Embed Size (px)
Citation preview
AORN J O U R N A L
Opinion
AUGUST 1989, VOL. 50, NO 2
Perioperative nurses must prepare themselves to monitor patients receiving local anesthesia
ith the increased use of local anesthesia W on elderly and high-risk patients in ambulatory surgery, the challenge of providing safe. adequate patient care and supervision in the operating room has become an important issue to the OR nursing staff.
To the uninitiated. local anesthesia is equated with minor procedures. Patients receiving local anesthesia, however. may have serious health problems that preclude using general anesthesia. Those problems represent a challenging array of potential complications to OR nurses.
At times, OR nurses take responsibility for monitoring patients receiving local anesthesia without knowing the patients' medical or surgical history, laboratory results, or the status of their
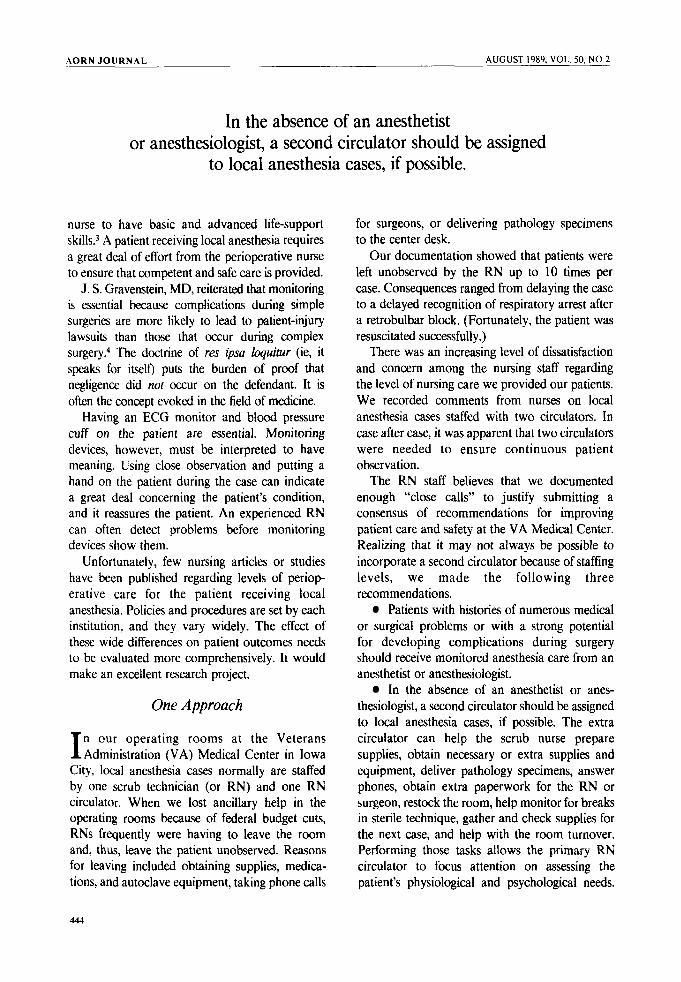
Sharon Petrone, RN, BSN, CNOR, CCRN, is an OR/PACU staff nurse at the Veterans Administration Medical Center, Iowa Civ. She received her bachelor of science degree in nursing from the University of Iowa College of Nursing, lo wa City.
electrocardiograms (ECGs). Often, the first time an OR nurse sees the patient and the chart is when they arrive simultaneously in the OR suite. In addition, many local anesthesia procedures are completed with the patient having only minimal laboratory tests and a brief history and physical examination.
On some cases, OR nurses perform their regular circulating duties in addition to monitoring the patient's condition, administering narcotics, determining arrhythmias, and anticipating and providing the necessary medications and emer- gency equipment, when needed.
Importance of Monitoring
number of articles have been written A regarding complications in patients receiving local anesthesia. Reviewing those articles will help the nurse prepare for the patient.
The articles cite the immense importance of closely monitoring the patient throughout the procedure. Monitoring is necessary to guard against human errors? which are common, and equipment failures, which are uncommon.l
One article stated that local anesthesia with careful monitoring is the preferred choice for older or sick patients for ophthalmic surgery.2 It cites respiratory arrest as a major complication with retrobulbar block occurring two to 40 minutes after injection, thus emphasizing the importance of close patient observation.
Another article stated that potential life- threatening complications can occur during local anesthesia cases, which require the perioperative
442
A O R N J O U R N A L AUGUST 1989. VOL. 50, NO 2
In the absence of an anesthetist or anesthesiologist, a second circulator should be assigned
to local anesthesia cases, if possible.
nurse to have basic and advanced life-support skills.3 A patient receiving local anesthesia requires a great deal of effort from the perioperative nurse to ensure that competent and safe care is provided.
J. S . Gravenstein, MD, reiterated that monitoring is essential because complications during simple surgeries are more likely to lead to patient-injury lawsuits than those that occur during complex surgery! The doctrine of res @a loquinrr (ie, it speaks for itself) puts the burden of proof that negligence did not occur on the defendant. It is often the concept evoked in the field of medicine.
Having an ECG monitor and blood pressure cuff on the patient are essential. Monitoring devices, however, must be interpreted to have meaning. Using close observation and putting a hand on the patient during the case can indicate a great deal concerning the patient’s condition, and it reassures the patient. An experienced RN can often detect problems before monitoring devices show them.
Unfortunately, few nursing articles or studies have been published regarding levels of periop- erative care for the patient receiving local anesthesia. Policies and procedures are set by each institution, and they vary widely. The effect of these wide differences on patient outcomes needs to be evaluated more comprehensively. It would make an excellent research project.
One Approach
n our operating rooms at the Veterans I Administration (VA) Medical Center in Iowa City, local anesthesia cases normally are staffed by one scrub technician (or RN) and one R N circulator. When we lost ancillary help in the operating rooms because of federal budget cuts, RNs frequently were having to leave the rmm and, thus, leave the patient unobserved. Reasons for leaving included obtaining supplies, medica- tions, and autoclave equipment, taking phone calls
for surgeons, or delivering pathology specimens to the center desk.
Our documentation showed that patients were left unobserved by the R N up to 10 times per case. Consequences ranged from delaying the case to a delayed recognition of respiratory arrest after a retrobulbar block. (Fortunately, the patient was resuscitated successfully.)
There was an increasing level of dissatisfaction and concern among the nursing staff regarding the level of nursing care we provided our patients. We recorded comments from nurses on local anesthesia cases staffed with two circulators. In case after case, it was apparent that two circulators were needed to ensure continuous patient observation.
The R N staff believes that we documented enough “close calls” to justify submitting a consensus of recommendations for improving patient care and safety at the VA Medical Center. Realizing that it may not always be possible to incorporate a second circulator because of staffing levels, we made the following three recommendations.
Patients with histories of numerous medical or surgical problems or with a strong potential for developing complications during surgery should receive monitored anesthesia care from an anesthetist or anesthesiologist.
In the absence of an anesthetist or anes- thesiologist, a second circulator should be assigned to local anesthesia cases, if possible. The extra circulator can help the scrub nurse prepare supplies, obtain necessary or extra supplies and equipment, deliver pathology specimens, answer phones, obtain extra paperwork for the RN or surgeon, restock the room, help monitor for breaks in sterile technique, gather and check supplies for the next case, and help with the room turnover. Performing those tasks allows the primary R N circulator to focus attention on assessing the patient’s physiological and psychological needs.
AORN J O U R N A L AUGUST 1989. VOL. 50. NO 2
Areas to assess include special positioning needs, allergies, complications from medications given with previous local anesthetics, beta-blockers that will affect epinephrine use during the case, the patient’s anxiety level, the operative permit, and all emergency equipment to ensure it is available and functional.
All patients receiving local anesthesia deserve continuous monitoring by an RN while in the OR suite. The AORN Journal has emphasized the importance of the anesthetist’s or nurse’s role in monitoring the patient and in providing physical and emotional support during surgery.’
In the event a second circulator is not available, the scrub technician or nurse should be ready before the patient is taken into the room. A “runner” should be available to allow the circulating nurse to monitor the patient throughout the procedure.
Notes 1. J S Gravenstein, D A Paulus, Clinical Monitoring
Practice, second ed (Philadelphia: J B Lippincott, 1987) 2- 12.
2. J M Nicoll et al, “Central nervous system complications after 6,000 retrobulbar blocks,” Anesthesia & Analgesia 66 (December 1987) 1298- 1302.
3. D F hey, “Local anesthesia: Implications for the perioperative nurse.” AORN Journal 45 (March 1987)
4. G A Blumenreich, “The doctrine of res ipsa loquitur,” Journal of the American Association of Nurse Anesthetists 55 (February 1987) 13-15.
5. D M Fog, “Recommendations for instrument counts: testing sterilizers with biological indicators; organizational structure of the OR,” (Clinical Issues) AORN Journal 49 (June 1989) 1669-1672.
682-689.
Suggested reading “Monitoring the patient receiving local anesthesia.” In
AORN Standarh and Recommended Practices for Perioperative Nursing. Denver: Association of Operating Room Nurses, Inc, 1989,1117-I to 7-2.
Discussion
erioperative nurses need the necessary P monitoring skills that come from knowledge, experience, and a genuine concern for the patients under your care. They trust you. You owe your full attention to their care throughout the procedure.
In deference to the time factor that has become so important in the operating room, it is our responsibility as advocates to insist on the few minutes it may take to familiarize ourselves with our patients, their medical history and problems, and their psychological preparation for the procedure. Only we know when the operating room is ready to accept the patient and when all emergency equipment, medications, and supplies are ready.
We have a duty to not allow surgeons to begin until we are fully satisfied that all preparations for safe patient care have been made. At one time or another, we have all allowed ourselves to be rushed into beginning a case before we felt prepared, and that unprepared feeling remained with us the entire case. For the patient’s sake, we must not allow that to happen.
SHARON PETRONE, RN, CNOR
Learning to Cope With Exercise-induced Asthma Despite experiencing exercise-induced asthma, people can still participate in recreational sports or competitive athletics, according to the June 1989 issue of Mayo Clinic Health Letter.
People who experience exercise-induced asthma usually have chronic asthma. The symp- toms are identical to chronic asthma symp- toms-congested lungs and difficult breathing.
Symptoms may begin either during strenuous activity or three to six hours after exercising. Peo- ple are more susceptible to an attack during the first six minutes of exercise. If they continue exer- cising beyond eight minutes, they may find that their symptoms improve. Most attacks go away by themselves within 45 minutes to an hour.
People should select activities that are less likely to cause exercise-induced asthma attacks (ie, indoor swimming as opposed to outdoor running). Other ways for people to reduce exercise-induced asthma attacks are to work out regularly, warm up before working out, and take appropriate medications before participating in a sport.



















![Anesthesia Management and Perioperative Mortality.30[1]](https://img.pdfslide.net/doc/110x75/5535981155034676718b4675/anesthesia-management-and-perioperative-mortality301.jpg)









