need # 1 (.4) 26 (10.8) 17 (7.1) 129 (53.5) 68 (28.2)
Run out of product(s) # 4 (1.7) 56 (24.2) 27 (11.7) 114 (49.4) 29 (12.6)
Product(s) not in convenient location # 7 (2.9) 82 (34.0) 16 (6.6) 104 (43.2) 31 (12.9)
Don’t like product(s) available # 7 (2.9) 63 (26.3) 23 (9.6) 124 (51.7) 22 (9.2)
When you do not disinfect
your hands (use soap or an
alcohol hand-rub to kill
microbes) when you should,
which reason can be
accepted?
Bad odor # 3 (1.3) 33 (14.0) 19 (8.1) 152 (64.4) 29 (12.3)
Note: # the negative statement.
5.1.2.3. Relationship of Demographic Characteristic with Knowledge and Attitude

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 63/121
This part aimed to present the relationship between HH knowledge and
demographic characteristics; as well as between attitudes toward HH and demographic
characteristics. ANOVA test was used as the statistical tool. The researcher wanted to
compare the mean of knowledge score and attitude score among categories of each
demographic variable. The results were showed in the two tables 10 and 11.
The table 10 began with the differences between two hospitals of knowledge
score and attitudes score. It showed that the difference of knowledge score between
the two hospitals was not significant (F =3.77, p = .53). Nevertheless, the knowledge
score of HCWs in the Pediatric Hospital was higher than in the Vietduc Hospital. In
addition, when comparing the attitude score the researcher found a significant
difference (F =4.15, p = .043). The mean of attitude score of participants in Vietduc
Hospital was higher than in Pediatric Hospital (82.65 vs. 81.89).
Next, the effect of the number of “patients each HCW have to care everyday”
played the important role in changing attitude score, the significant differences were
found among means of groups’ attitude score (F = 5.16, p = .002). The attitude of
the group of HCWs who had to serve 11-20 patients everyday was worse than the
group of participants who did not have to serve that many.
The equipments for HH (basins, handrubs) in each hospital did not affect to
room. Thus, the regular contacts with HH equipment helped HCWs to improve their
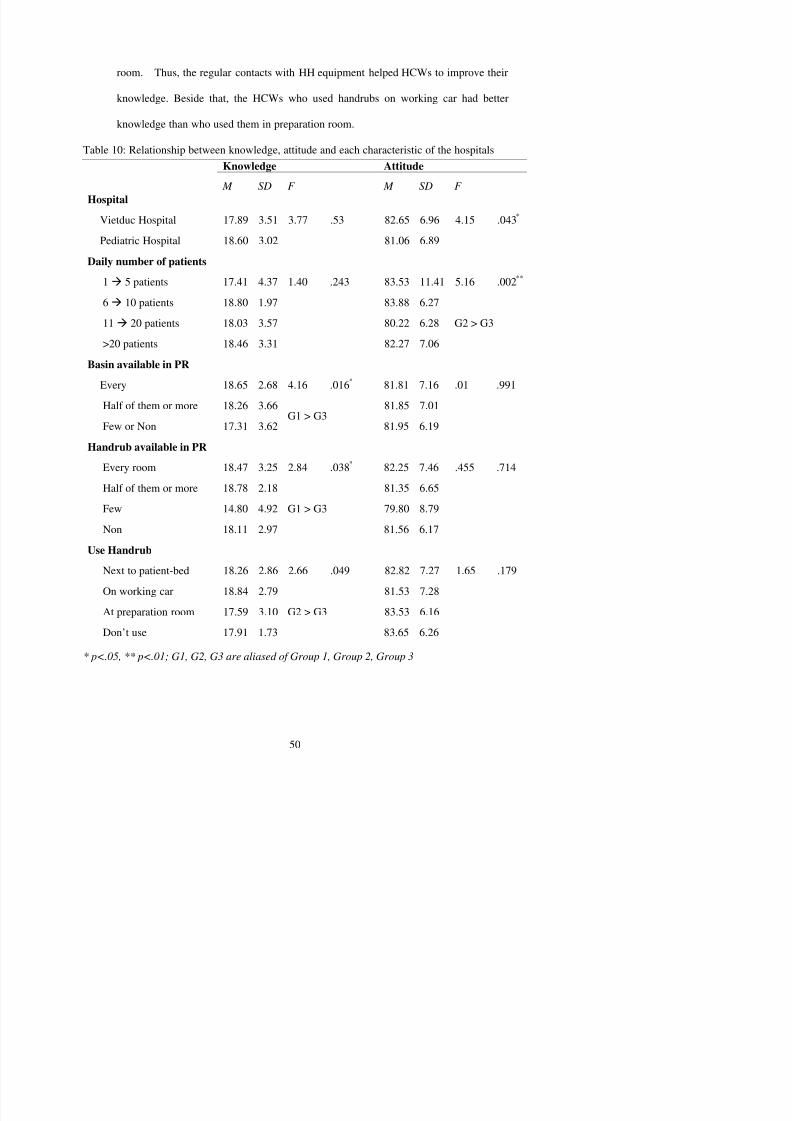
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 64/121
knowledge. Beside that, the HCWs who used handrubs on working car had better
knowledge than who used them in preparation room.
Table 10: Relationship between knowledge, attitude and each characteristic of the hospitals
Knowledge Attitude
M SD F M SD F
Hospital
Vietduc Hospital 17.89 3.51 3.77 .53 82.65 6.96 4.15 .043*
Pediatric Hospital 18.60 3.02 81.06 6.89
Daily number of patients
1 5 patients 17.41 4.37 1.40 .243 83.53 11.41 5.16 .002**
6
10 patients 18.80 1.97 83.88 6.2711 20 patients 18.03 3.57 80.22 6.28
>20 patients 18.46 3.31 82.27 7.06
G2 > G3
Basin available in PR
Every 18.65 2.68 4.16 .016* 81.81 7.16 .01 .991
Half of them or more 18.26 3.66 81.85 7.01Few or Non 17.31 3.62
G1 > G381.95 6.19
Handrub available in PR
Every room 18.47 3.25 2.84 .038* 82.25 7.46 .455 .714
Half of them or more 18.78 2.18 81.35 6.65
Few 14.80 4.92 79.80 8.79
Non 18.11 2.97
G1 > G3
81.56 6.17
Use Handrub
Table 11 focused on the relationship of the characteristics of HCWs between
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 65/121
knowledge score and attitude score. It started with comparing the mean of knowledge
score between two groups of gender. Even the knowledge score between the two
groups were similar ( M =18.15, SD=2.90 vs. M =18.21, SD=3.47), though the male
HCWs had better attitude than female colleagues did. Among the age groups, the
researcher found a significant difference of knowledge score (F = 4.4, p = .013), but he
did not find the similar difference of attitude score. In detail, the knowledge score of
the oldest groups was higher than the youngest group ( M = 18.97, SD = 2.72 vs.
M =17.48, SD= 4.12). The similar score of knowledge and attitude among doctors,
nurses and others had been found. It could be explained that, the job categories did not
affect to neither knowledge nor attitudes. This issue was going to explore more later
on. Education levels did not play role in changing the knowledge score (F = .11, p
= .89) and attitude score (F =1.59, p = .21). The similar finding was found with
“number years of clinical experience”; the data showed that there was no difference of
knowledge score (F = 2.17, p= .42) and attitude score (F = .34, p = .80) among the four
groups. Last, the researcher found that the mean of knowledge score as well as the
mean of attitude score among groups, which had different “daily working time”. It
meant that the pressing of daily working time on HCWs did not affect to their
knowledge and attitudes.
Table 11: Relationship between knowledge, attitude and each characteristic of the participants (N=312)
Knowledge Attitude
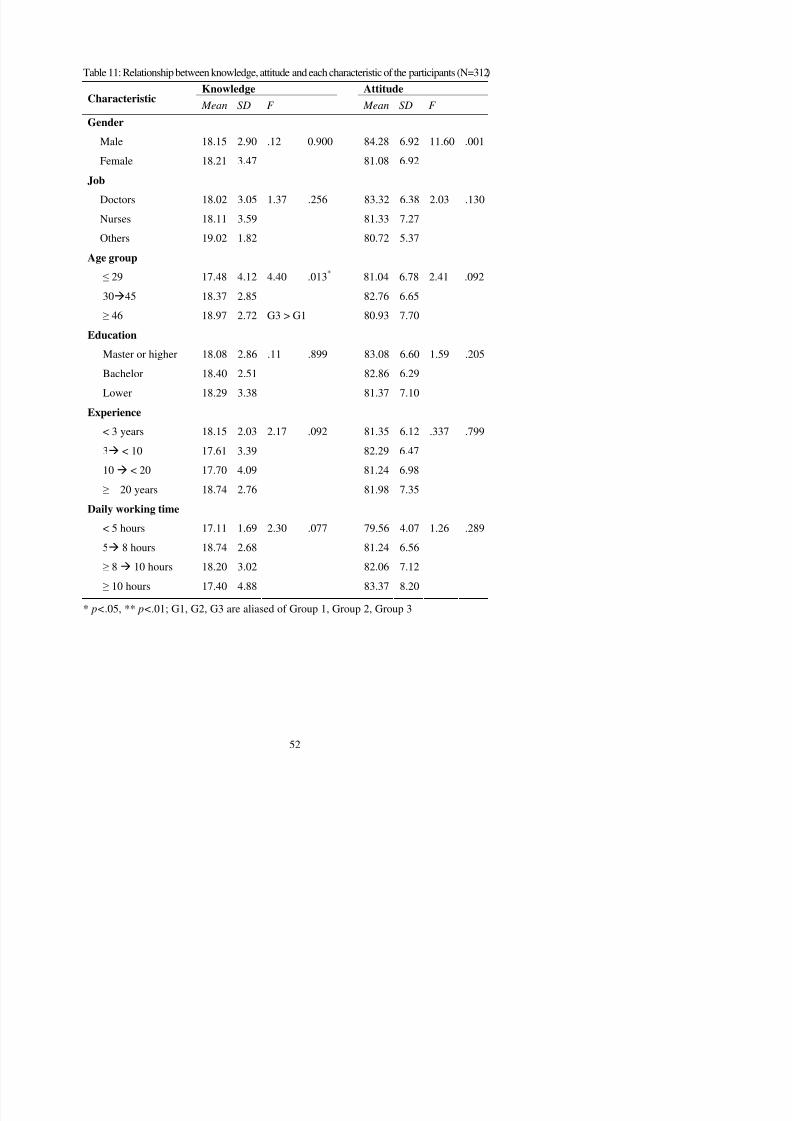
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 66/121
Knowledge AttitudeCharacteristic
Mean SD F Mean SD F
Gender
Male 18.15 2.90 .12 0.900 84.28 6.92 11.60 .001
Female 18.21 3.47 81.08 6.92
Job
Doctors 18.02 3.05 1.37 .256 83.32 6.38 2.03 .130
Nurses 18.11 3.59 81.33 7.27
Others 19.02 1.82 80.72 5.37
Age group
≤ 29 17.48 4.12 4.40 .013* 81.04 6.78 2.41 .092
3045 18.37 2.85 82.76 6.65
≥ 46 18.97 2.72 G3 > G1 80.93 7.70
Education
Master or higher 18.08 2.86 .11 .899 83.08 6.60 1.59 .205
Bachelor 18.40 2.51 82.86 6.29
Lower 18.29 3.38 81.37 7.10
Experience
< 3 years 18.15 2.03 2.17 .092 81.35 6.12 .337 .799
3 < 10 17.61 3.39 82.29 6.47
10 < 20 17.70 4.09 81.24 6.98
≥ 20 years 18.74 2.76 81.98 7.35
Daily working time
< 5 hours 17.11 1.69 2.30 .077 79.56 4.07 1.26 .289
5 8 hours 18.74 2.68 81.24 6.56
5.1.2.4. The Correlation between Knowledge and Attitude
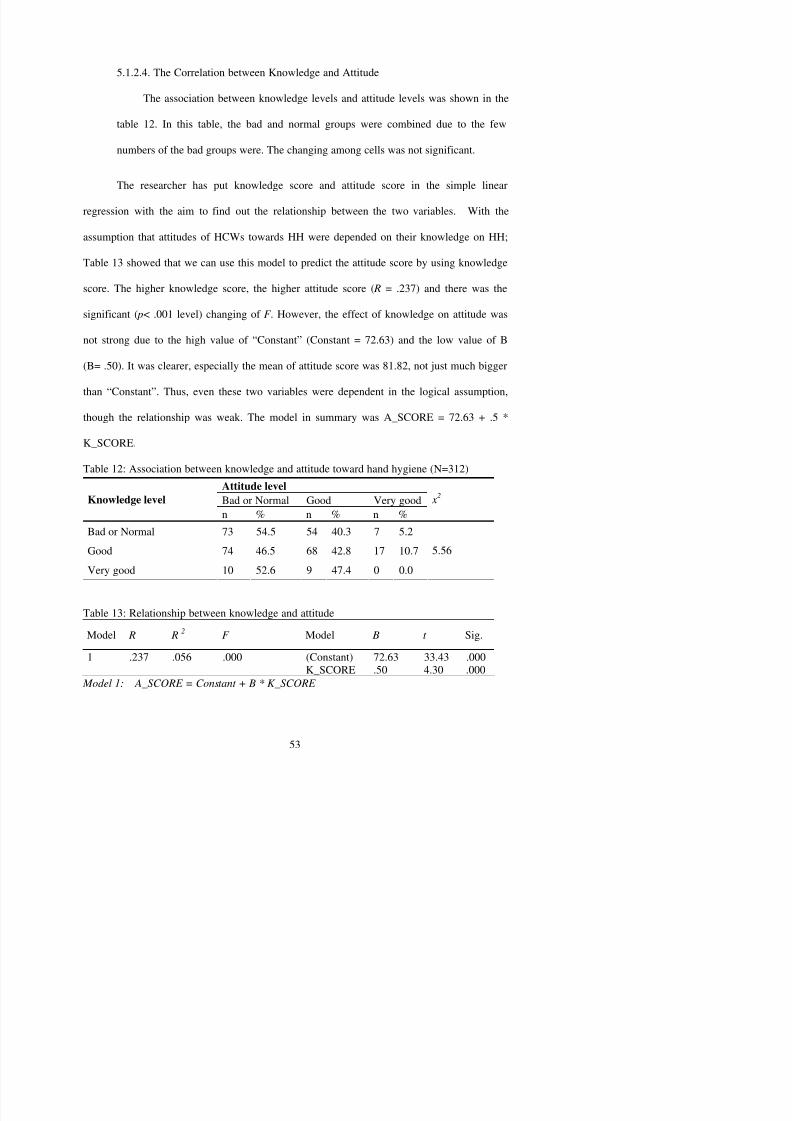
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 67/121
The association between knowledge levels and attitude levels was shown in the
table 12. In this table, the bad and normal groups were combined due to the few
numbers of the bad groups were. The changing among cells was not significant.
The researcher has put knowledge score and attitude score in the simple linear
regression with the aim to find out the relationship between the two variables. With the
assumption that attitudes of HCWs towards HH were depended on their knowledge on HH;
Table 13 showed that we can use this model to predict the attitude score by using knowledge
score. The higher knowledge score, the higher attitude score ( R = .237) and there was the
significant ( p< .001 level) changing of F . However, the effect of knowledge on attitude was
not strong due to the high value of “Constant” (Constant = 72.63) and the low value of B
(B= .50). It was clearer, especially the mean of attitude score was 81.82, not just much bigger
than “Constant”. Thus, even these two variables were dependent in the logical assumption,
though the relationship was weak. The model in summary was A_SCORE = 72.63 + .5 *
K_SCORE.
Table 12: Association between knowledge and attitude toward hand hygiene (N=312)
Attitude level
Bad or Normal Good Very goodKnowledge level n % n % n % x
2
Bad or Normal 73 54.5 54 40.3 7 5.2
Good 74 46.5 68 42.8 17 10.7 5.56
5.1.3. Hand Hygiene Compliance by Self-report
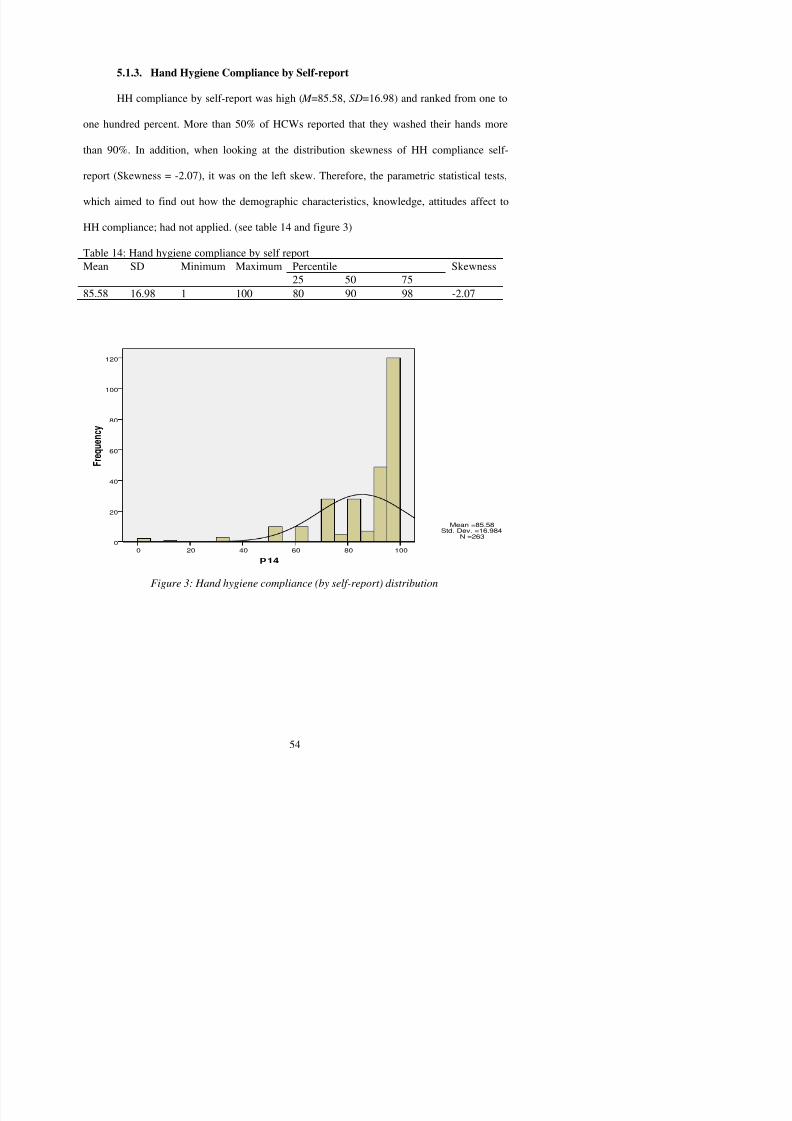
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 68/121
HH compliance by self-report was high ( M =85.58, SD=16.98) and ranked from one to
one hundred percent. More than 50% of HCWs reported that they washed their hands more
than 90%. In addition, when looking at the distribution skewness of HH compliance self-
report (Skewness = -2.07), it was on the left skew. Therefore, the parametric statistical tests,
which aimed to find out how the demographic characteristics, knowledge, attitudes affect to
HH compliance; had not applied. (see table 14 and figure 3)
Table 14: Hand hygiene compliance by self reportPercentileMean SD Minimum Maximum25 50 75
Skewness
85.58 16.98 1 100 80 90 98 -2.07
100806040200
F r e q u e n c y
120
100
80
60
40
20
0
Mean =85.58
Std. Dev. =16.984
N =263
5.2. Analyze the observation data

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 69/121
5.2.1. Describe Profiles
There are 4862 opportunities had been observed among 587 observation
periods (each period lasted after 20 minutes), in other words, the study observation
time was nearly 200 hours. The time of observation at Vietduc Hospital (334 periods
or more than 110 hours) was longer than it was at Pediatric Hospital (253 periods or
nearly 85 hours). (see table 15) Along with that, the number of observation
opportunities in the Vietduc Hospital (N=2641), was bigger than it was in the Pediatric
Hospital (N=2221). Ten wards in each hospital were observed on both weekends and
weekdays, nevertheless the table showed that the number of opportunities occurredduring weekend (N=670) was less than it was during weekdays (N= 4192). There were
2687 opportunities (55.3%) during 295 morning periods (50%), 1802 opportunities
(37.1%) during 238 afternoon periods (40.5%), and 373 opportunities (7.7%) during
54 periods (9.2%). Through that comparison, we recognized that HCWs had to work
harder in morning (at average of 9.11 opportunities/period) than in other day shifts
(afternoon: 7.57; and evening: 6.91).
The distance from the nearest workable basin to the patient room had been
divided into three subgroups. Mostly, the distance was less than or equaled four meters
(71.3%), another 18.7% of opportunities, it ranged from five to nine meters, 10% of
692 doctors (14.2%), 3253 nurses (66.9%) and 917 other HCWs (18.9%) needed to
l th i h d i t t l t iti H th h d j t l d th i h d i
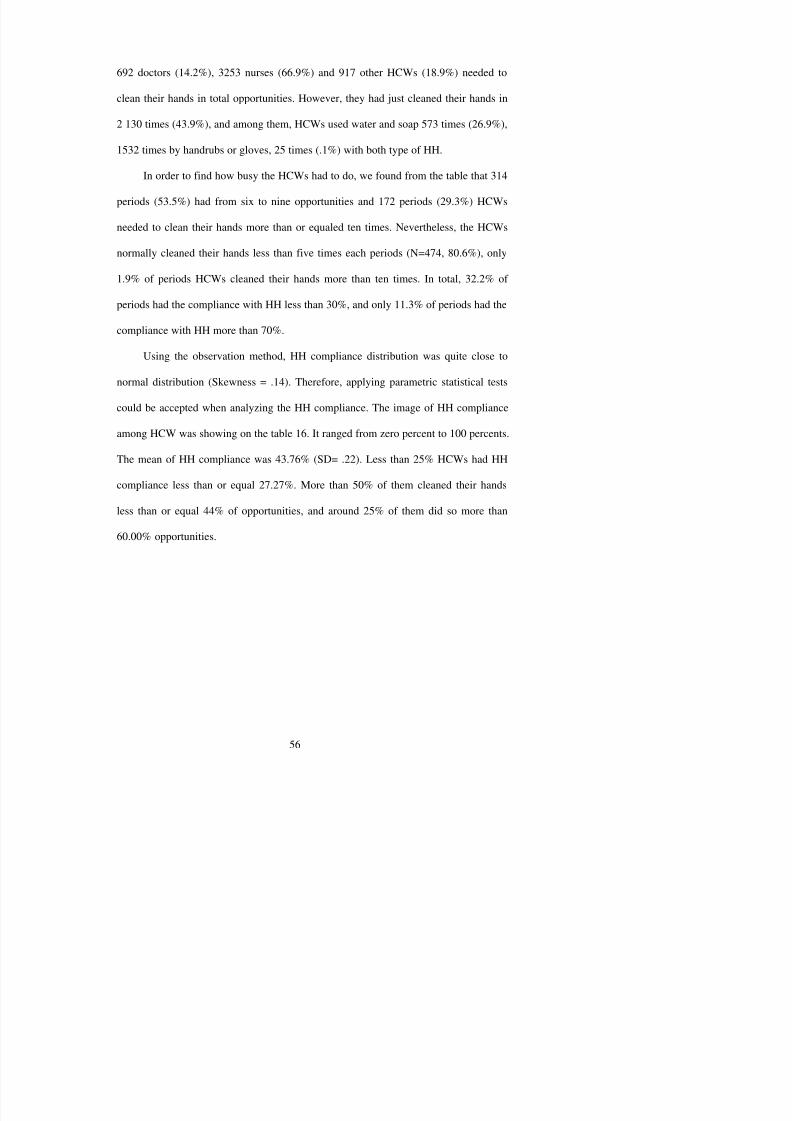
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 70/121
clean their hands in total opportunities. However, they had just cleaned their hands in
2 130 times (43.9%), and among them, HCWs used water and soap 573 times (26.9%),
1532 times by handrubs or gloves, 25 times (.1%) with both type of HH.
In order to find how busy the HCWs had to do, we found from the table that 314
periods (53.5%) had from six to nine opportunities and 172 periods (29.3%) HCWs
needed to clean their hands more than or equaled ten times. Nevertheless, the HCWs
normally cleaned their hands less than five times each periods (N=474, 80.6%), only
1.9% of periods HCWs cleaned their hands more than ten times. In total, 32.2% of
periods had the compliance with HH less than 30%, and only 11.3% of periods had thecompliance with HH more than 70%.
Using the observation method, HH compliance distribution was quite close to
normal distribution (Skewness = .14). Therefore, applying parametric statistical tests
could be accepted when analyzing the HH compliance. The image of HH compliance
among HCW was showing on the table 16. It ranged from zero percent to 100 percents.
The mean of HH compliance was 43.76% (SD= .22). Less than 25% HCWs had HH
compliance less than or equal 27.27%. More than 50% of them cleaned their hands
less than or equal 44% of opportunities, and around 25% of them did so more than
60.00% opportunities.
Table 15: Frequencies of the observation data (N=4862)
It (%) It (%)
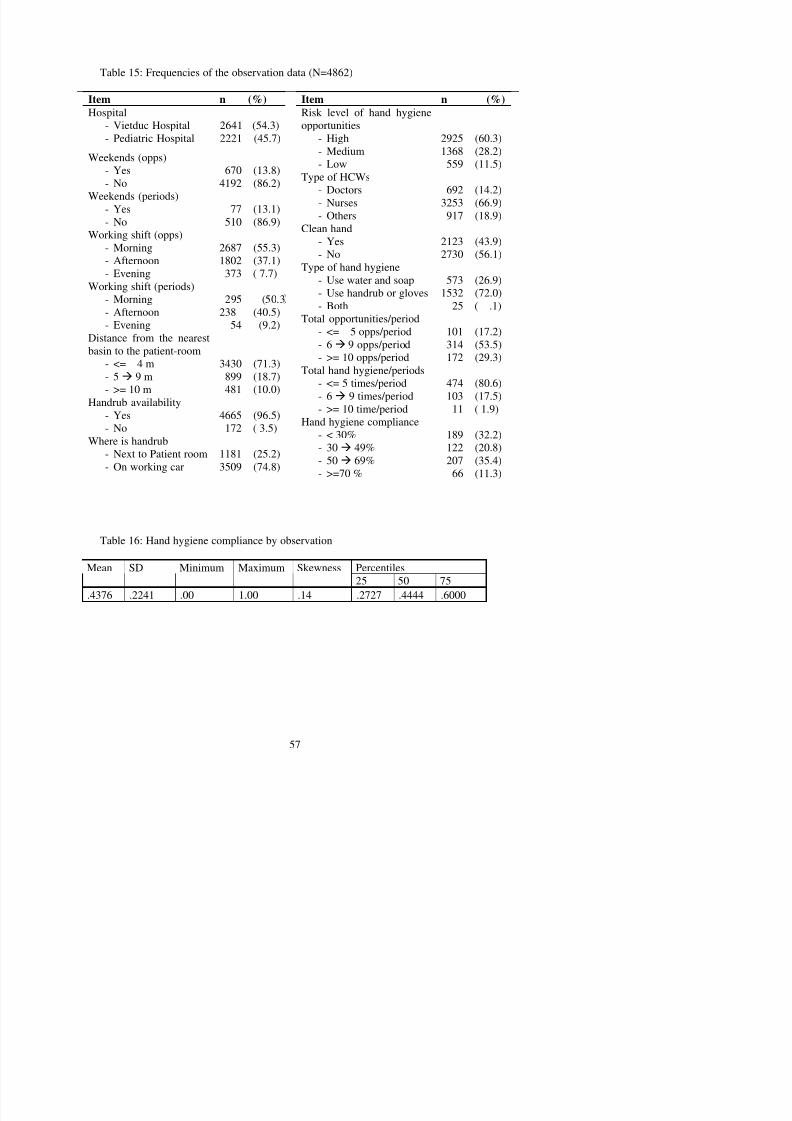
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 71/121
Item n (%)
Hospital- Vietduc Hospital- Pediatric Hospital
2641 (54.3)2221 (45.7)
Weekends (opps)- Yes- No
670 (13.8)4192 (86.2)
Weekends (periods)
- Yes- No 77 (13.1)510 (86.9)Working shift (opps)
- Morning- Afternoon- Evening
2687 (55.3)1802 (37.1)373 ( 7.7)
Working shift (periods)- Morning
- Afternoon- Evening
295 (50.3
238 (40.5)54 (9.2)
Distance from the nearestbasin to the patient-room
- <= 4 m- 5 9 m- >= 10 m
3430 (71.3)899 (18.7)481 (10.0)
Handrub availability- Yes- No
4665 (96.5)172 ( 3.5)
Where is handrub- Next to Patient room- On working car
1181 (25.2)3509 (74.8)
Item n (%)
Risk level of hand hygieneopportunities- High- Medium- Low
2925 (60.3)1368 (28.2)559 (11.5)
Type of HCWs- Doctors- Nurses
- Others
692 (14.2)3253 (66.9)
917 (18.9)Clean hand
- Yes- No
2123 (43.9)2730 (56.1)
Type of hand hygiene- Use water and soap- Use handrub or gloves
-
Both
573 (26.9)1532 (72.0)
25 ( .1)Total opportunities/period- <= 5 opps/period- 6 9 opps/period- >= 10 opps/period
101 (17.2)314 (53.5)172 (29.3)
Total hand hygiene/periods- <= 5 times/period- 6 9 times/period
- >= 10 time/period
474 (80.6)103 (17.5)
11 ( 1.9)Hand hygiene compliance
- < 30%- 30 49%- 50 69%- >=70 %
189 (32.2)122 (20.8)207 (35.4)
66 (11.3)
Table 16: Hand hygiene compliance by observation
5.2.2. Relationship of Hand Hygiene Compliance and Demographic characteristics
5 2 2 1 ANOVA tests
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 72/121
5.2.2.1. ANOVA tests
The ANOVA test had been applied to find out the relationship between HH and
each demographic separately, and putted in the table 17. The valid cases had been
calculate equal with the number of periods (N=587). The reason was the HH
compliance was only available with each periods but not with each opportunities. To
analyze the relationship in context of individual opportunities, the researcher was
going to present in the later section.
The difference of HH compliance mean between the two hospitals were
significant at p< .001 ( M =.3754; SD=.2172 in the Vietduc Hospital vs. M =.5196; SD = .2064 in the other). On weekdays, HCWs tend to clean their hands (44.33% of
needed) less often than on weekends (46.61% of needed). However, the difference
of HH compliance among shifts occurred on weekends and occurred on weekdays
were not significant (F =1.43, p = .231). The similar result was found with another
time variable, working shifts. The best compliance was found in evening shifts
(47.46%) and the lowest compliance was found in afternoon shifts (42.79%).
Moving to the next factors related to hospital equipments, they were “the
distance from the nearest basin to the patient room”, and “handrub availability”. The
result showed that “the distance from the nearest basin to the patient room” was very
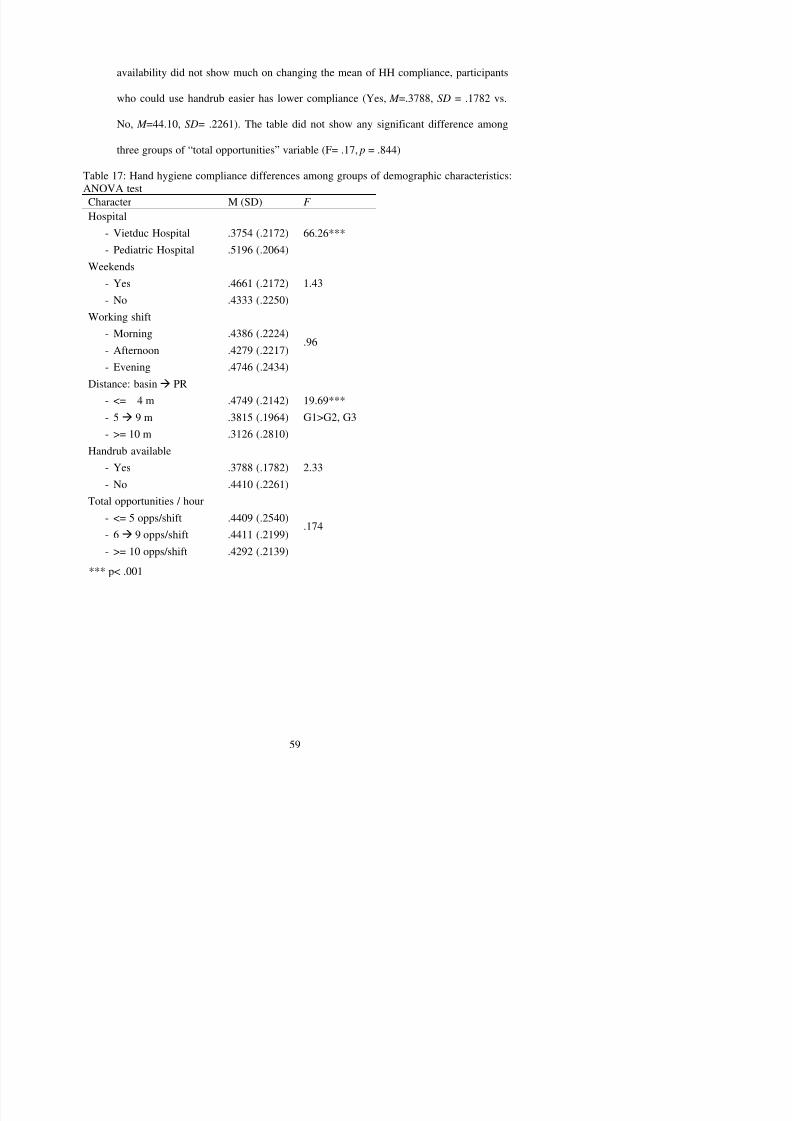
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 73/121
5.2.2.2. Chi-Square test
Chi-square tests had been used to find out the detail distribution of HH base on
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 74/121
Chi square tests had been used to find out the detail distribution of HH base on
the groups of demographic characteristics. During this section, the analysis had been
applied among individual participants. Therefore, this part could give the researcher
more detail information of the data. It was presented in the table 18.
The rate of HCWs in the Pediatric Hospital cleaned their hands (N= 1158,
52.14%) more frequently than their colleagues did in Vietduc Hospital (N=974, 36.88).
The difference of HH decision of HCWs in the two hospitals was significant when
Chi-square value was 114.08 and significant at p< .001. The OR (Vietduc/pediatric)
equal .54 emphasized strongly that there was a big difference in HH compliancebetween this two hospitals.
The OR (weekends/weekdays) equal 1.23 meant that HH compliance during the
weekends tended to be higher than during the weekdays. In addition, the exact rate of
seeing HH among HCWs during the weekends (48.21%) was higher than during the
weekdays (43.15%). Therefore, the significant difference was found when applying
Chi-square test; the χ 2 value was 6.00, which means the significant at p< .05 (p value
= .014). This finding would be discussing further later on.
The dramatically difference of HH practice was found between the group of
HCWs which was supplied handrub and the group which was not. Since the handrub
The table showed that, since the handrub was placed next to the patient-beds, HCW
would clean their hands more often than when it was put on the working car (55.88%
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 75/121
p g (
vs. 41.01%). The Chi-square value was 79.09 referring to the significant level of
p< .001. Moreover, the odds ratio was 1.82 which could also show how difference of
HH compliance between the two groups.
The differences of HH decision among three working shifts were not enough to
reach any standard statistical significant level. Even HH compliance tended to be
higher in the morning (44.40%) than two other shifts (afternoon, 43.01% and evening,
43.97%), thought the Chi-square value was small ( χ 2 = .85) which meant the
significant value was .654 ( p>.05).
The distance from the nearest workable basin to the patient room (Distance) was
important factor affected to the decision of cleaning hands. The worst HH compliance
was found with group that had the distance further than 10 meters (29.73%), and the
best HH compliance belonged to the group that had the distance less than or equal 4
meters (47.35%). As a result, the Chi-square value was 67.83, which also meant the
significant level was p< .001. The result could be represented that the nearer the
distance, the better HH compliance.
The next variable was analyzed in the table 4.10a, risk level of HH opportunity,
also played an important role in making decision of clean hands. The participants
The type of HCWs also played an important role in the changing HH
compliance. Nurses cleaned their hands more frequently than doctor (39.5%) and

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 76/121
p q y
others HCWs did (40.7%). The Chi-square test showed the difference significant
among the groups ( χ 2=13.62; p<.001). From this table we also could see that nurses
had done the most of HH opportunities.
Table 18: Hand hygiene compliance differences among groups of demographic characteristics:Chi-square tests (N=4862)
Hand hygiene2
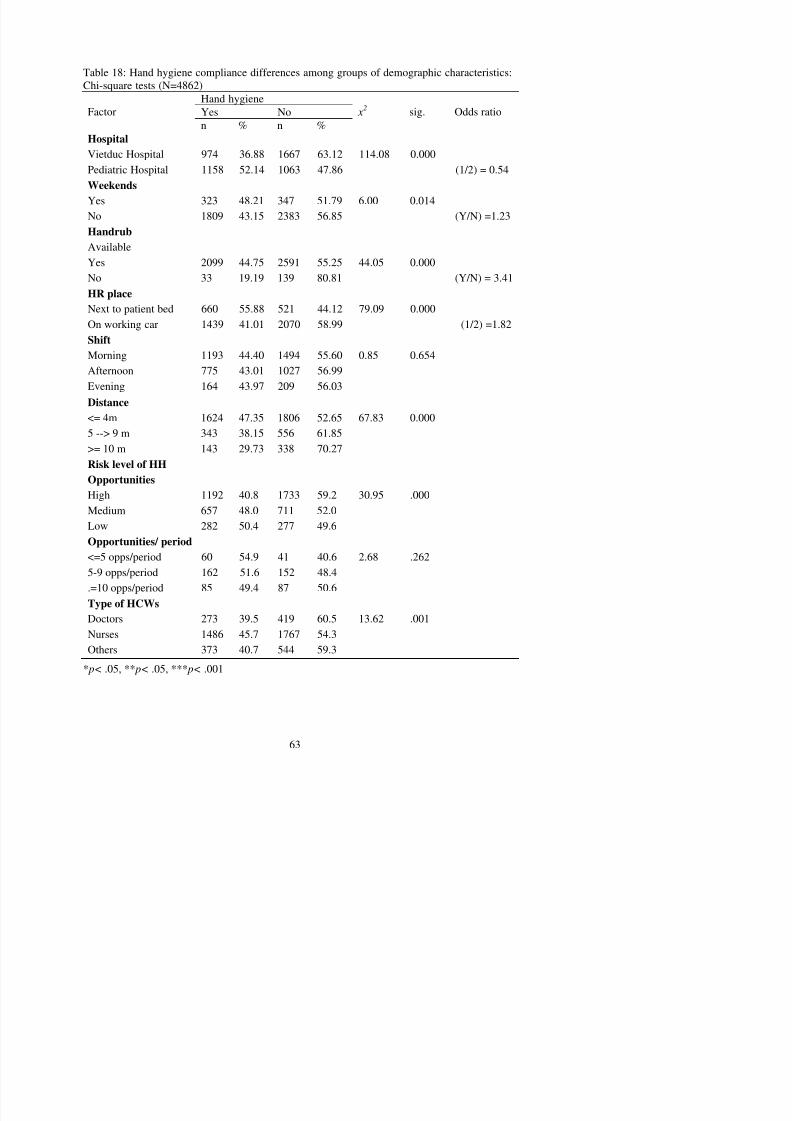
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 77/121
Yes NoFactor n % n % x
2
sig. Odds ratio
HospitalVietduc Hospital 974 36.88 1667 63.12 114.08 0.000Pediatric Hospital 1158 52.14 1063 47.86 (1/2) = 0.54
WeekendsYes 323 48.21 347 51.79 6.00 0.014
No 1809 43.15 2383 56.85 (Y/N) =1.23HandrubAvailableYes 2099 44.75 2591 55.25 44.05 0.000No 33 19.19 139 80.81 (Y/N) = 3.41
HR place
Next to patient bed 660 55.88 521 44.12 79.09 0.000On working car 1439 41.01 2070 58.99 (1/2) =1.82
ShiftMorning 1193 44.40 1494 55.60 0.85 0.654Afternoon 775 43.01 1027 56.99Evening 164 43.97 209 56.03
Distance <= 4m 1624 47.35 1806 52.65 67.83 0.0005 --> 9 m 343 38.15 556 61.85>= 10 m 143 29.73 338 70.27
Risk level of HHOpportunitiesHigh 1192 40.8 1733 59.2 30.95 .000
Medium 657 48.0 711 52.0Low 282 50.4 277 49.6
Opportunities/ period< 5 opps/period 60 54 9 41 40 6 2 68 262
A view on the difference of supplying HH facilities was analyzed. The table 19
showed that the Pediatric Hospital had been supplied HH facilities more sufficiently
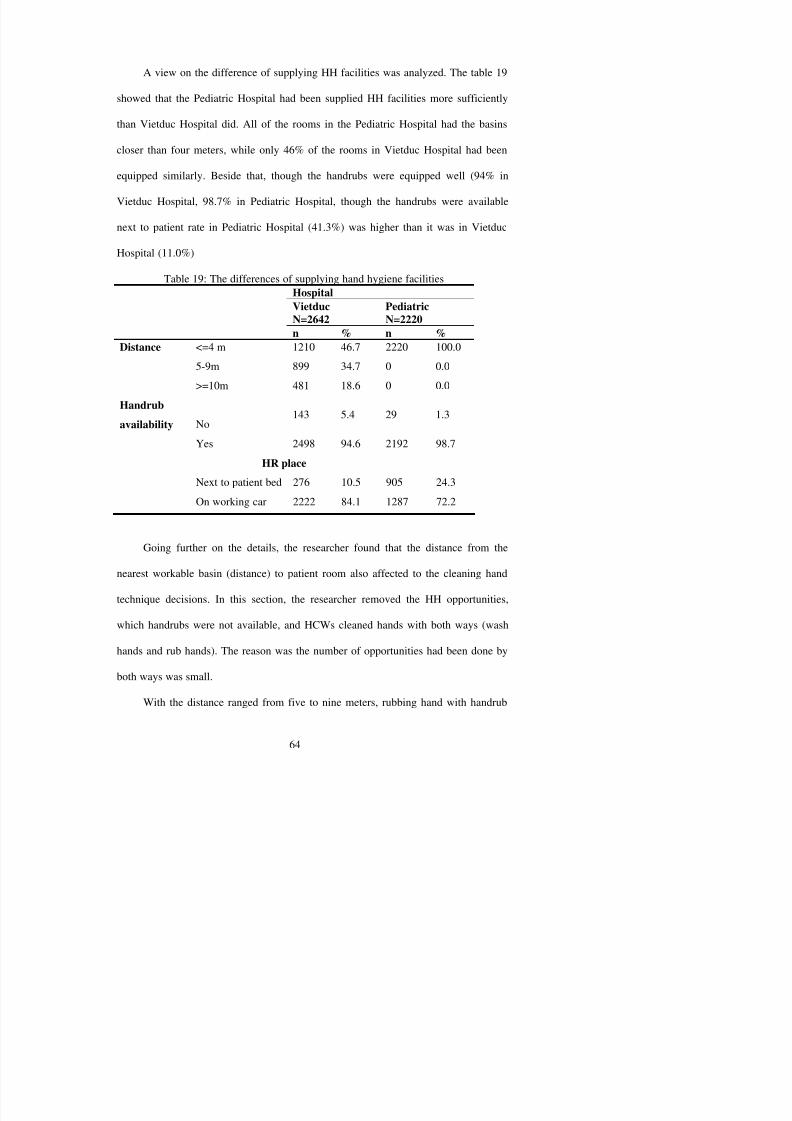
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 78/121
than Vietduc Hospital did. All of the rooms in the Pediatric Hospital had the basins
closer than four meters, while only 46% of the rooms in Vietduc Hospital had been
equipped similarly. Beside that, though the handrubs were equipped well (94% in
Vietduc Hospital, 98.7% in Pediatric Hospital, though the handrubs were available
next to patient rate in Pediatric Hospital (41.3%) was higher than it was in Vietduc
Hospital (11.0%)
Table 19: The differences of supplying hand hygiene facilitiesHospital
VietducN=2642 PediatricN=2220n % n %
Distance <=4 m 1210 46.7 2220 100.0
5-9m 899 34.7 0 0.0
>=10m 481 18.6 0 0.0
Handrubavailability No
143 5.4 29 1.3
Yes 2498 94.6 2192 98.7
HR place
Next to patient bed 276 10.5 905 24.3
On working car 2222 84.1 1287 72.2
Going further on the details, the researcher found that the distance from the
was chosen much more often than when the distance was less than or equal four
meters, as well as the distance was more than or equal ten meters (39.4 vs. 25.5 and

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 79/121
14.8). Discovering the data from the other view, the researcher found that the rate of
washing hand with water and soap was the lowest with the medium distance (at the
rate of 60.1%) and it was 14.4% higher with the closer distance. The Chi-square test
showed the significant difference of type of HH decision at p< .001 level ( χ 2 = 38.63).
Table 20: The relationship between Type of hand hygiene and the Patient room – Basindistance (N=4862)
Type of hand hygieneRub hand Wash handn % n %
x2 sig.
Distance <= 4m 410 25.5 1196 74.5 38.63 0.000***
5--> 9 m 132 39.4 203 60.1>= 10 m 21 14.8 121 85.2
***p< .001
5.2.3. Log-Linear Model analyses
In order to understand deeply about the associations among HH compliance with
some demographic characteristics, Loglinear model has been applied. The reasons of
choosing this model was that it could be applied for more than two categories
variables and it could analyze all the associations available among every groups of
each variable. The researcher chooses logically some variables to put in the model.
The first group of variable had chosen the factors including Distance, Handrub
availability, and HH. The distance variable had three categories, [distance=1] meant
terms until the fit of the model to the data became unacceptable base on the Likelihood
Ratio in the Goodness-of-fit tests (see table 21). The researcher also scanned all the

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 80/121
illogical associations, therefore the association between distance and handrub was
removed from the model design. Finally, the most parsimonious model was chosen:
[Constant + distance * hh + handrub * distance * hh]. The model fitted to explain all
the logical relationships among the categories of variables base on the Goodness-of-fit
statistics (table 21).
Table 21: Test of Goodness-of-fit for model 1DF Sig. X
2 Likelihood Ratio .0000 0Pearson .0000 0
The table 22 showed the summary of the Loglinear model for three variables
distance, hh and handrub. The parameter estimated in the table refers to the effect
sizes of the parameter. The predicted frequency of any cell (any parameter) was exp (µ
+ λ1…n), where µ was the constant estimate, λ1…n was the sum of the lambdas for all
effects in the model. Example, the frequency of [handrub=1]*[distance=1]*[hh=1]
was 1618 (exp (5.817 + λ[distance=1]*[hh=1] + λ[handrub=1]*[distance=1]*[hh=1] ) = exp (5.817 +
1.572 + 0) = exp (7.389) = 1618). Those frequencies were calculated and put in the
column named N. The odds ratio of each parameter was equal exponential of the
estimate value (OR=exp (estimate)). The odds ratio of parameters were calculated and
put in the column named OR.
N=340). This explanation would be seen more easily when looking at the effect size -
OR (OR = .96).
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 81/121
Four two-way parameters (effects) were contributed significantly to the model.
Three of them had the parameter estimate values larger than zero. Therefore, these
three parameters had the frequencies larger than the reference one did. In contract, the
other parameter estimate value was smaller than zero, which meant its frequencies
were smaller than the reference parameter. Among these four effects, the high Z
score absolutely found in [distance=1]*[hh=2] parameter ( Z =27.51), and in
[distance=1]*[hh=1] parameter ( Z =26.218) showed the strong positive effects in the
model. The lowest Z score absolutely belonged to parameter [distance=2]*[hh=2]
( Z =5.757) showed the weakest significant affecting to the model among two-way
interactions.
The previous statistical explanations could be explained as follows. The
opportunities, which the distance from the nearest basin to patient rooms was less than
or equal 4 meters, occurred very often because both two parameter estimate values
contributed the character were high. Beside that, the estimate value of
[distance=1]*[hh=1] was smaller than the estimate value of [distance=1]*[hh=2]
showed that if the distance was less than or equal 4 meters, the HCWs seemed to clean
their hands less frequently than did not they. While the distance was further or equal
[handrub=0]*[distance=3]*[hh=1] ( Z = -4.954) showed the weakest three-way effect
in the model. In contract, the strongest three-way effect in the model was the
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 82/121
parameter [handrub=0]*[distance=1]*[hh=2] due to the biggest parameter Z score
absolute ( Z = -26.675).
The findings about three-way interactions above could be explained as follows.
If the handrub was not available, HCWs did not clean their hands could be found
mostly when the distance was less than or equal four meters (N=76). Only one HCW
cleaned his/her hands when the handrub was not available and the distance was further
or equal ten meters.
From the table, the researcher found some other things when looking at the
group of opportunities which handrub was available. If the distance was less than or
equal four meters, the rate of HCWs cleaned their hands was 1618/(1618+1732) =
48.29%. If the distance ranged from five to nine meters, this rate was 321/(321+504)=
38.91%. If the distance was further or equal ten meters, the rate was
144/(144+336)=30.00%. In other words, among opportunities which the handrub were
available; the further the distance the worse the HH compliance. With opportunities,
which the handrub was not available. If the distance was less than or equal four
meter the HH compliance was 8/84=9.52%, it is 24/(24+54)=30.77% when the
distance ranged from five to nine meters, it was 1/(1+4) = 20% when the distance was
[handrub]*[distance]). The associations among the three variables were significant, yet
the single effect was not included in the model. Therefore, in order to understand
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 83/121
about the variable hh, we had to consider about the associations of the three variables
rather than every single effect. In other words, this model brought to the researcher the
better picture about the HH compliance in context of handrub availability and the
distance from the nearest workable basin to the patient room. It also gave the tool to
predict the frequency of each cell, listed the best suitable parameter which could be
used, and found out which parameter was more/less important to explain the data.
Table 22: Multi-Association among Patient room-Basin distance, Handrub availability, andHand hygiene performance (N=4862)Parameter n OR Estimate Z Sig.Std.
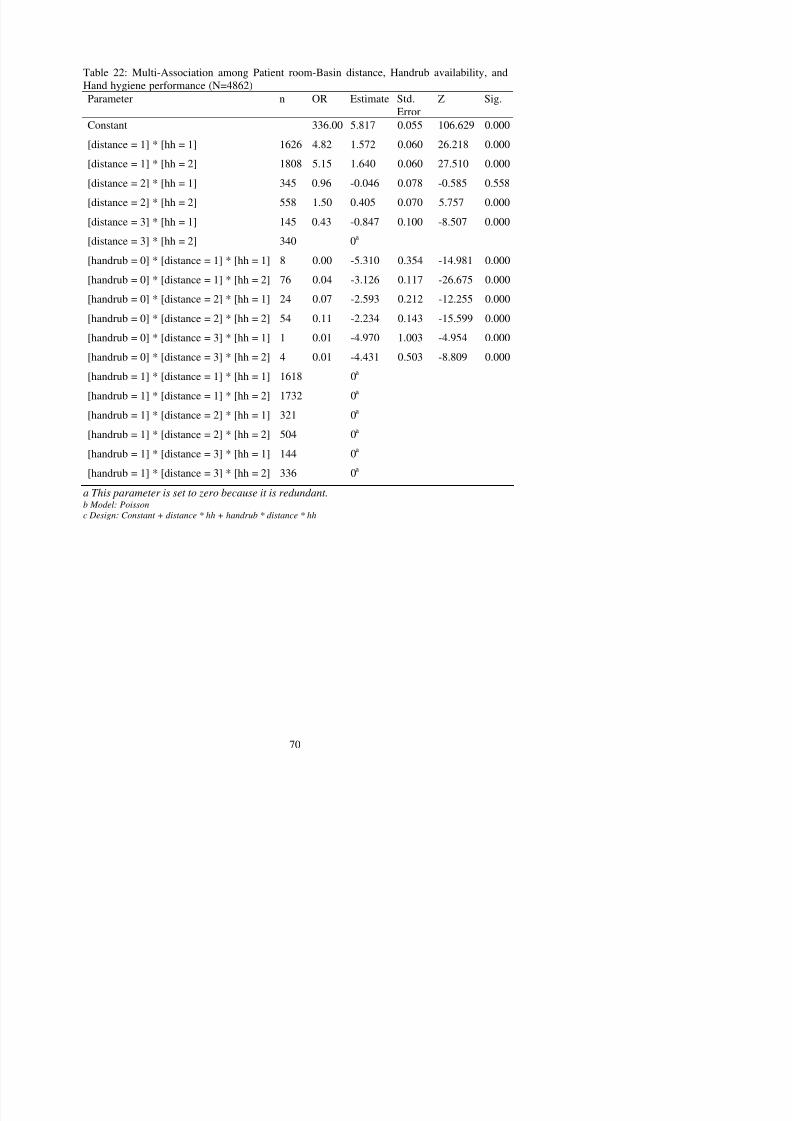
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 84/121
ErrorConstant 336.00 5.817 0.055 106.629 0.000
[distance = 1] * [hh = 1] 1626 4.82 1.572 0.060 26.218 0.000
[distance = 1] * [hh = 2] 1808 5.15 1.640 0.060 27.510 0.000
[distance = 2] * [hh = 1] 345 0.96 -0.046 0.078 -0.585 0.558
[distance = 2] * [hh = 2] 558 1.50 0.405 0.070 5.757 0.000
[distance = 3] * [hh = 1] 145 0.43 -0.847 0.100 -8.507 0.000
[distance = 3] * [hh = 2] 340 0a
[handrub = 0] * [distance = 1] * [hh = 1] 8 0.00 -5.310 0.354 -14.981 0.000
[handrub = 0] * [distance = 1] * [hh = 2] 76 0.04 -3.126 0.117 -26.675 0.000
[handrub = 0] * [distance = 2] * [hh = 1] 24 0.07 -2.593 0.212 -12.255 0.000
[handrub = 0] * [distance = 2] * [hh = 2] 54 0.11 -2.234 0.143 -15.599 0.000
[handrub = 0] * [distance = 3] * [hh = 1] 1 0.01 -4.970 1.003 -4.954 0.000
[handrub = 0] * [distance = 3] * [hh = 2] 4 0.01 -4.431 0.503 -8.809 0.000
[handrub = 1] * [distance = 1] * [hh = 1] 1618 0a
[handrub = 1] * [distance = 1] * [hh = 2] 1732 0a
[handrub = 1] * [distance = 2] * [hh = 1] 321 0a
[handrub = 1] * [distance = 2] * [hh = 2] 504 0a
[handrub = 1] * [distance = 3] * [hh = 1] 144 0a
[handrub = 1] * [distance = 3] * [hh = 2] 336 0a
a This parameter is set to zero because it is redundant.
b Model: Poissonc Design: Constant + distance * hh + handrub * distance * hh
The second group of variable had chosen the factors including the type of HCWs
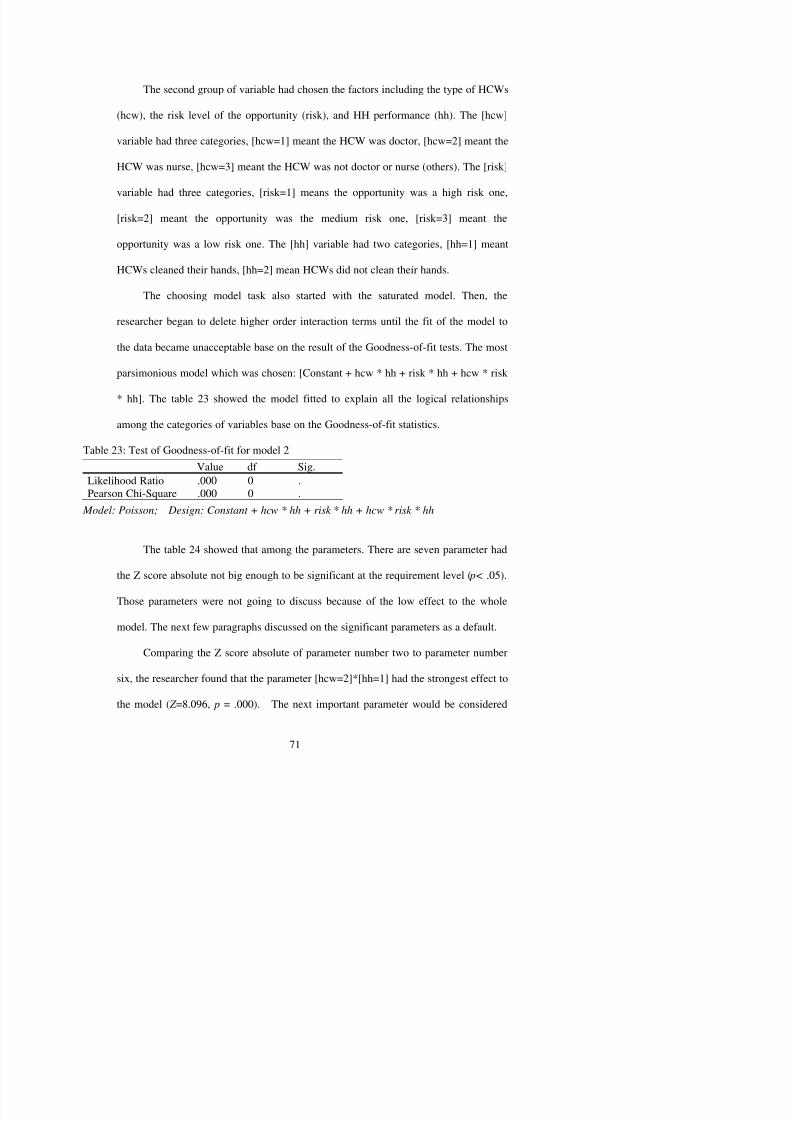
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 85/121
(hcw), the risk level of the opportunity (risk), and HH performance (hh). The [hcw]
variable had three categories, [hcw=1] meant the HCW was doctor, [hcw=2] meant the
HCW was nurse, [hcw=3] meant the HCW was not doctor or nurse (others). The [risk]
variable had three categories, [risk=1] means the opportunity was a high risk one,
[risk=2] meant the opportunity was the medium risk one, [risk=3] meant the
opportunity was a low risk one. The [hh] variable had two categories, [hh=1] meant
HCWs cleaned their hands, [hh=2] mean HCWs did not clean their hands.
The choosing model task also started with the saturated model. Then, the
researcher began to delete higher order interaction terms until the fit of the model to
the data became unacceptable base on the result of the Goodness-of-fit tests. The most
parsimonious model which was chosen: [Constant + hcw * hh + risk * hh + hcw * risk
* hh]. The table 23 showed the model fitted to explain all the logical relationships
among the categories of variables base on the Goodness-of-fit statistics.
Table 23: Test of Goodness-of-fit for model 2
Value df Sig.Likelihood Ratio .000 0 .Pearson Chi-Square .000 0 .
Model: Poisson; Design: Constant + hcw * hh + risk * hh + hcw * risk * hh
The table 24 showed that among the parameters. There are seven parameter had
was the parameter [hcw=2]*[hh=2] ( Z =6.694, p = .000). These showed the nurses’ HH
decisions were contributed much more than the rest were. The association between
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 86/121
[hcw=nurse] and [hh] needed to be strongly consider when explaining the data. While
the effect of the parameter [hcw=1=doctor]*[hh=1= ‘clean hands’] is less effective,
and then, the frequency of the parameter [hcw=1=doctor]*[hh= 1 = ‘clean hand’] is
the smallest one among these three significant parameters.
The parameters from eight to eleven were all significant taken part in the
association among the three variables. [risk=1=high]*[hh=2= ‘do not clean’] was the
most important parameter among these four parameters. This was cleared when
looking on the differences among the estimates of those effects. The high risk
opportunities was distributed the data sheet stronger than the low risk opportunities,
when the Z score of both parameters included [risk=1=high] were high ( Z 9=12.624
and Z8=8.589). In the meantime, the parameter [risk=2=medium]*[hh=1= ‘clean hand’]
has the lowest Z score ( Z =2.890), referred to the weakest effect to the whole model.
Thus, the researcher would use this parameter to explain the data, but more attention
should spend on it.
There were three parameters among three-ways could be trusted in when
explaining the data. The parameter number 15 and 16 show that doctors ([hcw=1])
tended to clean their hands less often with the medium risk opportunities
( Z 9=12.624 and Z 8=8.589); the two weakness ones were [hcw=1]*[hh=2] and
[hcw=1]*[risk=2]*[hh=1] (Z 2= -2.320 and Z 16= 2.722). Those suggested the researcher
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 87/121
about how to explain data accurately base on how much strong the associations were.
We could say, parameter eight and nine showed that the [risk=1=high] was the
important effect to HH [hh], in addition the higher OR of parameter number nine show
that HCWs tend to ‘not clean their hands’ among high risk opportunities. More explains
needed to be given out when talking about the parameter two and sixteen. The
significant associations were found weaker when comparing with other significant
parameters.
Table 24: Multi-Association among Type of HCWs , Risk level of HH opportunities and HH performance
No. Parameter N OR EstimateStd.Error
Z Sig.
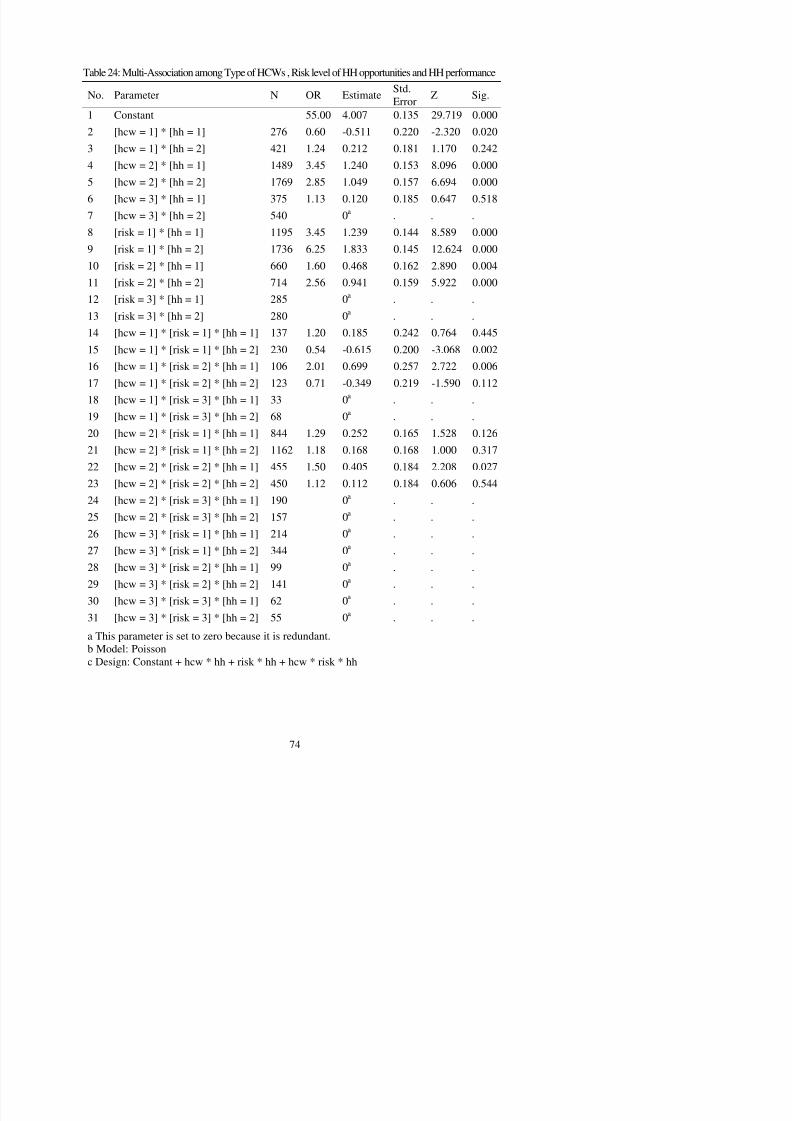
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 88/121
1 Constant 55.00 4.007 0.135 29.719 0.0002 [hcw = 1] * [hh = 1] 276 0.60 -0.511 0.220 -2.320 0.020
3 [hcw = 1] * [hh = 2] 421 1.24 0.212 0.181 1.170 0.242
4 [hcw = 2] * [hh = 1] 1489 3.45 1.240 0.153 8.096 0.000
5 [hcw = 2] * [hh = 2] 1769 2.85 1.049 0.157 6.694 0.000
6 [hcw = 3] * [hh = 1] 375 1.13 0.120 0.185 0.647 0.518
7 [hcw = 3] * [hh = 2] 540 0a
. . .8 [risk = 1] * [hh = 1] 1195 3.45 1.239 0.144 8.589 0.000
9 [risk = 1] * [hh = 2] 1736 6.25 1.833 0.145 12.624 0.000
10 [risk = 2] * [hh = 1] 660 1.60 0.468 0.162 2.890 0.004
11 [risk = 2] * [hh = 2] 714 2.56 0.941 0.159 5.922 0.000
12 [risk = 3] * [hh = 1] 285 0a . . .
13 [risk = 3] * [hh = 2] 280 0a . . .14 [hcw = 1] * [risk = 1] * [hh = 1] 137 1.20 0.185 0.242 0.764 0.445
15 [hcw = 1] * [risk = 1] * [hh = 2] 230 0.54 -0.615 0.200 -3.068 0.002
16 [hcw = 1] * [risk = 2] * [hh = 1] 106 2.01 0.699 0.257 2.722 0.006
17 [hcw = 1] * [risk = 2] * [hh = 2] 123 0.71 -0.349 0.219 -1.590 0.112
18 [hcw = 1] * [risk = 3] * [hh = 1] 33 0a . . .
19 [hcw = 1] * [risk = 3] * [hh = 2] 68 0a . . .20 [hcw = 2] * [risk = 1] * [hh = 1] 844 1.29 0.252 0.165 1.528 0.126
21 [hcw = 2] * [risk = 1] * [hh = 2] 1162 1.18 0.168 0.168 1.000 0.317
22 [hcw = 2] * [risk = 2] * [hh = 1] 455 1.50 0.405 0.184 2.208 0.027
23 [hcw = 2] * [risk = 2] * [hh = 2] 450 1.12 0.112 0.184 0.606 0.544
24 [hcw = 2] * [risk = 3] * [hh = 1] 190 0a . . .
25 [hcw = 2] * [risk = 3] * [hh = 2] 157 0a . . .
26 [hcw = 3] * [risk = 1] * [hh = 1] 214 0a . . .
27 [hcw = 3] * [risk = 1] * [hh = 2] 344 0a . . .
5.3. Other findings
The questionnaire was ended by an open question about the solution to improve HH
li Th k d di id d i fi f l i Th bl

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 89/121
compliance. The answers were taken note, and divided into five groups of solutions. The table
25 presented that summary. There were 130 participants’ responses. The most frequent
suggestion for improving HH compliance was “supplying enough equipment”, 61 responders
(46.9%) reported that. The second important solution was education, 30.8% responders
thought that educating HCWs could improve HH compliance. The equipment needed to set up
at the convenience place was also very important in their thinking, 23.1% of them mentioned
this. Observation HH compliance, improving the quality of equipments, reducing the number
of patients each HCWs had to take care of, building up reward and punishing policy were
some other solutions could be applied to improve HH compliance.
Table 25: Suggestion to improve Hand hygiene compliance by the opened question (N=130)
Suggestiton Order n %
1. The equipments need to be set in the convenient place 3rd 30 23.1
2. Need to supply enough equipment for HH 1st 61 46.9
3. The quality of equipment need to be improved 5th 15 11.5
4. Need to educate HCWs about HH 2nd 40 30.8
5. Construct the reward and punishment policy 7th 13 10.0
6. Observe HH compliance 4th 25 19.2
7. Reduce the patient/HCW rate 6th 14 10.8
5.4. Summary
The chapter has been presented the findings which relate to the purposes of the study.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 90/121
The questionnaire and observational forms have been analyzed by many statistical techniques
such as frequencies, Chi-square, ANOVA, and Loglinear model. The findings in this part will
be discussed more in the next chapter.
CHAPTER 6: DISCUSSION
This chapter will discuss the implications of the results presented in the chapter five

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 91/121
This chapter will discuss the implications of the results presented in the chapter five.
Firstly, the findings of the study will be discussed in the reference to possible explanations of
the findings and their convergence or divergence with previous literatures. Secondly, the
theoretical and research implications of the study will be made.
6.1. General discussion
The study used correlational design. It was strengthened by applying some techniques
such as the randomized sampling methods, doing the pilot, the single blind which was not
aware the HCWs about the observation, training observers. The supports from the experts in
validation the instruments, translation into Vietnamese helped the researcher improved the
quality of the data. In addition, the two hospitals are the teaching hospitals, where the
appearance of students did not affect much to the HCWs’ performance. Therefore, the data of
the study had high confidence, and could descriptive well the overall picture of HH
compliance among HCWs in the two hospitals in Vietnam.
The hospitals were the national leading specialty hospitals. Therefore, the findings of
the study might not be generated easily to other general hospitals or local hospitals.
Following characteristics should be considered while looking at the findings. The high-
educated HCWs in the hospitals had to serve quite a big number of patients; the HCWs had to
The equipments for HH in the two hospitals’ differences were significant. That would
effect to the HH decisions. In the Vietduc Hospital, the basin and handrub seemed to be
equipped not well when comparing with Pediatric Hospital The number of patient rooms
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 92/121
equipped not well when comparing with Pediatric Hospital. The number of patient rooms,
which did not have the basin inside occupied the percentage of 59.7% at Vietduc Hospital, but
just occupied 19.4% at the other. The handrub were also supplied better in the Pediatric
Hospital, many wards in this hospital had handrub inside. Therefore, the rate of HCWs use
handrub next to patient beds in the Pediatric was higher.
The observational data showed that the Vietduc Hospital was observed a little longer
than the Pediatric Hospital was. We observed them on the weekdays more than on the
weekends; and in the day shifts more than in the night shifts. The Vietduc Hospital seemed
not equip as well as the Pediatric Hospital. Those results also showed that the equipments for
HH in the two hospitals (even they are the national hospitals) could not compare with other
developed countries. There was still have nearly 30% of the patient rooms had the distance to
the nearest basin five meters or more. Beside that, only 24.3% of the rooms had the handrubsnext to patient bed and none of the HCWs had their own handrub bottle. The high risk
opportunities had the heavy weigh among opportunities that was similar with other studies
around the world. There was 66.9% of opportunities needed to do by nurses, the rest were
doctors and other HCWs.
One difficulty while conducting the study had been solved quite well that was ethical
6.2. Main Findings in Context of References
Hand hygiene compliance rate
The important finding of the study was: described the compliance of HH among HCWs
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 93/121
The important finding of the study was: described the compliance of HH among HCWs
in the two hospitals. The researcher applied both questionnaire and observation to find out it.
The result from the self-report of participants showed that the overall HH compliance rate was
85.58%. Most of HCWs tended to answer that they followed the recommendation. However,
the researcher found that the distribution of HH compliance rate was skewness (skewness =
2.07), which meant it was not a normal distribution. Therefore, the parametric tests could not
be applied. In addition, while looking on detail of the answer, the researcher found that the
HCWs tended to answer that they were applying hand hygiene very often, normally, more
than 90%; some participants even reported that their hand hygiene compliance rate was 100%,
which was utopian.
The HH compliance rate was lower by observation in comparing with self-reported
result, had been foreseen, it just was 43.9%. This finding agreed with the study of Pittet et al.(2004), which mentioned that if the participant awoke that they were observed, their HH
compliance rate would be higher than the compliance rate of those who did not know about
the observation. However, during the observation period, sometime, the observers still
recognized that the participants awoke that they were observed. Thus, it would be better if we
could use some other objective observation methods, such as video taping. This finding also
nine hospitals in Vietnam; the overall HH compliance rate was 13.4%. However, it was lower,
if compared with the other study conducted in the other three hospitals during few last months
of 2005 (Nguyen et al., 2007); the HH compliance rate was 6.3% at baseline and 65.7% after
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 94/121
of 2005 (Nguyen et al., 2007); the HH compliance rate was 6.3% at baseline and 65.7% after
intervention.
The factors associated with HH compliance
HCWs participated in the study showed the good knowledge on HH, yet had some
gaps. The average knowledge score was good (mean=18.26 in possible of 26), and not
significant difference between two hospitals. However, the findings also showed that there
were some gaps in the knowledge of HH. The time recommendation on handwashing, and
using gloves were not known well, they might due to the not up-to-date guideline. The low
rate of HCWs knew that using handrubs could remove bacteria even better than using soap
and water; and many of them did not know that handrubs made less skin irritation than
washing hand with soap and water. In addition, the HCWs seem lacked the knowledge on
colony pathogens on hands when saying that the innate bacteria are the main cause ofnosocomial infection. They show that the participants needed to be reeducated on these issues,
otherwise, those gaps would effect to the HH decisions.
The attitude score were positive (mean=81.82, SD=6.96 in possible of 115). Most of
HCWs had the attitude scores in rank of normal or good categories (from 70 to 92).
However, the results showed some conflicts in needing of explanation. Herein were details.
In addition, while most of HCWs agreed that if the patients reminded them, they would clean
their hands; only .7% of patients did this. Finally, the most acceptable reasons of “not clean
hands” were related to supplying equipments such as “not convenient”, “do not like the HH
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 95/121
pp y g q p ,
products” or “run out of the products”; and related to workload, “too busy”. In contract,
“unsure of needs”, and “forget” were not accepted widely as the reasons of “not clean hands”.
The findings were similar with the findings of some other studies such as the study of Wang
et al. (2006) or the study of Nobile et al. (2002), which also used questionnaire, and similar
outcomes.
Because of the fake results of the self-reported HH compliance, the statistical
techniques to find out the effect of Knowledge and Attitudes on HH compliance were not
performed. Thus, the researcher could not measure the hypotheses that knowledge and
attitudes were factors made the change of HH compliance. However, this would be considered
as normal result. The effects of knowledge and attitudes on HH behavior usually find out in
the longitudinal study with intervention. Some regular interventions could be education (toimprove knowledge and attitude of HH) or feedback (to improve attitudes toward HH).
Even the data of questionnaire could not give the researcher directly how much strong
the demographic characteristic, knowledge, attitude affected to HH compliance, however the
factors affected to HH compliance could be found in the open question analyses. The question
provides the researcher important suggestions to improve HH compliance, as the indirect way
mentioned in many responses. The roles of the administrators were important when HCWs
said that “observation was needed”, “the quality of product needed to be improved”, and
“Creating the reward and punishment policy”. “The number of patient, which HCWs have to
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 96/121
g p p y p ,
take care of”; and “Creating the reward and punishment policy” were also in the list of the
most important factors; even they were tended to be less important than the others were.
The results showed that there was a difference on HH compliances between the two
hospitals. This should be explained by looking on the difference between these two hospitals.
We found that the knowledge score was not different between these two hospitals; and the
knowledge score was even higher in the Vietduc Hospital. However, the facilities in the two
hospitals were different. The distance from the nearest basins to patient rooms at the Vietduc
Hospital were further than at the Pediatric Hospital, the and handrub at the Pediatric Hospital
was easier to access, in addition, the handrubs in the Pediatrics hospital were set next to
patient beds with higher rate. Those convenient equipments made the HH at the Pediatric
Hospital became easier to do rather than at Vietduc Hospital.The researcher went on the details to analyze every single demographic factor
affecting to the HH compliance. Though the researcher used both ANOVA and Chi-square to
analyze the association between HH compliance and the factors, the Chi-square test was more
sensitive than the ANOVA. The season was, the ANOVA analyzed the compliance of each
period, but the Chi-square analyzed for each opportunity.
available, the finding showed that handrubs set next to the patient bed could make the better
HH compliance rather than if they were in the working car. The similar findings were
reported by Bischoff et al. (1997) while they supplied more dispensers next to patient beds,
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 97/121
then the HH compliance increased. Thirdly, the distance from the nearest workable basin to
the patient room was also effected HH much. “The distance was five meters or more” could
be recognized as the barrier for HH. In the Vietnamese context, when “wash hands with
water and soap” was known as the better way to clean hands rather than “rub hands with
handrubs”, then it was still more popular (43.9%) rather than the other countries. The distance
from the basin to patient room became very important effect.
“The total opportunities in each period” did not affect to HH compliance, which could
be explained that the HCWs in these two hospitals seemed adapting with the workload. That
should be explored more while most of previous studies found that workload was the
important effect toward HH compliance (Pittet, Mourouga et al., 1999; Pittet et al., 2003).
The risk of HH opportunities, HCWs tended to wash their hands more often with the low risk,and medium risk, but not with high risk of the opportunities. This relationship between risk
level of the opportunities and HH compliance was reported in many other previous studies
(Raboud et al., 2004; Lipsett, & Swoboda, 2001; Wendt et al., 2004). The HCWs who were
nurses washed their hands more often than doctors and others; that was also recognized by
other researchers such as Rosenthal et al. (2003), etc.
The model could be added more variable in order to find out how much strong each
demographic characteristic related to HH compliance. This also emphasized that the factors
affected to HH compliance were not a single factor, thus, to improve the HH compliance, we

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 98/121
needed to pay attention on many factors.
6.3. Suggested Model
As the literature review, there were six most effective behavioral theories could use to
explain the compliance with HH. These were: (1) Biomedical model; (2) Operant behavior
and social learning;(3) Communications approach; (4) Theory of planned behavior; (5)
Precede health education theoretic model; (6) Diffusion of Innovation. The researcher focused
narrowly on discussing the findings in the theoretical view of the Theory of Planned Behavior
(TPB). Even in the study, the finding of study did not contain all the variables of the TPB
diagram, therefore the researcher could not apply the whole theory to explain the data.
However, its results tended to be closer with the TPB rather than other theories.
The TPB would be good guideline for the study which used the questionnaire as the
main instrument. The TPB considers one behavior is closed to intention, which meant want to
perform the action. However, as presented before, HH was a special behavior, therefore
before applying the Theory, researchers would better review more literature to decide how
could make TPB suitable with the study, such as adding some demographic variables. Other
notices were the way of measure the data, the formal questionnaire format (special for TPB).
Limitations
Firstly, the study design, this study was the cross-sectional study. The study was
conducted was conducted in a short period, thus it could not find out the trend of HH
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 99/121
compliance changing. Beside that, the study was conducted among health care workers in the
two national hospitals, and both two were not the general hospital. That meant the findings
could be generated well to the two hospitals’ population; but they needed to be considered
carefully when generating to the bigger population.
Secondly, the self-reported questionnaires, which supplied well the data of socio-
demographic characteristics, knowledge and attitudes toward HH. However, as many previous
studies, the self-reported HH compliance rate was exaggerated; in addition, some sensitivity
questions maybe result in incorrect response. This limitation was noticed in advance but was
still out of control; even the researcher tried to use the anonymous questionnaire, and
explained carefully. Another effort to find out the actual HH compliance rate was using the
observational method. It helped recording the actual HH compliance rate, yet it also could not
replace the self-reported data, because the participants of the two phases did not match
perfectly, even the two phases had been conducted in the same place.
Thirdly, even observers were not the staffs so they would be easier to give the honest
data. However, the observers were the freshmen nurses; they had just graduated from the
university, and did not have much experience on doing study as well as being a observer.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 100/121
Conclusions
HH is the simple most important procedure performed in hospital for preventing the
spread of nosocomial infection. However, the poor HH compliance is still found, the efforts in
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 101/121
changing the knowledge and attitude toward HH compliance are not effective. This could
again confirm that the issue of HH compliance is difficult to explain and chance.
The study described the compliance with HH among HCWs in the two Vietnamese
hospitals. The HH compliance rate was as low as many other studies, it was difference
significantly between self-reported result and observational result, thus the relationship
between HH compliance and the knowledge or attitudes toward HH could not be analyzed.
However, the effects of demographic characteristics on knowledge and attitude toward HH
compliance, as well as HH compliance, were analyzed deeply.
The picture of knowledge and attitudes toward HH was described. The HCWs in the
two hospitals showed the good knowledge but it still far from expectation, there were some
important issues had been misunderstood. Those mistakes needed to be considered seriously
by researchers and authorities. The study participants had the positive attitudes toward HH
compliance in general. However, the results showed that the HCWs did not really face with
the HH noncompliance. The feedback about HH noncompliance needed to be encouraged,
this task is not easy while it seemed be the culture among the population.
Many factors affected to HH compliance were found. The findings showed that the
was in Vietduc Hospital because of the hospital design and administrative support, but it also
could be caused by the total previous factors. Those findings supplied the evidence for HH
practice; they were valuable for building up the intervention plan in the hospitals and leading
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 102/121
future studies. The study did not find the relationship between HH compliance with some
other factors such as the working shifts, the number of opportunities per hour when analyzing
the observation data. However, basing on the opinions of participants about how to improve
HH compliance, the workload factor was still mentioned. Thus, more study need to be
conducted to confirm the findings of this study.
Last, the study is the fist study on HH of the author. Even its findings play some role
in HH practice and supply some evident for the studies in future, though it still has some
limitations due to the research experience of the author. To strength the results of the study,
the researcher plans to develop this study more in the future.
REFERENCES
Abouselof, R. H. (1999). Diffusion of Innovations: Describing the Perceptions of the Stages
in the Innovation-decision Process for Handwashing and Alcohol Hand Rubs. The
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 103/121
University of Utah Salt Lake.
Aizen, I. (2007). The figure of The Planned Behavior: Icek Aizen.
Askarian, M., Mirzaei, K., Mundy, L. M., & McLaws, M. L. (2005). Assessment of
knowledge, attitudes, and practices regarding isolation precautions among Iranian
healthcare workers. Infectious Control Hospitol Epidemiology, 26 (1), 105-108.
Bischoff, W. E., Reynolds, T. M., Sessler, C. N., Edmond, M. B., & Wenzel, R. P. (2000).
Handwashing compliance by health care workers: The impact of introducing an
accessible, alcohol-based hand antiseptic. Archives of Internal Medicine, 160(7), 1017-
1021.
Carter, K. C. (1981). Semmelweis and his predecessors. Medical History, 25(1), 57-72.
Conly, J. M., Hill, S., Ross, J., Lertzman, J., & Louie, T. J. (1989). Handwashing practices in
an intensive care unit: the effects of an educational program and its relationship to
infection rates. American Journal of Infection Control, 17 (6), 330-339.
Creedon, S. A. (2005). Healthcare workers' hand decontamination practices: compliance with
recommended guidelines. Journal Advanced Nursing, 51(3), 208-216.
Doebbeling, B. N., Stanley, G. L., Sheetz, C. T., Pfaller, M. A., Houston, A. K., Annis, L., et
practices of neonatal intensive care unit healthcare workers regarding nosocomial
infections, central venous catheter care, and HH. Infection Control and Hospital
Epidemiology, 25(9), 747-752.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 104/121
Kretzer, E. K., & Larson, E. L. (1998). Behavioral interventions to improve infection control
practices. American Journal of Infection Control, 26 (3), 245-253.
Lankford, M. G., Zembower, T. R., Trick, W. E., Hacek, D. M., Noskin, G. A., & Peterson, L.
R. (2003). Influence of role models and hospital design on HH of healthcare workers.
Emerging Infectious Disease, 9(2), 217-223.
Larson, E., & Kretzer, E. K. (1995). Compliance with handwashing and barrier precautions.
Journal Hospital Infection, 30 Suppl, 88-106.
Larson, E. (1999). Skin hygiene and infection prevention: more of the same or different
approaches? Clinical Infection Disease, 29(5), 1287-1294.
Larson, E. (2001). Hygiene of the skin: when is clean too clean? Emerging Infectious Disease,
7 (2), 225-230.
Lim, K. S., Yeh, Y. R., Jao, C. I., & Huang, C. C. (2001). A Survey of Knowledge and
Attitude towards Handwashing among Nurses. Nosocom Infection Control Journal, 11,
311-322.
Lipsett, P. A., & Swoboda, S. M. (2001). Handwashing compliance depends on professional
status. Surgical Infection (Larchmt), 2(3), 241-245.
Nobile, C. G., Montuori, P., Diaco, E., & Villari, P. (2002). Healthcare personnel and hand
decontamination in intensive care units: knowledge, attitudes, and behaviour in Italy.
Journal Hospital Infection, 51(3), 226-232.
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 105/121
O'Boyle, C. A., Henly, S. J., & Larson, E. (2001). Understanding adherence to HH
recommendations: the theory of planned behavior. American Journal of Infection
Control, 29(6), 352-360.
O’Boyce, J. M., & Wenzel, R. P. (2001). Antiseptic technology: access, affordability, and
acceptance. Emerging Infectious Diseases, 7 (2), 231-233.
O’Boyce, J. M., & Pittet, D. (2002). Guideline for HH in Health-Care Settings:
recommendations of the Healthcare Infection Control Practices Advisory Committee
and the HICPAC/SHEA/APIC/IDSA HH Task Force. Infection Control and Hospital
Epidemiology, 23(12 Suppl), S3-40.
Pessoa-Silva, C. L., Posfay-Barbe, K., Pfister, R., Touveneau, S., Perneger, T. V. & Pittet, D.
(2005). Attitudes and perceptions toward HH among healthcare workers caring for
critically ill neonates. Infection Control and Hospital Epidemiology, 26 (3), 305-311.
Pittet, D., Mourouga, P., & Perneger, T. V. (1999). Compliance with handwashing in a
teaching hospital. Infection Control Program. Annals Internal Medicine, 130(2), 126-
130.
Pittet, D., Hugonnet, S., Harbarth, S., Mourouga, P., Sauvan, V., Touveneau, S. et al. (2000).
Pittet, D., Simon, A., Hugonnet, S., Pessoa-Silva, C. L., Sauvan, V., & Perneger, T. V. (2004).
HH among physicians: performance, beliefs, and perceptions. Annals Internal Medicine,
141(1), 1-8.
R b d J S ki R W K M C P h G B J l (2004) P f
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 106/121
Raboud, J., Saskin, R., Wong, K., Moore, C., Parucha, G., Bennett, J. et al. (2004). Patterns of
handwashing behavior and visits to patients on a general medical ward of healthcare
workers. Infection Control and Hospital Epidemiology, 25(3), 198-202.
Rosenthal, V. D., Guzman, S., & Safdar, N. (2004). Effect of education and performance
feedback on rates of catheter-associated urinary tract infection in intensive care units in
Argentina. Infection Control and Hospital Epidemiology, 25(1), 47-50.
Rosenthal, V. D., McCormick, R. D., Guzman, S., Villamayor, C., & Orellano, P. W. (2003).
Effect of education and performance feedback on handwashing: the benefit of
administrative support in Argentinean hospitals. American Journal of Infection Control,
31(2), 85-92.
Rosenthal, V. D., McCormick, R. D., Guzman, S., Villamayor, C., & Orellano, P. W. (2003).
Effect of education and performance feedback on handwashing: the benefit of
administrative support in Argentinean hospitals. American Journal of Infection Control,
31(2), 85-92.
Sax, H., Perneger, T., Hugonnet, S., Herrault, P., Chraïti, M.-N., & Pittet, D. (2005).
Knowledge of Standard and Isolation Precautions in a Large Teaching Hospital.
Wendt, C., Knautz, D., & von Baum, H. (2004). Differences in HH behavior related to the
contamination risk of healthcare activities in different groups of healthcare workers.
Infection Control and Hospital Epidemiology, 25(3), 203-206.
W S P Ch H C H i h W S Ch C Y H S M T K I t l (2004)
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 107/121
Won, S. P., Chou, H. C., Hsieh, W. S., Chen, C. Y., Huang, S. M., Tsou, K. I. et al. (2004).
Handwashing program for the prevention of nosocomial infections in a neonatal
intensive care unit. Infection Control and Hospital Epidemiology, 25(9), 742-746.
Nguyen, P. T., Vuong, T. N. T., & Le, T. A. T. (2002). Đánh giá số lượ ng vi khuẩn trên tay
của nhân viên y tế. Unpublished Research. Cho Ray hospital.
Nguyen, V. H., Nguyen, X. Q., Truong, A. T., & Doan, M. P. (2007). Mức độ ô nhiễm vi
khuẩn ở bàn tay nhân viên y tế và hiệu quả khử khuẩn của một số hoá chất vệ sinh.
Paper presented at the Sum up meeting on Hand Hygiene in Hospitals.
Appendix
Appendix 1: The questionnaire of hand hygiene practice
Demographic characteristics information
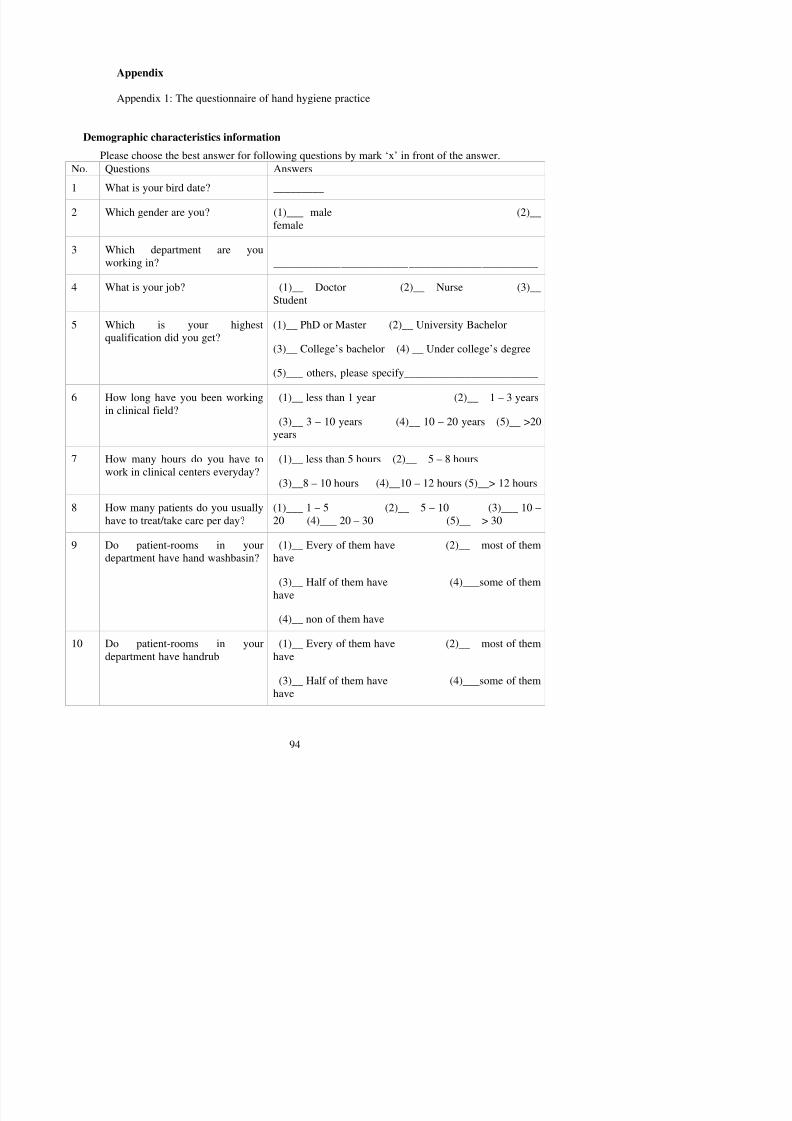
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 108/121
Please choose the best answer for following questions by mark ‘x’ in front of the answer.No. Questions Answers
1 What is your bird date? _________
2 Which gender are you? (1)___ male (2)__female
3 Which department are youworking in? _______________________________________________
4 What is your job? (1)__ Doctor (2)__ Nurse (3)__Student
5 Which is your highestqualification did you get?
(1)__ PhD or Master (2)__ University Bachelor
(3)__ College’s bachelor (4) __ Under college’s degree
(5)___ others, please specify________________________
6 How long have you been working
in clinical field?
(1)__ less than 1 year (2)__ 1 – 3 years
(3)__ 3 – 10 years (4)__ 10 – 20 years (5)__ >20years
7 How many hours do you have towork in clinical centers everyday?
(1)__ less than 5 hours (2)__ 5 – 8 hours
(3)__8 – 10 hours (4)__10 – 12 hours (5)__> 12 hours
8 How many patients do you usuallyhave to treat/take care per day?
(1)___ 1 – 5 (2)__ 5 – 10 (3)___ 10 –20 (4)___ 20 – 30 (5)__ > 30
9 Do patient-rooms in yourd t t h h d hb i ?
(1)__ Every of them have (2)__ most of themh
(5)__ non of them have
11 Where is the handrub available? (1)__ at the patient bed (2)__ in yourpocket
(3)__ on the working car (4)___in the prepare
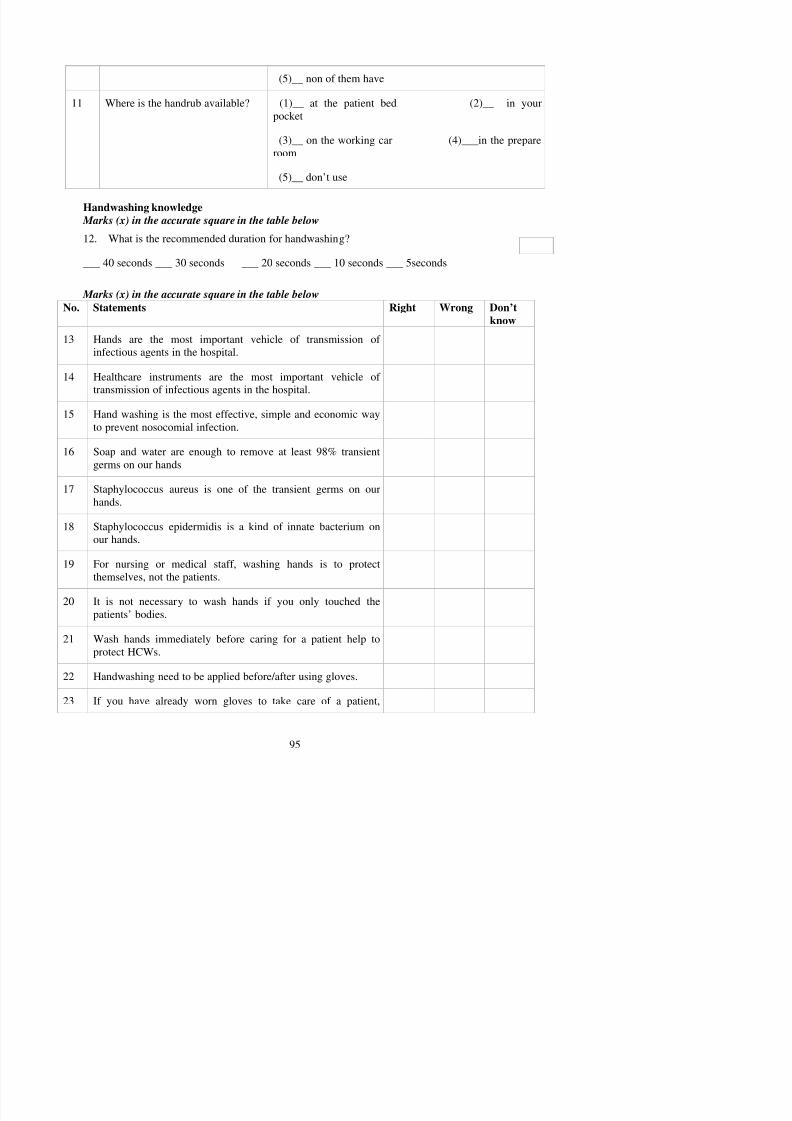
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 109/121
room
(5)__ don’t use
Handwashing knowledge
Marks (x) in the accurate square in the table below
12. What is the recommended duration for handwashing?
___ 40 seconds ___ 30 seconds ___ 20 seconds ___ 10 seconds ___ 5seconds
Marks (x) in the accurate square in the table below
No. Statements Right Wrong Don’t
know13 Hands are the most important vehicle of transmission of
infectious agents in the hospital.
14 Healthcare instruments are the most important vehicle oftransmission of infectious agents in the hospital.
15 Hand washing is the most effective, simple and economic wayto prevent nosocomial infection.
16 Soap and water are enough to remove at least 98% transientgerms on our hands
17 Staphylococcus aureus is one of the transient germs on ourhands.
18 Staphylococcus epidermidis is a kind of innate bacterium onour hands.
taking off the gloves will be enough, you do not have to washyour hands before looking after other patients.
24 It is not necessary to wash your hands if you only touched the
medical devices that the patients have touched.
25 Comparing to the hand drier, hand towel is a better tool to

8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 110/121
p g ,remove the germs on our hands.
26 It is necessary to wash your hands if you touched the patients’medical record.
27 The bacteria that will cause nosocomial infection are mainlyinnate bacteria.
28 Long fingernails are associated with higher gram-negativebacterial hand contamination.
29 Fingernails shorter than fingertips are not associated withhigher bacterial hand contamination.
30 Wearing rings are associated with higher gram-negativebacterial hand contamination.
31 After washing your hands, dry your hands with the handtowels; throw them away and then close the tap.
32 The patient’s family members also have to wash their handswhen they’re looking after the patient.
33 Hand washing is replaceable by using gloves.
34 Non-sterile gloves are used to protect patient againsttransmission of an infectious agent by the hands.
35 It is necessary to remove the ring, watch and other handornaments before washing your hands.
36 The effect of washing hands does not depend on how long you
Handwashing attitude:
Marks (x) in the accurate blank
38. When working with another caregiver and you forget to disinfect your hands beforetouching a patient, how often does your colleague remind you?
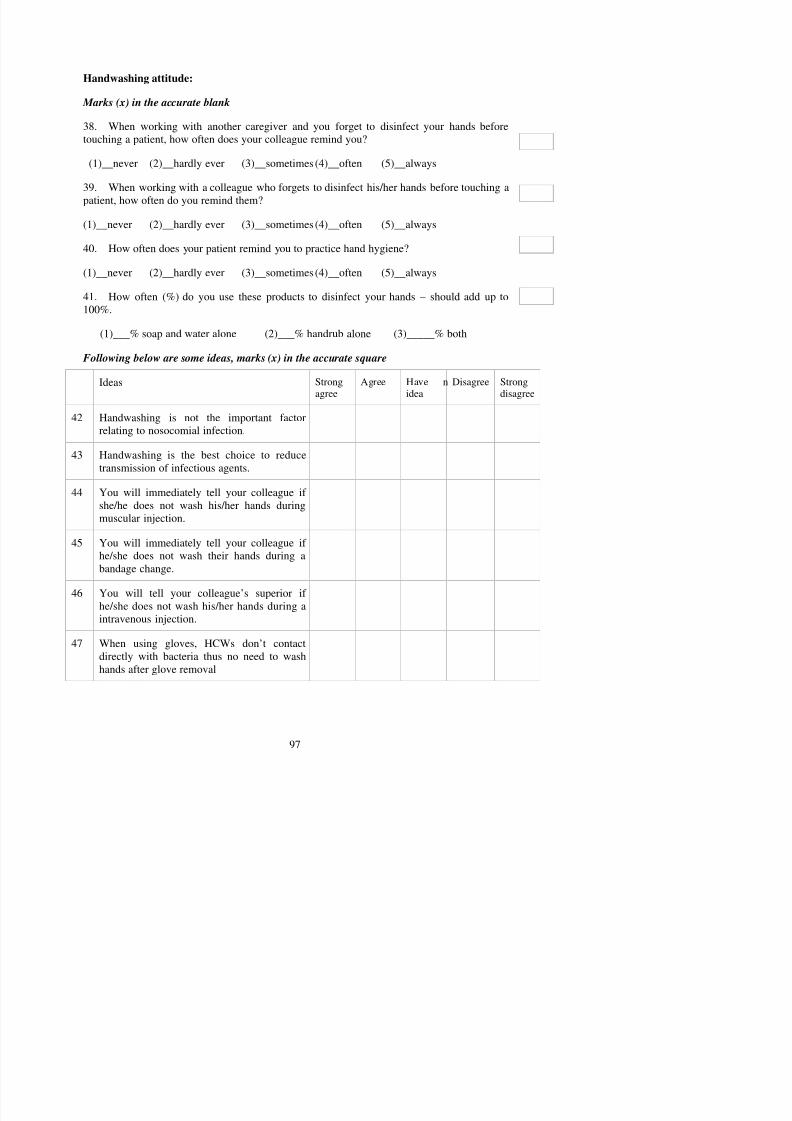
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 111/121
(1)__never (2)__hardly ever (3)__sometimes (4)__often (5)__always
39. When working with a colleague who forgets to disinfect his/her hands before touching apatient, how often do you remind them?
(1)__never (2)__hardly ever (3)__sometimes (4)__often (5)__always
40. How often does your patient remind you to practice hand hygiene?
(1)__never (2)__hardly ever (3)__sometimes (4)__often (5)__always
41. How often (%) do you use these products to disinfect your hands – should add up to100%.
(1)___% soap and water alone (2)___% handrub alone (3)_____% both
Following below are some ideas, marks (x) in the accurate square
Ideas Strongagree
Agree Have nidea
Disagree Strongdisagree
42 Handwashing is not the important factorrelating to nosocomial infection.
43 Handwashing is the best choice to reducetransmission of infectious agents.
44 You will immediately tell your colleague ifshe/he does not wash his/her hands during
muscular injection.
45 You will immediately tell your colleague ifhe/she does not wash their hands during a
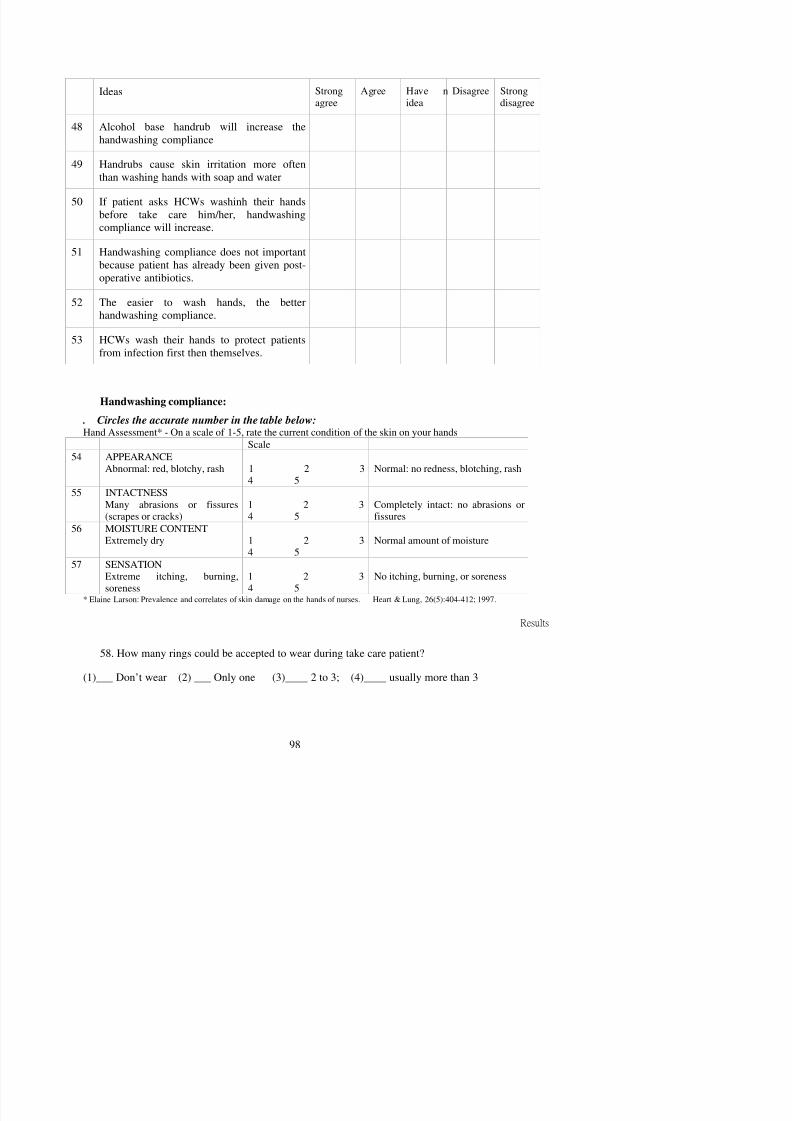
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 112/121
Strongagree
Agree Haveno idea
Dis-agree
Strongdisagree
When you don’t disinfect your hands(use soap or an alcohol hand-rub to killmicrobes) when you should, what is the
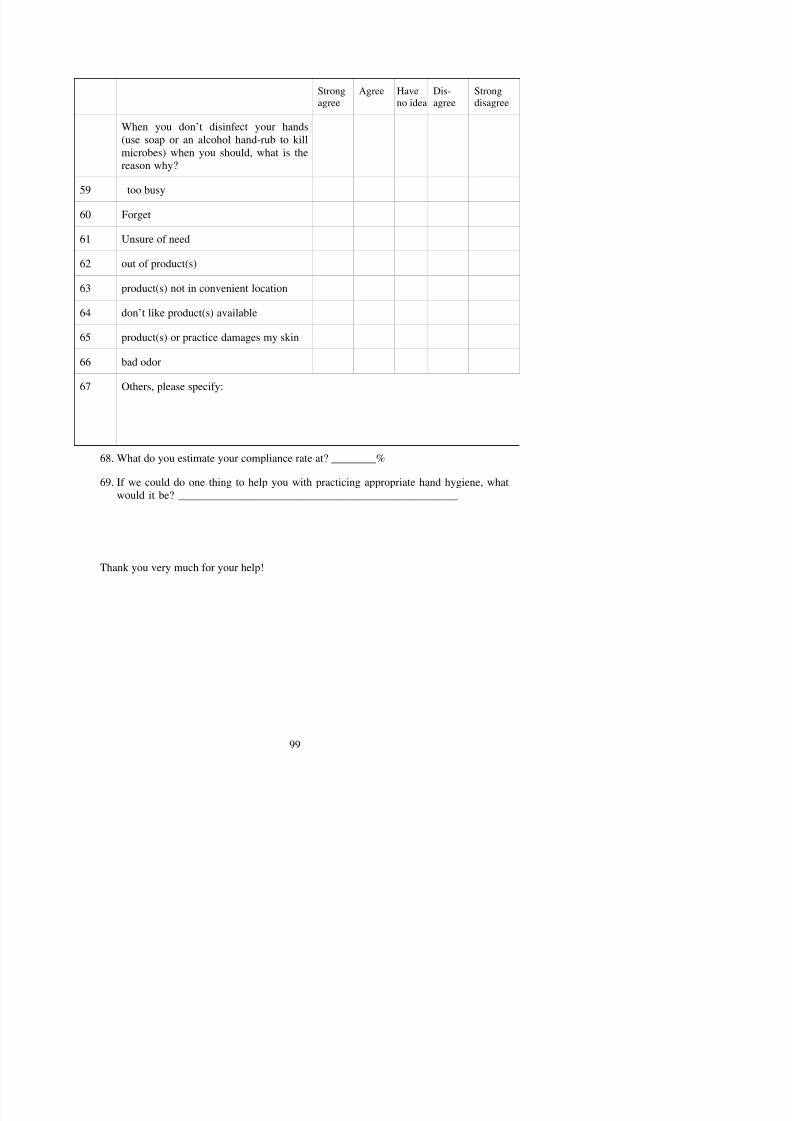
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 113/121
microbes) when you should, what is thereason why?
59 too busy
60 Forget
61 Unsure of need
62 out of product(s)
63 product(s) not in convenient location
64 don’t like product(s) available
65 product(s) or practice damages my skin
66 bad odor
67 Others, please specify:
68. What do you estimate your compliance rate at? ________%
69. If we could do one thing to help you with practicing appropriate hand hygiene, whatwould it be? __________________________________________________
Appendix 2: Hand hygiene observational form
Hospital:_____________________ Clinical ward:_____________________________
No. of patient bed:______________ Observation period: from___________ to __________Work shift: ____ morning; ____afternoon; ____ evening. Estimated distance from patient room to the nearest basin:____ m
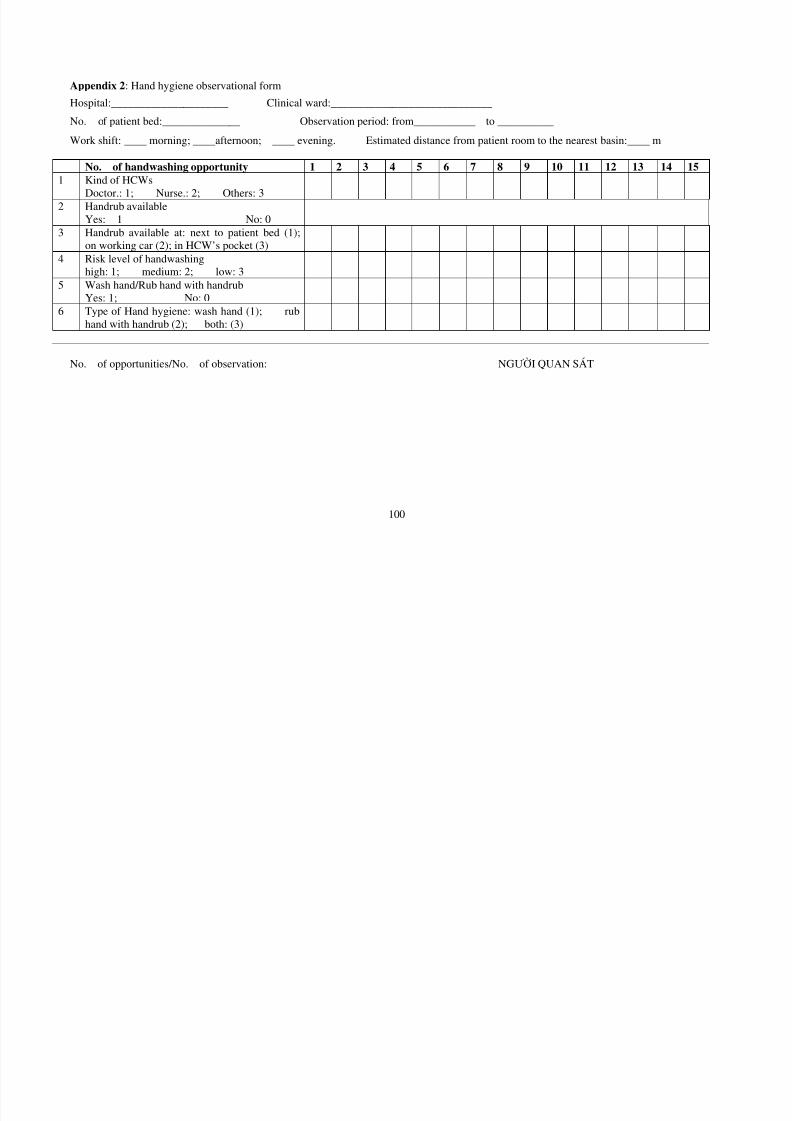
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 114/121
100
No. of handwashing opportunity 1 2 3 4 5 6 7 8 9 10 11 12 13 14 151 Kind of HCWs
Doctor.: 1; Nurse.: 2; Others: 32 Handrub available
Yes: 1 No: 03 Handrub available at: next to patient bed (1);on working car (2); in HCW’s pocket (3)
4 Risk level of handwashinghigh: 1; medium: 2; low: 3
5 Wash hand/Rub hand with handrubYes: 1; No: 0
6 Type of Hand hygiene: wash hand (1); rubhand with handrub (2); both: (3)
No. of opportunities/No. of observation: NGƯỜI QUAN SÁT
Appendix 3:Translated version of the questionnaire (Vietnamese version)
NGHIÊN CỨ U: MỐI TƯƠ NG QUAN GIỮ A KIẾN THỨ C, THÁI ĐỘ VÀSỰ TUÂN THỦ RỬ A TAY TRONG NHÂN VIÊN Y TẾ.
BỘ CÂU HỎI KHẢO SÁT VỀ RỬ ATAY
ầ
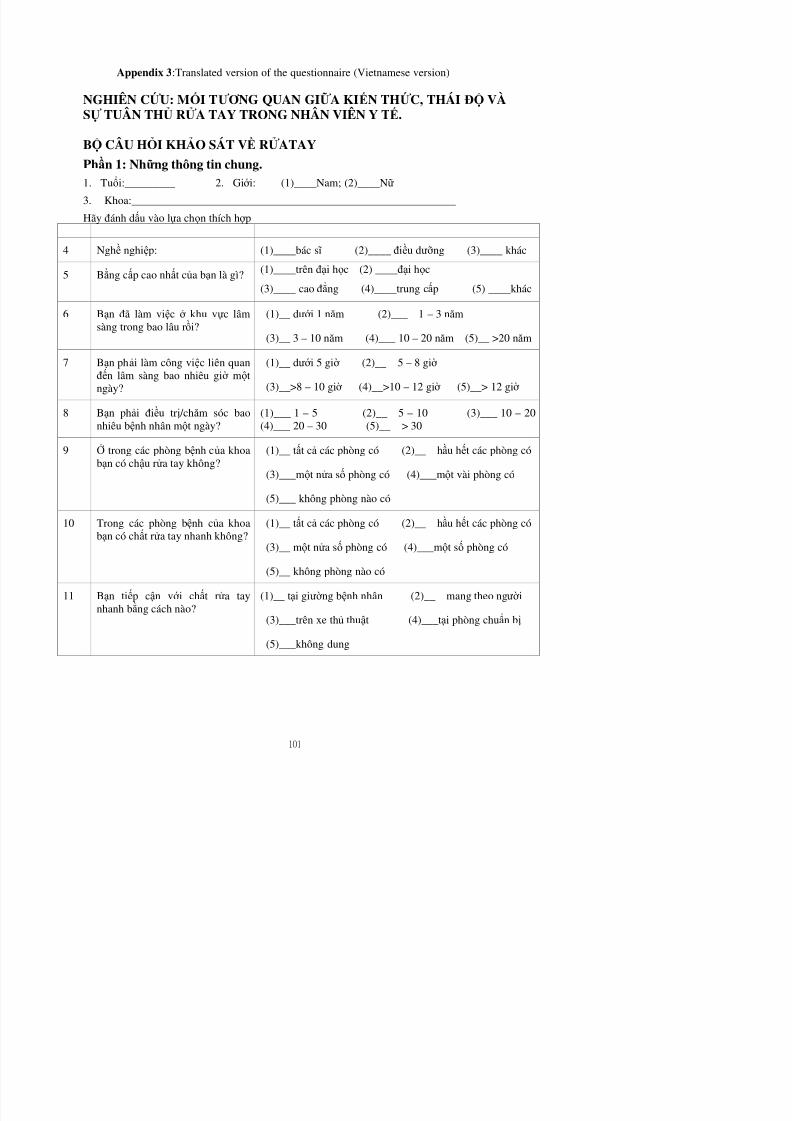
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 115/121
Phần 1: Nhữ ng thông tin chung.1. Tuổi:_________ 2. Giớ i: (1)____Nam; (2)____Nữ
3. Khoa:__________________________________________________________
Hãy đánh dấu vào lựa chọn thích hợ p
4 Nghề nghiệp: (1)____bác s ĩ (2)____ điều dưỡ ng (3)____ khác
5 Bằng cấp cao nhất của bạn là gì? (1)____trên đại học (2) ____đại học
(3)____ cao đẳng (4)____trung cấp (5) ____khác
6 Bạn đã làm việc ở khu vực lâmsàng trong bao lâu rồi?
(1)__ dướ i 1 năm (2)___ 1 – 3 năm
(3)__ 3 – 10 năm (4)___ 10 – 20 năm (5)__ >20 năm
7 Bạn phải làm công việc liên quanđến lâm sàng bao nhiêu giờ mộtngày?
(1)__ dướ i 5 giờ (2)__ 5 – 8 giờ
(3)__>8 – 10 giờ (4)__>10 – 12 giờ (5)__> 12 giờ
8 Bạn phải điều trị /chăm sóc baonhiêu bệnh nhân một ngày? (1)___ 1 – 5 (2)__ 5 – 10 (3)___ 10 – 20(4)___ 20 – 30 (5)__ > 30
9 Ở trong các phòng bệnh của khoabạn có chậu rửa tay không?
(1)__ tất cả các phòng có (2)__ hầu hết các phòng có
(3)___một nửa số phòng có (4)___một vài phòng có
(5)___ không phòng nào có
10 Trong các phòng bệnh của khoabạn có chất rửa tay nhanh không?
(1)__ tất cả các phòng có (2)__ hầu hết các phòng có
(3)__ một nửa số phòng có (4)___một số phòng có
Phần 2: Kiến thứ c về rử a tay Đ ánh d ấ u (x) vào l ự a chọ n phù hợ p trong bả ng sau đ ây
12. Thờ i gian cần thiết để rửa tay thườ ng quy là bao lâu?
(1)____1 phút (2)___ 40 giây (3)___ 30 giây
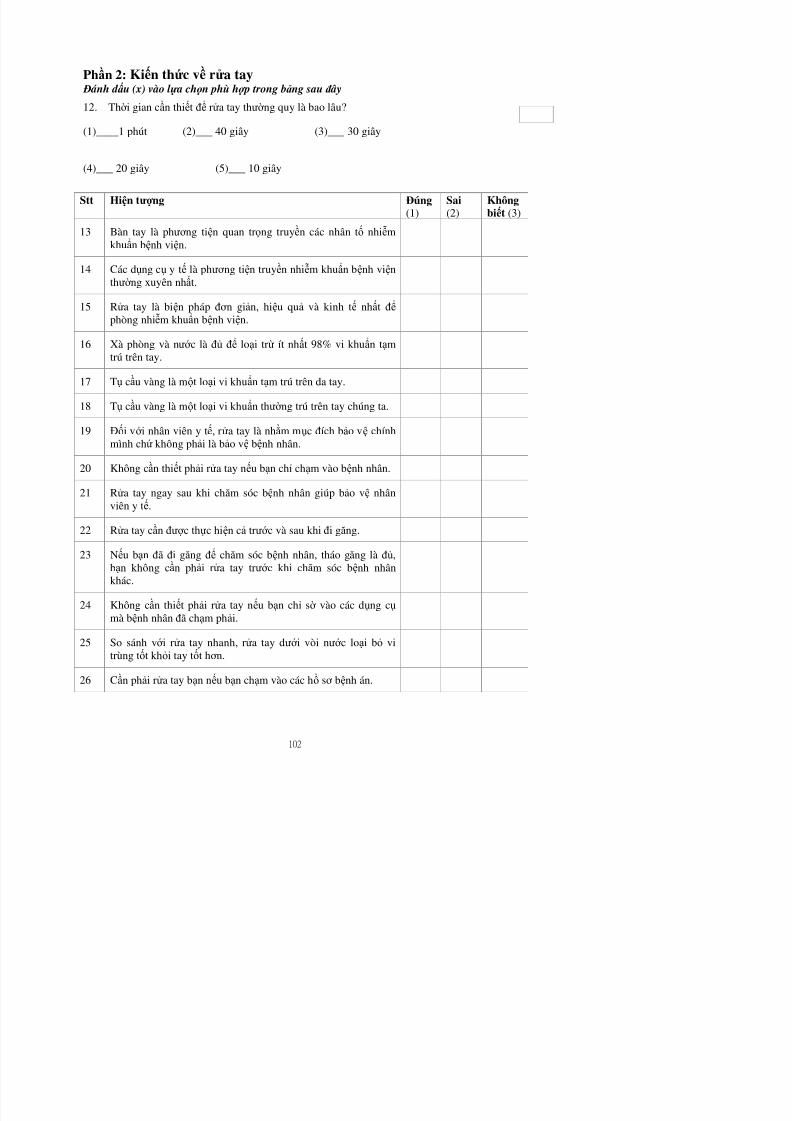
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 116/121
(4)___ 20 giây (5)___ 10 giây
Stt Hiện tượ ng Đúng(1)
Sai(2)
Khôngbiết (3)
13 Bàn tay là phươ ng tiện quan trọng truyền các nhân tố nhiễmkhuẩn bệnh viện.
14 Các dụng cụ y tế là phươ ng tiện truyền nhiễm khuẩn bệnh việnthườ ng xuyên nhất.
15 Rửa tay là biện pháp đơ n giản, hiệu quả và kinh tế nhất để
phòng nhiễm khuẩn bệnh viện.
16 Xà phòng và nướ c là đủ để loại trừ ít nhất 98% vi khuẩn tạmtrú trên tay.
17 Tụ cầu vàng là một loại vi khuẩn tạm trú trên da tay.
18 Tụ cầu vàng là một loại vi khuẩn thườ ng trú trên tay chúng ta.
19 Đối vớ i nhân viên y tế, rửa tay là nhằm mục đích bảo vệ chínhmình chứ không phải là bảo vệ bệnh nhân.
20 Không cần thiết phải rửa tay nếu bạn chỉ chạm vào bệnh nhân.
21 Rửa tay ngay sau khi chăm sóc bệnh nhân giúp bảo vệ nhânviên y tế.
22 Rửa tay cần đượ c thực hiện cả trướ c và sau khi đi găng.
23 Nếu bạn đã đi găng để chăm sóc bệnh nhân tháo găng là đủ
Stt Hiện tượ ng Đúng Sai Khôngbiết
27 Vi khuẩn có thể gây nhiễm trùng bệnh viện chủ yếu là vi khuẩnthườ ng trú.
28 Móng tay dài có liên quan đến sự nhiễm cao hơ n các vi khuẩn
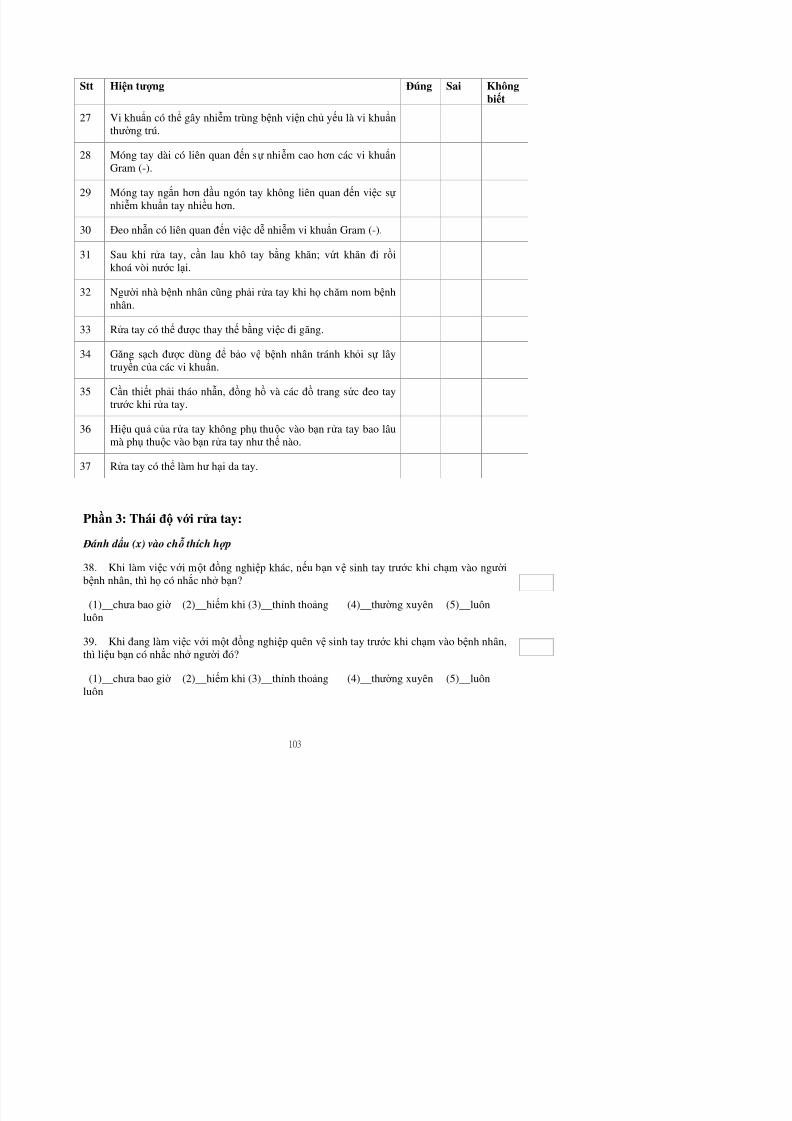
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 117/121
Gram (-).
29 Móng tay ngắn hơ n đầu ngón tay không liên quan đến việc sự nhiễm khuẩn tay nhiều hơ n.
30 Đeo nhẫn có liên quan đến việc dễ nhiễm vi khuẩn Gram (-).
31 Sau khi rửa tay, cần lau khô tay bằng khăn; vứt khăn đi rồikhoá vòi nướ c lại.
32 Ngườ i nhà bệnh nhân cũng phải rửa tay khi họ chăm nom bệnhnhân.
33 Rửa tay có thể đượ c thay thế bằng việc đi găng.
34 Găng sạch đượ c dùng để bảo vệ bệnh nhân tránh khỏi sự lâytruyền của các vi khuẩn.
35 Cần thiết phải tháo nhẫn, đồng hồ và các đồ trang sức đeo taytrướ c khi rửa tay.
36 Hiệu quả của rửa tay không phụ thuộc vào bạn rửa tay bao lâumà phụ thuộc vào bạn rửa tay như thế nào.
37 Rửa tay có thể làm hư hại da tay.
Phần 3: Thái độ vớ i rử a tay:
Đ ánh d ấ u (x) vào chỗ thích hợ p
Đ ánh d ấ u (x) vào chỗ thích hợ p
40. Bệnh nhân có bao giờ nhắc bạn vệ sinh tay?
(1)__chưa bao giờ (2)__hiếm khi (3)__thỉnh thoảng (4)__thườ ng xuyên (5)__luônluôn
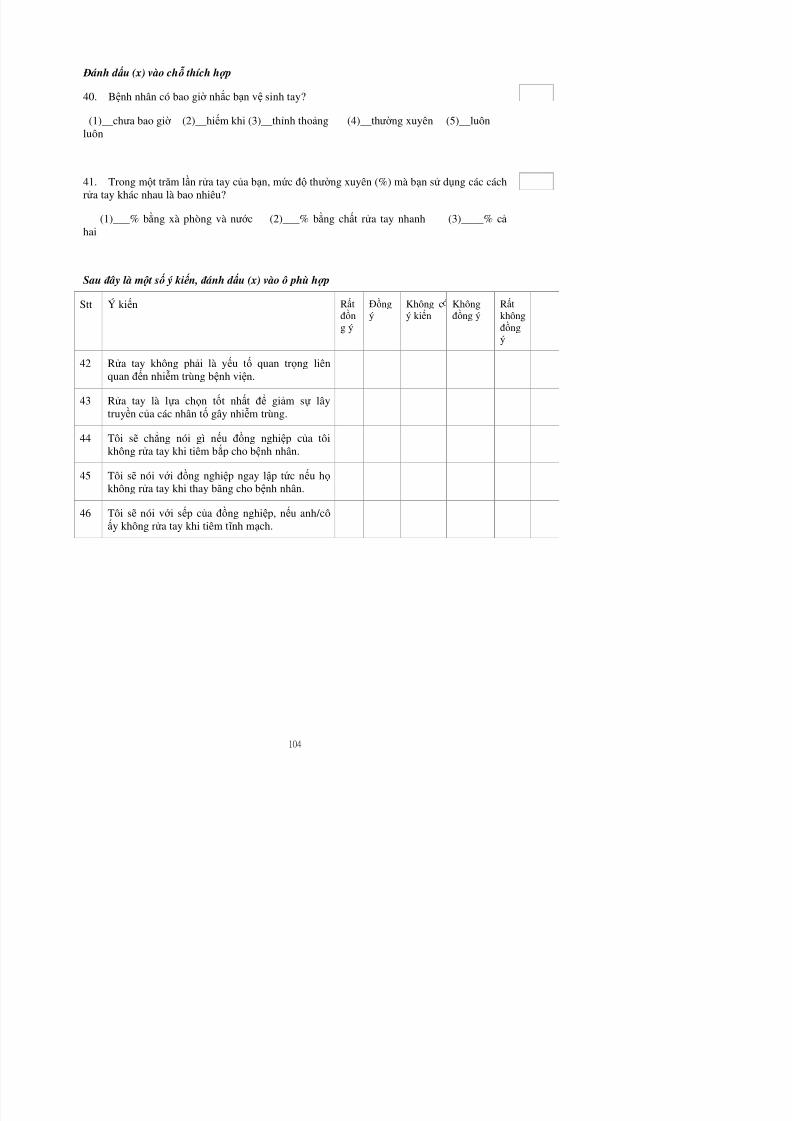
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 118/121
41. Trong một trăm lần rửa tay của bạn, mức độ thườ ng xuyên (%) mà bạn sử dụng các cáchrửa tay khác nhau là bao nhiêu?
(1)___% bằng xà phòng và nướ c (2)___% bằng chất rửa tay nhanh (3)____% cả hai
Sau đ ây là mộ t số ý kiế n, đ ánh d ấ u (x) vào ô phù hợ p
Stt Ý kiến Rấtđồ
ng ý
Đồng
ý
Không c
ý kiến
Khôngđồ
ng ý
Rất
khôngđồngý
42 Rửa tay không phải là yếu tố quan trọng liênquan đến nhiễm trùng bệnh viện.
43 Rửa tay là lựa chọn tốt nhất để giảm sự lây
truyền của các nhân tố gây nhiễm trùng.44 Tôi sẽ chẳng nói gì nếu đồng nghiệp của tôi
không rửa tay khi tiêm bắp cho bệnh nhân.
45 Tôi sẽ nói vớ i đồng nghiệp ngay lập tức nếu họ không rửa tay khi thay băng cho bệnh nhân.
46 Tôi sẽ nói vớ i sếp của đồng nghiệp, nếu anh/côấy không rửa tay khi tiêm t ĩ nh mạch.
Stt Ý kiến Rấtđồng ý
Đồngý
Không cý kiến
Khôngđồng ý
Rấtkhôngđồng ý
47 Khi đã đi găng, nhân viên y tế không tiếp xúctrực tiếp vớ i vi khuẩn nên không cần rửa tay saukhi đi găng.
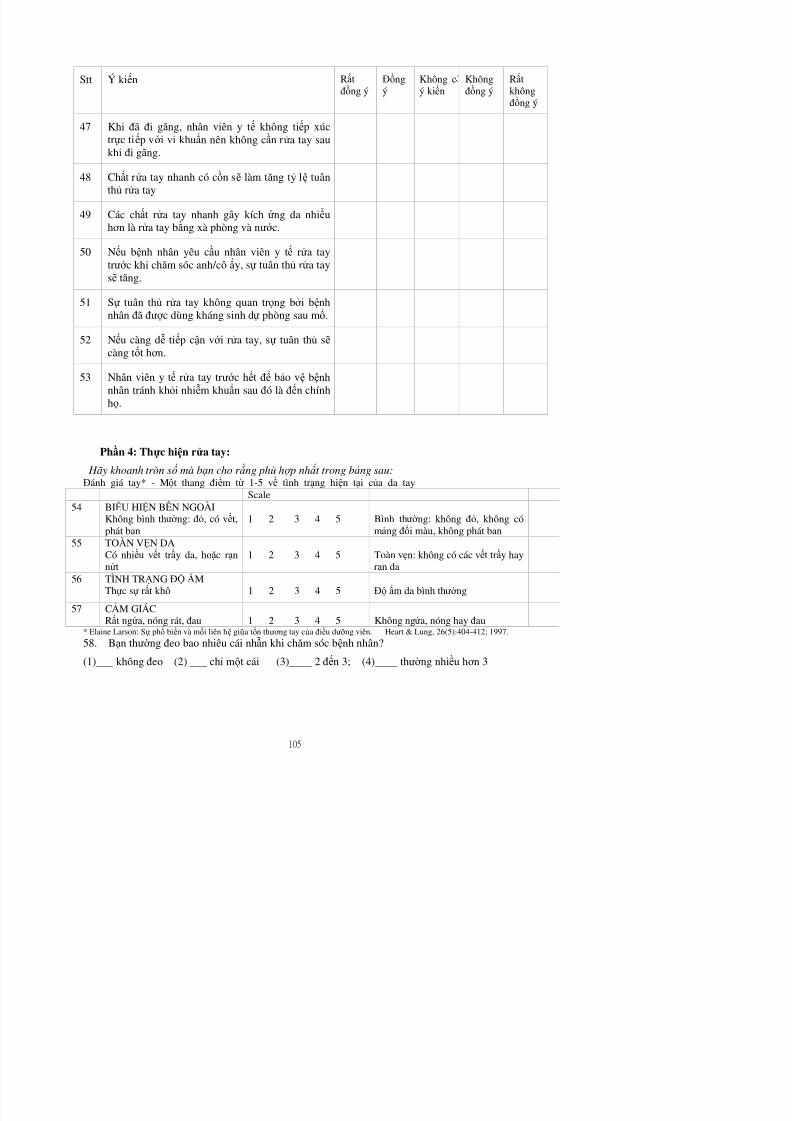
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 119/121
48 Chất rửa tay nhanh có cồn sẽ làm tăng tỷ lệ tuânthủ rửa tay
49 Các chất rửa tay nhanh gây kích ứng da nhiều
hơ n là rửa tay bằng xà phòng và nướ c.
50 Nếu bệnh nhân yêu cầu nhân viên y tế rửa taytrướ c khi chăm sóc anh/cô ấy, sự tuân thủ rửa taysẽ tăng.
51 Sự tuân thủ rửa tay không quan trọng bở i bệnhnhân đã đượ c dùng kháng sinh dự phòng sau mổ.
52 Nếu càng dễ tiếp cận vớ i rửa tay, sự tuân thủ sẽ càng tốt hơ n.
53 Nhân viên y tế rửa tay trướ c hết để bảo vệ bệnhnhân tránh khỏi nhiễm khuẩn sau đó là đến chínhhọ.
Phần 4: Thự c hiện rử a tay:
Hãy khoanh tròn số mà bạn cho r ằ ng phù hợ p nhấ t trong bảng sau:Đánh giá tay* - Một thang điểm từ 1-5 về tình trạng hiện tại của da tay
Scale54 BIỂU HIỆN BÊN NGOÀI
Không bình thườ ng: đỏ, có vết,phát ban
1 2 3 4 5 Bình thườ ng: không đỏ, không cómảng đổi màu, không phát ban
55 TOÀN VẸN DACó nhiều vết trầy da hoặc rạn 1 2 3 4 5 Toàn vẹn: không có các vết trầy hay
Stt Rấtđồng ý
Đồng ý Không cý kiến
Khôngđồng ý
Rấtkhôngđồng ý
Khi bạn không vệ sinh tay (dùng nướ c vàxà phòng hoặc bằng chất rửa tay nhanh)khi đó lý do là gì
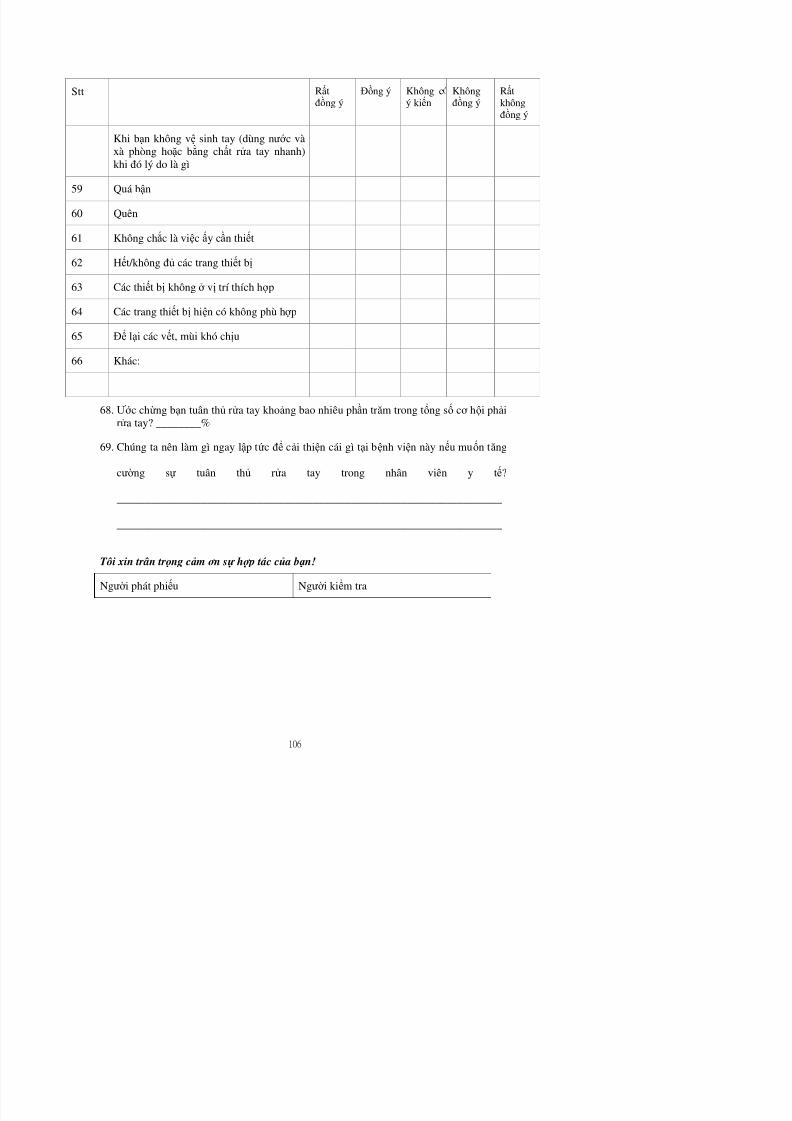
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 120/121
khi đó lý do là gì
59 Quá bận
60 Quên
61 Không chắc là việc ấy cần thiết
62 Hết/không đủ các trang thiết bị
63 Các thiết bị không ở vị trí thích hợ p
64 Các trang thiết bị hiện có không phù hợ p
65 Để lại các vết, mùi khó chịu
66 Khác:
68. Ướ c chừng bạn tuân thủ rửa tay khoảng bao nhiêu phần trăm trong tổng số cơ hội phải
rửa tay? ________%
69. Chúng ta nên làm gì ngay lập tức để cải thiện cái gì tại bệnh viện này nếu muốn tăng
cườ ng sự tuân thủ rửa tay trong nhân viên y tế?
_____________________________________________________________________
_____________________________________________________________________
Appendix 4: Translated version of the Observational form (Vietnamese version)PHIẾU QUAN SÁT HÀNH VI RỬ A TAYBệnh viện:_____________________ Khoa:_____________________________
Buồng bệnh số:______________ TG quan sát: từ___________đến__________
Ca làm việc: ____ sáng; ____chiều; ____ tối. Khoảng cách từ buồng bệnh đến chậu rửa còn hoạt động gần nhất:____ m
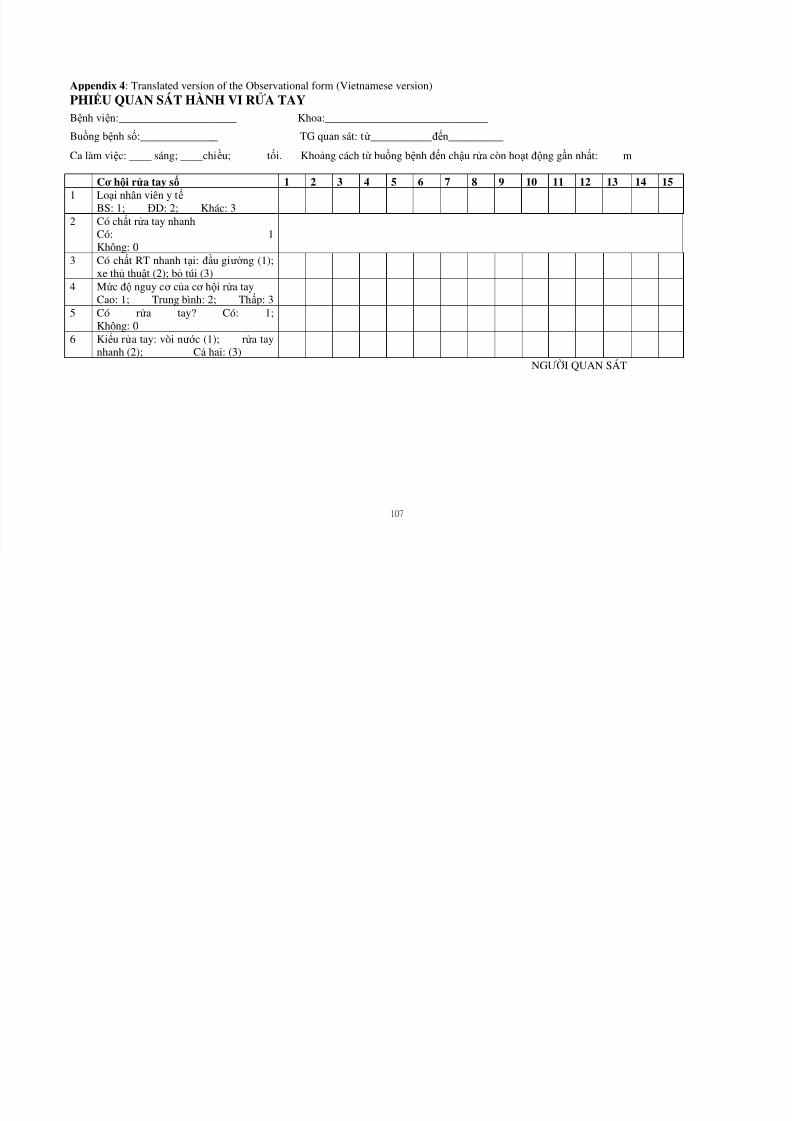
8/9/2019 Pengetahuan Dg Tingkat Pendidikan
http://slidepdf.com/reader/full/pengetahuan-dg-tingkat-pendidikan 121/121
107
Cơ hội rử a tay số 1 2 3 4 5 6 7 8 9 10 11 12 13 14 151 Loại nhân viên y tế
BS: 1; ĐD: 2; Khác: 3
2 Có chất rửa tay nhanhCó: 1Không: 0
3 Có chất RT nhanh tại: đầu giườ ng (1);xe thủ thuật (2); bỏ túi (3)
4 Mức độ nguy cơ của cơ hội rửa tayCao: 1; Trung bình: 2; Thấp: 3
5 Có rửa tay? Có: 1;Không: 0
6 Kiểu rửa tay: vòi nướ c (1); rửa taynhanh (2); Cả hai: (3)
NGƯỜI QUAN SÁT





























