Embed Size (px)
Citation preview
Peri Operative Management of Anti Coagulation
Dr Nihar Pandit September 14th, 2013
Consultant, General Medicine Tan Tock Seng Hospital

Objectives
To understand the characteristics of the patient population requiring peri-operative anti coagulation
To help decide between the perioperative risk of thrombosis Versus the risk of bleeding
To familiarize with the available protocols
‘Bridging Anticoagulation’
Substitution of another anti coagulant (typically Heparin derivative) when Warfarin is interrupted for an
invasive procedure.
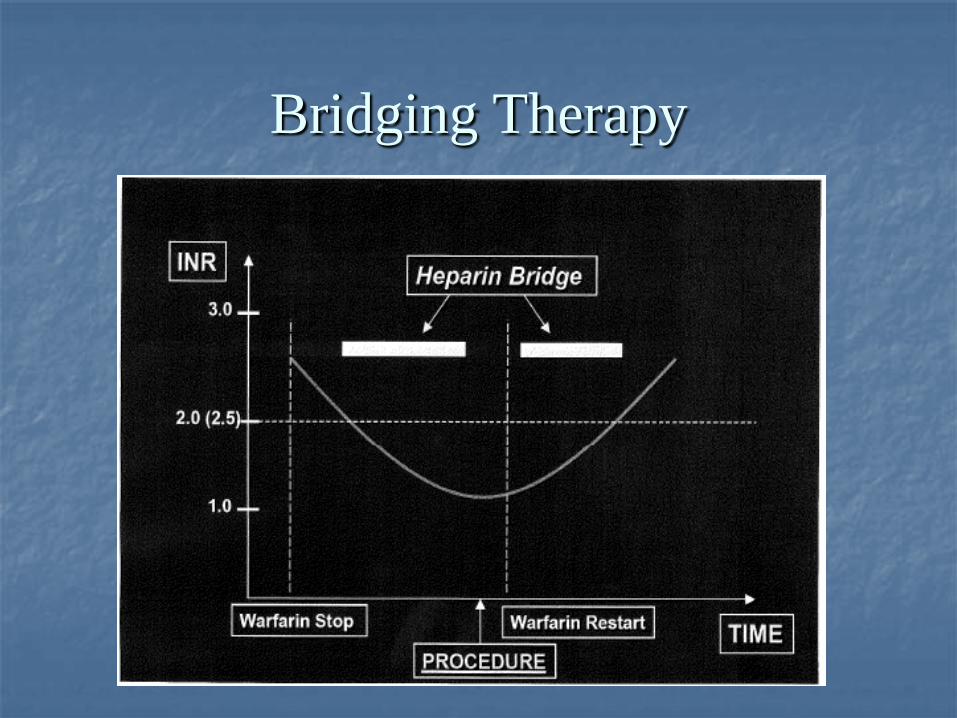
Bridging Therapy

Cross Coverage to Therapeutic INR
Requiring AC but have not achieved
Therapeutic INR Peri-procedural:
RATIONALE FOR BRIDGING
Already Rxed w chronic AC and
now documented drop in INR
mechanical heart valves
A Fib w risk factors for emboli
recent VTE (< 3 months)
hypercoaguable states
BENEFITS Supporting Need for
Bridge Therapy
high risk for thrombosis when patients remain unprotected for several days peri-procedure
Subtherapeutic INR offers little or no protection
Possible rebound hypercoaguable state, especially when warfarin reinitiated leading to thrombosis
Bleeding complications can be controlled while stroke or PE may have lasting effect
New drugs and new data offer increased ease of therapy
Expert Opinion on Bridge Therapy
British Society of Hematology
American College of Chest Physicians (ACCP)
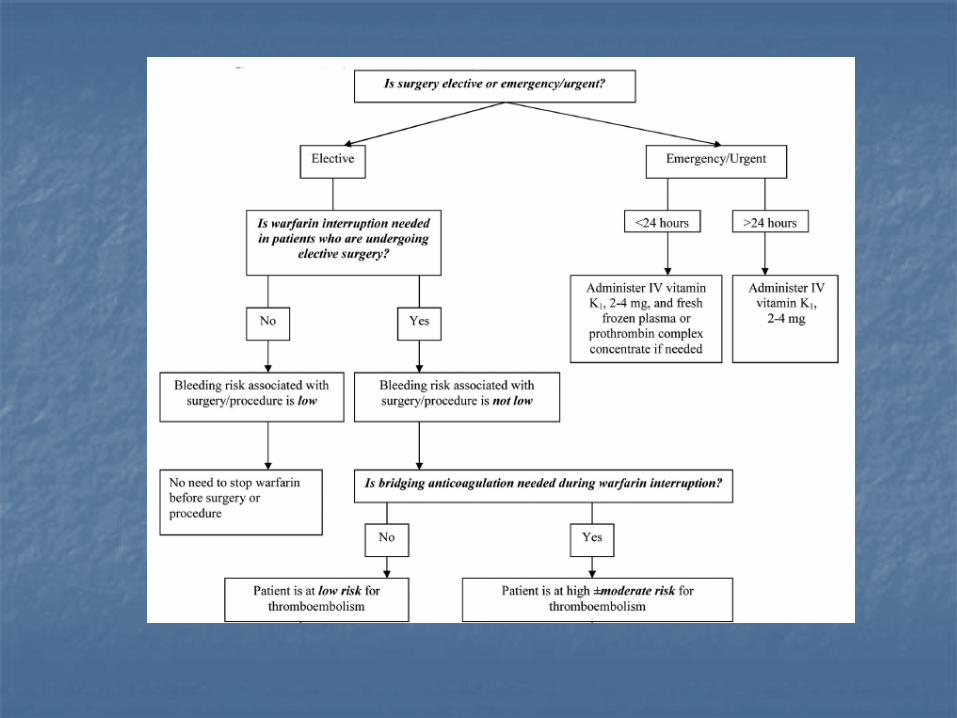
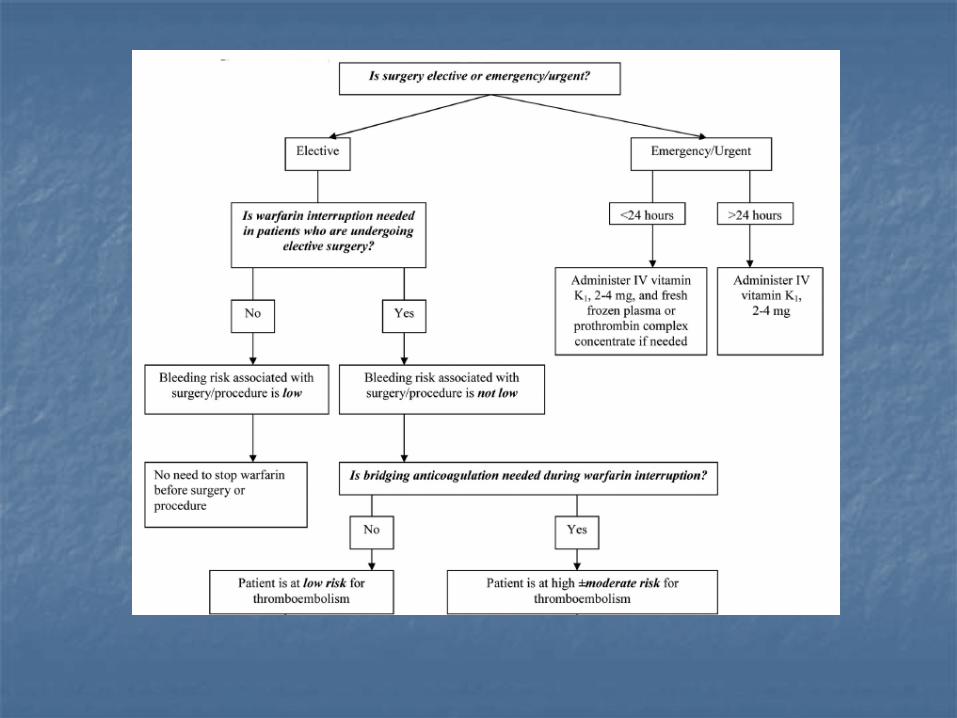
Does the surgery matter ?
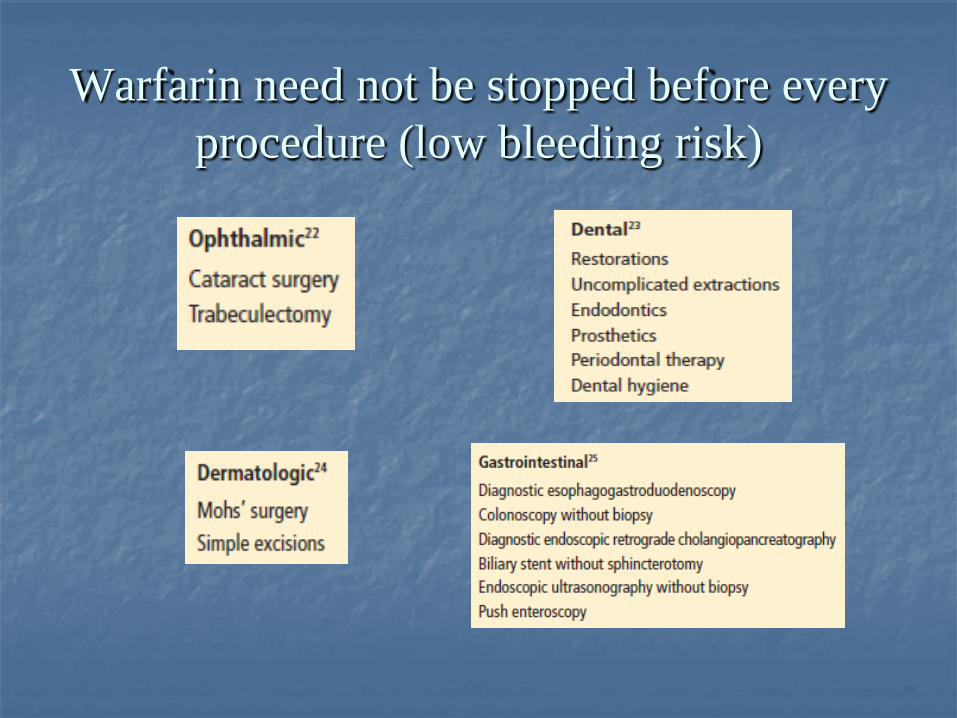
Warfarin need not be stopped before every procedure (low bleeding risk)
For surgeries in which the bleeding Risk is not low …
Common indications for anti coagulation
1. Atrial Fibrillation 2. Deep Vein Thrombosis and Pulmonary Embolism (VTE) 3. Mechanical Heart Valves (MHV)
Atrial Fibrillation
A 77 year old man having a history of Hypertension, Atrial fibrillation and Diabetes Mellitus is scheduled to undergo TURP for BPH. He has no history of CVA or CCF
What would you advise: 1. Stop Warfarin 5 days before the procedure, give therapeutic
dose LMWH pre and post op 2. Continue Warfarin without dose reduction 3. Stop Warfarin 2 days before the procedure and resume 2
days later 4. Stop Warfarin 5 days before and resume 1 week post op
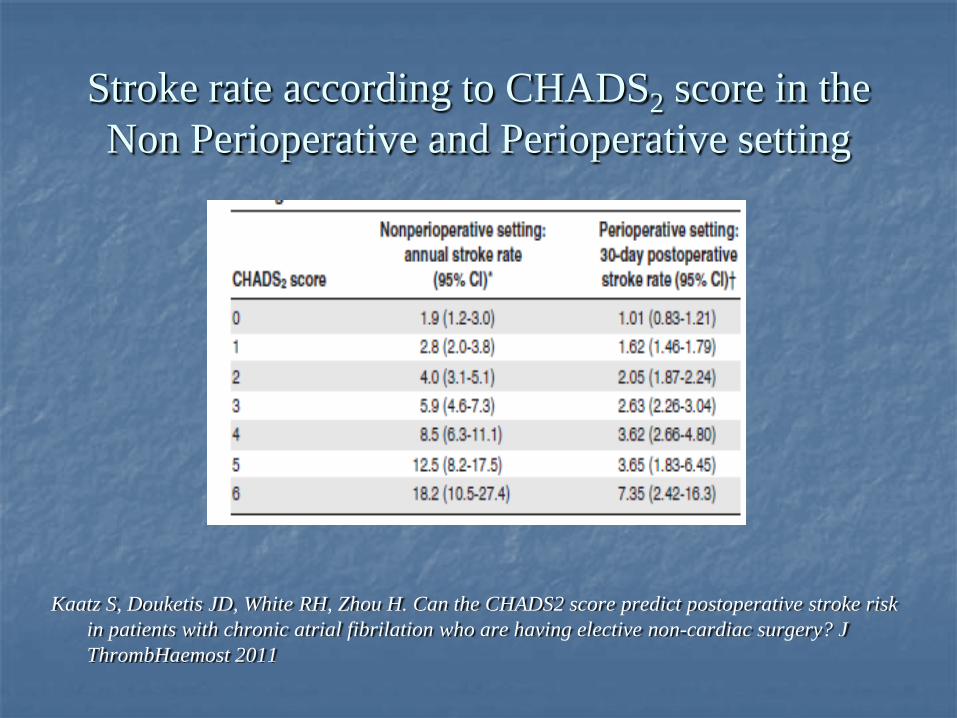
Stroke rate according to CHADS2 score in the Non Perioperative and Perioperative setting
Kaatz S, Douketis JD, White RH, Zhou H. Can the CHADS2 score predict postoperative stroke risk in patients with chronic atrial fibrilation who are having elective non-cardiac surgery? J ThrombHaemost 2011

Bridging Therapy for A fib
Risk Characteristics Bridging Therapy High Any of the following:
CHADS2 3-6 Previous CVA or TIA Intra Cardiac thrombus
Rheumatic Afib
Yes
Low CHADS2 0-2 And no CVA or TIA
No
Wysokinski et al Mayo Clinic Proc, June 2008; 83(6), 639- 645 Chest June 2008 133:6 suppl 299S- 339S
VTE 72 year old woman has been taking Warfarin for DVT and PE
five years ago. She has no known Cancer or thrombophilia. She is scheduled for THR for Degenerative Joint disease. What would you advise this patient ? 1. Stop Warfarin 5 days pre-op and administer therapeutic dose
LMWH pre-op and post-op 2. Stop Warfarin 5 days pre-op and administer low dose
LMWH pre and post-op 3. Continue Warfarin but reduce the dose 50% pre-op 4. Stop Warfarin 5 days pre-op and resume post-op with
Warfarin and LMWH.

Bridging Therapy for VTE
Risk Level
Characteristics Bridging Therapy
High One of the following: Severe thrombophilia
Active Cancer or cancer treatment Recurrent VTE
Recent VTE within 3 months
Yes
Low Last VTE > 3 months ago and no additional risk factors
No
McBane et al, Arterioscler Thromb Vasc Bio, June 2010, 30: 442- 448 Chest June 2008 133:6 suppl 299S- 339S
What is severe Thrombophilia?
Protein C or Protein S deficiency
Antithrombin III deficiency
Antiphospholipid antibodies Multiple defects, homozygous Factor V Leiden or
Prothrombin gene 20210 mutation
Mechanical Heart Valve
62 year old gentleman with a St Jude (Bileaflet) Mechanical AV and Afib but no prior thromboembolism, Rheumatic heart disease or CCF.
He is scheduled for partial colectomy for colon cancer.
Would you give this patient bridging ? Yes ? No ?

Thrombosis risk of Mechanical Heart Valves (MHV) without Anti coagulation
Characteristic Low Risk High Risk Number of Valves Single Multiple
Position of valve Aortic Mitral
Type of valve Bi leaflet Tilting disc and Caged ball
Other A fib, low EF,
prior embolism
Cannegleter et al, Circulation; 1994, 89: 635- 641
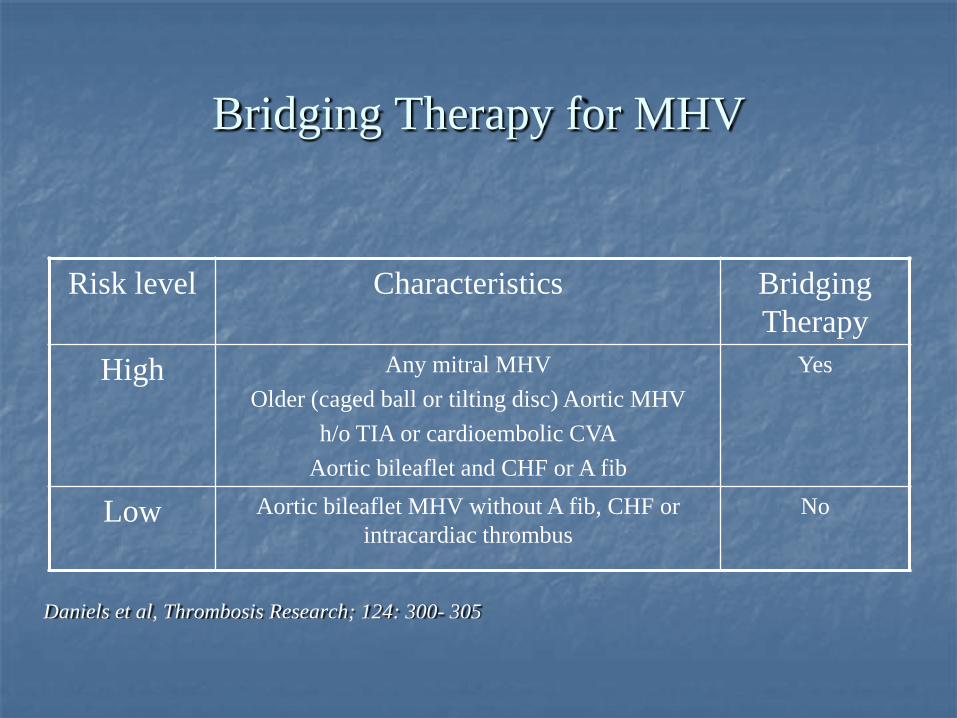
Bridging Therapy for MHV
Risk level Characteristics Bridging Therapy
High Any mitral MHV Older (caged ball or tilting disc) Aortic MHV
h/o TIA or cardioembolic CVA Aortic bileaflet and CHF or A fib
Yes
Low Aortic bileaflet MHV without A fib, CHF or intracardiac thrombus
No
Daniels et al, Thrombosis Research; 124: 300- 305
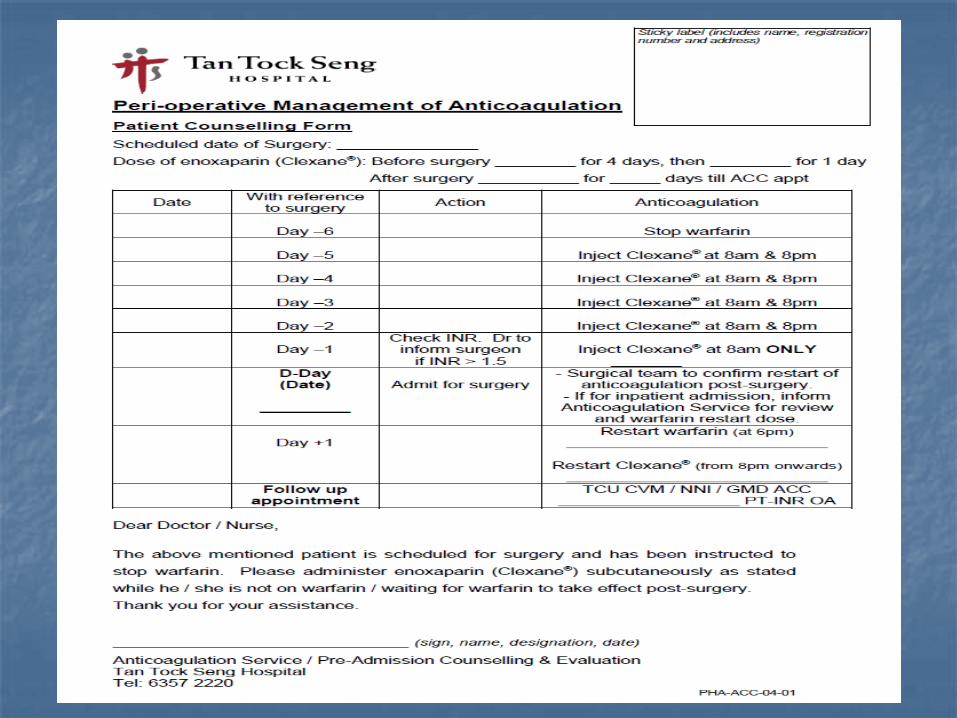
Pre procedure management for those requiring interruption of Warfarin
Stop Warfarin 5 days before the procedure
Check INR One day prior to the procedure, ensuring <1.3
Pre procedure LMWH/ UFH dosing for Bridging (if given)
Start LMWH when INR below the therapeutic range
- Enoxaparin: 1 mg/kg SC q 12 hours - Enoxaparin 1.5 mg/kg SC q 24 hour
Last dose of LMWH given
24 hours before the procedure
- Enoxaparin 1 mg/kg 24 hours before the procedure
UFH: Start Heparin when INR below the therapeutic range
- Discontinue UFH 4-6 hours before the procedure
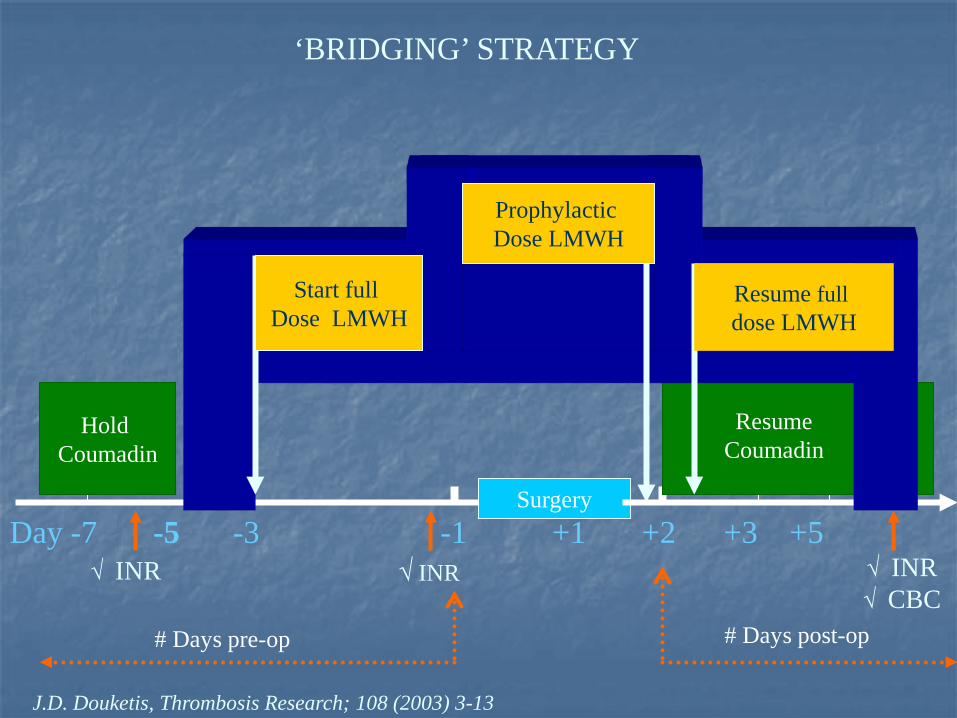
Day -7 -5 -3 -1 +1 +2 +3 +5
Surgery
√ INR √ CBC
√ INR
Hold Coumadin
J.D. Douketis, Thrombosis Research; 108 (2003) 3-13
√ INR
Coumadin
‘BRIDGING’ STRATEGY
# Days pre-op # Days post-op
Resume Coumadin
Start full Dose LMWH
Resume full dose LMWH
Prophylactic Dose LMWH
How and when do we restart Anticoagulation after a procedure?
Depends on the risk of post procedure bleeding Consider the procedure: Is it a major surgery Is the operative site observable or compressible? Is it neuraxial anaesthesia? Consider the patient: Does the patient have any issues with hemostasis? Does the patient have a history of bleeding ?

Classifying Bleeding Risk of procedures:
High risk Cardiovascular surgery- Valve replacement, CABG, AAA repair Cancer surgery, Neuro surgery Intra abdominal surgery Others: TKA, laminectomy, TURP, Kidney biopsy
Non High Risk
All others
Douketic et al, Arch Internal Med. 2004; 164: 1319- 1326
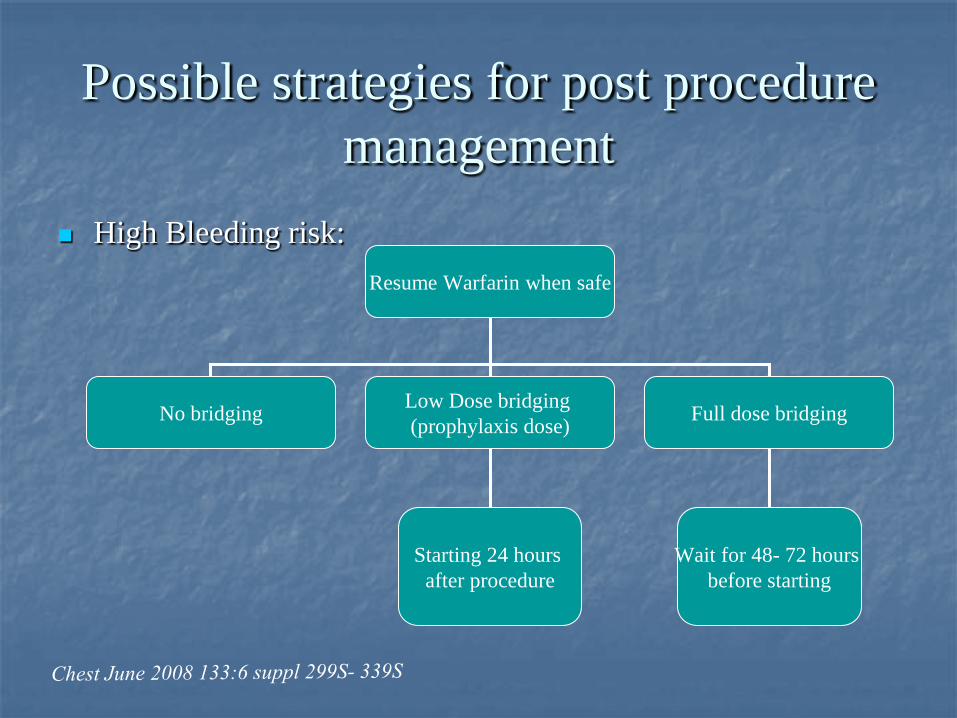
Possible strategies for post procedure management
High Bleeding risk:
Resume Warfarin when safe
No bridging Low Dose bridging (prophylaxis dose) Full dose bridging
Starting 24 hours after procedure
Wait for 48- 72 hours before starting
Low dose versus Full dose bridging Heparin
Low dose Thromboprophylaxis dosing of LMWH or UFH Not specifically studied- could reduce thrombosis yet mitigate
post procedure bleeding Full dose Therapeutic bridging – treatment doses Enoxaparin 1.5mg/kg every 24 hours
Which is to be used ? LMWH or UFH ?
REGIMEN REGISTRY
Multicenter Observational Study Compared safety and efficacy of UFH Versus LMWH as
bridging anticoagulants

REGIMEN REGISTRY Outcome % with outcome in each group
UFH (N= 164) LMWH (N= 668)
ATE 2.4 0.6
VTE 0 0.3
Major bleed 5.5 3.3
Minor bleed 9.1 12
Death 1.2 0.6
LoS 10.3 4.6
Days of heparin 6.8 8.6
Spyropoulos et al, Journ Throm and Hemostasis, 2006; 4: 1246: 1252
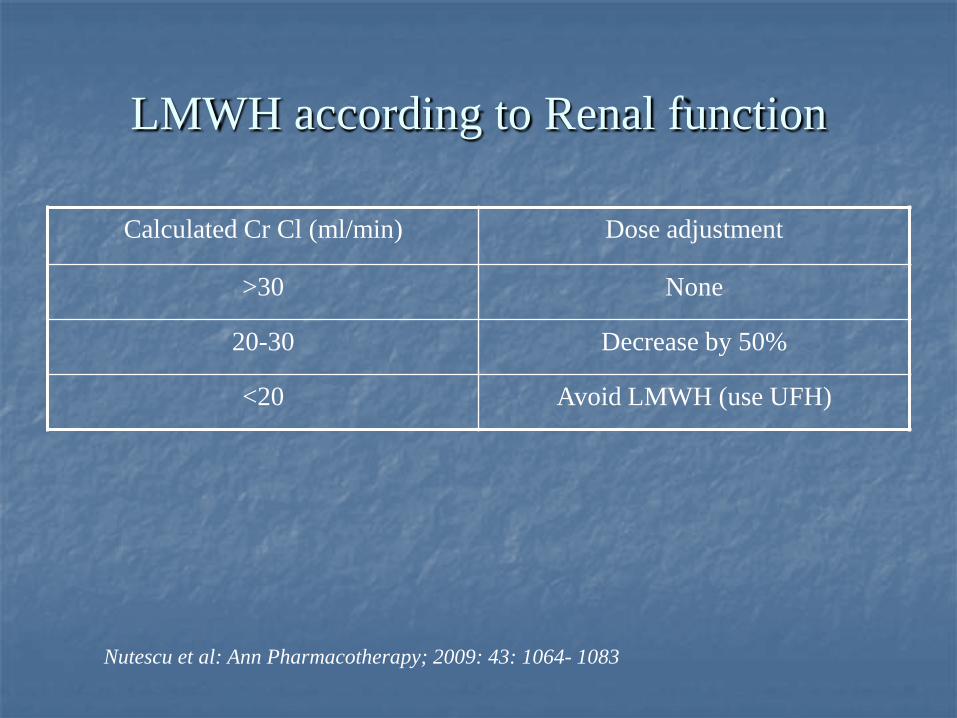
LMWH according to Renal function
Calculated Cr Cl (ml/min) Dose adjustment
>30 None
20-30 Decrease by 50%
<20 Avoid LMWH (use UFH)
Nutescu et al: Ann Pharmacotherapy; 2009: 43: 1064- 1083

Post procedure Warfarin dosing
Resume at the dose the patient was stable pre- procedure
CAUTION: More senstitive to Warfarin after a procedure due to NBM,
Antibiotics, so may require a lower dose at re-initiation and a closer monitoring of the INR
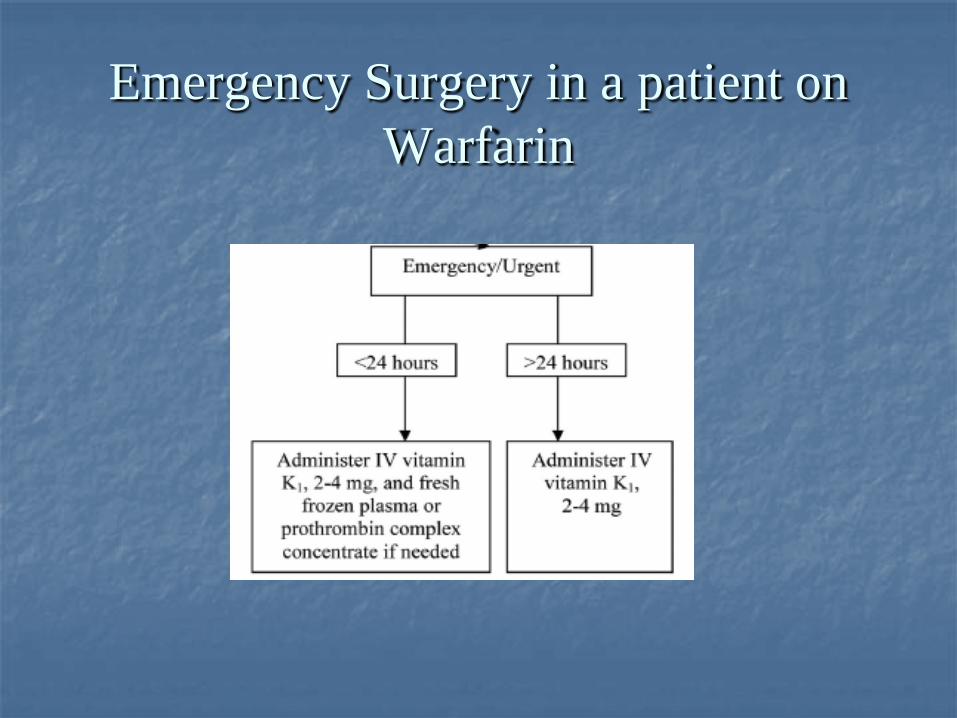
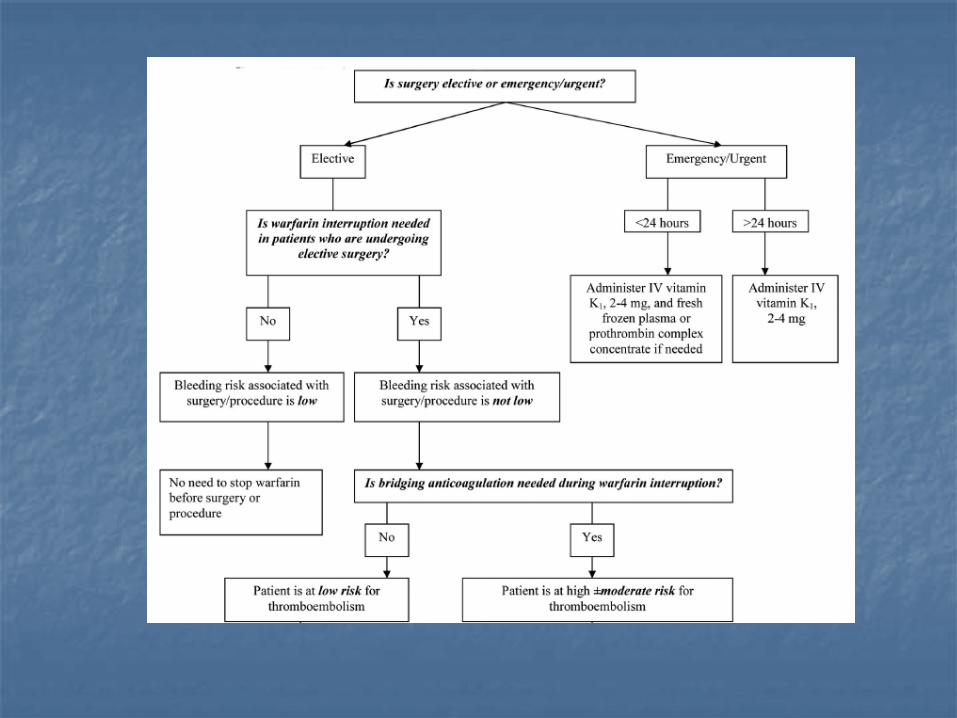
Emergency Surgery in a patient on Warfarin
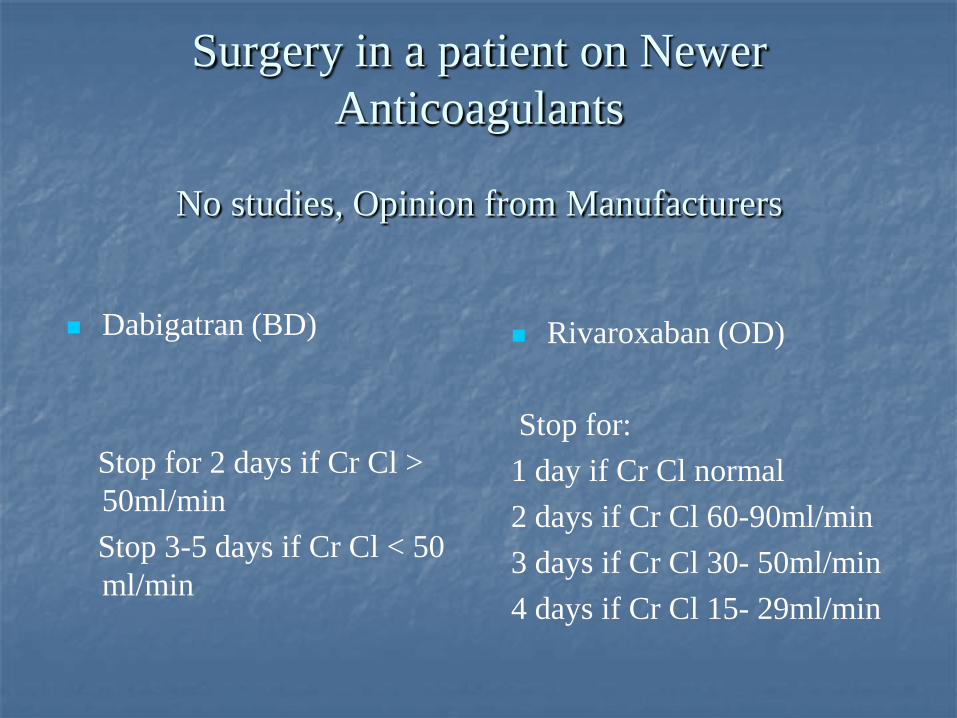
Surgery in a patient on Newer Anticoagulants
No studies, Opinion from Manufacturers
Dabigatran (BD) Stop for 2 days if Cr Cl >
50ml/min Stop 3-5 days if Cr Cl < 50
ml/min
Rivaroxaban (OD) Stop for: 1 day if Cr Cl normal 2 days if Cr Cl 60-90ml/min 3 days if Cr Cl 30- 50ml/min 4 days if Cr Cl 15- 29ml/min
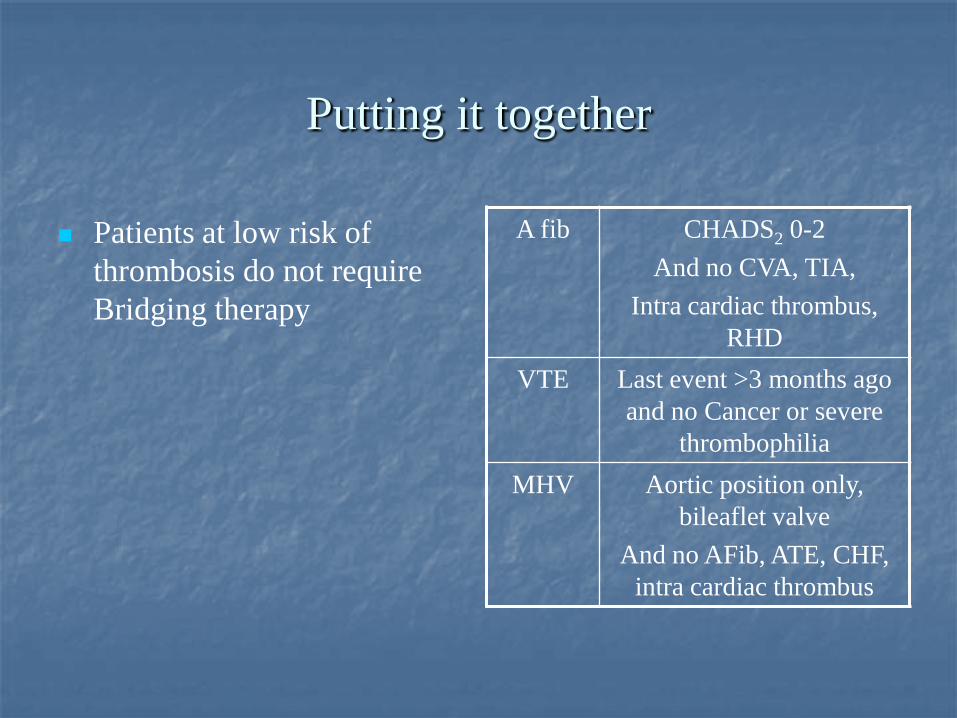
Putting it together
Patients at low risk of thrombosis do not require Bridging therapy
A fib CHADS2 0-2 And no CVA, TIA,
Intra cardiac thrombus, RHD
VTE Last event >3 months ago and no Cancer or severe
thrombophilia MHV Aortic position only,
bileaflet valve And no AFib, ATE, CHF,
intra cardiac thrombus
Putting it together
LMWH is advised for bridging therapy – need to be aware of
Renal function
Last dose of LMWH is 24 hours before the procedure, this dose is half the usual full daily dose

Timing of Post Procedure Anti coagulation (assuming adequate Hemostasis)
Thrombosis Risk level Warfarin Heparin
Low 12-24 hrs post procedure
NA
High 12-24 hrs post procedure
Low bleeding risk: 24 hrs post procedure
High Bleeding Risk: 1. no bridging or
2. low dose bridging or 3. Full bridging 48- 72 hrs
post procedure
Atrial Fibrillation
A 77 year old man having a history of Hypertension, Atrial fibrillation and Diabetes Mellitus is scheduled to undergo TURP for BPH. He has no history of CVA or CCF
What would you advise: 1. Stop Warfarin 5 days before the procedure, give therapeutic
dose LMWH pre and post op 2. Continue Warfarin without dose reduction 3. Stop Warfarin 2 days before the procedure and resume 2
days later 4. Stop Warfarin 5 days before and resume 1 week post op
CHADS2 score is 3 Risk for perioperative ATE is high
He would be a candidate for bridging LMWH (provided Cr Cl >20 mls/min) Anticoagulation could be resumed: Warfarin 12- 24 hours post procedure Heparin 48-72 hrs post procedure prophylactic dose 24 hrs post procedure (?benefit)
VTE 72 year old woman has been taking Warfarin for DVT and PE
five years ago. She has no known Cancer or thrombophilia. She is scheduled for THR for Degenerative Joint disease. What would you advise this patient ? 1. Stop Warfarin 5 days pre-op and administer therapeutic dose
LMWH pre-op and post-op 2. Stop Warfarin 5 days pre-op and administer low dose
LMWH pre and post-op 3. Continue Warfarin but reduce the dose 50% pre-op 4. Stop Warfarin 5 days pre-op and resume post-op with
Warfarin and LMWH.
No known thrombophilia or Cancer Last VTE was >3 months ago
Low risk of Perioperative VTE Not a candidate for pre-operative bridging Post operative Anti coagualtion with Warfarin 12- 24 hours
after the procedure and LMWH

Mechanical Heart Valve
62 year old gentleman with a St Jude Bileaflet Mechanical AV and Afib but no prior thromboembolism, Rheumatic heart disease or CCF.
He is scheduled for partial colectomy for colon cancer.
Would you give this patient bridging ? Yes ? No ?

Single (Aortic) MHV Bileaflet (low risk)
However he has Afib which places him in a high risk category
and hence would be a candidate for Bridging.
Thank you













![PRODUCT MONOGRAPH · 2020. 9. 8. · FEIBA NF [Anti-Inhibitor Coagulant Complex] Page 1 of 39. PRODUCT MONOGRAPH . FEIBA NF . Anti-Inhibitor Coagulant Complex, Freeze-Dried Substance](https://img.pdfslide.net/doc/110x75/60ae9ad8667adb43ce7aabf3/product-monograph-2020-9-8-feiba-nf-anti-inhibitor-coagulant-complex-page.jpg)















