Embed Size (px)
Citation preview

Persistence of Cognitive, Psychiatric, and Functional Declines following COVID‐19
Tracy D. Vannorsdall, PhD, ABPP/CNMid-Atlantic Regional Conference in Occupational and Environmental Medicine
10.16.2021

Objectives
• Neuropsychological and neuropsychiatric symptoms and methods
• JH PACT outcomes
• Management of cognitive and neuropsychiatric changes following COVID‐19 illness

WHO Post‐COVID‐19 Case Definition
Cognitive and neuropsychiatric symptoms• Reduce quality of life • May limit participation in rehabilitative interventions • Can hinder return to work efforts
Post COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include fatigue, shortness of breath, cognitive dysfunction but also others* and generally have an impact on everyday functioning. Symptoms may be new onset following initial recovery from an acute COVID-19 episode or persist from the initial illness. Symptoms may also fluctuate or relapse over time.

Functional Limitations Post‐COVID‐19
Up to 67% of non‐hospitalized patients report functional limitations 3 to 6 months following COVID‐19 illness (*survey data*)
Self‐care ADLs Return to Work
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/7october2021https://pubmed.ncbi.nlm.nih.gov/32932582/https://pubmed.ncbi.nlm.nih.gov/34308300/https://www.medrxiv.org/content/10.1101/2021.03.21.21253968v2

Functional Limitations Post‐COVID‐19
Roughly 20% to > 50% of patients report functional limitations up to 8 months following COVID‐19‐related hospitalization
Risk factors: ICU, length of stay, female sex, age
https://www.journalofinfection.com/article/S0163‐4453(21)00391‐1/fulltexthttps://www.journalofinfection.com/article/S0163‐4453(20)30784‐2/fulltext
Self‐care ADLs Return to Work

Post-COVID Neuropsychiatric Conditions
• Marked variability in symptoms across patients
• Multiple plausible biological mechanisms
• Unclear trajectory
• Possibility of unmasking previously undetected cognitive and psychiatric issues
• Reactions to pandemic-related stress, social isolation, etc.
• Effects of the virus vs pre-existing conditions vs treatmentsChallenges

⁍ Direct and indirect mechanisms affecting brain health:⁍ Systemic inflammatory response
⁍ Inflammatory cascade
⁍ Hypoxia
⁍ Delirium/encephalopathy
⁍ Acute respiratory distress syndrome
⁍ Prothrombotic state / Stroke

Assessing CognitionNeuropsychological assessment – performance‐based method to determine cognitive functioning and abilities across domains• Traditional neuropsychological exam
• Pros – Structured, objective, norm‐derived outcomes, comprehensive, tailored to the individual and referral question, sensitive to dysfunction, provides intervention targets
• Cons – time, availability • Screeners (e.g., MMSE, MOCA)
• Pros – quick, free/inexpensive, objective • Cons – lack sensitivity, not tailored to the individual

Assessing CognitionSelf‐report instruments(e.g., Perceived Deficits Questionnaire – Dep’n, 5‐item; PDQ‐D‐5; Patient‐Reported Outcomes Measurement Information System; PROMIS Cognitive Function 4a)
• Pros – quick, free/inexpensive, subjective• Cons – subjective, may not correlate with cognitive ability, can be driven by psychiatric issues, sleep/fatigue, stress, personality, etc.

Assessing Neuropsychiatric Symptoms
Domain Instruments
Depression PHQ‐9Beck Depression Inventory IIHADS
Anxiety GAD‐7Beck Anxiety InventoryHADS
PTSD/Trauma‐related Impact of Events Scale‐6 (IES‐6) PTSD Checklist for DSM 5 (PCL‐5)
https://www.cdc.gov/coronavirus/2019‐ncov/hcp/clinical‐care/post‐covid‐assessment‐testing.html


Domain Finding (n = 12 studies; n = 8‐185 patients)
Global Cognitive Functioning Deficits in 100% of n = 12 studies15 – 80% of patients
Attention & Executive Function Deficits reported in 100% of n = 7 studies
Memory Deficits in 3 of 4 studies
Language Deficits in 100% of n = 4
Visuospatial Function Deficits in 2 of 4 studies
Conclude: Patients with recent SARS-CoV-2 infection appear to experience global cognitive impairment, impairment in memory, attention and executive function, and in particular verbal fluency.

Johns Hopkins Post-Acute COVID-19 Team
Brigham et al. American Journal of Medicine, 2021

JH PACT Telephone Battery
Test DomainRAVLT
Verbal learningDelayed recall
Oral Trail Making Test Part APart B
Processing speedExecutive functioning
Number SpanForward
BackwardAttentionWorking memory
Verbal FluencyLetter-cued
Category-cuedExecutive functioningLanguage retrieval
Mild/Moderate Impairment: ≥1.5 SD below age‐adjusted means (i.e. <7th%ile)Severe Impairment: ≥2 SD below age‐adjusted means (i.e., <2nd %ile

JH PACT Telephone Battery
Domain Instrument
Depression PHQ-9
Anxiety GAD-7
Trauma/PTSD Impact of Events Scale-6
Functional Decline Quick Dementia Rating Scale
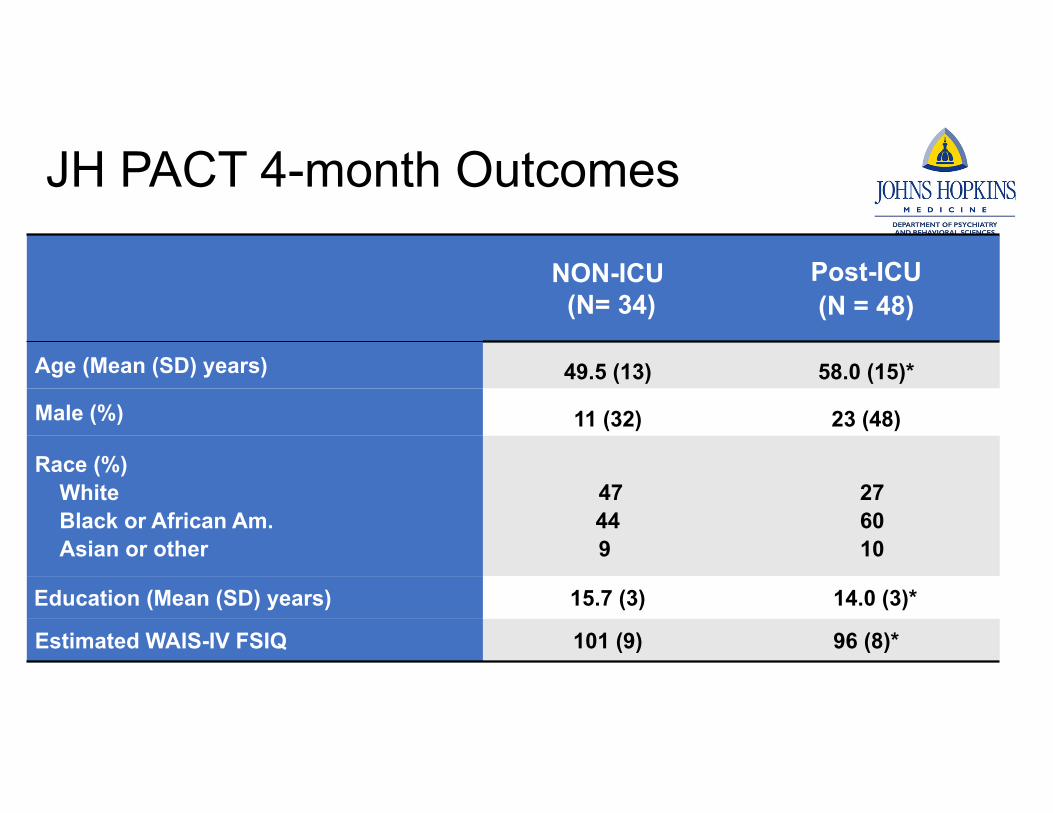
JH PACT 4-month Outcomes
NON-ICU(N= 34)
Post-ICU(N = 48)
Age (Mean (SD) years) 49.5 (13) 58.0 (15)*
Male (%) 11 (32) 23 (48)
Race (%)WhiteBlack or African Am.Asian or other
47449
276010
Education (Mean (SD) years) 15.7 (3) 14.0 (3)*
Estimated WAIS-IV FSIQ 101 (9) 96 (8)*

Age-adjusted Standard Scores
To ask a question: please use the Q&A feature to direct any questions to one of the moderators, Julia Maietta or Alexander Tan.
75
80
85
90
95
100
105
110
115
RAVLTAcquisition
(n = 82)
RAVLTDelayedRecall
(n = 82)
Oral TrailMaking Test
Part A(n = 82)
Oral TrailMaking Test
Part B(n = 77)
Number SpanForward(n = 82)
Number SpanBackward(n = 82)
Letter-cuedVerbal Fluency
(n = 81)
Category-cuedVerbal Fluency
(n = 81)
CognitiveComposite
(n = 82)
Non-ICU Post-ICU

Rates of Low Scores
To ask a question: please use the Q&A feature to direct any questions to one of the moderators, Julia Maietta or Alexander Tan.
0
10
20
30
40
50
60
70
80
90
100
Learning(n = 82)
Memory(n = 82)
ProcessingSpeed
(n = 82)
ExecutiveFunction(n = 77)
Attention(n = 82)
WorkingMemory(n = 82)
Letter-cuedVerbal Fluency
(n = 81)
Category-cuedVerbal Fluency
(n = 81)
CognitiveComposite
(n = 82)
Severe Mild/Moderate Normal
67% of PACT patients showed mild/moderate cognitive deficit on ≥ 1 test
≥2 scores mild/mod impaired:32% Non‐ICU58% Post‐ICU
≥2 scores severely impaired:15% Non‐ICU31% Post‐ICU

Mental Health & Functional Decline
To ask a question: please use the Q&A feature to direct any questions to one of the moderators, Julia Maietta or Alexander Tan.
NON-ICU(N= 34)
Post-ICU(N = 48)
Domain Tool % above threshold % above threshold
Mild Moderate Mild Moderate
Depression PHQ-9 68 29 67 19
Anxiety GAD-7 53 15 48 15
PTSD IES-6 -- -- 25
Fx Decline QDRS 62 18 69 13
78% reported mild elevations on ≥ 1 measure35% reported moderate elevations on ≥ 1 Measure

JH PACT Key Findings at ~4 months post-COVID-19
⁍ 67% show dysfunction in ≥1 domain of cognition⁍ Processing speed, verbal fluency, learning, memory deficits are
common
⁍ Dysfunction frequently occurs in both Post-ICU & Non-ICU pts⁍ Post-ICU impairments are more severe and broad relative to non-ICU
⁍ Substantial mental health and functional impairments⁍ Clinically meaningful levels of psychiatric distress and/or decline
reported by ≥35% of patients

• Cross-sectional, retrospective study of 88 clinically-referred patients
• Across 4 sites (3 US, 1 European) and 3 languages (English, Spanish, German)
• Excluded those with prior dementia & low effort
Under Review
• 48%-71% were unable to return to work at baseline capacity (mean 7 mos. post-COVID-19)
• 0% to 71% lost employment
Long-term neuropsychological outcomes of COVID-19: A multicenter, cross-cultural study
Christina D. Kay, PhD*1, Ana Sofia Costa, PhD*2,3, Tracy D. Vannorsdall, PhD4,5, Paula Aduen,PhD6, Clara Vila-Castelar, PhD6, Sarah M. Burstein, BA1, Lauren Pollak, PhD1, Daniel K. Leibel, PhD4, Janet C. Sherman, PhD1, Julia Bungenberg, MD2, Kathrin Reetz, MD2,3, Yakeel T. Quiroz, PhD6

WHO Recommendations for Clinical Management of Cognitive & Neuropsychiatric Symptoms
• Cognition• Education should be provided, and advice on strategies to help establish expectations and to alleviate stress and anxiety
• Cognitive restorative rehabilitation may support with cognitive exercises and compensation tools and breaking down activities
• Encourage participation in daily activities that are meaningful for the patient
• Psychiatric symptoms• Basic mental health and psychosocial support by appropriately trained health or non‐health workers should be provided.

Management of Neuropsychiatric Symptoms Post‐COVID‐19
Very little COVID‐specific research thus far
• The critical illness literature suggests that multi‐modal rehab (including cognitive rehab) improves executive functioning and disability following hospitalization (e.g., Jackson et al, Critical Care Med, 2012)
• A 6‐week rehabilitation program starting 125 days post‐COVID‐19 diagnosis(Daynes et al., Chronic Respiratory Disease, 2021)
• Psychoeducation on emotional and cognitive changes, sleep, etc. from https://www.yourcovidrecovery.nhs.uk/
• Pre‐rehab MoCA 25/30 (SD 3), Post‐rehab = 27/30 (SD = 2), p < 0.01, exceeds minimal important difference for pulmonary rehab patients

Psychoeducation Behavioral activation
Cognitive approaches
Goal setting Diaries Relaxation training
Self‐care
Increase understanding and setting expectations
Scheduling enjoyable and important activities
Reframing exercises
SMARTSpecific MeasurableAttractive/action orientedRealisticTime‐bound
Aid understanding of patterns of antecedents, behaviors, and consequences
Progressive muscle relaxationMindfulness mediation
Sleep hygieneNutrition, Physical activitySocialization
Management of Cognitive & Neuropsychiatric Symptoms Post‐COVID‐19

Cognitive and Mental Health Referral Resources
American Academy of Clinical Neuropsychology • https://theaacn.org/directory/
Rehabilitation Psychology• https://abpp.org/Directory

Future Work
⁍ Characterization ⁍ Large, longitudinal studies of neuropsychological and functional
outcomes relative to well-matched controls are ongoing ⁍ https://c4r‐nih.org⁍ https://g2aging.org⁍ https://hrs.isr.umich.edu⁍ https://www.recovercovid.org/
⁍ Treatment studies⁍ What cognitive remediation and mental health interventions work? ⁍ For whom? ⁍ When?⁍ What are the critical elements?
Acknowledgements
Ann Parker, MD PHDAlly Gorgone, MSKostas Lyketsos, MD MHSEsther Oh, MD PhDAnupama Kumar, MBBSDaniel Leibel, PhDEmily Duggan, PhDNeuroCOVID International Neuropsychology Taskforce
NIH: K23ES029105, K23HL138206, K12HL143957, R01AG057725
Johns Hopkins Alzheimer’s Disease Research Center (P30AG066507)
The Richman Precision Medicine Center of Excellence in Alzheimer’s Disease

















![Light therapy for managing cognitive, sleep, functional ... · [Intervention Review] Light therapy for managing cognitive, sleep, functional, behavioural, or psychiatric disturbances](https://img.pdfslide.net/doc/110x75/5f16ae12df4c3207b02ccd6b/light-therapy-for-managing-cognitive-sleep-functional-intervention-review.jpg)










