-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
1/27
PERIOPERATIVE CARDIAC
DYSRRHYTHMIAS
Agya Boakye Prempeh
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
2/27
FORMAT
INTRODUCTION
ANATOMY OF THE CARDIAC CONDUCTION SYSTEM
NORMAL CARDIAC ELECTROPHYSIOLOGY
MECHANISM
RISK FACTORS
MANAGEMENT
ANAESTHETIC CONSIDERATION
CONCLUSION
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
3/27
INTRODUCTION
DEFINITION Abnormal cardiac rate or rhythm
- Asymptomatic/Symptomatic/lethal
INCIDENCE Most frequent perioperative cardiovascular
abnormality
- In a multicenter study with 17,201 patients
70.2% of cases had dysrrhythmias duringcardiac or noncardiac
surgery combined,1.6% were treated
>90% of cases had dysrrhythmias during cardiac surgery
alone
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
4/27
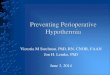
ANATOMY OF THE CARDIAC
CONDUCTION SYSTEM
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
5/27
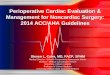
NORMAL CARDIAC
ELECTROPHYSIOLOGY
SINOATRIAL NODE VENTRICULAR MUSCLE
4
0
1
2
3
4
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
6/27
MECHANISM OF CARDIAC
DYSRRHYTHMIAS
There are two(2) broad groups:
A) Disorders of impulse initiation
B) Disorders of impulse conduction
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
7/27
DISORDERS OF IMPULSE INITIATION
This also grouped into two(2)
1) Alteration of Automaticity
2) Triggered Activity
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
8/27
ALTERATION OF AUTOMATICITY
A
Maximum diastolic potential(K+ conductance)
- Ach eg. Vagal manuevres
- Hypoxia/Hypokalaemia
B Slope of phase 4 (Na+ leak)
-Catecholamines eg. pain
- Ach
C Threshold of Action Potential
AB
C
Defn: Alteration of spontaneous phase 4 depolarisation
Origin: SA node / Ectopic Focus(nonpacemaker attributes)
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
9/27
TRIGGERED ACTIVITY
Defn: Action Potential(AP) which initiates membrane
potential oscillations(afterdepolarisation)
during late phase 2 or Phase 3 or Phase 4.
When the membrane potential oscillations reach
threshold potential a new AP is formed.
aetiology : intracellular calcium overload( Digitalis toxicity,
long QT syndrome)
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
10/27
DISORDERS OF IMPULSE CONDUCTION
This is grouped into two(2)
1) Conduction blocks along normal pathway
2) Abnormal pathway conduction
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
11/27
CONDUCTION BLOCKS ALONG NORMAL PATHWAY
Defn: There is failure of successful conduction of
impulse along normal pathway.
Aetiology : - Reduction in tissue excitability
- Abnormalities of gap junctions btn cells
Site of Block : a) SA node
b) AV node
c) Intraventricular(BBB) doesnt slow heart
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
12/27
ABNORMAL PATHWAY CONDUCTION
Defn: Conduction of an impulse along an abnormal tract
Tract maybe anatomical-(WPW) or functional-(SVTA)
3 Conditions to be satisfied
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
13/27
RISK FACTORS FOR DEVELOPING
CARDIAC DYSRRHYTHMIAS
This can be grouped into three(3)
- Patient related factors
- Anaesthesia related factors
- Surgery related factors
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
14/27
PATIENT RELATED FACTORS
1) CVS abnormality Preexisting cardiac disease eg. MI
- Pulmonary/Coronary thrombosis
2) Respiratory abnormality : Tension pneumothorax
3) CNS abnormality : Intracranial diseases esp. SAH may
show ECG abnormalities such as
Q waves, ST segment changes, QT
interval changes, U waves
4) Aging Degenerative changes in atrial anatomy
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
15/27
ANAESTHESIA RELATED FACTORS
Technique GA / CNAB
Direct laryngoscopy and tracheal intubation -commonest cause
Hypoxia/Hypercarbia/Acidosis
Hypothermia/Hyperthermia
Hypovolaemia
Central venous cannulation
Pressure from fingers can stimulate carotidsinus reflexes during
jugular venous cannul.
- Excessive insertion of catheter into rightatrium
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
16/27
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
17/27
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
18/27
SURGERY RELATED FACTORS
1) General surgery
Traction on peritoneum (bradyarrhythmias)
2) Dental surgery Profound stimulation of both
parasympathetic and sympathetic
nervous systems
3) Cardiac surgery Retraction of beating heart
- Taking sutures over the right atrium
- Damage to conduction pathway by
surgical incision- Immediate period following release of
aortic cross clamp
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
19/27
MANAGEMENT OF CARDIAC
DYSRRHYTHMIAS
Dependent on whether bradydysrrhythmia/tachydysrrhythmia
BRADYDYSRRHYTHMIAS
Defn: Heart rate < 60bpm and inadequate for clinical
condition
Origin SA node (examples)/ AV node(examples)
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
20/27
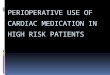
MANAGEMENT OF BRADYDYSRRHYTHMIAS
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
21/27
TACHYDYSRRHYTHMIAS
Defn: Heart rate > 100 bpm
Classification based on:
1. Appearance of QRS Complexes Narrow(0.12 sec)
2. Rhythm Regular/ irregular
3. Origin SA node/ atria/ AV node/ Ventricle
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
22/27
MANAGEMENT OF TACHYDYSRRHYTHMIAS
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
23/27
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
24/27
ANAESTHETIC CONSIDERATION
ECG monitoring All patients
- Lead 11 and V5
Routine measures intraop Airway patent eg. SAB
- Breathing: Adequate
ventilation andoxygenation
- Cardiac history/pathology
reevaluation
- Depth of anaesthesia adequate
- Electrolytes and ABGs optimum- Temperature
Specific therapy depends on type of dysrrhythmia
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
25/27
CONCLUSION
Most perioperative dysrrhythmias are benign without
significant
haemodynamic consequences.
However symptomatic patients whose dysrrhythmias can evolve to
life-
threatening ones should be treated with anti-dysrrhythmic drugs
or
electrotherapy promptly.
Finally, anti-dysrrhythmic drugs can also cause dysrrhythmias
and often
times the anaesthetist in an attempt to treat perioperative
dysrrhythmias
causes iatrogenesis and as such the knowledge of the physiology
of cardiac
rhythm, pathogenesis of dysrrhythmias, anaesthetic pharmacology
and riskto benefit of anti-dysrrhythmic drugs are mandatory.
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
26/27
ACKNOWLEDGEMENT
Dr Baddoo
Dr Djagbletey
-
8/13/2019 Perioperative Cardiac Dysrrhythmias Presentation
Final
27/27
THANK YOU