Embed Size (px)
Citation preview

ItalIan Journal of Dental MeDIcIne vol. 3/1-201812
leading to the destruction of the tissues (2) (Fig. 2, 3). The progression and severity of the disease depend
on how much the aggressiveness of the sub-gingival biofilm is countered by the host’s immune response (3, 4), which is further modulated by the genetic and epigenetic context and also environmental factors such as gender, age, smoking and oral hygiene (5, 6) (Fig. 4). It is increasingly clear that, due to bacteraemia and the systemic release of endotoxins, the presence of pathogenic bacteria in periodontal lesions is also correlated to various systemic disorders, including cancer, diabetes mellitus, rheumatoid arthritis, cardiovascular disease, infertility and adverse birth outcomes (7).
From a recent study of nearly 3,000 patients, it appears that periodontitis affects women more than men at a ratio of 3:2 (8) and the literature supports the evidence that, in women, there is an association between periodontitis and puberty, menstruation, pregnancy, use of oral contraceptives and menopause (9-11). Fundamental aspects to consider for understanding the pathogenic mechanisms underlying this association are the periodical and age-related physiological changes in oestrogen and progesterone levels, the tissue distribution of the related receptors and the metabolism of the hormones. The cyclical
IntroductionGrowing attention by the medical community to
the potential impact of gender differences on the pathophysiology of many diseases has generated a new branch of medicine: “gender medicine”. Meanwhile, the association between periodontal infection and certain systemic diseases has been demonstrated, and the idea of “periodontal medicine” is gaining ground in the dental community. The aim of this paper is to merge these two new concepts, reporting the evidence from the literature of an association between periodontitis and certain specific or prevalent systemic diseases in women, and trying to evaluate the possible mechanisms involved in order to improve the approach to female health.
Periodontitis is the result of an inflammatory response by the host to a bacterial infection of periodontal tissues. Numerous species of pathogenic bacteria present in sub-gingival plaque can disrupt the normal homeostatic processes, attack the surfaces of the tooth, infiltrate periodontal tissues and organise themselves in the form of biofilm (1) (Fig. 1).
The host’s immune response, triggered by microorganisms and their metabolites, activates the synthesis and release of cytokines, inflammation mediators and metalloproteinases of the matrix,
Periodontitis, female pathophysiology and systemic diseases in women
Francesco Martelli1, Piero Nobili2, Federico Ronchi2, Alberto Zanvit2, Roberto Ferdeghini2, Antonio Vimercati2
1 IMI (International Microdentistry Institute), Florence, ItalyAIMOP (Italian Academy of Oral Medicine and Periodontology), Milan, Italy2 ISI - Italian Stomatological Institute, Department of Biological Dentistry, Milan, Italy
Periodontal medicine, Gender medicine, Female health.
Two concepts are gaining ground in the dental community: the association between periodontal infection and certain systemic diseases, in other words “periodontal medicine”, and the growing awareness and interest in gender differences on the pathophysiology of many diseases, that is “gender medicine”. The aim of this paper is to report the evidence from the literature of the association between periodontitis and certain specific or prevalent systemic diseases in women, in order to evaluate the possible mechanisms involved with the ultimate aim of improving the approach to female oral health. The literature analysed suggests an implication of periodontal disease in many systemic disorders specific to women or with a major impact on them, and reveals the importance of a joint effort by doctors and dentists towards better managing women’s health. In this regard, a gender-specific approach should be applied.
KEYWORDS ABSTRACT
ItalIan Journal of Dental MeDIcIne vol. 3/1-2018 13
reduction in sex hormone levels, leading to increased vasodilation and capillary permeability, makes women transiently more susceptible to periodontitis, and increased levels of progesterone are associated with changes in the bacterial population, especially with an increase in Gram-negative anaerobic bacteria (12). Also oral contraceptives, which act by mimicking pregnancy although with individual variability, are associated with the same gingival disorders and the same generalised osteoporosis that characterise gestation (13, 14). The decrease in levels of progesterone and oestrogen circulating at menopause often cause oral problems, osteoporosis and recurrence of periodontal disease or its worsening if previously existing (15).
Apart from acting on specific target tissues, sex hormones also act on cells of the immune system, adipose, bone and nerve tissues, and gender differences in susceptibility to certain diseases are historically described in the literature (9, 16-18). In basic research and in developing new treatments, the biological differences between the sexes are often not considered and, since periodical age-related hormonal changes make women unstable models, the preference is to study diseases and drugs on males. This lack of interest in specifically female conditions, such as pregnancy and menopause, and the scarce presence of women in clinical trials, can lead to gender disparities in healthcare, and so the development of “gender medicine” is the opportunity to take account of the pathophysiological differences between men and women in modern biomedical research.
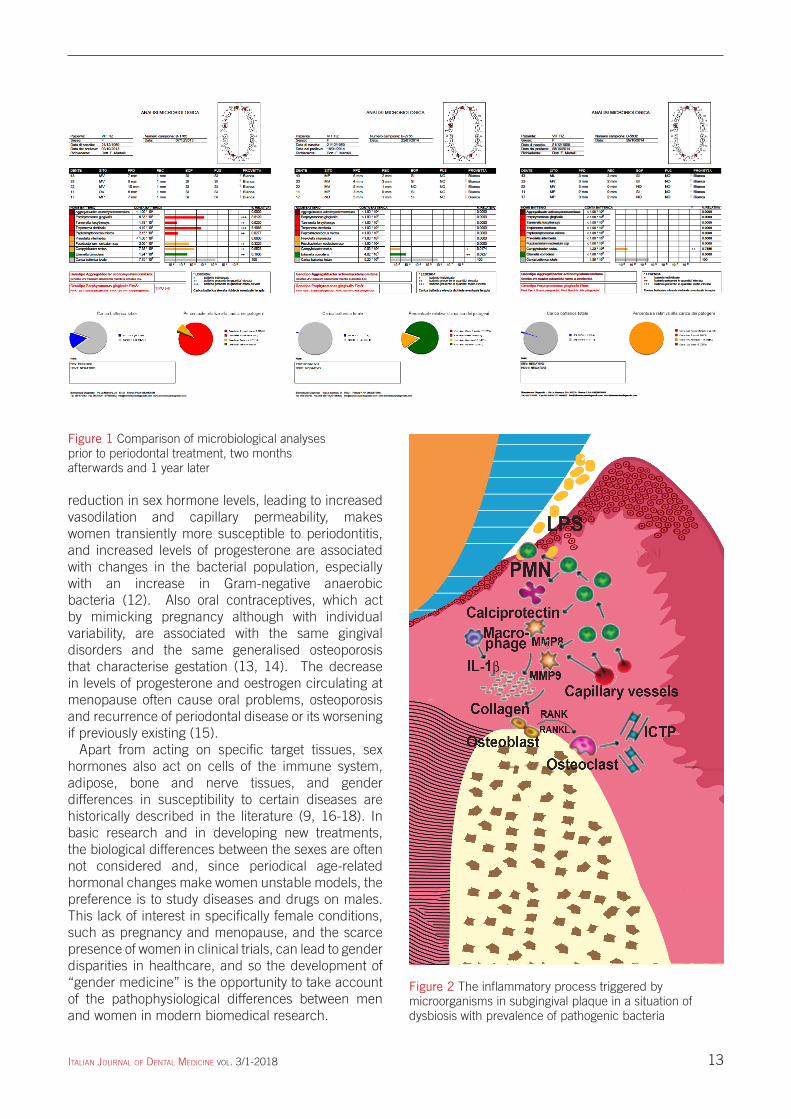
Figure 1 Comparison of microbiological analyses prior to periodontal treatment, two months afterwards and 1 year later
Figure 2 The inflammatory process triggered by microorganisms in subgingival plaque in a situation of dysbiosis with prevalence of pathogenic bacteria

ItalIan Journal of Dental MeDIcIne vol. 3/1-201814
cytokines released in circulation, both able to bring about the contraction of myocytes and premature birth.
Supporting the hypothesis that oral bacteria can reach and colonise the maternal-foetal unit and result in infertility and pregnancy problems, P. gingivalis, F. nucleatum and A. actinomycetemcomitans have been found in amniotic fluid or in samples of placenta of women who gave birth prematurely and suffered from periodontitis (23,24) (Fig. 5). Furthermore, metagenomic data confirm similarities between the placental and oral microbiome, and differences with the genitourinary or intestinal microbiome (25) (Fig. 6). Also inflammation mediators induced by periodontal pathogens, whether disseminated by oral lesions or produced by infected endometrial and placental tissues, can cause infertility and pregnancy problems (26).
Several studies suggest a correlation between periodontitis and bacterial vaginosis in women aged over 35 (27) and between periodontitis and endometriosis (28, 29), with a consequent greater risk of infertility in both cases. For endometriosis, a multifactor disease that affects 6-10% of women of reproductive age and which, like periodontitis, originates from an altered immune response and consequent chronic
Infertility and adverse childbirth outcomesInfertility is a disorder that causes anxiety, depression
and stress to many couples of reproductive age all over the world. While not putting life at risk, its negative influence on patients, families and societies makes it a serious problem that, in the West, affects one in six couples, with a 1.9% rate of primary infertility and 10.5% in secondary infertility (19). Infertility is also associated with a high risk of adverse outcomes of pregnancy, such as premature and underweight babies (20). Several risk factors have been identified: drinking alcohol, smoking, drug-taking, mother’s age (young or advanced), low socio-economic level, poor prenatal care, high blood pressure, diabetes, history of previous premature births, multiple pregnancies, infections and chronic inflammation (21). Nonetheless, in half of cases the cause remains unknown and a large number of epidemiological and clinical studies reliably report a possible association between infertility and periodontal problems (22-24), imputed both to the systemic dissemination of oral bacteria and to the high levels of pro-inflammatory
Figure 3 Quantitative enzymatic analyses of matrix metalloproteinases-8 (MMP-8) before and after periodontal treatment

ItalIan Journal of Dental MeDIcIne vol. 3/1-2018 15
Figure 5 Analysis of the vaginal microbiome (Vaginal Path Test, VPT)

ItalIan Journal of Dental MeDIcIne vol. 3/1-201816
bone resorption, modulating osteoblast and osteoclast activity, and that oestrogen, by regulating important immunity mediators, has a fundamental role in both inflammation and homeostasis of the bone. In fact, the decrease in oestrogen levels is considered one of the main risk factors for osteoporosis in women (33). Vitamin D also plays an important role and its deficiency, or the presence of polymorphisms in the gene of its receptor, are considered risk factors for osteoporosis (34), immune system disorders, chronic inflammatory diseases and cancer (35).
Osteoporosis and periodontitis are both characterised by bone destruction and share several risk factors, such as advanced age, deficiencies in the sex hormone and vitamin D (or the presence of polymorphisms in the receptor) (36). The association between the two diseases has been studied for decades and much evidence is shown in the literature. For example, menopausal women with osteoporosis are more likely to develop periodontal disease and in more severe form (37) and BMD is an important indicator of this risk (38). In a large-scale population study, an
inflammation, a cause-effect relationship has been suggested whereby an altered inflammatory response to periodontal pathogenic bacteria could increase the susceptibility to endometriosis in women suffering from periodontitis (28, 2).
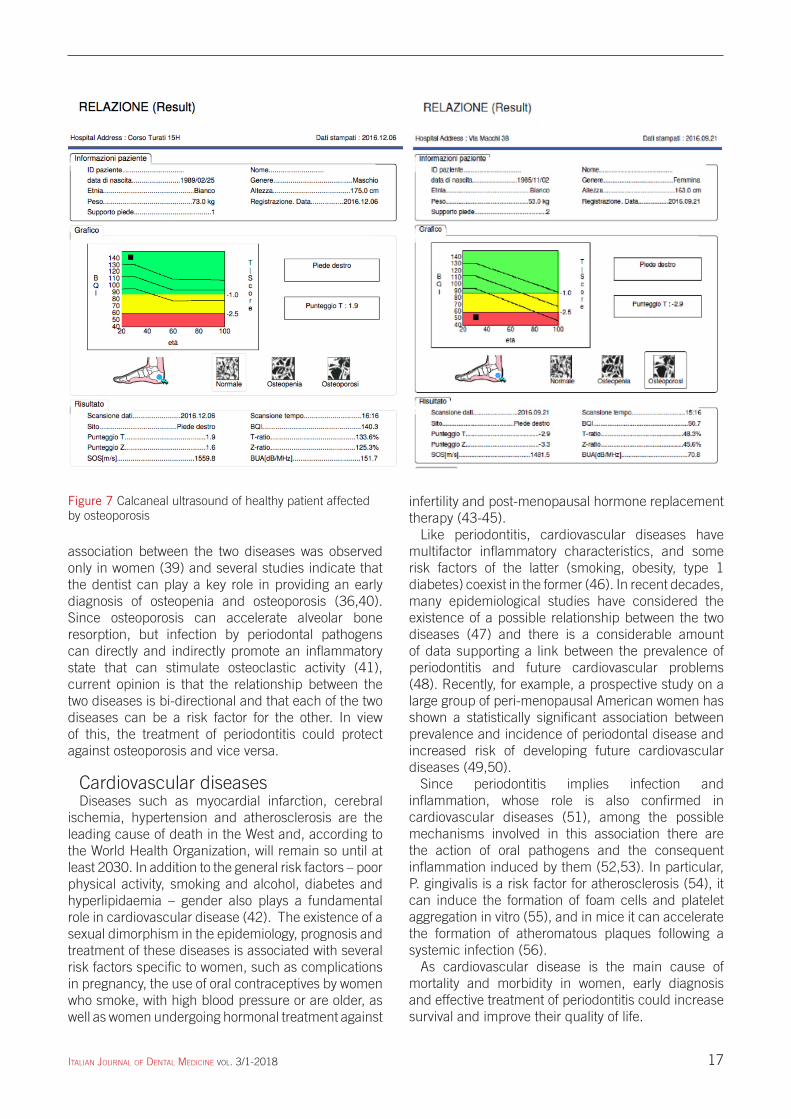
OsteoporosisIn the bone tissue, homeostasis is finely regulated
by osteoclastic and osteoblastic activity. If the former becomes excessive, bone resorption exceeds its neoformation, with a consequent decrease in BMD (Bone Mineral Density), degeneration of bone micro-architecture and development of osteoporosis, clinically associated with increased bone fragility and susceptibility to fractures (30) (Fig. 7, 8). BMD is not particularly gender-specific until after the age of 50, when it typically becomes lower in females and the prevalence of osteoporosis and rate of fractures associated with it is twice as high as in males (31). Non-modifiable risk factors are being older, being female, the menopause and genetic makeup, while risk factors that can be modified are the reduction of levels of sex hormones, treatment with drugs, insufficient intake of calcium and vitamin D, a low body mass index, smoking, alcoholism and physical inactivity (32). Pro-inflammatory cytokines have been shown to regulate
Figure 6 The placental microbiome has a taxonomic profile similar to the oral microbiome (Aagaard K, Ma J, Antony KM, Ganu R, Petrosino J, Versalovic J. The placenta harbors a unique microbiome. Sci Transl Med. 2014 May)
ItalIan Journal of Dental MeDIcIne vol. 3/1-2018 17
infertility and post-menopausal hormone replacement therapy (43-45).
Like periodontitis, cardiovascular diseases have multifactor inflammatory characteristics, and some risk factors of the latter (smoking, obesity, type 1 diabetes) coexist in the former (46). In recent decades, many epidemiological studies have considered the existence of a possible relationship between the two diseases (47) and there is a considerable amount of data supporting a link between the prevalence of periodontitis and future cardiovascular problems (48). Recently, for example, a prospective study on a large group of peri-menopausal American women has shown a statistically significant association between prevalence and incidence of periodontal disease and increased risk of developing future cardiovascular diseases (49,50).
Since periodontitis implies infection and inflammation, whose role is also confirmed in cardiovascular diseases (51), among the possible mechanisms involved in this association there are the action of oral pathogens and the consequent inflammation induced by them (52,53). In particular, P. gingivalis is a risk factor for atherosclerosis (54), it can induce the formation of foam cells and platelet aggregation in vitro (55), and in mice it can accelerate the formation of atheromatous plaques following a systemic infection (56).
As cardiovascular disease is the main cause of mortality and morbidity in women, early diagnosis and effective treatment of periodontitis could increase survival and improve their quality of life.
association between the two diseases was observed only in women (39) and several studies indicate that the dentist can play a key role in providing an early diagnosis of osteopenia and osteoporosis (36,40). Since osteoporosis can accelerate alveolar bone resorption, but infection by periodontal pathogens can directly and indirectly promote an inflammatory state that can stimulate osteoclastic activity (41), current opinion is that the relationship between the two diseases is bi-directional and that each of the two diseases can be a risk factor for the other. In view of this, the treatment of periodontitis could protect against osteoporosis and vice versa.
Cardiovascular diseasesDiseases such as myocardial infarction, cerebral
ischemia, hypertension and atherosclerosis are the leading cause of death in the West and, according to the World Health Organization, will remain so until at least 2030. In addition to the general risk factors – poor physical activity, smoking and alcohol, diabetes and hyperlipidaemia – gender also plays a fundamental role in cardiovascular disease (42). The existence of a sexual dimorphism in the epidemiology, prognosis and treatment of these diseases is associated with several risk factors specific to women, such as complications in pregnancy, the use of oral contraceptives by women who smoke, with high blood pressure or are older, as well as women undergoing hormonal treatment against
Figure 7 Calcaneal ultrasound of healthy patient affected by osteoporosis

ItalIan Journal of Dental MeDIcIne vol. 3/1-201818
to infectious agents, elements of diet, chemicals, toxins and stress (58), and the existence of a sexual dimorphism, varying in degree depending on the pathology (59). The last of these can be attributed to the greater female immunological reactivity, both humoral and cellular (60), but also to the action of oestrogens which activate the lymphocytes and the production of immunoglobulins (61), in addition to the X chromosome dosage, epigenetic factors, genomic imprinting and the contribution of microRNAs (62, 63).
Rheumatoid arthritis, the most common autoimmune pathology, is an inflammatory arthropathy that affects 1% of the population, with the highest rate among
AutoimmunityThis includes a range of systemic pathologies or
specific organs that originate from the loss of natural immune tolerance towards self-antigens. The most frequent are Graves’ disease, rheumatoid arthritis, Hashimoto’s thyroiditis, inflammatory bowel disease, type 1 diabetes, multiple sclerosis, systemic lupus erythematosus and Sjögren’s syndrome. Both types of response, cellular and humoral, can contribute to autoimmunity, and their interaction makes the situation more serious (57). Regarding susceptibility to autoimmune disease, several studies have confirmed the importance of the individual genetic structure, of environmental factors such as exposure
REPORT (Result) REPORT (Result)
Data printed: 6.12.2016 Data printed: 21.09.2016
Patient information Patient information
Patient ID Name Patient ID Name
date of birth: 25/02/1989 Gender: Male date of birth: 2/11/1985 Gender: Female
Ethnic group: Caucasian Height: 175 cm Ethnic group: Caucasian Height: 163 cm
Weight: 73kg Registration Date: 6.12.2016 Weight: 53 kg Registration Date: 21.09.2016
Foot support: 1 Foot support: 2
Graph Graph
Right foot Right foot
T-score: 1.9 T-score: -2.9
age age
NormalOsteopeniaOsteoporosis
NormalOsteopeniaOsteoporosis
Result Result
Data scan: 6.12.2016 Scan time: 16:16 Data scan:2016.09.21 Scan time: 15:16
Site: Right foot BQI: 140.3 Site: Right foot BQI: 50.7
T-score: 1.9 T-ratio: 133.6% T-score: -2.9 T-ratio: 48.3%
Z-score: 1.6 Z-ratio: 125.3% Z-score: -3.3 Z-ratio: 45.6%
SOS (m/s); 1559.8 BUA (dB/MHz): 151.7 SOS (m/s); 1481.5 BUA (dB/MHz): 70.8
Table 1 Table showing how the inflammatory parameters of a young female patient affected by systemic lupus erythematosus (SLE) improve or even normalise after periodontal treatment
TESTSBeforetreatment
After treatment
Anti-nuclear antibodies(ANA) (n.v. <1:80)
1:1280 1:640
C3 (n.v. 0.80-1.52) 0.58 g/L 0.68 g/L
C4 (n.v. 0.80-1.52) 0.12 g/L normal
IgG (n.v. 7.51 – 15.60) 17.00 g/L normal
Table 2 Table showing how the inflammatory parameters of a woman aged 45, affected by disabling rheumatoid arthritis, twenty years from the onset of the autoimmune disease, improved or even normalised after periodontal treatment
TESTSBeforetreatment
After treatment
ESR (n.v. <35) 120 mm/h 108 mm/h
C-reactive protein (n.v. <0.5)
1.09 mg/dL normal
Ra-Test (n.v. <30) 110 U/ml 70 U/ml

ItalIan Journal of Dental MeDIcIne vol. 3/1-2018 19
CancerAfter cardiovascular disease, tumours are the
main cause of female death, and epidemiological and socio-economic evidence reveals its heavy impact both individually and on the community. The most common cancers in women are breast, colon, endometrial, lung, cervix, skin and ovary cancer (81, 82). There are numerous data to back an association between chronic periodontitis and cancer (83, 84), particularly as regards oral-oesophageal, head and neck cancer, pancreatic, lung and breast cancer (85-88). In fact, fundamental to carcinogenesis is an inflammatory microenvironment and periodontitis is typically associated with infection, inflammation, bacteraemia and immune response (89).
Recently it has been shown that menopausal women with a history of periodontitis have a 14% higher risk of developing upper quadrant breast cancer compared to the rest of the population and even 36% higher if formerly smokers (87). Similarly, in another population of menopausal women, a history of periodontitis is associated with a 25% higher risk of developing lung cancer, especially for female former smokers (90) and a similar association is also demonstrated for head and neck cancer (91). In a large prospective study that recently took place, the association between periodontitis and mortality from oral-oesophageal and pancreatic cancer was investigated. Even after all the normalisations for the other risk factors, the IgG levels in serum against P. gingivalis correlated both with the severity of the periodontitis and with the risk of tumours of this type (86). Furthermore, the oral microbiome of patients with pancreatic cancer is different from that of the control subjects (92) and P. Gingivalis has been identified as a specific microbial marker of the risk of developing this type of cancer. These findings suggest the need to further characterise the pathogenic bacteria involved in cancer and show how oral hygiene and the dentist can play an important role in eliminating oral pathogens and thus prevent tumours.
menopausal women (64). It is also the one most closely related to periodontitis, shown by historical epidemiological, pathological and immunological data (65, 66). In both diseases, the deregulating of the immune response and the increase in the levels of the mediators of inflammation lead to the destruction of the tissues, respectively periodontal and synovial. A genetic susceptibility is associated with rheumatoid arthritis in 25% of cases, but the contribution of environmental or epigenetic factors seems fundamental (67). Some HLA-DRb1 variants, associated with periodontitis, are also closely related to rheumatoid arthritis and it has been hypothesised that oral bacteria may trigger or advance the disease in genetically predisposed individuals (68). Recent studies have evaluated the effects of periodontal treatment for preventing the onset of rheumatoid arthritis and attenuating its symptoms (69, 70) (Table 1, 2) and, although the mechanisms underlying this association are yet to be fully understood, effective prevention and effective treatment of periodontitis could offer a better quality of life for patients suffering from rheumatoid arthritis.
Alzheimer’s DiseaseAlzheimer’s disease is a progressive and fatal
neurodegenerative disease and a serious geriatric problem worldwide. Clinical signs are cognitive impairment, behavioural changes and communication difficulties (71), while the biochemical signs are the extracellular formation of b-amyloid protein aggregates and intraneuronal neurofibrillary tangles, leading to progressive depressing of synaptic function through to neurodegeneration (72). The early onset form is considered a genetic disease, while the sporadic type is influenced by environmental factors such as age, diet, diabetes, hypertension and a history of head trauma (73, 74). It is also characterised by a strong gender imbalance (two out of three patients are women), partly attributed to longer female life expectancy but also to sex hormones and genetic factors (75).
Several studies have suggested, and sought to clarify, the enigmatic role of periodontal disease as a risk factor for Alzheimer’s disease and vice versa (76, 77). While it is true that people suffering from Alzheimer’s disease may, over time, become less able to take care of their oral hygiene, given the chronic inflammatory nature of both diseases, periodontitis could in turn contribute to the onset of low-grade systemic inflammation and bolster the neurodegenerative process of Alzheimer’s disease (78, 79). If a causal relationship between periodontitis and cognitive impairment were to be demonstrated, then effective periodontal treatment could be beneficial for Alzheimer patients. A study has already yielded promising results in this respect (80).
Figure 8 Dual-energy X-ray absorptiometry (DXA) in a young woman with aggressive periodontitis and osteoporosis at the femoral neck
ItalIan Journal of Dental MeDIcIne vol. 3/1-201820
between periodontal infections and systemic disease. Clin Microbiol Infect 2007;13(4):3-10.
8. Martelli FS, Fanti E, Rosati C et al. Long-term efficacy of microbiology-driven periodontal laser-assisted therapy. Eur J Clin Microbiol Infect Dis 2016;35(3):423-431.
9. Shiau HJ, Aichelmann-Reidy ME, Reynolds MA Influence of sex steroids on inflammation and bone metabolism. Periodontol 2000 2014;64(1):81-94.
10. Shourie V, Dwarakanath CD, Prashanth GV et al. The effect of menstrual cycle on periodontal health - a clinical and microbiological study. Oral Health Prev Dent 2012;10(2):185-92.
11. Suri V, Suri V. Menopause and oral health. J Midlife Health 2014 Jul;5(3):115-20.
12. Wojcicki CJ, Harper DS, Robinson PJ. Difference in periodontal disease-associated microorganisms of subgingival plaque in prepubertal, pubertal, and postpubertal children. J Periodontol 1987;58:219-223.
13. Saini R, Saini S, Sharma S. Oral contraceptives alter oral health. Ann Saudi Med 2010;30(3):243.
14. Salles JP. Bone metabolism during pregnancy. Ann Endocrinol (Paris) 2016;77(2):163-168.
15. Lamonte MJ, Hovey KM, Genco RJ, et al. Five-year changes in periodontal disease measures among postmenopausal women. The Buffalo osteoperio study. J Periodontol. 2013;84:572–584.
16. McCarthy MM, Arnold AP, Ball GF et al. Sex differences in the brain: the not so inconvenient truth. J Neurosci 2012;5:2241-2247.
17. Maas AH, Appelman YE. Gender differences in coronary heart disease. Neth Heart J 2010;5:598-602.
18. Voskuhl R. Sex differences in autoimmune diseases. Biol Sex Differ 2011;2(1):1.
19. Mascarenhas MN, Flaxman SR, Boerma T et al. National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. PLOS MED 2012;9(12):e1001356.
20. Thomson F, Shanbhag S, Templeton A et al. Obstetric outcome in women with subfertility. Br J Obstet Gynaecol 2005;5:632-637.
21. Blencowe H, Cousens S, Chou D et al. Born too soon: The global epidemiology of 15 million preterm births. Reprod Health 2013 10(Suppl 1):S2.
22. Corbella S, Taschieri S, Del Fabbro M, et al. Adverse pregnancy outcomes and periodontitis: A systematic review and meta-analysis exploring potential association. Quintessence Int 2016;47(3):193-204.
23. Gonzales-Marin C, Spratt DA, Allaker RP. Maternal oral origin of Fusobacterium nucleatum in adverse pregnancy outcomes as determined using the16S-23S rRNA gene intergenic transcribed spacer region. J MedMicrobiol 2013;62:133-144.
24. Katz J, Chegini N, Shiverick KT, et al. Localization of P. gingivalis in preterm delivery placenta. J Dent Res 2009;88(6):575-578.
25. Aagaard K, Ma J, Antony KM et al. The placenta harbors a unique microbiome. Sci Transl Med 2014;6(237):287ra65.
26. Vannuccini S, Clifton VL, Fraser IS et al. Infertility and reproductive disorders: impact of hormonal and inflammatory mechanisms on pregnancy outcome. Hum Reprod Update 2016;22(1):104-15.
27. Pretorius C, Jagatt A, Lamont RF. The relationship between periodontal disease, bacterial vaginosis, and preterm birth. J Perinat Med 2007;35(2):93-99.
ConclusionsData in the literature suggest that oral pathogenic
bacteria may promote the development of systemic diseases through two pathways: systemic dissemination from oral sites to distal tissues and the furthering of local inflammatory phenomena, and/or chronic systemic inflammation induced by bacteraemia and inflammatory cytokines produced in periodontal lesions that have entered the circulation.
The direct involvement of oral pathogenic bacteria is documented as the prime mover in endothelial dysfunction (93), in the association between periodontitis and rheumatoid arthritis (94) and between periodontitis and Alzheimer’s disease (95). Furthermore, the presence of F. nucleatum and P. gingivalis bacteria is directly correlated to colorectal cancer (96) and to orodigestive and pancreatic tumours (86) respectively.
Systemic inflammation is implicated in endothelial dysfunction (97), in the cognitive impairment typical of Alzheimer’s disease (98) and in molecular mechanisms linked to the development and progression of cancer (99, 100).
Although further investigations aimed at clarifying the mechanisms underlying the association between periodontitis and systemic diseases are necessary and desirable, the hypothesis that periodontal disease is a significant risk factor for many of these disorders is evident (101). It is also increasingly urgent that a gender-specific approach be applied in considering epidemiology and disease progression. The literature analysed in this paper suggests an implication of periodontal disease in many systemic disorders specific to women or with a major impact on them, and reveals the importance of a joint effort by doctors and dentists towards better managing women’s health.
References1. Socransky SS, Haffajee AD, Cugini MA, et al. Microbial
complexes in subgingival plaque. J Clin Periodontol 1998;25(2):134-144.
2. Yucel-Lindberg T, Båge T. Inflammatory mediators in the pathogenesis of periodontitis. Expert Rev Molecular Med 2013;15:e7
3. Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontology 2000 2013;62(1):59–94.
4. Loos BG, John RP, Laine ML. Identification of genetic risk factors for periodontitis and possible mechanisms of action. J Clin Periodontol 2005;32(supplement 6):159–179.
5. Nibali L, Donos N, Henderson B. Periodontal infectogenomics. J Med Microbiol 2009;58:1269-1274.
6. Stabholz A, Soskolne WA, Shapira L. Genetic and environmental risk factors for chronic periodontitis and aggressive periodontitis. Periodontology 2000 2010;53(1):138–153.
7. Seymour GJ, Ford PJ, Cullinan MP et al. Relationship

ItalIan Journal of Dental MeDIcIne vol. 3/1-2018 21
47. Van Dyke TE, van Winkelhoff AJ. Infection and inflammatory mechanisms. J Periodontol 2013;84(4 suppl):S1–S7.
48. Ahmed U, Tanwir F. Association of periodontal pathogenesis and cardiovascular diseases: a literature review. Oral Health Prev Dent 2015;13(1):21-27.
49. Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation 2011;123:933-944.
50. Yu YH, Chasman DI, Buring JE et al. Cardiovascular risks associated with incident and prevalent periodontal disease. J Clin Periodontol 2015;42(1):21-28.
51. Zebrack JS, Anderson JL. The role of infection in the pathogenesis of cardiovascular disease. Prog Cardiovasc Nurs 2003;18(1):42-49.
52. Teles R, Wang CY. Mechanisms involved in the association between periodontal diseases and cardiovascular disease. Oral Dis 2011;17(5):450-61
53. Schenkein HA, Loos BG. Inflammatory mechanisms linking periodontal diseases to cardiovascular diseases. J Periodontol 2013;84(4 Suppl):S51-69.
54. Inaba H, Amano A. Roles of oral bacteria in cardiovascular diseases from molecular mechanisms to clinical cases: Implication of periodontal diseases in development of systemic diseases. J Pharmacol Sci 2010;113(2):103-109.
55. Wada K, Kamisaki Y. Roles of oral bacteria in cardiovascular diseases from molecular mechanisms to clinical cases: Involvement of Porphyromonas gingivalis in the development of human aortic aneurysm. J Pharmacol Sci 2010;113(2):115-119.
56. Li L, Messas E, Batista EL Jr, et al. Porphyromonas gingivalis infection accelerates the progression of atherosclerosis in a heterozygous apolipoprotein E deficient murine model. Circulation 2002;105:861–867.
57. Mackay IR. Tolerance and autoimmunity. West J Med 2001;174:118-123.
58. Willer CJ, Dyment DA, Risch NJ, et al. Canadian Collaborative Study. Twin concordance and sibling recurrence rates in multiple sclerosis. Proc Nat Acad Sci USA 2003;100:12877-12882.
59. Ngo ST, Steyn FJ, McCombe PA. Gender differences in autoimmune disease. Front Neuroendocrinol 2014;35(3):347-369.
60. Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol 2016 Oct;16(10):626-638.
61. Asaba J, Bandyopadhyay M, Kindy M, Dasgupta S. Estrogen receptor signal in regulation of B cell activation during diverse immune responses. Int J Biochem Cell Biol 2015 Nov;68:42-47.
62. Migeon BR. The role of X inactivation and cellular mosaicism in women’s health and sex-specific diseases. J Am Med Assoc 2006;295:1428-1433.
63. Camprubi C, Monk D. Does genomic imprinting play a role in autoimmunity? In: Ballestar, E. (Ed.), Epigenetic contributions in autoimmune disease. Springer New York, USA; 2011.
64. McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med 2011;365:2205-2219.
65. Dissick A, Redman RS, Jones M, et al. Association of periodontitis with rheumatoid arthritis: a pilot study. J Periodontol 2010;81:223-230.
28. Prescott J, Farland LV, Tobias DK, et al. A prospective cohort study of endometriosis and subsequent risk of infertility. Hum Reprod 2016;31(7):1475-1482.
29. Lebovic DI, Mueller MD, Taylor RN. Immunobiology of endometriosis. Fertil Steril 2001;75:1-10.
30. Lane NE. Epidemiology, etiology, and diagnosis of osteoporosis. Am J Obstet Gynecol 2006;194(2 Suppl):S3-11.
31. Rosen CJ. in: De Groot LJ, Beck-Peccoz P, Chrousos G et al. editors. The Epidemiology and Pathogenesis of Osteoporosis. Endotext (Internet). South Dartmouth (MA) 2014.
32. Wehren LE. The epidemiology of osteoporosis and fractures in geriatric medicine. Clin Geriatr Med 2003;19:245-258.
33. Gao Y, Qian WP, Dark K, et al. Estrogen prevents bone loss through transforming growth factor beta signaling in T cells. Proc Natl Acad Sci USA 2004;101:16618–16623.
34. Thakkinstian A, D’Este C, Eisman J et al. Meta-analysis of molecular association studies: vitamin D receptor gene polymorphisms and BMD as a case study. J Bone Miner Res 2004;19:419-428.
35. Khadilkar VV, Khadilkar AV. Use of vitamin D in various disorders. Indian J Pediatr 2013;80(3):215-218.
36. Martelli FS, Martelli M, Rosati C et al. Vitamin D: relevance in dental practice. Clin Cases Miner Bone Metab 2014;11(1):15-19.
37. Groen JJ, Menczel J, Shapiro S. Chronic destructive periodontal disease in patients with presenile osteoporosis. J Periodontol 1968;39(1):19-23.
38. Pereira FM, Rodrigues VP, de Oliveira AE, et al. Association between periodontal changes and osteoporosis in postmenopausal women. Climacteric 2015;18(2):311-315.
39. Lin TH, Lung CC, Su HP, et al. Association between periodontal disease and osteoporosis by gender: a nationwide population-based cohort study. Medicine (Baltimore) 2015;94(7):e553.
40. Guiglia R, Di Fede O, Lo Russo L, et al. Osteoporosis, jawbones and periodontal disease. Med Oral Patol Oral Cir Bucal 2013;18(1):e93-9.
41. Lerner UH. Inflammation-induced Bone remodelling in periodontal disease and the influence of post-menopausal osteoporosis. J Dent Res 2006;85:596-607.
42. Banos G, Guarner V, Perez-Torres I. Sex steroid hormones, cardiovascular diseases and the metabolic syndrome. Cardiovascular & Hematological Agents in Medicinal Chemistry 2011;9:137-146.
43. Ahmed R, Dunford J, Mehran R et al. Preeclampsia and future cardiovascular risk among women. A review. J Am Coll Cardiol 2014;63:1815-1822.
44. Udell JA, Lu H, Redelmeier DA. Long-term cardiovascular risk in women prescribed fertility therapy. J Am Coll Cardiol 2013; 62: 1704–1712.
45. Writing Group for the Women’s Health Initiative Investigators: Risks and benefits of estrogen plus progestin in healthy postmenopausal women. Principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002;288:321–333.
46. Lindhe J, Haffajee AD, Socransky SS. Progression of periodontal disease in adult subjects in the absence of periodontal therapy. J Clin Periodontol 1983;10(4):433-442.

ItalIan Journal of Dental MeDIcIne vol. 3/1-201822
87. Freudenheim JL, Genco RJ, LaMonte MJ et al. Periodontal disease and breast cancer: prospective cohort study of postmenopausal women. Cancer Epidemiol Biomarkers Prev 2016;25(1):43-50.
88. Nwizu NN, Marshall JR, Moysich K et al. Periodontal disease and incident cancer risk among postmenopausal women: results from the Women’s Health Initiative Observational Cohort. Cancer Epidemiol Biomarkers Prev 2017 Aug;26(8):1255-1265.
89. Colotta F, Allavena P, Sica A et al. Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis 2009;30:1073-1081.
90. Mai X, LaMonte MJ, Hovey KM et al. History of periodontal disease diagnosis and lung cancer incidence in the Women’s Health Initiative Observational Study. Cancer Causes Control 2014;25(8):1045-1053.
91. Tezal M, Sullivan MA, Hyland A et al. Chronic periodontitis and the incidence of head and neck squamous cell carcinoma. Cancer Epidemiol Biomarkers Prev 2009;18(9):2406-2412.
92. Farrell JJ, Zhang L, Zhou H, et al. Variations of oral microbiota are associated with pancreatic diseases including pancreatic cancer. Gut 2012;61:582-588.
93. Gurav AN. The implication of periodontitis in vascular endothelial dysfunction. Eur J Clin Invest 2014;44(10):1000–1009.
94. Bartold PM, Marino V, Cantley M, et al. Effect of Porphyromonas gingivalis-induced inflammation on the development of rheumatoid arthritis. J Clin Periodontol 2010;37(5):405-411.
95. Noble JM, Scarmeas N, Celenti RS et al. Serum IgG antibody levels to periodontal microbiota are associated with incident Alzheimer Disease. PLoS ONE 2014;9(12):e114959.
96. Whitmore SE, Lamont RJ. Oral bacteria and cancer. PLoS Pathog 2014;10:e1003933.
97. Iwai T. Periodontal bacteremia and various vascular diseases. J Periodont Res 2009;44:689-694.
98. Ide M, Harris M, Stevens A et al. Periodontitis and cognitive decline in Alzheimer’s Disease. PLoS One 2016;11(3):e0151081.
99. Mantovani A, Allavena P, Sica A et al. Cancer-related inflammation. Nature 2008;454:436–444.
100. Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol 2015;15(1):30-44.
101. Nazir MA. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int J Health Sci (Qassim) 2017 Apr-Jun;11(2):72-80.
66. Mercado FB, Marshall RI, Klestov AC, et al. Relationship between rheumatoid arthritis and periodontitis. J Periodontol 2001;72:779-787.
67. Viatte S, Barton A. Genetics of rheumatoid arthritis susceptibility, severity, and treatment response. Semin Immunopathol 2017 Jun;39(4):395-408.
68. Ogrendik M, Kokino S, Ozdemir F et al. Serum antibodies to oral anaerobic bacteria in patients with rheumatoid arthritis. Med Gen Med 2005;7(2):2.
69. Scher JU, Bretz WA, Abramson SB. Periodontal disease and subgingival microbiota as contributors or RA pathogenesis: modifiable risk factors? Curr Opin Rheumatol 2014;26(4):424-429.
70. Roman-Torres CV, Neto JS, Souza MA et al. An evaluation of non-surgical periodontal therapy in patients with rheumatoid arthritis. Open Dentistry J 2015;9:150-153.
71. Galimberti D, Scarpini E. Progress in Alzheimer’s disease. J Neurol 2012;259:201-211.
72. Alzheimer’s Association. 2014 Alzheimer’s disease facts and figures. Alzheimers Dement 2014;10(2):e47-92.
73. Bertram L, Lill CM, Tanzi RE. The genetics of Alzheimer disease: back to the future. Neuron 2010;68:270-281.
74. Barnes LL, Wilson RS, Schneider JA et al. Gender, cognitive decline, and risk of AD in older persons. Neurology 2003;60(11):1777-1781.
75. Seshadri S, Wolf PA, Beiser A et al. Lifetime risk of dementia and Alzheimer’s disease. The impact of mortality on risk estimates in the Framingham Study. Neurology 1997;49:6.
76. Abbayya K, Puthanakar NY, Naduwinmani S et al. Association between Periodontitis and Alzheimer’s Disease. N Am J Med Sci 2015;7(6):241-246.
77. Ganesh P, Karthikeyan R, Muthukumaraswamy A, Anand J. A potential role of periodontal inflammation in Alzheimer’s disease: a review. Oral Health Prev Dent 2017;15(1):7-12.
78. Martande SS, Pradeep AR, Singh SP et al. Periodontal health condition in patients with Alzheimer’s disease. Am J Alzheimers Dis Other Demen 2014;29:498-502.
79. Gurav AN. Alzheimer’s disease and periodontitis: an elusive link. Rev Assoc Med Bras 2014;60(2):173-180.
80. Rolim Tde S, Fabri GM, Nitrini R, et al. Evaluation of patients with Alzheimer’s disease before and after dental treatment. Arq Neuropsiquiatr 2014;72:919-924.
81. American Cancer Society. Cancer facts and Figures 2014. Atlanta (GA): 2014.
82. Torre LA, Bray F, Siegel RL et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65(2):87-108.
83. Fitzpatrick SG, Katz J. The association between periodontal disease and cancer: a review of the literature. J Dentistry 2010;38:83-95.
84. Dizdar O, Hayran M, Guven DC, Yılmaz TB, Taheri S, Akman AC, Bilgin E, Hüseyin B, Berker E. Increased cancer risk in patients with periodontitis. Curr Med Res Opin 2017 Aug 11:1-6.
85. Ahn J, Segers S, Hayes RB. Periodontal disease, Porphyromonas gingivalis serum antibody levels and orodigestive cancer mortality. Carcinogenesis 2012;33:1055-1058.
86. Michaud DS, Izard J, Wilhelm-Benartzi CS et al. Plasma antibodies to oral bacteria and risk of pancreatic cancer in a large European prospective cohort study. Gut 2013;62:1764-1770.





![Microbial and metabolomic analysis of gingival crevicular ... · 2]. Periodontitis affects the majority of adults worldwide and may cause various systemic diseases, including dia-betes](https://img.pdfslide.net/doc/110x75/5ffe1bd5f6ee7b7ad975583c/microbial-and-metabolomic-analysis-of-gingival-crevicular-2-periodontitis.jpg)























