Embed Size (px)
Citation preview

oriGinaL artiCLE
Percutaneous Mitral Valve repair: initial Experience with MitraClip™
Reparación Valvular Mitral por Cateterismo: Experiencia Inicial con MitraClip®
1 Department of Interventional Cardiology, Instituto de Cardiología y Cirugía Cardiovascular. Hospital Universitario Fundación Favaloro2 Echocardiography and Vascular Doppler Laboratory, Instituto de Cardiología y Cirugía Cardiovascular. Hospital Universitario Fundación Favaloro3 Department of Anesthesia. Instituto de Cardiología y Cirugía Cardiovascular. Hospital Universitario Fundación Favaloro
carlos FaVa1*, FaBIÁn salMo2, gustaVo leV1, gaspar caponI1, eduardo gueVara2, carMen goMeZ3, leÓn ValdIVIeso1, paul gaMBoa1, Juan MouKarZel2*, oscar MendIZ1
ABSTRACT
Background: The aim of this study was to analyze and report the initial results of a series of patients with severe symptomatic mitral regurgitation (MR) and high surgical risk who underwent percutaneous mitral valve repair (PMVR) with MitraClip™.Methods: Twelve consecutive patients with severe symptomatic MR and high surgical risk or contraindication for surgery under-went PMVR with MitraClip™ between March 2016 and October 2018. Implant success was defined as adequate leaflet grasping, with mild or moderate residual MR at the end of the procedure, and 30-day procedural success as implant success without any major adverse cardiovascular event, including death, acute myocardial infarction (AMI), stroke, need for valve surgery, pericardial effusion, cardiac tamponade or major bleeding.All patients were in functional class III-IV and with history of previous hospitalizations due to heart failure. Echocardiographic find-ings were: left ventricular end-diastolic diameter (LVEDD): 61.8±6.4 mm, left ventricular end-systolic diameter (LVESD): 46.3±2.1 mm and left ventricular ejection fraction (LVEF): 47.5±13.4% (25-60%). The cause of MR was degenerative in 7 patients and func-tional in 5. Risk evaluation showed EuroSCORE of 9.6±6.8, Society of Thoracic Surgeons (STS) mortality score of 16.1±13.5 and STS morbidity and mortality score of 22.8±17.7results: Implant success was achieved in all patients; a single clip was implanted in 7 patients and 2 clips in 5. Mean post-implant residual gradient was 3.6±0.2 mmHg. Post-procedural MR was mild in 11 patients and trivial in one. Mean hospital stay was 1.9 ± 0.8 days (range 1-3 days).At 30 days all patients were in FC I-II and no patient presented major events or readmission for heart failure.Follow-up was performed in all patients for a mean period of 8.8±6.7 months (range1-30 months). Two patients died (1 from pneu-monia 14 months after the procedure and another at 30 months due to refractory heart failure after transcatheter aortic valve implantation (TAVI), preserving mild MR. There were no other complications. All patients were in FC I-II, and one patient required readmission due to heart failure 7 months after the procedure. Echo Doppler at follow-up showed mild MR in 11 patients and moder-ate to severe MR in one. Quality of life improved in all patients.Conclusion: In this initial, single center series that includes the learning curve of the team, PMVR with MitraClip™ in patients with severe symptomatic MR and high surgical risk was safe and effective, with a significant clinical and quality of life improvement during follow-up.
Key words: Edge-to-edge – MitraClip™ – Mitral regurgitation
RESUMEN
objetivos: Reportar y analizar los resultados iniciales de una serie de pacientes con insuficiencia mitral (IM) grave sintomática y alto riesgo para cirugía que recibieron reparación percutánea de la válvula mitral (RPVM) con MitraClip®.Material y métodos: Entre marzo de 2016 y octubre de 2018 recibieron RPVM con MitraClip® en forma consecutiva 12 sujetos con IM grave sintomática, con alto riesgo o contraindicación para cirugía. Se consideró “éxito del implante” (EI) el correcto agarre de las valvas con el clip que dejó una IM residual leve o moderada al finalizar el procedimiento, y “éxito del procedimiento (EP) a 30 días” el EI en ausencia de eventos adversos mayores, los que incluyeron muerte, infarto agudo de miocardio (IAM), accidente cerebrovas-cular (ACV), necesidad de cirugía valvular, derrame pericárdico, taponamiento o sangrado mayor.Todos los pacientes estaban en clase funcional (CF) III-IV, con antecedentes de internaciones por insuficiencia cardíaca (IC). Carac-terísticas ecográficas: diámetro diastólico del ventrículo izquierdo (DDVI): 61,8±6,4 mm; diámetro sistólico (DSVI): 46,3±2,1 mm; fracción de eyección del ventrículo izquierdo (FEVI): 47,5±13,4% (rango: 25-60%). La causa de la IM era degenerativa en 7 pacientes y funcional en 5. La evaluación del riesgo mostró un EuroSCORElog de 9,6±6,8; el STS score de mortalidad fue 16,1±13,5 y el de morbimortalidad 22,8±17,7.resultados: Se obtuvo EI en todos los pacientes; en 7 enfermos se implantó 1 solo clip y en los otros 5 se colocaron 2 clips; el gradi-ente residual medio posimplante fue 3,6±0,2 mmHg. La IM posprocedimiento fue leve en 11 y mínima en 1. La estadía hospitalaria media fue de 1,9±0,8 días (rango: 1-3 días).En el seguimiento, todos los sujetos se encontraban en CF I-II; ningún paciente presentó eventos mayores o reinternación por IC.
REV ARGENT CARDIOL 2019;87:212-218. http://dx.doi.org/10.7775/rac.v87.i3.15252
Received: 12/15/2018 – Accepted: 03/23/2019
Address for reprints: Oscar A. Mendiz. [email protected]. ICyCC-Fundación Favaloro. Avda. Belgrano 1746. 4º Piso. (1093)
Ciudad Autónoma de Buenos Aires. Argentina

213
INTRODUCTIONMitral regurgitation (MR) involves approximately 25% of all prevalent heart valve diseases, (1) and in its advanced stage, is a strong predictor of mortality. (2) Currently, the treatment of choice is mitral valve repair instead of valve replacement surgery, but the number of repair cases with respect to the total num-ber of potential cases where it could be applied is very low and estimated at a rate of 50%. (3) This may be at-tributed to a population with high incidence of comor-bidities, including advanced age, poor left ventricular function, prior cardiac surgery, mediastinal radiother-apy, kidney disease, frailty and other comorbidities that rule out surgery. (4, 5)
In patients at high risk, medical treatment is usu-ally efficient in the early stage of the disease, but, as the disease progresses, ventricular and kidney failure develops which increases readmissions and the risk of death, indicating the need for surgery. However, when this is not feasible, the percutaneous strategy is a val-id option. (6)
The percutaneous treatment aimed at grasping both leaflets, a technique called “edge-to-edge” in the literature, reproduces the surgery introduced by Dr. O. Alfieri several years ago, and is performed with a MitraClip™ device (Abbott Vascular, Santa Clara, Cal-ifornia). The EVEREST II study (7) showed its fea-sibility and safety with a significant improvement in functional class (FC), comparable to surgery at 5-year follow-up, at the expense of greater need for reinter-vention, especially within the first 6 months after the percutaneous treatment.
This clinical study was followed by numerous pub-lications reporting improved results with decreased duration of the procedure due to the “learning curve” both in patient selection as in the procedure itself. Moreover, the development of 3D-Doppler echocardi-ography not only allowed a better selection of cases but has been vital for the optimization of the tech-nique and hence of results.
METHODSFrom March 2016 to October 2018, 12 patients with severe symptomatic MR and high surgical risk or contraindication for surgery, who underwent percutaneous mitral valve re-pair (PMVR) with MitraClip™ were consecutively included in the study. They were all under complete and tolerable op-timal medical treatment.
All the patients underwent 2D-3D transesophageal echo-cardiography (TEE). Regurgitation was assessed according to specific guidelines. (8) Severe organic MR (primary) was defined as that presenting an effective regurgitant orifice area (EROA) ≥0.4 cm2, and functional MR (secondary) as that presenting EROA ≥0.2 cm2. Volumetric images were ac-quired by 3D echocardiography. (9) Patients with flail width ≤15 mm and flail gap ≤10 mm were included for organic MR, and patients with coaptation depth from the mitral annu-lus ≤10 mm and coaptation height between leaflets ≥2 mm were included for functional MR. All patients should have a planimetry-estimated mitral valve area ≥4 cm2 and mean gradient ≤5 mmHg.
The EVEREST study selection criteria were used to evaluate the technical feasibility of the procedure.
Mild or moderate MR at the end of the procedure defined implant success (IS) and procedural success (PS) at 30 days was IS in the absence of major adverse cardiovascular events [death, acute myocardial infarction (AMI), stroke, need for valve surgery, pericardial effusion, cardiac tamponade or major bleeding].
The procedure was performed under general anesthesia using propofol, remifentanil and dexmedetomidine as adju-vant due to the use of TEE.
A right femoral vein access was used. In 10 cases per-cutaneous wound closure was accomplished with Preclose technique (Prostar XL 10 Fr, Abbott Vascular, Santa Clara, California) and in 2 via a compressive cutaneous closure with Vycril 3.0 (using the compressive stitch called “figure-of-8”).
Then, a TEE-guided high transeptal puncture was per-formed and anticoagulation was achieved with sodium hepa-rin 10,000 IU. Subsequently, a Mullins sheath was advanced inserting a 5 Fr pigtail catheter in the left atrium to record the curve and pressures during the procedure, and the 24 Fr MitraClip™ steerable guidewire catheter (SGC).
The procedure was performed under 2D and 3D TEE control and once the correct grasping (>4 mm for each leaf-
EEP Efficacy endpoint
FC Functional class
iS Implant success
KCCQ-12 Kansas City Cardiomyopathy Questionnaire
LVEDD Left ventricular end-diastolic diameter
LVESD Left ventricular end-systolic diameter
Mr Mitral regurgitation
PMVr Percutaneous mitral valve repair
PS Procedural success
SGC Steerable guidewire catheter
tEE Transesophageal echocardiography
abbreviations
El seguimiento abarcó a todos los pacientes y se extendió por un tiempo medio de 8,8±6,7 meses (rango: 1-30 meses). Dos pacientes fallecieron: 1 de neumonía a los 14 meses y otro a los 30 meses por IC refractaria luego de un reemplazo valvular aórtico por cate-terismo (TAVI), manteniendo IM leve. No hubo otras complicaciones. En el seguimiento todos se encontraban en CF I-II, 1 requirió reinternación por IC (a los 7 meses). El eco-Doppler cardíaco de seguimiento demostró IM leve en 11 pacientes y moderada a grave en 1. Hubo una mejoría en la calidad de vida en todos los casos.Conclusiones: En esta serie inicial de un solo centro y que incluye la curva de aprendizaje, la RPVM con MitraClip® en pacientes con IM grave sintomática y alto riesgo quirúrgico fue segura y efectiva, con una mejoría clínica significativa y también en la calidad de vida en el seguimiento.
Palabras clave: Borde-a-borde - MitraClip® - Insuficiencia mitral
percutaneous MItral ValVe repaIr WItH MItraclIp / carlos Fava et al.

ARGENTINE JOURNAL OF CARDIOLOGY / Vol 87 nº 3 / June 2019214
let) and reduction of MR ≤2+ was confirmed, the clip was deployed. In case the maneuver was unsuccessful, a second clip was implanted or as many as necessary.
The pigtail catheter was used to monitor the atrial V wave and pressures to assess the hemodynamic impact of the procedure. Usually, a good leaflet clipping leads to a marked reduction of the left atrial V wave and pressures. Today this may be performed through a lateral port in the new SGC. Also, flow through the pulmonary veins was as-sessed, for a better evaluation of residual MR. Patient qual-ity of life was analyzed before the procedure and at 6-month follow-up with the Kansas City Cardiomyopathy Question-naire (LCCQ). (10)
Follow-up was conducted on-site by the patient’s clinical cardiologist, the interventional cardiologist and the echocardi-ologist. Echo-Doppler was performed at one month, 6 months, one year and thereafter, once a year. After discharge, patients received complete medical therapy at tolerable doses.
Statistical analysisThis was a prospective, observational, non-randomized, sin-gle-center study. Due to the low number of patients, absolute numbers, and mean and standard deviations were used for data analysis.
Ethical considerationsThe procedure was performed under international stand-ards according to the protocol indicated. All patients were explained the procedure, its risks and benefits, all their ques-tions were answered and an informed consent was signed. RESULTSMean age of patients, including 7 men and 5 women was 74.1±8.9 years. The following comorbidities were found: hypertension and dyslipidemia (n=10), atrial fibrillation (n=5), EPOC (n=4), current smok-ers (n=4), prior cardiac surgery (n=4), previous AMI (n=3), diabetes (n=3), prior percutaneous coronary intervention (PCI) (n=2) and permanent pacemak-er (n=2). The estimated glomerular filtration rate (eGFR) was 73.8±34.8 ml/m2; in 2 patients it was < 60 ml/m2 and one patient was in dialysis. No patient presented previous stroke.
All patients were in FC III-IV, with history of hos-pitalizations for heart failure within the previous year. The echocardiogram showed that left ventricular end-diastolic diameter LVEDD was 61.8±6.4 mm, left ven-tricular end-systolic diameter (LVESD) 46.3±2.1 mm and left ventricular ejection fraction (LVEF) 50±11%. Mitral regurgitation was degenerative in 7 patients and functional in 5.
Risk evaluation by the Heart Team showed Eu-roSCORE of 9.6±6.8, Society of Thoracic Surgeons (STS) mortality score of 16.1±13.5 and STS morbidity and mortality score of 22.8±17.7.
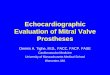
Implant success was attained in all patients (Fig-ure 1 and 2); this was accomplished with the implan-tation of a single clip in 7 patients while 5 patients required 2 clips in the same procedure. Mean post-implant residual valve gradient was 3.6±0.2 mmHg. Post-procedural MR was mild (≤2+) in 11 patients and trivial in one patient. No deaths or AMI, pericardial
effusion, cardiac tamponade, stroke, major bleeding, transfusion, need for reintervention, urgent surgery or conversion to open surgery occurred either during hospitalization or after discharge. Mean hospital stay was 1.9 ± 0.8 days (range 1-3 days).
Procedural success at 30 days was achieved by all patients, as all of them preserved IS free from any major adverse event or readmission for heart failure. They all improved to FC I-II.
Clinical follow-up was conducted in all patients for a mean period of 8.8±6.7 months (range 1-30 months). Two deaths occurred during follow-up: one death due to pneumonia in the 14th month after the procedure and another after transcatheter aortic valve implan-tation (TAVI) at 30 months of follow-up, unrelated to MR or clip failure. No patient suffered from stroke or AMI, or underwent mitral valve surgery or reinter-vention. All patients were in FC I-II (Figure 3); a pa-tient required hospitalization for heart failure due to chronic ventricular dysfunction while preserving MR <2 (the same patient that afterwards received TAVI and died). Follow-up cardiac echo-Doppler showed that 11 patients had mild MR and one moderate to severe MR (Figure 4). Quality of life improved during follow-up (29.09 vs. 48.97 p <0.001) (Figure 5).
DISCUSSIONPercutaneous treatment of severe symptomatic MR in patients at high surgical risk was feasible and safe in this initial series, demonstrating that after a success-ful procedure, hospital stay is short and a significant clinical benefit and improved quality of life is achieved with a low rate of readmissions for heart failure at 30 days and in the short-term follow-up.
The learning curve was reflected in the procedure times which lasted 2 hours in the first cases and ap-proximately 1 hour in the last ones.
The procedure seems complex and the device scarcely friendly at the beginning, with a high de-pendency on the good synchronization between the echocardiologist, the interventional cardiologist and the anesthesiologist.
A good start is of vital importance to achieve a good and easily accessible result. Therefore, the transeptal puncture must be performed under TEE guidance, since a puncture in the inadequate place may compli-cate SGC management and the clip delivery system.
Among the possible complications is partial clip detachment after deployment, as was reported in the first studies. (11) However, this complication has dras-tically decreased with greater operator experience and in our series, it did not occur in any patient.
The correct evaluation of the amount of leaflet tis-sue that has been grasped by the clip arms is done by the echocardiologist, who after ensuring this step, authorizes the interventional cardiologist final clip deployment. In case this step is not certain, the clip should be opened and repositioned.
Although medical treatment in severe secondary

215percutaneous MItral ValVe repaIr WItH MItraclIp / carlos Fava et al.
Fig. 1. Functional severe mi-tral regurgitation (a-b-c) and trivial mitral regurgitation after the implantation of two clips (d-e-f)
Fig. 2. Organic severe mitral regurgitation (a-b-c) and triv-ial mitral regurgitation after the implantation of one clip (d-e)
Fig. 3. Functional class
Baseline 30 days Follow-up
a b c
d e f
99
33
9
3
0
2
4
6
8
10
12
14
IV
III
II
I

ARGENTINE JOURNAL OF CARDIOLOGY / Vol 87 nº 3 / June 2019216
MR with preserved ejection fraction has revealed its effectiveness, these patients have shown high mortal-ity with the passage of time, as reported by Barakat et al., (12) who analyzed 400 patients with severe MR and LVEF ≥60%. In the 12-month and 3-year follow-up period, mortality was 19.1% and 26.3%, respective-ly. In addition, these patients required more frequent hospitalizations for heart failure and greater need of transapical ablation for atrial fibrillation, cardiac re-synchronization therapy, angioplasty, ventricular as-sist devices or heart transplantation.
As already stated, guidelines recommend valve re-pair or replacement surgeries for patients with severe symptomatic MR, but the number of patients effec-tively undergoing surgery are few compared with the potential cases carrying the disease. (14)
To reduce this deficit and offer a less invasive treat-ment, different technologies have been developed for transapical mitral valve repair or valve replacement surgery. MitraClip™ is one of the first and most used device, which has been employed in >60,000 cases
worldwide up to 2017, and is also the first registered in a randomized study versus surgery.
The EVEREST II study (6) was the first study analyzing this strategy versus surgery in 279 patients randomized in a 2:1 ratio. The study showed that, in the initial stage, patients receiving MitraClip™ had less complications, especially bleeding, but required more surgery within the first 6 months. In the 5-year follow-up, the composite endpoint of survival free from mortality, surgery and severe MR was 44.2% vs. 64.3% (p=0.01) in favor of surgery. This was the con-sequence of greater incidence of MR 3+ or 4+ (12.3% vs. 1.8%; p=0.02) and the need for surgery (27.9% vs. 8.9%; p=0.003). Surgery after MitraClip™ was with-in the first 6 months in most cases (78%); after this period, the evolution was similar in both groups. No difference was found in 5-year mortality (20.8% vs. 26.8%), and FC and quality of life were preserved.
It is interesting to point out that when this clinical study was carried out, 3D TEE was not available in daily practice, which may have influenced in the re-
Fig. 4. Baseline and follow-up echo-Doppler: mitral regurgi-tation
Fig. 5. Quality of life evolution. KCCQ at 6 months
1
11
11
9
1
3
0
2
4
6
8
10
12
14
4+
3+
=2+
=1
Baseline 30 days Follow-up
Baseline
Follow-up
P<0.001
29.1
49

217
sults. Similarly, the technique employed has changed, as the use of multiple clips to achieve maximal reduc-tion of MR.
Kortlandt et al. (15) performed a very interest-ing analysis comparing the outcome of 1,036 patients with symptomatic MR; 568 received MitraClip™, 173 surgery and 295 medical treatment. Although clinical characteristics were similar, those receiving MitraClip had lower LVEF and higher surgical risk scores (STS 7.7 for MitraClip™, 2.7 for surgery and 3.5 for medi-cal treatment). In the 5-year follow-up, survival was lower in patients receiving medical treatment and was similar in those receiving MitraClip™ or surgery, but we must take into account that patients receiving the percutaneous treatment were older, had lower left ventricular function and greater surgical risk.Patients at high surgical risk, as the ones in our se-ries, generate great management difficulty and this was analyzed in the EVEREST II High Risk Registry study, (16) which included 351 patients with STS >12. An important reduction of MR was found at one-year follow-up, with 84% of patients presenting MR ≤2+. Also, there was a significant reduction of ventricular diameters, 83% were in FC I-II, and this was accom-panied by a decreased need of readmissions for heart failure and improved quality of life and mental health status tests. Survival free from mortality was 77.2% and from mitral valve surgery 97.8%.
One of the great challenges presented by either functional or secondary severe MR treatment is asso-ciated with left ventricular dysfunction. Even though previous studies have reported a similar outcome but with more readmissions due to heart failure in the group treated with conventional medical therapy, (17, 18) there are currently two randomized studies ana-lyzing the percutaneous invasive strategy and the con-ventional medical therapy.
The first is the MITRA FR study (19) including 152 symptomatic patients with secondary MR divided into two groups: MitraClip™ + medical therapy vs. optimal medical treatment alone. The primary effica-cy endpoint (EEP) was all-cause death and unplanned readmission for heart failure at 12 months. Mean age was 70 years and the rest of patient characteristics were similar in both groups: LVEF was 33%, EROA 31 mm2 and EuroSCORE II predicted risk 6. Implant success was 95.8% in all cases. At one-year follow-up, EEP was similar in both treatment groups (54.6% vs. 51.3%, p=0.53), and neither were differences found in mortality nor in new readmissions for heart failure.
We must take into account that in this study there was an important loss of echocardiographic, BNP dos-age, quality of life and clinical outcome data in the one-year follow-up period. Also, the minimum re-quirement for operators was 5 previous cases, though expert assistance (proctoring) was allowed.
The other important study is the COAPT trial, which randomized 614 patients with symptomatic moderate or severe MR and high surgical risk (STS
score >8): 302 patients received MitralClip™ and 312 optimal medical treatment. The EEP was all the hos-pitalizations for heart failure within 24 months. There was no difference between the two groups in terms of age (71 years), atrial fibrillation (present in more than 50% of patients) and ischemic etiology (60%). Left ventricular ejection fraction was 31.3% and EROA 40 mm2. Implant success was 97%. The EEP favored those receiving MitralClip™ (35.8 vs. 67.9, p <0.001; HR=0.53, 95% CI 0.40-0.70, p <0.001), with a number needed to treat at 24 months (NNT24 m)=3.1 (95% CI 1.9-8.2). In addition, this group presented lower mortal-ity (29.1% vs. 46.1%, p <0.001; HR=0.62, 95% CI 0.46-0.82, p <0.001) with NNT24m=5.9 (95% CI 3.9-11.7) and significant improvement in FC, quality of life and the 6-minute walk test. In the echocardiographic analy-sis, MitralClip™ treatment showed better left ventricu-lar function, lower MR and enhanced left ventricular remodeling. The invasive treatment also decreased the need for ventricular assistance or heart transplanta-tion during follow-up (4.4% vs. 9.5% HR=0.37, 95% CI 0.17-0.81, p=0.01). It should be pointed out that one third of patients in the medical treatment group also received resynchronization therapy.
There are several possible explanations for the dif-ferences between these two studies, much discussed in the medical community. First, the medical treat-ment in the COAPT trial was in charge of heart fail-ure specialists, and patients received medical therapy at maximum tolerated doses before randomization, so patients with refractory severe MR were the ones who entered the study, a situation not present in the MITRA FR study. Also patients in the MITRA FR study presented less heart failure (FC I-II), more hos-pitalizations for heart failure, higher BNP levels and larger end-diastolic volume. Second, EROA was high-er in the COAPT trial (41±15 mm2 vs. 31±10 mm2) with a lower end-diastolic volume and third, a greater number of patients received more than one clip in the COAPT trial. (20)
In addition, some analyses have demonstrated that it is very important to surgically treat patients before ventricular function impairment and ventricular dila-tion begin, since it has been shown that they lead to the emergence of kidney failure (21) and atrial fibril-lation, (22) generating a strong negative impact on the prognosis.
Although it has been demonstrated that MR ≥+2 is associated with poor clinical outcome, we should not forget the residual gradient after implantation. This was analyzed by Neuss et al., (23) who evaluated 200 patients, 50 of whom presented a post MitralClip™ implant gradient >5 mmHg. They observed that there were no differences in baseline clinical characteristics of the two groups; however, the Kaplan-Meier analysis during follow-up showed higher mortality when the gradient measured invasively was >5 mmHg or >4.4 mmHg when it was measured by echocardiography. Therefore, the number of clips to implant to eliminate
percutaneous MItral ValVe repaIr WItH MItraclIp / carlos Fava et al.

ARGENTINE JOURNAL OF CARDIOLOGY / Vol 87 nº 3 / June 2019218
1. Iung B, Baron G, Butchart E, Delahaye F, Gohlke-Bärwolf C, Levang O. A prospective survey of patients with valvular heart dis-ease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J 2003;24:1231-43. http://doi.org/cphdzn2. Trichon BH, Felker GM, Shaw LK. Relation of frequency and se-verity of mitral regurgitation to survival among patients with left ventricular systolic dysfunction and heart failure. Am J Cardiol 2003;91:538-43. http://doi.org/cp556k3. Vesely MR, Benitez RM, Robinson SW, Collins JA, Dawood MY, Gammie JS. Surgical and Transcatheter Mitral Valve Repair for Se-vere Chronic Mitral Regurgitation: A Review of Clinical Indications and Patient Assessment. J Am Heart Assoc. 2015;4(12). pii: e002424 http://doi.org/c68x4. Metze C, Matzik AS, Scherner M, Körber MI, Michels G, Baldus S. Impact of Frailty on Outcomes in Patients Undergoing Percuta-neous Mitral Valve Repair. J Am Coll Cardiol Intv 2017;10:1920-9. http://doi.org/gb2k3r5. Borger M, Alam A, Murphy P, Doenst T, David T. Chronic ischemic mitral regurgitation: repair, replace or rethink? Ann Thorac Surg 2006;81:1153-61. http://doi.org/bhw3ms6. Kortlandt F, Velu J, Schurer R, Hendriks T, Van den Branden B, Bouma B, et al. Survival After MitraClip Treatment Compared to Surgical and Conservative Treatment for High-Surgical-Risk Patients With Mitral Regurgitation. Circ Cardiovasc Interv 2018 Jun;11(6):e005985. http://doi.org/c68z7. Feldman T, Kar S, Elmariah S, Smart S, Trento A, Siegel R. Ran-domized Comparison of Percutaneous Repair and Surgery for Mi-tral Regurgitation 5-Year Results of EVEREST II. J Am Coll Cardiol
REFERENCES
or maximally reduce MR is based on this residual gra-dient. In our series, mean gradient at the end of the procedure was 3.6±0.2 mmHg and in no case was it above 5 mmHg.
Secondary MR due to left ventricular dilation is associated with mitral annulus dilation; in this case, PMVR is performed using a prosthetic mitral annulus together with valve and subvalvular apparatus repair. Probably, with further technological development, percutaneous mitral annuli associated to clips will be available to treat this group of patients in whom potential annulus dilation might hamper the initial result achieved.
In our group, with a minimalist approach for valve or aortic repair, we have tried to maximally reduce in-vasiveness in these patients. Thus, even though gener-al anesthesia is very necessary for patients’ wellbeing and to tolerate the echocardiographic transesopha-geal probe for a long period, we have limited the use of central lines or urinary bladder catheters, as this provides more comfort to the patients as well as early deambulation.
CONCLUSIONIn this initial, single-center series, PMVR with Mitra-Clip™ in patients with severe symptomatic MR and high surgical risk was feasible and safe, with a signifi-cant clinical improvement at 30 days and enhanced quality of life during follow-up. These findings, which include the learning curve of all the team, show re-sults similar to those of large international series.
Conflicts of interestNone declared. (See authors’ conflicts of interest forms on the website/Supplementary material).
2015;66:2844-54. http://doi.org/c6828. Lancellotti P, Tribouilloy C, Hagendorff A, Popescu B, Edvardsen T, Pierard L, et al. Recommendations for the echocardiographic as-sessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2013;14:611-44. http://doi.org/bk289. Lang R, Badano L, Tsang W, Adams D, Agricola E, Buck T, et al. Recommendations for Image Acquisition and Display Using Three-Dimensional Echocardiography. 2012. J Am Soc Echocardiogr 2012;25:3-46. http://doi.org/dt5z3f10. Spertus J, Jones P. Development and Validation of a Short Ver-sion of the Kansas City Cardiomyopathy Questionnaire. Circ Car-diovasc Qual Outcomes. 2015;8:469-76. http://doi.org/c68311. Feldman T, Kar S, Rinaldi M, Fail P, Hermiller J, Smalling R, et al. Percutaneous Mitral Repair With the MitraClip System. Safety and Midterm Durability in the Initial EVEREST (Endovascular Valve Edge-to-Edge Repair Study) Cohort. J Am Coll Cardiol 2009;54:686-94. http://doi.org/bwqf9712. Barakat A, Raza M, Banerjee K, Tsutsui R, Mentias A, Abdur Rehman K et al. Long-term mortality in patients with severe second-ary mitral regurgitation and normal left ventricular ejection frac-tion: interventional perspective. EuroIntervention 2018;13:1881-8. http://doi.org/gc5vz413. Baumgartner H, Falk V, Bax J, De Bonis M, Hamm C, Holmet P, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. The Task Force for the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the Euro-pean Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2017;38:2739-91.14. Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Détaint D, Vanoverschelde JL, et al. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied sur-gery? Eur Heart J 2007;28:1358-65. http://doi.org/dhp23k15. Kortlandt F, Velu J, Schurer R, Hendriks T, Van den Bran-den B, Bouma B, et al. Survival After MitraClip Treatment Com-pared to Surgical and Conservative Treatment for High-Surgical-Risk Patients With Mitral Regurgitation. Circ Cardiovasc Interv 2018;11:e005985. http://doi.org/c68z16. Glower D, Kar S, Trento A, Lim S, Bajwa T, Quesada R, et al. Percutaneous Mitral Valve Repair in High Risk Patients. Results of the EVEREST II Study. J Am Coll Cardiol 2014;64:172-81. http://doi.org/f2sxfd17. Nickenig G, Estevez-Loureiro R, Franzen O, Tamburino C, Van-derheyden M, Luscher TF, et al. Percutaneous Mitral Valve Repair Edge-to-Edge Repair. In-Hospital Results and 1-Year Follow-Up of 628 Patients of the 2011-2012 Pilot European Sentinel Registry. J Am Coll Cardiol 2014;64:875-84.18. Nickenig G, Estevez-Loureiro R, Franzen O, Tamburino C, Van-derheyden M, Luscher T, et al. Percutaneous Mitral Valve Repair Edge-to-Edge Repair. In-Hospital Results and 1-Year Follow-Up of 628 Patients of the 2011-2012 Pilot European Sentinel Registry. J Am Coll Cardiol 2014;64:875-84. http://doi.org/f2tqjt19. Obadia JF, Messika-Zeitoun D, Leurent G, Iung B, Bonnet G, Piriou N, et al. Percutaneous Repair or Medical Treatment for Sec-ondary Mitral Regurgitation. N Engl J Med 2018 13;379:2297-306. http://doi.org/gfj3wd20. Nishimura, R, Bonow R. Percutaneous Repair of Secondary Mi-tral Regurgitation. A Tale of Two Trial. N Engl J Med 2018;379:2374-6. http://doi.org/c68421. Schueler R, Nickenig G, May A, Schillinger W, Bekeredjian R, Ouarrak T, et al. Predictors for short-term outcomes of patients un-dergoing transcatheter mitral valve interventions: analysis of 778 prospective patients from the German TRAMI registry focusing on baseline renal function. EuroIntervention 2016;12:508-14. http://doi.org/f8xzd522. Jabs A, von Bardeleben R, Boekstegers P, Puls M, Lubos E, Bekeredjian R, et al. Effects of atrial fibrillation and heart rate on percutaneous mitral valve repair with MitraClip: results from the TRAnscatheter Mitral valve Interventions (TRAMI) registry. Euro-Intervention 2017;12:1697-705. http://doi.org/f9q5k223. Neuss M, Schau T, Isotani A, Pilz M, Schöpp M, Butter C. El-evated Mitral Valve Pressure Gradient After MitraClip Implantation Deteriorates Long-Term Outcomes With Severe Mitral Regurgita-tion and Severe Heart Failure. J Am Coll Cardiol Intv 2017;10:931-9. http://doi.org/c685
















![Percutaneous Intervention in Mitral Valve Disease · Prediction of Long-Term Results of PMC HR [95% CI] p Points Age (y) and final mitral valve area (cm²)](https://img.pdfslide.net/doc/110x75/604f6e9825a32966b043f04d/percutaneous-intervention-in-mitral-valve-disease-prediction-of-long-term-results.jpg)