Embed Size (px)
Citation preview
P E R S A T U A N P E R U B A T A N M A L A Y S I A • M A L A Y S I A N M E D I C A L A S S O C I A T I O N
PP 1285/02/2013 (031328)PP 1285/02/2013 (031328)
April 2018Berita MMA Vol. 48 No. 4
(For Members Only)
OSH
Vulnerability
of Young
Workers
World Day for Safety and
Health at Work
28 April 2018

beritaMMA Vol.48 • April 2018
MMA EXECUTIVE COMMITTEE2017/18
PresidentDr Ravindran R Naidufl [email protected]
Immediate Past PresidentDr John Chew Chee [email protected]
President – ElectDr Mohamed Namazie [email protected]
Honorary General SecretaryDr Koh Kar [email protected]
Honorary General TreasurerDr Rajan [email protected]
Honorary Deputy SecretariesDr Vasu Pillai [email protected]
Dr Muruga Raj [email protected]
SCHOMOS ChairmanDr Arvindran [email protected]
PPS ChairmanDr Thirunavukarasu [email protected]
Editorial Board 2017/18
Honorary AdvisorDato’ Pahlawan Dr R. [email protected]
EditorAssoc Prof Dr Jayakumar [email protected]
Ex-Offi cioDr Koh Kar [email protected]
Editorial Board MembersDr Gayathri K. [email protected]
Dr Juliet [email protected]
Dr Edwin Ho Jim [email protected]
Major (Dr) Eugene Tan Choon [email protected]
Publication AssistantMs Nor Iza [email protected]
The views, opinions and commentaries expressed in the Berita MMA (MMA News) do not necessarily refl ect those of the Editorial Board, MMA Council, MMA President nor VersaComm, unless expressly stated. No part of this publication may be reproduced without the permission of the Malaysian Medical Association. Facts contained herewith are believed to be true as of the date that it is published. All content, materials, and intellectual property rights are owned and provided for by Malaysian Medical Association and its members. VersaComm makes no guarantees or representations whatsoever regarding the information contained herewith including the truth of content, accuracy, safety, or the absence of infringement of rights of other parties. In no circumstances shall VersaComm be held liable for the contents, materials, advertisements contained in this publication. VersaComm has no infl uence over the contents of Berita MMA and all opinions, statements and representations made do not in any manner refl ect that of VersaComm or its employees.
Published byMalaysian Medical Association4th Floor, MMA House, 124, Jalan Pahang, 53000 Kuala LumpurTel: +603 4042 0617; Fax: +603 4041 8187, 4041 9929Email: [email protected] / [email protected]: https://www.facebook.com/malaysianmedicalassociationWebsite: www.mma.org.my© Copyright ReservedISSN 0216-7140 PP 1285/02/2013 (031328) MITA (P) 123/1/91
Consultant
12-A, Jalan PJS 8/4, Mentari Plaza, Bandar Sunway,46150 Petaling Jaya, Selangor Darul Ehsan.Tel: +603 5632 3301; Fax: +603 5638 9909Email: [email protected]
PrinterAtlas Cetak (M) Sdn BhdNo. 2, Persiaran Industri, Bandar Sri Damansara52200 Kuala Lumpur. Tel: 03-6273 3333
ContentsEditorial 4
EXCOPresident’s Message 6
From the Desk of the HGS 10
MMA Convention 2018Tentative Programme 16
Registration Form 18
In the SpotlightGeneration Safe and Healthy 20
SCHOMOS Updates 22
PPSMMA Updates 24
SMMAMSLight of Love Run 2018 26
General White Coat: The End of a Generation? 28
Cries of the Rohingyas 31
Strength in Numbers 33
Humour 34
PersonalityHumble Beginnings to CEO 36
Branch News
MMA-PADU Futsal Games 2018 42
Journey to Hanoi & Halong Bay Cruise 44
Mark Your Diary 46
This Berita MMA is a publication only for the members of the Malaysian Medical Association. The Malaysian Medical Association does not warrant, represent or endorse the accuracy, reliability or completeness of the contents of Berita MMA (including but not limited to the advertisements published therein). Under no circumstances shall the Malaysian Medical Association be liable for any loss, damage, liability or expense incurred or suffered in respect of the advertisements and/or from the use of the contents in the Berita MMA. Reliance upon any such advice, opinions, statements, advertisements or other information shall be at the readers’ own risk and the advertisers are responsible for ensuring the material submitted for inclusion in Berita MMA complies with all legal requirements. The advice, opinions, statements and other information does not necessarily refl ect those of the Malaysian Medical Association. Nothing in this disclaimer will exclude or limit any warranty implied by law that it would be unlawful to exclude or limit.
OSH
Vulnerability
of Young
Workers
World Day for Safety and
Health at Work
28 April 2018
beritaMMA Vol.48 • April 2018
editorial4
What is your Occupation?
28 April 2018 is the World Day for Safety and Health at Work with the theme “Occupational Safety and Health Vulnerability of Young
Workers’. The campaign aims to reduce work-related disease and accidents.
I vividly recall attending to a case of occupational lead poisoning in my early years. A 15-year-old boy was referred by a Surgeon to an Occupational Medicine (OM) clinic with a history of lethargy, nausea, vomiting, abdominal pain and constipation of one year duration. His doctors could not pinpoint his cause of abdominal pain earlier even after numerous lengthy tests and referrals elsewhere. The patient underwent an appendicectomy few months prior to the current referral to the OM clinic. However, his symptoms remained unresolved.
A thorough history revealed two pertinent points not elucidated from the patient. The occupational history revealed the child was a school dropout who was working at his father’s backyard lead battery recycle workshop. It was assumed earlier he was not working as he was a child. The second important aspect was the nature of his job was not explored. A visit to his workplace as part of a worksite health risk assessment visit unravelled a deplorable workplace with probable excess exposure of lead. His blood lead level was 70µg/dL which was much beyond the safe threshold limit. He subsequently recovered with chelation therapy.
The learning points from this case are not to assume children do not work, and secondly a good as well as a meticulous occupational history often remains the cornerstone to clinch a diagnosis of an occupational disease. We need to take cognisance that occupational or work-related diseases often have long latent periods. Mesotheliomas has a latent period of 30 years from the time of occupational exposure to asbestos to development of signs and symptoms. Job history has to be obtained in detail, covering the present and all previous jobs, part-time jobs, probable hazards as well as the safety and health precautions at the workplaces. Lastly, a worksite visit by an Occupational Physician is of paramount importance to aid in the diagnosis. This is one classic case I often share with my students who are posted to the clinics.
Historically, the famous composer Beethoven is speculated to have died of lead poisoning. A four-year analysis of his hair (apparently snipped after his death at the age of 56 years) in 1827 revealed lead levels almost 100 times more than what is found in people today. Interestingly, during the mediaeval era in Europe, there was a practice of adulterating wines of modest vintage with lead.
Occupational and environmental exposure to lead is another alarming problem. It is probably under-diagnosed and remains at the tip of the iceberg phenomena. A recent study published at the Lancet Public Health indicated persistent low-level exposure to lead over decades to the population is statistically linked to some 400,000 premature deaths in the United States each year. The study reviewed two decades of health data of more than 14,000 adults in the United States of America. The study concluded that nearly 30% of all deaths due to cardiovascular diseases like myocardial infarction and strokes could be attributable to lead exposure. Over-exposure to inorganic lead affects numerous systems in the body.
Workers who are involved in battery manufacturing, chemical industry, construction, lead mining, lead smelting, pigment manufacturing, plastics industry, pottery and printing have possible increase risk of exposure to lead.
Responsibility for Health and Safety rest with both employers and employees; neither can be alone. Employers need to have the mindset that investing
in Health and Safety for their employees is good business for their
organisat ions. It is commonly s a i d , i f t h e employer does not ca re , the employee w i l l not care either for their organisation.
Better work safe than be sorry!
Assoc Prof Dr Jayakumar GurusamyEditor
good bus
nenth
Betha
Source – Malay Mail (13 March 2018)Source – New Strait Times
(19 October 2000)


beritaMMA Vol.48 • April 2018
exco • president’s message6
What Can MMA Do For You? Dr Ravindran R Naidu
President fl [email protected]
This is the topic I was given to present at the recent 8th Annual Scientifi c Meeting & Regional Update 2018 in Kuantan, Pahang on 18 March 2018. This
reminded me of the late John F. Kennedy a former President of the United States of America who once said, “Ask not what the country can do for you, but what you can do for the country”. What an appropriate statement. Can I say the same for MMA as to “What you can do for MMA?” I am sure the answer will be a NO. I have been asked on numerous occasions on “What can MMA do for me?” Why should I join the MMA and what are the benefi ts for ME?
For over fi ve decades since the Malaysian Medical Association embarked on a path for the medical profession, the main objectives of the Association have always been to maintain a high standard of Medical Ethics and Conduct, to promote social, cultural and
professional activities among those in the medical profession, to enlighten and direct opinions on health problems and to express the views of the profession to Government and other bodies. Finally, to maintain the highest standard of healthcare for the people of this country. After all, MMA is an association by doctors for doctors.
The history and growth of the MMA is an impressive one, it is indeed an honour for me to talk about the aptitude of MMA and what exactly MMA can do for you.
1. Striving for the General Practitioners (GPs) and Specialists in Malaysia
We at MMA strongly feel that the GPs and specialists need more representation to voice the diverse and innumerable issues faced by the profession.
Meeting with MPS on 12 March 2018 Meeting JK CPD Technical for Non Specialist on 13 March 2018
Meeting with KSU on 14 March 2018

beritaMMA Vol.48 • April 2018
exco • president’s message8
i. Third Party Administrators Issue The biggest concern that has been constantly
and repeatedly voiced out by the GPs and Specialists about TPAs over the years is the lack of, or no regulatory framework, for operation of TPAs. This has become crucial since it involves major ethical facets of doctors in their healthcare service deliveries to patients. For the past 23 years, we have seen many Ministers of Health and Directors General of Health walking the corridors of power of the MOH, nevertheless there has been no importance or urgency given to resolve the countless legitimate issues faced between the GPs and the TPAs.
There are 7000 GP clinics in the country and the time has come for the Ministry Of Health and Malaysian Medical Council to not only listen to the dissatisfaction and discontentment of GPs, but to be responsive by taking the obligatory action in resolving the issue.
MMA sincerely expects the MOH, as well as the MMC, to be fi rm in deciding for short- and long-term solutions on this issue. In view of that, MMA has been striving hard to address the TPA issues and convey the grievances of the GPs to the MOH and MMC, for response to be instantaneous and prompt.
ii. Premise License The implementation of premise license fees
on 1 September 2016 by DBKL on all private clinics was included. The doctors were very unhappy with this new imposition as they are already registered under the Private Healthcare Facilities and Services Act 586 and this fee by DBKL is viewed as redundant and a way to make money.
In reciprocation, MMA in its constant fi ght for the welfare of the GPs, has urged the DBKL through letters, press statements and meetings to waive the premise license fee for medical clinics. MMA is deeply concerned that over-regulation and overlapping of regulations might increase the cost of practice and inconvenient to the doctors, hence violating the aims of increasing productivity and safeguarding consumers. As of today, the matter has not been resolved but rest assured that MMA will fi ght to the extremes.
2. CPD Administrator
We understand that the implementation of the amended Medical Regulations 2017 and Medical Act 2012 by the MMC has created a huge impact and confusion among the medical practitioners particularly on the mandatory 20 CPD points, to be accompanied with indemnity insurance
for the renewal of Annual Practicing Certifi cate (APC). MMA is actively working on facilitating the doctors on CPD matters and to ensure that all the processes will be made easier instead of burdening the profession.
MMA, as one of the CPD administrators, has Tan Sri Dato’ Dr Abu Bakar Suleiman as our CPD Advisor for the MMA-CPD Committee. An interesting fact is that MMA has developed a Mobile Apps for CPD providers and all registered medical practitioners be it members or non-members for their ease and convenience. This is part of our “Corporate Social Responsibility” to the medical fraternity. Our goal is to automate the system so that registered participants can check their accrued CPD points easily and in real time. The capabilities of this Mobile Apps include the following:
i Registration of non-members
ii. Registration of CPD providers
iii. Process applications for accreditation of educational events by providers
iv. Record attendance instantaneously during educational activities (swipe profi le QR Code)
We will go electronic. However, for those whose requirement needs to be manual, it will be made available by the MMA.
MMA is also in the process of linking ADHOC CPD to the Mobile Apps which is meant for overseas conferences and online CPD modules only.
Doctors can also apply for Medical Indemnity Insurance through MMA by joining either the Medical Protection Society (MPS) or Medical Practitioners Indemnity (MPI).
This service is provided to both members and non-members without any fee. MMA is doing this for the medical profession. If there is concern on how the members are getting less privileges as compared to non-members, fear not and rest assured, we shall give back to our members in some other form. We will never forsake the exclusive privileges and extensive range of benefi ts that a member of this esteemed organisation can obtain.
Based on our outs tand ing records and achievements, you are assured that MMA’s credibility as a CPD administrator is in a position of unchallenged supremacy.
3. HELPDOC
MMA is constantly working on helping you even in the darkest of time without being judgemental. On the 26 August 2017, MMA launched a support group for doctors called ‘HELPDOC’, to act as

beritaMMA Vol.48 • April 2018
a safety net for many issues faced by doctors in Malaysia. This is intended to enable doctors to air their grievances especially those who feel harassed at work and being bullied at work. This phone service is accessible to doctors at all levels of seniority. The response that we received so far has been exceedingly acceptable.
Please contact 03-4041 1140 for this service.
4. Safeguarding the Future of the Medical Graduates
MMA’s anguish for the new medical graduates is immense. The waiting time for employment as House-Offi cers is still at 9-12 months now. We hope that there will be good news soon so that the waiting time can be reduced.
MMA is also very concerned about the situation with surplus doctors and the uncertainty that awaits them. Our young medical graduates are facing placement problems. It is a fact that we have an oversupply of medical graduates and insuffi cient training positions in our hospitals. We believe that entry requirements for medical universities and colleges need to be improved.
Apart from continuously trying to seek solutions for the above concerns, MMA has established a program called ‘Mentor-Mentee.’
This Mentor-Mentee Program serves as a platform for doctors waiting for housemanship to keep abreast with their medical knowledge through attachment to a clinic near their homes. We are in the process of acquiring all names for the mentors and mentees and this will be done on a voluntary basis and no payment is involved for both mentor and mentee.
There is a curriculum being developed to act as guidelines for the training, running up to 20 weeks at a time.
MMA is very concerned about the future and ever-growing problems faced by young doctors. It is the responsibility of the senior doctors to show them the way to improve and safeguard the standard of ethics and professionalism. This is what we do to strive towards maintaining the standards of excellence in medical practice. Further, we are looking at ways and possibilities these young doctors may be employed if they have no interest in clinical medicine. In January 2021, when the fi rst batch of contract doctors complete their contract, there will be doctors who may not be employed by the Ministry of Health. We need to show them the path for other options that may be available.
5. Protect our doctors
MMA is keen in protecting doctors from any abuse by public, patients or any other parties. We can agree to the fact that usage of the social media now has become massive and with many cases that went viral on social media. It is easy to tell that the public seem to view social media as a platform to express their dissatisfaction towards several issues. Social media is often used as a medium to voice whatever thoughts they have in mind pertaining to any issue, however it does not necessarily depict the truth or lead to a positive outcome. The same situation goes to the patient-doctor relationship whereby doctors are often exposed to social media abuse.
MMA has always been concerned when doctors are abused wrongly and would take necessary action to prevent the issue from getting worse. However, this does not mean that MMA is protecting doctors blindly, patients do have their right to complain if they have been mistreated or misled by the doctors. There are several grievous mechanisms for patients to channel their complaints including the Ethics Committee of the MMA, and the MOH and MMC.
6. Privileges
On the light side, MMA has negotiated with several organisations for exclusive discounts and deals for members. Our travel partner AIR ASIA is available for all members. Please contact MMA for your user name and password to avail yourself of this privilege. Many hotels have agreed to give our MMA members special room rates. Other privileges include travel discounts with travel agencies, purchase of motor vehicles, insurance for life and general, and many more.
Conclusion
MMA is always concerned about producing the best quality of doctors in Malaysia. As of now, the Association has been providing services and programs that are undeniably benefi cial for the betterment of the profession. We are aware that the expectation for the association will go higher from time to time and that is why MMA has continuously embarked on services and programmes that we believe are instrumental in safeguarding the present and future of the medical profession in Malaysia.
What else can MMA do for you?????

beritaMMA Vol.48 • April 2018
exco • hgs10
REMINDER: The 58th Annual General Meeting of the Malaysian Medical Association will be held from 4.30pm, Friday, 29 June 2018 at Royale Chulan Kuala Lumpur.
Dear Members,
It is a disappointment that we still have brickbats hurled at the Malaysian Medical Association (MMA) over the facilitation of the MMC-CPD Grading System. The MMA CPD Committee has been labelled as little Napoleons in the way Continuous Professional Development (CPD) Providers are being registered as well as the way CPD points are being allocated to CPD events.
Do note that the MMA is only facilitating the MMC-CPD Grading System for the Malaysian Medical Council (MMC) based on the guidelines provided by the MMC. Any dissatisfaction with the guidelines may please be taken up with the MMC.
However, based on the complaints received, it was noted that the MMC-CPD System Grading Scoring Schedule for certain events may have been wrongly interpreted, thus resulting in the wrong number of points being allocated and also sometimes being rejected. If any provider or medical practitioner feels that the CPD Committee may have erred in their judgement, do feel free to contact us for assistance. As this system is still in its infancy, there is still much to learn and we need to do this together. It won’t do anyone any good by going on social media to voice out your discontentment with harsh words.
Dr Koh Kar ChaiHon. General Secretary [email protected]@gmail.com
From the Desk of theHon. General Secretary
Mr Harikannan, Ms Ratna, Dr KC Koh, Dato Dr Tharmaseelan and Dr John Chew at the Risk Management Seminar in Kuching
With Dr Kalwinder Singh Khaira, Chairman, Sarawak Branch
Continuous Training Improves Effi ciency: MMA Secretariat Staff in IT Workshop

beritaMMA Vol.48 • April 2018
It is rather hurtful when our own members resort to such actions but it is doubly so when we see non-members doing it, particularly so when the MMA has reached out to them by offering the MMA Mobile Application for CPD points allocation for their use without any fi nancial obligations. The MMA has spent a considerable sum of money on the development of its software and mobile application and has allowed its use by non-members for free. The MMA is still incurring a high cost every month in terms of money spent on maintenance and regular updates of the software and the number of backbreaking man hours endured by our staff members as well as committee members (who, by the way, are all volunteers of our association) in going through all the CPD applications which have to be approved.
Positive FeedbackI normally do not share praises nor bouquets from the medical fraternity as we are all here as volunteers who feel that we can contribute to the association and medical fraternity; not to collect well deserved praises. But I will share some of them here, some of which are slightly edited for clarity.
“Online is linked with MMA App, I tried it last month. After passing 1 module the points appeared immediately on MMA App, thanks MMA. Our unsung heroes.”
“MMA has put in many efforts to represent us doctors. All the EXCO and committee members have been ‘brave’ to voice out opinions and statements concerning the welfare of doctors to the government, even for the benefits of those Doctors who have chosen NOT to be members of MMA. I salute them for spending so much personal time and efforts to fi ght for us, esp during the income tax fi asco. Now with the CPD thingy, MMA has come up with the app that is convenient for us to use and for FREE. FREE even to those who chose not to support MMA or other doctors in Malaysia by joining as members. Talk is easy and cheap. Putting in effort to make things work is not.”
“I just want to say MILLIONS Of THANKS to all MMA leaders, nation and state and branch for all that you have done, are doing and will do for me and us who are members BUT also gracefully extending the effects of your countless hours of meetings and negotiation to ALL Doctors (yes, ALL, including non-members in Malaysia).”
“THANKS MMA. Now MMA Apps has been upgraded to refl ect the CPD events that we had attended or engaged. And the CPD points from MIMS-CPD was being updated in the MMA Apps at lightning speed. Yesterday I did the MIMS-CPD, today early am I already seen the CPD points being added to the MMA Apps. However, there is still a let-down, that there is no indication of whether those CPDs belongs to what specialties.”
“I am happy with the MMA CPD so far; the app works fi ne. There were teething problems but so far good progress. MMA has my thumb up.”
“Yes... extremely happy. I totally agree MMC should continue vetting which section or speakers can be recognised as “expert” in their fi eld. And I have to apologise BUT everyone can give feedback or comment but please don’t give unjustifi ed and unnecessary complaint especially for Non MMA members using the MMA CPD-platform. Give the team time.”
The MMA accepts constructive criticisms. In fact it thrives and improves itself from the feedback it receives from members. Without communication from grass-root members, the MMA would have just gone on its own lofty trajectory without serving any purpose. But with members who are willing to come o ut and contribute their services willingly, and for those who are not able to do so but still chip in with their ever ready support in whatever way possible, our association will grow to be one which we can claim as an association ever ready to represent the medical fraternity of Malaysia.
Medical IndemnityGoing from the need of CPD points for the renewal of the Annual Practising Certifi cates to the necessity of having Medical Indemnity coverage – there are still a large number of doctors who feel that since they are practicing “safe” medicine, there is no real need for such indemnity coverage. Please don’t assume so. Throughout my years of practice, I have encountered near “misses” and I know of doctors who were thankful for such coverage and those who regretted that they did not buy in to this idea of medical indemnity cover when they ran into trouble.
Having a medical indemnity coverage protects the registered medical practitioner and also provides for the unfortunate patient and kin should the unthinkable occur. However, there is no need to fret over this as it will soon be compulsory to have medical indemnity coverage if you are to practice medicine in Malaysia.
The MMA acts for two medical indemnity schemes in Malaysia, namely the Medical Protection Society (MPS) of which many of us are familiar with on account of the many years that they have been in Malaysia, and the relatively younger Medical Protection Indemnity (MPI) which is rather proactive at the moment. Which one to choose is the often asked question, for which I have no reply except to say that you need to study both in detail to see which has the benefi ts that you are looking for. Both are equally good, and I will advise you to spend some time on the prospectus to understand what each scheme is offering you.
Both MPS and Jardine Lloyd Thompson (which manages MPI) have been conducting risk management seminars all over the country for the benefi t of our doctors, and in the process, also marketing themselves and their products. Do attend these seminars to arm yourself with risk management skills. Participation is free.

The MMA was visited by representatives of MPS, Mr Steve White, Senior International Project Manager and Mr Adrian Brown, Member Operations Manager-International on 12 March 2018 for a discussion on MPS operational matters. MMA Exco represented by Dr Ravinaidu, Dr Namazie and myself voiced our members’ concerns for them to bring back to MPS for discussion.
Running for CharityThe SCHOMOS Section of MMA Sarawak held its Charity Health Run 2.0 recently on 18 March 2018 at Kuching. Participation stood at 1,500 runners. The ever
enthusiastic YB Senator Prof Dr Sim Kui Hian’s (Minister for Local Government and Housing, Sarawak and Past MMA Sarawak Chairman) participation at this event, along with Datuk Haji Abang Abdul Wahap bin Haji Abang Julai, Datuk Bandar, Dewan Bandaraya Kuching Utara further lightened up the event for MMA Sarawak.
Mention is made of Sarawak Branch and its active SCHOMOS Section for its successful hosting of this run. It was a joy to be able to participate in this event and thanks for making me feel at home during my visits to Sarawak.
Looking lively in the early morning darknessYB Senator Prof Dr Sim and Datuk Haji Abang Abdul Wahap at the starting grid.
exco • hgs12
Dr Saravanan A.Santhirarajan
Honorary Secretary 2017/18MMA Wilayah
D S
National MMA Convention & Scientific Congress 2018
In view of the rebranding of the MMA AGM to the National MMA Convention And Scientifi c Congress 2018,the Organising Committee have come up with a Lunch Symposium Talk on 28 June 2018 and a full day programme on CPD talks on 29
June 2018 to keep members abreast on the latest medical advances.
The programme for the National MMA Convention and Scientifi c Congress 2018 has been prepared in good faith and it is as follows.
The organising committee advises members keen to attend the National MMA Convention and Scientifi c Congress 2018 to register for the convention by logging on to www.mmaconvention.org.my.
Members and non-member spouses who are keen to take part in the sports programme and tour programmes are also encouraged to log on to the above website and register online for the programmes.
beritaMMA Vol.48 • April 2018
mma convention 201814
Tentative Programme
Thursday, 28 June 2018
6.30am – 12.00pm Healthy Lifestyle ProgrammeSports Programme – Golf, Badminton, TennisTour Programme
Kelab Darul Ehsan
12.00pm – 1.00pm Registration Registration Area, Lobby
1.00pm – 2.00pm Sponsored Lunch Symposium Tamingsari 1 & 2
2.00pm – 4.00pm SCHOMOS AGMPPS AGM
Tamingsari 1Tamingsari 2
2.30pm – 4.00pm Healthy Vegetarian Cooking Demo Taman Mahsuri
4.00pm – 4.30pm Tea Break
4.30pm – 5.00pm Opening Ceremony of Trade Exhibition Lobby
5.00pm – 7.00pm Hospitality Suite 13th Floor
7.30pm – 11.00pm Welcome Reception – “Ragga Jungle”Informal Night Dinner (PPS & SCHOMOS Night)
Taman Mahsuri
* Subject to changes
beritaMMA Vol.48 • April 2018
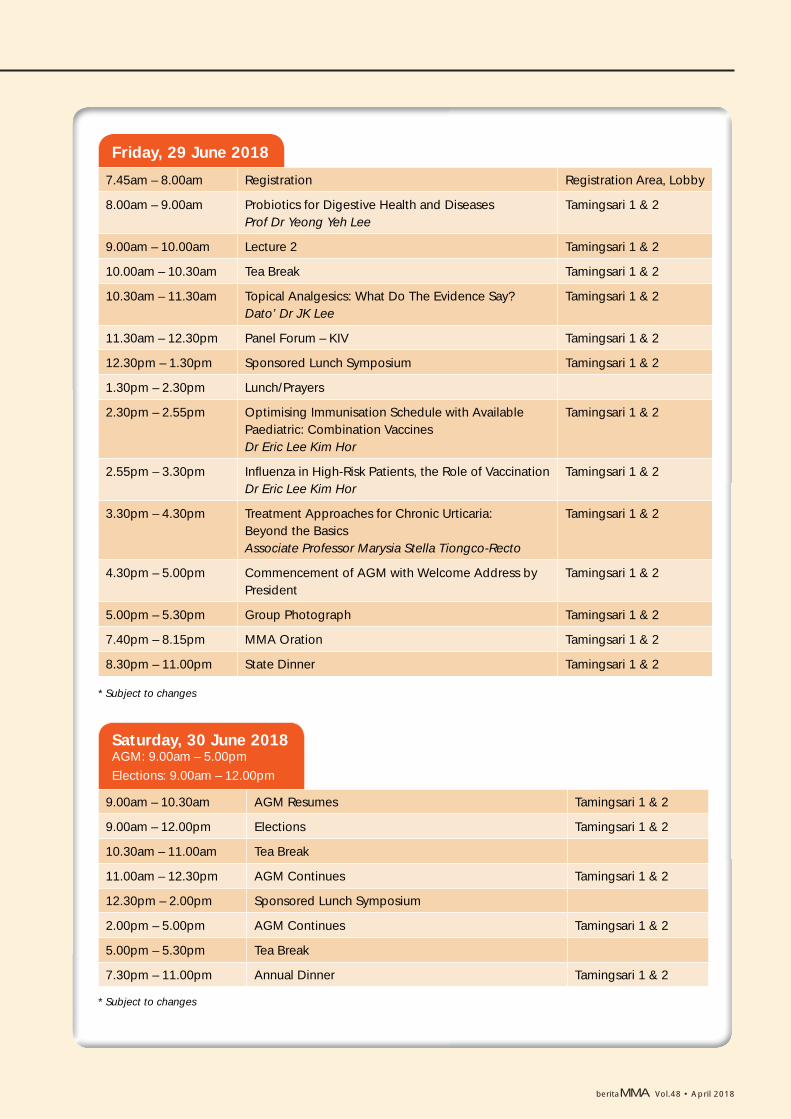
Friday, 29 June 2018
7.45am – 8.00am Registration Registration Area, Lobby
8.00am – 9.00am Probiotics for Digestive Health and DiseasesProf Dr Yeong Yeh Lee
Tamingsari 1 & 2
9.00am – 10.00am Lecture 2 Tamingsari 1 & 2
10.00am – 10.30am Tea Break Tamingsari 1 & 2
10.30am – 11.30am Topical Analgesics: What Do The Evidence Say?Dato’ Dr JK Lee
Tamingsari 1 & 2
11.30am – 12.30pm Panel Forum – KIV Tamingsari 1 & 2
12.30pm – 1.30pm Sponsored Lunch Symposium Tamingsari 1 & 2
1.30pm – 2.30pm Lunch/Prayers
2.30pm – 2.55pm Optimising Immunisation Schedule with Available Paediatric: Combination VaccinesDr Eric Lee Kim Hor
Tamingsari 1 & 2
2.55pm – 3.30pm Infl uenza in High-Risk Patients, the Role of VaccinationDr Eric Lee Kim Hor
Tamingsari 1 & 2
3.30pm – 4.30pm Treatment Approaches for Chronic Urticaria:Beyond the BasicsAssociate Professor Marysia Stella Tiongco-Recto
Tamingsari 1 & 2
4.30pm – 5.00pm Commencement of AGM with Welcome Address by President
Tamingsari 1 & 2
5.00pm – 5.30pm Group Photograph Tamingsari 1 & 2
7.40pm – 8.15pm MMA Oration Tamingsari 1 & 2
8.30pm – 11.00pm State Dinner Tamingsari 1 & 2
* Subject to changes
Saturday, 30 June 2018 AGM: 9.00am – 5.00pm Elections: 9.00am – 12.00pm
9.00am – 10.30am AGM Resumes Tamingsari 1 & 2
9.00am – 12.00pm Elections Tamingsari 1 & 2
10.30am – 11.00am Tea Break
11.00am – 12.30pm AGM Continues Tamingsari 1 & 2
12.30pm – 2.00pm Sponsored Lunch Symposium
2.00pm – 5.00pm AGM Continues Tamingsari 1 & 2
5.00pm – 5.30pm Tea Break
7.30pm – 11.00pm Annual Dinner Tamingsari 1 & 2
* Subject to changes

beritaMMA Vol.48 • April 2018
mma convention 201816

beritaMMA Vol.48 • April 2018
beritaMMA Vol.48 • April 2018
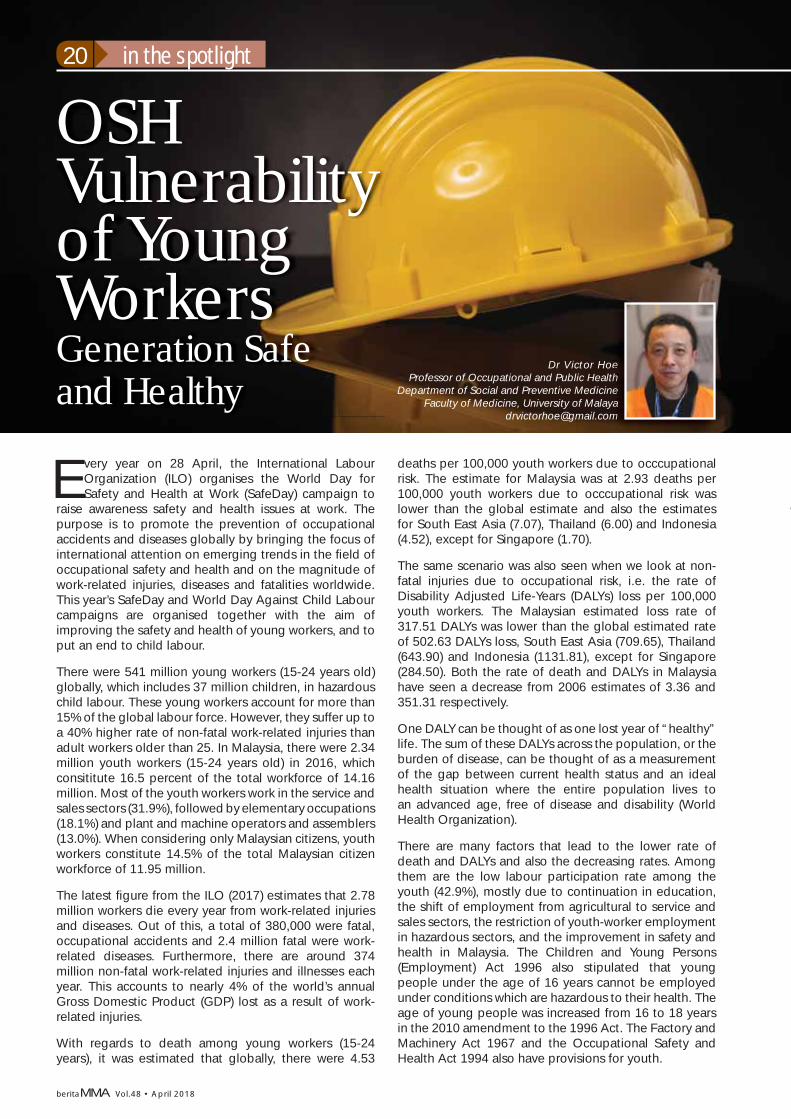
in the spotlight20
OSH Vulnerability of Young WorkersGeneration Safe and Healthy
Every year on 28 April, the International Labour Organization (ILO) organises the World Day for Safety and Health at Work (SafeDay) campaign to
raise awareness safety and health issues at work. The purpose is to promote the prevention of occupational accidents and diseases globally by bringing the focus of international attention on emerging trends in the fi eld of occupational safety and health and on the magnitude of work-related injuries, diseases and fatalities worldwide. This year’s SafeDay and World Day Against Child Labour campaigns are organised together with the aim of improving the safety and health of young workers, and to put an end to child labour.
There were 541 million young workers (15-24 years old) globally, which includes 37 million children, in hazardous child labour. These young workers account for more than 15% of the global labour force. However, they suffer up to a 40% higher rate of non-fatal work-related injuries than adult workers older than 25. In Malaysia, there were 2.34 million youth workers (15-24 years old) in 2016, which consititute 16.5 percent of the total workforce of 14.16 million. Most of the youth workers work in the service and sales sectors (31.9%), followed by elementary occupations (18.1%) and plant and machine operators and assemblers (13.0%). When considering only Malaysian citizens, youth workers constitute 14.5% of the total Malaysian citizen workforce of 11.95 million.
The latest fi gure from the ILO (2017) estimates that 2.78 million workers die every year from work-related injuries and diseases. Out of this, a total of 380,000 were fatal, occupational accidents and 2.4 million fatal were work-related diseases. Furthermore, there are around 374 million non-fatal work-related injuries and illnesses each year. This accounts to nearly 4% of the world’s annual Gross Domestic Product (GDP) lost as a result of work-related injuries.
With regards to death among young workers (15-24 years), it was estimated that globally, there were 4.53
deaths per 100,000 youth workers due to occcupational risk. The estimate for Malaysia was at 2.93 deaths per 100,000 youth workers due to occcupational risk was lower than the global estimate and also the estimates for South East Asia (7.07), Thailand (6.00) and Indonesia (4.52), except for Singapore (1.70).
The same scenario was also seen when we look at non-fatal injuries due to occupational risk, i.e. the rate of Disability Adjusted Life-Years (DALYs) loss per 100,000 youth workers. The Malaysian estimated loss rate of 317.51 DALYs was lower than the global estimated rate of 502.63 DALYs loss, South East Asia (709.65), Thailand (643.90) and Indonesia (1131.81), except for Singapore (284.50). Both the rate of death and DALYs in Malaysia have seen a decrease from 2006 estimates of 3.36 and 351.31 respectively.
One DALY can be thought of as one lost year of “healthy” life. The sum of these DALYs across the population, or the burden of disease, can be thought of as a measurement of the gap between current health status and an ideal health situation where the entire population lives to an advanced age, free of disease and disability (World Health Organization).
There are many factors that lead to the lower rate of death and DALYs and also the decreasing rates. Among them are the low labour participation rate among the youth (42.9%), mostly due to continuation in education, the shift of employment from agricultural to service and sales sectors, the restriction of youth-worker employment in hazardous sectors, and the improvement in safety and health in Malaysia. The Children and Young Persons (Employment) Act 1996 also stipulated that young people under the age of 16 years cannot be employed under conditions which are hazardous to their health. The age of young people was increased from 16 to 18 years in the 2010 amendment to the 1996 Act. The Factory and Machinery Act 1967 and the Occupational Safety and Health Act 1994 also have provisions for youth.
Dr Victor HoeProfessor of Occupational and Public Health
Department of Social and Preventive MedicineFaculty of Medicine, University of Malaya
oeeeeethhhhneeeeeyaaaaammmmm

beritaMMA Vol.48 • April 2018
The SafeDay campaign of the ILO aims for safe and secure working environments for all workers and seeks an ending to all forms of child labour based on the Sustainable Development Goal (SDG) targets of 8.8 and 8.7. To achieve these, a concerted and integrated approach to eliminating child labour and promoting a culture of prevention on occupational safety health (OSH) should be promoted for the benefi t of the next generation of the global workforce. The reason for the focus on youth is due to the many factors that increase youth vulnerability to occupational safety and health (OSH) risks. Among them are their physical and psychological stage of development, lack of work experience, lack of training, limited awareness of work-related hazards and a lack of bargaining power that can lead young workers to accept dangerous tasks or jobs with poor working conditions. Youth also have different risk perception and risk-taking behaviour which may lead them to engage in more risk-taking activities, and this will affect the OSH risks.
Although the situation in Malaysia is good, we still need improve it further to reduce the fatal and non-fatal injuries among the youth while also focusing on promoting a culture of prevention on occupational safety health. However, improvement in the OSH among youth cannot just be focused on issues at the workplace, but at
the overall risk that youth are engaged, e.g. substance abuse, dangerous driving, and risky sexual behaviour. This is particular important with regards to commuting accidents, in the Social Security Organisation reports, the number of commuting accidents have increased from 17,000 in 2016 to 31,000 in 2016, although during the same period, the number of industrial accident has decreased from 40,000 to 35,000.
Researchers in the universities, Ministry of Health and non-governmental organisations, are working together in engaging youths to promote a safer and more productive future for them. Among them were the Malaysian Care for Adolescent Project (http://myadolescenthealth.org), Malaysian Clearinghouse Centre for Adolescent Health (http://myadolescenthealth.org/MyCCAdH/), HIPSTAR (Hidup Sihat Tanpa Rokok) workshop, No-Cotine Club, as well as the Smoking Cessation Organising, Planning and Execution Training (SCOPE) programme.
The 2018 SafeDay campaign highlights the critical importance of addressing these challenges and improving safety and health for young workers, not only to promote decent youth employment, but also to link these efforts to combat hazardous, and all other forms of child labour.
CongratulationsMalaysian Medical Association
congratulates
Dato’ Sri Dr Mohammed Azman bin Dato’ Aziz Mohammed (Life Member, Wilayah Branch)
on the award ofDarjah Sri Sultan Ahmad Shah Pahang (SSAP)
byDuli Yang Maha Mulia Paduka Seri Sultan Pahang
Sultan Ahmad Shah
on the occasion of the 87th Birthday of His Royal Highness
on16 December 2017
beritaMMA Vol.48 • April 2018
schomos22
SCHOMOS Updates Dr Velkanthan Muniandy
Hon. Assistant Secretary [email protected]
The fi rst quarter of 2018 has arrived and SCHOMOS can gladly say that we have kick started this period with enthusiasm.
SCHOMOS was invited to be a part of the ‘Program Pemukiman Pemantapan Kepimpinan Kementerian Kesihatan Malaysia’ that was held at Kem Bina Negara Ulu Sepri, Negeri Sembilan from 8-9 February 2018. SCHOMOS was represented by Dr Velkanthan, the Honorary Deputy Assistant Secretary of SCHOMOS and Dr Mitesh, SCHOMOS Chairman Melaka Branch.
Around 120 participants from various societies and agencies attended this course. The two-day event was kicked off with several talks by renowned speakers. A few of the points highlighted were: serve the government with honesty and pride, not to spread fake news, do not victimise or be a victim of fi ctitious information and all facts should be research thoroughly before being shared with others.
It was followed by a speech by the Deputy Health Minister, YBhg Dato’ Seri Dr Hilmi Yahaya. The participants were then divided into several groups and presented important topics related to health and our nation, which included topics such as ‘Managing the Well Being of the People’, ‘Social Media Perception and Misuses’, ‘Ensuring Social Network Sustainability’, ‘Erosion of Trust in a Multiracial Community’, and ‘Loyalty to the State and the King; Role and Contribution of Civil Servants and Healthcare in Malaysia’. The fi nale of the event was the speech by the Director General of MOH, YBhg Dato’ Seri Dr Chen Chaw Min.
The next event attended by SCHOMOS was the PHOENIX 2.0 programme. Phoenix 2.0 is the second edition of the Pre-Housemanship Essential Nourishing Intensive Exclusive Course organised by Universiti Kebangsaan Malaysia (UKM) from 24-25 February 2018.
Dr Ravi Naidu, MMA President, and Dr Arvindran, SCHOMOS Chairman, were the representatives for SCHOMOS. Befi tting his experience as ex-House Offi cer Supervisor, Dr Arvin gave an interesting, as well as intellectual talk, regarding Housemanship Training in Malaysia. This was followed by an interactive forum regarding Contract House Offi cers. The session was
lively and many queries that the House Offi cers had raised were addressed.
Other contents of the programme included ‘ABG Interpretation’, ‘Dengue Crash Course’ and ‘Why Should You Join the MMA’. An overview of the housemanship postings was also given. Overall the event was a great success and we received positive reviews. We would also like to express our heartfelt gratitude to Dr Fikri B Ujang, Deputy Director, Medical Development Division, Medical Professional Development Section, MOH on the excellent opening speech.
Our next big event is just ahead of us. The second SCHOMOS Cybersports Tournament is coming. To
Cybersports Poster

beritaMMA Vol.48 • April 2018
jog your memory, the fi rst SCHOMOS Cybersports Tournament was successfully held on 22 April 2017. It involved 80 doctors from around Malaysia coming together to battle it out in the game Dota 2. This year, we are pleased to inform you that the SCHOMOS Cybersports Tournament 2018 will be taking place on 28 April 2018 at the Orange E- Sports Stadium at Setapak, Kuala Lumpur.
Competitive computer gaming requires planning, strategy, good reflexes and most importantly teamwork to defeat the opponent team. Lately, cybersports has been gaining popularity among young doctors in Malaysia. SCHOMOS & MMA views this positively and encourages these young gamer-doctors as these games not only instils teamwork but also inculcates organisational skills, promotes multitasking and enhances mental agility which can be incorporated during daily routines in the hospital to increase productivity and effi ciency.
The aim of organising this event is to encourage doctors to be all-rounders with robust mental and physical health, and promote cybersports among doctors. It also acts as a reminder for our doctors to stay in touch with all areas of fi tness amidst their busy working schedule as well as attracts young doctors from all over the country to unite under the umbrella of MMA as members.
The game which will be played is Dota 2. Entries are open to 16 teams each consisting of fi ve players.
However, only medical doctors, medical graduates and medical students are eligible to join.
The tournament will be played in a single elimination format. The fi rst round, quarterfi nals, semi-fi nals will be played as a best-of-one game while the grand fi nal will be played as a best of 3 games. The game mode will be Captain’s Mode.
We would like to invite all MMA members to join this illustrious tournament.
To join, please scan the QR code below and fi ll up the relevant information. Tournament Rules and Regulations are listed there as well.
berberberberberbb iitattatataitaaaitatatatttaattaataMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMM AA A VVVolVVVVoVoVoolVolVolVVVoVoll.4.48.48484488884888888.48484848488488.44.4....44444 ••••••••••••••••••• AprAprAprAAAprApApAprAprAprAprAprAApAAAprAprpAprAprAprAApAAAAApAprApAprAAAA rprAprAAprAAApAprAprApAApAAAppAAAAAAAppAAAAAAAAAprApppppp iiliiilllliiilliliilll iill l 220120120201202 120222222220 8888
KSU Program Pemukiman
Phoenix 2.0

beritaMMA Vol.48 • April 2018
ppsmma24
PPSMMA Updates
MMA had a meeting with ETIQA and Maybank, regarding their recent circular to provider clinics. Another meeting was held with
them at Ministry of Health (MOH). The summary of meeting follows. ETIQA does not restrict the patient or staff from seeing the GP doctor for follow up monthly, bi-monthly, quarterly or as per the doctor’s discretion based on the patient’s condition. However, upon request, GP’s can provide the patient with the prescription. The prescription is only valid for two other refi lls, i.e. at the end of three months, a staff must go back to see a doctor. Hence they should see a doctor four times yearly for their chronic health management.
FaceTime prescription is not allowed, e.g. Doctor on call, eDoctor. Consultation RM35 is agreed pending the gazettement of the Revised 7th Fee Schedule. A referral fees & prescription fees of RM10-15 each will be charged if the patient requires prescription or referrals .If patient requires both, i.e. consultation and prescription, the total fees will be RM50.
ETIQA is moving towards an online submission with payment within 14 days and GPs’ may accord walk-in rate if the payment is prompt with less hassle. Insurer and TPAs will use the MOH formulary for the guidance
on medicines covered. Generics have gone through many generations and their effi cacy is equivalent to patented drugs. These should be prescribed by doctors in long term management, instead of patented drugs. More meetings will be held for a seamless working relationship between the GP Clinic Providers & ETIQA.
Third Party Administrators (TPAs)The 12th meeting with the TPAs was held on 13 Feb 2018. We have fi nalised the draft terms of reference for the Grievance Mechanism. The Grievance Mechanism will comprise of 10 members, fi ve from doctors and another fi ve from the TPAs. The Grievance Mechanism committee will be a platform for the general practitioners and TPAs to bring any issues faced by both parties.
We have also proposed to have a representative from the Medical Practice Division of MOH to be an observer initially. We have moved on to the fi nal phase of this meeting, focusing on contracts and agreements. We have listed all the trade and regulatory issues that need to be sorted out in the contract. We would also like to thank the Director General of Health, Datuk Dr Noor Hisham Abdullah for issuing two circulars, fi rst
Dr Thirunavukarasu Rajoo PPSMMA Chairman
o n
m
Meeting chaired by Datuk Seri Dr Jeyaindran

beritaMMA Vol.48 • April 2018
on the compliance to the PHFSA and its regulations by both the Registered Medical Practitioners and Third Party Administrators when they go into any contracts and the secondly on the specifi cs of fee splitting.
MMA is also reaching out to the stakeholders, namely the employers via Malaysian Employers Federation, to create awareness on various acts and regulations that govern the profession and its facility. This is to make them to understand when their patients seek treatment at PHFSA registered facilities and also when they go into a contract with any TPAs. We have done this in Wilayah Persekutuan, Selangor, and Negeri Sembilan. Will be covering all the other states gradually.
FOMEMA-Income can be declared under companyMMA received numerous requests from members to seek clarifi cation when the income derived from FOMEMA was told to be declared under individual rather than company by the Inland Revenue Department (IRD), especially for clinics operated under private limited or partnership. Some of the clinics operate as a private limited entity, with doctors being employed to run the clinic.
FOMEMA pays directly to the doctors as per the contractual agreement with FOMEMA and the private limited registered clinics. The money is subsequently reimbursed by the doctors to the private registered clinics. However, the doctor is penalised for not declaring the income as he/she assumes that he/she didn’t make any earnings from FOMEMA.
This letter from the Inland Revenue Board is to clarify that the income can be declared under the Sdn Bhd or the company if the FOMEMA registered doctor had offered his/her services through the Sdn Bhd or the Company. Kindly write and email to fi nance and MSPD unit of FOMEMA for any changes in payment for clinics operated under Sdn Bhd.
Sub Committee on Private Specialists Affairs Some of the immediate issues being handled are lopsided contracts that some of the private specialist may have gone into, which may contravene the code of professional conducts. This refers to the unethical practice of arm-twisting the doctors to give discounts from their regulated professional fees.
There are also issues whereby treatment is delayed or denied because of a lack of clear protocols when admitting patients with medical cards at the emergency department. The committee will be having a meeting with the Association of Private Hospitals, Malaysia (APHM). The same will be highlighted to the Medical Practice Division, MOH.
Revised 7th Fee ScheduleThe documents are currently at the Malaysian Productivity Corporation undergoing the due process. The President has met YBMK and Datuk Seri KSU, on this matter. We will be meeting with Datuk Seri KSU Dr Chan Chaw Min, on 14 March 2018 and awaiting another appointment to present to YBMK before the document is sent to Attorney General’s Chambers.
Meeting chaired by Dr Vasu Pillai

beritaMMA Vol.48 • April 2018
The sky was clear, light blue painted the horizon. Not a sign of one or two, big or small, white fl uffy clouds, fl oating across the sky, looking like sulci
and gyri of the cerebral cortex. And the wind, the wind is like nothing but calm air. There were enthusiastic participants, chattering around with each other at the wide platform at MAEPS, Serdang,
It was the second walkathon organised by the student representative council (SRC) of Perdana University, together with the Society of MMA for Medical Students (SMMAMS) known as the “Light of Love Run 2018”. This event was held after the great response from the cancer themed walk “Walk-and-Roll-athon 2016” in which a total of more than RM5k was donated to the National Cancer Society Malaysia (NCSM). Again, aimed for charity, this meaningful event was intended to create awareness of mental health among medical students and the public. As such, donations were made to Malaysian Mental Health Association (MMHA).
According to estimates up till last year, four out of every 10 Malaysians will fall victim to some form of mental health issue in the course of their lives and psychiatrists believe that the numbers will continue to rise. According to the National Health and Morbidity Survey 2015, the prevalence of mental health problems among adults increased from 10.7% in 1996, to 11.2% in 2006, to 29.2% in 2015. Shockingly, the prevalence in our capital, Kuala Lumpur, is 39.8%. Mental illness is expected to be the second biggest health problem affecting Malaysians after heart diseases by 2020. Hence, we should not underestimate the situation by taking issues like depression, bipolar disorder and other mental health issues lightly. This is not something that only attacks the poor, weak and lonely. It happens to anyone and the World Bank had predicted that 340 million people will suffer from depression by 2020.
Malaysian Mental Health Association (MMHA) is a non-profi t voluntary organisation formed in 1967, managed by a group of mental health professionals and community leaders. With the aim to promote mental health, raise standard of treatment, prevention and research in mental health, and at the same time, to safeguard the welfare of psychiatric patients and to
smmams26
Light of Love Run 2018 Hian Chuan Kai
Hon. Assistant Secretary SMMAMSPerdana [email protected]
SMMAMS Committee (L-R): Hian Chuan Kai, Langkeas, Magendran, Kavinesh Kupusamy

beritaMMA Vol.48 • April 2018
support to their family members, MMHA praovides community service, rehabilitation program, and caregiver and peer support groups.
LOL Run started off in the morning with a fi tness warm-up session at 8.00 am. Participants had a wonderful time stretching their body while following the tempo of the Pop music. After an opening speech given by the Vice Chancellor of Perdana University, Professor Dr Zabidi Azhar bin Mohd Hussin and the director of the event, Ms Kasturi Subramaniam, the run fi nally began.
The MAEPS exhibition park which is one of the largest exhibition park and showground resides on a 130 hectares land belonging to the Malaysian Research and Development Institute (MARDI). Along the 5km trail, the whole landscape was bathed in the warm glow of the rising sun. Palm trees swayed gently in the breeze in the warm tropical sunshine along the Perdana University campus. The pond beside MAEPS Bistro was bathed in a golden hue by the gentle sunlight and the water was as clear as crystal. The breath-taking scenery captivated every participant.
Booths were setup by volunteers with the aim of creating awareness and raising funds for mental health. SMMAMS had a booth near the entrance of the event hall and some medical students were enthusiastic enough to join as a member, while others were enquiring about the upcoming conferences and interesting events by MMA or SMMAMS.
The run came to an end when the sun climbed towards its zenith. Wonderful prizes were given away to the top 10 fi nishers of the run. Before the end of the event, everyone was reminded by an administrative staff of MMHA to understand and acknowledge patients with mental disability who require love, care and support.
LOL Run Starting and Finishing Point
Participants with Prof Zabidi (dressed in black)
Standalone established Medical & Gastro Centre, JB
or Physician with GI interest
beritaMMA Vol.48 • April 2018
general28
Nostalgia is one word that describes the white coat as it is the most recognisable garment that represents our noble profession. It is still vivid among many of us today who began our careers with the white coat. The white coat was simply meant
to protect one’s clothing beneath and act as a uniform. It was easy to clean and robust, easily withstanding repeated washing and external abuse of the clinical environment. It also had handy pockets for stationaries and one large enough for our extended ears, the stethoscope! Let’s take a walk and reminisce about ‘our’ white coat.
Early YearsPrior to the ‘White Coat’ era, medical students and trainee doctors used to wear black lab coats during cadaveric dissection. Black coats were also popular in laboratories. The black coats were simply meant to respect the dead. It was only in the 1920s that the white coat became part of the doctor’s uniform. In modern times, it symbolises the most distinctive uniform of practitioners and witnessing its popularity remains in the centre of our practice.
In came the 19th century and out went the art of mysticism in treating patients [1]. Doctors were seen as ‘men or women of science’, thus carrying the responsibility of a scientist with the emergence of research and subsequently, evidence-based medicine. Doctors became respected professionals. More doctors shifted their offi ces to the dungeons of the white-walled lab, looking for the power of medicine and a scientifi c explanation to the mysteries of the human body. Hence, what can better represent a scientist other than a white laboratory coat?
A Symbol of SterilityThe end of the 18th century saw the use of antiseptics to reduce surgical site infections. English surgeon Sir Joseph Lister who served at the Glasgow Royal Infi rmary pioneered
White Coat The End of a Generation?
Donning a white coat for the fi rst time is often an unforgettable start to one’s journey as a practitioner of the trade.
Dr Hardip Singh GendehMember, MMA [email protected]
Co-authorsDr Sanjiv Rampal
Life MemberMMA Wilayah
Datuk Dr Kuljit SinghLife Member
MMA Wilayah
D H di Si h G d

beritaMMA Vol.48 • April 2018
the idea of sterile surgery with an antiseptic (carbolic acid/phenol) for surgical instruments sterilisation and wound cleaning. The Father of Modern Surgery’s discovery led to a reduction in post-operative infections and undoubtedly, there was a push for medicine and clinical practice to be sterile.
The white coat, on the other hand, was pure, clean and represented none other than sterility. Atul Gawande in the New Yorker wrote on surgeons, “They traded in their black coats for pristine laboratory whites, refashioned their operating rooms to achieve the exacting sterility of a bacteriological lab, and embraced anatomic precision over speed” [2,3].
Some even claimed the earlier coats to be a shade of beige which transformed to white with time, fi fty shades of white perhaps? [4].
The White Coat CeremonyMany medical schools in the United States of America (USA) and several others around the globe have adopted the white coat ceremony to don a white coat and recite the good old Hippocratic Oath. Those involved are medical students either transitioning from pre-clinical to clinical years of training or those graduating from medical school. Dental schools and several allied healthcare professionals have also taken up the custom. Call it a ritual, a tradition or a rite of passage to becoming a healthcare professional, it is certainly unique and something to remember among those getting ‘cloaked’ [5].
A Popular UniformThe white coat has since become a uniform for doctors, at least for hospital or institutional-based practices. TV shows and cartoons often represent a doctor with his or her white coat and a stethoscope. As a child, many of us will picture a doctor or dentist as the one with the white coat and the large syringe! No doubt, the white coat was the representation of modern medicine.
Many white coats bear the physicians or surgeons name badge, making it easier for identifi cation. Patients knew whom to stop and direct their questions to, surely the chap or chappette in the white cloak often seen scuffi ng away in the corridors! It serves as a mechanism for patient safety too. Recent times have seen white coats being used by quacks to mimic a practitioner. Hence it would be advised to have the name of the institution or hospital embroidered onto the white coat to make it more diffi cult to duplicate.
ConvenienceA busy call may render some of us to be consigned to the oblivion of using our messy and creased shirts. Thankfully, a white coat does come in handy during a bad wardrobe day. In the past white coats were available as long coats (to just above the knee) and short coats (down to waistline), allowing senior doctors to be distinguished from their junior counterparts and/or medical students.
However, in Malaysia, our tropical climate of high temperatures and humidity makes wearing a white coat
almost impossible, especially the long sleeved coats. Furthermore, these coats were popularised in the West, where temperatures are relatively lower with bearable humidity. As many hospitals are not fully air-conditioned, the poor doctor will be sweltering in the heat of his or her white coat even if it is short sleeved. To make matters worse, junior doctors, and almost all medical students, are made to wear neckties with white coats (which is again a culture of the West), that we feel is just plain impractical.
Nosocomial Infection Transmission White coats have shown to harbour bacterial contaminants such as diphtheroids, staphylococcus, and gram-negative bacilli. More interestingly, Uneke at el in 2010 reported that although bacterial contaminants were present in 91.3% (94 out of 103 patients) of hospital acute care setting, contaminants were less among white coats that were washed daily, less than one year old and among doctors whom only wore them in a clinical setting compared between non-clinical and clinical setting. However, what is clearly evident is that white coats do harbor bacteria. What was once thought to promote sterility is not actually sterile, at least at the microscopic level [6].
The Department of Health in the United Kingdom devised a set of good clinical practices, which brought to an end of white coats. Among some of the highlighted alteration of practice to the then norm are shown in the box below [BMJ 2008;337:a938,7]. NHS hospitals were strict to adherence of these practices and conducted regular audits on compliance with the new guidelines upon its introduction.
1. Wear short-sleeved shirts and blouses without the white coat
2. Although there is no evidence to suggest infection risk, it is advised to change into and out of uniform while at work and leaving work respectively
3. Change uniforms immediately when soiled or contaminated
4. Tie long hair back, off the collar
5. Avoid wearing hand or wrist jewelry as it may harbour micro organisms
6. Wear soft-soled (to prevent noise) and closed-toe footwear (to get protection from spillage)
7. Neck ties (bow-ties exempted) not to be worn during direct clinical care
Bare Below the Elbows The NHS subsequently adopted the Bare Below Elbows (BBE) policy which prevents the use of white coats, neckties (if worn they have to be tucked in), long-sleeved clothing (long sleeves had to be rolled above the elbow), no wristwatches (watches were worn on belts and subsequently made pinned body watches popular again), no hand or wrist jewelleries (one wedding band exempted) and no hanging name tags on lanyards

� Preferably 3 years working experience as a specialist
� Registered with MMC & NSR
1. Nephrologist2. Rheumatologist3. Urologist4. Neurologist
5. O&G6. Paediatrician7. Physician8. Other Specialties
Come join us for a rewarding career!Interested applicants are invited to submit their detailed resume to
[email protected]: +6012-393 7131 Tel No: +082-234 466 Fax: +082-232 259
Timberland Medical Centre, 5164-5165, Block 16 KCLD, Taman Timberland, 2 ½ Mile, Rock Road, 93250 Kuching, Sarawak
Timberland Medical Centre is an 85-bed multi-disciplinary private hospital in Kuching, Sarawak that opened in 1994. As one of the most established hospitals in the city with a large customer base of local and Indonesian patients, we seek to enhance our facilities and services to remain the market leader. Strategically located, our expansion plans include building a new hospital as well as recruitment of new specialist doctors in this exciting phase of our journey.
We invite doctors of all specialties to submit their resume; especially
RESIDENT CONSULTANTS
� Possess valid APC � Possess Medical Indemnity
Insurance
general30
beritaMMA Vol.48 • April 2018
(tags were worn on trousers or skirts). The explanation given is that these clothing and associates may come in contact with the patient and surroundings during clinical examination, thus resulting in them being a vector for the transmission of infection. More so since accessories like watches, ties and name tags do not see the inside of a laundry machine.
It was an unpopular move at fi rst especially among senior healthcare professionals who were used to the good old days. However, many complied. Many healthcare professionals in their well-pressed suits had to remove their jackets, remove their cuffs, tuck in their neck ties or scarfs and reattach their wristwatches to their trousers or skirts during wad rounds and clinics. Not surprisingly, male doctors were hoarding the gentlemen’s store for bow ties instead!
BBE had its critics. Burger at al in 2011 reported that adequate hand-washing with the correct technique and not BBE resulted in a reduction in the bacterial count on hands [8]. However, this doesn’t dismiss the fact that clothing exposed to patients still harbors bacterial contaminations and may be a vector to bacterial spread due to direct contact with patient’s skin or clothing.
As a result, many healthcare institutions in Malaysia and the USA especially acute care settings such as the intensive care unit have adopted similar policies to curb Hospital Associated Infections (HAIs).
Is Blue the New White?Scrubs that are often termed theatre blue are sanitary clothing worn by healthcare professionals. Originally started off as clothes for surgeons and operation theatre staff, its use has extended to healthcare providers (including primary care settings) in the community in recent years.
It is comfortable, easily cleaned when soiled and relatively cheaper to manufacture. Many healthcare institutions have adopted disposable scrubs to ensure
a one-time use only. In the USA, scrubs are often worn for inpatient clinical settings, whilst the white coat and business clothing are worn in an outpatient setting. This, in the opinion of the authors, would be an ideal solution for practice in Malaysian shores and the future look of medical practice in Malaysia.
The Fate of the White CoatEverything good has to come to an end. There may be a time where we have to consider hanging up our white coats for good. There should be clear evidence-based guidelines on white coats and accessories in hospital-based practice in Malaysia. If white coats are to be worn, there needs to be clear guidelines on how and when we ought to wear them to curb the spread of HAIs. We are still very much a scientifi c healer without the additional external white apparel.
References
[1] White Coat. Available at: https://en.wikipedia.org/wiki/White_coat
[2] It’s time for doctors to hang up the white coats for good. The Conversation. Available at: https://theconversation.com/its-time-for-doctors-to-hang-up-the-white-coats-for-good-47536
[3] Slow Ideas. The New Yorker. Available at: https://www.newyorker.com/magazine/2013/07/29/slow-ideas
[4] Why Do Doctors Wear White Coats? http://www.slate.com/articles/news_and_politics/explainer/2009/06/why_do_doctors_wear_white_coats.html
[5] Veatch RM. White coat ceremonies: a second opinion. J Med Ethics. 2002;28(1):5-9.
[6] Uneke CJ, Ijeoma PA. The potential for nosocomial infection transmission by white coats used by physicians in Nigeria: implications for improved patient-safety initiatives. World Health Popul. 2010;11(3):44-54.
[7] What should doctors wear?BMJ 2008; 337 doi: https://doi.org/10.1136/bmj.a938 (Published 24 September 2008)
[8] Burger A, Wijewardena C, Clayson S, Greatorex RA. Bare below elbows: does this policy affect handwashing effi cacy and reduce bacterial colonisation? Ann R Coll Surg Engl. 2011;93:13–16.
An example of the NHS bare below the elbows policy

general 31
beritaMMA Vol.48 • April 2018
I had the opportunity to be the team’s psychiatrist for the Malaysian Field Hospital in Cox’s Bazar, Bangladesh from 7 Jan – 5 Feb 2018. Thanks to the Ministry of Health Malaysia, my experience in serving this humanitarian aid mission was worthwhile,
self-refl ective and worth sharing, in particular on the Rohingyas’ cases that I had seen in the outpatient clinic.
Our arrival in Cox’s Bazar’s airport was smooth as the local plane touched the short runway. The moment we disembarked, we were greeted by the cool wind that caressed our faces on a sunny day. The town was quite a view to behold, suffi ced to say it was both an eye-opener and nausea-inducing at the same time.
Yet for me, the journey to the Malaysian Field Hospital was a memorable one, one that triggered memories of sombre accounts that the persecuted Rohingya minority in Myanmar suffered. As we sat on the coach en route to the fi eld hospital, the sun rays were peering through the windows. My face was basking in the morning sun but my mind lingered on the plight of Rohingya patients.
A Disfi gured Image
An adolescent’s father was apparently arrested by the Myanmar military offi cers and no one knew the father’s exact whereabouts. Twenty-four days later, the villagers stumbled upon the father’s dead body that was left abandoned on a hillside. It was a gruesome sight to behold and the stench of the corpse was unbearable, yet they managed to wrap the body with a plastic sheet and carry all the way back to his house.
When the daughter saw the remains of her beloved dead father, her misery was inconsolable. Her last memory of her father’s face was of a disfi gured face covered by the scalp scraped off from the back of his head, exposing the blood-stained tissues that overlaid the skull. She was incessantly haunted by this traumatic sight, which warped her sense of reality, causing it to slowly disintegrate. She gradually became psychotic and for years, her woe was never treated.
Though the whole journey to the hospital was almost an hour long, it was a twenty-minute scenic view of long smooth sandy beach with crescent-shaped boats berthed onshore and swaying coconut trees. From afar, the waves came crashing and rippled off as it reached the shorelines. However, a heart that has been crushed would be diffi cult to ‘ripple off’.
Crashed Hearts
A helpless Rohingya father could only hug his dying son in anguish as he suffered from fatal gunshot wounds to his chest. His son was on the way to the mosque when he was ambushed by the Myanmar military and shot repeatedly in his chest. The father could not seek immediate medical treatment for him as they were hiding in a shelter from the patrolling military troops, who would shoot any Rohingya on sight. He died the next morning and was buried in a hurried manner before the army came for another assault.
A relative was aghast at the injury his cousin sustained to his left hip; the bone was exposed after the military bombed the area. He survived the blast and crawled for 200 yards while screaming for help. His heart kept pounding as he was determined to live. He was newly married and ready to start a family. Sadly, his heart literally crashed as it yielded to too much blood loss. He died on the makeshift stretcher in his attempt to reach the Bangladesh border.
Cries of the Rohingyas
Dr Kenny OngNeuropsychiatrist
Hospital Kuala LumpurMember, MMA Selangor [email protected]
D K O
beritaMMA Vol.48 • April 2018
general32
As the journey continued and we passed through the villages, the ride became bumpy due to the uneven road surfaces. The coach driver wove in and out of traffi c in order to overtake slow vehicles while evading on-coming ones. From the windows, we could see the small-scaled paddy fi elds, thin-looking cows chewing the scanty grass on the roadside and greenhouse-like shelters made of dried coconut palm fronds erected to protect the growing betel leaf plants.
The Rohingyas’ live in houses with thatched roofs that are easily razed and destroyed in minutes. Villages were put to the torch by grenades or with kerosene and many helpless men, women, children and babies were massacred.
Merciless
A neighbour watched in great terror as a group of young women were raped and tied-up while elderly men were locked in shelters and all of them were burned alive. The Myanmar armed forces would torture the Rohingyas of all ages.
The Rohingyas were forced to stand in the paddy fi eld (or assume a squatting position with their hands folded in between the inner thighs while touching their ears) in the heat of the sun and instructed not to move. Any movement would result in death by being shot, even babies who cried were immediately shot and thrown into the burning fl ames from the houses.
Bodies were buried in mass graves or dumped into the paddy fi elds or river banks. The remaining villages were bulldozed and turned into fl at desolate lands.
The fi eld hospital was in close proximity to the last security checkpoint, beyond which in the hills were the Rohingya camps. The hospital coach, recognized by the uniformed offi cers would pass through the post with much ease. One could see the enforcement of tight security to ensure safety in the country.
Desperate Escape
The Rohingyas fl ed desperately from the brutal mass killing and heartless inhumane torture. Although they endeavoured to cross the border to Bangladesh, the journey itself was precarious and a test of great endurance to survive.
The physical and mental agony was tremendous to bear as they struggled to traverse the hills and jungles for days. They had to contend with muddy ground caused by rainy days, and without adequate food, some ate tree leaves from the surrounding jungle and drank murky water from the paddy fi elds or canals.
Some of the elderly and babies died from hunger or succumbed to medical illnesses and some sacrifi ced themselves to protect others from military ambushes.
Most of them also tried crossing by sea or river on boats, usually with some form of monetary payment to the boat owner. A villager who was at the river bank witnessed three boats, each carrying 30-40 people onboard, bombed by a helicopter. The boats were blown to pieces and all perished at once. A young Rohingya man frantically swam across the Bay of Bengal as he could not afford to pay the boat fare and the military was chasing after him. For more than an hour he struggled to swim and kept afl oat, only to witness more than 1000 others drown from sheer muscle cramps and fatigue.
The exodus was a search for hope but a despair for some. On reaching the fi eld hospital, I walked with a heavy heart towards the gate entrance. Seeing cases in the outpatient clinic had painted a picture, a mental picture of the Rohingyas’ plight that became clearly much gloomier and darker to behold. We treated their aches and pains but their agony ran deeper into their emotions. Their physical complaints manifested in their mental distress.
Sorrows I could only listen with great sorrow, their tears tugging at my heartstrings. Medication could ease the pain for a while but the scars may remain forever. Nightmares of the past may be less debilitating with time for some, yet constant fear grips the Rohingyas as the uncertainty of their future becomes their current haunting nightmare.
Thoughts of forced repatriation and their children’s future are some of the challenging issues they are facing. The losses are not only materials, as the lives of loved ones are taken as well. In the end, will they also lose their future?
The sky above the hospital was almost cloudless in the warm weather. When the clouds do appear, let’s pray that each cloud will have a silver lining and that the Rohingyas will see it soon.
Hope
With the new day, comes new hope. Let us continue to serve in the fi eld hospital with passion, to serve without boundaries. We may not remember the days in the hospital but we cherish the moments of each day. Remember the moments we spent with these Rohingya refugees, their cries, and their stories as we treat them.
beritaMMA Vol.48 • April 2018
general 33
Doctors in Malaysia are a fortunate lot. Despite all the changes that have occurred in the last 60 years we are still, to a large degree, trusted and respected.
The populace is, of course, much better educated now. The Internet makes self-diagnosis possible, though more commonly we deal with self-misdiagnosis and misinformation.
To some extent, then, we have forgotten that there might be dangers lurking in our path. I am not referring to the risk that someone might sue you. I am talking about the fact that doctors are being shot at, bombed, shelled and imprisoned.
We know, though we don’t have it at the front of our minds, that medical personnel in Afrin and Eastern Ghouta work every day under impossible conditions – overwhelming numbers of patients, lack of essential medicines and supplies, and frequent bombing and shelling.
Far fewer of us would have heard of Dr Ahmadreza Djalali. He is an Iranian born doctor, who was resident in Sweden. While back in Iran, he was arrested and after a trial that was far from fair, he was sentenced to death for “corruption on earth” – a rather vague term used against those the regime wishes to kill.
Another case we might have heard of recently is the matter of the leaders of the Turkish Medical Association. They were detained by the government because they issued a statement calling war a danger to public health and urging restraint to prevent further death and damage to health.
For us these events, though sad, disturbing or even tragic, are remote, almost unreal. In fact, even a small change in circumstances may lead us into the same or similar problems. It is not diffi cult to imagine an authoritarian government taking draconian action against doctors, who are bound by oath to treat everyone equally, whether the government considers them worthy of treatment or not.
In any case, even if we never face such problems, should we just ignore them? They will never affect us. Let us just live our lives and do our work.
I hope that is not our response. As John Donne said, no man is an island. We should be concerned by these events not only because we might end up in the same boat, but also because of our common humanity.
Even if we agree with these sentiments, we can feel helpless. What are we, as individuals, to do about these distant events? How do we affect the actions of states and governments which are not even our own? It is diffi cult, but not entirely hopeless.
As social animals, we instinctively know the strength to be found in numbers. We naturally form alliances and unions to help us deal with the problems we face.
In our own country, we have formed the MMA, which we look to as a vehicle for us to protect the interests of our profession and the people who practice it. In the international arena, though, the MMA is not exactly a force to be reckoned with. Even at home, our infl uence could be greater if we band together with others. It is for this reason, mainly, that the MMA has been for decades a member of the World Medical Association (WMA).
The WMA is an association of associations, formed, like many such international groupings, in the aftermath of the Second World War. It now has 111 member associations. It is, by any measure, a large and infl uential association. It partners with the WHO and many other organisations. The Declaration of Geneva, a version of which many universities use in lieu of the Hippocratic Oath, is the best known of the WMA’s many declarations. Strangely though, many more people know of the Declaration than of the organisation behind it!
In the troubles mentioned above, the WMA has been active in making statements and working with its allies and associates to try and alleviate or mitigate the diffi culties of the doctors. At least in the case of the Turkish Medical Association, many of those detained have been released. While the WMA cannot work magic, social media ensures that its statements have a wide reach.
Of course, we as members must also support and participate in its activities and efforts. I urge you, therefore, to follow the WMA on Facebook (https://www.facebook.com/WorldMedicalAssociation) and on Twitter (@medwma) to keep track of what is going on and to help with their campaigns. Remember, their campaigns also include working on immunisation, fi ghting fake drugs and medical education, in addition to helping colleagues in dire need.
I have also often been surprised by the wide variety of topics the WMA’s Declarations, Resolutions, Statements and Position Papers cover. For instance, there is a “Declaration on Quality Assurance in Medical Education”, a “Statement on Epidemics and Pandemics” and a “Statement on Bullying and Harassment within the Profession”. There are also topics which we might have wondered about such as the “Statement on Mobile Health”, which deals with the increasing use of our mobile devices in monitoring and maintaining our health.
There is even a “Statement on Aesthetic Treatment” and a “Resolution on Medical Assistance in Air Travel”. All these documents can be freely accessed at www.wma.net/policy/.
In order to strengthen the WMA, let us lend it our voices and reach. Once strengthened, it can help us better.
Strength in Numbers Dr Ashok Zachariah Philip
Past President MMA [email protected]

Humour
Remote Adventures After nearly 50 years of marriage, and many years of abstinence , as a couple was lying in bed one evening, the wife felt her husband slowly beginning to massage her in ways he hadn’t in quite some time. It almost tickled as his fingers traced down from her neck, and then began moving, very gently past the small of her back.
He next caressed her shoulders and neck, slowly worked his hand down, stopping just over her stomach. He proceeded to place his hand on her left inner arm, working down her side, passing gently over her buttock and down her leg to her calf. Then, he proceeded up her thigh, stopping just at the uppermost portion of her leg. He continued in the same manner on her right side, then, after a satisfactory sigh, stopped, rolled over and became silent.
As she had become quite aroused by this process, she asked in a loving voice, ‘Honey that was wonderful. Why did you stop?’
He responded matter-of-factly: ‘I found the remote.’
The Mysteries of AnatomyWhere can a man buy a cap for his knee,Or the key to a lock of his hair?Can his eyes be called an academy...Because there are pupils there?
In the crown of your head can jewels be found?Who crosses the bridge of your nose?If you wanted to shingle the roof of your mouth,Would you use the nails on your toes?
Can you sit in the shade of the palm of your hand,Or beat on the drum of your ear?Can the calf in your leg eat the corn off your toe?Then why not grow corn on the ear?
Can the crook in your elbow be sent to jail?If so, just what did he do?How can you sharpen your shoulder blades?I’ll be darned if I know. Do you?
compiled from here & there.
Maintain and Attain!Husband Husband frantically calls up the Hotel Manager from the room :” Please come fast, I am having an argument with my wife ! She is so angry and says she will jump from your hotel window. We are on the 21st floor! “
Hotel ManagerHotel Manager : “Sir, I am sorry, but this is your personal issue.”Husband Husband , flustered and panicky now , retorts sharply “ Hello Sir! This is NOT a personal problem, the bloody window is not opening! Get the maintenance fellas up here NOW!
humour34
beritaMMA Vol.48 • April 2018
beritaMMA Vol.48 • April 2018
Reproduced with permission from Carlo Jose San Juan, MD (http://www.callouscomics.com)
Reproduced with permission from Carlo Jose San Juan, MD (http://www.callouscomics.com)
beritaMMA Vol.48 • April 2018
personality36
Humble Beginnings to CEO Dato’ Sri Dr Mohammed Azmanbin Dato’ Aziz Mohammed
Interviewed and written by,Dr Edwin HoSenior Occupational PhysicianCountry Health Manager Shell Malaysia LimitedBerita MMA Editorial Board [email protected]
About Dato’ SriDato’ Sri Dr Mohammed Azman holds an Honorary Doctorate in Safety and Health Management from Cyberjaya University College of Medical Sciences (CUCMS), a Master of Science (Occupational Safety and Health Management) from University Utara Malaysia, and a Master in Business Administration from the Oxford
Business College, UK as well as a Bachelor of Medicine and Bachelor of Surgery from University of Malaya, Kuala Lumpur.
A medical doctor by profession, Dato’ Sri Dr Mohammed Azman has had an illustrious career especially in the fi eld of social insurance. He started his career in 1993 as a young medical doctor and has held various positions since then. In 2001, he became the fi rst medical doctor to be employed by the Social Security Organisation of Malaysia (SOCSO). He was promoted to Senior General Manager of Operations in 2007 and later, as Deputy Chief Executive (Operations) in 2011. Currently, he is the Chief Executive Offi cer (CEO) of SOCSO.
Stepping into the CEO’s offi ce, I was greeted with a warm smile and before me stood this great man whom I knew very little of prior to writing this article.
I was ushered to the sofa where I sat across him, slightly nervous but very excited to get to know more about him. As we began introducing ourselves, I found him to be very friendly and down to earth. More interestingly, I discovered that we share many common interests right from our early medical career, our interests in cardiothoracic surgery and procedures, but later moving on to occupational medicine. Being an important person, naturally his time was limited and we were only scheduled to have 90 minutes to speak. However, the conversation was immensely engaging that time fl ew quickly by. We were almost at the 2-hour mark when we decided it was a wrap. It was very interesting getting to know more about him and his achievements; I could have stayed for another two hours! Unfortunately, he had a fl ight to catch and time did not permit us to carry on such a wonderful conversation. As I refl ected on our conversation and the person he is, it felt as if I could write a book about him, which brings me to the points that even though this article is limited, I will try to cover most of Dato’ Sri’s amazing life journey.
Personal LifeDato’ Sri was born in Mentakab, Pahang. The second in a family of seven and the eldest son, he proudly shared that he grew up as a “kampung boy”. During his early years, he stayed with his grandmother and grew
Sekolah Rendah Kebangsaan Jalan Bahagia Temerloh, Pahang
last row, 5th from right.
At Sekolah Menengah Sains Raub Pahang – standing, 2nd from right

beritaMMA Vol.48 • April 2018
up in Bentong. He switched schools several times as his father (a government servant) was relocated several times. During his school days, he was very active in football and hockey.
Currently, he is happily married with fi ve children, two girls and three boys. His eldest son is pursuing medicine in Ireland and his second son is a cadet pilot at a local fl ying school. While his fi rst two children are pursuing their tertiary education, the other three are still in school.
Early Medical CareerIt is interesting to know that Dato’ Sri’s initial ambition was to be a pilot. However, there was no opening at the time of his application, hence he decided to take up medicine. Once he entered medical school, he knew it was the right choice for him as his interest in medicine grew substantially over time. After completing his MBBS in University of Malaya, he started as a House Offi cer in Penang Hospital and later returned to his hometown in Bentong, Pahang as a Medical Offi cer (MO).
In Bentong, he served at the very same hospital in which his grandfather used to be an attendant, and it was also where Dato’ Sri would usually go for treatment during his childhood when he was ill. He was honoured that
he got to serve his own people and meet his former schoolmates, childhood friends and the older generation who were all close to his family. This speaks volumes of Bentong being a small town with a close-knit community. As a Medical Offi cer, he was passionate about conducting procedures, and dreamt of becoming a cardiothoracic surgeon. However, his priorities changed after getting married and he decided against pursuing his Master’s in Surgery. He then moved to private practice where he worked in a clinic in Genting, seeing mostly URTI cases, in addition to injury cases of construction workers who were working at the construction site in Genting as it was being developed. This led to an interest in Occupational Medicine (OM), which coincidentally happened to be the specialty of Dato’ Dr Krishnan, who was then a partner of the clinic in Genting where Dato’ Sri worked.
Medical Career in Occupational Medicine and Its Future With interest in Occupational Medicine and encouragement from Datuk Dr P. Krishnan, a Past MMA President and an Occupational Medicine stalwart, Dato’ Sri pursued the Licentiate of the Faculty of Occupational Medicine (LFOM) of the Royal College of Physicians, Ireland, which he did locally as a distant learning programme. After completing his LFOM, he moved on to a health care management company where he worked for a short period before the opportunity to work for SOCSO arose. He remembers vividly that there were only fi ve candidates, out of which only two had qualifi cations in Occupational Medicine. I recall him smiling widely as he shared that he was not keen to join SOCSO, even after being offered the job. That led him to postpone his reporting date twice until, at the end of 2000, he fi nally agreed to join and reported to work in early 2001.
Dato’ Sri realised that a lot of improvements were needed in SOCSO and in the fi eld of Occupational Medicine. Today, there is better awareness of OM and we can also see interests among doctors to take up OM. SOCSO has started to make qualifi cation in Occupational Medicine compulsory for panel doctors. He hopes that there will be a concerted effort to move towards this and to make it legal for Clinical Offi cers (CO) to provide OM services. In OM, practitioners are focused on knowing the root cause of the disease and more importantly, how to prevent it.
Key Difference Made in SOCSODato’ Sri Dr Mohammed Azman is a visionary leader, who never fails to come up with ideas to enhance the social protection in our country. His exemplary leadership and commitment led to him being chosen as the Lead Person in the Business Process Reengineering Project of SOCSO. He is a strong believer in Dynamic Social Security and mooted a few fl agship programmes in SOCSO. In summary, he:
1. initiated Occupational Health Training for doctors in 2001, followed by the production of the fi rst Disability Assessment Guideline in Malaysia (2004)
2. introduced 143 new occupational diseases to the SOCSO’s existing list
With family
Receiving M.B.B.S from Universiti Malaya 1992

beritaMMA Vol.48 • April 2018
personality38
3. introduced the CMIA (Certifi ed Medical Impairment Assessor), a certifi cation for SOCSO Medical Board Members.
4. standardised the medical report for Invalidity claim and Employment Injury claim
5. started training of Occupational Medicine (OM) for General Practitioners (GPs) and came up with Occupational Medicine Guideline.
6. introduced Return to Work (RTW) programme in 2007, with an investment of RM238 million in The SOCSO Tun Razak Rehabilitation Center in Melaka year 2015. In 2012, the RTW programme received International Social Security Association’s Good Practice Award (Certifi cate of Merit) For Asia Pacifi c. A year later, the programme was recognised b y t h e H u m a n Rights Commission (SUHAKAM) with the Human Rights Award in 2013. In 2017, SOCSO’s Job Placement and Employment Support Services ( w h i c h i s a component of the RTW programme) was awarded with the Zero Project A w a r d o n Innovative Policy 2017 in Vienna. (More details on the program below)
7. initiated SOCSO’s Commuting Accident Prevention approach through smart partnership with other agencies and NGOs in 2010, to raise awareness on commuting accidents.
8. pioneered the Health Screening Programme (HSP) for Non-Communicable Diseases (NCDs) in 2013, as a preventative measure for lifestyle diseases with more than 3,000 panel clinics, pathological laboratories and mammogram centres to provide health screening to hundreds of thousands of Malaysian workers.
9. compulsory training in Occupational Medicine for all SOCSO’s panel doctors, totalling over 4,000 doctors.
Life at the Top of SOCSO as CEO and Its Corporate CultureDato’ Sri Dr Mohammed Azman was the fi rst medical doctor to be the CEO of SOCSO and also the fi rst internal staff to be promoted to this level. The Social Security Organisation of Malaysia manages a fund of over RM27 billion and processes over 60,000 new claims a year.
Under his leadership, the success of SOCSO’s Return to Work and Prevention in social protection in Malaysia has seen SOCSO awarded the International Social Security Association Good Practice Award (Certifi cate of Merit) in 2012 for Asia Pacifi c for the Return to Work Program and Commuting Accident and Prevention Plan. Last year, SOCSO earned the Zero Project Award on Innovative Policy 2017 for its Job Placement & Employment
Support Services while its human resource initiatives were recognised with the Asia HRD “Contribution to Organisation” Award 2017.
Dato’ Sri Dr Mohammed Azman plays a key role in improving the collection of contributions through inspection activities as well as increasing investments in selected assets. He also introduced ‘PERKESO Prihatin and S4P’ concept, with the aim to improve SOCSO’s delivery services for the well-being of customers.
He spearheaded SOCSO’s transformation through the launch of SOCSO Strategic Plan 2016-2020 that would realise SOCSO’s aim to be a leading and excellent social security provider. Under Dato’ Sri Dr Mohammed Azman’s leadership, SOCSO has come out with a fi ve-year Investment Strategy Blueprint to guide SOCSO in achieving better long-term returns. SOCSO is also a signatory to the Malaysian Code for Institutional Investors to enhance its corporate governance.
His capability and contributions in the fi eld of social security, occupational safety and health and public health are recognised not only in Malaysia but also on the international front where he has been elected as the Head of Health and Function of Rehab International. In addition, Dato’ Sri has been appointed as the International Social Security Association (ISSA) Bureau Member and Chairman of ISSA Technical Commission of Organisational, Management and Innovation since 2016. He is actively involved in the Royal College of Physicians of Ireland since 2005 and is a Fellow of the Faculty of Occupational Medicine since 2010 and also a Member of
Dato’ Sri visits counter Feb 2018 Dato’ Sri visits SIP registration Feb 2018
Ikrar Bebas Rasuah Pejabat Perkeso 2017

beritaMMA Vol.48 • April 2018
International Disability Management Standards Council (IDMSC).
On the local front, Dato’ Sri Dr Mohammed Azman is active in Occupational Safety and Health through membership in NGOs and a member of Board of Directors of National Institute of Occupational Safety and Health (NIOSH). He is a Fellow of the Academy of Occupational and Environmental Medicine Malaysia. He is also a member of the Malaysian Society of Safety and Health, Society of Occupational and Environmental Medicine of the MMA, Academy of Occupational & Environmental Medicine Malaysia, Malaysian Society of Occupational Health Physician and the National Council for Occupational Safety and Health. In 2017, Dato’ Sri Dr Mohammed Azman was accorded the prestigious Outstanding Public and Healthcare Services Award by the Malaysian Medical Association.
As a strong advocate of prevention, health promotion, early intervention and return to work programmes, Dato’
Sri has always been invited to deliver speeches and present papers at local and international seminars and conferences on Social Security, Disability Assessment and Occupational Safety and Health. To date, he has presented over 200 papers locally and abroad including events such as The Singapore WSH Conference 2016, the 2016 European Forum on The Insurance Against Accidents at Work and Occupational Diseases, the ILO Occupational Safety & Health Seminar, and the 30th International Congress on Occupational Health.
Detail of Programmes in SOCSO Here are some of Dato’ Sri Dr Mohammed Azman’s innovative strategies that were implemented:
RTW (Return to Work) ProgrammeIt was introduced in 2007 as part of the efforts to ensure sustainable social security and to prevent loss of productivity caused by employment injury and invalidity. The RTW programme is a comprehensive rehabilitation programme, designed for workers with disabilities arising out of injuries or illnesses, to restore their physical and mental capacity to enable them to resume work quickly in a healthy and safe manner.
The implementation of this programme is based on early intervention concept using a biopsychosocial approach that combines biological, psychological and social aspects using a multi-disciplinary method with the emphasis given on reducing the disability duration to enable the insured person (workers insured by SOCSO) to return to work in a safe and fast manner.
Types of physical and vocational rehabilitation under the RTW programme: • Limb Therapy, Breathing Therapy, Neurology Therapy,
Sensory Therapy, Cardiology Therapy, Speech Therapy, Burn Therapy
• Work Place Therapy• Pain Management• Health Education and Employee Safety• Counselling• Job Placement• Workplace Assessment• Employee Assistive Devices & Assistance• Skills Training
These rehabilitation services are available at SOCSO’s Tun Razak Rehabilitation Centre in Melaka and any rehabilitation centres appointed by SOCSO. For workers who require training to obtain new skills and expertise, they will be sent for vocational training that suit their capability and educational background.
Since its introduction in 2007 until November 2017, the RTW programme has assisted 18,098 workers w i th employment injuries or illness to return to work. SOCSO’s RTW programme
has received local and international recognition and accolades, and it has become the Best Practice in international social security system.
The Culture of S4P (Senyum, Sapa, Salam, Santun & Prihatin) – Smile, Acknowledge, Greet, Polite and Caring‘PERKESO Prihatin and S4P’ concept was introduced in 2015 to improve SOCSO’s delivery of services for the wellbeing of its clients. The S4P encourages good interpersonal skills among SOCSO staff and forms the basis of interaction with clients for all SOCSO staff, particularly the counter staff.
SOCSO’s S4P, ingrained in its organisational culture, is a noble practice to create a prosperous, inclusive and productive society through the willingness to offer sincere assistance with care and affection. The enculturation of positive values among SOCSO staff through the practice of S4P as well as the empowerment of human capital is one of the four change drivers aimed at accelerating the transformation of SOCSO into a premier, dynamic and outstanding leader in social security.
Deepavali Celebration with Socso benefi t recipients and their families 2017

beritaMMA Vol.48 • April 2018
personality40
SOCSO’s Prihatin concept means not only having empathy for workers with disabilities and their dependents but SOCSO employees must also be social security practitioners who are professional, dynamic and aware of changes in the international social security landscape.
The S4P Campaign was launched by Dato’ Sri at SOCSO Headquarters in Menara PERKESO, Kuala Lumpur on 22 May 2015, a month after he became a CEO. The S4P campaign was subsequently launched at SOCSO branches nationwide.
SOCSO’s S4P module was recognised by the Public Services Department (JPA) with an award under the Innovative category, in conjunction with the national level AKRAB Convention on 13 May 2016.
PERKESO Prihatin SquadPERKESO Prihatin Squad was established on 10 September 2015 and was offi cially launched by the Minister of Human Resources on 26 October 2016. The formation of PERKESO Prihatin Squad was mooted by Dato’ Sri who wanted a special team to deliver immediate aid to insured persons or their dependents in the event of an unexpected incident or misfortune. The main objective is to enable SOCSO to take proactive actions in providing speedy assistance to insured persons and their dependents in its effort to improve service delivery for the well-being of clients.
The Squad consists of a team of SOCSO employees in every offi ce throughout the country. They work beyond offi ce hours and even on weekends and public holidays, where they are always on the alert and will take immediate action as soon as they are informed. They will promptly check the eligibility of the victim in order to deliver SOCSO benefi ts. This is immediately done without waiting for the insured persons to submit applications for benefi ts.
If necessary, rehabilitation equipment will be supplied within a day to the insured person who meets all the eligibility requirements. For death cases, funeral benefi t will be paid as soon as possible followed by pension payments to dependents.
Members of PERKESO Prihatin Squad monitor and obtain information of accidents or sickness from the prints, electronic and social media including other reliable sources such as from other government agencies and community leaders. Information is then be channelled to branch offi ces located nearest to the incident or accident for investigation and immediate action is taken within the same day.
SOCSO obtained a 5-star rating from MAMPU for the year 2015-2016, for its excellence in service delivery that exceeds clients’ expectations. The setting up of Prihatin Squad is among SOCSO’s initiatives that contribute to such outstanding rating.
PERKESO Town Hall MeetingsDato’ Sri started a series of town hall meetings at SOCSO branches nationwide in 2016. The town hall meetings are still ongoing, covering major SOCSO branches including those in Sabah and Sarawak.
During each town hall meeting, which usually lasts about two hours, Dato’ Sri shares updates about the organisation’s strategic plans, human capital development and explains the roles played by the staff to achieve the organisation’s missions and visions. He reaches out to the employees by thanking them for their continuous support, hard work and achievements, and further motivates them to be more productive and to always aim higher.
He also speaks about the importance of SOCSO Rebranding, effective service delivery to SOCSO clients, the S4P culture and embracing PERKESO Prihatin values. He emphasises the importance of SOCSO employees str iv ing to be social secur i ty practitioners, and advises them about integrity, discipline and their wellness. Dato’ Sri is a strong advocate for workplace wellness as he believes that this will help create a productive and engaged workforce.
Connection with MMA Dato’ Sri has been a life member since 1993, a CLM (Contributory Life Member). He is involved in the Society of Occupational and Environmental Medicine-MMA (SOEM-MMA) and as a Fellow of the Academy of Occupational and Environmental Medicine Malaysia (AOEMM). Dato’ Sri thinks that MMA has two important roles, fi rstly the development of Occupational Medicine in the country
and secondly in Non-Communicable Diseases (NCD) prevention. The association should serve as a platform to further promote Occupational Medicine among doctors to be part of their practice. As the saying goes, ‘every doctor should seek the occupation of their patients’, and the MMA has a big role to play in promoting Occupational Medicine practice among its members.
The entry point for any of the benefi ciaries of SOCSO schemes are through injuries or diseases. Therefore, as the main association representing the medical practitioners in Malaysia, MMA also plays an important role in the interest of the insured person. Medical practitioners who are members of MMA are often the fi rst who treat an injured or diseased worker, either in hospitals or general practices. Therefore, it is important for the members of
PERKESO Majlis Berbuka Puasa

beritaMMA Vol.48 • April 2018
MMA to understand the roles and functions of SOCSO to maximise the treatment provided to their patients.
On a different note, the impact of the non-communicable disease on Malaysian workers is increasing every year. MMA has an important role to play with regards to this issue, not only in the treatment and management of diseases by its members, but also in the promotion of healthy lifestyle among the population. It is much appreciated by Dato’ Sri for the cooperation of many members of MMA by becoming panels of the SOCSO Health Screening Programme, and he hopes to see further collaboration between the MMA and SOCSO in this area.
MMA is also a perfect platform for SOCSO to engage medical practitioners in the country to facilitate mutual relationship for the betterment of our insured persons. Collectively, the other roles that MMA plays in promoting health and safety of workers in the country will also directly impact the organisation, in view of the high number claims for injuries and diseases that SOCSO receives annually.
Advice to Young Doctors“Firstly, once you have decided to be a doctor, devote your time to give your heart and soul to this noble profession. You shouldn’t complain that you are overworked because we are talking about life - saving lives and getting people to stay healthy,” advises Dato’ Sri.
Medicine is a noble profession that demands high commitment and devotion to the profession and to the patients. Hard work and functioning under stressful situations are to be expected. Therefore, young doctors should be prepared to give their heart and soul to the betterment of their patients. Gone are the days where long hours and extended on calls are being practised in this country.
“Young doctors should toughen up and avoid complaining about being overworked. The profession takes pride in saving lives and improving the health of the patients, and this should be the focus of all young doctors so that it will be embedded in their practice throughout their medical career,” adds Dato’ Sri.
He also reveals that in the current job market, young doctors face stiff competition among peers. It will be an advantage for young doctors to plan and be prepared on the career path that they want to pursue. It can be any specialty or general path, but they have to make up their mind early and not wait until later in their services to fi nally make up their mind. Specialty training should start early, so that their progression into sub-specialty training can be expedited.
What Doctors Should Know about SOCSO Medicine is not only about what you see within the clinic or at the patient’s bedside. Young doctors especially, need to also be well-versed with other health providers or services that can be utilised by their patients. Hence, young doctors should know about the benefi ts provided by SOCSO to its insured persons, basic requirements for qualifi cation, rehabilitation facilities and support and prevention services. They need to understand the principle
of dynamic social security, as practiced by SOCSO and other agencies in the country providing social security net to the population.
This will enable a swift provision of our benefi ts and medical or rehabilitation support to the insured persons. They should also learn about proper requirements for reporting and assessment of insured persons as practiced in the country and as required by law, to avoid from falling into the trap of fraudulent claims or malpractices.
MMA’s Role MMA has a role to play in protecting not just Doctors, but also the nation as a whole. This can be achieved by a bigger national agenda towards promoting health and safety among workers, through their participation in national level committees such as the National Council of Occupational Safety and Health.
“MMA should not only show measured response in issues regarding the medical profession, but also on other issues of health within the population. Putting aside any political or personal agenda, the voice of MMA on national health issues is seen as scientifi c and unbiased, and should be taken more seriously in the future,” suggests Dato’ Sri.
Principles in life: “I always like to help people no matter where and how. My motto in life is ‘Be humble and give your best while you can’. I strongly believe that humility is one of major characteristic of leadership, especially in today’s complex environment. A humble and selfl ess leader leads through actions and not just by words. He should lead by example, following the values he believes in and encouraging his team to do the same. A humble leader can create a sense of belonging among the employees and inspire them to be innovative and certainly go the extra mile,” discloses Dato’ Sri.
“At the end of the day, what matters most is a person’s core values. My core values, amongst others, are sincerity, discipline, willingness to change, continuous learning and many others. How one adapts and applies these values will create a difference,” advises Dato’ Sri.
*Special acknowledgement to Hamisah Hamid, Strategic Communications Offi ce (CEO’s offi ce) for her assistance in supporting the write-up of this article.
Invited to MHI programme at TV3 2016
MMA-PADU Futsal Games 2018 has successfully held on 3 Feb 2018 at KB Futsal
Arena, Pengkalan Chepa, Kelantan. The event was held in collaboration with Persatuan Alumni Doktor USM (PADU) and School of Medical Sciences USM. The objectives of the event were to promote healthy activities and to bring doctors together while promoting MMA.
The event was graced with the presence of USM Health Campus Director cum Hospital USM Director,
Prof Dato’ Dr Ahmad Sukari Halim and Dean of School of Medical Sciences USM, Prof Dr Shaiful Bahari Ismail. MMA was represented by Dr Ahmad Filza Ismail, the state MMA-SCHOMOS Chairman.
Six teams participated in this league format games namely; MMA, PADU, Hospital USM (HUSM), Hospital Raja Perempuan Zainab II (HRPZII), Pusat Pengajian Sains Perubatan A (PPSP A) and Pusat Pengajian Sains Perubatan B (PPSP B). The HUSM team has emerged as champion
while PPSP B and PADU teams were the fi rst and second runners-up respectively. Dr Idris from HUSM team was picked as the top scorer while Mr Azhan of HRPZII team was named as the best goalkeeper.
With the success of the event, the organiser plans to have it as an annual event in promoting healthy lifestyle while enhancing the collaboration and interaction between doctors in Kelantan. It also concurs with the #usmfi t tagline which was launched recently.
MMA-PADU Futsal Games 2018
Maj (Dr) Ahmad Filza bin Ismail (Rtd)
Life Member, MMA Kelantanafi [email protected]
ASH 1 for Prof Dato’ Ahmad Sukari Halim Kelantan MMA Team
Participants with Prof Dato’ Dr Ahmad Sukari and Prof Shaiful Bahari
branch news • kelantan42
beritaMMA Vol.48 • April 2018
beritaMMA Vol.48 • April 2018
Berita MMA Editorial Board Policy
Berita MMA is an offi cial publication of Malaysian Medical Association. The purpose of Berita MMA is to disseminate timely information of members’ views, reports, news and leisure articles that interest a broad spectrum of readership. The bulletin is also intended to be a conduit for discussion of issues facing the medical fraternity or highlight thought-provoking articles. Personal attacks, political statements or innuendos are unwelcome.
Any reports of activities like MMA branch events are encouraged to have more insight on a certain topic held; rather than the mundane line of just reporting the date of event, venue, number of participants or chief guest present.
All articles are in English Language. Contributors of articles should make an effort to vet through their articles or seek assistance from their colleagues to have a minimum standard of language that is acceptable for publication. Plagiarism is frowned upon.
Submitted articles are subject to revisions and minimum language corrections by the editor. We envisage having a diverse range of both articles and contributors. The right to publish is at the sole discretion of the Editorial Board of Berita MMA.
The policy was approved by the Berita MMA Editorial Board on 22 April 2015.
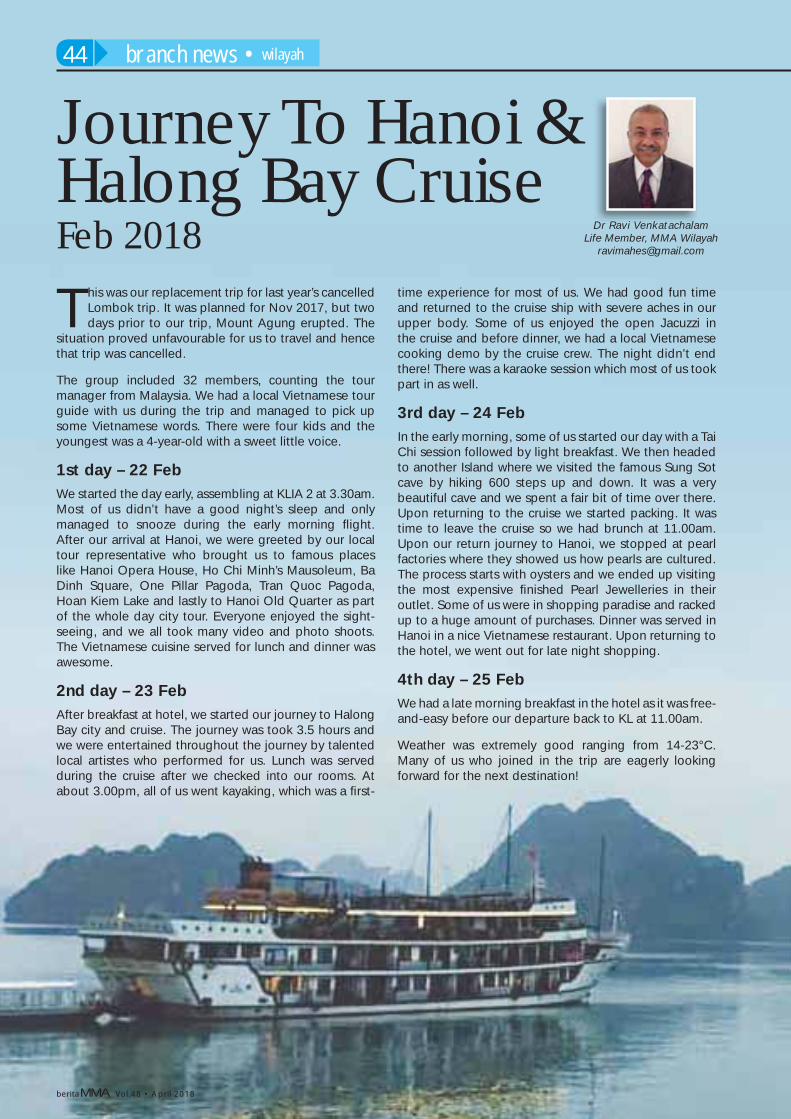
beritaMMA Vol.48 • April 2018
Journey To Hanoi & Halong Bay CruiseFeb 2018
This was our replacement trip for last year’s cancelled Lombok trip. It was planned for Nov 2017, but two days prior to our trip, Mount Agung erupted. The
situation proved unfavourable for us to travel and hence that trip was cancelled.
The group included 32 members, counting the tour manager from Malaysia. We had a local Vietnamese tour guide with us during the trip and managed to pick up some Vietnamese words. There were four kids and the youngest was a 4-year-old with a sweet little voice.
1st day – 22 Feb We started the day early, assembling at KLIA 2 at 3.30am. Most of us didn’t have a good night’s sleep and only managed to snooze during the early morning fl ight. After our arrival at Hanoi, we were greeted by our local tour representative who brought us to famous places like Hanoi Opera House, Ho Chi Minh’s Mausoleum, Ba Dinh Square, One Pillar Pagoda, Tran Quoc Pagoda, Hoan Kiem Lake and lastly to Hanoi Old Quarter as part of the whole day city tour. Everyone enjoyed the sight-seeing, and we all took many video and photo shoots. The Vietnamese cuisine served for lunch and dinner was awesome.
2nd day – 23 Feb After breakfast at hotel, we started our journey to Halong Bay city and cruise. The journey was took 3.5 hours and we were entertained throughout the journey by talented local artistes who performed for us. Lunch was served during the cruise after we checked into our rooms. At about 3.00pm, all of us went kayaking, which was a fi rst-
time experience for most of us. We had good fun time and returned to the cruise ship with severe aches in our upper body. Some of us enjoyed the open Jacuzzi in the cruise and before dinner, we had a local Vietnamese cooking demo by the cruise crew. The night didn’t end there! There was a karaoke session which most of us took part in as well.
3rd day – 24 Feb
In the early morning, some of us started our day with a Tai Chi session followed by light breakfast. We then headed to another Island where we visited the famous Sung Sot cave by hiking 600 steps up and down. It was a very beautiful cave and we spent a fair bit of time over there. Upon returning to the cruise we started packing. It was time to leave the cruise so we had brunch at 11.00am. Upon our return journey to Hanoi, we stopped at pearl factories where they showed us how pearls are cultured. The process starts with oysters and we ended up visiting the most expensive fi nished Pearl Jewelleries in their outlet. Some of us were in shopping paradise and racked up to a huge amount of purchases. Dinner was served in Hanoi in a nice Vietnamese restaurant. Upon returning to the hotel, we went out for late night shopping.
4th day – 25 Feb
We had a late morning breakfast in the hotel as it was free-and-easy before our departure back to KL at 11.00am.
Weather was extremely good ranging from 14-23°C. Many of us who joined in the trip are eagerly looking forward for the next destination!
Dr Ravi VenkatachalamLife Member, MMA Wilayah
branch news • wilayah44

beritaMMA Vol.48 • April 2018

beritaMMA Vol.48 • April 2018
mark your diary46
14 April 2018 20* & 21 – 22** April 2018
22 – 24 June 201811 – 13 May 2018 28 – 30 June 2018
4 – 6 May 2018 5 – 6 May 2018 8 May 2018
20 – 21 April 20186TH EVIDENCE BASED SEMINAR ON TRADITIONAL AND COMPLIMENTARY MEDICINE
Theme : Advances in TnCM in Malaysia
Venue : Grand Seasons Hotel Kuala Lumpur
Organiser : Malaysian Medical Association (MMA)
Contact : +603-4041 1375 ext 127 (Ms Jasmeet)
Email : [email protected]
10TH SABAH MMA PRIMARY CARE CONFERENCE
Venue : * (Pre-Conference) PGMC, Queen Elizabeth Hospital, Kota Kinabalu Sabah
** (Conference) Pacifi c Sutera Harbour Kota Kinabalu, Sabah
Organiser : MMA Sabah BranchContact : Elsie +6012-805 5009 /
Merelyn +6010-243 5008Email : [email protected]
NUTRITIONAL CERTIFICATION COURSE – MODULE 2 & NUTRITIONAL ADVANCED COURSE
Venue : Royale Chulan Kuala Lumpur
Organiser : Society for the Advancement of Hormones and Healthy Aging Medicine in Malaysia
Contact : Ms Sathi Bhaskaran +603-7493 5083Ms Vasantha+6016-307 8074
Email : [email protected] / [email protected]
1ST ASEAN CONFERENCE ON TOBACCO CONTROL
Theme : Towards Healthy CitiesVenue : Dewan Tun Dr Ismail
Putra World Trade Centre Kuala Lumpur
Organiser : Malaysian Council for Tobacco Control
Contact : +603-4252 9100Email : [email protected]
NATIONAL MMA CONVENTION AND SCIENTIFIC CONGRESS 2018 & 58TH MMA ANNUAL GENERAL MEETING
Venue : Royal Chulan Hotel Kuala Lumpur
Contact : Ms Josephine (Secretariat Staff) +6016-223 8079
Email : [email protected]
9TH MEMS ANNUAL CONGRESS (MAC 9) 2018
Theme : Evolving Towards Excellence in Endocrinology
Venue : Hilton Kuala LumpurOrganiser : Malaysian Endocrince &
Metabolic SocietyContact : Amy Yu / NaraTel : + 03-7726 8000Fax : +603-7733 7007Email : [email protected]
MMA INAUGURAL CONFERENCE ON HEALTH OF THE OLDER PERSON
Theme : Into The Future We Transform
Venue : Grand Seasons HotelKuala Lumpur
Organiser : MMA Committee for the Health of the Older Person
Contact : Ms Muthuletchumi (MMA Secretariat)
+603-4041 1375Fax : +603-4041 8187 /
+603-4041 9929Email : [email protected]
SYMPOSIUM – A DATE WITH OCCUPATIONAL HAZARD @ HEALTHCARE FACILITIES
Venue : Perdana UniversityOrganiser : Academy of Occupational
& Environmental Medicine Malaysia (AOEMM) & Perdana University
Contact : Ms Hema +603-4050 8211 / +6012-602 0778
(Monday – Friday 9 a.m. – 5 p.m.)
Email : [email protected]
14TH NATIONAL SYMPOSIUM ON ADOLESCENT HEALTH (NSOAH)
Theme : Adolescent PotpourriVenue : Institute of Leadership &
DevelopmentUiTM Bandar Enstek Negeri Sembilan
Co-Organiser(s): Malaysian Medical Association, Malaysian Paediatric Association & Malaysian Association of Adolescent Health
Contact : Ms Norlailatul Asikin Mohamad Nor (MAAH)+6013-266 5911Ms Smidha Nair (MMA)
+603-4031 1375 ext 129 Email : [email protected]