Embed Size (px)
Citation preview
FEBRUARY 1995, VOL 61, NO 2 *McNurnura* .
Perioperative Nurses’ Perceptions of Caring Practices
ndividuals who are unfamiliar with the periopera- tive environment often view perioperative nursing practice as being technically centered and having a limited emphasis on caring.’ Much of perioperative I nursing research has been technical, quantitative
studies designed to validate the visual aspects of pen- operative nursing practice. Minimal documentation of caring practices in perioperative nursing exists, and the essence of caring in this setting often is invisible.
UlZRATURE R M E W Examination of the literature revealed a growing
body of research based on the theory developed by M. Jean Watson, RN, PhD, FAAN. Dr Watson’s the- ory, Nursing: Human Science and Human Care, is based on her views of personhood and human exis- tence. This existence of persons is greater than just being physical, mental, and emotional parts. Dr Wat- son’s notions of personhood transcend the objective time and space through the “concept of soul . . . spirit, inner self, or essence of the person.”2 Her beliefs are reflected in the value system of the theory, which places great regard and reverence for the person and
A B S T R A C T
life with autonomy and freedom of choice. Dr Wat- son believes the highest value is the subjective inter- nal world of the experiencing person and how the person (both patient and nurse) perceives and experi- ences his or her inner world. According to Dr Wat- son, nursing is a human-to-human caring process that responds to each person’s unique inner world. The goal of nursing is to help the person achieve harmony through self-healing, self-care, and self-actualization. According to this theory, nursing practice is based on 10 carative factors:
humanistic/altruistic system of values, faithhope; sensitivity to self and others; helpinghusting, human care relationships; expressing positive and negative feelings; creative problem-solving caring process; transpersonal teachindearning; supportive, protective, and/or corrective mental, physical, societal, and spiritual environment; human needs assistance; and existential/phenomenological/spiritual forces.
These factors are preceded by a humanistic value system, a scientific knowledge base, and the nurse’s clinical competence. Dr Watson em-
This study was designed to determine how caring is practiced in peri- operative nursing. The theory of nursing by M. Jean Watson, RN, PhD, FAAN, provided the conceptual framework for the study. The researcher used a qualitative, descriptive methodology to analyze data collected in audiotaped interviews with five perioperative nurses and used standard qualitative research procedures for transcribing and analyzing the interview data. The five study participants identified their perceptions of caring behav- iors with conscious and unconscious patients in the preoperative, intraoper- ative, and postoperative periods. They described the essential structure of caring as the establishment of a human care relationship and provision of a supportive, protective, and/or corrective psychological, physical, and spiritu- al environment. AORN J 61 (Feb 1995) 377-388.
phasizes that the patient and nurse find meaning in each car- ing experience, which promotes the caring transaction and the process of being and becoming that restores inner h a r m ~ n y . ~
Numerous other models of caring have been developed and r e p ~ r t e d , ~ and several authors have addressed the dual aspects of caring in nurs- ing (ie, the delicate balance
S H A R O N A . M c N A M A R A , R N
377 AORN JOURNAL

FEBRUARY 1995, VOL 61, NO 2 9 McNamara
between art and ~c ience) .~ Articles in the literature also address the concept of caring as having central importance to nursing.6 One group of researchers studied new methods for measuring competency- based caring nursing practice: and another researcher examined practicing nurses’ experiences of caringx Two other researchers studied nurses’ understanding of the meaning of the caring relationships that exist between patients and nurse^.^
A researcher in New York reviewed and synthe- sized nine nursing studies of the behaviors that patients identify as evidence of caring by nurses.10 In two other studies, researchers shared methodologies and an instrument to investigate nurses’ caring behaviors as described by patients who were recov- ering from ambulatory surgery and myocardial infarctions.!’
The literature review uncovered only minimal work in the area of perioperative nurses’ caring behaviors. Two researchers in the 1980s studied OR personnel by observing 23 functions (eg, preoperative assessment, patient teaching, documentation of care in the OR, maintenance of sterile fields).’? Although these functions were evaluated only as behaviors that were observed (ie, they were not evaluated as caring behaviors), they provide a matrix from which to build a view of caring in perioperative practice.
More recently, another researcher identified car- ing activities described by five OR nurses from a Toronto hospital. In this study, which was based on the competency work by Patricia Benner, RN, PhD,I3 the participants related nursing competence, true presence, touching, and reassurance as caring behaviors, with an overall theme that the patient was the center of all care, duties, and preparation in surgery. This study also identified two competencies (ie, protecting, using humor) that Dr Benner had not identified.14
The paucity of research on perioperative nurses’ caring behaviors supported this researcher’s belief that a study was warranted to explore caring practices in perioperative nursing.
SlUDY PURPOS& O W s n O N S
was to answer these research auestions. The purpose of this qualitative, descriptive study
How is caring practiced in perioperative nursing? What behaviors do perioperative nurses identify as caring behaviors? How do perioperative nurses care for unconscious patients?
MEIWODOUWiY The researcher received approval from the insti-
tutional review board of the college in which she was a graduate student. The study was conducted in a metropolitan area in the northeastern United States.
Sample. In qualitative research, the number of interviews conducted in a study is less important than the extent to which the phenomenon is explored in each interview.ls The researcher selected the sample using a convenience, purposive sample design. She met with surgical supervisors from eight hospitals, each of which had at least eight operating rooms. Dur- ing these meetings, the researcher requested the names of perioperative nurses who had at least two years of perioperative experience and who might be willing to participate and see the project to completion and be able to verbalize caring experiences. Additional selec- tion criteria were that potential participants should not have any personal or professional ties to the researcher or have attended a seminar on holistic perioperative practice that the researcher had presented.
Four of the six nurses who responded had diplo- mas in nursing, one had an associate degree in nurs- ing, and one had a baccalaureate in nursing. Two of the six respondents held CNOR certification. The respondents all were female and had two to 26 years of perioperative nursing experience.
Znshumenf. A review of the literature failed to uncover a tool that complemented the purpose of this study. The researcher thus developed a semistruc- tured interview guide, which was composed of 12 open-ended questions that were used to stimulate descriptions of the nurses’ actual experiences of car- ing rather than their conceptualized experiences. The questions evolved from Dr Watson’s 10 carative fac- tors and from information gathered from various studies reported in the literature. Two nursing faculty members with expertise in interviewing and qualita- tive inquiry provided input into the tool development. To determine clarity of the questions and content validity of the instrument, the researcher pilot tested the interview guide with one of the nurses who responded and met the sample criteria but was not part of the final sample. Analysis of the transcribed pilot interview revealed themes that demonstrated caring nursing interventions, which reflected Dr Wat- son’s 10 carative factors. No changes, therefore, were made in the interview guide as a result of the pilot test. Additional research using this interview guide could further validate the instrument.
Interview. The researcher conducted individual
380 AORN JOURNAL

FEBRUARY 1995. VOL 61, NO 2 McNumaro
interviews with five perioperative nurses at sites that were away from the hospital settings and were chosen by the participants. The interview environments were quiet, secluded, and conducive to uninterrupted discus- sion. The researcher asked each participant the 12 ques- tions from the interview guide. Data generated consist- ed of audiotaped interviews and limited field notes the researcher took when clarification, affect, and nonver- bal communication were important to remember.
Data analysis. After each interview, the researcher transcribed the audiotape and the limited field notes and sent a copy of each transcription to each participant for additions, deletions, and correc- tions. The researcher performed content analysis on the transcribed interviews after receiving validation from each participant.
The researcher read each transcript and concur- rently listened to the taped interviews several times to gain a sense of the whole experience. Preliminary analysis involved extracting statements, phrases, and words pertaining to caring behaviors. These were coded by participant letter and interview question number. Responses from the nurses who consented to being cited by name after they read the transcripts were recoded by name.
The researcher formulated categorical meanings from the extracted segments and statements of the nurses’ lived experiences. These meanings were then incorporated into appropriate theme labels that char- acterized the phenomenon of caring. The nurses whose responses demonstrated each theme were counted to visualize the overall pattern of their expe- riences. The researcher was cognizant of her own preconceptions and judgments about caring and attempted to set these aside and concentrate on the participants’ experiences while analyzing the data. After completing the coding procedure, the researcher wrote a description of what was learned about the perioperative caring phenomenon and the caring dimensions of perioperative nursing with con- scious and unconscious patients.
RESULTS All five participants completed their entire inter-
views. One nurse, however, did not answer one yues- tion because of limited experience caring for postop- erative patients.
Within the 189 transcribed pages of interviews, the five nurses consistently identified nursing inter- ventions they perceived as caring. They showed no hesitancy in recalling and describing some of the
caring occasions they had experienced. Practice of caring. The perioperative nurses
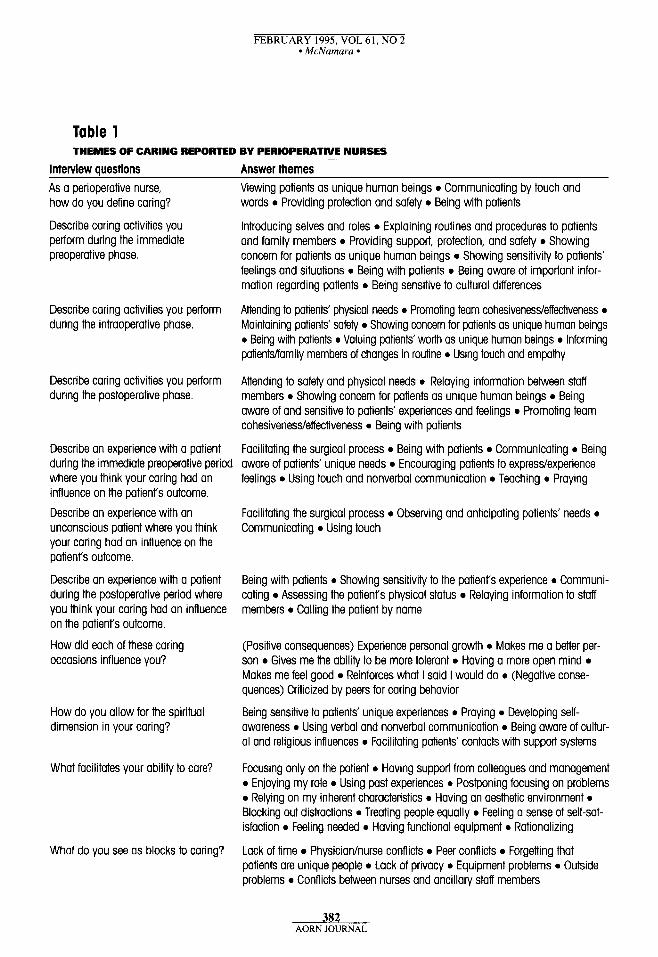
identified a broad range of caring behaviors that were present in more than 20 themes (Table 1). Recurring themes demonstrated how caring is practiced by peri- operative nurses. When these themes were compared, the nurses ’ perceptions demonstrated key elements that focused on patients and the influence of the nurse/patient relationship on patients’ experiences. These elements were
showing concern for patients as unique human beings, communicating, using touch, and being aware of and sensitive to patients’ experi- ences and feelings.
Themes such as communicating by touch and word, being with patients, introducing selves and roles, and showing sensitivity to patients’ feelings and situations, suggested that the nurses placed great value in establishing relationships with patients as part of the healing process. The nurses demonstrated concern with providing supportive spiritual and psychological environments for patients, expressing themes such as
providing support, protection, and safety; praying; and facilitating patients’ contacts with support systems (eg, ministers, rabbis, priests).
The nurses’ responses about the technical areas of patient care were reflected in the theme of physical safety and protective measures. When the nurses were performing technical procedures, their major focus was valuing patients as unique individuals as evidenced by their consistent cognitive assessment processes.
Caring behaviors. The nurses in the study fur- nished a wide range of responses to the question, “What behaviors do you identify as caring ones?” The themes demonstrate the value that all five nurses placed on a holistic view of caring for patients during all three phases of the surgical experience.
Preoperative. The nurses focused on establish- ing trusting nurse/patient relationships in the preoper- ative phase. Communication between the nurses and patients consisted of the nurses introducing them- selves, getting to know patients, explaining to patients and family members what would occur dur- ing surgery, and establishing the rapport and trust necessary for caring relationships. The nurses report- ed using verbal messages, gestures, posture, touch, tone of voice, facial expressions, and listening to communicate as caring behaviors practiced during
38 1 AORN JOURNAL
FEBRUARY 1995, VOL 61, NO 2 MrNamara
Table 1 THEMES OF CARING REPORTED BY PERIOPERATIVE NURSES
~
Interview questions Answer themes As a perioperative nurse, how do you define caring?
Describe caring activities you perform during the immediate preoperative phase.
Describe caring activities you perform during the intraoperative phase.
Describe caring activities you perform during the postoperative phase.
Describe an experience with a patient during the immediate preoperative period where you think your caring had an influence on the patient's outcome,
Describe an experience with an unconscious patient where you think your caring had an influence on the patienrs outcome.
Describe an experience with a patient during the postoperative period where you think your caring had an influence on the patient's outcome.
How did each of these caring occasions influence you?
How do you allow for the spiritual dimension in your caring?
What facilitates your ability to care?
What do you see as blocks to caring?
Viewing patients as unique human beings 0 Communicating by touch and words 0 Providing protection and safety 0 Being with patients
Introducing selves and roles 0 Explaining routines and procedures to patients and family members 0 Providing support, protection, and safety 0 Showing concern for patients as unique human beings 0 Showing sensitivity to patients' feelings and situations 0 Being with patients 0 Being aware of important infor- mation regarding patients 0 Being sensitive to cultural differences
Attending to patients' physical needs 0 Promoting team cohesivenesdeffectiveness 0
Maintaining patients' safety 0 Showing concern for patients as unique human beings 0 Being with patients 0 Valuing patients' worth as unique human beings 0 Informing patienklfamily members of changes in routine 0 Using touch and empathy
Attending to safety and physical needs 0 Relaying information between staff members 0 Showing concern for patients as unique human beings 0 Being aware of and sensitive to patients' experiences and feelings 0 Promoting team cohesivenesdeffectiveness 0 Being with patients
Facilitating the surgical process 0 Being with patients 0 Communicating 0 Being aware of patients' unique needs 0 Encouraging patients to expresdexperience feelings 0 Using touch and nonverbal communication 0 Teaching 0 Praying
Facilitating the surgical process 0 Observing and anticipating patients' needs 0
Communicating 0 Using touch
Being with patients 0 Showing sensitivity to the patient's experience 0 Communi- cating 0 Assessing the patient's physical status Relaying information to staff members 0 Calling the patient by name
(Positive consequences) Experience personal growth 0 Makes me a better per- son 0 Gives me the ability to be more tolerant 0 Having a more open mind 0
Makes me feel good 0 Reinforces what I said I would do 0 (Negative conse- quences) Criticized by peers for caring behavior
Being sensitive to patients' unique experiences 0 Praying 0 Developing self- awareness 0 Using verbal and nonverbal communication 0 Being aware of cultur- al and religious influences 0 Facilitating patients' contacts with support systems
Focusing only on the patient 0 Having support from colleagues and management 0 Enjoying my role 0 Using past experiences 0 Postponing focusing on problems 0 Relying on my inherent characteristics 0 Having an aesthetic environment 0
Blocking out distractions 0 Treating people equally 0 Feeling a sense of self-sat- isfaction 0 Feeling needed 0 Having functional equipment 0 Rationalizing
Lack of time 0 Physicianhurse conflicts 0 Peer conflicts 0 Forgetting that patients are unique people 0 Lack of privacy 0 Equipment problems 0 Outside problems 0 Conflicts between nurses and ancillary staff members
382 AORN JOURNAL
FEBRUARY 1995, VOL 61, NO 2 McNnmuru -
the preoperative phase. They placed importance on understanding the personal meanings of patients’ words, behaviors, and feelings.
All five nurses identified providing support, pro- tecting, and promoting safety for patients as primary caring behaviors in the preoperative phase. These behaviors (eg, providing psychological support through developing caring/trusting relationships, decreasing physical stress and anxiety through com- fort measures) related to the external and internal variables that significantly influence preoperative patients’ well-being. The nurses frequently described patient-specific situational support (eg, being sensi- tive to patients’ and family members’ feelings of fear, anxiety, loss of control, possible lack of knowledge, cultural differences) as caring.
Three nurses perceived physical presence with patients as an important caring behavior. Two nurses identified assessment of important patient informa- tion (eg, consents, laboratory results, past medical problems, histories, physical examinations) as a car- ing behavior. One nurse introduced the caring behav- ior of praying with patients, and another nurse spoke of patient teaching as a specific caring behavior.
Intraoperative. In this phase of the surgical experience, the nurses’ caring behaviors shifted to attending to patients’ physical needs and maintaining safety precautions. All five nurses emphasized actions that ensure the physical and safety needs of patients when they described their perceptions of car- ing behaviors in the intraoperative phase. Examples of these actions included providing warm blankets or patient warming devices to prevent hypothermia associated with cold IV and irrigating fluids and cold room temperatures. The nurses also identified
proper positioning of patients, safe application of electrosurgical unit dispersive pads, use of wet eye pads for protecting patients’ retinas during laser use, correct use of monitoring devices, and conscientious monitoring of blood loss, urinary output, and spongeisharp counts
as caring nursing actions in the intraoperative period. The nurses demonstrated that their caring behav-
iors involved using highly technical machines and participating in technical procedures that required constant assessment and evaluation of the effects on patients. They also perceived promoting team cohe- siveness and effectiveness (ie, listening, anticipating the needs of other team members, observing the
team’s aseptic technique, promoting staff safety through use of personal protective equipment) as being important to patient care. The nurses demon- strated that, as part of their competence in caring, they were involved intricately in maintaining a cohe- sive, supportive, efficient atmosphere in which surgi- cal teams could provide care for patients.
Humanistic caring behaviors also were reflected in the nurses’ intraoperative patient care. Four nurses continued viewing patients as unique human beings and demonstrated this value through intraoperative caring behaviors, such as waiting until children were asleep before removing the children’s clothes or their favorite toys, not restraining patients until they were anesthetized, maintaining the dignity of patients, and allowing patients to retain control when possible. Three nurses identified maintaining physical contact with the anesthetized patient as a caring behavior. Two nurses acknowledged patients’ unique worth as human beings. Other humanistic caring behaviors that were reported included informing patients’ fami- ly members about the progress of surgery and using touch and empathy.
Postoperative. All five nurses reported caring behaviors that attended to patients’ safety and physi- cal needs in the postoperative phase. Perceived caring behaviors during the time when patients emerge from anesthesia and are transported to postanesthesia care units (PACUs) included
keeping patients warm and covered; safely moving patients to transportation carts while maintaining airways, IV lines, Foley catheters, tubes, drains, and dressings; raising side rails on carts; and providing smooth, efficient rides to the PACU.
Four of the nurses addressed continuity of care, which involved the caring behaviors of relaying infor- mation about patients to the PACU nurses. Three of the nurses identified caring behaviors that supported team cohesiveness and effectiveness (eg, maintaining control of the room, ensuring sufficient numbers of staff during patient transfers, turning rooms over quickly to facilitate care of subsequent patients).
Three nurses expressed the value of viewing patients as unique individuals and demonstrated this value by calling patients by their names, knowing the names of children’s special toys, understanding the identity of individuals for whom patients were asking, being aware that patients’ hearing is the first sense to return after anesthesia, and talking with patients. Three nurses emphasized that caring consisted of
384 AORN JOURNAL
FEBRUARY 1995, VOL 61, NO 2 8 McNumaru
being sensitive to patients’ feelings and experiences, and they identified behaviors such as
being aware that nursing procedures could cause pain in patients who are not fully awake, avoiding inappropriate conversation that could hurt patients’ feelings, and being cognizant that patients are aware and possi- bly frightened as they emerge from the effects of anesthesia.
Two nurses identified their physical presence in patients’ environments (eg, being next to patients as they emerge from anesthesia, talking to patients, ori- enting patients) as being a caring behavior.
Spiritual. Question nine on the interview guide addressed the spiritual dimension of patient care. All five nurses viewed spiritual care as being psychoso- cial, individualized, and involving behaviors that com- forted patients or increased their feelings of security. Spiritual caring behaviors addressed patients’ unique experiences as the foundation for understanding, which four of the nurses viewed as a mystery of human life that reflects on patients’ unique ways of coping. These nurses emphasized the importance of maintaining nonjudgmental attitudes about patients’ religious beliefs, listening to patients about their beliefs, and being aware of patients’ cultural and reli- gious views. Three nurses noted that they prayed with or for their patients and believed this action enhanced the human care relationship. Two nurses identified facilitating contact with support systems (eg, minis- ters, rabbis, priests) for patients and their families as being a caring behavior. All five nurses demonstrated the ability to incorporate existential/phenomenologi- cal/spiritual forces into their caring behaviors and con- sequently minister to the wholeness of their patients.
Care of unconscious patients. The nurses report- ed giving the same care to unconscious and conscious patients. They were cognizant of the importance of their role as advocates for patients who cannot support their own care. Two of the nurses gave these exam- ples of caring for unconscious patients:
confronting a surgeon about improper positioning of a patient, assessing improper placement of an endotracheal tube and alerting the anesthesia care provider, and suggesting the use of antiembolism stockings.
The nurses identified instituting protective and safety measures as a major part of nursing care of unconscious surgical patients. One of the nurses explained that caring for unconscious patients involves being aware of what is communicated, because these
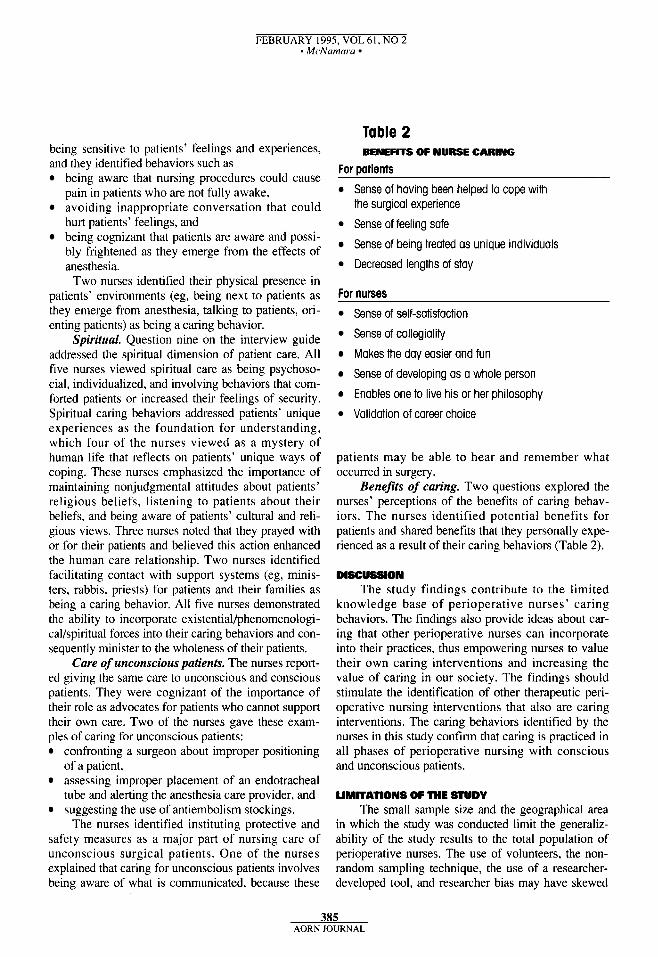
Table 2 BENEFITS OF NURSE CARING
For oatients
Sense of having been helped to cope with the surgical experience
Sense of feeling safe Sense of being treated as unique individuals
Decreased lengths of stay
For nurses Sense of self-satisfaction
Sense of collegiality Makes the day easier and fun
Sense of developing as a whole person
Enables one to live his or her philosophy
Validation of career choice
patients may be able to hear and remember what occurred in surgery.
Benefits of caring. Two questions explored the nurses’ perceptions of the benefits of caring behav- iors. The nurses identified potential benefits for patients and shared benefits that they personally expe- rienced as a result of their caring behaviors (Table 2) .
DISCUSSION The study findings contribute to the limited
knowledge base of perioperative nurses’ caring behaviors. The findings also provide ideas about car- ing that other perioperative nurses can incorporate into their practices, thus empowering nurses to value their own caring interventions and increasing the value of caring in our society. The findings should stimulate the identification of other therapeutic peri- operative nursing interventions that also are caring interventions. The caring behaviors identified by the nurses in this study confirm that caring is practiced in all phases of perioperative nursing with conscious and unconscious patients.
LIMITATIONS OF THE STUDY The small sample size and the geographical area
in which the study was conducted limit the generaliz- ability of the study results to the total population of perioperative nurses. The use of volunteers, the non- random sampling technique, the use of a researcher- developed tool, and researcher bias may have skewed
385 AORN JOURNAL
FEBRUARY 1995, VOL 61, NO 2 8 McNamara 9
the results and limited the generalizability of the study. The participants were all female, thus limiting the gen- eralizability of the findings to one gender.
IMPLICATIONS FOR NURSING The study findings have implications for nursing
education, nursing management, and future nursing research.
Education. The specialty of perioperative nursing is a significant modality for teaching the concept of holistic care to nursing students. Experiences in the preoperative, intraoperative, and postoperative care of surgical patients enrich nursing students’ learning and understanding of the effects of surgery on patients. l6
With the number of patients admitted the morning of surgery, nursing students can practice interviewing techniques, learn to establish transpersonal relation- ships, and perfect health assessment skills needed for effective implementation of the nursing process in the intraoperative phase. Intraoperative experiences assist students in understanding the physical and psychologi- cal trauma that surgery can create. Perioperative nurs- ing exposure provides students valuable experiences that they can generalize to all areas of nursing and helps students develop their awareness of the whole person. This exposure also allows nursing students to experience caring in an environment that has a high potential to dehumanize patients and nurses. Through experiences in the perioperative environment, students can acquire valid knowledge of technical procedures and a caring, holistic orientation to patient care.
Management. The nurses in this study indicated that nurse managers must value caring in periopera- tive practice, and they stated that nurse managers must take leadership roles in supporting caring peri- operative environments. This support may take the form of providing functional equipment, ensuring adequate staffing, rewarding caring behaviors, sup- porting nursing staff members in conflicts with physi- cians, and scheduling cases to allow for realistic turnover times. Nurse managers can provide time for nurses to perform caring interventions and can facili- tate inservice sessions that support and encourage car- ing nursing interventions with patients and peers. Nurse managers can incorporate caring behaviors into performance reviews and can encourage and empow- er nurses to overcome barriers to caring. Nurse man- agers also can encourage nurses to conduct research on caring in their perioperative practices.
Future research. The importance of caring is uni- versal. It is a moral ideal that must be nurtured to grow
within each nurse so that nurses can shape conditions needed to sustain themselves as persons and sustain caring in environments where humanity is threatened.17
This study needs to be repeated using a larger sample and incorporating perioperative nurses of both genders and from several geographic areas. Other recommendations for future research include
comparing perceptions of caring behaviors of peri- operative nurses with varied educational prepara- tion, comparing perceptions of caring behaviors of peri- operative nurses with differing amounts of work experience, cornparing perioperative nurses’ perceptions of car- ing behaviors with the perceptions of their patients, studying the crucial behaviors of all carative factors, identifying why nurses’ caring behaviors are not supported by peers or managers, comparing perceptions of caring behaviors prac- ticed by nurses in religious and secular hospitals, and examining nursing educators’ experiences in peri- operative nursing and determining whether they value perioperative experiences for students and whether they perceive surgical environments as car- ing.
The findings of this study, although limited in scope, validate Dr Watson’s 10 carative factors and present a view of the caring dimensions of periopera- tive nursing. The findings substantiate that caring exists in perioperative nursing practice and that peri- operative nurses can identify caring behaviors. Fur- ther research on this subject can open the closed OR
doors and enhance continuity of perioperative care by empowering nurses and patients. A
Sharon A. McNamara, RN, MS, CNOR, is a perioperative clinical nurse specialist, Millard Fillmore Health System, Buffalo.
The author conducted this research as a master’s degree candidate at D’ Youville College, Buffalo. The author acknowledges partial finding for this study through a research grant fiom the AORN Foundation, Denver. The author also acknowledges the contributions of Christine Esperson, RN. CNOR, CRNFA; Michele M. Mas, RN, BS; Joan M. Syhlowy, RN, ADN, CNOR; Paula M. Williams, RN, CNOR; and the other two study participants who chose to remain anonymous.
387 AORN JOURNAL
FEBRUARY 1995, VOL 61, NO 2 9 Mi,Nurnuru
NOTES 1. C A Smith, ‘Solving the mys-
tery of perioperative nursing: An OR nurse week program,” AORN Jour- nal 56 (November 1992) 847-856.
2. J Watson, Nursing: Human Science and Human Care: A Theory ofNursing (New York: National League for Nursing, 1988).
3. Ihid. 4. P Bums, “Elements of spiritu-
ality and Watson’s theory of transpersonal caring: Expansion of focus,” in Anthology on Caring, ed P L Chinn (New York: National League for Nursing Press, 1991) 141- 153; Y Chipman, “Caring: Its mean- ing and place in the practice of nurs- ing,” Journal of Nursing Education 30 (April 1991) 171-175; C M Lem- mer, “Parental perceptions of caring following perinatal bereavement,” Western Journal of Nursing Research 13 (August 1991) 475-493; B Lyne, P Waller, “The Denver Nursing Project in Human Caring: A model for AIDS nursing care and professional education,” Family and Community Health 13 (February 1990) 78-84; L S Martin, “Using Watson’s theory to explore the dimensions of adult polycystic kid- ney disease,” ANNA Journal 18 (October 1991) 493-499; C Schroed- er, M K Maeve, “Nursing care part- nerships at the Denver Nursing Pro- ject in Human Caring: An application and extension of caring theory in practice,” Advances in Nursing Sci- ence IS (December 1992) 25-38; N Engel, “Confirmation and validation: The caring that is professional nurs- ing,” IMAGE: Journal $Nursing Scholarship 12 (March 1980) 53-56; S A Gadow, “Nurse and patient: The caring relationship,” in Caring, Cur- ing, Coping: Nurse, Physician, and Patient Relationships. ed A H Bish- op, J R Scudder, Jr (Tuscaloosa, Ala: University of Alabama Press, 1985) 3 1-43; D A Gaut, “Development of a theoretically adequate description of caring,” Western Journal of Nursing Research 5 (Fall 1983) 3 13-324; D A Gaut, “Evaluating caring competen- cies in nursing practice,” Topics in
Clinical Nursing 8 (July 1986) 77- 83; M M Leininger, “Leininger’s the- ory of nursing: Cultural care diversity and universality,” Nursing Science Quarterly 1 (November 1988) 152- 160; J Mantle, “Caring, the essence of nursing,” Canadian Operating Room Nursing Journal 6 (June 1988) 14-19; J M Morse et al, “Compara- tive analysis of conceptualizations and theories of caring,” IMAGE: Jaurnal of Nursing Scholarship 23 (Summer 1991) 119-126; M Rawns- ley, “Of human bonding: The context of nursing as caring,” Advances in Nursing Science 13 (September 1990) 41-48; Z R Wolf, “The caring concept and nurse-identified caring behaviors,” Topics in Clinical Nurs- ing 8 (July 1986) 84-93.
5 . A Boykin, S Schoenhofer, “Caring in nursing: Analysis of extant theory,” Nursing Science Quarterly 3 (Winter 1990) 149-155; D Forsyth et al, “Can caring behavior be taught?” Nursing Outlook 37 (July/August 1989) 164-166; R J Kurtz, J Wang, “The caring ethic: More than kindness, the core of nurs- ing science,” Nursing Forum 26 no 1
6. Leininger, “Leininger’s theory (1991)4-8.
of nursing: Cultural care diversity and universality,” 152- 160; A McBride, “Knowledge about care and caring: State of the art and future development,” Reflections 15 no 2 (1989) 5-7; J Watson, Nursing: The Philosophy and Science ($Caring (Boston: Little, Brown and Co, 1979); J Watson, Nursing: Human Science and Human Care (Norwalk, Conn: Appleton-Century-Crofts, 1985); Watson, Nursing: Human Sci- ence and Human Care: A Theory of Nursing.
cy-based testing,” Nursing Outlook 30 (May 1982) 303-309; P Benner, From Novice to Expert: Excellence and Power in Clinical Nursing Prac- tice (Menlo Park, Ca: Addison-Wes- ley Publishing Co, Inc, 1984); P Ben- ner, C Tanner, C Chesla, “From beginner to expert: Gaining a differ- entiated clinical world in critical care
7. P Benner, ‘‘Issues in competen-
nursing,” Advances in Nursing Sci- ence 14 (March 1992) 13-28.
8. D Forrest, “The experience of caring,” Journal of Advanced Nurs- ing 14 (October 1989) 815-823.
9. D L Kahn, R H Steeves, “Car- ing and practice: Construction of the nurse’s world,” Scholui-ly Inquiry for
221. 10. L D Warren, “Review and syn-
thesis of nine nursing studies on care and caring,” Journal cfthe New York State Nurses Association 19 (Decem- ber 1988) 20-26.
1 1. S N Cronin, B Harrison, “Importance of nurse caring behav- iors as perceived by patients after myocardial infarction,” Heart & Lung 17 (July 1988) 374-380; E C Parsons, C C Kee, D P Gray, “Peri- operative nurse caring behaviors: Perceptions of surgical patients,” AORN Journal 57 (May 1993) 1106- 1 1 14.
12. R L Hanson, A H Nelson, “OR personnel functions: Testing of observabihty,” AORN Journal 42 (September 1985) 376-387.
13. C Lenox, “Identification of Caring Activities as Described by Operating Room Nurses” (Master’s thesis, D’Youville College, Buffalo, NY, 1990).
14. Benner, From Novice to Expert: Excellence and Power in Clinical Nursing Practice.
15. N Drew, “The interviewer’s experience as data in phenomenolog- ical research,” Western Journal of Nursing Research 1 1 (August 1989) 43 1-439.
16. Hanson, Nelson, “OR person- nel functions: Testing of observabili- ty,” 376-387; J A Lierman, “Teach- ing perioperative nursing: A pro- posed design for a curriculum,” AORN Journal 45 (May 1987) 1180- 1189; A Reynolds, M H Sizemore, “Perioperative clinical experiences: Opportunities for baccalaureate nurs- ing students,” AORN Journal 43 (April 1986) 901-906.
17. Watson, Nursing: Human Sci- ence and Human Caw: A Theory o f Nursing, 30.
388 AORN JOURNAL





























