Embed Size (px)
Citation preview

Peripheral Retinal Cryopexy for Subtotal Vitreous Hemorrhage
Will iam H. Ross, M . D . , and Michael J. Gottner, M . D .
We used peripheral retinal cryopexy to treat 20 eyes in 15 patients with subtotal vitreous hemorrhage secondary to proliferative diabetic retinopathy. In 18 eyes, complete panretinal photocoagulation had been performed before the subtotal vitreous hemorrhage and the subsequent cryopexy. The length of follow-up averaged 16 months. The vitreous hemorrhage completely cleared in 11 eyes (55%) and partially cleared in six eyes (30%). Visual acuity after treatment improved in 13 eyes (65%), remained unchanged in six eyes (30%), and decreased in one eye (5%).
DIABETIC RETINOPATHY is the leading cause of blindness in North Americans between the ages of 30 and 60 years. Better diabetic control, the use of multiple daily injections of insulin and infusion pumps, and improved education will increase the life expectancy of diabetic patients. Therefore, the complications of diabetes, including vitreous hemorrhage and fractional retinal detachment, are likely to increase. While panretinal photocoagulation has been shown to be effective in reducing the risk of vitreous hemorrhage and fractional retinal detachment in patients with proliferative diabetic retinopathy,34 vitreous hemorrhage still occurs. Early vitrectomy for vitreous hemorrhage has been advocated by some researchers,5,6 but the complications and morbidity of vitreous surgery are significant.7,8 Because of the risks of early vitrectomy, there has been renewed interest in the use of peripheral retinal
Accepted for publication Jan. 22, 1988. From the Department of Ophthalmology, University
of British Columbia, Vancouver, British Columbia. Reprint requests to William H. Ross, M.D., Retina
Service, Department of Ophthalmology, St. Paul's Hospital, 1081 Burrard St., Vancouver, BC, Canada V6Z 1Y6.
cryopexy in the treatment of patients with vitreous hemorrhage secondary to proliferative diabetic retinopathy.912 We studied 20 eyes in 15 patients with subtotal vitreous hemorrhage secondary to proliferative diabetic retinopathy treated with peripheral retinal cryopexy and evaluated the effect on visual acuity, clearing of vitreous hemorrhage, and recurrent vitreous hemorrhages.
Patients and Methods
Twenty eyes in 15 patients with proliferative diabetic retinopathy who developed one or more recurrent subtotal vitreous hemorrhages from disk or retinal neovascularization, despite panretinal photocoagulation, were included in this study. Eighteen of the eyes had previously undergone panretinal photocoagulation using between 1,500 and 3,000 burns of 200- to 500-u.m spot size.
We allowed three months for the vitreous hemorrhage to clear before determining that further laser photocoagulation was not possible because of hazy media. Subtotal vitreous hemorrhage was defined as bright red blood within the vitreous cavity, which obscured the posterior pole. In most cases, the hemorrhage was darker red and more dense inferiorly. In all cases, at least 50% of the far peripheral retina superiorly was visible with the indirect ophthalmoscope.
Ultrasonic examination was performed pre-operatively in all eyes to rule out the presence of traction retinal detachments. Patients with dense yellow ocher or total red vitreous hemorrhage with no view of the peripheral retina and patients with ultrasonic evidence of traction detachment of the posterior pole were not included in the study and were treated with vitrectomy surgery.
All treatments were performed in the opera-
©AMERICAN JOURNAL OF OPHTHALMOLOGY 105:377-382, APRIL, 1988 377

378 AMERICAN JOURNAL OF OPHTHALMOLOGY April, 1988
ting room by using either retrobulbar blocks with intravenous sedation or general anesthesia. The pupil was dilated with one drop each of phenylephrine 2.5% or 10% and cyc-lopentolate 1% every ten minutes for 30 minutes preoperatively. The technique was similar to that described by Mosier, Del Piero, and Gheewala.12 A 360-degree conjunctival perit-omy was performed. The recti muscles were isolated and a 4-0 black silk suture was placed beneath each muscle to improve manipulation during surgery. Using a 2.5-mm retinal cryo-probe, the superior retina was treated under direct visualization using the indirect ophthalmoscope. A tip temperature of —60 C was achieved. The end point of each treatment was a soft white retinal opacity, which was usually evident after five to ten seconds. Applications beneath the recti muscles, because of the thinner sclera in this location, were usually of two to three seconds' duration. Three rows of four to five evenly spaced applications were made in each of the four quadrants. The anterior applications were made at the level of an imaginary line connecting the insertions of the recti muscles. This approximates the location of the ora serrata. The posterior applications were made at the equatorial region. Each treatment spot was placed approximately one spot size apart. No treatments were made posterior to the equator for fear of increasing contraction of possible preexisting epiretinal membranes.9
When visualization was not possible because of dense vitreous hemorrhage, especially in the inferior quadrants, the average time needed to produce a soft white lesion in the upper quadrants was used. A total of 48 to 60 applications were made between the ora serrata and the equator in each eye treated.
After treatment, the muscle sutures were removed and the conjunctiva reapproximated using interrupted 6-0 plain sutures. Gentami-cin ointment was applied and the eye was patched. Total operating time was approximately 40 minutes. Most of the patients were discharged from the hospital on the first postoperative day. Patients were monitored for clearing of vitreous hemorrhage, improvement of visual acuity, the development of recurrent vitreous hemorrhage, and surgical complications.
Twenty eyes in 15 patients were treated (Table). Eight patients were women and seven were men. They ranged in age from 34 to 76
years (average, 65 years). The duration of diabetes mellitus ranged from ten to 41 years (average, 21 years). Twelve right eyes and eight left eyes were treated. All eyes were phakic. Extensive panretinal photocoagulation had been performed in 18 of the 20 eyes before the vitreous hemorrhage and the retinal cryopexy. Vitreous hemorrhage on initial examination prevented complete panretinal photocoagulation in two patients (Patients 6 and 13), where only 50% and 10%, respectively, of the peripheral retina could be treated.
Results
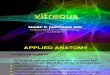
The postoperative follow-up period ranged from 12 to 21 months (average, 16 months). After treatment, there was clearing of the vitreous hemorrhage in 17 of the 20 eyes. The vitreous hemorrhage cleared completely in 11 eyes and partially in six eyes. In three eyes, the vitreous hemorrhage did not clear (Fig. 1). Two eyes with nonclearing hemorrhages have recently undergone vitrectomy surgery. Patient 7, who is in renal failure and on peritoneal dialysis, suffered a stroke and no further treatment was performed on his left eye.
Of the 11 eyes that showed complete reab-sorption of the vitreous hemorrhage, seven cleared completely within eight weeks. In the remaining four eyes, the hemorrhage had cleared by 13 weeks. After 13 weeks, ten of these 11 eyes remained free of any further hemorrhage. Patient 7 suffered a rebleed in his right eye five months after treatment. This rehemorrhage slowly cleared over a two-month period and he has not suffered any further hemorrhage.
After reabsorption of the vitreous hemorrhage, it was possible to visualize atrophic vessels on the optic disk or along the major retinal vessels in eight of 11 eyes. These atrophic vessels were presumably the source of the previous vitreous hemorrhage. In three eyes, there was persistent disk and retinal neovascu-larization and further panretinal laser photocoagulation therapy was applied. This retreat-ment produced complete regression of the disk and retinal vessels in two eyes and partial regression in the third.
Recurrent vitreous hemorrhage occurred in five eyes (25%) (Fig. 1). One case of tractional

Vol. 105, No. 4 Peripheral Retinal Cryopexy 379
PATIENT NO., AGE (YRS),
SEX
1,66, F
2, 72, F
3, 61, M 4,61, M 5, 76, M 6, 74, F 7, 48, M
8, 67, M 9, 72, M
10, 56, F 11,34, F
12,76, F 13, 77, F 14, 67, F
15,61, M
NO. OF YEARS
DIABETIC
41
23
21 20 26 19 19
15 24 26 24
10 12 22
15
EYE
R.E. LE. R.E. L.E. R.E. R.E. R.E. LE. R.E. LE. LE. L.E. R.E. R.E. LE. R.E. R.E. R.E. L.E. R.E.
THETIC
General General Local Local General General General Local General General Local General Local General General Local General General General General
TABLE SUMMARY OF CLINICAL DATA
% OF PREOPERATIVE PANRETINAL
PHOTOCOAGULATION
100 100 100 100 100 100 100 50
100 100 100 100 100 100 100 100 10
100 100 100
VISUAL ACUITY*
PREOPERATIVE
HM HM HM HM 20/200 HM CF HM HM HM HM CF 20/400 20/50 CF 20/200 CF 20/200 20/400 HM
POSTOPERATIVE
20/80 20/80-2 HM CF 20/50+1 20/200 20/50 HM CF HM 20/400 20/200 20/80 20/200 20/200 20/80 CF 20/200 20/80 HM
LENGTH OF
FOLLOW
(MOS)
21 16 19 13 19 19 16 16 16 16 13 19 18 16 16 19 13 12 12 12
VITREOUS CLEARING
Complete Complete Partial Complete Complete Complete Complete None Complete None Complete Partial Complete Partial Partial Complete Partial Partial Complete None
REGRESSION OF
IRIDIS f
N/A N/A Complete N/A N/A Complete N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A Complete
RECURRENT
HEMORRHAGE
No No Yes No No No No No Yes Yes No Yes No No Yes No No No No No
*HM, hand motions; CF, counting fingers. fN/A, not applicable, rubeosis iridis not present before treatment.
20
w c 15 Q.
o 10 I . CD
E
Vitreous Clearing Recurrent Vitreous Hemorrhage
Complete Partial None Recurrence Fig. 1 (Ross and Gottner). Vitreous hemorrhage
completely cleared in 11 of 20 eyes (55%), partially cleared in six eyes (30%), and did not clear in three eyes (15%). Vitreous hemorrhage recurred in five eyes (25%).
20
W c 15 Q) CS Q .
O 10 0) .a E 3 5 -
0
-
-
WW////////M&/A
Improved Same Worse
Post-op vision Fig. 2 (Ross and Gottner). Postoperatively, visual
acuity improved in 13 of 20 eyes (65%), remained unchanged in six eyes (30%), and worsened in one eye (5%).

380 AMERICAN JOURNAL OF OPHTHALMOLOGY April, 1988
retinal detachment developed postoperatively. Visual acuity improved in 13 eyes, remained unchanged in six eyes, and decreased in one eye (Fig. 2). In three eyes with rubeosis iridis as well as vitreous hemorrhage, complete regression of the iris neovascularization was noted after treatment. In two of these eyes, the rubeosis iridis involved only the pupillary margin preoperatively. In the third case (Patient 15), there was evidence of extensive rubeosis with closure of the anterior chamber angle from the 8 o'clock to the 4 o'clock meridian. Only the inferior angle remained open. After peripheral retinal cryopexy, the iris vessels regressed and the inferior angle continued to be patent. Intraocular pressure in this patient has been controlled with one drop of timolol maleate 0.5% twice daily. In three of the 20 eyes treated with peripheral retinal cryopexy, the eye treated was the one eye with useful vision. In two of these patients, the other eye had undergone unsuccessful vitrectomy surgery for vitreous hemorrhage and traction detachments (Patients 5 and 9). The third patient (Patient 10) showed evidence of massive proliferative vitreoretinop-athy in her left eye, which was believed to be inoperable.
Discussion
The Diabetic Retinopathy Study demonstrated that panretinal photocoagulation can produce regression of disk and retinal neovascularization and prevent severe visual loss in patients with diabetic retinopathy who have high-risk characteristics.3,4 Panretinal photocoagulation presumably decreases the production of a vasoproliferative factor by the ischemic retina and induces regression of the disk and retinal neovascularization. The same mechanism is believed to account for the regression of iris neovascularization. However, despite panretinal photocoagulation, 20.1% of patients with high-risk characteristics suffer recurrent vitreous hemorrhage.4 Once vitreous hemorrhage occurs, further laser therapy is not possible, and other treatment modalities must be considered.
Early vitrectomy in these patients has been advocated by Shea, Young, and Howcroft5 and Blankenship and Machemer.6 However, complications of vitrectomy are considerable78 and include rubeosis iridis in 13% of phakic eyes
and 32% of aphakic eyes, iatrogenic retinal breaks during surgery in 20% of cases, postoperative retinal detachments in 16% of cases, intraoperative and postoperative vitreous hemorrhage in 4% and 29% of cases, respectively, and visually significant lens opacities in 17% of phakic eyes. Reoperation in up to 25% of eyes with vitrectomies has been reported secondary to retinal detachment or nonclearing of vitreous hemorrhage.78 Many patients with proliferative diabetic retinopathy are also medically unstable and some are undergoing peritoneal or hemodialysis. Therefore, there can be a significant degree of morbidity in these patients undergoing prolonged surgical procedures.
Peripheral cryopexy offers a less invasive form of management in diabetic patients with subtotal vitreous hemorrhage and has, therefore, been advocated.913 As with panretinal photocoagulation, the supposed mechanism of action is to decrease the production of a vasoproliferative factor, the stimulus for neovascularization, by ablating the peripheral ischemic retina. The result is regression of existing disk and retinal neovascularization and the prevention of further vitreous hemorrhage. Histologic studies of thermal lesions resulting from diathermy, photocoagulation, and cryopexy have been studied extensively1415 and have been found to produce similar retinal destruction.
Clinically, we were impressed with the rapid reabsorption of the vitreous hemorrhage after peripheral retinal cryopexy. On the first postoperative day, it is often possible to obtain a gross view of the posterior pole. In seven of 11 eyes that cleared completely, the hemorrhage was totally reabsorbed by eight weeks. By 13 weeks, the remaining four eyes had cleared. The relatively rapid clearing of the vitreous hemorrhage differs significantly from the slow absorption of vitreous blood that occurs in untreated eyes. Although the exact mechanism of this rapid clearing is not known, the choroi-dal lesions produced by cryopexy may aid the reabsorption of hemorrhage by producing inflammatory changes in the blood-retinal barrier. Alterations of the retinal pigment epithelium may also be a factor in this rapid clearing.
In this study, complete clearing of vitreous hemorrhage was achieved in 11 eyes (55%) and partial clearing was achieved in six eyes (30%); three eyes (15%) did not clear (Fig. 1). Visual acuity improved in 13 eyes (65%) (Fig. 2). Visual acuity of 20/200 or better was achieved in 11 eyes (55%). In three patients, the treated eye

Vol. 105, No. 4 Peripheral Retinal Cryopexy 381
was the only eye with useful vision and these patients regained independence and were able to move about freely and care for themselves without the risk of vitrectomy.
Our results are similar to those reported by Mosier, Del Piero, and Gheewala.12 They found complete vitreous clearing in 56% of their cases, improvement in visual acuity in 65%, and a visual acuity of 20/200 or better in 56%. In a series of 100 cases reported by Daily and Gieser,11 complete clearing of the vitreous hemorrhage was achieved in 75% of patients and improved vision in 46%. In their series, 83% of patients achieved a visual acuity of 20/200 or better.
Tractional retinal detachment with macular involvement occurred in one of our patients. This 5% incidence is similar to that reported previously. Mosier, Del Piero, and Gheewala12
reported a 4% incidence (one of 24 eyes), Benedett and associates13 found a 3.2% incidence (five of 158 eyes), and Daily and Gieser11
found a 6% incidence (six of 100 eyes) of traction detachments. These figures are much lower than those reported by Oosterhuis and Bijlmer-Gorter9 and Ramsay, Cantrill, and Knobloch.10 In Oosterhuis and Bijlmer-Gorter's9 series of 21 cases, seven (33%) were found to have traction detachments after clearing of the vitreous hemorrhage. However, preoperative ultrasound studies were not performed to determine if the traction detachments were present before cryopexy. In Ramsay, Cantrill, and Knobloch's10 series of 14 cases, five (36%) developed traction detachments after cryoablation. In both of these series, the cryoapplications were made posterior to the equator, and, in many cases, confluent applications were made to the level of the vascular arcades. Their high incidence of traction detachments may have been caused by these posterior applications of cryopexy with resultant inflammation of the vitreous and secondary contraction of preexisting fibrovascular membranes. Lincoff and McLean16 described vitreoretinal adhesions and condensation of vitreous fibrils at the point of excessive cryo-application. They postulated that the fibrils may also have been indirectly damaged by cryopexy-induced uveitis.
Recurrent vitreous hemorrhage occurred in five eyes, or 25% of our cases.2 These results are similar to those reported by Mosier, Del Piero, and Gheewala12 and Benedett and associates.13
Regression of rubeosis iridis was noted in
three treated patients. A similar result was reported by Ramsay, Cantrill, and Knobloch10
in three patients with rubeosis. Again, this is believed to be secondary to the decreased production of angiogenesis factor by the ischemic retina.
In view of the good result in this study and in that reported by Mosier, Del Piero, and Gheewala12 using peripheral cryotherapy as well as the low incidence of complications, the following protocol in the management of patients with proliferative diabetic retinopathy seems reasonable. All patients with proliferative diabetic retinopathy and high-risk characteristics4 should undergo panretinal photoco-agulation therapy in an attempt to induce regression of the disk and retinal neovascular-ization. If vitreous hemorrhage occurs despite panretinal photocoagulation and if the hemorrhage is subtotal, peripheral cryopexy treatment should be performed as described. In one case in this series and in another reported by Mosier, Del Piero, and Gheewala12 a patient with a visual acuity of 20/50 or better developed a tractional retinal detachment with macular involvement and resultant severe loss of visual acuity. Therefore, in patients with a visual acuity of better than 20/200, observation for spontaneous clearing of vitreous hemorrhage is advisable so that additional panretinal photo-coagulation can be performed. Patients with unresolved total vitreous hemorrhage and tractional detachments with macular involvement should undergo vitrectomy.
References
1. Kohner, E. M, and Oakley, N. W.: Diabetic retinopathy. Metabolism 24:1085, 1975.
2. Kahn, H. A., and Hiller, R.: Blindness caused by diabetic retinopathy. Am. J. Ophthalmol. 78:58, 1974.
3. The Diabetic Retinopathy Study Research Group: Preliminary report on effects of photocoagulation therapy. Am. J. Ophthalmol. 81:383, 1976.
4. The Diabetic Retinopathy Study Research Group: Four risk factors for severe visual loss in diabetic retinopathy. The third report from the Diabetic Retinopathy Study. Arch. Ophthalmol. 97:654, 1979.
5. Shea, M., Young, P. W., and Howcroft, M. J.: "Early" vitrectomy for vasoproliferative retinopathy in patients with insulin-dependent diabetes mellitus. Can. J. Ophthalmol. 8:150, 1982.
6. Blankenship, G. W., and Machemer, R.: Prophy-

382 AMERICAN JOURNAL OF OPHTHALMOLOGY April, 1988
lactic vitrectomy in proliferative diabetic retinopa-thy. Mod. Probl. Ophthalmol. 18:236, 1977.
7. Oyakawa, R. T., Schachat, A. P., Michels, R. G., and Rice, T. A.: Complications of vitreous surgery for diabetic retinopathy. I. Intraoperative complications. Ophthalmology 90:517, 1983.
8. Schachat, A. P., Oyakawa, R. T., Michels, R. G., and Rice, T. A.: Complications of vitreous surgery for diabetic retinopathy. II. Postoperative complications. Ophthalmology 90:522, 1983.
9. Oosterhuis, J. A., and Bijlmer-Gorter, H.: Cryo-treatment in proliferative diabetic retinopathy. Oph-thalmologica 181:81, 1980.
10. Ramsay, R. C , Cantrill, H. L., and Knobloch, W. H.: Cryoretinopexy for proliferative diabetic retinopathy. Can. J. Ophthalmol. 17:17, 1982.
11. Daily, M. J., and Gieser, R. G.: Treatment of proliferative diabetic retinopathy with panretinal cryotherapy. Ophthalmic Surg. 15:741, 1984.
12. Mosier, M. A., Del Piero, E., and Gheewala, S. M.: Anterior retinal cryotherapy in diabetic vitreous hemorrhage. Am. J. Ophthalmol. 100:440, 1985.
13. Benedett, R., Oik, R. J., Arribas, N. P., Okun, E., Johnston, G. P., Boniuk, I., Escoffery, R. F., Grand, M. G., and Schoch, L. H.: Transconjunctival anterior retinal cryotherapy for proliferative diabetic retinopathy. Ophthalmology 94:612, 1987.
14. Kurtin, G. T., Fujino, T., and Norton, G. W.: Comparative histopathology of cryosurgery and photocoagulation. Arch. Ophthalmol. 35:674, 1966.
15. Zauberman, J.: Tensile strength of chorioretinal lesions produced by photocoagulation, diathermy and cryopexy. Br. J. Ophthalmol. 53:749, 1969.
16. Lincoff, H. A., and McLean, J. M.: Cryosurgical treatment of retinal detachment. Part II. Am. J. Ophthalmol. 61:1227, 1966.
OPHTHALMIC MINIATURE His right eye gradually regained normal vision, and his left eye, though oddly 's tained, ' regained enough sight to help its colleague. He had worn glasses before, and now with perceptibly thicker lenses was able to envisage, and then attain, a return to an ordinary life of walking and reading. The situation was even likely to improve further, and he might expect to be able to drive a car again. 'You don ' t just see with your eyes, you see with your brain, ' his cheerful doctor told him, ' and it's amazing what ingenious adjustments it can make!' The same doctor assured him that his 'funny eye, ' certainly noticeable, looked 'fascinating, ' even 'positively attractive. '
Iris Murdoch, The Book and the Brotherhood New York, Viking Penguin Inc., 1988, p. 93



















![Why worry about strabismus? [1,8] Vitreous Hemorrhage (dark reflex) Hypopyon (layering of WBCs in anterior chamber)](https://img.pdfslide.net/doc/110x75/5697bfc21a28abf838ca5133/why-worry-about-strabismus-18-vitreous-hemorrhage-dark-reflex-hypopyon.jpg)