Embed Size (px)
Citation preview
1 Peoples Perspective Research Nepal, draft; 7 February 2011
Peoples Perception Research: Findings of Nepal
7 February 2011

2 Peoples Perspective Research Nepal, draft; 7 February 2011
Executive Summary All the community leaders, regardless of age, gender, caste/ethnicity and urban-rural differences, have been found knowledgeable about the importance of and need for sanitation and hygiene for better health. They have good knowledge about the personal as well as as public health and hygiene including environmental health. They know safe drinking water and sanitation as basic human right. They have pointed out the need for targeting disadvantaged and vulnerable sections of society while rendering drinking water and sanitation services as they are the neediest ones. Based on their existing knowledge regarding sanitation and hygiene, they have reported that people get suffered from several waterborne and other diseases and ailments in the absence of safe drinking water and sanitation and consequently they have been living a worst form of life. They have widely reported diseases like dysentery, diarrhea, skin diseases and allergies, jaundice, acute fevers, pneumonia, cold and cough, headache, eye infections, tuberculosis, polio, hysteria, diabetes, hypertension, stone in gallbladder and kidney, asthma, leprosy, fileria, and digestive disorders. Strong commitment of supporting organizations, active participation of community people, responsiveness to local needs, sense of ownership, accountable and responsive leadership, mutual cooperation and positive attitude toward health and sanitation are the factors that has made many of the sanitation programmes successful. The sanitation programmes having balanced emphasis on both hardware and software components, according to them, are found effective in bringing about desired changes. Moreover, increased self-esteem and dignity of the community people and efforts to personal and community level sanitation and hygiene initiatives have been sustained through increased awareness, need-based activities, and proportionate investment of community people and the external support organizations. According to them, strong and well-designed monitoring of the sanitation initiatives have made these programmes successful. Community leaders' perspectives suggest that support to infrastructure alone is not sufficient to make the sanitation initiatives successful. This is because unless the principles of sanitation and hygiene are translated into real life situations, infrastructure alone cannot be instrumental in changing human behaviour. According to them, irresponsiveness, lethargy, unaccountability and vested interest of local community leaders and the VDC/municipality authorities lead to failure or collapse of sanitation infrastructure. Some community leaders perceive that local government bodies and user committees are not active enough to bring better results even after local people have received external support. In this regard, they have pointed out the need for increasing awareness, ensuring active participation of local people for lobbying and advocacy, enabling environment for investment of community people and the external support organizations, developing systems for reward and punishments, and devising strong participatory monitoring of the sanitation infrastructure development and usage. Community leaders have asked for sanitation programmes to be implemented where such initiatives are absent. They have further suggested first to sensitize community people, support to construct public and private toilets, and engage local people to monitor and maintain the

3 Peoples Perspective Research Nepal, draft; 7 February 2011
initiatives because unless people take ownership of what (support) they receive, success, they insist upon, is not possible because it is community level awareness and participation which can bring sustained change in sanitation and hygiene. Almost all the schools have separate toilets for boys and girls, however, some schools have not paid sufficient attention to the needs of girl students and small children while constructing the toilet. Type of schools in terms of their locality (urban and rural), levels of education they have been providing (primary, secondary and higher secondary) and, ownership and management (public and private) has been found to be associated with the nature of sanitation facilities, especially toilets, they have been providing to the students. Differences in sanitary behavior during menstruation have been reported. This is because menstruation has manifold connotations with culturally embedded symbolic practices. Practices during menstruation are linked with the concepts of purity and pollution as perceived by people and the nature and mode of this perception of purity and pollution varies from society to society. Some mythic superstitions and conservative practices are also associated with menstruation. Desired changes cannot be brought unless these issues are well-addressed while designing, implementing and monitoring the sanitation programmes. Non Governmental Organizations (NGOs) are working effectively and efficiently in sensitizing people about sanitation, and engaging people in infrastructure development and monitoring. In most of the communities where they are working with, the sanitation programmes are found successful due to active participation of community people, responsiveness to local needs, sense of ownership among the local people, accountable and responsive community leadership, mutual cooperation between community and support organizations, and positive attitude toward health and sanitation. In some communities, sanitation infrastructures have been defunct due to a lack of proper maintenance. These systems have become defunct or almost collapsed due to multiple factors such as the lack of sense of ownership among the local people, irresponsiveness, lethargy, unaccountability of the local community leaders and the local governments. However, despite of a few such exceptional cases, almost all the programmes implemented by these NGOs have been reported to be instrumental in bringing about changes in sanitary behaviour of the community people. People have learned to defecate in toilet and keep their environment clean, have learned the essentials of basic sanitation and hygiene and as a result many of the rural and urban communities after support to sanitation have declared their communities open defecation-free places. They have learned the importance of safe drinking water and have realized the importance of collective action to manage water as 'common pool resources'. People are being relieved from life-threating waterborne diseases and other health problems. It has also impacted on their household economy as, compared to earlier days, they have to spend less in health check-ups, diagnosis, treatment and drugs. The number of days children have been able to attend their schools have been increased and similarly, the number of working days for the parents has also increased which has greater economic significance. Another major impact of sanitation programme can be traced in the overall personality of the people who use toilet, drink safe water and keep themselves tidy and clean. All the community leaders have expressed their common feelings that improved sanitation condition in their houses and in their communities have increased their self-esteem and social dignity as some of the communities and community leaders have become role-models for other communities.

4 Peoples Perspective Research Nepal, draft; 7 February 2011
The sociocultural factor, as a complex set of social values and norms, perceptions, and wide range of context-bound personal and group behaviour and lifestyles reflected in fooding, clothing, washing, bathing, defecating, etc. has been affecting the success and failure of the sanitation programme. The economic or financial factors play decisive role in the success and failure of the sanitation programme as people who are below the poverty line are unable themselves to construct toilet and drainage systems. They cannot afford for installing tube-wells. VDCs and municipalities also do not give priority for their problems and do not disburse sufficient resources/funds. The situation points out the need for revising policy and guidelines so as to mainstream water, sanitation and hygiene as basic right of people. The sociopolitical environment are not also favorable in this regard. Political leaders and their all-party mechanisms (sarbadaliya samyantra) pay attention to disbursing heavy budgets on road construction and other physical infrastructure due to their economic and other vested political interests. The external and internal political/ideological division of their mindsets have also limited the scope of collective actions for fulfilling common interest like sanitatiion. The institutional factors like organizational support, social mobilization and community participation through user committee, and networking and linkages play vital role for the successful completion of the sanitation system, its operation and maintenance and sustained ownership. Whereas the lack of proper identification of local people's needs, lack of social mobilization, lack of accountability and responsiveness of local leaders, increased dependency syndrome among the community people, lack of ownership of the sanitation infrastructure, and lack of effective linkage and coordination between concerned stakeholders have made some sanitation systems useless or defunct. Similarly, the financial factors like fund disbursement, and transparency in the use of funds and resources have serious implication in successful completion and maintenance of the sanitation system. In the communities where user committees are not transparent and do not involve public auditing/hearing, the funds have been reported to be abused. Despite being aware of the need and significance, a considerable number of men and women are somehow reluctant and not proactive for taking sanitary initiatives themselves. The root of the problem is dependency syndrome. Putting another way, the inhabitants expect some sort of initiations from government line agencies and I/NGOs in this regard. Some view that it is incapability of the community leader. In the communities where people are sensitized and mobilized by NGO, people have been actively cooperating with the NGOs and other actors working in water and sanitation sector. They possess positive attitude towards the role of multiple actors for water and sanitation related activities, and they have been maintaining both the private and public sanitary systems well. According to the community leaders, constructive dialogue, cooperation and collaboration between and among different stakeholders are needed for monitoring of sanitation initiatives at local level. Though some civil society organizations like CFUG, local clubs, women groups are engaged in water and sanitation related activities, there are a number of problems associated with monitoring of operation of the water and sanitation systems.

5 Peoples Perspective Research Nepal, draft; 7 February 2011
Table of Contents Executive Summary ...................................................................................................................... 2 1. Introduction of Peoples Perception Research ..................................................................... 7
1.1 Background ........................................................................................................................... 7
1.2 Objectives .............................................................................................................................. 8
1.3 Approach and Methodology .................................................................................................. 8 2. Overivew of Sanitation and Water Sector in Nepal ............................................................ 9
2.1. Water and sanitation coverage ............................................................................................. 9
2.2. Institutional mechanism ..................................................................................................... 11
2.3. Sector financing trends ....................................................................................................... 12 3. Highlights of Key Issues Emerging from Narrative ......................................................... 13
3.1 Understanding about Sanitation .......................................................................................... 13
3.2 Understanding about Water and Sanitation as Human Rights ............................................ 13
3.3 Understanding about Basic Hygiene ................................................................................... 14
3.4 Common Diseases in the Area/Locality .............................................................................. 14
3.5 Status of Sanitation Infrastructure and Usage ..................................................................... 15
3.6 Status of Toilet Facilities in the Schools ............................................................................. 17
3.7 Practices during Menstruation ............................................................................................. 17
3.8 Sanitation Programmes in the Communities ....................................................................... 18
3.9 Impacts of Sanitation Programmes in Everyday Life ......................................................... 18
3.10 Factors Affecting the Success and Failure of the Sanitation Programme ......................... 19
3.11 Factors Contributing to Function or Dysfunction of Sanitation System ........................... 20
3.12 Problems Faced in Absence of Sanitation ......................................................................... 20
3.13 Institutional role and arrangements ................................................................................... 21
3.14 Peoples participation ......................................................................................................... 22
3.15 Monitoring at local level ................................................................................................... 23
3.16 Availability of resources, targeting and use ..................................................................... 23 Annex - 1: Narratives of Community Leaders' Voices ............................................................ 24
Representative Case 1: Poverty and Innocence Matter ............................................................. 25
Representative Case 2: People Need Helping Hands ................................................................ 25
Representative Case 3: Local Level Unity and Initiation Ensures External Support................ 26
Representative Case 4: Relevance, Effectiveness, Efficiency and Sustainability Matter ......... 26
Representative Case 5: Change Is Really Possible ................................................................... 27
Representative Case 6: Way Out From Dependency Syndrome............................................... 29
Representative Case 7: Need for a Joint Effort ......................................................................... 30
Representative Case 8: Sanitary Problems Persist Even After the Intervention ....................... 31
Representative Case 9: External Support is Not Sufficient ...................................................... 32
Representative Case 10: Perceptions of differently abled people ............................................ 33
Representative Case 11: Community People Are Really Cooperative ..................................... 33

6 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 12: The Politics and Pollution in the Public Toilet .................................. 34
Representative Case 13: Accountability, Participation and Commitment Matter .................... 34
Representative Case 14: Success is a Common End ................................................................. 35
Representative Case 15: Who is Responsible, Local People or Service Provider? .................. 35
Representative Case 16: Ignorance of the Indigenous Practices May Result in Failure ........... 36
Representative Case 17: Enlightened by NGO's Programme ................................................... 37
Representative Case 18: Awareness Campaigns Are Essential ................................................ 39
Representative Case 19: Some Sanitation Programmes Are Partially Successful .................... 39
Representative Case 20: Local Leaders' Role Is Crucial........................................................... 40
Representative Case 21: Female Health Volunteers Also Contribute....................................... 41
Representative Case 22: People's Participation Is Gradual Process .......................................... 41 Annex - 2: Guiding Notes for Information Collection ............................................................. 42

7 Peoples Perspective Research Nepal, draft; 7 February 2011
1. Introduction of Peoples Perception Research
1.1 Background Human development and dignified lives are possible only with access to safe water, adequate sanitation and improved hygiene. It is estimated that 1.027 billion (64%) out of 1.595 billion people in South Asia are deprived from improved sanitation. The story does not end here as almost two thirds of the population in the region defecate in open spaces and are exposed to severe health hazard risks as well as seen as the pollutants of environmental sanitation. Urban and rural divides are prominent in sanitation access. The disparity is high in countries like Pakistan, Bhutan, India, Afghanistan and Nepal. The slow pace of progress coupled with geographical and regional disparity is a huge challenge in the region.
Graph 1: Location of 1.027 billion people not using improved sanitation (millions)1
Deprivation of sanitation access has affected poor people in economic aspect both in terms of health investment as well as their inability to earn because of illness caused by water borne diseases. It has been estimated that at any one time, more than half of the poor in the developing world are ill from causes related to hygiene, sanitation and water supply2. It is revealed that economic return from every US $ 1 invested in water and sanitation is estimated at US$ 93. It has been estimated that in world 443 million school days are lost each year due to water borne diseases.4 UK DFID study revealed that 11% more girls attend school when sanitation is available. It is also estimated that 53% adolescent school girls absent schools during menstruation period. There is improvement in school attendance of girls as it is mainly women and girls who shoulder most water collecting burden and walk an average of 6 km a day. 1 JMP 2010. UNICEF/WHO 2 Water Supply and Sanitation Collaborative Council (WSSCC). 2008. A Guide to Investigating One of the Biggest Scandals of the Last 50 Years. 3 WHO.2008. Sanitation generates economic benefits, fact sheet. http://esa.un.org/iys/docs/2%20fact-sheet_economic%20benefits.pdf 4 http://www.wateraid.org/uk/what_we_do/statistics/default.asp

8 Peoples Perspective Research Nepal, draft; 7 February 2011
There has been a slow progress in the region in terms of increasing access of sanitation and people are forced to lead lives without dignity as they have to defecate openly each morning and have to suffer and even die from preventable diseases caused due to inadequate sanitation and safe drinking water. MDG target of achieving access of sanitation to half of the population seemed far-fetched dream for most of the countries in South Asia.
Graph 2: South Asia in journey of meeting MDG Target 5
South Asian Conference on Sanitation (SACOSAN) has emerged as a strong political avenue for increasing political commitment and actions to enhance sanitation progress in the region. Journey of promoting sanitation access has encountered both success and failures. In order to provide people insights of these sanitation success and failures the Peoples Perspective Research has been conceptualized.
1.2 Objectives The main objective of peoples perception research is to analyze peoples impression and observation on overall scenario of sanitation progress. The research is aimed to achieve following objectives:
• Highlight factors which have contributed for success and failure in sanitation and hygiene improvement, from peoples’ perspective
• Identify key challenges/issues faced in sustainable sanitation in the south Asia region • Input to the pre SACOSAN 4 CSO meet in Colombo in 2011 and for the official
SACOSAN 4 meet thereafter
1.3 Approach and Methodology The peoples perception research is a qualitative research based on 128 case studies collected from 17 districts of Nepal. Interview method was applied to obtain primary information from selected sites representing both rural and urban areas. Besdies, the site selection team have paid attenttion to following three major categories:
• Successful sanitation efforts • Failure interventions of sanitation or sanitation effort success follwed by relapse in
increased open defecation or in case of urban dysfunctional sanitation system • No sanitation efforts/interventions
5 Sanitation Crisis Continues in South Asia, WaterAid 2010

9 Peoples Perspective Research Nepal, draft; 7 February 2011
The respondents for the study were identified in consultation with partner organizations and individuals working in/near by stations so that proper channel of information is maintained. Besides, as per the guiding note of the research socio-demographic factors like age group, gender, rurality and urbanity, social stratifications in terms of caste/ethnicity, inclusion of differently able people and other excluded groups (HIV, etc) were also considered while selecting the cases.
Orientation to enumerators of the case study collection was based on the guiding notes prepared in Nepali lanaguage to ease information collection process. The questionnaires were further contextualized in Nepali for increasing efficacy of information collection. Besides, case study format was also developed to maintain uniformity of the cases and easing compilation of the information. The guiding note also provided information on potential sources of information collection besides interview questionnaires of the selected community member. Collective effort was adopted in collecting the information as FEDWASUN and NEWAH were responsible for collecting rural cases whereas Lumanti was responsible in collecting urban cases. A national consultant was hired to compile and analyze questioannires and narratives for producing a national report with best representative case studies.
2. Overivew of Sanitation and Water Sector in Nepal
2.1. Water and sanitation coverage Access to safe drinking water and sanitation is a basic fundamental right that paves path for sustainable social and economic development. Recent government data revealed that still five and half million Nepalis out of total 28 million are deprived from safe drinking water access. On contrary, the deprived population figure is estimated to be 13 million if the functional water coverage of 53% is considered.
Scenario of sanitation access is further worse as almost half of the total population i.e. sixteen million Nepalis are deprived from sanitation access. There are 3915 Village Development Committees (VDCs) that is lower level of local governance, out of it only 125 VDCs are declared open defecation free. It has been estimated that 10,500 children below five years die annually due to diseases caused due to inadequate access to safe drinking water and sanitation. However, if JMP 2010 figure is considered then the outstanding population having no access to sanitation right is nearly 18 million.
It is estimated that richest people are 8 times more likely to have access to sanitation than poor people. On the other hand, richest people are 13 times more likely to have access to safe drinking water. Therefore, it can be stated that deprivation of sanitation and water access affects dignity of poor people.
It is found that 88% of cases of diarrhea worldwide are attributable to unsafe water, inadequate sanitation or insufficient hygiene.6 It is the second leading cause of child mortality in Nepal. WASH related diseases attributed large section of deaths and disability that is evident from Table
6 Water Supply and Sanitation Collaborative Council (WSSCC). 2008. A Guide to Investigating One of the Biggest Scandals of the Last 50 Years.

10 Peoples Perspective Research Nepal, draft; 7 February 2011
1. It has been estimated that the country has to bear annual death of 10,500 children below 5 years due to water borne diseases7.
Table 1: Statistics on death and disability from WASH related diseases8
Total WaSH-related deaths or DALYs DEATHS DALY
Nepal 17,900 (7.5%) 835,000 (10.7%) SEAR-D Sub-region 681,231 (5.4%) 30,571,650 (8.2%) World 2,461,811 (8.4%) 103,232,988 (6.8%)
Onset of summer brings alertness in the country to minimize diarrhoeal outbreaks. The disastrous outbreak on 2009 killed more than 300 people and adversely affected 46,000 Nepalis dwelling in far and mid western parts having lower sanitation coverage. The linkage of sanitation and diarrhoea incident is clear from the graph 3.
Graph 3: Sanitation coverage and incidence of diarrhoea9 Graph 4: Prevention strategies of Diarrhoea10
It has been proved that simple act of handwashing can prevent diarrhoeal incident by 45% followed by sanitation access that can prevent the killer disease by 36% followed by hygiene education.
7 Nepal Demographic Health Survey.2006????? 8 WHO.2008 9 DHS and NMIP, 2006 10 Esrey SA, et al. Bulletin, WHO :609-21.

11 Peoples Perspective Research Nepal, draft; 7 February 2011
2.2. Institutional mechanism Water and sanitation services in Nepal are provided by many agencies. The MoF allocates public sector finance to the sectoral ministries. MoPPW is the lead sector ministry. Working with the NPC, MoPPW has the responsibility to formulate policies, plans and strategies. It has two operational arms: the Department of Water Supply and Sewerage (DWSS) and the Nepal Water Supply and Sewerage Corporation (NWSC). DWSS is responsible for water supplies in small towns and rural areas. The 2004 RWSS policy sought to shift implementation responsibility to local authorities and communities and restructure DWSS’s role to that of facilitation and oversight. In practice, this has not been implemented fully. A proposal supported by ADB has outlined specific strategies for DWSS to take on a facilitating, monitoring, policy advisory role and restructure itself with a reform unit to make this shift.
The Local Self Governance Act (1999) provides for local authorities to plan and manage WSS. The Ministry of Local Development (MLD) is responsible for supporting District Development Committees (DDCs) and Village Development Committees (VDCs) to develop small water supplies and sanitation. MLD has established District Technical Offices (DTOs) to provide technical support to local authorities. However the armed conflict has significantly affected the operations of many rural local authorities and prevented the appointment of locally elected representatives into local government bodies. Community management is the preferred means of rural water supply service management, but studies show that there are major limitations to its effectiveness: both technically and financially. The breakdown rate remains high and community-level financial management remains weak.
NWSC is responsible for water supply, sewerage and drainage services in main metropolitan municipalities and 23 sub-metropolitan areas outside the Kathmandu valley. The Kathmandu Valley water services are now under the Kathmandu Valley Water Supply Management Board and operated by Kathmandu Upatkya Khanepani Limited (KUKL) — a company established under a public private partnership. NWSC has been unable to manage services effectively and will hand over its sector assets to municipalities. Other major stakeholders in the sector include: WB that supports the rural sector through the semiautonomous Fund Board (RWSSFDB2) mentioned above, and the ADB that has invested over $300 m. in urban and rural water projects in Nepal since 1984 and been a significant partner to DWSS and MoPPW in national sector policy development. It presently supports DWSS implementation of a Community Based Water Supply and Sanitation Project (CBWSSP) and a Secondary Towns Urban Environmental Improvement Project. These two projects are improving services in small towns and urban communities and assisting DWSS to undertake further reforms. The investment banks/ donors (ADB, WB) also support a major source replenishment plan ($500 m.) developed for the Kathmandu valley, namely the Melamchi and Kathmandu Urban Water Management Projects. Progress is slow and the projects had to be reorganized due to resistance to private sector involvement.

12 Peoples Perspective Research Nepal, draft; 7 February 2011
2.3. Sector financing trends During four decades starting from 1970’s to fiscal year 2010/011, Nepal government had allocated about Rs. 77 billion. At the present population size, per capita budget allocation is 2700 (approx). However, if discounted Melamchi and institutional reform total budget allocation in four decade is about 43 billion rupees, which implies per capita budget allocation about Rs, 1,700. 11
Recent national budget allocation of FY:2010/11 for the sector is Rs. 9.35 billion (USD 130 million). It should be noted that the budget without Melamchi and sector reforms is 6 billion. But a trend analysis of the budget of the last four years shows that the budget allocation growth rate has actually gone down this year when compared to that for sectors such as education and health. On contrary, sanitation stand alone budget has seen dramatic increase of 21 crore in comparison to 6.2 crore expense this year.
Graph 5: Comparative analysis of social sector budget12 Ministry of Physical Planning and Works continues to lead on spending in the sector with 75% of sectoral fund. There is a decreasing dependency in the sectoral budget. It is evident from the fact that there is 7% more increment in the government committed funding than previous year. It can be something that is inspiring for water, sanitation and hygiene advocates. The budget speech has mentioned that girls’ toilets in each community school will be made mandatory. It is anticipated that the policy will not be faded as “One House One Toilet Policy” endorsed in last year’s budget speech. Nepal can be a model country by show casing girl friendly toilets in each community schools so that these children should not miss their classes during menstruation and can fearlessly drink water without thinking of emabarssment of open urination. Not every district is equal when it comes to needing the most of water and sanitation funds. Districts such as Bajura, Bajhang, Salyan, Darchula, Mahottari and Sarlahi are way behind other districts in terms of their access to sanitation. From the point of view of equity, these districts
11 Draft Global Flagship Report, Nepal section, WaterAid Nepal.2011 12 Budget speech annexes. 2010/11http://www.mof.gov.np/publication/speech/2010_1/pdf/annex_english.pdf

13 Peoples Perspective Research Nepal, draft; 7 February 2011
should be given a high priority so that they address their sanitation issues before they start showing good results in health, educationa and livelihood sectors.
3. Highlights of Key Issues Emerging from Narrative This section is based on the narratives of community leaders regarding the institutional role and arranegements, people's participation in water and sanitation related activities, mechanisms of monitoring at local level and their effectiveness and effeciency, and the availability, targeting and use of resources.
3.1 Understanding about Sanitation Regardless of gender, caste/ethnicity and urban-rural differences, all the community leaders have been found quite knowledgeable regarding the importance of and need for sanitation and hygiene for better health. They have good knowledge about the personal as well as as public health and hygiene. Some of them have also shown "environmental kinship" through their concern toward the environmental health. In other words, they can think of health of other living creatures, and biotic and abiotic thing around us. However, educational attainment has positive correlation with the knowledge regarding sanitation, i.e. higher the educational status community leaders have possessed, better the the knowledge regarding sanitation and related issues they do have.
3.2 Understanding about Water and Sanitation as Human Rights Community leaders have expressed their views in their everyday simple language and according to them; they have nothing to do with the grand narratives constructed by experts and professionals, and big-people (specifically ministers and top level bureaucrats) gathering in national and international seminars and conventions. They simply know that they have to drink safe water and keep themselves healthy and hygienic so that they can live easily. Almost all the community leaders are quite aware about people's right to safe drinking water and sanitation. They know human being, like other biotic elements of the nature, cannot live without water. In the absence of safe drinking water and sanitation, people get attacked by various diseases and ailments, which ultimately lead to worst form of life. Some community leaders have spelled out that declaration and documentation of the right to safe drinking water and sanitation is worthless unless it is translated into grassroots reality through effective, efficient and sustainable programmes. They have also pointed out the need for targeting disadvantaged and vulnerable sections of society while rendering drinking water and sanitation services as they are most needy ones who themselves cannot afford to physical infrastructure due to extreme poverty. In this case, some community leaders who have obtained higher education, and those who have been representing the areas where support agencies have worked for sanitation have been found more knowledgeable regarding the declaration made by UN General Assembly about Water and Sanitation as Human Rights and endorsement of the same by the government of Nepal.

14 Peoples Perspective Research Nepal, draft; 7 February 2011
3.3 Understanding about Basic Hygiene Almost all the community leaders are found knowledgeable about basic hygiene. Basic hygiene, according to them, helps keep them healthy and helps prevent from diseases. Use of safe drinking water and sanitary precautions keeps them away from various water-borne diseases like typhoid, jaundice, dysentery, diarrhea, etc. Besides, they have mentioned that basic hygiene is equally important as it affects their economic life, educational attainment, and dignified social life. They have further expressed that basic hygiene and education are interrelated as one affects another. This is because education imparts them knowledge about basic sanitation and hygiene and makes them aware of the ways they can keep themselves healthy through basic hygiene. Similarly, if one is quite aware of basic hygiene becomes healthy and can pursue better education physically and mentally. The community leaders perceive that basic hygiene further helps alleviate their poverty because they can get involved in income generating activities if they are healthy. If they are unhealthy and get diseased, they have to spend a lot of money for treatments and the money that is spent on treatments can be saved if they become healthy through sanitation and hygiene as preventive aspects of human health. Basic hygiene, as they perceive, helps promote their self-esteem as one who is tidy, clean and healthy is respected in society and s/he becomes a role model in society. They have further expressed that those who do not have toilet find themselves inferior to those using toilet.
3.4 Common Diseases in the Area/Locality During study, a number of health problems have been reported. These health problems, both acute and chronic ones, have some spatial significance. For example, diabetes and hypertensions have been widely reported from urban places whereas dysentery, diarrhea and other waterborne diseases are reported more from rural areas. More specifically, another example of place specific health problems is that most of the community leaders of Doti district have mentioned pneumonia among the children. Waterborne diseases like dysentery, diarrhea, skin diseases and allergies, jaundice, acute fevers have been reported widely in almost all places. Pneumonia, Cold and cough, headache, eye infections, tuberculosis, polio, hysteria, diabetes, hypertension, stone in gallbladder and kidney, asthma, leprosy, elephantitis, digestive disorders are the other common health problems reported by the community leaders. It has been also noticed that the educated male community leaders of rural areas and all the community leaders from urban areas can tell more types of specific diseases by their common name (both Nepali and English).

15 Peoples Perspective Research Nepal, draft; 7 February 2011
3.5 Status of Sanitation Infrastructure and Usage Methodologically, the research was designed to represent all types of sanitary situations in terms of infrastructure and usage. If we analyze the scenario in following four different types of status:
• Sanitation efforts made, infrastructure developed but have not been successful • Sanitation efforts made, infrastructure developed and have been successful • Santiation efforts made, infrastructure developed and have been successful but followed
by a relapse in increased open defecation or in case of urban these are dysfunctional. • No sanitation efforts and no sanitation infrastructure developed
In the first category, responses obtained from the community leaders suggests that support to infrastructure alone is not sufficient to make the sanitation initiatives successful. This is because unless sanitation and hygiene is practiced in real life, infrastructure cannot alone be instrumental in changing human behaviour. For example, people in some communities have not paid sufficient attention toward the sanitation of public places. Regarding sanitary behavior during menstruation, the girl students have been facing problems due to lack of convenient toilet facilities in schools. Some community leaders perceive that local bodies and user committees are not active enough to bring better results even after local people have received external support. Some petulant personalities in the communities motivated by pride and prejudice misinterpret the programme and create hurdles and do not cooperate with the majority of poor and disadvantaged groups. Such people do not cooperate with the project and even do not agree to allow their land for drainage. Despite of series of meetings, dialogues and protests, the task of constructing drainage, water supplies and toilet construction become incomplete. Weaker attention on community mobilization and management is regarded as one of the reasons of failure and continued efforts of sanitation. Due to a lack of clear laws and regulations, local people keep on waiting for formal and legal action against those petulant persons. This indicates that these persons who possess knowledge about sanitation do not ensure that they possess better attitude and practice better and physical infrastructure alone cannot support. Community leaders, in such conditions, have also pointed out the need for active participation of local people for lobbying, advocacy, social punishment and strong monitoring of the sanitation infrastructure development and usage. In the second category, community leaders perceive that strong commitment of supporting organizations, active participation of community people, responsiveness to local needs, sense of ownership, accountable and responsive leadership, mutual cooperation and positive attitude toward health and sanitation were the factors that makes sanitation program successful. The sanitation programmes embedded with both hardware and software components, according to them, have helped increase self-esteem and dignity of the community people, and have decreased the rate of absence of students in schools. In their opinion, efforts to personal and community level sanitation and hygiene initiatives can be sustained through increased awareness, need-based activities, and proportionate investment of community people and the external support organizations. According to them, strong and well-designed monitoring of community initiatives and infrastructures are essential for sustained benefits from sanitation initiatives. In the third category, urban life is somewhat different that of the rural ones. It is often counter-successful to take one particular hamlet as a single project site to work with/for. This is because infrastructures like drainage and public toilets might be common to many of the streets/hamlets within the municipality area. In some places, as reported by the community leaders, public places

16 Peoples Perspective Research Nepal, draft; 7 February 2011
are highly polluted though almost all the households have private toilets. Such conditions are due to the sewage coming from other parts of the municipality. According to them, some households still defecate in the open spaces, especially in the areas resided by landless squatter/slums. According to the community leaders, Drinking Water and Corporation and the municipality have not supplied drinking water in their communities and the people are compelled to use tube-well and the water drink using these tube-wells is not safe and consequently, they are not able to enjoy basic human right to safe drinking water and sanitation. Though people have been paying Rs. 5-10 per week for the so-called maintenance of public toilet, for example in Hadtali Hat Tole of Biratnagat Municipality-19, the toilet has not been maintained and the toilet is almost defunct. In the past, such public toilets were being used by almost all the households when number of households were also lesser than present and the local households at that time did not have private toilet. Now at present, though almost all the households have toilets, many people, especially those who are landless and do not have private toilet, have still been using these public toilets. Even after support made from different agencies, renovation of these public toilet has remained incomplete. According to the community leaders, such a failure or collapse of infrastructure is due to the irresponsiveness, lethargy, unaccountability and vested interest of local community leaders and the municipality authorities. In their view, efforts to community level sanitation initiatives can be sustained through increased awareness, local good governance, and proportionate investment of community people and the external support organizations. In the fourth category where sanitation initiatives have not been intervened, some well-off people and people who are well aware of the need for and importance of sanitation and hygiene have been using toilets privately and take all precautionary measures to be healthy through proper sanitary efforts. But either due to a lack of awareness of the importance of sanitation or owing to the lack of land for making private toilet, or due to lack of affordability to construct toilet many of the squatter/slums living in urban areas and local residents of rural communities have been defecating in open spaces. Many of these people do not purify drinking water properly and do not wash hands with soap. Women use to put cloths used during menstruation in cool and dark corners which is not safer in terms of their health. Majority of the girls do not go to schools during menstruation period. Most of the community leaders of such communities show their dissatisfaction regarding the sanitary condition of their community. According to them, children are victimized most due to the lack of proper sanitation and get suffered from diseases like dysentery, diarrhea, pneumonia, cholera, meningitis, etc. They have asked for a sanitation programme which would first sensitize community people, support to construct public and private toilets, and engage local people to monitor and maintain the initiatives because unless people take ownership of what (support) they receive, success, they insist upon, is not possible because it is community level awareness and participation which can bring sustained change in sanitation and hygiene.

17 Peoples Perspective Research Nepal, draft; 7 February 2011
3.6 Status of Toilet Facilities in the Schools In almost all the places, both urban and rural, schools have managed toilets for the students. Almost all these schools have separate toilets for boys and girls. According to the community leaders, some schools have not paid sufficient attention to the needs of small children while constructing the toilet. However, type of schools in terms of their locality (urban and rural), levels of education they have been providing (primary, secondary and higher secondary) and, ownership and management (public and private) has been found to be associated with the nature of sanitation facilities, especially toilets, they have been providing to the students. Some schools in rural areas do have toilet but these are in poor condition. It does not mean that toilets in the schools of urban areas are in better condition. Due to lack of sufficient running water, condition of toilets in these schools is even poorer than that of rural ones. A few numbers of public schools have good toilet facilities but the toilets in majority of the privately operated schools have better. Community leaders' response has also revealed that the secondary and higher secondary schools have better toilets than in primary schools. In some places, they have also reported that toilets in some public schools which were operated well in the past have now become defunct due to irresponsiveness of the school administration.
3.7 Practices during Menstruation Menstruation has manifold symbolic connotations with culturally embedded practices. Practices during menstruation are linked with the concepts of purity and pollution as perceived by people and the nature and mode of this perception of purity and pollution varies from society to society. This is why practices related to sanitation and hygiene and the way family members, kin group members and larger society treats women during menstruation vary from one cultural group to the other. As Nepali society is a composite of a number of cultural groups, there are varieties of sanitary practices during menstruation. One of the dalit community leaders of Doti district mentioned that women are still put in isolation in animal-sheds, also widely known as during menstruation which is also widely known as chhaupadi system. Women cannot enter into their house, cannot touch other people, water and utensils and they are prone to vulnerability in terms of their health due to poor sanitation in the animal-sheds. Women are deprived of nutritious food and they are not allowed to drink milk. There are some superstitions associated with such practice. For example, if the women during menstruation enter the home and touch other members, utensils and water, then the spirit of ancestors and gods and goddesses will get angry and consequently they have to bear risks. However, women who stay in animal-sheds take daily bath during menstruation. Community leaders are aware that such rigid practices which are against the women's right to freedom and sanitation are not observed in other communities like in the Tharu community. However, in Hindu male-dominated caste groups like Brahman, Chhetri and dalit, women are found suffered from untouchability during menstruation period, which is practiced rigidly in rural communities than in urban communities.

18 Peoples Perspective Research Nepal, draft; 7 February 2011
3.8 Sanitation Programmes in the Communities Similar to the conditions presented in section 3.5, sanitation programmes in the communities can be categorized into varieties of situations. Some communities do not have any sanitation infrastructure like toilet and provision for safe drinking water. People defecate in open spaces. In most of the communities where better sanitation conditions have been reported, are found supported by governmental and non-governmental organizations. A number of cases reported from different parts of the country reveal that sanitation programmes have been effective in sensitizing people about sanitation, engaging people in infrastructure development and monitoring. In these communities, the sanitation programmes are found successful due to active participation of community people, responsiveness to local needs, sense of ownership among the local people, accountable and responsive community leadership, mutual cooperation between community and support organizations, and positive attitude toward health and sanitation. In some communities, sanitation infrastructures have been defunct due to a lack of proper maintenance. These systems have become defunct or almost collapsed due to multiple factors such as the lack of sense of ownership among the local people, irresponsiveness, lethargy, unaccountability of the local community leaders and the municipality authorities.
3.9 Impacts of Sanitation Programmes in Everyday Life Sanitation programmes implemented have been found focusing on promoting awareness among the community people, supporting communities to develop infrastructure like toilets, drainage, tube-wells and water supply. Besides some exceptional cases, almost all these programmes have been reported to be instrumental in bringing about changes in sanitary behaviour of the community people. People have learned to defecate in toilet and keep their environment clean. They have learned the essentials of basic sanitation and hygiene. Many of the rural and urban communities after support to sanitation have declared their communities open defecation-free places. They have learned the importance of safe drinking water and consequently they have started to purify using various methods. They have realized the importance of collective action to manage 'water as common pool resources' and have begun to harvest purposelessly running water for multiple uses. They have been also made aware about child health. They have begun to manage solid waste using improved methods. Some communities have begun microfinance operations through saving/credit groups. Community leader's voices reveal that sanitation programmes have impacted on various aspects of individual and social lives. The main and long-lasting impact of the programmes is that people have learned to live a hygienic life through improved sanitary condition. Their children have become more healthy and the occurrence of waterborne diseases has been declined as compared to previous years when people used to defecate in open spaces and they were less aware of the need for and importance of sanitation. People's perception and behaviour during menstruation has also been reported to be changed due to increased awareness. One of the major impacts of the sanitation programmes, however indirect and implict, is that people are being relieved from life-threating waterborne diseases and other health problems. It

19 Peoples Perspective Research Nepal, draft; 7 February 2011
has also impacted on their household economy as they have to spend less in health check-ups, diagnosis, treatment and drugs. The number of days children have been able to attend their schools have been increased and similarly, the number of working days for the parents has also increased which has greater economic significance. Another major impact of sanitation programme can be traced in the overall personality of the people who use toilet, drink safe water and keep themselves tidy and clean. All the community leaders have expressed their common feelings that improved sanitation condition in their houses and in their communities have increased their self-esteem and social dignity.
3.10 Factors Affecting the Success and Failure of the Sanitation Programme Narratives collected from the community leaders shows that there are a number of factors affecting the success and failure of sanitation programmes. Some broader factors are sociocultural, socioeconomic, and sociopolitical ones. These factors are again associated with the organizational/institutional, financial, technical and attitudinal aspects of the prorgammes. The sociocultural factor that affects sanitation programmes is a combination of social values and norms, perceptions, and wide range of context-bound personal and group behaviour reflected in everyday practices related to the everyday lifestyles manifested in fooding, clothing, washing, bathing, defecating and, disposal and use of human and animal excreta. It is harder to change people's behaviours which are culturally embedded and sanctioned. For instance, our efforts to bring changes in chaupadi system takes a long time. Community people are still reluctant and hesitant to discuss the socially prescribed human behaviour deliberately. The economic or financial factors play decisive role in the success and failure of the sanitation programme. In most of the communities where people are below the poverty line are unable themselves to construct toilet and drainage systems. They cannot afford for installing tube-wells. VDCs and municipalities also do not give priority for their problems and do not disburse sufficient resources/funds. The sociopolitical environment in rural as well as urban communities are not also favorable in this regard. Political leaders and their all-party mechanisms (sarbadaliya samyantra) pay attention to disbursing heavy budgets on road construction and other physical infrastructure due to their economic and other vested political interests can be fulfilled. Local people in the communities, except in a few cases, are not organized and they cannot claim their rights. The external and internal political/ideological division of their mindsets have limited the scope of collective actions for fulfilling common interest like sanitatiion.

20 Peoples Perspective Research Nepal, draft; 7 February 2011
3.11 Factors Contributing to Function or Dysfunction of Sanitation System As discussed above in section 3.10, a number of technical, organizational/institutional, financial and attitudinal factors are found associated with the function and dysfunction of sanitation system. The community leaders have reported wide range of cases/narratives that reflect these factors. The institutional factors are the combination of internal and external conditions that comprises organizational support, social mobilization and its repercussions on the public awareness and community participation, user committee formation and functioning, networking and linkages leading to cooperation, and definition of specific roles each stakeholder has to play for the successful completion of the sanitation system, its operation and maintenance and sustained ownership of the communities and individual households. All these factors have been found playing crucial role in making the sanitation systems function well. Contrary to this, the lack of proper identification of local people's needs, lack of social effective mobilization of the community people, lack of accountability and responsiveness of local leaders, increased dependency syndrome among the community people and lack of ownership of the sanitation infrastructure, and lack of effective linkage and coordination between concerned stakeholders have made the sanitation systems useless or defunct. The financial factor is also associated with the functioning of the systems. Community leaders' voices have clearly pointed out that better transparency in the use of funds and resources has led to the successful completion and maintenance of the sanitation system. In the communities where user committees are not transparent and do not involve public auditing/hearing, the funds have been reported to be abused. In the communities where the partner NGOs have paid sufficient attention to explore the internal dynamics of social, cultural, economic and political realities and have been successful in orienting people, mobilizing them for personal and impersonal sanitation and hygiene related activities, and ensuring the sustainability of the systems through an integrated efforts have been reported successful. In the absence of these things, in a number of communities, the sanitation progammes have been found failed as they could not pay proper attention both on the knowledge and attitudinal dimension of behavioural change.
3.12 Problems Faced in Absence of Sanitation Community leaders have mentioned that a number of personal and public (community level) problems have been increasing due to the absence of sanitation. In the absence of sanitation, local people have been defecating in open spaces, pigs and dogs freely roam in public places, kitchen garden and home-yards are polluted by human and animal excreta. Water in public ponds and canal are contaminated. Houseflies and other pests have increased day by day. Women have been facing problems during menstruation due to the absence of toilet. Children have been suffering from waterborne diseases, especially during late spring, monsoon and early autumn. Pollution of the whole environment is explicitly observed problem due to the absence of sanitation. Community leaders, as they know about sanitation and its need and importance, have stated that they feel disgraceful when some outsiders come to their village. It is pollution due to open defecation which makes them feel inferior and lose their self-esteem.

21 Peoples Perspective Research Nepal, draft; 7 February 2011
A number of health problems were mentioned as the direct effects in absence of sanitation facilities. Both acute and chronic diseases have been mentioned. Waterborne diseases have been reported as the direct consequences they have faced in absence of sanitation.
3.13 Institutional role and arrangements The community leaders have also put their views regarding the role of different institutions. According to them, it is often thought that some people in Nepal are intolerant to some unilateral or multilateral support organizations due to different conflicting interests which are against the fulfillment of such basic and humanitarian needs of the people. Such hindering trends need to be corrected for common welfare. Supporting institutions, according to the community leaders, need to be alert and distinguish genuine need or flattery with narrow and vested interests on the one hand, and they have to avoid the sense of servitude. Due to growing competition and mistrust among the public and private sector institutions, the amount of loss is alarming that warrants consensus of all actors to solve the problem in sustainable way at individual, households and community levels. It would be better to develop a democratic and transparent modus operandi for rational intervention at each level in participatory manner. The narratives collected from the community leaders reveals that water and sanitation related specific package programmes have not yet reached in almost all the places. The Village Development Committee (VDC) and municipality offices, have not paid adequate attention to the water and sanitation sector. In a few places, local NGOs have taken initiatives for constructing temporary toilets. Some local schools have toilet facilities. In some places community forest user group (CFUG) has made some contribution to drinking water and sanitation. However, most of the water systems are getting dysfunct due to the lack of proper maintenance. The community leaders have pointed out the following specific roles of the state, local NGOs, community and, supporting institutions and donor organizations. State
• Maintain the order of the things, and create enabling environment for collaboration through appropriate policies accordingly
• Create environment for generation, proper mobilization and regulation of the resources • Sensitize the actors at different levels and people on the need of the sanitation • Solve the problems related to agriculture and irrigation, education, health, transportation,
safe drinking water, etc, • Regulate different activities of various actors and establish coordination among them for
better result and common good

22 Peoples Perspective Research Nepal, draft; 7 February 2011
NGOs • Work for ascertaining public welfare as per the policy direction of the government in the
sector of drinking water and sanitation • Assist and complement the government as its extended hands • Identify, design and implement development projects to solve the above mentioned
problems • Work in coordination with government line agencies, donors, people and concerned
stakeholders as per the existing legal provisions Community
• Activate all people including the excluded and deprived groups • Mobilize human and other local resources to solve the water and sanitation problems • Declare the community as open defecation free area • Realize and sensitize community people for the genuine needs and issues of drinking
water and sanitation related problems and encourage to take required initiations Supporting agencies, donors, international agencies, private sectors and leaders etc.
• Support as per the felt/real need of the community • Work "with" community people, not "for" them • Formulate need-based programmes and develop participatory monitoring mechanisms in
cooperation with the government agencies
3.14 Peoples participation Despite being aware of the need and significance, a considerable number of men and women are somehow reluctant and not proactive for taking sanitary initiatives themselves. The root of the problem is dependency syndrome. Putting another way, the inhabitants expect some sort of initiations from government line agencies and I/NGOs in this regard. Some view that it is incapability of the community leader. The dependency syndrome of the community is equally threatening to all actors whether they are educated or illiterate, rich or poor, national or international, pro-democratic or status quo alike in the context of the highly globalized world and social order of increasing interdependence. From cursory view of the outsider (etic perspective), it is the result of incapability of the local people. From emic view, it seems that there are complexities and contradictions if someone goes deeper. According to them, the solution can be political, socio-cultural, technical, economic and legal in priority order. Therefore, trustworthy expertise of high caliber, though it seems debatable, may only work out a lasting solution if all the actors take it seriously and rise above personal or group ego, sense of prestige or any type of indifference. To ameliorate the situation in the real sense, all people of different class, caste, creed or mindsets need to be (re)oriented and provoked genuinely and convincingly on its spirit, pros and cons and the associated sanctions. Then, it would be better to approve and implement it strictly. As a consequence it would be clear to people and their voluntary acceptance and conformity can be increased. In the beginning it would be difficult to implement it, but when we establish system or order of things once, it would be less hectic or resistance later on to perpetuate it.

23 Peoples Perspective Research Nepal, draft; 7 February 2011
In the communities where people are sensitized and mobilized by NGO, people have been actively cooperating with the NGOs and other actors working in water and sanitation sector. They possess positive attitude towards the role of multiple actors for water and sanitation related activities, and they have been maintaining both the private and public sanitary systems well. Examples can be taken from some communities where Plan Nepal has rendered support to water and sanitation. However, dependency syndrome has been widely reflected in the narratives. Local people, especially in rural areas, still perceive that it is the government or the state or any of the organizations, which is responsible to work for water and sanitation.
3.15 Monitoring at local level According to the community leaders, constructive dialogue, cooperation and collaboration between and among different stakeholders namely the government, NGOs, international agencies, private sectors, leaders and the community people are needed for monitoring of sanitation initiatives at local level. Though some civil society organizations like CFUG, local clubs, women groups are engaged in water and sanitation related activities, there are a number of problems associated with monitoring of operation of the water and sanitation systems.
3.16 Availability of resources, targeting and use As mentioned earlier, local government bodies (DDC, VDC and municipalities) have not been disbursing sufficient fund for water and sanitation related programmes. The situation points out the need for revising policy and guidelines so as to mainstream water, sanitation and hygiene as basic right of people. Moreover, the policy should also incorporate the specified roles of concerned stakeholders in order to mobilize human, physical and financial resources. In the rural areas, community people have been using available local resources like bamboo, woods, hay, clay and other raw materials to build toilets.

24 Peoples Perspective Research Nepal, draft; 7 February 2011
Annex - 1: Narratives of Community Leaders' Voices This section includes the cases/narratives obtained from the community leaders who are directly and indirectly engaged in sanitation initiatives. The community leaders can also be considered as the key informants who know the overall situation of their communities and their voices have represented the voices of the local people residing in the communities of different parts of Nepal. The cases/narratives presented hereunder have represented the following physio-geographic, socio-demographic, and socioeconomic features of the country:
• Rural and Urban Differences • Caste/Ethnic Variations • Hill and Tarai Communities • Age and Gender Differences
As discussed in section 1.3, the cases/narratives have also represented the different conditions/status of sanitation as follows:
• Where sanitation efforts were made and they were successful • Where sanitation efforts were made and they were not successful and where santiation
efforts were made and they were successful but this was followed by a relapse in increased open defecation or in case of urban these are dysfunctional.
• Where there were no sanitation efforts/interventions

25 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 1: Poverty and Innocence Matter Resided by Brahman, Chhetri, Magar and Dalit people, Makawanpurgadhi of Makawanpur District has 2 secondary, 5 lower secondary and 10 primary schools. Eighty-five per cent of the people are dependent on agriculture as their main occupation. Only 25 per cent households have toilet. Mr. Shiva Ram Rimal, 51 years of Makawanpurgadhi-7 has studied up to grade eight and he is well-aware about the need of sanitation for human and environmental health. He is also aware of basic human right to safe drinking water and sanitation. For him, sanitation denotes to washing hands after defecation, before and after meal, washing cloths and utensils, covering food items to protect from pests, using toilets and keeping home-yards and other public places clean. Mr. Rimal says that the people in his community are less aware of the importance of sanitation and safe drinking water. Lack of capacity to afford for toilet construction due to extreme poverty, and lack of external support for safe drinking water and sanitation are other causes behind open defecation and increased pollution in his community. However, according to him, some people have gradually learned to wash hands, and they have started to keep their house clean. Mr. Rimal has pointed out the role of different stakeholders, including local people themselves, for sensitizing people, rendering support to sanitation infrastructure development and regular monitoring for achieving successful sanitation outcomes in his community.
Representative Case 2: People Need Helping Hands Raigaun is located in the Siwalik foothills along the Basin of Bagmati River resided predominantly by the Rai Danuwars, the Tamang and the Pahari people. This village borders with Sindhuli and Rautahat district. It is one of the remotest places of Makawanpur district having no electricity, road and other infrastructure. None of the sanitation progammes have ever been implemented in the community. People defecate openly and human and animal excreta are found here and there. Almost all the places in the village, especially foot trails, are found polluted. Home yards and public places are also dirty, as if people do not care about sanitation and hygiene. According to Mr. Sanjaya Rai, 47 years who is simply literate, sanitation is the habit of washing hands, bathing, washing cloths and using toilet. He is confident that sanitation and other forms of improvement in his community is not possible without a long-term, well-planned and participatory approaches and methods. He has further pointed out the catalytic role of the CBO/NGO in sensitizing local people and mobilizing them for increasing sense of ownership. Similarly, he points out the need for external support, especially for infrastructure development. He also knows that such progammes will not be successful without local people's active participation and contribution. He has also suggested that the resources allocated for sanitation and other purposes must be spent in a transparent way.

26 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 3: Local Level Unity and Initiation Ensures External Support Hatiya Chisapani is located to the east from Hetauda, the district headquarters of Makawanpur district. The communities in the vicinity have 475 households comprising major caste/ethnic groups like Brahman, Chhetri, dalit, Danuwar, Chepang, and Newar. According to Ms. Kanchhi Danuwar, 60 years who is illiterate knows basics of the sanitation. She says that it was nine years ago, almost all the community people gathered in a public place, discussed the need for drinking water and decided to install a lift-pump and approached Drinking Water and Sanitation Division Office for support. The then Division Chief sanctioned additional 75 sets of latrine-pan. As a multiplier effort and local people's additional contribution, now there are 312 water taps and all the households have been using toilet. Ms. Danuwar finds timely and appropriate support of Drinking Water and Sanitation Division Office and community people's active participation and contribution as the main reasons behind the success of the safe drinking water and sanitation initiatives. She has also mentioned that after they have water running through pipes, community people have been growing fresh seasonal vegetables, they have been keeping their houses, home yards, foot-trails and other public places clean. According to her, people in her community are fully aware of the need for and importance of sanitation and they are well-motivated to mobilize people through user groups and committees and sensitizing people for sustaining the outcomes of drinking water and sanitation initiatives. Ms. Danuwar is well aware that such initiatives are essential for other villages and communities.
Representative Case 4: Relevance, Effectiveness, Efficiency and Sustainability Matter Padampokhari VDC of Makawanpur district is predominantly inhabited by the Tamang people. The VDC has one health post, three secondary schools, 3 lower secondary and 7 primary schools. The Lamatole lies in ward no. 3 of the VDC. Ms. Ganga Kumari Gole, 25 years old community leader is simply literate. She knows the basics of sanitation and safe drinking water. According to her, a NGO had provided support for sanitation in the community nearly three years ago. During the project period, according to her, was neat and clean. The community was declared as open defecation-free area. But after the project was phased out, sanitary condition of the village has been worsened. Ms. Gole has reported that the lack of running water, lack of versatile and dynamic local leadership and lack of active involvement of the user committee were the major causes behind the failure of the project and its outcomes. People have learned the basics of sanitation through that project but they have not translated that knowledge into everyday practices and the scarcity of water has also triggered the worsening situation. She has asked for another drinking water and sanitation programme that would pay more (compared to what was done before) attention to identify actual/real needs of the community, sensitize and mobilize people and increase sense of ownership with a strong monitoring mechanism.

27 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 5: Change Is Really Possible There are 75 households and 601 people. Out of them, 73 households are the Tharu and a household of the Rai and the Brahman. The sanitary situation of Chhotipaliya village of Kailai district was very poor few years ago. Open defecation, indiscriminate throwing of solid wastes, negligence to household and community sanitation, non-sanitary ways of keeping birds, pigs and other animals were some unpleasant instances. Consequently, people used to frequently suffer from fever, diarrhea, filaria, cholera, common colds, dysentery etc, resulting in more expenditure in health. Despite the persisting sanitary and drinking water problems, the people and the community were away from attention of the governmental and non-governmental institutions. The villagers were in one or other way despised due to the sanitary problems by the neighboring villagers. Nobody was taking initiation to solve the problem in the past. According to Maya Chaudhari, 18, a local club of the village approached with other national NGOs for possible support. They assessed the need of the community in the first place. After the community consensus to demand support, the National NGO approved a plan to work with the community in 2007/8 together with its partner CBOs. According to the Ms. Chaudhari, the approach of the NGO has been participatory and transparent. People were encouraged to formulate a user committee first and it provided health and sanitation education to them. With their facilitation, they have built a reliable and safe drinking water supply system. They have also run a health and sanitation education programme which has made each member of the community sensitive to health and hygiene issues. All of the households have constructed temporary or permanent type of toilets nearby their house. Now there is no problem of open defecation and urination in the community. The villagers have pit for solid waste management. Every household has made a safe rack of wood or bamboo for placing the cleaned utensils of the kitchen which is above the reach of the children or any birds or animals. The villagers are aware that the sunlight also helps kill the germs. NGO staffs have persuaded villages to consider sanitation aspect while raising their livestocks. Earlier the intervention, the villagers used to think that visibly clean water was safe for drinking. But the motivators have convinced the villagers that the visibly clean water may also contain pathogens. Therefore, the villagers now boil water, treat it properly or adopt sodish method before drinking. These are incredible changes in the village. Due to improved sanitary conditions in short duration of time, prestige of the villagers has been augmented among neighboring settlements. The village has been treated as a model and therefore, people from other parts of the district come to Chhotipaliya and realizes that if people really want, change is definitely possible.

28 Peoples Perspective Research Nepal, draft; 7 February 2011
Photo 1: Clean environment of Chhotipaliya
Photo 2: Collecting naratives from Maya Chaudhari

29 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 6: Way Out From Dependency Syndrome Resided by 75 households and 525 people, the Bangara community is situated in Dhangadhi Municipality. It is heterogeneous comprising of three major caste/ethnic groups, namely the Tharu, Dalit and Brahman. Hinduism and Christianity are their primary religions. Their life style, dressing and food habits somehow accord with their cultural patterns.
A public primary school is in operation in the community. The residents are almost educated. Out of 75, 25 households do not have toilets however and therefore are compelled for open defecation. In the light of their educational status, it may seem irrational to label them as dirty in sanitary terms only. A local resident known as Radheshyam Chaudhari of 37 is probably of the opinion that sanitation is concerned with the activities like washing hands and mouth, eating clean or hygienic dishes, cleaning house and the surroundings.
Mr. Chaudhari thinks that the wastes and pollution are piled up and are being aggravated cumulatively. Therefore the risks of health hazards have been decreased and social esteem has been increasing day after day. According to him, if all actors realize this pressing reality quickly, develop strong team spirit, become more accountable and committed, we can expect positive changes in sanitary behavior in the community. He also says that we citizens, students, actors, change agents and experts of development have understood the goals of anticipated changes in drinking water and sanitation sector.
Photo 3: Bangara community in way to progress
According to Mr. Chaudhari, people have to cooperate with the institutions that are facilitating to solve long felt needs for sanitation in the community. He also pointed out the need for constructive dialogue, cooperation and collaboration between and among different stakeholders.

30 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 7: Need for a Joint Effort Bhadrapur is Tharu Community of Dhangadhi Municipality where 28 households and 302 people have been residing. They largely follow Hindu religion. Their life style, food habit, and dressing somehow suit with their broader cultural patterns. There is not any school in the community. Except homestead, all inhabitants do not have any land for cultivation. Women in this community do not observe any taboo during menstruation. Open defecation, solid wastes scattered here and there together with other sanitary problems can easily be observed in the community. The reasons behind the poor sanitary situation can be attributed to their low educational status, negligence and inadequate leadership quality.
Photo 4: Scattered waste in community
According to community leader Mr. Tek Bahadur Chaudhari of 30, washing body, having clean food and keeping house and surrounding are parts and parcels of sanitation. Despite their knowledge and positive attitudes, they lag far behind in following sanitary and hygienic behaviors. According to him, people expect external support from government agencies and I/NGOs for community sanitation as if solving the problem of drinking water and pollution can be solved only through outsiders' support. But he also knows that keeping their households and surroundings clean can be possible by their own initiations. However, governmental and nongovernmental organizations can facilitate them for sensitization and social mobilization. "If all join the hands, even though the problems can be solved by ourselves", he said.

31 Peoples Perspective Research Nepal, draft; 7 February 2011
Photo 5: People playing cards in community
Representative Case 8: Sanitary Problems Persist Even After the Intervention Gohawa village of Rajhena VDC in Banke district is a bad example of safe drinking water and sanitation programme. A total of 190 households with 1303 population have been residing over there. The major caste/ethnic groups are the Tharu, Dalit, and Brahman. They observe Hindu and Christian religions. There is a primary school in the vicinity. Except among Brahman, they do not keep their females in the dark huts during menstruation period. The Dalits have been practicing early marriage of their children which has somehow hampering their sanitary and reproductive health conditions. The village was not safe in terms of sanitation and health earlier the intervention of a NGO during 2007/8. Open defecation, indiscriminate placement of the solid wastes, dirty ways of keeping birds and animals together with others were the non-sanitary practices in the community. As a result, the chances of villagers to be suffered from diseases like fever, cholera, diarrhea, common cold, abdominal pain, filarial, etc were high. By realizing the situation and need of the community, the NGO launched a safe drinking water, health and sanitation programme in 2007/8. During the project period, the people followed the instructions of the staff. After the termination of the project, the motivators left to visit and instruct them. The villagers left the sanitary practices taught by the motivators and have started to do what they used to follow before intervention. In this way, the aim of the project has been failed and the investment has become futile. What may be the reason behind the failure? It is natural that all projects do not end in success. However, it would be better to seek factors triggering for the failure for betterment in the future. The project was based on subsidy approach and the prime causes is that the people could not feel sense of ownership of the project. They were highly dependent on external support than

32 Peoples Perspective Research Nepal, draft; 7 February 2011
internalizing the concept of sanitation as the approach that promotes their dignified lives. They have blurred view that the programme was intended for them. Even the user committee did not become active. It indicated need of more efforts of community based institutional development for sustaining the efforts. The heterogeneity can be one factor for not summoning meeting, discussing the real needs and implementing them. Some opine that it is the poverty of the villagers that compelled them to think more on the bread-and-butter problems. How can they think about the long term development of the community? Therefore, the situation of the community is not different than before the intervention. The other side of the reality is the role of donor, partner NGO/CBOs and the local change agents involved. They could coordinate the government agencies, local leaders, and other stakeholders in time. Anyway, the community was deserving and needy for support. Other implication is that the project needs to be alert about follow up schemes. Similarly, other channels available were not mobilized by the staff which could alter the scenario.
Representative Case 9: External Support is Not Sufficient There are 29 households in Janapriya Tole of Biratnagar Municipality-7 where a NGO has implemented "Integrated Drinking Water, Health and Environmental Sanitation programme" in collaboration with Biratnagar Municipality for the last two years. The project has also worked for micro-finance and children-related activities. Community Leader Goma Chaudhari, a widow of 37 years has passed School Leaving Certificate. She knows sanitation as a combination of cleanliness of human body, home yards, public places and the whole 'environment' and she knows that sanitation is essential for the promotion of human health and prevention from diseases. She also knows that a person who keeps her/himself neat and clean becomes a role model in society and her/his increased self-esteem and dignity ensures a respectful personality. She finds sanitation as one of the fundamental human rights and everybody must have access to water and sanitation. She has mentioned cold and coughs, skin diseases, eye infections as the major health problems in her community. In her community, almost all households do have toilets but the sewage and drainage system is open and poorly managed. She mentions that some people, especially children, still defecate openly. Regarding awareness about sanitation, hygiene and health, she perceives that knowledge alone is not sufficient unless it is practiced in real life. For example, people in her community have not paid sufficient attention toward the sanitation of public places. Regarding sanitary behavior during menstruation, she has found women of richer class using sanitary-pads and her observation is that the girl students have been facing problems due to lack of convenient toilet in schools. Ms. Chaudhari perceives that local bodies and User Committee are not active enough to bring better results even after local people have received external support. There are some people in the community having pride and prejudice who do not cooperate with the majority of poor and disadvantaged groups. In her community a local person has not cooperated with the project and he has not agreed to use his land for drainage. They involved in series of meetings and dialogues, and protests. The task of constructing drainage is incomplete. Local people are waiting for formal and legal action against the person. This indicates that the persons who possess knowledge about sanitation do not ensure that they possess better attitude and practice better. She has also pointed out the need for active participation of local people strong monitoring of these sanitation programmes.

33 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 10: Perceptions of differently abled people Stories of Jeevan Dhakal from Ilam and Dhan Prasad Subedi from Dhading are inspiring cases of sanitation. It is true that lives of both these differently abled people have been dignified by sanitation interventions in their areas. They believe that sanitation is essential component of life that affects healthy environment of any community. Availability of safe water is essential to sustain sanitation services. Successes of sanitation interventions are possible because of ownership and community engagement. The aspiring involvement of community during planning phase assured needs of differently abled people residing there. They were able to participate in awareness raising and sensitization camps that supported in internalizing relevance of sanitation and hygienic behavior for ensuring healthy lives. Participation in these planning meetings provided them space to share their needs and helped in the process of acquiring ownership towards the sanitation programs. Community leadership should be promoted to sustain sanitation initiatives. These people at the ground should be given responsibility of monitoring and evaluating progress to ensure fair judgment based on community requirements. Mobilization of community and ownership are essential to change behavior and sustain sanitation progress and performance.
Representative Case 11: Community People Are Really Cooperative A NGO has worked for sanitation in Pashupati Tole, Biratnagar Municipality-19 in collaboration with Biratnagar Municipality for the last two years and has supported to construct toilets through its "Integrated Drinking Water, Health and Environmental Sanitation programme" project and has provided sanitation service to 72 households of the hamlet. Local people were made aware about the need for and importance of sanitation. The project constructed tube-well for the purpose of drinking water. Programmes for micro-finance, public awareness, advocacy and childhood development were also parts of the project. According to Omkar Acharya, a Community Leader of 28 having an M.Sc. degree, there are two privately run schools and sanitary status of both of these schools is good and have separate toilets for boys and girls. He is an educated person. Mr. Acharya is quite knowledgeable regarding health and hygiene. He is also quite aware of that access of all to drinking water, health and sanitation is one of the basic human rights. He says that each household in his hamlet has toilet and the people first sort out the decomposable and non-decomposable waste and put them in container. The hamlet, as he says, has totally stopped open defecation. People of the area wash hand before and after work, and before and after meal. They purify water using different methods like boiling, filtration, and sodis. They wash raw vegetables before cooking and wash their utensils with soap. However, there is no provision of drainage for sewage management in the area. Mr. Acharya perceives strong commitment of supporting organizations, active participation of community people, responsiveness to local needs, sense of ownership, accountable and responsive leadership, mutual cooperation and positive attitude toward health and sanitation were the factors that made sanitation program successful. The sanitation program, according to him, has helped increase self-esteem and dignity of the community people, and decreased the rate of

34 Peoples Perspective Research Nepal, draft; 7 February 2011
absence of students in schools. In his view, efforts to personal and community level sanitation initiatives can be sustained through increased awareness, need-based activities, and proportionate investment of community people and the external support organizations. He finds strong, well-designed monitoring of community initiatives and infrastructures essential for sustained benefits from sanitation initiatives.
Representative Case 12: The Politics and Pollution in the Public Toilet There are 190 households in Hadtali Hat Tole of Biratnagat Municipality-19 where the Municipality Office and Biratnagar Jute Mills Ltd. had constructed a public toilet and the toilet was being maintained by the staff of the Jute Mill. After the Jute Mill is closed, the toilet has been almost defunct. Though Rs. 5-10 per week is levied from each household, it is not maintained and the toilet is almost defunct. The toilet was being used by almost all the households in the past days when number of households were also lesser than present and the local households at that time did not have private toilet. Now almost all the households have toilets. About 40% people still use it as the hamlet is also resided by the slums. In this regard, the Support to Housing programme implemented by a NGO that has supported for the renovation of this public toilet. However, the toilet renovation has not yet been completed. The failure of renovation work, according to Mr. Bharat Lama, is due to the irresponsiveness, lethargy, unaccountability and vested interest of local community leaders and the municipality authorities. According to Mr. Lama, 32, who has studied up to higher secondary level, all the households have private toilets but their hamlet is highly polluted due to the sewage coming from other parts of the municipality. However, according to him, about five per cent of the households still defecate openly. Personally, Mr. Lama knows well about the need for and importance of sanitation for human as well as environmental health. He says that the Drinking Water Corporation and the municipality have not have not supplied drinking water in this hamlet and the people are compelled to use tube-well which is not safe drinking water and consequently, they are not able to enjoy basic human right to safe drinking water and sanitation. In his view, efforts to community level sanitation initiatives can be sustained through increased awareness, local good governance, and proportionate investment of community people and the external support organizations.
Representative Case 13: Accountability, Participation and Commitment Matter The Bank Road Street of Biratnagar Municipality-19 has been resided by 72 households. All the households use toilet with drainage and waste disposal facilities. None of the people defecate openly. NGO in cooperation with Biratnagar Municipality has worked in sanitation sector for the last two years and has supported to construct toilets. Besides, the project also worked for microfinance, physical infrastructure development in the community. According to Ms. Kalpana Shrestha, 50 years, SLC passed Community Leader, responsive and accountable community leadership, active participation and cooperation of community people especially women, equity based benefit sharing, use of locally viable technology and continued external support to physical infrastructure development and awareness programmes made possible to make the hamlet neat and clean. People put their waste in the container send which is regularly send by the municipality office. Though she is not highly educated, but she is quite aware of the causes and consequences of pollution and contaminations. She knows about the importance of sanitation and hygiene very well. She perceives basic human right to water and sanitation. According to her,
35 Peoples Perspective Research Nepal, draft; 7 February 2011
local people in her community have undergone through a series of orientation training regarding sanitation and related issues and consequently they have been purifying drinking water and washing their hands. Some women use sanitary pads and some use clean cotton cloths during menstruation. There are separate toilets for the girl students in the schools. In her opinion, changes in bad habits that create sewage and pollutions, sense of ownership on the physical infrastructure developed in support of the external agencies, and regular participatory monitoring are essential elements for sustaining the impacts of sanitation and community development initiatives.
Representative Case 14: Success is a Common End Ms. Manju Chaudhari, 27 years, a simply literate community leader, lives in Bramhapura Tola of Biratnagar Municipality-7. She knows well about the need for and importance of safe drinking water and sanitation. She reports that the NGO has worked in sanitation sector for the last two years and has supported to construct toilets in cooperation with Biratnagar Municipality and as a result, every household has toilet. The hamlet which was highly polluted in the past days is now tidy and clean. Besides, the NGO has also worked for microfinance and child welfare. However, the street does not have drainage facility and consequently, the hamlet becomes polluted during raining season. According to Ms. Chaudhari, people have changed their habit of open defecation. Schools also have provisioned separate toilet for girl and boy students. The organization has also sensitized the students and teachers in these schools regarding the importance of sanitation. She says that it is community people's cooperation that has made the mission for making pollution-free hamlet successful. Beside, accountable and responsive support of the NGO and Biratnagar Municipality and increased awareness of community people has succeeded the programme. She concludes that regular monitoring and evaluation of the sanitation initiatives and awareness campaigns are essential for achieving sustainable benefits from safe drinking water and sanitation programmes.
Representative Case 15: Who is Responsible, Local People or Service Provider? Ms. Romila Rajbhandari, 32, a simply literate community leader, lives in Swayambhu Tole, Biratnagar Municipality-18. Ms. Rajbhandari is knowledgeable regarding the importance of safe drinking water and sanitation for human as well as animal health. She also knows that a tidy and clean person and his family having toilet has better dignity and self-esteem than the others who do not have toilets. She also knows that safe drinking water and sanitation are the fundamental human rights. There are 35 households in Swayambhu Tole. Almost half of them are the landless people. Fifteen households have toilet and other defecate in open spaces. Ms. Chaudhari opines that community people are not fully aware of the need for and importance of sanitation. Some people do not purify drinking water properly and do not wash hands with soap. Women use to put cloths used during menstruation in cool and dark corners. Majority of the girls do not go to schools during menstruation period. There is one college which runs Masters level programme in science and the college has separate toilets for girl and boys. There are no other schools. Ms. Chaudhari shows her dissatisfaction regarding the sanitary condition for her community. She says that children are victimized most due to the lack of proper sanitation and get suffered from

36 Peoples Perspective Research Nepal, draft; 7 February 2011
diseases like dysentery, diarrhea, cholera, meningitis, etc. Most of the adult males residing in the hamlet are the rickshaw-riders and people in the community are not educated. There is not any sanitation programme implemented ever in the community. She asks for a sanitation programme which would first sensitize community people, support to construct toilets, and engage local people to monitor and maintain the initiatives because unless people take ownership of what (support) they receive, success is not possible. In addition to external support for infrastructure development, it is community level awareness and participation which can bring sustained change in sanitation and hygiene.
Representative Case 16: Ignorance of the Indigenous Practices May Result in Failure Lakhanawar village is mixed dwelling of Tharu and Dalits. It is situated in ward no 6 of Kohalpur, Banke. All the inhabitants are Hindus. There is a primary school in the village. However, the community is not found pleasant in terms of its sanitary condition as perceived by Thagga Tharu Chaudhari of 40. According to her, people's perception about sanitation is customary. Open defecation, solid wastes scattered here and there, unsafe and even dirty way of keeping birds and animals all suggested the overall scenario of the community. As a result, trends of falling ill or even increased rate of mortality are considerable. The often detected diseases among the dwellers are fever, cholera, diarrhea, dysentery, filaria, typhoid, common cold, etc. Taking the gravity of the problems into consideration, a NGO had launched a safe drinking water, health and sanitation programme in the community. Even after the intervention, according to Thagga Chaudhari, it is hoped that the situation of the community would be improved. It has been difficult to the people to employ scientific sanitary habits taught by the NGO staff instead of their customary ways. Unfortunately, even after termination of the project, no behavior change has been resulted considerably. Why the project failed? A local woman who has passed school leaving certificate as well accredits the inactiveness of the user committee members for the failure. She said, "They did not understand the spirit of the project, meet adequately and mobilize the community for the aspired transformation". She has suggested the project team to explore the triggering reasons with adequate seriousness. Even the reporting of the project personnel are unreliable, derogatory and ethnocentric (biased). From cursory view, inadequate understanding of indigenous practices and felt needs might be one of the causes of the unexpected result of the inputs.

37 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 17: Enlightened by NGO's Programme Tilakhanipur of Pahalmanpur VDC is situated in Kailali district. Some 88 households and 575 people reside there in the community. All of them are the Tharu, an indigenous community, and they largely observe the rites and rituals of Hinduism. Their dressing, food habits and overall life styles are somehow in accordance with their customary practices. The women do not observe taboo like other high caste Hindus during menstruation and do not reside separate from the family members.
The community was far away from the development and modern ways of sanitary practices. According to Durbesh Chaudhari, they perceive that sanitation is only related to washing hands and mouths before and after eating, keeping house, courtyard and the surroundings neat and clean. There was some sort of gap between their customary knowledge, their practical lapses and the scientifically preferred ways. Open defecation, throwing wastes here and there indiscriminately, keeping birds and animals beyond sanitary ways could easily be observed in the community. The frequency of falling ill due to waterborne and other seasonal and chronic diseases is common.
Photo 6: Discussing with Durbesh Chaudhari
The days of the non-sanitary practices are gone in the community now. People practice scientific ways of sanitation, wash hands with soap after touching any unsafe thing, use safe latrines, and are sensitive on sanitary and hygienic issues more. The credits of the pleasant changes go to the safe drinking water, health and sanitation programme of the NGO working with its local partner. Now-a-days, each household in the programme area has a safe pit for solid waste management. The households have made a rack with wood or bamboo to place the cleaned kitchen wares. They are above the reach of children and ruminants. All people know that the sunlight kills the pathogens if any.
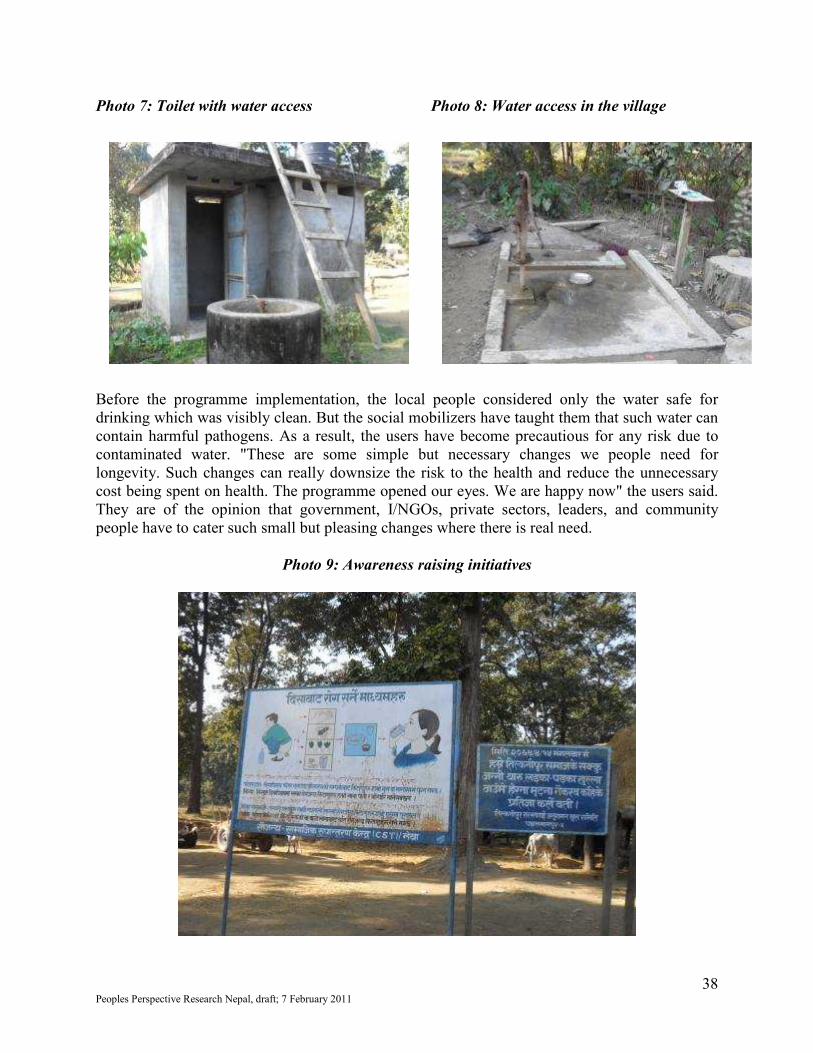
38 Peoples Perspective Research Nepal, draft; 7 February 2011
Photo 7: Toilet with water access Photo 8: Water access in the village Before the programme implementation, the local people considered only the water safe for drinking which was visibly clean. But the social mobilizers have taught them that such water can contain harmful pathogens. As a result, the users have become precautious for any risk due to contaminated water. "These are some simple but necessary changes we people need for longevity. Such changes can really downsize the risk to the health and reduce the unnecessary cost being spent on health. The programme opened our eyes. We are happy now" the users said. They are of the opinion that government, I/NGOs, private sectors, leaders, and community people have to cater such small but pleasing changes where there is real need.
Photo 9: Awareness raising initiatives
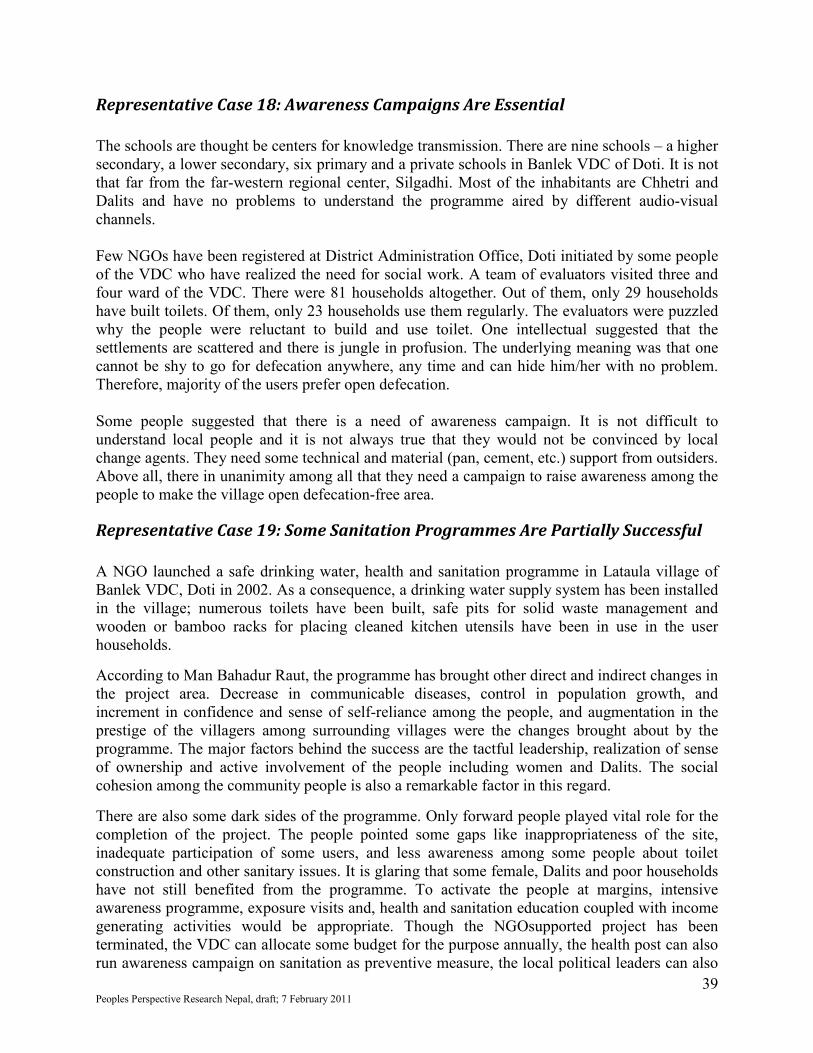
39 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 18: Awareness Campaigns Are Essential The schools are thought be centers for knowledge transmission. There are nine schools – a higher secondary, a lower secondary, six primary and a private schools in Banlek VDC of Doti. It is not that far from the far-western regional center, Silgadhi. Most of the inhabitants are Chhetri and Dalits and have no problems to understand the programme aired by different audio-visual channels. Few NGOs have been registered at District Administration Office, Doti initiated by some people of the VDC who have realized the need for social work. A team of evaluators visited three and four ward of the VDC. There were 81 households altogether. Out of them, only 29 households have built toilets. Of them, only 23 households use them regularly. The evaluators were puzzled why the people were reluctant to build and use toilet. One intellectual suggested that the settlements are scattered and there is jungle in profusion. The underlying meaning was that one cannot be shy to go for defecation anywhere, any time and can hide him/her with no problem. Therefore, majority of the users prefer open defecation. Some people suggested that there is a need of awareness campaign. It is not difficult to understand local people and it is not always true that they would not be convinced by local change agents. They need some technical and material (pan, cement, etc.) support from outsiders. Above all, there in unanimity among all that they need a campaign to raise awareness among the people to make the village open defecation-free area.
Representative Case 19: Some Sanitation Programmes Are Partially Successful A NGO launched a safe drinking water, health and sanitation programme in Lataula village of Banlek VDC, Doti in 2002. As a consequence, a drinking water supply system has been installed in the village; numerous toilets have been built, safe pits for solid waste management and wooden or bamboo racks for placing cleaned kitchen utensils have been in use in the user households.
According to Man Bahadur Raut, the programme has brought other direct and indirect changes in the project area. Decrease in communicable diseases, control in population growth, and increment in confidence and sense of self-reliance among the people, and augmentation in the prestige of the villagers among surrounding villages were the changes brought about by the programme. The major factors behind the success are the tactful leadership, realization of sense of ownership and active involvement of the people including women and Dalits. The social cohesion among the community people is also a remarkable factor in this regard.
There are also some dark sides of the programme. Only forward people played vital role for the completion of the project. The people pointed some gaps like inappropriateness of the site, inadequate participation of some users, and less awareness among some people about toilet construction and other sanitary issues. It is glaring that some female, Dalits and poor households have not still benefited from the programme. To activate the people at margins, intensive awareness programme, exposure visits and, health and sanitation education coupled with income generating activities would be appropriate. Though the NGOsupported project has been terminated, the VDC can allocate some budget for the purpose annually, the health post can also run awareness campaign on sanitation as preventive measure, the local political leaders can also

40 Peoples Perspective Research Nepal, draft; 7 February 2011
mobilize their cadres for sanitation, and occasional public hearing programmes can also contribute to pressurize the concerned stakeholders to work for the improvement of human and environmental health through sanitation initiatives.
Representative Case 20: Local Leaders' Role Is Crucial Dil Bahadur Khati is a resident of Kalena 6, Doti. He has been active for the development of drinking water supply system and conduction of sanitary campaign in his village. Now days, people pay tribute to him and he has a say among local leaders, stakeholders and I/NGOs. Before 2002, nobody would bother or take responsibility even for fulfillment of their basic needs like drinking water and sanitation related activities. Wastes used to be scattered here and there. Open defecation was common. The frequency for falling ill due to waterborne diseases among the villagers was significant. Due to the sanitary problems in the village, they were often disparaged by outsiders. After need assessment, NGO decided to launch a safe drinking water and sanitation programme in the village in 2002. The approach of the programme was to mobilize the community for its own development. That ensured people's participation and the impact has been sustainable. Dil Bahadur came easily on the fore from the beginning of the intervention. A user committee was formed in the first place. Local people nominated him as a secretary of the committee. Frequent meeting, interactions, and trainings with the NGO, partner CBOs, and local stakeholders capacitated him for leadership. He became truly active in the sector incessantly. As the part of the programme, 87 toilets have been constructed in the village. Each user household dug a pit for solid waste management. Every household made a rack for keeping the cleaned kitchen wares nearby their courtyard. The villagers gave up the habit of open defecation. To condition the fellow being for using toilets, they made provisions to punish the open defecators. As a result, the village has been neat and clean. The contamination of communicable and other diseases has been rare. By seeing their success; the neighboring villagers also have started to construct toilet and make their community clean. Mr. Dil Bahadur is still active to extend the campaign to other parts of the village. Whenever he meets women, Dalits and excluded, he tries to sensitize them for sanitation and need for participation in such programmes. He still lobbies with the VDC officials, NGO personnel and other stakeholders to allocate budget for carrying out similar activities in the unreached communities as sanitation programme is social in nature and requires collaborated efforts of all the stakeholders concerned. He further opines that frequent public hearings can make the stakeholders responsive to such genuine issues and concerns of the rural people.

41 Peoples Perspective Research Nepal, draft; 7 February 2011
Representative Case 21: Female Health Volunteers Also Contribute Khima Devi Raut is a female health volunteer. She is a resident of Banlek VDC – 3, Doti. Her prime duties are to make people aware about the need of sanitation, health and nutrition, teach mothers ways to cope with their and children's health, and make people aware of preventive and curative aspects of health. After the initiation of safe drinking water and sanitation programme in her village during 2002, she also became active somehow. She was also selected as a member of user committee by mass meeting. During the project cycle, she regularly took part in meeting, interaction, training and sensitization campaigns in the community. Despite her multiple workload, she encouraged local people to construct 29 toilets, safe pits for solid waste management and making a rack for placing the cleaned kitchen wares. However, the programme failed in the community to meet the major objectives. She is sad due to the result. The reason behind the failure was the lack of participation of women, poor, Dalits and people at margin. Due to her involvement in farming, household chores, and other social duties, she has heartily realized that she could not give adequate time for the programme. However, she would contribute more time and energy for such programmes in the days to come. The situation could not be put in the right place by her capacity and the collaborated efforts for such programmes can be possible either by strong leadership or public pressures.
Representative Case 22: People's Participation Is Gradual Process Pari Auji is a resident of Kalena-6, Doti. As an illiterate Dalit woman, initially she did not properly understand the need for and significance of safe drinking water and sanitation programme launched in the village. She found herself in frenzy to meet the hand-to-mouth problems; she had no time to think about sanitation. Due to poverty, compulsion to involve in household and outside chores to eke out livelihood simultaneously, she was away from the process of sanitation programme. She had no knowledge and clarity on the urgency of the sanitary habits and therefore she was not active. She was even irritated by the people's activities then. "The rich people have no work and make fuss in the village", she used to think. But she has now noticed some glaring changes after NGO's intervention in the village. She has mentioned that a drinking water supply system has been installed in the village, the trend of constructing and using toilets have been increased, the user households have dug a pit at their disposal for managing solid wastes, the participating households have made a rack for keeping cleaned kitchen wares out of the rich of the children, birds and animals. However, she has belatedly realized the need, relevance and significance of such programme. She dreams at present, "if some governmental and nongovernmental organizations bring similar programme, I will definitely participate in some ways". Due to the change came in the mentality of a poor Dalit woman like Pari, it can be inferred that it takes time for people to identify and realize own needs. When they understand the issue and the process completely, people cannot help participating in any programme intended for their welfare.

42 Peoples Perspective Research Nepal, draft; 7 February 2011
Annex - 2: Guiding Notes for Information Collection Guiding notes for information collection These notes have been prepared to facilitate the national committees to collect information for country research. The outcome of the survey will be a synthesized brief country paper with case studies. At regional level these country papers will be further consolidated into a joint regional paper. These guiding notes have been prepared in the light of agreed methodology/ToR and should be read along with ToR. Since this is a qualitative and perception survey, we should not develop a structured questionnaire, but following broader questions will help to collect the information. It may not be necessary to go all the questions in sequence. Also you may add and adjust if any other information is coming. Common questions for all categories 1. Community Profile Total population Number of households Social profile of community Number and types of schools Common diseases in the area/locality
2. Profile of the community leader/women/representatives of marginal groups Name of the person Locality Urban/Rural Name of town and district Sex (Male or Female) Education Social Profile Minority any socially excluded group, differently able etc.
3. What is your understanding about sanitation? What do you think sanitation is? 4. Status of sanitation infrastructure and usage
a. What kind of sanitation system is available at house hold and locality level? b. Percentage of households using
sanitation facilities last year :
c. Percentage of households always defecating in the open
:
d. Sewerage system : e. Drainage :

43 Peoples Perspective Research Nepal, draft; 7 February 2011
f. Solid waste disposal system : If this is a slum, with a public toilet facility:
A Who built the toilet?
(Government / NGO / Joint Collaboration)
:
B Is it well maintained? : C Community contribution in
construction? :
D Do all people use the toilet (Percentage of HH using the toilets)
:
E Who manages the toilet?
:
F Do you pay for usage? :
5. Does all the school have functional and usable toilets for the school children? (Yes/No):
6. Are these present and being used? If not, why? Please write a narrative
7. Are there separate, functional and usable toilet facilities for girls? (Yes/No)
8. Are these present and being used? If not, why? Please write a narrative 9. Do you think that sanitation is important? If yes, why, if no why? 10. Do you think that sanitation has a role to play in?
Please tick in order of priority (1-most important, 5-least important)
o Disease prevention,
o Is important for health,
o Education,
o Poverty reduction,
o Dignity Any other ___________________________
Please record the narrative of the respondent 11. In Sept 2010 the UN General Assembly declared Water and Sanitation as Human Rights
and the national governments have endorsed this.
What does this mean for you?
In the rural context: what does this mean

44 Peoples Perspective Research Nepal, draft; 7 February 2011
In the urban slums context: what does this mean 12. Are people aware about basic hygiene (Yes/ No):
Record a narrative where the response is mixed or needs to be explained
i. home and personal hygiene, ii. food hygiene
iii. safe handling of water and hand washing and iv. Are people aware about this and do they practice?
If not , why? 13. What practices you adopt during menstruation? How does it affect your daily life?
Hygiene, cultural practices etc. Observation by the person taking the interview: 14. Is the village/slum clean and open defecation free or not? 15. Please explain the status of the environment in a few lines, based on visual perception. If there is no sanitation system – why is there such situation and how people cope with it. If open defecation, what are their feelings about it. How women, excluded communities, disabled and any other marginal communities think about this situation and what kind of problems they face either in rural or urban areas. What do the teachers think in schools? It would be desirable to take video clips of all or some of the interviews Also take picture of the community leader and the location (village/slum/public toilets) 16. If a sanitation programme was introduced? (Yes/No) If No – Go to Section C If yes – Continue… Details of the Sanitation Programme Programme information 17. Who introduced the programme in your village/slum? What do you know about the
programme? Govt/NGO/Private/Self initiated
18. Which year was it started? 19. What were major components of the programme? If the sanitation programme was successful go to Section A
If the sanitation programme was not successful go Section B

45 Peoples Perspective Research Nepal, draft; 7 February 2011
Section- A: Where sanitation efforts were made and they were successful 1. Do you think that the village/slum is clean and open defecation free (ODF), has adequate
sewerage and drainage? Yes/No Please record the perception of the interviewee (Why do you consider your village/ slum is successful in improving sanitation and hygiene) 2. What are the contributing factors in successful sanitation programme or system in your
area? Be open ended and may need to explore following factors in details but not in hurry: i. Regular maintenance by programme authorities or communities
ii. Community participation in the programme/project or activity and they were aware of the benefits-Behavior change
iii. Local leadership who understands benefits of sanitation and cares about it iv. Adequate finances were available, better targeted and utilized and community have a say in
fund utilization v. Better local level institutional mechanism (whether local bodies, NGOs, Public Health
Engineering Departments etc) and accountable to people vi. Solutions were not imposed but locally agreed-whether small, simple or large sewerage system
vii. Women’s participation and leadership role viii. Incentives
ix. Hygiene education x. Technology
xi. Water availability xii. Any other reason
Record narrative: 3. What needs to be done to make the sanitation a sustained success in the coming years?
a. What is the most critical area of follow up?
b. What needs to be monitored? 4. What is the difference that sanitation has brought about in your life, the lives of your
household members, the community? Guidance: Please make a special mention for the difference it has made to women, the disabled, the elderly, and children. Perceived benefits could be: Reduction in diarrhea, Convenience, Dignity/Privacy, Safety, School attendance, Livelihoods, etc. Please record narratives in peoples own words
Any other relevant question
46 Peoples Perspective Research Nepal, draft; 7 February 2011
Section –B: Where Sanitation efforts were made and they were not successful 1. How the existing sanitation system (toilets, sewerage lanes etc) was built, who built it? 2. If programme is not successful and structures created was not functioning or not in use?
What are the reasons? Be open ended but for further exploration can keep following in mind or ask.
i. Technology was not appropriate, location was not suitable
ii. Structures (toilets, drainage, solid waste disposal, sewerage lanes) were not properly constructed.
iii. If toilets or other infrastructure not constructed what are the reasons iv. If constructed but not used what are the reasons v. Community was not aware or not involved in the project/programme/activity
vi. No follow-up actions, no funds for maintenance vii. Lack of proper institutional ownership or arrangement whether by LGs or community
viii. Lack of local leadership ix. Water is not easily available for flushing the toilet? x. Incentive available was not given to the eligible persons?
xi. Inadequate role of the local government institution and the VWSC? xii. Toilet construction is not a priority of the people?
xiii. Any other reason(please specify)
Guidance: Please tick appropriate reason according to discussion and note the narrative 3. If there was a slippage from higher levels of sanitation coverage;
i. What was the reason
ii. What was done about this problem(by the LGI/NGO/Community)
iii. What needs to be done now
iv. According to you, what needs to be done to make the total sanitation a success in the village/ slum?
4. What should be the role of a. The government
b. NGOs
c. Community
Any other question
Section – C: No sanitation intervention was done 1. What is the current sanitation situation in your community? (village / slum )
o Practicing ODF – problems
o Difficulties faced by women / children/ old / disabled people

47 Peoples Perspective Research Nepal, draft; 7 February 2011
o Dirty environment
o No problem
Any other _______________________________________
2. Due to the lack of sanitation facility, what problems do you see in your community?
o Dishonored
o Isolated
o Disease / Life threatening outbreaks
o Low attendance in schools
o Dirty environment
o No other development initiatives
o No problem
Any other _______________________________________
3. What are the sanitation needs in your community?
4. Why there have been no sanitation initiatives in your community? What do you think are the important reasons?
o Lack of awareness / education
o Lack of affordability
o No initiative from Govt / NGOs
o Local govt. has no budget
o Community not in the priority
o Land issues
o Not organized
o Lack of water facility
o Low density of population
o Remoteness
Any other _____________________________________________

48 Peoples Perspective Research Nepal, draft; 7 February 2011
5. Did you make attempts to get sanitation facilities for your community or yourself?
What did you do and what was the response?
6. How do you feel because you and other members of the community do not have access
to sanitation facility?
7. What are the development priorities of your local government / govt.? What do you think?
8. How sanitation can be improved in your community? What steps need to be taken?
i. Role of community
ii. Role of government
iii. Role of NGO















![Adolescent Body Perception: Urban, Rural and Suburban ... · Findings on rural–urban differences in perception have been inconsistent [22], showing variation in weight-related behaviors](https://img.pdfslide.net/doc/110x75/5f7cb259bfbc7459381089a7/adolescent-body-perception-urban-rural-and-suburban-findings-on-ruralaurban.jpg)













