Embed Size (px)
Citation preview

Persistence.Persistence. Focus:Focus: Treatment and Medico-legal Treatment and Medico-legal
IssuesIssues
33rdrd Jack Pepys Workshop Jack Pepys Workshop
Susan M TarloSusan M TarloUniversity of TorontoUniversity of Toronto
University Health Network and University Health Network and Gage Occupational and Gage Occupational and
Environmental Health UnitEnvironmental Health Unit
DisclosuresDisclosures
Patients are seen for medical assessment at Patients are seen for medical assessment at the request of the Ontario Workplace Safety the request of the Ontario Workplace Safety and Insurance Board (WSIB), approx 1 new and Insurance Board (WSIB), approx 1 new patient per weekpatient per week
Patients referred by other physicians may Patients referred by other physicians may have claims submitted by me to WSIBhave claims submitted by me to WSIB
Files being appealed from WSIB may be Files being appealed from WSIB may be reviewed for an independent medical opinion reviewed for an independent medical opinion from WSIATfrom WSIAT
Research funding has been received from Research funding has been received from WSIB RAC WSIB RAC

77. Despite strong medical advice to discontinueexposure to a work sensitizer, some patients with OA continue to work in the same environment with the same or reduced exposure. What is the value of inhaled steroids in such patients?
78. Subjects with OA are exposed to commonallergens after being removed from work. In the case of OAdue to low molecular weight agents, is there cross-reactivity with other common environmental chemicals that resemble the causal agent?
79. In aiming to assess the efficacy of intervention inwork-related asthma, a problem in the design of post-intervention studies is that there is usually no control group.How can this study design problem be overcome?
From 100 questions/needsFrom 100 questions/needstreatment/medicolegaltreatment/medicolegal

Current management of Current management of sensitizer-induced OA sensitizer-induced OA during/post diagnosisduring/post diagnosis
Initiate appropriate compensation claim Initiate appropriate compensation claim (early)(early)
Control the asthma - throughoutControl the asthma - throughout Evaluate and control exposure to Evaluate and control exposure to
relevant non-occupational triggersrelevant non-occupational triggers Asthma medications as per guidelinesAsthma medications as per guidelines
Evaluate appropriate work accommodationEvaluate appropriate work accommodation For the patientFor the patient Consider co-workers and possible work Consider co-workers and possible work
intervention to protect other workers intervention to protect other workers

Evaluate appropriate work Evaluate appropriate work accommodationaccommodation
for the patient when the for the patient when the sensitizer is knownsensitizer is known Where possible, completely avoid further Where possible, completely avoid further
exposure to the relevant sensitizer after exposure to the relevant sensitizer after diagnosisdiagnosis
If impossible for socio-economic reasons, If impossible for socio-economic reasons, reduce exposure – compensation issues may reduce exposure – compensation issues may be relevant here be relevant here – if this is the required – if this is the required approach, either pending a compensation approach, either pending a compensation claim or for other reasons such as lack of claim or for other reasons such as lack of eligibility for compensation, there must be eligibility for compensation, there must be careful medical monitoring, and further careful medical monitoring, and further intervention if asthma is worseningintervention if asthma is worsening
Exposure ManagementExposure ManagementAHRQ Evidence Report #129, Nov 2005, AHRQ Evidence Report #129, Nov 2005,
Beech et alBeech et al
52 cohort studies52 cohort studies Due to vagaries of reporting, statistical Due to vagaries of reporting, statistical
analyses of published studies not analyses of published studies not feasiblefeasible
Graphic display of results suggested Graphic display of results suggested worse outcomes (FEV1 and worse outcomes (FEV1 and methacholine responsiveness) for those methacholine responsiveness) for those remaining at work vs those removed. No remaining at work vs those removed. No clear difference in trend for HMWt vs clear difference in trend for HMWt vs LMWt sensitizersLMWt sensitizers
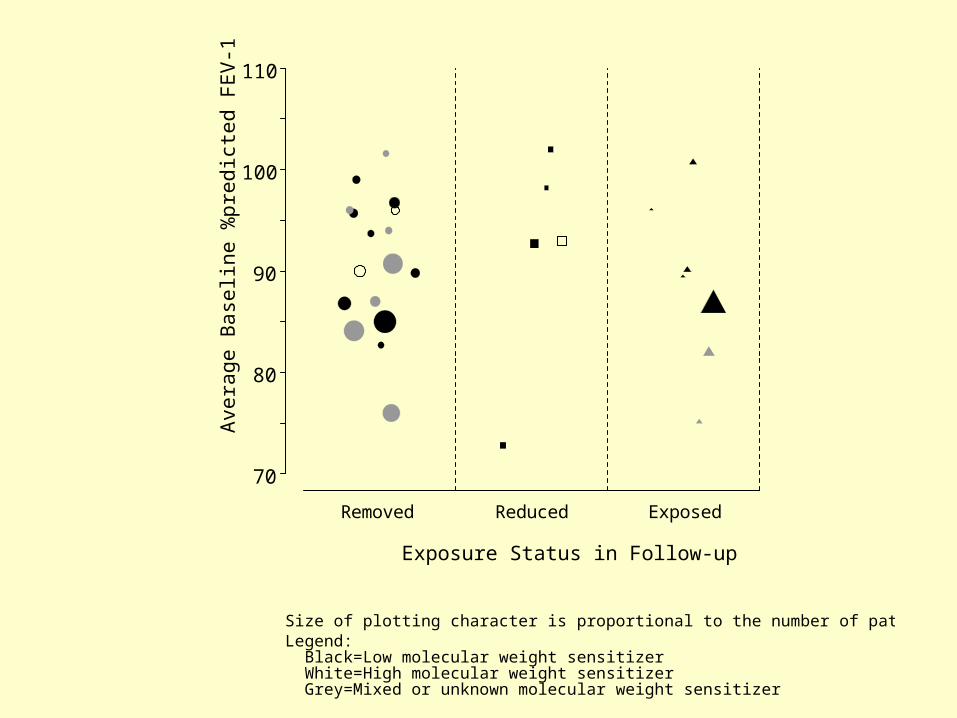
Removed Reduced Exposed
Exposure Status in Follow-up
70
80
90
100
110
Ave
rage
Bas
elin
e %
pre
dic
ted
FE
V-1
Size of plotting character is proportional to the number of patients followedLegend: Black=Low molecular weight sensitizer White=High molecular weight sensitizer Grey=Mixed or unknown molecular weight sensitizer

0 2 4 6 8-20
-10
0
10
20 Removed
0 2 4 6 8-20
-10
0
10
20 Reduced
0 2 4 6 8-20
-10
0
10
20 ExposedCh
ang
e in
Ave
rag
e %
pre
dic
ted
FE
V-1
Length of Follow-up (years)
Size of plotting character is proportional to number of patients followedStudies with multiple follow-up visits are joined by dashed linesLegend: Black=Low molecular weight sensitizer White=High molecular weight sensitizer Grey=Mixed or unknown molecular weight sensitizer
0 2 4 6 80
1
2
3
4
5Removed
0 2 4 6 80
1
2
3
4
5Reduced
0 2 4 6 80
1
2
3
4
5Exposed
Ra
tio o
f F
ollo
w-u
p a
nd
Ba
selin
e M
ea
n H
ype
resp
on
sive
ne
ss
Length of Follow-up (years)
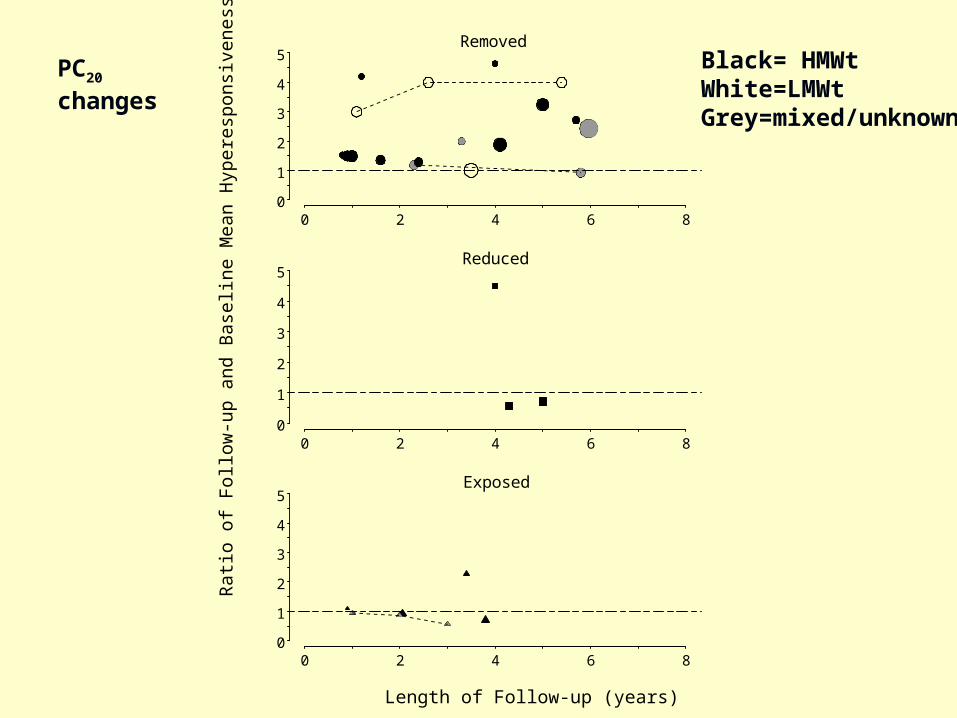
Size of plotting character is proportional to number of patients followedStudies with multiple follow-up visits are joined by dashed linesLegend: Black=Low molecular weight sensitizer White=High molecular weight sensitizer Grey=Mixed or unknown molecular weight sensitizer
Black= HMWtWhite=LMWtGrey=mixed/unknown
PC20 changes

Possible measures to Possible measures to avoid/limit exposureavoid/limit exposure
Best to worst optionsBest to worst options AvoidanceAvoidance – complete - change of – complete - change of
process, e.g.process, e.g.non-latex gloves, enzyme change, paint non-latex gloves, enzyme change, paint changechangeChange of work area/workplace (with Change of work area/workplace (with review of exposures in new area)review of exposures in new area)
Partial reductionPartial reduction e.g. low-protein, low powder e.g. low-protein, low powder latexlatexMove to low-exposure areaMove to low-exposure areaImproved occ hygiene measures, e.g. Improved occ hygiene measures, e.g. ventilation/exhaustventilation/exhaustImprove resp protectionImprove resp protection

Outcome with removal vs Outcome with removal vs continued exposure continued exposure (Moscato (Moscato
et al Chest ’99)et al Chest ’99) 25 with OA confirmed by challenge, 25 with OA confirmed by challenge,
followed for 1yfollowed for 1y 13 left exposure – significantly worse 13 left exposure – significantly worse
asthma at diagnosis, FEVasthma at diagnosis, FEV11 and PD and PD2020
At 1y those who left had improved At 1y those who left had improved more than those who stayed – more than those who stayed – decreased medication needs vs decreased medication needs vs increased needs in those who stayedincreased needs in those who stayed
However only those who left had a However only those who left had a loss in income (>25% median loss)loss in income (>25% median loss)

Inhaled steroids for those who Inhaled steroids for those who
cannot avoid exposurecannot avoid exposure (Marabini et (Marabini et al Chest ’03)al Chest ’03)
20 subjects with OA (20 subjects with OA (mean sx 13+/-13ymean sx 13+/-13y), still working. ), still working. 12 moderate, 8 mild12 moderate, 8 mild
3 y f-up, protective equipment as able3 y f-up, protective equipment as able 10 retired/changed jobs (significantly younger than 10 retired/changed jobs (significantly younger than
those who stayed). Only 2 clearedthose who stayed). Only 2 cleared Those who stayed were treated with high dose inhaled Those who stayed were treated with high dose inhaled
steroids and bronchodilatorssteroids and bronchodilators No statistically significant change over the 3y in No statistically significant change over the 3y in
spirometry, bd needs for those who stayed,spirometry, bd needs for those who stayed, PD20 mg yearly mean: 1.4, 1.3, 1.2, 0.8 (NS)PD20 mg yearly mean: 1.4, 1.3, 1.2, 0.8 (NS)Findings limited by small numbers. Trends to decline in Findings limited by small numbers. Trends to decline in
PD20. ?? Whether applicable to those with earlier PD20. ?? Whether applicable to those with earlier diagnosisdiagnosis
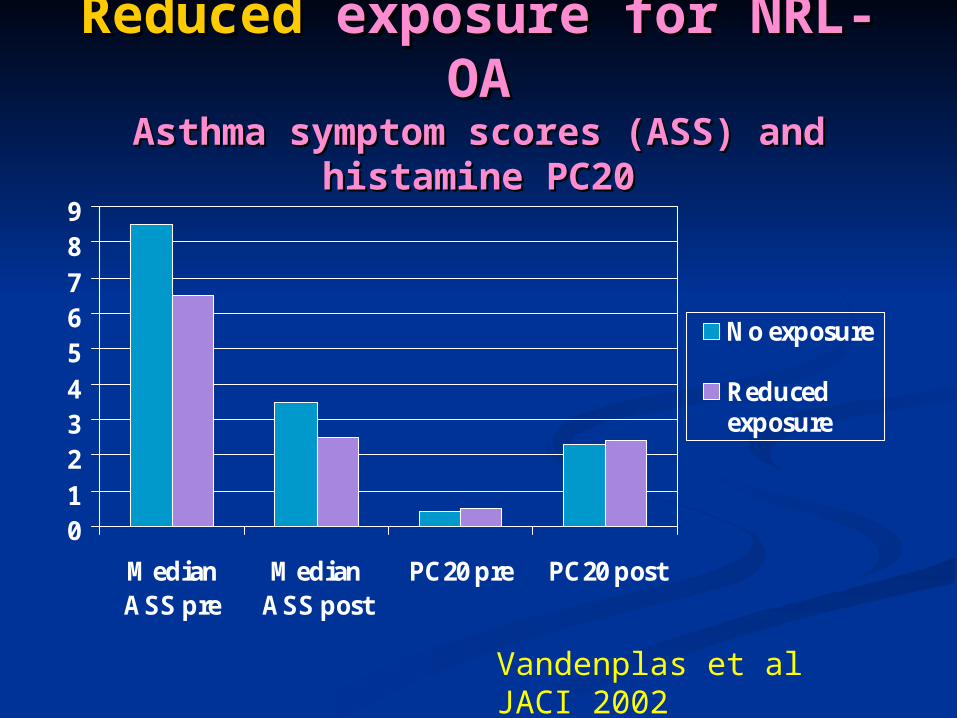
ReducedReduced exposure for NRL- exposure for NRL-OAOA
Asthma symptom scores (ASS) and Asthma symptom scores (ASS) and histamine PC20histamine PC20
0123456789
MedianASS pre
MedianASS post
PC20 pre PC20 post
No exposure
Reducedexposure
Vandenplas et al JACI 2002
Monitor asthma closely with Monitor asthma closely with occupational changes (changes in occupational changes (changes in
exposures/job)exposures/job) When the sensitizer is unknown and/or When the sensitizer is unknown and/or
may be present in a new environmentmay be present in a new environment When there may be cross-reacting agents When there may be cross-reacting agents
in the environment where the patient is in the environment where the patient is moved tomoved to
When the exposure is reduced but not When the exposure is reduced but not eliminatedeliminated
Symptoms/medications/pulmonary function Symptoms/medications/pulmonary function parameters/? NO, ? induced sputumparameters/? NO, ? induced sputum
Cross-reacting agentsCross-reacting agents
Other than similar chemical Other than similar chemical sensitizers, e.g., other diisocyanates sensitizers, e.g., other diisocyanates in or out of the workplace, little in or out of the workplace, little published data on agents cross-published data on agents cross-reacting with work-sensitizersreacting with work-sensitizers
- a few older reports of colophony - a few older reports of colophony and non-occupational pine products and non-occupational pine products
? Any current research in this area? Any current research in this area
PharmacotherapyPharmacotherapy
Inhaled steroids – 2 older clinical Inhaled steroids – 2 older clinical trials suggested benefit, no recent trials suggested benefit, no recent trialstrials
No recent studies of No recent studies of pharmacotherapy among those pharmacotherapy among those remaining in exposureremaining in exposure
Immunotherapy? Immunotherapy?
Small trials of immunotherapy have been Small trials of immunotherapy have been reported for NRL allergy and asthmareported for NRL allergy and asthma
Benefit found more for nasal/eye symptoms Benefit found more for nasal/eye symptoms than for asthma to date (Sastre et al, JACI than for asthma to date (Sastre et al, JACI ’03)’03)
Sublingual treatment appears to be better Sublingual treatment appears to be better tolerated but local reactions(89% patients) tolerated but local reactions(89% patients) and systemic reactions (46% patients) were and systemic reactions (46% patients) were still common (Cistero Bahima et al J Invest All still common (Cistero Bahima et al J Invest All Clin Immunol ’04)Clin Immunol ’04)
Not considered standard treatment for OANot considered standard treatment for OA

Immunotherapy with other Immunotherapy with other agentsagents
Beekeepers with anaphylaxis (± asthma) Beekeepers with anaphylaxis (± asthma) respond well to venom immunotherapy respond well to venom immunotherapy (Muller, Curr Opin All Clin Immunol (Muller, Curr Opin All Clin Immunol 2005)2005)
Armentia ’90 assessed 30 bakers with Armentia ’90 assessed 30 bakers with wheat immunotherapy (20 active, 10 wheat immunotherapy (20 active, 10 placebo) with significant benefit – no placebo) with significant benefit – no recent studiesrecent studies
Common allergens, cat, pollen, not Common allergens, cat, pollen, not specifically addressed in OAspecifically addressed in OA
Omalizumab not reported as yet for OAOmalizumab not reported as yet for OA

Some reasons for poor Some reasons for poor medical outcomemedical outcome
Severe asthma at diagnosisSevere asthma at diagnosis Late diagnosis (2◦ to patient or physician), delay or Late diagnosis (2◦ to patient or physician), delay or
no compensation: leading to prolonged exposureno compensation: leading to prolonged exposure Occupational factorsOccupational factors
Ongoing exposure to the work sensitizer or Ongoing exposure to the work sensitizer or cross-reacting agents (known or unknown) at cross-reacting agents (known or unknown) at work or in other environmentswork or in other environments
Workplace irritant exposure aggravating asthmaWorkplace irritant exposure aggravating asthma Other contributing factorsOther contributing factors
Non-occupational allergen exposure/ irritantsNon-occupational allergen exposure/ irritants GERD, VCD, non-asthma causes of symptomsGERD, VCD, non-asthma causes of symptoms
Compensation/medicolegal Compensation/medicolegal issuesissues
Different systems in different provinces, states, Different systems in different provinces, states, countriescountries
Some issues likely to be common in many regions Some issues likely to be common in many regions where others may be specificwhere others may be specific
Criteria for acceptance may differ - e.g., need for Criteria for acceptance may differ - e.g., need for SIC for OA, acceptance of WEASIC for OA, acceptance of WEA
Process might contribute to persistence of Process might contribute to persistence of asthma/disability – no identified published data on asthma/disability – no identified published data on thisthis
More likely if workers continue exposure because: More likely if workers continue exposure because:
Ineligible for compensationIneligible for compensation
Reluctance to apply for a claim – no dataReluctance to apply for a claim – no data
Delays in a claim decision – could be years Delays in a claim decision – could be years
E.g., Ontario WSIB E.g., Ontario WSIB www.wsib.on.cawww.wsib.on.ca
Began 1915 as WCBBegan 1915 as WCB Financed by employer premiums (adjusted by risk)Financed by employer premiums (adjusted by risk) No-fault collective liability: workers give up their No-fault collective liability: workers give up their
right to sueright to sue 1998 Changed name to WSIB and mandate 1998 Changed name to WSIB and mandate
changed to include promoting changed to include promoting preventionprevention of work- of work-related injuries and illnesses. It now also oversees related injuries and illnesses. It now also oversees Ontario’s system of workplace safety education Ontario’s system of workplace safety education and training, and supports research via an and training, and supports research via an independent Research Advisory Council and independent Research Advisory Council and Centres for Research Expertise, e.g. CREOD. Centres for Research Expertise, e.g. CREOD.
Mandate includes disability benefits, monitoring Mandate includes disability benefits, monitoring quality of healthcare, and assisting in early safe quality of healthcare, and assisting in early safe return to workreturn to work

Ontario WSIBOntario WSIB Policy: In determining a claim the decision shall Policy: In determining a claim the decision shall
be made in accordance with the real merits and be made in accordance with the real merits and justice of the case. ..When the evidence for or justice of the case. ..When the evidence for or against the issue is approximately equal in against the issue is approximately equal in weight, the issue shall be resolved in favor of weight, the issue shall be resolved in favor of the person claiming benefits (not to be used as a the person claiming benefits (not to be used as a substitute for evidence). substitute for evidence).
Decisions on claim acceptance and Decisions on claim acceptance and compensation made by claims adjudicators – compensation made by claims adjudicators – they are usually assigned by work sector rather they are usually assigned by work sector rather than by disease/injury. They can get advice from than by disease/injury. They can get advice from the “complex case unit” WSIB physicians who the “complex case unit” WSIB physicians who may request additional external independent may request additional external independent medical assessments, e.g., from the medical assessments, e.g., from the occupational disease specialty program. WSIB occupational disease specialty program. WSIB pays for costs of assessments/investigations.pays for costs of assessments/investigations.
Support provided for accepted OA Support provided for accepted OA claimsclaims
Economic loss - 85% provided for limited time Economic loss - 85% provided for limited time after claim accepted if further job is feasible, after claim accepted if further job is feasible, supplement if lower-paying job obtainedsupplement if lower-paying job obtained
Cost of medications/medical devicesCost of medications/medical devices Non-economic loss: disability (usually assessed Non-economic loss: disability (usually assessed
at the time of considered maximum medical at the time of considered maximum medical recovery, e.g. often 1-2 y after an OA claim is recovery, e.g. often 1-2 y after an OA claim is accepted). Includes disability from asthma plus accepted). Includes disability from asthma plus disability from sensitization if present.disability from sensitization if present.
Training for new work if approved – labor Training for new work if approved – labor market re-entry skills, re-training market re-entry skills, re-training (secondary/post secondary ed)(secondary/post secondary ed) Examples: 18 y old baker, 45 y old plasma welderExamples: 18 y old baker, 45 y old plasma welder

Work-exacerbated/Work-exacerbated/aggravated asthmaaggravated asthma
Policy: “In cases where the worker has a pre-Policy: “In cases where the worker has a pre-accident impairment and suffers a minor work-accident impairment and suffers a minor work-related injury or illness to the same body part or related injury or illness to the same body part or system WSIB considers entitlement to benefits on system WSIB considers entitlement to benefits on an aggravation basis.”an aggravation basis.”
““Generally entitlement is for the acute episode only Generally entitlement is for the acute episode only and benefits continue until the worker returns to and benefits continue until the worker returns to the pre-accident state.”the pre-accident state.”
Entitlement is not limited when there is no pre-Entitlement is not limited when there is no pre-accident impairment or if the severity of the accident impairment or if the severity of the exposure/accident on its own would have resulted exposure/accident on its own would have resulted in additional impairment – i.e. potential for in additional impairment – i.e. potential for “permanent aggravation”“permanent aggravation”
Aggravation is the effect that the injury/illness has Aggravation is the effect that the injury/illness has on pre-accident impairment, requiring healthcare on pre-accident impairment, requiring healthcare and/or leading to loss of earning capacity – can and/or leading to loss of earning capacity – can include permanent impairmentinclude permanent impairment

Compensation issuesCompensation issues Not all workers are covered Not all workers are covered Processes for decisions and levels of Processes for decisions and levels of
compensation differs widely between and compensation differs widely between and even within countrieseven within countries
Process can be complicated and time-Process can be complicated and time-consuming for workers and physicians – consuming for workers and physicians – forms for worker/physician/workplaceforms for worker/physician/workplace
Decisions can take months to yearsDecisions can take months to years Workers with OA often do not have skills to Workers with OA often do not have skills to
transfer to other similar-paying occupationstransfer to other similar-paying occupations Job-market re-entry programs may provide Job-market re-entry programs may provide
some skills but will usually not find some skills but will usually not find replacement work, and self-found jobs may replacement work, and self-found jobs may pay less than former work pay less than former work

More compensation More compensation issuesissues
Workers may lose non-compensated benefits Workers may lose non-compensated benefits from previous job, e.g. dental plans, general from previous job, e.g. dental plans, general medication coverage medication coverage
Even with accepted workers’ compensation Even with accepted workers’ compensation claims, significant socio-economic loss is claims, significant socio-economic loss is reportedreported
Effects of having a previous compensation Effects of having a previous compensation claim on chance of employment, not publishedclaim on chance of employment, not published
Some workers are reluctant to accept advice to Some workers are reluctant to accept advice to initiate a compensation claim and prefer to initiate a compensation claim and prefer to continue working with OA as long as possible – continue working with OA as long as possible – may lead to less reversibility and greater long may lead to less reversibility and greater long term asthma morbidityterm asthma morbidity
Suggests that further improvements are needed Suggests that further improvements are needed for compensation issuesfor compensation issues

Ontario WSIB appealsOntario WSIB appeals
Worker or workplace can appeal Worker or workplace can appeal decision to WSIB – issues of stress, decision to WSIB – issues of stress, income lossincome loss
Next decision can be appealed to an Next decision can be appealed to an independent Workplace Safety and independent Workplace Safety and Insurance Appeals Tribunal an agency Insurance Appeals Tribunal an agency within the Ontario administrative within the Ontario administrative justice system who may ask for justice system who may ask for further independent medical reviewfurther independent medical review

ConclusionsConclusions Early diagnosis and removal from further Early diagnosis and removal from further
exposure (for sensitizer-OA) offers best medical exposure (for sensitizer-OA) offers best medical outcome - but often at a significant socio-outcome - but often at a significant socio-economic cost despite workers’ compensation economic cost despite workers’ compensation systems. Other management options (e.g. systems. Other management options (e.g. greatly reduced exposure for NRL), are an greatly reduced exposure for NRL), are an alternative for some agents and are selected by alternative for some agents and are selected by other workers with OA against medical advice.other workers with OA against medical advice.
Immunotherapy may benefit some patients but Immunotherapy may benefit some patients but few allergens have been assessed and few allergens have been assessed and monoclonal anti IgE has not been assessed. monoclonal anti IgE has not been assessed. Pharmacotherapy + reduced exposure has not Pharmacotherapy + reduced exposure has not currently been proven of benefit currently been proven of benefit
The effects of compensation systems on asthma The effects of compensation systems on asthma persistence have not been documentedpersistence have not been documented





























