Embed Size (px)
Citation preview

Pericardial Closure Decreases Right Ventricular Load Tolerance in the Dog
Steven M. Scharf, Kenneth G. Warner, Robert Brown, and Shukri Khuri
Previous studies using graded pulmonary artery (PA) occlusions were unable to determine whether the Frank-Starling relationship contributed significantly to right ventricle (RV) afterload tolerance. Hence, we wished to determine whether limitation of RV filling could decrease RV load tolerance. Anesthetized mongrel dogs were instrumented for the measure- ment of mean aortic pressure, pulmonary arterial flow, RV systolic (Ps) and diastolic (Pd) pressures, and myocardial segment length of the RV inflow (INF) and outflow (OUT) tracts. Filling of RV was limited by pericardial closure (PC). Before and after PC we performed graded occlusions of the PA to the point of cardiocirculatory failure IF). The magnitude of RV after load that could be tolerated without F was called the highest load tolerable (HLT). At HLT, with the pericardium open (PO), PA circumference had decreased by 33.9% f 9.5%. and there were in- creases in Ps (from 28.3 + 6.6 to 57.2 f 17.7 torr, P < 661). Pd (from 4.4 & 1.9 to 6.1 + 1.5 torr, P < .Ol 1, and diastolic regional myocardial segment lengths (10.4 + 4.2 to 11.6 + 4.5 mm for INF, 10.4 f
S EVERE acute increases in pulmonary arte- rial (PA) pressure, such as might occur with
massive pulmonary embolism or with the adult respiratory distress syndrome, especially in asso- ciation with high levels of positive end-expiratory pressure, can lead to right ventricular (RV) failure and circulatory collapse.1-6 In previous studies,’ using graded constrictions of the PA to increase RV afterload, we found that the RV was able to tolerate nearly a threefold increase in RV systolic pressure (Ps) with relatively small changes in preload. By contrast, during RV failure (F), defined as the onset of cardiocircula- tory collapse, there were large increases in re- gional myocardial segment length. The finding
From the Pulmonary Section, Medical, Surgical. and Research Services. Brockton/West Rosbury VA Medical Center, Boston, MA; and Departments of Medicine and Surgery, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA. Dr Scharf is now with the Long Island Jewish Medical Center, New Hyde Park, NY
Supported by the Richard A. Warren Fund and VA funding.
Address reprint requests to Steven M. Scharf; MD, PhD. Pulmonary and Critical Care Division, Long Island Jewish Medical Center, New Hyde Park, NY 11042.
o 1990 by W.B. Saunders Company. 0883-9441/90/0501-0003$05.00/0
20
0.9 to 11.5 + 0.5 mm for OUT: P < .05). Compared to PO, with PC, RV load tolerance decreased in that PA circumference could be decreased by only 26.2% + 15.7% (P < .05), and Ps increased to only4B.4 f 22.5 torr (P < .05). With PC, there was a significant decrease in end-diastolic fiber length for OUT, but not for INF. Further, with PC, at HLT, INF end- diastolic segment length increased (to 11.2 + 3.3 mm) but, unlike with PO, there was no significant increase in OUT. However, for INF as well as for OUT, maximum diastolic length was significantly less with PC than with PO. By empirically fitting pressure- segment length curves to an exponential equation, we obtained an index of regional stiffness. Following PC, this was unchanged for the INF. but had in- creased significantly for the OUT. We conclude (I) the Frank-Starling relationship contributes to the capacity of the RV to tolerate increased afterload; and (2) the effects of pericardial closure on regional stiffness are nonhomogeneous, the outflow tract being more constrained than the inflow tract. 0 1990 by W.9. Saunders Company.
that maximum ventricular filling was not achieved prior to F suggested that the contribution of the Frank-Starling mechanism to RV load tolerance was not determined by the maximum possible dilation of the RV, the theoretical maximal limits of this mechanism. In fact, based on those studies, we could not determine whether or not the Frank-Starling mechanism contributed at all to RV load tolerance. This is of potential clinical importance. While intravascular volume loading leading to increased RV preload is frequently advocated as a treatment for acutely increased RV afterload, there are theoretical disadvan- tages to this form of therapy. These include increased RV myocardial oxygen consump- tion,7-9 and limitation of RV myocardial blood flow lo due to increased intramyocardial wall tension. Thus, the role of the Frank-Starling mechanism in determining RV tolerance should be defined. If this mechanism plays little role in determining load tolerance, then perhaps the potential adverse effects of intravascular volume expansion would outweigh possible therapeutic benefit, and this mode of therapy should not be considered in most cases.
In order to determine the potential role of the Frank-Starling mechanism in determining RV load tolerance, we performed a series of experi-
Journal of Critical Cara, Vol 5, No 1 (March), 1990: pp 20-26

RV LOAD TOLERANCE 21
ments in a previously characterized model of acute RV overload before and while RV filling was limited by the pericardium.11912 Our hypoth- esis was that limiting RV filling by closing the pericardium would decrease its capacity to toler- ate increased afterload. We found that pericar- dial limitation of RV preload did, in fact, de- crease RF load tolerance. Furthermore, we found that pericardial closure inhibited RV filling more in the outflow than in the inflow tract.
MATERIALS AND METHODS
We used a previously developed canine model of acute RV overload, the characteristics and reproducibility of which have been described previously.’ Twelve mixed-breed dogs of either sex were premeditated with acepromazine (0.1 mg/ kg) and atropine (0.5 mg) by intramuscular injection. Anes- thesia was induced by intravenous injection and sodium pentobarbital, 25 mg/kg, and the animals were paralyzed by intravenous injection of 20 mg of succinyl choline. Following intubation, mechanical ventilation was begun (tidal volume 12 mL/kg, respiratory rate adequate to maintain arterial pC0, 35 to 40 torr, inspiratory 0, concentration 35% to 45%). Thirty milligrams of pentobarbital and 10 mg of succinyl choline were given every 1 to 2 hours to maintain anesthesia and paralysis. Animals were placed in the left lateral decubitus position (left side down) for the remainder of the studies. The following intravascular catheters were placed: femoral venous catheter for administration of fluids and medications, femoral arterial catheter for measurement of aortic blood pressure (Pao) and withdrawal of blood for measurements of blood gas tensions, micromanometer-tipped catheter (Millar Mfg, Houston, TX) into the RV via a jugular vein for high fidelity recordings of RV pressure. All pressures were measured relative to atmospheric pressure.
The pericardium was widely incised over its right lateral surface and the heart suspended in a pericardial sling. The main trunk of the PA was dissected free of the aortic root, and an electromagnetic flow probe, calibrated against simulta- neous measurements of cardiac output by the Fick principle for each animal, was placed around the PA for measuring pulmonary arterial flow (Qpa). A piece of umbilical tape was passed around the PA distal to the flow probe through a small plastic cannula to form a loop which was tightened until it fit snuggly around the PA without actually constricting it. The length of the loop was measured and assumed to be the external circumference of the main PA.
Changes in myocardial segment length of the RV outflow (OUT) and inflow (INF) tracts were measured using pairs of implanted sonomicrometer crystals (Triton Mfg, San Diego, CA). The crystal pair for measurement of OUT was im- planted approximately 1 cm apart in the outflow tract parallel to the plane of and approximately 1.5 cm cauded to the pulmonic valve annulus. The crystal pair for measurement of INF was implanted in the myocardium of the inflow tract, approximately 1 cm apart, parallel to the orientation of the superficial fibers.
Measurements of all variables were made during expira- tion with paper speed 200 mm/s. Data were analyzed using a
magnetic digitizing board connected to a microcomputer. Three successive heart beats were analyzed for each datum point. Data were digitized at intervals of approximately 12.5 ms. For assessing the maximum velocity of fiber shortening (dl/dt max), the digitizing interval was decreased to 5 ms. Data for Qpa and Pao were meaned over the entire cardiac cycle. End-diastole was taken at the point of sudden upstroke in the RV pressure tracing and end-systole was taken at the point of maximal fiber shortening. Since there is a delay of approximately 25 ms between maximal fiber shortening of INF and OUT,‘,” the end-systolic values for each RV region did not occur at the same point in time. RV pressures were measured at end-diastole (Pd) and at its peak value, consid- ered to be peak Ps.
Variables Measured For each condition, the following variables were measured:
Ps, Pd, heart rate, Pao, mean Qpa. stroke volume (SV, Qpa/heart rate), end-diastolic (Ldia) and end-systolic (Lsys) fiber length for INF and OUT, percent fiber shortening, and maximum velocity (dl/dt max) of fiber shortening
Experimental Protocol The capacity of the RV to tolerate increased afterload was
assessed as previously described.’ After baseline measure- ments were taken, PA circumference was decreased in steps of 0.25 cm. Following each decrease in circumference, approximately 10 minutes were allowed before making mea- surements. As circumference was progressively decreased, Ps progressively increased, until a critical circumference was reached such that further decreases caused a precipitous drop in Ps and Qqa. This state was defined as circulatory failure (F), since, if sustained, it would have led to the death of the animal. The PA occluder was opened within 2 minutes of the onset of F and recovery was allowed to occur. The greatest PA occlusion that could be tolerated without the occurrence of F was called the highest load tolerable (HLT), and was considered to be an index of the capacity of the RV to tolerate increased afterload. It took three to eight steps to reach HLT. Data are presented at baseline, at HLT, and at F. Whereas measurements at baseline and HLT were at steady state, F was not a steady state and data obtained at F were those obtained immediately before release of the PA occluder.
Following constriction of the PA to cause F with pericar- dium open (PO), animals were allowed to recover for approx- imately 30 minutes. At this point the pericardium was closed by approximating its cut edges with a continuous suture. The above protocol was then repeated with pericardium closed (PC).
Reproducibility studies. Six of the animals reported here had also been studied as part of a previously reported series of experiments on RV load tolerance.’ In these animals, follow- ing PA constriction with PC, the pericardium was reopened and PA occlusion repeated. This allowed us to assess the reproducibility of the preparations, and to determine whether or not there was degeneration of the preparation. As previ- ously reported,’ there were no significant differences in any index of RV function or load tolerance between the initial and final PA occlusions, thus demonstrating that any changes observed with PC were not due to degeneration of the experimental preparation with time.

22
Table 1. Effects of Pericardial Closure on Right Ventricular Load Tolerance
Variable PO PC PO VPC
Pa0 (tow)
Baseline HLT
F Qpa (I/min)
Baseline
HLT F
PS (tow) Baseline
HLT F
PD (torr) Baseline
HLT F
85.4 f 19.2 77.7 + 22.4. 26.8 f 13.8$
2.2 f 0.9
1.5 i 0.8t 0.5 f .3$
28.3 f 6.6
57.2 f 17.7t 36.2 i 10.4
4.4 * 1.9 6.1 f 1.5.
8.8 f 1.7. Heart rate (bpml
Baseline 381 i 36
HLT 375 + 34 F 401 f 44
Change in PA circumference (%I
HLT -33.9 f 9.5$ F -41.8 + 8.8$
86.5 f 30.2 NS 59.2 * 21.9t P < .05 25.3 i 7.6$ NS
2.1 * 1.0 NS 1.6 f 1.3. NS
0.4 * 1.3$ NS
31.5 f 17.7 NS
48.4 f 22.5t P< .05 31.7 * 8.6 NS
8.7 f 3.8 P< .Ol 10.6 + 5.3. Pi.01
10.9 f 3.04 P: .05
450 f 99 NS 438 f 101 NS 502 + 166 NS
-26.2 f 15.7% P -z .02 -32.4 A 16.3$ PC .02
Note. N = 12. Data are expressed es mean f SD.
Abbreviation: NS = not significant for difference between PO
and PC. l P < .05.
tPC .Ol. #P-L ,001.
Statisticul analysis. Data were collated and expressed as the mean * standard deviation of the mean. Effects of PA constriction on RV function for any given treatment group were analyzed by repeated measures analysis of variance. When significance was found, Newman-Keuls test was per- formed to determine which differences were significant. Statistical comparison between treatment groups was done by pairwise comparisons at baseline and HLT and F. Signifi- cance was assessed by Student’s t test for paired variates adjusting for the number of comparisons (Bonferroni’s correc- tion).
RESULTS
Load Tolerance of the Right Ventricle
Table 1 shows the effects of pericardial closure on RV load tolerance. At HLT there was a significant decrease in Pao and Qpa. While there was no significant difference between baseline values for Pao between PO and PC, Pao was less at HLT with PC than with PO. While Qpa decreased at HLT under both conditions, there was no difference in Qpa at HLT for PO and PC. Ps increased twofold to threefold with PA con- striction. Systolic pressure at HLT was signifi-
SCHARF ET AL
cantly less with PC than with PO. With PO, Pd was significantly increased both at baseline and at HLT. Pulmonary arterial constriction led to increased Pd at HLT for both PC and PO, but the magnitude of the increase, approximately 2 torr, was not significantly different between the conditions. Although mean heart rate was less with PC than with PO, the differences were not significant. There were no significant changes in heart rate with PA constriction to HLT. Last, at HLT, the degree of PA constriction was signifi- cantly less with PC than with PO. In other words, less PA constriction could be tolerated by the RV with PC than with PO.
Changes in Regional Myocardial Segment Length
Of the 12 animals, we were able to obtain technically satisfactory data in six for OUT, in 11 for INF, and in five for both (Table 2). There were no significant changes in baseline myocar- dial segment lengths with PC compared to PO.
End-diastolic segment lengths. There were significant increases in end-diastolic segment
Table 2. Effects of Pericardial Closure on Regional Length
Variable PO PC PO VPC
Ldia INF (mm) Baseline 10.4 zt 4.2 HLT 11.6 f 4.5’
F 13.2 zt 4.9’ Lsys INF (mm)
Baseline 8.6 f 3.6 HLT 9.3 + 3.8
F 11.4 + 4.5t
% Shortening INF
Baseline 20 + 8.2 HLT 20.3 f 10.1 F 13.8 + 5.8t
Ldia OUT (mm) Baseline 10.4 f 0.9 HLT 11.5 * 0.5.
F 13.3 f 2.0t
Lsys OUT (mm) Baseline 9.1 + 0.8 HLT 9.6 f 0.8
F 11.4 + 2.1t % Shortening OUT
Baseline 13.7 f 2.2 HLT 15.5 f 6.1 F 14.6 + 5.6
10.7 * 3.7
11.2 f 3.3.
11.2 * 3.4*
9.0 f 3.4
9.7 f 3.9 10.0 f 3.3
17.9 zt 9.8
17.3 f 10.1 11.4 k 6.9t
9.2 zt 2.5 9.4 f 2.8
9.7 f 3.0
8.2 f 2.3 8.5 zt 2.5
9.0 * 2.9
9.9 f 2.8 9.7 f 3.8 7.0 f 3.1.
NS NS
P-c .05
NS NS
P-c .05
NS
NS NS
P< .05 P< .05
PC .Ol
NS NS
P<.Ol
P<.O2 P< .02 P<.Ol
Note. For INF, N = 11; for OUT, N = 6. Data expressed as mean + SD.
‘P < .05.
tP< .Ol.

RV LOAD TOLERANCE 23
Table 3. Comparison of Regional and Global Stroke Changes
Condition
BASE HLT
F
INF (mm)
2.1 + 1.1 2.2 f 1.2
1.7 k 1.0
PO PC
OUT sv INF OUT sv (mm1 (mL) hm) (mm) IrnL)
1.5 f 0.3 14.1 + 6.9 1.9 + 1.0 0.9 r 0.4 15.6 + 8.6
1.8 f 0.9 9.4 * 5.6 1.8 + 1.0 0.8 + 0.6 10.5 + 7.8
1.9 + 0.8 2.8 f 1.4 1.2 + 0.7 0.6 + 0.3 4.3 f 3.8
Note. For INF, N = 1 1; for OUT, N = 6; for SV, N = 12. Data expressed as mean f SD.
lengths for INF at HLT and F with both PO and PC. However, the increase in INF at F was less with PC than with PO. For OUT there was a significant increase in end-diastolic segment length at HLT and F only for PO. With PC there were no significant changes in OUT.
End-systolic segment lengths. For both INF and OUT, with PO, there was a significant increase in end-systolic segment length only at HLT compared with baseline. With PC, there were no significant changes in end-systolic seg- ment lengths at either HLT or F.
Regional myocardial shortening. There were no significant changes in regional shortening at HLT, while regional shortening decreased at F for INF with both PO and PC, and for OUT only with PC. For neither PO nor PC were there significant changes in dl/dt max, or time to dl/dt max, at HLT. In order to compare regional myocardial shortening with global RV ejection, we have shown regional diastolic-systolic length changes (stroke length) and SV (calculated as cardiac output/heart rate) in Table 3. Stroke volume decreased equivalently for PO and PC with increased RV afterload. With PO, changes in regional stroke length did not parallel those in SV. There was no change in INF at HLT, even
0 l
0
CD l 00
0 0
13 15 LENGTH - (MM)
17 19
though SV had decreased. For OUT, stroke lengths actually increased with increased after- load in spite of the fact that SV decreased. With PC, however, changes in regional stroke length did parallel those in SV for both INF and OUT.
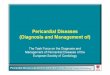
Regional pressure-segment length curves. To better compare the regional effects of pericar- dial closure, for the five dogs in which satis- factory data from both INF and OUT were obtained, we plotted Pd as a function of end- diastolic length for INF and OUT during PA constriction to F. Figure 1, left, shows a plot for INF and Fig 1, right, shows a plot for OUT. Using the approach of Assanelli et al,” we fit the curves to an exponential equation of the form
Pressure = Aekue”sth)
where k is a shaping constant measuring the overall “stiffness” of the curve, and A is the pressure intercept at zero length. This was done following natural log transform of the pressure, and performing least squares analysis of the plot of In (pressure) as a function of length.
Table 4 presents the data and pairwise compar- isons for the data from both RV regions for PO and PC. The data demonstrate a significant increase in stiffness with PC for the OUT region.
0 l
0 l 0
10 11 12 13 14 15 LENGTH - (MM)
Fig 1. (Left) End-diastolic pressure-segment length plot for INF in a dog no. 11; inflow tract. Pressure is in tow. (Right) End-diastolic pressure-segment length plot for OUT in a dog no. 11: outflow tract. Open circles = pericardium open. Closed circles = pericardium closed.

24 SCHARF ET AL
Table 4. Regression Parameters for Diastolic Pressure-Segment Length Curves
Variable PO
INF OUT
PC P Value PO PC P Value
k 0.34 f 0.31 0.39 f 0.28 NS 0.35 f 0.18 0.95 f 0.62 .05 A -3.2 i 6.7 -5.4 + 8.2 NS -2.2 + 1.8 -6.4 + 6.0 NS
Note. N = 5 for animals in which satisfactory data from both INF and OUT were obtained. Data are shown as mean f SD. “Pvalue” is for difference between PO and PC.
Abbreviations: k, overall stiffness constant; A, zero length axis intercept for In (pressure).
Changes in stiffness for INF were inconstant and we detected no significant trend. Changes in intercept were inconstant and showed no signifi- cant trend for either region.
DISCUSSION
In these studies we demonstrated that PC decreased the capacity of the RV to tolerate increased afterload. With PC, the degree to which PS could be increased and PA circumfer- ence decreased before the onset of F was signifi- cantly less than with PO. These data were consistent with the hypothesis that limiting RV filling limits RV load tolerance, ie that the Frank-Starling relationship does contribute to the capacity of the RV to tolerate increased afterload. Further, there appeared to be a differ- ential effect on different regions of the RV free wall in that OUT showed no significant increase with PC while INF continued to increase with PA constriction. Analysis of end-diastolic pres- sure-segment length curves confirmed this inter- pretation, since the constant k, an indicator of overall stiffness, significantly increased with PC for OUT, but not for INF. In the ensuing discussion we evaluate these findings in the light of the limitations of the experimental prepara- tion and currently available literature.
At HLT, Pao fell more with PC than with PO (see Table 1). That this was due to decreased systemic vascular resistance is demonstrated by the fact that at HLT cardiac output decreased to the same degree with PO as with PC. In our previously reported studies on six of the animals we demonstrated that Pao was also lower at HLT, even when PA occlusions were repeated with PO. Thus, this finding represents a change in the preparation over the course of the experi- ment and not an effect due to PC. However, as noted in the Methods section, repeated PA occlu- sions with PO were not associated with changes in any index of RV load tolerance or function.
Hence, changes seen with PC could not have been due to degeneration of the experimental preparation. Further, there was no reason to believe that changes in baseline RV function due to PC led to changes in RV load tolerance, since there were no significant changes in either base- line cardiac cycle time (ie, heart rate) or contrac- tile function (as measured by dl/dt max or end-systolic fiber length).
Our work is consistent with previous studies demonstrating that the pericardium inhibits filling of the RV,12*‘3 as it does of the left ventricle.13-15 Maximum myocardial segment lengths (present at F) were significantly less with PC for both INF and OUT. It should be noted, however, that under the conditions of our experi- ments the effect of the pericardium on RV filling would most likely be greater than that present in the normal, undisturbed state. This is because of the necessity for opening the pericardium in order to instrument the heart. Because the cut edges of the normal pericardium retract,16 when the pericardium is reclosed it will most likely exert greater force on the underlying heart and inhibit its filling more. However, the purpose of these studies was not to determine the degree to which the normal pericardium inhibits RV filling, but to determine whether or not inhibiting RV filling would decrease RV load tolerance.
In previous studies on the effects of RV after- loading, changes in regional diastolic RV myocar- dial segment length were shown to be uniform,7 and to correspond to changes in RV septal-free wall dimension.13 These findings suggested that changes in regional myocardial segment lengths reflect changes in overall RV end-diastolic vol- ume reasonably well. However, the present stud- ies suggest that, with PC, this may not be the case. This is because with PC we found nonhomo- geneous changes, ie, OUT decreased with no change in INF. These findings are consistent with a shape change in the RV free wall due to

RV LOAD TOLERANCE 25
nonhomogeneous changes in RV surface pres- sure with PC. Smiseth et al” found that intraperi- cardial pressure could change differently be- tween the pericardial space over the right and left ventricles. The present studies extend these obser- vations and infer that changes in intrapericardial pressure may even be nonhomogeneous over different regions of the same ventricle.
As well, nonhomogeneity of regional diastolic filling was evident in the afterload response with PC. Since maximum Ldia was decreased with PC for both INF and OUT, the data were consistent with the notion that filling was inhib- ited in both INF and OUT. However, filling was inhibited even more in the OUT. This is because there was no significant increase in end-diastolic OUT with PA constriction following PC. The data in Table 4 further confirm the differential effect of PC on OUT versus INF, since the overall stiffness constant increased significantly only with OUT.
The data presented in Table 3 indicate that with PO, regional shortening changes do not reflect changes in global shortening, ie, stroke volume. This probably relates to the geometry of the RV. The normal RV is a crescent-shaped highly compliant chamber in which INF and OUT contract sequentially during ejection.’ It is not difficult to imagine that, during afterloading, this chamber could change its geometry in a complex manner such that different segments non-uniformly reflect overall ejection. This neces- sitates that other measurements of RV geometry, for example septal-free wall dimension, would have better reflected stroke volume with PO. Thus with PO the RV must behave as a system with more than one degree of freedom, and not all regional changes reflect global changes. On the other hand, with PC, changes in regional shortening did parallel those in global shortening (SV). These findings suggest that with pericar- dial constraint the RV behaves as a system with few, perhaps even only a single, degrees of freedom, and that changes in global dimensions are reflected more uniformly by changes in various regions.
During changes in RV preload, Assanelli et al” found nonhomogeneous changes in regional RV compliance in the presence of the pericar- dium. However, unlike us, these authors found that compared with pericardiectomy, when the
pericardium was present, regional stiffness in INF increased while there were inconstant changes in OUT. The reasons for the difference in findings between the studies of Assanelli et al” and ours are not immediately obvious. However, differences in experimental technique may ac- count for some of the discrepancies. The “pericar- dium intact” condition of those authors was actually a condition whereby sonomicrometer crystals were sutured onto the RV surface via 1 cm incisions through the pericardium. These were left open during the experiment. When viewed en face, the RV is roughly pear-shaped, with the “base” of the pear being the INF, and the tapering apex being the OUT. Thus, a 1 cm incision would leave a greater regional opening relative to the surface area of the underlying myocardium over the OUT than over the INF. Perhaps this had the effect of reducing pericar- dial constraint over the OUT, even with the pericardium intact (PC). For this reason, the effect of opening the pericardium in their studies could have been less in the OUT, as they found. Another possibility is that the animals of Assinelli et al were most likely studied while supine (median sternotomy, bilateral thorocotomy), while ours were studied in the left lateral decubi- tus position. Possibly regional pericardial pres- sure gradients and the effects of pericardial constraint differ when the position of the animal is changed.
Although our data were consistent with the hypothesis that the Frank-Starling relationship does contribute to RV afterload tolerance, cau- tion must be urged before recommending intra- vascular volume expansion in cases of severe, acute elevations in pulmonary vascular resis- tance. Experimental evidence has been presented that, at load levels near HLT, further increase in RV preload may be detrimental to RV func- tion.8”s However, at load levels less than HLT, or when intravascular volume and RV preload are decreased, as with dehydration and blood loss, volume replacement to increase RV preload may well be indicated. Last, when decreasing peri- cardial capacity or compliance, as with pericardi- tis or pericardial effusion, consideration should be given to early therapeutic intervention in cases when there is a coexisting increase in RV after- load.

26 SCHARF ET AL
REFERENCES
1. Fineberg MH, Wiggers CT: Compensation and failure of the right ventricle. Am Heart J 11:255-263, 1936
2. Taquini AC, Fermosa JD, Armendia P: Behavior of the right ventricle following acute constriction of the pulmonary artery. Circ Res 8:315-318, 1960
3. Guyton AC, Lindsey AW, Gilluly JJ: The limits of right ventricular compensation following acute increases in pulmo- nary vascular resistance. Circ Res 2:326-332, 1955
4. Zapol WM, Snider MT: Pulmonary hypertension in acute respiratory failure. N Engl J Med 246:476-486, 1977
5. Greene R, Zapol WR, Snider MT, et al: Early detection of pulmonary occlusion during acute respiratory failure. Am Rev Respir Dis 124:593-601, 1981
6. Dhainaut JF, Schlemmer B, Monsallier JF, et al: Behavior of the right ventricle following PEEP in patients with mild and severe ARDS. Am Rev Respir Dis 129:A95, 1984
7. Scharf SM, Warner KG, Brown R, et al: Load toler- ance of the right ventricle: Effect of increased aortic pressure. J Crit Care 1:163-173, 1986
8. Ghignone M, Girley L, Prewitt RM: Volume expansion versus norepinephrine in treatment of a low cardiac output complicating an acute increase in right ventricular afterload in dogs. Anesthesiology 60:132-135, 1984
9. Molloy WD, Lee KY, Girling L, et al: Treatment of shock in a canine model of pulmonary embolus. Am Rev Respir Dis 130:870-874
10. Dyke CM, Brunsting LA, Saltes DR, et al: Preload dependence of right ventricular blood flow. I. The normal right ventricle. Ann Thorac Surg 43:478-483, 1987
11. Janicki JS, Weber KT: The pericardium and ventricu- lar interaction, distensibility, and function. Am J Physiol 238:H494-H503,1980
12. Assanelli D, Lew WYW, Shabetai R, et al: Influence of the pericardium on right and left ventricular filling in the dog. J Appl Physiol63:1025-1032, 1987
13. Santamore WP, Meier GD, Bove AA: Effects of hemodynamic alterations on wall motion in the canine right ventricle. Am J Physiol236:H254-H262, 1972
14. Glantz SA, Misbach GA, Moores WY, et al: The pericardium substantially affects the left ventricular diastolic pressure-volume relationship in the dog. Circ Res 42:433- 441,1978
15. LeWinter MM, Pavelec R: Influence of the pericar- dium on left ventricular end-diastolic pressure-Segment length relation during early and later stage of experimental chronic volume overload in dogs. Circ Res 50:501-509, 1982
16. Crawford MH, Badke FR, Amon KW: Effect of the undisturbed pericardium on left ventricular size and perfor- mance during acute volume loading. Am Heart J 105:267- 272,1983
17. Smiseth OA, Scott-Douglas NW, Thompson CR, et al: Nonuniformity of pericardial surface pressure in dogs. Circulation 75:1229-1236, 1987
18. Prewitt RS, Ducas J: Hemodynamic management of acute respiratory failure, in Scharf SM, Cassidy SS (eds): Heart-Lung Interactions in Health and Disease. New York, NY, Dekker, 1989, pp 915-982










![Fulminant isolated cardiac sarcoidosis with pericardial effusion … · 2017. 4. 18. · if associated with new ventricular tachyarrhythmias or ... case report[2 ,14 15]. Conduction](https://img.pdfslide.net/doc/110x75/6119971c0f2ccf10175eeb3e/fulminant-isolated-cardiac-sarcoidosis-with-pericardial-effusion-2017-4-18.jpg)