Embed Size (px)
Citation preview

Current Eye Research, Early Online, 1–7, 2013! Informa Healthcare USA, Inc.
ISSN: 0271-3683 print / 1460-2202 online
DOI: 10.3109/02713683.2013.803288
ORIGINAL ARTICLE
Permeability of the Anterior Lens Capsule forLarge Molecules and Small Drugs
Christian Kastner1, Marian Lobler1, Katrin Sternberg1, Thomas Reske1, Oliver Stachs2,Rudolf Guthoff2 and Klaus-Peter Schmitz1
1Institute for Biomedical Engineering and 2Department of Ophthalmology, University of Rostock,Rostock, Germany
ABSTRACT
Purpose: For developing injectable lenses the retention properties of the capsular bag are important. Thereforethe apparent permeability coefficients of sodium fluorescein and fluorescent dextrans of different sizes weredetermined for the human anterior lens capsule to calculate a molecular weight cutoff from these data. Inaddition, permeability coefficients of drugs helpful for the suppression of secondary cataract were determined.
Materials and Methods: Capsulorhexis specimens were fixed in a specially designed two compartment diffusionchamber to investigate the permeation of sodium fluorescein and fluorescent dextrans of different sizes (10, 40,70 and 150 kDa) for 24 h (n� 3) and of the antiproliferative drugs actinomycin D and methotrexate for 0.5, 24, 48and 72 h (n� 3).
Results: The molecular weight cutoff of the anterior lens capsule was found to be 166� 82 kDa. After 0.5 h, nopassage of actinomycin D and methotrexate was detectable through the lens capsule. The apparent permeabilitycoefficients for actinomycin D and methotrexate were calculated to 0.71� 0.02 mm/s and to 0.80� 0.13 mm/s,respectively.
Conclusions: The capsular bag retains fluorescent dextrans with a molecular weight of 4166 kDa. Hence,prepolymers are required to polymerize rapidly to be retained inside of the capsular bag. In addition, low-molecular substances intended as antiproliferative drugs for secondary cataract prevention should be appliedwithin a time frame of five minutes in such a way that cells adjacent to the capsular bag will not be damaged.
Keywords: Actinomycin D, anterior lens capsule, apparent permeability coefficient, methotrexate, molecularweight cutoff
INTRODUCTION
Cataract is the most common cause of reversibleblindness worldwide, accounting for nearly half of allcases of blindness.1 The prevalence of cataractincreases with age and will increase in both develop-ing and developed countries due to demographicdevelopment.2 In cataract formation, transparency ofthe natural lens is lost and visual acuity impaired.The mechanical strength of the lens capsule allowsfor implantation and a good fit of well-designedintraocular lenses.3
Since the first implantation of an artificial lens bySir Harold Ridley in 1949, the design of intraocularlenses has been improved continually. Today ophthal-mologists strive to sustain accommodation followingcataract surgery. One strategy is the development ofa polymer-based lens injectable into the capsularbag with properties comparable to the crystallinelens.4 During the process the capsular bag will bepreserved after lens removal, and the natural capabil-ity of accommodation via the ciliary musclesand the zonula fibers will be maintained.5 Leakageof lens constituents from the capsular bag has still
Correspondence: Christian Kastner, Institute for Biomedical Engineering, University of Rostock, F.-Barnewitz-Str. 4, D-18119 Rostock,Germany. E-mail: [email protected]
Received 20 September 2012; revised 25 February 2013; accepted 1 May 2013; published online 22 July 2013
1
Cur
r E
ye R
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
11/1
3Fo
r pe
rson
al u
se o
nly.

to be addressed beyond proper sealing of themini-rhexis.
Material convenient for lens refilling could be aninjectable soft polymer with an appropriate refractiveindex and corresponding viscoelastic properties of thecrystalline lens. Using an in situ two componentsystem of curable prepolymers may prevent leakageof the polymer from the capsular bag.6 As withimplantable artificial lenses secondary cataract,caused by proliferation and extracellular matrix pro-duction of lens epithelial cells (LECs), occurs withinjectable lenses as well.5
One way to prevent secondary cataract sustainablyis short-term treatment of the capsular bag withdistilled deionized water leading to a decrease ofviable lens epithel cells in the capsular bag.7,8 Afurther approach avoiding secondary cataract in thelong term is local administration of antiproliferativesubstances to prevent cell proliferation and consecu-tive fibrosis. Actinomycin D (AM) and methotrexate(MTX) were chosen as candidates for antiproliferativeagents, because they inhibit cell proliferation in ex vivoand in vivo models.9–11 AM intercalates into the DNAimmobilizing the transcriptional complex and inter-fering with the elongation of RNA.12 MTX is anantagonist of folic acid synthesis and thus inhibitsproliferation of cells, and it is further used as anti-inflammatory agent to treat rheumatoid arthritis.13 A5 min treatment of human capsulorhexis specimenswith 1�10�5 mol/l MTX and 1�10�5 mol/l AM,applied in 1% sodium hyaluronate for a safe drugadministration, reduced the number of viable LECs to0.27� 0.50% and 0.07� 0.19%, respectively.9 Similarly,different in vivo studies demonstrated a reducedsecondary cataract formation after drug treatment,where after phacoemulsification the inside of thecapsular bag was incubated for 5 min with either amixture of 1�10�5 mol/l MTX and 1�10�5 mol/l AMin 1% sodium hyaluronate9,10 or a combination of25 mg/ml (8.89� 10�5 mol/l) cycloheximide with10 mg/ml (0.80� 10�5 mol/l) AM in 1% sodium hya-luronate.11 A 5 min intraoperative drug administra-tion followed by implantation of rigid lenses showedno secondary cataract formation up to four monthsafter implantation.9 When MTX and AM were used inconjunction with the injection of two componentsilicone polymer lenses, secondary cataract formationwas absent 12 months postoperatively and negligible3 years after surgery.10 Treating the capsular bagwith AM in combination with cycloheximide alsoreduced the development of secondary cataract after3 months.11
To address the questions whether there could be apermeation of injectable lens constituents or drugsthrough the lens capsule and affect adjacent tissue, aspecially designed two compartment diffusion cham-ber was used to determine the molecular weightcutoff of the human anterior lens capsule by means of
fluorescent dextrans, and to calculate the apparentpermeability coefficients for the antiproliferative andantifibrotic drugs AM and MTX for the humananterior lens capsule.
MATERIALS AND METHODS
Chemicals
To assess the molecular weight cutoff of the anteriorlens capsule, sodium fluorescein with a molecularweight of 376.27 g/mol and fluorescein isothiocyan-ate (FITC) dextrans with average molecular weightsof 10,000, 40,000, 70,000 and 150,000 g/mol wereused as easily quantifiable model substances andnon-fluorescent dextrans of comparable molecularweight as counterparts to prevent osmotic effects(Sigma-Aldrich Chemie GmbH, Steinheim,Germany). For use, the dextrans were dissolved ata concentration of 1�10�5 mol/l in phosphate buf-fered saline (PBS) (PAA, Colbe, Germany). Toaddress the question whether the lens capsule ispermeable for antiproliferative substances, the drugsAM (1255.42 g/mol) (Sigma-Aldrich) and MTX(454.44 g/mol) (Ubichem Ltd., Eastleigh,Hampshire, UK) were used. Stock solutions of1�10�1 mol/l AM in ethanol or 1�10�1 mol/l ofMTX in dimethyl sulfoxide were prepared andfurther diluted with ultrapure water (Ultra ClearUV Plus, SG Water, Hamburg-Barsbuttel, Germany)to 1�10�5 mol/l. Analyical grade ethanol anddimethyl sulfoxide were received from VWRInternational GmbH (Darmstadt, Germany).
Human Capsulorhexis Specimens
Human capsulorhexis specimens were obtainedduring standard cataract surgery from patients aged49–89 years following the principles in the Declarationof Helsinki. The circular specimens had a diameter ofapproximately 3 mm. Immediately after resection,they were placed in Dulbecco’s modified Eagle’smedium with 4.5 g/l D(þ)-glucose, 4� 10�3 mol/l L-glutamine, and 1�10�3 mol/l sodium pyruvate(PAA), supplied with 44� 10�3 mol/l NaHCO3
(Merck, Darmstadt, Germany), 20� 10�3 mol/lHEPES (PAA), 5 mg/ml gentamicin (Sigma-Aldrich),2.5 mg/ml amphotericin B (PAA), and 10% FCS(PAA), adjusted to pH 7.4. The specimens wereused within two days after resection. Beforethe permeability experiments, the anterior lenscapsules were examined by light microscopyand should not contain any breaks or injuries.In order to decellularize the lens capsules, thespecimens were briefly placed into sterile filtereddeionized water.
2 C. Kastner et al.
Current Eye Research
Cur
r E
ye R
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
11/1
3Fo
r pe
rson
al u
se o
nly.

Permeability Experiments
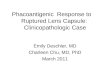
The permeability experiments were performed in aPMMA diffusion chamber with two compartments,separated by the capsulorhexis specimen (Figure 1).While fixing the specimen, the orientation of the innerand the outer surface was not considered. Eachcompartment was frustum-shaped, had a capacity ofabout 1.5 ml, and could be fitted one to the other by twopins and fixed by three screws. The permeation areaof the lens capsules was 1 mm2. Each chamber couldbe filled and sampled via a sampling channel, withan additional channel allowing for pressure com-pensation. The channels were closed by plastic pegs.
In case of assessing the molecular weight cutoff thedonor compartment was filled with sodium fluores-cein or fluorescent dextrans in PBS, the acceptorcompartment was filled with PBS or the non-fluor-escent dextrans of corresponding molecular weight inPBS to maintain a constant pH value. For investigatingdrug permeation through the lens capsule, the donorcompartment was filled with AM or MTX in ultrapurewater, the acceptor compartment was filled withultrapure water. Investigating the fluorescent dextrans,the chambers were incubated at 37 �C on a shakerat 100 rpm (Heidolph Inkubator 1000 and Unimax1919, VWR, Darmstadt, Germany). Investigating thedrugs, the chambers were incubated at 37 �C, 5% CO2
and 95% relative humidity in a cell incubator (HeraeusBB 6220 CU O2 incubator, Fisher Scientific, Schwerte,Germany). To determine the molecular weight cutoff,the permeability experiments with each type of fluor-escent dextrans were performed for 24 h with n� 3.The permeability experiments using the drugs wereperformed for 0.5, 24, 48 and 72 h with n� 3.
Quantitative Determination of SubstancesFollowing the Permeability Experiments
After the indicated times of incubation, the contentsof donor and acceptor compartment were removed,and their volume was determined. In case ofsodium fluorescein or the fluorescent dextransfluorescence was measured in black 96-wellmicroplates (greiner bio one, Frickenhausen,Germany) by a microplate fluorescence reader,with an excitation wavelength of 485 nm andan emission wavelength of 520 nm (FLUOstarOPTIMA, BMG Labtech, Offenburg, Germany).Concentration of fluorescent molecules in each com-partment was calculated from calibration curves from1�10�8 to 1�10�5 mol/l of fluorescent substance.The limit of quantitation (LOQ) was 2.55� 10�9 mol/lfor sodium fluorescein or below for all FITC dextrans.
The antiproliferative drugs AM and MTX wereanalyzed by means of high performance liquid chro-matography (HPLC) (Knauer GmbH, Berlin,Germany). For each drug a Chromolith�
FastGradient RP-18 e 50-2 column (Merck KGaA,Darmstadt, Germany) with a particle size of 5 mmand a dimension of 100� 4.6 mm2 was used. Forcalibration, standards of these drugs were used withconcentrations of 0.1, 0.5, 1.0, 2.0, 5.0 and 10.0 mg/ml.
AM was measured in a gradient run at 25 �C, using5� 10�3 mol/l ammonium acetate (pH 3.5) as eluent Aand methanol as eluent B. For the first 7 min a lineargradient ranged from 35 to 10% A to elute AM,followed by another linear gradient from 10 to 35% Afor 1 min, and finally AM was run isocratically with35% A for 4 min to equilibrate the column for the nextsample. The injection volume was 20 ml, the flow rate1.0 ml/min. The detection wavelength was set to443 nm. The retention time was 6.6 min. LOQ was0.32� 10�6 mol/l.
MTX was run isocratically at 40 �C with a 5:95%mixture (v/v) of acetonitrile and ammonium acetate(1�10�3 mol/l, pH 6) as mobile phase with a detec-tion wavelength of 301 nm, a retention time of 6.5 min,and injection volume and flow rate as above for AM.LOQ was 0.11�10�6 mol/l.
For better comparison values below LOQ were setto zero. The ratios of acceptor and donor compart-ment concentrations were calculated, given asmeans� standard error of the mean (SEM).
Calculation of the Apparent PermeabilityCoefficient
To determine the apparent permeability coefficient ofthe fluorescent substances and the drugs, the follow-ing equation was used:14,15
Papp ¼ DQ=ðDt � A� C0Þ mm=s½ � ð1Þ
FIGURE 1 PMMA diffusion chamber for permeability meas-urements, a: donor compartment, a’: acceptor compartment,b: fixed capsulorhexis specimen, c: fixing screw, d: fittingpin, e: sampling channel, e’: pressure compensating channel,f: plastic peg.
Anterior Lens Capsule Permeability 3
! 2013 Informa Healthcare USA, Inc.
Cur
r E
ye R
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
11/1
3Fo
r pe
rson
al u
se o
nly.

with Papp being the apparent permeability coefficientand DQ [mg] representing the mass difference ofthe acceptor compartment after the time periodDt [s]. A [mm2] is the permeation area of thecapsulorhexis specimen and C0 [mg/mm3] denotesthe initial concentration of the fluorescent substancesand the drugs in the donor compartment, calculatedfrom the values determined by fluorescence andHPLC measurements [mmol/l]. Values are given asmeans� SEM.
RESULTS
The permeability of the human anterior lens capsulewas probed with sodium fluorescein and fluorescentdextrans in the range of 376.27–150,000 g/mol. Withincreasing molecular weight, decreasing amountsof fluorescent substance were detected in the acceptorcompartment. After 24 h, 0.67� 0.21�10�6 mol/lof sodium fluorescein and 0.09� 0.05� 10�6 mol/l ofthe largest FITC dextran (150,000 g/mol) were mea-sured (Table 1). In the donor compartment, theamount of fluorescent substance ranged between8.59� 0.09� 10�6 mol/l and 9.98� 0.04� 10�6 mol/l(Table 1).
Permeability was inversely proportional to themolecular weight of the probe. The ratios calculatedfrom the concentrations of fluorescent substance,measured in the acceptor and donor compartments,ranged between 0.079� 0.025 for sodium fluorescein
and 0.009� 0.005 for the largest FITC dextran(150,000 g/mol) (Figure 2A, Table 1).
From the permeability data the apparent perme-ability coefficients (Papp) were calculated and plottedagainst the molecular weight (Figure 2B). Papp
decreased with increasing molecular weight, rangingfrom 0.92� 0.29 mm/s to 0.12� 0.07 mm/s (Table 1).Linear regression (Figure 2B) resulted in the followingequation:
y ¼ �4:542� 10�6 � xþ 0:7542 ð2Þ
The molecular weight cutoff of the anterior lenscapsule is defined as the x-intercept of166,036� 81,656 g/mol (¼^ 166� 82 kDa).
If antiproliferative drugs such as AM or MTX areconsidered as an option for preventing cataractformation, the permeability through the lens capsulehas to be taken into account. Over time, increasingamounts of AM were detected in the acceptor com-partments. After 0.5 h, the amount of AM was belowLOQ and after 72 h 1.42� 0.41�10�6 mol/l AM werefound (Figure 3A, Table 2). In the donor compart-ments the AM amount decreased with time from8.83� 0.01�10�6 mol/l after 0.5 h to 6.70� 0.38� 10�6 mol/l after 72 h (Figure 3A, Table 2).
Considering the concentrations found in the accep-tor compartments in relation to these measured in thedonor compartments, it can be stated that thecalculated ratios ranged between zero after 0.5 h and0.225� 0.077 after 72 h (Figure 3B, Table 2).
FIGURE 2 (A) Ratios of acceptor and donor compartment concentrations of sodium fluorescein and FITC dextrans with averagemolecular weights of 10,000, 40,000, 70,000 and 150,000 g/mol after 24 h (means� SEM). (B) Apparent permeability coefficients (Papp)of sodium fluorescein and FITC dextrans plotted against their molecular weights (means� SEM). The molecular weight cutoff of theanterior lens capsule is defined as the x-intercept obtained by linear regression.
TABLE 1 Measured concentrations of sodium fluorescein and FITC dextrans (10, 40, 70 and 150 kDa) in the donor and acceptorcompartments, calculated acceptor to donor ratios and apparent permeability coefficients after 24 h.
MW (�103 g/mol) 0.376 10 40 70 150
[Donor] (�10�6 mol/l) 8.59� 0.09 9.55� 0.08 9.98� 0.04 9.20� 0.62 9.87� 0.004[Acceptor] (�10�6 mol/l) 0.67� 0.21 0.46� 0.13 0.38� 0.24 0.26� 0.10 0.09� 0.05Ratio [acceptor]/[donor] 0.079� 0.025 0.048� 0.013 0.039� 0.023 0.028� 0.015 0.009� 0.005Papp (mm/s) 0.92� 0.29 0.62� 0.16 0.52� 0.33 0.35� 0.14 0.12� 0.07
Means� SEM. LOQ� 2.55� 10�9 mol/1.
4 C. Kastner et al.
Current Eye Research
Cur
r E
ye R
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
11/1
3Fo
r pe
rson
al u
se o
nly.

A drug permeation through the capsulorhexisspecimens within a time period of 72 h was alsoobserved for MTX. The amount of MTX in theacceptor compartments was below LOQ after 0.5 h,whereas 0.76� 0.09� 10�6 mol/l were found after 72 h(Figure 4A, Table 2). In the donor compartments5.37� 0.07� 10�6 mol/l were detected after 0.5 h and4.28� 0.10� 10�6 mol/l after 72 h (Figure 4A, Table 2).
The ratios calculated from the MTX concentrationsmeasured in the acceptor and donor compartmentsranged from zero after 0.5 h to 0.178� 0.021 after 72 h(Figure 4B, Table 2).
The apparent permeability coefficients (Papp) forAM and MTX are summarized in Table 2. The meansof the apparent permeability coefficients of 24, 48 and72 h incubations were calculated to 0.71� 0.02 mm/sfor AM and to 0.80� 0.13 mm/s for MTX.
To estimate the time for the drugs being quantify-able in the acceptor compartment linear regressions ofthe time-dependent increase of concentration wereperformed for both AM
y ¼ 2:10� 10�8 � x ð3Þ
FIGURE 4 Quantification of MTX. (A) HPLC chromatogram of a 1�10�5 mol/l MTX solution. The inserts show representativeconcentration peaks from the donor and the acceptor compartment after 0.5, 24, 48 and 72 h. (B) Ratios of acceptor and donorcompartment concentrations of MTX after 0.5, 24, 48 and 72 h (means� SEM). After 0.5 h, the amount of MTX was below LOQ.
FIGURE 3 Quantification of AM. (A) HPLC chromatogram of a 1�10�5 mol/l AM solution. The inserts show representativeconcentration peaks from the donor and the acceptor compartment after 0.5, 24, 48 and 72 h. (B) Ratios of acceptor and donorcompartment concentrations of AM after 0.5, 24, 48 and 72 h (means� SEM). After 0.5 h, the amount of AM was below LOQ.
TABLE 2 Measured concentrations of AM and MTX in the donor and acceptor compartments, calculated acceptor to donor ratios andapparent permeability coefficients after 0.5, 24, 48 and 72 h.
Drug T (h) 0.5 24 48 72
AM [Donor] (�10�6 mol/l) 8.83� 0.01 8.58� 0.14 8.14� 0.13 6.70� 0.38[Acceptor] (�10�6 mol/l) 5LOQ 0.54� 0.09 1.16� 0.41 1.42� 0.41Ratio [acceptor]/[donor] 0.000� 0.000 0.065� 0.012 0.141� 0.049 0.225� 0.077
Papp (mm/s) 0.00� 0.00 0.69� 0.12 0.75� 0.26 0.68� 0.19MTX [Donor] (�10�6 mol/l) 5.37� 0.07 4.83� 0.03 5.11� 0.11 4.28� 0.10
[Acceptor] (�10�6 mol/l) 5LOQ 0.49� 0.04 0.81� 0.14 0.76� 0.09Ratio [acceptor]/[donor] 0.000� 0.000 0.101� 0.009 0.161� 0.030 0.178� 0.021
Papp (mm/s) 0.00� 0.00 0.65� 0.11 1.05� 0.19 0.69� 0.08
Means� SEM. LOQAM = 0.32� 10�6 mol/l, LOQMTX = 0.11�10�6 mol/l.
Anterior Lens Capsule Permeability 5
! 2013 Informa Healthcare USA, Inc.
Cur
r E
ye R
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
11/1
3Fo
r pe
rson
al u
se o
nly.

and MTX
y ¼ 1:31� 10�8 � x: ð4Þ
The linear regression resulted in crossing LOQtimes of 15.25� 2.5 h for AM and 8.41� 0.90 h forMTX.
DISCUSSION
Designing an injectable polymer-based lens requiresan exact knowledge of the human lens capsulepermeability qualities, which depends on its struc-ture. Danysh & Duncan provided a comprehensivereview about lens capsule characteristics.16 The lenscapsule consists of a relatively thick basement mem-brane, thickening with age,17,18 and viable LECs liningthe inner surface of the lens equator and the anteriorlens capsule. The basement membrane is predomin-antly composed of the extracellular matrix moleculescollagen IV, laminin, nidogen and heparan sulfateproteoglycans.19,20 The lens is enclosed by the lenscapsule, representing a barrier against bacterial andviral infections.21,22 Further, the lens capsule transmitsthe accommodative forces from the zonula fibers tothe lens.23 Since the lens is avascular, lens capsulepermeability for small nutrient molecules and metab-olites is essential for the viability of the LECs withinthe capsule. So, permeability for electrolytes, water,sugars, amino acids, and, to a lesser extent, forhemoglobin was shown for different species.24–27
To investigate lens capsule permeability we haveused human capsulorhexis specimens from the anter-ior lens capsule from routine cataract surgeries whichwere readily available and fluorescent dextrans withdifferent molecular weights were chosen, since theyare soluble in water and easy to quantify. An inverserelation of permeability with molecular weight wasdemonstrated (Figure 2B) similar to the inverserelation of diffusivity with molecular weight.28,29
It was also assessed that the molecular weight cutoffof decellularized lens capsules of 166� 82 kDa(Figure 2B) is in good agreement with a molecularweight cutoff of 150� 40 kDa, as determined for thedenatured human lens capsule.29 In addition to apermeability of 3–150 kDa dextrans, Danysh et al.30
found a limited diffusion of the 250 kDa dextran intothe lens capsule and assumed that the observeddiffusion is exclusively caused by the small sizeddextran byproducts. The 250 kDa dextran moleculecorresponds to an average Stokes radius of 10.9 nm.Further, maximum diameters of superficial openingsof a native mouse lens of near 25 nm were found byhelium ion microscopy, but the effective pore size wasestimated to be smaller due to overlap of different lenscapsule layers.30 According to literature31 and sup-pliers data, the molecular weights of the fluorescent
molecules, 0.376, 10, 40, 70 and 150 kDa correspond toStokes radii of 0.45, 2.3, 4.5, 6.0 and 8.5 nm, respect-ively. A linear regression of the Stokes radii andthe apparent permeability coefficients is similar toFigure 2B, and a cutoff Stokes radius of 9.7� 4.5 nmcan be calculated, supporting further the results ofDanysh et al.30 As the dextrans are valuable for thedetermination of the pore size of the capsular bag,modification of charge in a molecule may consider-ably alter diffusion behavior in the lens capsule as hasbeen demonstrated convincingly.30 When polymersfor an injectable lens are chosen, their chemicalproperties have to be taken into account, and stillthe question has to be adressed if there will be aleakage of injected lens refilling material from thecapsular bag. After a rapid polymerization minuteamounts of prepolymer might diffuse through thecapsular bag, but the concentrations are expected tobe too low to negatively affect adjacent tissue.
In contrast to high molecular weight dextransantiproliferative drugs such as AM and MTX withlow molecular weight easily pass the human anteriorlens capsule. A linear regression of the time-depen-dent increase of the AM and MTX concentrations inthe acceptor compartment resulted in crossing LOQtimes of 15.25� 2.5 h for AM and 8.41� 0.90 h forMTX (Table 2, Equations 3 and 4). However, at a shortincubation period of 0.5 h no permeation could bedetected (Figures 3 and 4, Table 2). This observation isin accordance with absence of undesirable side effectsin rabbit eyes 4 months postoperatively with a 5 minintraoperative application of sodium hyaluronatehydrogels containing 1�10�5 mol/l AM/MTX.9
However, the anterior pole of the lens capsule is 5–10 times thicker than the posterior pole.16 Assuming alinear relationship between caspule thickness andpermeation time, the crossing LOQ times at theposterior lens capsule can be estimated to 2 h forAM and one hour for MTX which is well above a5 min instillation period. A drug treatment constitut-ing a perioperative rinsing of the interior of thecapsular bag for 5 min represents a safe drug admin-istration time frame. Residual amounts in the capsularbag will be too low to cause damage to adjacent tissueor the retina, because within the short rinsing time of5 min, only minute amounts will permeate the lenscapsule. However, the capsular bag should be intactbeyond the mini-rhexis, and great care should betaken when applying the drugs to prevent spillingduring surgery.
In summary, we used human anterior lenscapsules to determine apparent permeability coeffi-cients of sodium fluorescein and differentlysized fluorescent dextrans calculating a molecularsize cutoff of 166� 82 kDa from these data.Further, the apparent permeability coefficients foractinomycin D (0.71� 0.02 mm/s) and methotrexate(0.80� 0.13 mm/s) intended as antiproliferative drugs
6 C. Kastner et al.
Current Eye Research
Cur
r E
ye R
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
11/1
3Fo
r pe
rson
al u
se o
nly.

for secondary cataract prevention were ascertained.We conclude that prepolymers for an injectable lensare required to polymerize rapidly to be retainedinside of the capsular bag. Further, the antiprolifera-tive drugs should be applied within a time frame offive minutes in such a way that cells adjacent to thecapsular bag will not be damaged.
ACKNOWLEDGEMENTS
The authors thank Thom Terwee and Volkmar Senzfor their helpful notes and suggestions. We arefurthermore grateful to Thomas Langer for his sup-port during the HPLC measurements, Peter Enzenrossand Jens Grossmann for developing the diffusionchambers, and to Andrea Rohde, Martina Nerger,Gabriele Karsten, and Babette Hummel for experttechnical assistance.
DECLARATION OF INTEREST
This work was funded by a grant from the GermanFederal Ministry of Education and Research withinthe REMEDIS consortium ‘‘Hohere Lebensqualitatdurch neuartige Mikroimplantate’’ (FKZ: 03IS2081).
The authors report no conflict of interest. Theauthors alone are responsible for the content andwriting of the paper.
REFERENCES
1. Tabin G, Chen M, Espandar L. Cataract surgery for thedeveloping world. Curr Opin Ophthalmol 2008;19:55–59.
2. Brian G, Taylor H. Cataract blindness – challenges for the21st century. Bull World Health Organ 2001;79:249–256.
3. Krag S, Andreassen TT. Mechanical properties of thehuman lens capsule. Prog Retin Eye Res 2003;22:749–767.
4. Nishi Y, Mireskandari K, Khaw P, Findl O. Lens refilling torestore accommodation. J Cataract Refract Surg 2009;35:374–382.
5. Koopmans SA, Terwee T, Glasser A, Wendt M, VilupuruAS, van Kooten TG, et al. Accommodative lens refilling inrhesus monkeys. Invest Ophthalmol Vis Sci 2006;47:2976–2984.
6. Hao X, Jeffery JL, Wilkie JS, Meijs GF, Clayton AB, WatlingJD, et al. Functionalised polysiloxanes as injectable, in situcurable accommodating intraocular lenses. Biomaterials2010;31:8153–8163.
7. Crowston JG, Healey PR, Hopley C, Neilson G, MilvertonEJ, Maloof A. Water-mediated lysis of lens epithelial cellsattached to lens capsule. J Cataract Refract Surg 2004;30:1102–1106.
8. Auffarth GU, Rabsilber TM, Reuland AJ. Neue Methodender Nachstarpravention. Ophthalmologe 2005;102:579–586.
9. Sternberg K, Terwee T, Stachs O, Guthoff R, Lobler M,Schmitz KP. Drug-induced secondary cataract prevention:experimental ex vivo and in vivo results with disulfiram,
methotrexate and actinomycin D. Ophthalmic Res 2010;44:225–236.
10. Stachs O, Langner S, Terwee T, Sternberg K, Martin H,Schmitz KP, et al. In vivo 7.1 T magnetic resonance imagingto assess the lens geometry in rabbit eyes 3 years after lens-refilling surgery. J Cataract Refract Surg 2011;37:749–757.
11. Koopmans SA, Terwee T, van Kooten TG. Prevention ofcapsular opacification after accommodative lens refillingsurgery in rabbits. Biomaterials 2011;32:5743–5755.
12. Sobell HM. Actinomycin and DNA transcription. Proc NatlAcad Sci USA 1985;82:5328–5331.
13. Chan ESL, Cronstein BN. Molecular action of methotrexatein inflammatory diseases. Arthritis Res 2002;4:266–273.
14. Schoenwald RD, Huang HS. Corneal penetration behaviorof beta-blocking agents I: physiochemical factors. J PharmSci 1983;72:1266–1272.
15. Kim JH, Green K, Martinez M, Paton D. Solute permeabil-ity of the corneal endothelium and Descemet’s membrane.Exp Eye Res 1971;12:231–238.
16. Danysh BP, Duncan MK. The lens capsule. Exp Eye Res2009;88:151–164.
17. Fisher RF. Elastic constants of the human lens capsule.J Physiol (Lond) 1969;201:1–19.
18. Barraquer RI, Michael R, Abreu R, Lamarca J, Tresserra F.Human lens capsule thickness as a function of age andlocation along the sagittal lens perimeter. InvestOphthalmol Vis Sci 2006;47:2053–2060.
19. Cammarata PR, Cantu-Crouch D, Oakford L, Morrill A.Macromolecular organization of bovine lens capsule.Tissue Cell 1986;18:83–97.
20. Rossi M, Morita H, Sormunen R, Airenne S, Kreivi M,Wang L, et al. Heparan sulfate chains of perlecan areindispensable in the lens capsule but not in the kidney.EMBO J 2003;22:236–245.
21. Beyer TL, Vogler G, Sharma D, O’Donnell FE. Protectivebarrier effect of the posterior lens capsule in exogenousbacterial endophthalmitis – an experimental primate study.Invest Ophthalmol Vis Sci 1984;25:108–112.
22. Karkinen-Jaaskelainen M, Saxen L, Vaheri A, Leinikki P.Rubella cataract in vitro: sensitive period of the developinghuman lens. J Exp Med 1975;141:1238–1248.
23. Koretz JF, Handelman GH. Model of the accommodativemechanism in the human eye. Vision Res 1982;22:917–927.
24. Friedenwald JS. The permeability of the lens capsule towater, dextrose, and other sugars. Trans Am OphthalmolSoc 1930;28:195–211.
25. Friedenwald JS. Permeability of the lens capsule withspecial reference to the etiology of senile cataract. ArchOphthalmol 1930;3:182–193.
26. Fels IG. Permeability of the lens capsule to tryptophan.Exp Eye Res 1971;12:51–59.
27. Hockwin O, Poonawalla N, Noll E, Licht W.Durchlassigkeit der isolierten Rinderlinsenkapsel furAminosauren und wasserlosliche Eiweibe. Albrecht VonGraefes Arch Klin Exp Ophthalmol 1973;188:175–181.
28. Lebrun L, Junter GA. Diffusion of dextran through micro-porous membrane filters. J Membr Sci 1994;88:253–261.
29. Lee CJ, Vroom JA, Fishman HA, Bent SF. Determination ofhuman lens capsule permeability and its feasibility as areplacement for Bruch’s membrane. Biomaterials 2006;27:1670–1678.
30. Danysh BP, Patel TP, Czymmek KJ, Edwards DA, Wang L,Pande J, et al. Characterizing molecular diffusion in thelens capsule. Matrix Biol 2010;29:228–236.
31. Montermini D, Winlove CP, Michel C. Effects of perfusionrate on permeability of frog and rat mesentericmicrovessels to sodium fluorescein. J Physiol 2002;543:959–975.
Anterior Lens Capsule Permeability 7
! 2013 Informa Healthcare USA, Inc.
Cur
r E
ye R
es D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
11/1
3Fo
r pe
rson
al u
se o
nly.


![MAX VISION Tablet: A Perfect Formulation to Support the ... · posterior pole. The lens capsule may be involved with the higher anterior curvature than posterior of the lens.[3] Lens](https://img.pdfslide.net/doc/110x75/5ffd3e0819710b5969179155/max-vision-tablet-a-perfect-formulation-to-support-the-posterior-pole-the.jpg)