Embed Size (px)
Citation preview

CONTINUING EDUCATION
Perioperative Nursing Careof the Patient UndergoingBariatric Revision Surgery
JANICE A. NEIL, PhD, RN 3.5www.aorn.org/CE
Continuing Education Contact Hoursindicates that continuing education contact hours are
available for this activity. Earn the contact hours by reading
this article, reviewing the purpose/goal and objectives, and
completing the online Examination and Learner Evaluation
at http://www.aorn.org/CE. A score of 70% correct on the
examination is required for credit. Participants receive feed-
back on incorrect answers. Each applicant who successfully
completes this program can immediately print a certificate of
completion.
Event: #13505
Session: #0001
Fee: Members $21, Nonmembers $42
The contact hours for this article expire February 29, 2016.
Purpose/GoalThe purpose of this activity is to enable the learner to more
effectively care for patients undergoing bariatric revision
surgery.
Objectives
1. Describe types of bariatric surgery.
2. Explain why people undergo bariatric revision surgery.
3. Discuss complications that patients undergoing bariatric
revision surgery may experience.
4. Identify safety precautions that perioperative nurses
should institute for patients undergoing bariatric revision
surgery.
210 j AORN Journal � February 2013 Vol 97 No 2
AccreditationAORN is accredited as a provider of continuing nursing
education by the American Nurses Credentialing Center’s
Commission on Accreditation.
ApprovalsThis program meets criteria for CNOR and CRNFA recertifi-
cation, as well as other continuing education requirements.
AORN is provider-approved by the California Board of
Registered Nursing, Provider Number CEP 13019. Check with
your state board of nursing for acceptance of this activity for
relicensure.
Conflict of Interest DisclosuresDr Neil has no declared affiliation that could be perceived as
posing a potential conflict of interest in the publication of this
article.
The behavioral objectives for this program were created
by Rebecca Holm, MSN, RN, CNOR, clinical editor, with
consultation from Susan Bakewell, MS, RN-BC, director,
Perioperative Education. Ms Holm and Ms Bakewell have
no declared affiliations that could be perceived as posing
potential conflicts of interest in the publication of this article.
Sponsorship or Commercial SupportNo sponsorship or commercial support was received for this
article.
DisclaimerAORN recognizes these activities as continuing education for
registered nurses. This recognition does not imply that AORN
or the American Nurses Credentialing Center approves or en-
dorses products mentioned in the activity.
http://dx.doi.org/10.1016/j.aorn.2012.11.013
� AORN, Inc, 2013

I
Perioperative Nu
rsing Careof the Patient UndergoingBariatric Revision SurgeryJANICE A. NEIL, PhD, RN 3.5www.aorn.org/CE
ABSTRACT
Obesity has become a major health concern in the United States. The number of
patients seeking bariatric surgery has grown exponentially in recent years because of
the proven success of weight-loss surgery, greater public acceptance, and the
increasing number of insurers who will pay for these surgeries. Patients may seek
bariatric revision procedures if the primary procedure does not achieve the desired
results, if he or she gains back the weight lost after the primary procedure, if the
comorbid conditions associated with obesity were not resolved, or if severe adverse
effects and complications have occurred as a result of the primary bariatric proce-
dure. Perioperative nurses must be knowledgeable about how to care for bariatric
surgery patients with skill and compassion. AORN J 97 (February 2013) 211-226. �AORN, Inc, 2013. http://dx.doi.org/10.1016/j.aorn.2012.11.013
Key words: obesity, bariatric surgery, restriction surgery, malabsorptive surgery,
bariatric revision surgery.
n the United States, obesity is the second leading
cause of preventable death related to the co-
morbidities associated with it.1 Lifestyle changes
and dieting rarely produce sustained weight loss
and often are ineffective in achieving long-term
improvement in comorbidities.2 Bariatric surgery
has become an effective method for sustained
weight loss and improvement of obesity-related
comorbid conditions.1,3,4
Patients who have undergone bariatric surgery
may have problems that need to be corrected as a
result of the procedure itself or, more commonly,
they either did not lose the desired amount of weight
or they regained the weight lost from the primary
bariatric procedure. Perioperative nurses must
learn how to care for a potential new population
http://dx.doi.org/10.1016/j.aorn.2012.11.013
� AORN, Inc, 2013
of patientsdthose seeking bariatric revision sur-
gery. This article describes the types of revision
surgery available and the perioperative nursing im-
plications involved in caring for patients undergoing
bariatric surgery. Table 1 defines some common
terms related to bariatric surgery.
BACKGROUND
It is estimated that 32.2% of adult men and 35.5%
of adult women are obese.5 Patients who strongly
desire to lose weight and whose body mass index
(BMI) exceeds 40 kg/m2 are potential candidates for
bariatric surgery. Patients who are severely obese
(ie, with a BMI between 35 kg/m2 and 39 kg/m2)
also can be considered for bariatric surgery if they
have comorbid conditions, such as hypertension,
February 2013 Vol 97 No 2 � AORN Journal j 211

TABLE 1. Glossary of Terms1,2
n Bariatric surgery: A surgical procedure performed forthe purpose of producing weight loss.
n Biliopancreatic limb: The segment of small bowelconnecting the bile duct to the distal end of the Rouxlimb. The segment follows the Roux limb and is thebile-carrying limb.
n Common channel: The segment of small bowel wherethe biliopancreatic limb and the Roux limb becomeone and continue to the cecum. Complex proteins,fats, and carbohydrates are digested in the commonchannel.
n Ergonomics: The science of fitting the demands ofwork to the anatomical, physiological, and psycho-logical capabilities of the worker to enhance efficiencyand well-being.
n Malabsorption: Incomplete digestion or absorption offood intake.
n Morbid obesity: Having a body mass index greaterthan 40 kg/m2.
n Pouch: A surgically created portion of the stomachthat serves as a reservoir for food immediately afterfood exits the esophagus.
n Restrictive: Decreasing or limiting the amount of foodintake.
n Roux limb: The segment of small bowel where foodexits the stomach and enters the bowel. The Rouxlimb starts where food enters the bowel and endswhere the biliopancreatic limb joins to form thecommon channel.
n Staple line: A row of staples placed in the bowel orstomach by a surgical stapling device. Staples can beused to create an anastomosis, create a partition, orsecure the end of a segment of bowel when a sideanastomosis is performed.
1. AORN Bariatric surgery guidelines. In: Perioperative Standards andRecommended Practices. Denver, CO: AORN, Inc; 2010:490.2. Recommended practices for positioning the patient in the peri-operative practice setting. In: Perioperative Standards and Recom-mended Practices. Denver, CO: AORN, Inc; 2012:422.
February 2013 Vol 97 No 2 NEIL
sleep apnea, diabetes mellitus, or musculoskeletal
issues, that interfere with employment and ambula-
tion.6 In addition, people who are obese with lower
BMIs are now seeking weight-loss procedures to
achieve sustained weight loss and prevent comor-
bidities and health-related quality of life issues.7
The number of bariatric procedures performed in
the United States during the past 20 years has
212 j AORN Journal
increased 20% annually.3 Reasons for this increase
include the use of laparoscopic techniques, the
proven success of weight-loss surgery, and in-
creased public acceptance.2 In 1998, 12,775 bari-
atric procedures were performed in the United
States.8 Currently, more than 200,000 procedures
are performed annually in the United States.8 Al-
though this represents only 1% of the eligible,
severely obese population, it is estimated that a
growing number of insurers will have paid for bar-
iatric surgery in 2012, allowing many more people,
even some teens, to benefit from the health advan-
tages of weight-loss surgery.9 With the increased
number of procedures being performed each year,
some patients will seek revision surgery if the
primary procedure did not achieve the desired
results.10,11
All types of bariatric surgery involve restriction
to reduce the quantity of food that can be ingested.
The types of procedures that are only restrictive in
nature include vertical-banded gastroplasty, lapa-
roscopic adjustable banding, and vertical sleeve
gastrectomy. Some types of procedures have both
restrictive and malabsorptive properties (eg, Roux-
en-Y gastric bypass, biliopancreatic diversion with
duodenal switch).2 Malabsorptive-only procedures
that bypass a large portion of the small intestine and
intentionally cause malabsorption by decreasing
absorption of protein and nutrients (eg, jejunoileal
bypass) can produce significant adverse effects, so
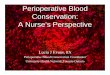
they are no longer performed. Figure 1 illustrates the
four most prevalent procedures being performed
today.
CONSIDERATIONS FOR BARIATRICREVISION SURGERY
Although most people are successful in losing large
amounts of weight after bariatric surgery, some
people will need revisions to their primary proce-
dures. People seeking revision surgery may have
inadequate weight loss (ie, they did not lose the
desired amount of weight) or may regain weight
they lost after the primary procedure. Revision
surgery also can treat severe adverse effects and

Figure 1. Illustration of different bariatric procedures: adjustable gastric band (A); gastric bypass (B); gastricsleeve (C); and duodenal switch (D). The dark pink color in the illustration indicates functioning gastrointestinal(GI) tract. The orange-brown color indicates bypassed GI tissues; the green-gray color indicates bypassed andisolated GI tissues (ie, portion of the stomach).
BARIATRIC REVISION SURGERY www.aornjournal.org
complications from the primary bariatric proce-
dure, such as gastrogastric fistulas and pouch dili-
tation.8 Some people may seek revision surgery
because the comorbidities associated with obesity
were not resolved as a result of poor weight loss
or weight regain.
Revision surgery should not be undertaken lightly.
The decision to undergo revision surgery should be
made based on the type of procedure performed in-
itially, the risks and possible benefits of the proposed
procedure, and the person’s condition (eg, comor-
bidities). Generally, a revision procedure presents a
higher risk of postoperative complications than the
first weight-loss procedure because of manipulation
of previously manipulated tissue.8 This can result in
higher mortality and a greater number of adverse
outcomes.8,12
The Longitudinal Assessment of Bariatric Sur-
gery Consortium, a large multisite institutional
group, maintains a database with a wide demo-
graphic profile of patients (eg, patients of both
genders, varying ages and races, multiple co-
morbid conditions) who have had bariatric pro-
cedures. From a study of 255 patients who have
undergone revision surgery, the consortium deter-
mined that adverse outcomes were more likely to
occur with a revision procedure than with a primary
procedure.8 Patients especially at risk include those
with a history of deep vein thrombosis or a preop-
erative diagnosis of sleep apnea.3
Often, the primary reason for bariatric surgery
is to help resolve comorbidities, such as diabetes
mellitus, hypertension, joint pain, and high choles-
terol.2,13 If weight is regained, comorbidities can
return. The solution may be to convert the failed
bariatric procedure to a more metabolically active
type of procedure (eg, one with greater malabsorp-
tive properties). All factors should be examined,
therefore, when revision surgery is being consid-
ered. The risks of revision surgery are outlined
in Table 2.
Research indicates that about 10% of patients
who have bariatric weight-loss procedures experi-
ence unsatisfactory weight loss or will regain some
or all of the weight they lost.14 Frank and Crookes13
estimate that weight regain may be as high as 20%.
AORN Journal j 213

TABLE 2. Risks of Revision Surgery1
n The procedures usually take longerdup to twice aslong as the primary procedure because of the tech-nical difficulty; therefore, patients will require anes-thesia longer.
n Laparoscopic approaches may be more difficult; openincisions may be required because of previous boweland stomach manipulation.
n Generally, there is greater blood loss than with primaryprocedures.2
n Anastomotic leaks and infections occur morefrequently than after the primary procedure.2
n The leak rate increase may be caused by changesin blood flow to the stomach.
n The risk of injury to the intestines is higher becauseof previous manipulation, which may lead to leaksor infections.
n The effect of revision surgery is not as clear as theoriginal procedure. Prediction of the weight loss thatresults from a revision procedure is less accurate. Itis not uncommon to see less weight loss becausemetabolic adaptations that occurred after the originalprocedure may make it more difficult for the patient tolose weight after revision. The patient may be “meta-bolically obstinate,” meaning that his or her metabo-lism may be slower, which may not facilitate quickweight loss.
n Adverse surgical outcomes and medical complicationssuch as deep vein thrombosis, pulmonary embolism,and the need for reintubation are 2.3 times more likelyto occur.2
1. Colquitt JL, Picot J, Loveman E, Clegg AJ. Surgery for obesity.Cochrane Database Syst Rev. 2009;15(2):CD003641.2. Inabnet WB III, Belle SH, Bessler M, et al. Comparison of 30-dayoutcomes after non-LapBand primary and revisional bariatric surgicalprocedures from the Longitudinal Assessment of Bariatric Surgerystudy. Surg Obes Relat Dis. 2010;6(1):22-30.
February 2013 Vol 97 No 2 NEIL
This inadequate weight loss or weight regain may
be attributed to frequent snacking, high-calorie food
intake, or lack of exercise. Anatomical problems
(eg, a stretched pouch, separated sutures) also can
contribute to weight regain.2
Sometimes, when patients realize what and how
often they are eating, they can get back on track
without surgery. For some, the problem may simply
be noncompliance. The nature of compliance is
complex. Good eating habits are often not part of
normal life for a person who is obese. The person
214 j AORN Journal
may not be able to change his or her eating habits
permanently despite the assistance of a smaller gas-
tric capability.15 The type of surgical procedure
chosen may not have been suitable for the patient
and, as a result, did not work for that patient.
Some of the reasons patients do not lose ade-
quate amounts of weight or regain weight are
the following:
n The procedure performed did not address the
metabolic or mechanical needs of the person.
Weight-loss success involves more than just
eating a nutritional diet, it involves the person’s
metabolic rate. Correcting metabolic failure
involves converting the person’s bariatric sur-
gery type to a more metabolically active type.15
n The anatomical changes of the surgery were
not maintained; thus, mechanical or metabolic
failure occurs. Mechanical failures result when
the anatomical changes made during the primary
procedure are not maintained. These include a
stretched gastric pouch, increased outlet size at
the gastric pouch, formation of a gastrogastric
fistula between the gastric pouch and bypassed
stomach, increased absorptive abilities beyond
expectations, or decreased restriction as a result
of band slippage.16
n The person was unable to adapt to the lifestyle
required for the type of bariatric surgery. This
includes making proper food choices and ex-
ercising.14
n The person was not properly educated on how
to achieve permanent weight loss. When weight
is regained, it is very difficult to lose again.
n Long-term care and support were not provided
or sought to keep the person on track.16
Candidates for revision surgery include those
who have a BMI greater than 35 kg/m2 and those
who failed to achieve 50% of their weight-loss goal
by 18 months after surgery.10 The threshold crite-
rion for revision surgery is weight gain of more
than 10 kg (22 lb).17 However, insurance coverage
for revision surgery is often denied in the United
States for patients who have weight regain without

BARIATRIC REVISION SURGERY www.aornjournal.org
clear-cut problems, such as a mechanical failure.13
Generally, to qualify for initial bariatric surgery
coverage from most insurance companies, the
person must have a BMI of 35 kg/m2 to 39 kg/m2
with two comorbidities or a BMI greater than 40
kg/m2 without comorbidities. Revision surgery
criteria vary according to the problem and are
more stringent.
SPECIFIC PROCEDURES AND REVISIONS
Gastric restrictive procedures include
n Roux-en-Y gastric bypass,
n vertical-banded gastroplasty,
n laparoscopic adjustable banding,
n biliopancreatic diversion with duodenal
switch, and
n vertical sleeve gastrectomy.
These procedures result in a significant reduction
in the stomach size, ensuring early satiety (ie,
satisfied appetite). Patients feel full with a small
quantity of food. Advantages of these procedures
include not only weight loss but also improve-
ment of comorbidities, such as type 2 diabetes
mellitus, hypertension, gastroesophageal reflux
disease, sleep apnea, stress incontinence, and
low back pain.1,15,18 However, there are possible
complications related to each of these proce-
dures. Potential complications and revisions for
each type of bariatric procedure are shown in
Table 3.
Roux-en-Y Gastric Bypass
The Roux-en-Y gastric bypass is the most common
bariatric procedure in the United States,1 comprising
65% of the bariatric surgeries performed.10,13,18 It
has restrictive and malabsorptive properties. During
the procedure, the surgeon creates a small gastric
pouch that holds 15 mL to 30 mL; this restricts food
intake. The gastrojejunostomy provides a mild mal-
absorptive component that also results in weight
loss. The small gastric pouch is joined to the limb
of the jejunum (ie, Roux limb) that is then joined
further down in the jejunum coming from the
duodenum (ie, pancreaticobiliary limb). This forms
a “Y” configuration.19
Bessler et al10 reported an average gastric bypass
failure rate of 15% (ranging from 5% to 40%)
mostly related to weight regain. Mechanical rea-
sons for gastric bypass failure that lead to revision
procedures are gastrogastric fistula, pouch dilata-
tion, anastomotic dilatation, and shortened ali-
mentary segment (Figure 2).
A gastrogastric fistula is a rare complication.20 It
is an abnormal communication between the gastric
pouch and the gastric remnant. The stomach that was
divided during the primary procedure reconnects
via a fistula so the stomach pouch is reconnected
to the bypassed stomach. This often occurs when the
pouch develops a non-acute local inflammation at
the staple line, resulting in a leak that partially re-
verses the gastric bypass. Food can now pass from
the pouch to the bypassed stomach, which is almost
like a reversal of the bypass, and weight regain can
occur.
Although some gastrogastric fistulas can be
treated conservatively, a revision procedure is re-
quired if the person experiences symptoms such
as abdominal pain. Diagnosis of this condition is
made by radiologic study, computed tomography,
and upper endoscopy. Revision surgery involves
closing the fistula to restore the bypassed anat-
omy.20 Repair of this phenomenon can be techni-
cally challenging and can be associated with high
morbidity and mortality. In some situations, endo-
scopic repair can be performed using hemoclips,
fibrin glue, or argon plasma coagulation.21 Fistula
size is often a factor in deciding whether to perform
the procedure endoscopically.
Pouch dilatation occurs when the stomach
pouch stretches and enlarges, thus stretching the
intestine as well. This also can occur at the site
of the anastomosis. Both situations allow for larger
consumption of food. During revision surgery,
the surgeon retrims the pouch to make it smaller.
Transoral endoscopic suturing and plication are
less invasive endoluminal therapies for pouch en-
largement issues.
AORN Journal j 215

TABLE 3. Possible Complications and Revisions for Each Type of Bariatric Procedure
Procedure Complication Potential revision
Roux-en-Y gastric bypass n Gastrogastric fistula: abnormal communi-cation between the gastric pouch and thegastric remnant that allows for largerconsumption of food and, ultimately,weight regain
n Perform revision surgery that involvesclosing the fistula to restore the bypassedanatomy
n Pouch and/or anastomotic dilatation: astretched gastric pouch or an increasein outlet size at the gastric pouch
n Retrim the pouch
n Poor metabolism that leads to weightregain
n Perform a more metabolically activeprocedure (eg, duodenal switch)
Vertical-banded gastroplasty n Band erosionn Stenosis
n Revise to Roux-en-Y or vertical sleevegastrectomy
Laparoscopic adjustable band n Tubing and port issues: twisting, flipping, orleaking of port so that no restriction occurs
n Locate the issue and replace the port
n Band leakage (very rare): leakage at bandbladders with no restriction
n Replace the band
n Poor weight loss/weight regain: restrictionthat is not producing desired weight loss
n Remove the band and convert to aRoux-en-Y gastric bypass, duodenalswitch, or vertical sleeve gastrectomy
Biliopancreatic diversion withduodenal switch
n Inadequate weight loss (rare complication) n Further reduce the stomach size
Vertical sleeve gastrectomy n Sleeve dilatation: the stomach pouch hasstretched or dilated, may be in an “hour-glass” shape
n Resize the sleeve or convert to aRoux-en-Y gastric bypass
n Weight regain, poor weight loss n Convert to a Roux-en-Y gastric bypass orduodenal switch1,2
1. Langer FB, Shakeri-Leidenm€uhler S, Bohdjalian A, et al. Strategies for weight regain after sleeve gastrectomy. Surg Laparosc Endosc Percutan Tech.2010;20(3):159-161.2. Keidar A, Appelbaum L, Schweiger C, Elazary R, Baltasar A. Dilated upper sleeve can be associated with severe postoperative gastroesophagealdysmotility and reflux. Obes Surg. 2010;90(2):140-147.
February 2013 Vol 97 No 2 NEIL
Injecting sodium morrhuate around the dilated
stoma is also a method to reduce stoma size in
response to anastomotic dilatation.10 Endoscopic
fixation is an approach to remedy this problem
aimed at restoring the smaller pouch. Performing
a vertical sleeve gastrectomy-type procedure is
another option, especially if the gastric bypass is
complicated by nutrient malabsorptive issues, such
as osteoporosis and anemia.
Adjustable banding may be another option for
revising a gastric bypass. A band is placed around
216 j AORN Journal
the proximal pouch and adjusted six weeks later
and as necessary. This is an attractive approach
because it requires no anastomosis, and no change
in absorption occurs. Whereas some revision pro-
cedures are technically complex, challenging, and
associated with a variety of postoperative compli-
cations, an adjustable band is an easier approach
and may be the solution to correct weight regain.10
A shortened alimentary segment, although a rare
complication, also can occur. Normally, the segment
that comes from the gastric pouch is approximately

Figure 2. Anatomical causes of weight regain ingastric bypass: dilated anastomosis or dilated pouch;gastrogastric fistula; or short alimentary segment.The dark pink color in the illustration indicatesfunctioning gastrointestinal (GI) tract. The orange-brown color indicates bypassed GI tissues.
BARIATRIC REVISION SURGERY www.aornjournal.org
100 cm to 150 cm in length. The length is variable
and can be affected by anesthetics. Preoperative
medications and anesthetics can cause the portion
of the small bowel used for the segment to contract.
The alimentary segment may have shortened be-
cause it contracted or adhesions are present (W.
Pories; past president, American Society for Bari-
atric Surgery and professor of surgery, East Caro-
lina University; oral communication; April 12,
2012). The revision surgery to correct this involves
lengthening the limb by moving the biliopancreatic
limb down further in the jejunum.22 However, pa-
tients must be watched more closely for protein
malnutrition with a more distal Roux-en-Y.23
In some situations of weight regain, a more
metabolically active approach can be taken by
changing to a duodenal switch. This approach
addresses inadequate weight loss by correcting
metabolic failure and maladaptive eating because
of the increased malabsorptive properties of this
procedure. There is less absorption of food, so
weight can be lost. However, a potential concern
is proper stomach functioning after surgery. The
bypassed stomach is brought back to use, but in
some situations, the nerves were cut during the
primary procedure. In time, the nerves may re-
generate and become active again. In some cases,
excessive scar tissue makes it unsafe to reconnect
the gastric pouch to the bypassed stomach. Revi-
sion to a biliopancreatic diversion is technically
complex and, as a result of significant malabsorp-
tion, protein malnutrition and vitamin and iron
deficiencies can occur.
Vertical-Banded Gastroplasty
Vertical banding involves partitioning and stapling
the fundus of the stomach. Although this was a
common bariatric procedure in the past, adjustable
gastric banding has replaced it.24 Band erosion
and stenosis are late complications. Optional revi-
sions include revising to a Roux-en-Y or vertical
sleeve gastrectomy.15
Laparoscopic Adjustable Banding
The laparoscopic adjustable band was introduced
in 1993. This procedure is restrictive in nature. A
silicone band with an inflatable inner collar is placed
around the upper stomach. The band is connected to
a port that is placed in the soft tissue of the abdomen.
The inner diameter of the band can be adjusted
later using bimanual palpation of the abdominal
port and injecting saline into the port to create more
restriction.1
Data suggest that patients lose an average of more
than 50% of excess weight.1 Excess weight is
defined as the starting weight minus the goal weight.
Currently, about 25% of bariatric surgery proce-
dures involve gastric banding.4,13,25 This procedure
has a very good perioperative safety record, very
low mortality, and a beneficial effect on comorbid-
ities related to the weight loss, and it is minimally
invasive and reversible. In 2011, the US Food and
AORN Journal j 217

February 2013 Vol 97 No 2 NEIL
Drug Administration released a statement that
expanded the use of the laparoscopic adjustable
band system to include people with BMIs in the
30 kg/m2 to 34 kg/m2 range, especially for those
who have at least one comorbidity.26
Weight regain is the usual reason for revision.
Because it does not make anatomical changes, the
laparoscopic adjustable band is considered a device
that influences eating behaviors by acting as a tool
to decrease food intake. However, patients may
have eating behaviors incompatible with the band.
These include sweet eating (ie, eating foods high in
sugar) and grazing (eg, eating smaller quantities of
food at frequent intervals).15 Tubing and port issues
(eg, tube disconnection, port leakage) can result in
poor weight loss or weight regain. A patient with
a laparoscopic adjustable band who had adequate
restriction may lose that restriction if the band de-
velops a leak, which can happen suddenly or over
time. If the band leaks, the band may not be able to
be filled properly and will not provide restriction.
People with this issue often feel a loss of restriction
or a change in the restriction. This may be accom-
panied by weight regain or inability to lose more
weight because they can eat larger volumes of food.4
There are four likely sites for band leakage:
n The band balloon around the stomach may leak
as a result of factory defects causing a weak
point or a needle puncture occurring uninten-
tionally during surgery (a very rare occurrence,
especially with the newer bands).
n The tube connection may leak as a result of
a break or fracture of the tube next to the metal
connection where the tubing connects to the
port. This can happen as a result of physical
movement over time.
n The body of the tube may leak; this is usually
caused by unintentional needle punctures when
the band is filled. There is always a risk of punc-
turing the tube with an adjustment even in the
best of circumstances, including when fluoros-
copy is used for port visualization. The band and
the port can both be visualized by fluoroscopy.
218 j AORN Journal
n The port membrane can leak if the port has been
accessed multiple times or if a Huber needle
was not used for the fill. The silicone part of the
port can be damaged if any other type of needle
is used.27
If any of these situations occur, the part of the band
system that is leaking can be replaced or the entire
band can be replaced.
The laparoscopic adjustable band is removable
and can be converted to a Roux-en-Y gastric bypass
or duodenal switch in patients for whom the band
did not have the desired effects. The Roux-en-Y
gastric bypass is the most commonly performed
revision for poor weight loss. Topart et al found
that nearly 40% of patients with laparoscopic bands
had a five-year failure rate.28 Some people may not
have a high enough metabolism needed to lose
weight with the band or have the proper eating
habits to ensure success. Metabolically, more active
types of surgery instead of restrictive types of sur-
gery may produce the desired weight-loss goals in
these patients. However, converting to a gastric
bypass may put the person at risk for an anasto-
motic leak. The vertical sleeve gastrectomy and
the duodenal switch with ileal transposition may
also be choices for revision because of their
metabolic properties that cause weight loss in
addition to restrictive properties. Figure 3 shows
the possible revision procedures for a laparoscopic
band. Sometimes the band is removed in one
procedure, and after healing occurs, the new
procedure is performed.
Biliopancreatic Diversion With DuodenalSwitch
The biliopancreatic diversion with duodenal switch
has significant malabsorptive and restrictive prop-
erties. The patient is able to eat normally while
developing a metabolism similar to that of a lean
person. The surgery has three components:
n removing a large portion of the stomach to
promote smaller meal sizes (ie, vertical gastric
sleeve),

Figure 3. Options to revise a failed laparoscopicband: convert the band to a gastric sleeve or con-vert the band to a gastric bypass. The dark pink colorin the illustration indicates functioning gastrointes-tinal (GI) tract. The orange-brown color indicatesbypassed GI tissues; the green-gray color indicatesbypassed and isolated GI tissues (ie, portion of thestomach).
BARIATRIC REVISION SURGERY www.aornjournal.org
n re-routing the food away from the small intes-
tine to partially prevent absorption of food, and
n re-routing bile and other digestive juices, which
impairs digestion.14
The procedure begins with a vertical sleeve gas-
trectomy that reduces the patient’s stomach size to
90 mL to 120 mL.14,19 This leaves a vertical tube
with the pylorus intact. The remainder of the stom-
ach is removed. Beyond the pylorus, the duodenal
segment is divided and the proximal end is anasto-
mosed to a section of ileum to become the “alimen-
tary channel.” This segment is then anastomosed to
the segment coming from the duodenum at an area
50 cm to 100 cm from the ileocecal valve. This
very short tract is where food is digested and ab-
sorbed, which causes 90% of the intestines to be
bypassed, resulting in major malabsorptive effects.
The biliopancreatic diversion with duodenal
switch leaves 75 cm to 100 cm of small bowel
available for absorption of nutrients.15 This effec-
tively re-routes the small bowel so less food is ab-
sorbed. Excess fat and carbohydrates are present in
the stool, leading to two to four bowel movements
a day.15 This surgery achieves major weight loss
and the least amount of weight regain of all the
procedures, but it has the highest complication rate.
Protein and vitamin supplements are essential
for persons who have this type of surgery because
so much of the small bowel is bypassed. The sur-
gery is also excellent for decreasing or alleviating
comorbidities because the person’s diabetes melli-
tus, hypertension, gastroesophageal reflux disease,
sleep apnea, and osteoarthritis often are improved
or eliminated. However, the food is bypassing most
of the duodenum, which can lead to malabsorption.
Vitamin and mineral deficiencies can occur as a
result.
Duodenal switch is the most aggressive type
of bariatric surgery and, therefore, has the highest
potential for complications. The duodenal switch
more likely results in excessive weight loss rather
than inadequate weight loss. In the rare case that
there is weight regain after this procedure, it may
be a result of snacking or grazing behaviors where
there is intake of food at frequent intervals. Only
2% to 5% of duodenal switch patients require re-
vision weight-loss surgery. With the assumption
that nonsurgical weight-loss attempts have been
tried and failed, there are two theoretical approaches
to solve this problem: reduce the stomach size or
shorten the length of the common limb. Although
the results of these two revisions vary, reductions
in stomach size seem to generate superior results
over shortening the length of the common limb.15
Vertical Sleeve Gastrectomy
The vertical sleeve gastrectomy is a restrictive
procedure that reduces the stomach size by 85%
through stapling and removal of the portion of the
stomach that has been walled off.14 This leaves the
pylorus and nerve supply intact, thus avoiding
AORN Journal j 219

February 2013 Vol 97 No 2 NEIL
complications, such as anemia and vitamin defi-
ciencies. There is no bypass of the intestinal tract.
Another benefit is that the portion of the stomach
that secretes ghrelin (ie, a hunger-producing hor-
mone) is removed.17 Historically, the vertical sleeve
gastrectomy had been performed as the first stage
of a biliopancreatic diversion. Now it is performed
alone. This procedure restricts food intake and does
not lead to decreased absorption of food.
Patients often seek revisions of this type of sur-
gery because of weight regain. Dilatation of the
narrow sleeve can occur that results in an increased
capacity for food. Conversion to more metaboli-
cally active types of procedures may be the solu-
tion if restriction alone did not result in adequate
weight loss. Revisions to the sleeve gastrectomy
include sleeve resizing, extending the procedure to
a duodenal switch, or converting to a Roux-en-Y
gastric bypass.17 In fact, the vertical sleeve is the
first step of the duodenal switch procedure, so when
converting to a duodenal switch, a significant
portion of the procedure has already been per-
formed. Stomach stretching may occur in a uni-
form way, producing an hourglass configuration
where the top and bottom of the stomach are large,
separated by a narrower part. This causes an un-
comfortable feeling when the patient consumes
food and may be a reason for revision. Another
possibility is placing an adjustable band to add
more restriction.
PERIOPERATIVE NURSING CARE
AORN’s perioperative standards and recommended
practices explain that the morbidly obese pop-
ulation presents special challenges. These stan-
dards provide recommendations for practice that
include creating the proper environment for the
unique psychosocial and physiological needs of
this patient population.29 The bariatric standards
are based on those set by the National Institutes
of Health and the American Society of Bariatric
Surgeons. The standards for selecting bariatric
surgery patients include the following6:
220 j AORN Journal
n performing an in-depth, preoperative assess-
ment of the patient’s risks and surgical benefits;
n selecting a well-informed, motivated patient
who presents acceptable surgical risks;
n selecting a patient based on a low probability of
weight-loss success without a bariatric proce-
dure; and
n choosing a procedure based on the patient’s
functional impairments and comorbidities.
Nurses should realize that patients having revision
surgery may have psychological or social factors that
prevented them from losing adequateweight. Seeking
revision surgery is evidence that the person is at-
tempting to address these issues. Others are having
revision surgery because of complications that have
occurred as a result of the primary weight-loss
procedure that have now resulted in weight regain.
Patients who are obese often have had negative
psychosocial interactions and humiliating experi-
ences with insensitive care providers, so perioper-
ative team members should take care to prevent
this from occurring.30 Perioperative nurses should
prepare a care plan specific to the patient who is
undergoing bariatric revision surgery (Table 4).
Preoperative Nursing Care
Using the Perioperative Nursing Data Set can help
perioperative nurses develop individualized plans
of care based on the needs of patients who are
obese or morbidly obese. The outcome indicators
should include the patient’s knowledge about the
surgery, accurate clinical documentation, sup-
portive resources, and patient satisfaction.31
Obesity has adverse effects on most body sys-
tems. Care begins with a thorough and accurate
assessment. The preoperative nurse should review
the patient’s medical history and physical exami-
nation results and should identify the primary
bariatric procedure and determine whether the
possible reasons for failure were addressed. Pre-
existing respiratory, circulatory, neurological, skin,
and immune system problems should be noted.
Routine skin assessment may be difficult because

TABLE 4. Nursing Care Plan for a Patient Undergoing Bariatric Revision Surgery
Diagnosis Nursing interventionsInterim outcome
statement Outcome statement
Nausea; risk for deficient fluidvolume
n Identifies baseline gastro-intestinal status.
n Identifies physiologicalstatus.
n Reports deviation in diag-nostic study results.
n Monitors physiologicalparameters.
n Evaluates gastrointestinalstatus.
n The patient is NPO asinstructed preoperatively.
n The patient is free fromnausea and vomiting.
n The patient can tolerateclear liquid by mouth beforedischarge postoperatively.
n The patient’s gastrointes-tinal status is maintained ator improved from baselinelevels.
Imbalanced nutrition: less thanbody requirements; imbal-anced nutrition: more thanbody requirements
n Identifies baseline gastro-intestinal status.
n Assesses nutritional habitsand patterns.
n Assesses psychosocialissues specific to thepatient’s nutritional status.
n Includes the patient ordesignated support personin perioperative teaching.
n Provides instructionregarding dietary needs.
n Evaluates response toinstructions.
n Evaluates response tonutritional instruction.
n The patient verbalizescompliance with food andfluid restrictions beforesurgery.
n The patient describesappropriate home man-agement of symptomsthat affect nutritional intake(eg, sore throat, nausea,vomiting) at the time ofdischarge.
n The patient describesthe recommendedpostoperative nutritionalintake regimen for therecovery period at thetime of discharge.
n The patient or designatedsupport person demon-strates knowledge of nutri-tional management relatedto the operative or invasiveprocedure.
Risk for perioperative posi-tioning injury; risk forimpaired skin integrity
n Assesses baseline skincondition.
n Identifies baseline tissueperfusion.
n Identifies baseline muscu-loskeletal status.
n Identifies physical alter-ations that require addi-tional precautions forprocedure-specificpositioning.
n Positions the patient.n Implements protective
measures to prevent skin ortissue injury caused bymechanical sources.
n Applies safety devices.n Evaluates tissue perfusion.
n The patient’s pressurepoints demonstrate hyper-emia for less than 30minutes.
n The patient’s peripheraltissue perfusion is consis-tent with preoperativestatus at discharge from theOR or procedure room.
n The patient is free from painor numbness associatedwith surgical positioning.
n The patient is free fromsigns and symptoms ofinjury related to positioning.
(table continued)
AORN Journal j 221
BARIATRIC REVISION SURGERY www.aornjournal.org

TABLE 4. (continued) Nursing Care Plan for a Patient Undergoing Bariatric Revision Surgery
Diagnosis Nursing interventionsInterim outcome
statement Outcome statement
n Evaluates musculoskeletalstatus.
n Evaluates for signs andsymptoms of physical injuryto skin and tissue.
Deficient knowledge; impairedphysical mobility; ineffectivefamily therapeutic regimenmanagement
n Identifies patient’s anddesignated supportperson’s educationalneeds.
n Identifies expectations ofhome care.
n Includes the patient ordesignated support personin perioperative teaching.
n Provides instruction basedon age and identifiedneeds.
n Evaluates environment forhome care.
n Evaluates response toinstructions.
n The patient voices con-cerns related to post-operative recovery andrehabilitation.
n The patient and designatedsupport person verbalizerealistic expectationsregarding rehabilitationafter surgery.
n The patient verbalizes signsand symptoms to reportimmediately to the surgeon.
n The patient describes theprescribed rehabilitationregimen to follow immedi-ately after discharge fromthe facility.
n The patient participates inthe rehabilitation process.
February 2013 Vol 97 No 2 NEIL
of extra skin folds, lack of landmarks, or chronic
skin conditions. The nurse should document in-
formation on the patient’s age, height, weight,
BMI, skin condition, nutritional status, and aller-
gies. A thorough medication history that includes
what vitamins and herbs the patient is taking is
also essential.
In addition, the nurse should review the patient’s
laboratory test results. Pulmonary function tests and
arterial blood gas results along with ventilation/
perfusion scans often are performed, and the nurse
should ensure that the results are on the patient’s
preoperative chart. The preoperative nurse should
note abnormalities and include them in the plan
of care as well as share concerns with the anesthesia
professional and surgeon. Recent advances in the
care of the bariatric patient include the use of
clinical pathways. The development of ergonomic
technology and use of special bariatric equipment
have improved safety for staff members and
222 j AORN Journal
patients. The nurse should ensure that this equip-
ment is available to safely care for the patient. The
nurse should note whether the patient has any
physical limitations and mobility issues.
The issues of immobility and increased risk for
deep vein thrombosis are always present, especially
in patients who are obese. Prophylaxis may include
administration of low-molecular-weight heparin,
use of thromboembolic device stockings, use of
sequential compression device leggings, and place-
ment of a vena cava filter, particularly for patients
with a history of deep vein thrombosis or hyper-
coagulable states or for those who will not be able
to ambulate easily after surgery. In addition, the
surgeon may request an endocrine evaluation that
includes the status of the patient’s diabetes mellitus.
Skin integrity requires careful assessment. The
nurse should look for areas of irritation, infection,
and ulceration, including under skin folds. The
patient who is morbidly obese may have atypical

BARIATRIC REVISION SURGERY www.aornjournal.org
pressure areas that could lead to pressure sores.
People who have lost large amounts of weight may
have redundant skin, which can result in excessive
skin folds that are areas for potential skin break-
down, particularly in people who have difficulty
performing adequate hygiene. Nurses should assess
the patient’s skin condition for color, edema, evi-
dence of previous surgery (eg, scars), moisture, evi-
dence of fragile tissue, obvious lesions or wounds,
temperature, texture, turgor, and vascularity.31
Intraoperative Nursing Care
In many institutions, designated teams work with
bariatric surgeons on a regular basis. If the patient
has a BMI greater than 35 kg/m2, this should be
noted on the OR schedule so adequate preparations
can be made, including obtaining proper equip-
ment.30 The circulating nurse also should ensure
that adequate personnel are available to safely
move and position the patient.
Positioning is of the upmost importance not only
to prevent injury to pressure areas, but also to ensure
maximum respiratory excursion. Safety consider-
ations for positioning the patient who is morbidly
obese include the following32,33:
n The procedure bed should be able to articulate
and support a patient weighing 800 lb to 1,000 lb.
n Specialized hydraulics capable of lifting pa-
tients weighing as much as 1,000 lb should be
available.
n The mattress should provide sufficient support
and padding and not sag under the weight of the
patient.
n The width of the patient’s legs determines
whether the legs will remain on the bed or
be supported by stirrups or side attachments.
n The patient’s arms may need to be placed in
padded toboggans to support them at the sides
of the patient’s body.
n Extra wide and long safety straps should be
available. In some situations, two safety straps
may be needed, one over the patient’s thighs
and one over the patient’s lower legs. Sheets
should not be used as substitutes for safety
straps.
n If the patient is placed in the supine position,
a roll or wedge may need to be placed under the
right flank to relieve compression on the vena
cava.
n Placing the patient in the Trendelenburg posi-
tion should be avoided because the added
weight of the abdominal contents against the
diaphragm may result in respiratory compro-
mise. Vascular congestion can result if the pa-
tient is placed in the Trendelenburg position
because the blood from the patient’s lower
extremities moves into the central and pulmo-
nary circulation.
n When using reverse Trendelenburg, the circu-
lating nurse should align the patient’s feet flat
on the foot board to prevent rotation and pres-
sure on the patient’s ankles.
A patient who is obese may have decreased chest
wall compliance, increased respiratory resistance,
decreased lung volume and residual capacity, and
increased oxygen consumption. The patient may
have a short, thick neck that can make intubation
more difficult, and he or she may experience rapid
oxygen desaturation. The circulating nurse should
obtain the difficult airway cart, fast-track laryngeal
mask airway, and a direct-visualization intubating
scope used for people with respiratory problems
that may involve difficult intubation. A patient can
experience hypoxia rapidly compounded by the
pressure on the diaphragm from body fat when
lying supine. There is an increased risk for aspira-
tion as well, so the anesthesia professional must
take care to prevent the patient from aspirating.34
Postoperative Nursing Care
The postanesthesia care unit (PACU) nurse should
carefully assess and monitor the patient’s respira-
tory status, including respiratory patterns and rate,
depth, and ease of breathing, because patients who
are obese are more prone to respiratory failure.2
The nurse should help the patient with deep breathing
AORN Journal j 223

February 2013 Vol 97 No 2 NEIL
and coughing exercises and should administer oxy-
gen as ordered. The patient may need bilevel positive
airway pressure or continuous positive airway pres-
sure. Some facilities allow patients to bring their own
masks if they use continuous positive airway pres-
sure at home.
Positioning also is important. The standard supine
and Trendelenburg positions should be avoided
because the weight of the abdominal contents com-
pressing the diaphragm makes breathing more dif-
ficult. The PACU staff should work together to place
the patient in a sitting position at a 45-degree angle
or the lateral position. Care must be taken when
The exponential increase in bariatric surgerywill result in the need for more revisionprocedures and present new challengesfor perioperative nurses.
a patient is in the
lateral position if the
patient has a large
panniculus (eg, a dense
layer of fatty tissue
growth consisting of
subcutaneous fat in the
lower abdominal area).
Staff members can displace the panniculus to the
side with support under it. Staff members should
remember that when a patient turns over, he or she
has an increased risk of falling if the panniculus
shifts. Extra wide stretchers or beds should be used
if available.
Postoperative care involves assessment and
identification of complications. Immediate post-
operative complications, such as anastomotic leaks,
often are manifested by tachycardia.
The patient should ambulate as soon as possible
and the nurse should ensure that proper equipment
is available for helping to lift and position the pa-
tient. Venous thromboembolism is also more prev-
alent in patients who are obese, so ambulation and
physical activity are important. The PACU nurse
should assess the patient for signs and symptoms of
venous thromboembolism (eg, pain or tenderness,
swelling, warmth, or redness in one leg or both
legs) and should include information about this
in the postoperative teaching materials.
The PACU staff should use equipment marked
with weight capacity to ensure safety for the patient
224 j AORN Journal
and staff members.16 People who are obese often
have poor posture that can result in pain, especially
in the spine, knees, and feet. They also have a slower
gait.35 The PACU staff should take special care
when transferring the patient to a wheelchair or
assisting with ambulation. It is best to allow the
patient to move without assistance as much as
possible. The PACU nurse should perform a thor-
ough postoperative skin assessment, noting any
changes from baseline.
The PACU nurse may need to crush medica-
tions into a powder form or use liquid preparations
of the medications because of the reduced size of
the patient’s stomach.
For outpatient proce-
dures, early moni-
toring of pain, activity
level, respiratory
status, urinary output,
fluid tolerance, and
ability to comply with
the medication regimen should be assessed.
For patients with diabetes, the nurse should
measure blood glucose levels at regular, prescribed
intervals while the patient is in the hospital and
instruct the patient to measure his or her blood
glucose levels after discharge. At discharge, the
American Society of Bariatric Surgeons recom-
mends that surgeons follow up with patients at
frequent intervals and should assess the patient’s
weight loss, presence of complications, and status
of comorbities.6 Typically, follow-up occurs with
the initial postoperative visit and then at three-, six-,
and 12-month intervals; after that, patients have
annual appointments. Health care providers should
encourage the patient to find and participate in sup-
port groups or motivational forums.
CONCLUSION
The popularity of bariatric surgery and its expo-
nential increase will result in the need for more
revision procedures to be performed. This will
present new challenges for perioperative nurses
and other health care providers. Postoperative

BARIATRIC REVISION SURGERY www.aornjournal.org
complications may necessitate revision; however,
the most common reasons for revision surgery are
failure to lose the desired amount of weight, regain
of weight lost, or metabolic issues related to the
procedure itself. Further investigation is needed
related to the appropriate interventional methods
for each type of problem and the inherent limita-
tions of the current evidence base for sustained
bariatric surgery success. It is important to develop
strategies to optimize the effectiveness of revi-
sion procedures and nursing care of bariatric
patients.
References1. Kasza J, Brody F, Vaziri K, et al. Analysis of poor
outcomes after laparoscopic adjustable gastric banding.
Surg Endosc. 2011;25(1):41-47.
2. Apau D, Whiteing N. Pre- and post-operative nursing
considerations of bariatric surgery. Gastrointest Nurs.
2011;9(3):44-48.
3. Longitudinal assessment of bariatric surgery (LABS).
How many people have had bariatric surgery? January
2010. Weight-Control Information Network. National
Institute of Diabetes and Digestive and Kidney Diseases.
http://win.niddk.nih.gov/publications/labs.htm#howmany.
Accessed September 14, 2012.
4. Ardestani A, Lautz DB, Tavakkolizadeh A. Band revi-
sion versus Roux-en-Y gastric bypass conversion as
salvage operation after laparoscopic adjustable gastric
banding. Surg Obes Relat Dis. 2011;7(1):33-37.
5. Overweight and obesity statisticsdoverweight and obe-
sity prevalence estimates. Weight-Control Information
Network. National Institute of Diabetes and Digestive and
Kidney Diseases. http://win.niddk.nih.gov/statistics/index
.htm#overweight. Updated February 2010. Accessed
September 14, 2012.
6. Rationale for surgical treatment of morbid obesity.
American Society for Metabolic & Bariatric Surgery.
http://asmbs.org/rationale-for-surgical-treatment. Upda-
ted November 23, 2005. Accessed September 14, 2012.
7. Colquitt JL, Picot J, Loveman E, Clegg AJ. Surgery
for obesity. Cochrane Database Syst Rev. 2009;15(2):
CD003641.
8. Inabnet WB III, Belle SH, Bessler M, et al. Comparison
of 30-day outcomes after non-LapBand primary and re-
visional bariatric surgical procedures from the Longitu-
dinal Assessment of Bariatric Surgery study. Surg Obes
Relat Dis. 2010;6(1):22-30.
9. Bariatric surgery forecasts for 2010. HealthNewsDigest
.com http://www.healthnewsdigest.com/news/Forecast
_630/10_Bariatric_Surgery_Forecasts_for_2010.shtml.
Accessed September 14, 2012.
10. Bessler M, Daud A, DiGiorgi MF, et al. Adjustable
gastric banding as revisional bariatric procedure after
failed gastric bypassdintermediate results. Surg Obes
Relat Dis. 2010;6(1):31-35.
11. Ryou M, Mogabgab O, Lautz DB, Thompson CC. Endo-
scopic foreign body removal for treatment of chronic ab-
dominal pain in patients after Roux-en-Y gastric bypass.
Surg Obes Relat Dis. 2010;6(5):526-531.
12. Hallowell PT, Stellato TA, Yao DA, Robinson A,
Schuster MM, Graf KN. Should bariatric revisional
surgery be avoided secondary to increased morbidity
and mortality? Am J Surg. 2009;197(3):391-396.
13. Frank P, Crookes PF. Short- and long-term surgical
follow-up of the postbariatric surgery patient. Gastro-
enterol Clin North Am. 2010;39(1):135-146.
14. Bariatric surgery for severe obesity. Weight-Control
Information Network. National Institute of Diabetes
and Digestive and Kidney Diseases. http://win.niddk
.nih.gov/publications/gastric.htm. Accessed September
14, 2012.
15. Husted J. Revision weight loss surgery. WLS Revi-
sions Forum. ObesityHelp. http://www.obesityhelp.com/
forums/revision/revision-weight-loss-surgery.html. Sep-
tember 14, 2012.
16. Mulligan AT, McNamara AM, Boulton HW, Trainor LS,
Raiano C, Mullen A. Best practice updates for nursing
care in weight loss surgery. Obesity (Silver Spring). 2009;
17(5):895-900.
17. Langer FB, Shakeri-Leidenm€uhler S, Bohdjalian A, et al.
Strategies for weight regain after sleeve gastrectomy. Surg
Laparosc Endosc Percutan Tech. 2010;20(3):159-161.
18. Kurian MS, Thompson B, Davidson BK. Weight Loss
Surgery for Dummies. Hoboken, NJ: Wiley Publishing,
Inc; 2005:352.
19. Ide P, Farber ES, Lautz D. Perioperative nursing care of the
bariatric surgical patient. AORN J. 2008;88(1):30-54.
20. Maselli R, Rizzello M, Genco A, Fantini A, Basso N. Lap-
aroscopic sleeve gastrectomy as revisional surgery in a
vertical gastroplasty with gastrogastric fistula: a simplified
technique. Surg Laparosc Endosc Percutan Tech. 2011;
21(1):e4-e6.
21. Fernandez-Esparrach G, Lautz DB, Thompson CC. En-
doscopic repair of gastrogastric fistula after Roux-en-Y
gastric bypass: a less-invasive approach. Surg Obes Relat
Dis. 2010;6(3):282-288.
22. Feng JJ, Gagner M, Pomp A, et al. Effect of standard vs
extended Roux limb length on weight loss outcomes after
laparoscopic Roux-en-Y gastric bypass. Surg Endosc.
2003;17(7):1055-1060.
23. Fobi MA, Lee H, Igwe D Jr, et al. Revision of failed
gastric bypass to distal Roux-en-Y gastric bypass:
a review of 65 cases. Obes Surg. 2001;11(2):190-195.
24. Tevis S, Garren MJ, Gould JC. Revisional surgery for
failed vertical-banded gastroplasty. Obes Surg. 2011;
21(8):1120-1124.
25. More number of obese adults are turning to bariatric
surgery as a last resort, says WHO. December 9, 2009.
News Medical. http://www.news-medical.net/news/2009
1209/More-number-of-obese-adults-are-turning-to-baria
tric-surgery-as-a-last-resort-says-WHO.aspx. Accessed
September 14, 2012.
26. FDA expands use of banding system for weight loss. US
Food and Drug Administration. http://www.fda.gov/
NewsEvents/Newsroom/PressAnnouncements/ucm245617
.htm?sms_ss¼email&at_xt¼4d7a6ccec62ec632,0. Upda-
ted March 3, 2011. Accessed September 14, 2012.
AORN Journal j 225

February 2013 Vol 97 No 2 NEIL
27. Rodriguez A. LapBand leaks: what you should know.
http://arturorodriguezmd.com/lap-band-leaks. Updated
March 7, 2009. Accessed September 14, 2012.
28. Topart P, Becouarn G, Ritz P. Biliopancreatic diversion
with duodenal switch or gastric bypass for failed gastric
banding: retrospective study from two institutions with
preliminary results. Surg Obes Relat Dis. 2007;3(5):
521-525.
29. AORN Bariatric surgery guidelines. In: Perioperative
Standards and Recommended Practices. Denver, CO:
AORN, Inc; 2010:490.
30. Graham D, Faggionato E, Timberlake A. Preventing
perioperative complications in the patient with a high
body mass index. AORN J. 2011;94(4):334-347.
31. Petersen C, ed. Perioperative Nursing Data Set: The
Perioperative Nursing Vocabulary. 3rd ed. Denver, CO:
AORN, Inc; 2011:2.
32. Recommended practices for positioning the patient in
the perioperative practice setting. In: Perioperative
226 j AORN Journal
Standards and Recommended Practices. Denver, CO:
AORN, Inc; 2012:421-444.
33. Dybec RB. Intraoperative positioning and care of the
obese patient. Plast Surg Nurs. 2004;24(3):118-122.
34. Brodsky JB. Positioning the morbidly obese patient for
anesthesia. Obes Surg. 2002;12(6):751-758.
35. Fabris de Souza SA, Faintuch J, Valezi AC, et al. Pos-
tural changes in morbidly obese patients. Obes Surg.
2005;15(7):1013-1016.
Janice A. Neil, PhD, RN, is an associate pro-
fessor at East Carolina University, College of
Nursing, Greenville, NC.Dr Neil has no declared
affiliation that could be perceived as posing
a potential conflict of interest in the publication
of this article.

EXAMINATION
CONTINUING EDUCATION PROGRAM3.5
www.aorn.org/CEPerioperative Nursing Care ofthe Patient Undergoing BariatricRevision Surgery
PURPOSE/GOAL
�
The purpose of this activity is to enable the learner to more effectively care for
patients undergoing bariatric revision surgery.
OBJECTIVES
1. Describe types of bariatric surgery.
2. Explain why people undergo bariatric revision surgery.
3. Discuss complications that patients undergoing bariatric revision surgery may
experience.
4. Identify safety precautions that perioperative nurses should institute for patients
undergoing bariatric revision surgery.
The Examination and Learner Evaluation are printed here for your conven-
ience. To receive continuing education credit, you must complete the Exami-
nation and Learner Evaluation online at http://www.aorn.org/CE.
QUESTIONS
1. All types of bariatric surgery involve _________
to reduce the quantity of food that can be
ingested.
a. absorption b. restriction
AORN, Inc, 2013
c. absorption and restriction
2. People seek revision bariatric surgery
1. because they experienced inadequate weight
loss after the primary bariatric procedure.
2. because they regained weight they lost after
the primary bariatric procedure.
3. to treat severe adverse effects and compli-
cations from the primary bariatric procedure.
4. because the comorbidities associated with
obesity were not resolved after the primary
bariatric procedure.
a. 1 and 3 b. 2 and 4
February 2013 Vo
c. 1, 2, and 4 d. 1, 2, 3, and 4
3. Mechanical failures that result when the anat-
omical changes made during the primary proce-
dure are not maintained include
1. a stretched gastric pouch.
2. increased outlet size at the gastric pouch.
3. formation of a gastrogastric fistula between
the gastric pouch and bypassed stomach.
4. increased absorptive abilities beyond
expectations.
l 97 No 2 � AORN Journal j 227

February 2013 Vol 97 No 2 CE EXAMINATION
5. decreased restriction as a result of band
slippage.
a. 4 and 5 b. 1, 2, and 3
228 j AORN Journal
c. 1, 2, 3, and 4 d. 1, 2, 3, 4, and 5
4. The threshold criterion for revision surgery is
weight gain of more than 20 kg (44 lb).
a. true b. false
5. The most common bariatric procedure in the
United States is the
a. biliopancreatic diversion with duodenal
switch.
b. laparoscopic adjustable band.
c. Roux-en-Y gastric bypass.
d. vertical-banded gastroplasty.
6. To resolve a dilated pouch or stoma, the surgeon
may
1. inject sodium morrhuate around the dilated
stoma.
2. move the biliopancreatic limb down further
in the jejunum.
3. perform endoscopic fixation.
4. perform a vertical sleeve gastrectomy-type
procedure.
a. 1 and 3 b. 2 and 4
c. 1, 3, and 4 d. 1, 2, 3, and 4
7. During a vertical sleeve gastrectomy, the part of
the stomach that produces ghrelin, a hormone that
_____________________________, is removed.
a. decreases taste sensitivity
b. produces hunger
c. promotes weight gain
d. stimulates salivary production
8. Prophylaxis for patients with a history of deep vein
thrombosis or hypercoagulable states may include
1. administration of low-molecular-weight
heparin.
2. placement of a vena cava filter.
3. use of sequential compression device
leggings.
4. use of thromboembolic device stockings.
a. 1 and 3 b. 2 and 4
c. 1, 2, and 4 d. 1, 2, 3, and 4
9. Safety considerations for positioning a patient
who is morbidly obese may include
1. employing the Trendelenburg position
whenever possible to shift the patient’s
excess abdominal skin out of the way.
2. placing a roll or wedge under the right
flank if the patient is placed in the supine
position.
3. placing the patient’s arms in padded
toboggans to support them at the sides
of the patient’s body if needed.
4. using sheets as substitutes for safety straps if
needed.
5. using stirrups or side attachments to support
the patient’s legs if needed.
a. 4 and 5 b. 2, 3, and 5
c. 1, 2, 3, and 4 d. 1, 2, 3, 4, and 5
10. Immediate postoperative complications, such as
anastomotic leaks, are often manifested by
a. bloody emesis.
b. bradycardia.
c. rebound tenderness.
d. tachycardia.

LEARNER EVALUATION
CONTINUING EDUCATION PROGRAM3.5
www.aorn.org/CEPerioperative Nursing Care ofthe Patient Undergoing BariatricRevision Surgery
This evaluation is used to determine the extent
to which this continuing education program
met your learning needs. Rate the items as
described below.
OBJECTIVES
To what extent were the following objectives of this
continuing education program achieved?
1. Describe types of bariatric surgery.
Low 1. 2. 3. 4. 5. High
2. Explain why people undergo bariatric revision
surgery. Low 1. 2. 3. 4. 5. High
3. Discuss complications that patients undergoing
bariatric revision surgery may experience.
Low 1. 2. 3. 4. 5. High
4. Identify safety precautions that perioperative nurses
should institute for patients undergoing bariatric re-
vision surgery. Low 1. 2. 3. 4. 5. High
CONTENT
5. To what extent did this article increase your
knowledge of the subject matter?
Low 1. 2. 3. 4. 5. High
6. To what extent were your individual objectives met?
Low 1. 2. 3. 4. 5. High
7. Will you be able to use the information from this
article in your work setting? 1. Yes 2. No
� AORN, Inc, 2013
8. Will you change your practice as a result of reading
this article? (If yes, answer question #8A. If no,
answer question #8B.)
8A. How will you change your practice? (Select all that
apply)
1. I will provide education to my team regarding
why change is needed.
2. I will work with management to change/
implement a policy and procedure.
3. I will plan an informational meeting with
physicians to seek their input and acceptance
of the need for change.
4. I will implement change and evaluate the
effect of the change at regular intervals until
the change is incorporated as best practice.
5. Other: ________________________________
8B. If you will not change your practice as a result of
reading this article, why? (Select all that apply)
1. The content of the article is not relevant to my
practice.
2. I do not have enough time to teach others
about the purpose of the needed change.
3. I do not have management support to make
a change.
4. Other: ________________________________
9. Our accrediting body requires that we verify
the time you needed to complete the 3.5 con-
tinuing education contact hour (210-minute)
program:__________________________________
February 2013 Vol 97 No 2 � AORN Journal j 229