Embed Size (px)
Citation preview

Persistence of Nutritional Deficiencies afterShort-term Weight Recovery in Adolescents
with Anorexia Nervosa
Josefina Castro,1* Ramon Deulofeu,2 Araceli Gila,1 Josefina Puig,1 and Josep Toro1
1 Eating Disorders Unit, Department of Child and Adolescent Psychiatry and Psychology,Institute of Psychiatry and Psychology, Hospital Clınic Universitari Barcelona,
IDIBAPS, Spain2Department of Clinical Chemistry, CDB (Centre de Diagnostic Biomedic), IDIBAPS(Institute de Investigacio Biomedica August Pi Sunyer), Hospital Clınic Universitari,
Barcelona, Spain
Accepted 14 April 2003
Abstract: Objectives: To study nutritional abnormalities in adolescent anorexia nervosa andto establish whether certain abnormalities persist after short-term refeeding. Method: Sixty-one patients (10–19 years old) admitted to a reference unit for eating disorders between 1999and 2000 with a diagnosis of anorexia nervosa were evaluated at admission and at dis-charge. A range of biochemical, nutritional, and hormonal parameters were determined.Results: At admission, no protein or lipid deficiencies were found, although many patientspresented with hormonal abnormalities and red blood cell folate and zinc deficiencies.Hormonal abnormalities reverted significantly (p < .000) after renutrition. There weredecreases in erythrocytes and in levels of hemoglobin (p < .000) and folic acid (p < .05).Red blood cell folate and zinc increased but did not reach normal levels. Conclusions: In alarge proportion of adolescent anorexic patients, supplementation of folic acid and zinc isrecommended although protein or hormonal replacement does not seem to be necessary.# 2004 by Wiley Periodicals, Inc. Int J Eat Disord 35: 169–178, 2004.
Key words: nutritional deficiencies; anorexia nervosa; adolescents
INTRODUCTION
Malnutrition in anorexia nervosa patients can be severe but assessment of nutritionalstatus yielded inconsistent and sometimes contradictory results. This may be due to hetero-geneity in age and the duration of the disorder or to the small sample size in some studies(Langan & Farrell, 1985; Rock & Curran-Celentano, 1994; Rock & Vasantharajan, 1995; VanBinsbergen, Coelingh Bennink, Odink, Haspels, & Koppeschaar, 1990). Among the features
*Correspondence to: Josefina Castro, M.D., Department of Child and Adolescent Psychiatry and Psychology,Institute of Psychiatry and Psychology, Hospital Clınic Universitari, Sabino de Arana, 1, Barcelona 08028, Spain.E-mail: [email protected] online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/eat.10249
# 2004 by Wiley Periodicals, Inc.

most commonly described are anemia and leukopenia (Brotman, Rigotti, & Herzog, 1985;Lambert et al., 1997), which appear to be related to bone marrow changes, although themechanisms involved are not well known at present (Geiser et al., 2001). However, thesehematologic abnormalities are not seen in all studies (Van Binsbergen, Odink, Van den Berg,Koppeschaar, & Coelingh Benninck, 1988). Protein levels are also normal in many cases(Rigaud et al., 1989), albeit in the low to normal range.
Impairment of micronutrient status, especially iron and zinc, is also frequent (Casper,Kirschner, Sandstead, Jacob, & Davis, 1980; Humphries, Vivian, Stuart, & McClain, 1989;Katz et al., 1987; McClain et al., 1992), but reports of highly abnormal levels of vitamins(except for folic acid) are surprisingly rare (Langan & Farrell, 1985; Philipp et al., 1988;Van Binsbergen et al., 1988). A thiamin deficit was found in 19% of a sample of adultanorexics (Winston, Jamieson, Madira, Gatward, & Palmer, 2000), and it is common tofind high carotene concentrations (Boland, Beguin, Zech, Desager, & Lambert, 2001;Curran-Celentano, Erdman, Nelson, & Grater, 1985). Nevertheless, many of these studieswere carried out with adult anorexics with a long duration of the disorder and it is notclear whether young adolescents, in whom the evolution time of the disorder is shorter,present marked biochemical and nutritional deficiencies.
Endocrine abnormalities are also common in malnourished anorexia nervosa patients,especially low levels of thyroid hormones (Curran-Celentano et al., 1985; Kiyoara, Tamai,Takaichi, Nakagawa, & Kumagai, 1989) and insulin-like growth factor-I (IGF-I) and itsbinding protein 3 (IGBP-3; Argente et al., 1997; Caregaro et al., 2001; Counts, Gwirtsman,Carlsson, Lesem, &Cutler, 1992; Heer,Mika, Grzella, Drummer, &Herpertz-Dahlmann, 2002;Stoving et al., 1999). Among the most frequent alterations in anorexia nervosa are abnormal-ities of the hypothalamic-pituitary-gonadal axis, and impairment of the gonadotropin secre-tion pattern, which is similar to that of the prepubertal stage (Van Binsbergen et al., 1990).
The majority of studies are cross-sectional, making it impossible to establish whethervitamins or other micronutrients normalize after weight recovery or whether special nutri-tional supplements may be necessary (Kennedy & Shapiro, 1993). In this respect, Rock andVasantharajan (1995) found a normalization of vitamin abnormalities in 13 patients withrenutrition in about 2–6 weeks. Caregaro et al. (2001) found a prompt recovery of IGF-I in 20adult anorexic patients after a short-termweight increase. In a study of 33 eating-disorderedpatients, McClain et al. (1992) reported that zinc supplementation during hospitalizationincreased their plasma zinc level significantly in comparison to patients without supple-mentation. Nevertheless, no clear guidelines have yet been published for vitamins or tracemetals or other micronutrient supplementation in young patients with anorexia nervosa(American Psychiatric Association [APA], 2000; Steiner & Lock, 1998).
The objective of the current study was to determine whether adolescent patients with ashort duration of anorexia nervosa have abnormal biochemical, nutritional, and hormonalparameters andwhether these alterationsmay be reversed after short-termweight recovery.The results of the current study will allow us to establish the rationale for using vitamin orother micronutrient supplementation along with normal refeeding during hospitalization.
METHOD
Subjects and Procedures
The group of patients comprised 61 children and adolescents aged 10–19 years whofulfilled the diagnostic criteria for anorexia nervosa as outlined in the 4th ed. of the
170 Castro et al.
Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; APA, 1994). All patientswere admitted consecutively as inpatients between March 1999 and June 2000 to theEating Disorders Unit, Hospital Clınic Universitari (Barcelona, Spain). Clinical character-istics were recorded. Laboratory data were collected at admission and at discharge aspart of the normal follow-up procedures for anorexia nervosa patients. Parents andpatients were told why biochemical and hormonal parameters were being measured.Study procedures were approved by the ethics committee of the institution. Patients withconcomitant disease besides anorexia nervosa or patients receiving hormonal therapy orany vitamin complex at admission were excluded from the analysis.
During hospitalization, all patients initially received a complete diet of about 1,250calories per day, which increased progressively to 2,500 calories per day. However, theydid not receive vitamin or mineral supplements or any hormonal replacement therapy.The minimum weight increase per week required during hospitalization is 900 g, whichis achieved through a behavioral treatment program. Providing this minimum is reached,patients can decide freely the amount of food intake and if they prefer a somewhat higherrate of weight gain. Many patients with positive attitudes to admission and weightrecovery have achieved increases of 2–2.5 kg per week. Treatment during admission isbased on a multidisciplinary approach combining biologic management, nutritionalrehabilitation, a behavioral program aimed to improve eating patterns and weight,individual and group cognitive treatment, and individual and group parent counseling.The hospitalization program establishes that during admission, weight must increase atleast until a body mass index (BMI) of 17.5 is achieved before patients are released tooutpatient treatment. During follow-up, patients must achieve a normal BMI for sex andage. In young adolescents, a normal BMI is somewhat lower than in adult subjects andusually varies from 18.5 to 20.5 (Hernandez, Sanchez & Sobradillo, 2000).
Laboratory Tests
The biochemical and hematologic tests carried out at admission and at dischargeincluded all standard biochemical data, nutritional parameters, total proteins, prealbu-min, ions (potassium, sodium, magnesium, phosphorus, calcium, iron, and zinc), vita-mins (vitamins B1, B6, B12, C, E, and a-carotene and b-carotene), folic acid, red blood cellfolate, a complete hemogram (including a red blood cell count, hemoglobin, and aleukocyte and platelet count), and endocrine parameters such as cortisol, triiodothyro-nine (T3), thyroxin (T4), thyrotropin (TSH), IGF-I, IGFBP-3, and growth hormone (GH).All samples were taken in the morning. Gonadotropin levels were not considered for thecurrent study because they have been studied extensively elsewhere (Fichter, 1992) andbecause 14 (24.1%) of the female patients were still prepubertal.
Standard biochemical and hematologic parameters were measured in an OlympusAU450 analyzer (Cormedica, Barcelona, Spain) using Olympus reagents. Vitamin B12and folic acid were measured by immunoassay using an automated Immuno 1 systemfrom Bayer (Quimica Farmaceutica Bayer, Barcelona, Spain). Vitamins B1 and B6 weremeasured by high-performance liquid chromatography (HPLC) using reagents suppliedby Chromsystems (Munich, Germany). Vitamin C was measured by HPLC by fluoro-metric detection. Vitamin E and carotenes were measured by HPLC using ultraviolet(UV) and visible detection, respectively. Hematologic parameters were measured in anAdvia hematology analyzer (Quimica Farmaceutica Bayer). Cortisol, GH, IGF-1, andIGFBP3 were measured by commercially available radioimmunoassay as routinely meas-ured at our institution.
Nutritional Deficiencies in Anorexia Nervosa 171
Statistical Analysis
Differences between mean initial values and follow-up measurements were analyzedusing the Student’s t test for paired samples. The McNemar test was used to compare theincidence of abnormal parameters in the first and second determinations. The level ofstatistical significance was p < .05. Statistical analysis was performed using the SPSSpackage (Norusis, 1993).
RESULTS
General Characteristics
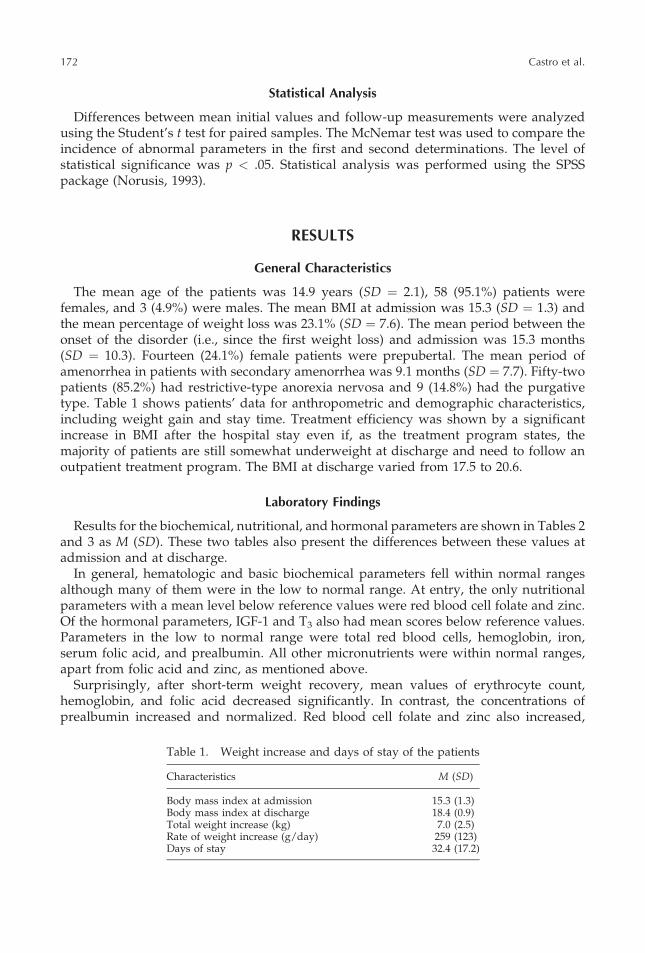
The mean age of the patients was 14.9 years (SD ¼ 2.1), 58 (95.1%) patients werefemales, and 3 (4.9%) were males. The mean BMI at admission was 15.3 (SD ¼ 1.3) andthe mean percentage of weight loss was 23.1% (SD ¼ 7.6). The mean period between theonset of the disorder (i.e., since the first weight loss) and admission was 15.3 months(SD ¼ 10.3). Fourteen (24.1%) female patients were prepubertal. The mean period ofamenorrhea in patients with secondary amenorrhea was 9.1 months (SD ¼ 7.7). Fifty-twopatients (85.2%) had restrictive-type anorexia nervosa and 9 (14.8%) had the purgativetype. Table 1 shows patients’ data for anthropometric and demographic characteristics,including weight gain and stay time. Treatment efficiency was shown by a significantincrease in BMI after the hospital stay even if, as the treatment program states, themajority of patients are still somewhat underweight at discharge and need to follow anoutpatient treatment program. The BMI at discharge varied from 17.5 to 20.6.
Laboratory Findings
Results for the biochemical, nutritional, and hormonal parameters are shown in Tables 2and 3 as M (SD). These two tables also present the differences between these values atadmission and at discharge.
In general, hematologic and basic biochemical parameters fell within normal rangesalthough many of them were in the low to normal range. At entry, the only nutritionalparameters with a mean level below reference values were red blood cell folate and zinc.Of the hormonal parameters, IGF-1 and T3 also had mean scores below reference values.Parameters in the low to normal range were total red blood cells, hemoglobin, iron,serum folic acid, and prealbumin. All other micronutrients were within normal ranges,apart from folic acid and zinc, as mentioned above.
Surprisingly, after short-term weight recovery, mean values of erythrocyte count,hemoglobin, and folic acid decreased significantly. In contrast, the concentrations ofprealbumin increased and normalized. Red blood cell folate and zinc also increased,
Table 1. Weight increase and days of stay of the patients
Characteristics M (SD)
Body mass index at admission 15.3 (1.3)Body mass index at discharge 18.4 (0.9)Total weight increase (kg) 7.0 (2.5)Rate of weight increase (g/day) 259 (123)Days of stay 32.4 (17.2)
172 Castro et al.
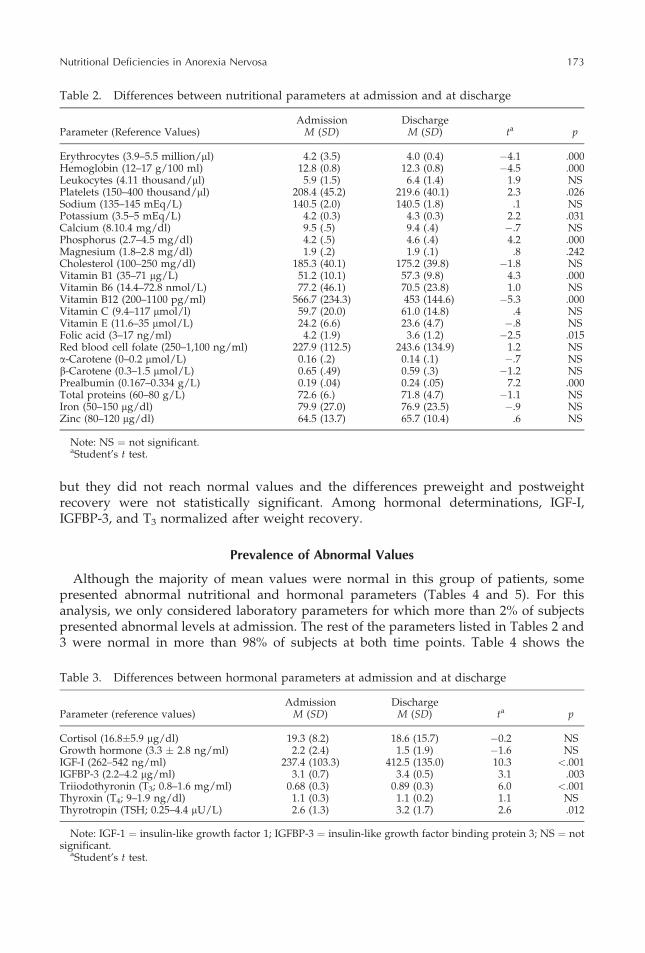
but they did not reach normal values and the differences preweight and postweightrecovery were not statistically significant. Among hormonal determinations, IGF-I,IGFBP-3, and T3 normalized after weight recovery.
Prevalence of Abnormal Values
Although the majority of mean values were normal in this group of patients, somepresented abnormal nutritional and hormonal parameters (Tables 4 and 5). For thisanalysis, we only considered laboratory parameters for which more than 2% of subjectspresented abnormal levels at admission. The rest of the parameters listed in Tables 2 and3 were normal in more than 98% of subjects at both time points. Table 4 shows the
Table 2. Differences between nutritional parameters at admission and at discharge
Admission DischargeParameter (Reference Values) M (SD) M (SD) ta p
Erythrocytes (3.9–5.5 million/ml) 4.2 (3.5) 4.0 (0.4) �4.1 .000Hemoglobin (12–17 g/100 ml) 12.8 (0.8) 12.3 (0.8) �4.5 .000Leukocytes (4.11 thousand/ml) 5.9 (1.5) 6.4 (1.4) 1.9 NSPlatelets (150–400 thousand/ml) 208.4 (45.2) 219.6 (40.1) 2.3 .026Sodium (135–145 mEq/L) 140.5 (2.0) 140.5 (1.8) .1 NSPotassium (3.5–5 mEq/L) 4.2 (0.3) 4.3 (0.3) 2.2 .031Calcium (8.10.4 mg/dl) 9.5 (.5) 9.4 (.4) �.7 NSPhosphorus (2.7–4.5 mg/dl) 4.2 (.5) 4.6 (.4) 4.2 .000Magnesium (1.8–2.8 mg/dl) 1.9 (.2) 1.9 (.1) .8 .242Cholesterol (100–250 mg/dl) 185.3 (40.1) 175.2 (39.8) �1.8 NSVitamin B1 (35–71 mg/L) 51.2 (10.1) 57.3 (9.8) 4.3 .000Vitamin B6 (14.4–72.8 nmol/L) 77.2 (46.1) 70.5 (23.8) 1.0 NSVitamin B12 (200–1100 pg/ml) 566.7 (234.3) 453 (144.6) �5.3 .000Vitamin C (9.4–117 mmol/l) 59.7 (20.0) 61.0 (14.8) .4 NSVitamin E (11.6–35 mmol/L) 24.2 (6.6) 23.6 (4.7) �.8 NSFolic acid (3–17 ng/ml) 4.2 (1.9) 3.6 (1.2) �2.5 .015Red blood cell folate (250–1,100 ng/ml) 227.9 (112.5) 243.6 (134.9) 1.2 NSa-Carotene (0–0.2 mmol/L) 0.16 (.2) 0.14 (.1) �.7 NSb-Carotene (0.3–1.5 mmol/L) 0.65 (.49) 0.59 (.3) �1.2 NSPrealbumin (0.167–0.334 g/L) 0.19 (.04) 0.24 (.05) 7.2 .000Total proteins (60–80 g/L) 72.6 (6.) 71.8 (4.7) �1.1 NSIron (50–150 mg/dl) 79.9 (27.0) 76.9 (23.5) �.9 NSZinc (80–120 mg/dl) 64.5 (13.7) 65.7 (10.4) .6 NS
Note: NS ¼ not significant.aStudent’s t test.
Table 3. Differences between hormonal parameters at admission and at discharge
Admission DischargeParameter (reference values) M (SD) M (SD) ta p
Cortisol (16.8�5.9 mg/dl) 19.3 (8.2) 18.6 (15.7) �0.2 NSGrowth hormone (3.3 � 2.8 ng/ml) 2.2 (2.4) 1.5 (1.9) �1.6 NSIGF-I (262–542 ng/ml) 237.4 (103.3) 412.5 (135.0) 10.3 <.001IGFBP-3 (2.2–4.2 mg/ml) 3.1 (0.7) 3.4 (0.5) 3.1 .003Triiodothyronin (T3; 0.8–1.6 mg/ml) 0.68 (0.3) 0.89 (0.3) 6.0 <.001Thyroxin (T4; 9–1.9 ng/dl) 1.1 (0.3) 1.1 (0.2) 1.1 NSThyrotropin (TSH; 0.25–4.4 mU/L) 2.6 (1.3) 3.2 (1.7) 2.6 .012
Note: IGF-1 ¼ insulin-like growth factor 1; IGFBP-3 ¼ insulin-like growth factor binding protein 3; NS ¼ notsignificant.
aStudent’s t test.
Nutritional Deficiencies in Anorexia Nervosa 173
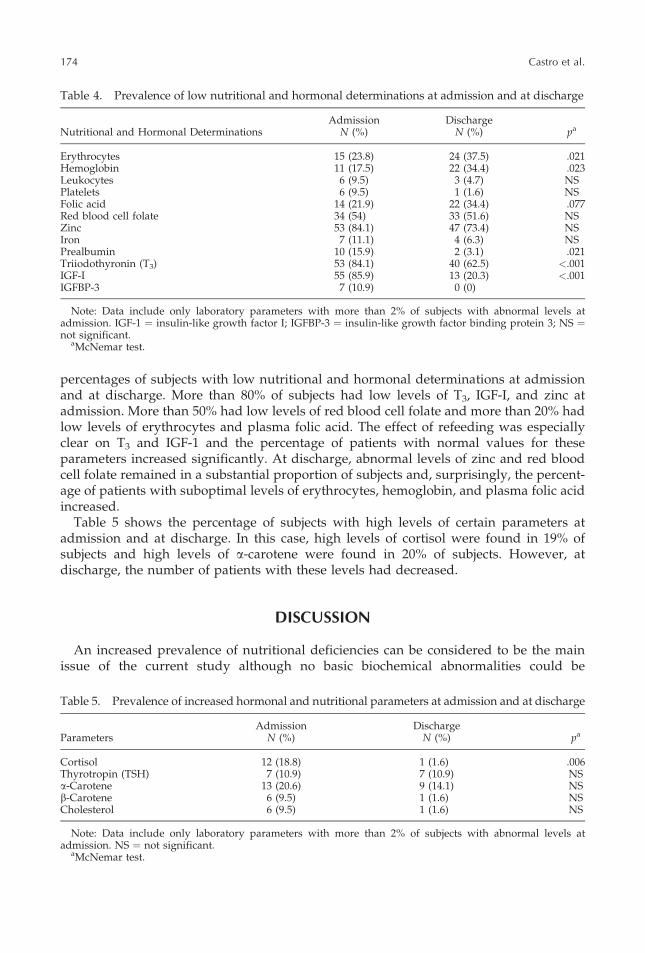
percentages of subjects with low nutritional and hormonal determinations at admissionand at discharge. More than 80% of subjects had low levels of T3, IGF-I, and zinc atadmission. More than 50% had low levels of red blood cell folate and more than 20% hadlow levels of erythrocytes and plasma folic acid. The effect of refeeding was especiallyclear on T3 and IGF-1 and the percentage of patients with normal values for theseparameters increased significantly. At discharge, abnormal levels of zinc and red bloodcell folate remained in a substantial proportion of subjects and, surprisingly, the percent-age of patients with suboptimal levels of erythrocytes, hemoglobin, and plasma folic acidincreased.
Table 5 shows the percentage of subjects with high levels of certain parameters atadmission and at discharge. In this case, high levels of cortisol were found in 19% ofsubjects and high levels of a-carotene were found in 20% of subjects. However, atdischarge, the number of patients with these levels had decreased.
DISCUSSION
An increased prevalence of nutritional deficiencies can be considered to be the mainissue of the current study although no basic biochemical abnormalities could be
Table 4. Prevalence of low nutritional and hormonal determinations at admission and at discharge
Admission DischargeNutritional and Hormonal Determinations N (%) N (%) pa
Erythrocytes 15 (23.8) 24 (37.5) .021Hemoglobin 11 (17.5) 22 (34.4) .023Leukocytes 6 (9.5) 3 (4.7) NSPlatelets 6 (9.5) 1 (1.6) NSFolic acid 14 (21.9) 22 (34.4) .077Red blood cell folate 34 (54) 33 (51.6) NSZinc 53 (84.1) 47 (73.4) NSIron 7 (11.1) 4 (6.3) NSPrealbumin 10 (15.9) 2 (3.1) .021Triiodothyronin (T3) 53 (84.1) 40 (62.5) <.001IGF-I 55 (85.9) 13 (20.3) <.001IGFBP-3 7 (10.9) 0 (0)
Note: Data include only laboratory parameters with more than 2% of subjects with abnormal levels atadmission. IGF-1 ¼ insulin-like growth factor I; IGFBP-3 ¼ insulin-like growth factor binding protein 3; NS ¼not significant.
aMcNemar test.
Table 5. Prevalence of increased hormonal and nutritional parameters at admission and at discharge
Admission DischargeParameters N (%) N (%) pa
Cortisol 12 (18.8) 1 (1.6) .006Thyrotropin (TSH) 7 (10.9) 7 (10.9) NSa-Carotene 13 (20.6) 9 (14.1) NSb-Carotene 6 (9.5) 1 (1.6) NSCholesterol 6 (9.5) 1 (1.6) NS
Note: Data include only laboratory parameters with more than 2% of subjects with abnormal levels atadmission. NS ¼ not significant.
aMcNemar test.
174 Castro et al.
observed. Probably, these findings are due to the finding that many parameters are understrict homeostatic control and are unlikely to be altered without longer-term deficienciesor until organ damage occurs. In our study, patients were very young and the duration ofstarvation or nutritional restrictions was relatively short. Low levels of red blood cellcounts, leukocytes, and platelets in anorexia nervosa patients have been reported bysome investigators (Lambert et al., 1997), but not by othersl (Van Binsbergen et al., 1988).In our sample, at admission, there were more patients with low levels of erythrocytes andhemoglobin than with low levels of leukocytes and platelets. Furthermore, after short-term weight recovery, the percentage of patients with low levels of leukocytes andplatelets decreased, whereas the percentage of patients with low levels of erythrocytesand hemoglobin increased. Initial hemoconcentration and subsequent rehydration maycause variations in red blood cell counts (Lambert & Lau, 1976). The plasma level of folicacid was in the low to normal range and red blood cell folate was clearly below thenormal level. These factors may have an important role in the development of anemia.After refeeding, the percentage of patients with low levels of red blood cell folate was stillvery high and the percentage of patients with abnormal plasma folic acid levelsincreased, suggesting the need for extra folic acid supplementation during renutrition.Other authors have pointed out the possibility of a folate deficiency in adolescents withanorexia nervosa (Moyano, Vilaseca, Artuch, Valls, & Lambruschini, 1998). Folate defi-ciency has also been related to depressive symptoms in several psychiatric disorders,including anorexia nervosa (Abou-Saleh & Coppen, 1986). It seems that a supplementa-tion of folic acid may be appropriate for management of this group of patients. Althoughfew subjects had low serum levels of iron (11%) and the mean level was normal, althoughin the low range , iron supplementation may be indicated in these patients to avoid irondeficiency during folic acid supplementation.
With the exception of folic acid, no absolute vitamin deficiency was seen in the currentstudy, which may be due to the finding that the subjects were adolescents with a shortduration of the disorder. Other authors have not found vitamin abnormalities in anorexianervosa patients (Van Binsbergen et al., 1988) and Roch and Vasantharajan (1995) foundsuboptimal vitamin status in 4 of 13 patients, which normalized after short-term refeed-ing. Winston et al. (2000) found a thiamin deficiency in about 19% of 37 adult anorexicpatients, but this was not the case in the current study. Serum concentrations ofa-carotene were high in 20% of subjects at admission. Other studies have found thata-carotene levels were significantly higher in patients with a greater degree of eatingpathology (Rock, Gorenflo, Drewnowski, & Demitrac, 1996). The percentage of subjectswith high b-carotene levels was lower than in other studies (Boland et al., 2001), althoughin our country, mean serum values of carotenes are lower than in other Caucasianpopulations (Olmedilla, Granado, Gil-Martinez, Blanco, & Rojas-Hidalgo, 1997).
Total protein levels were normal in all patients at admission and at discharge. However,prealbumin, the most sensitive marker of protein depletion, was low in 16% of patients atadmission. Low prealbumin levels are never found in healthy adolescents. Only 3% ofpatients had abnormal prealbumin levels at discharge, demonstrating the efficacy of therefeeding strategy for protein status. Russell et al. (1994) also found that anorexic patientsreadily replenish protein during refeeding. Rigaud et al. (1989) concluded that proteinmarkers are not sensitive to malnutrition in anorexia nervosa. However, this may havebeen because they considered only total proteins and albumin does not react so fast in thissituation, due to the fact that prealbumin and albumin have a half-life of 48 hr and 19 days,respectively (Tietz, 1994). In adult anorexic patients, low serum albumin levels may predicta lethal or chronic course of the disorder (Herzog, Deter, Fiehn, & Petzold, 1997).
Nutritional Deficiencies in Anorexia Nervosa 175

Zinc is a very important ion in many cell processes and in brain homeostasis (Fredickson,1989). Low levels and the lack of recovery after the refeeding period suggest theneed to accelerate zinc recovery with supplementation. Other studies have found lowlevels of zinc in anorexic patients, which did not increase with short-term renutrition ifsupplementation was not given (McClain et al., 1992). It has been suggested that zincdeficiency may be one of the factors that caused altered eating behavior, anxiety, anddepressive symptoms to persist (Humphries et al., 1989; Katz et al., 1987). In otherpopulations, such as elite athletes, unusual nutritional habits may also lead to suboptimalzinc intake and mild zinc deficiency (Micheletti, Rossi, & Rufini, 2001). It is well knownthat zinc deficiency may induce anorexia, weight loss, ageusia, hair loss, and moodchanges.
The hormones most likely to present abnormalities seem to be T3 and IGF-I, as otherstudies have pointed out (Argente et al., 1997; Caregaro et al., 2001; Counts et al., 1992;Heer et al. 2002). Low levels of T3 and IGF-1 are found in the majority of patients withmalnutrition, but with weight recovery, levels of T3 and IGF-I return to normal values inthe short term. Recovery of IGF-I may be related to bone formation and to the improve-ment in bone mass (Castro, Lazaro, Pons, Halperin, & Toro, 2001; Heer et al., 2002).
In summary, a great percentage of adolescent patients presented with nutritional andhormonal abnormalities, although none had severe vitamin deficiencies. It seems that themost persistent abnormalities after short-term weight recovery in adolescents with anor-exia nervosa are low levels of erythrocytes, hemoglobin, folic acid, and zinc. Further-more, folic acid deficiency may account for the persistence of anemia. Otherabnormalities tend to normalize fast after short-term refeeding and, therefore, it doesnot seem advisable to add protein or vitamin supplementations to the normal diet. Themain conclusion is that supplements of folic acid, iron, and zinc could be beneficial torapidly compensate for deficiencies that cannot be recovered only with short standardnutrition programs. These supplements may ameliorate anemia and folate and zincdeficiencies and improve certain psychological abnormalities. Further controlled studiesof the effects of these supplements on both physical and psychological symptomatologywould be of great interest.
REFERENCES
Abou-Saleh, M.T., & Coppen, A. (1986). The biology of folate in depression: Implications for nutritionalhypotheses of the psychoses. Journal of Psychiatric Research, 20, 91–101.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.).Washington, DC: Author.
American Psychiatric Association. (2000). Practice guidelines for the treatment of patients with eating disorders.American Journal of Psychiatry, 157 (Suppl.).
Argente, J., Caballo, N., Barrios, V., Munoz, M.T., Pozo, J., Chowen, J.A., Morande, G., & Hernandez, M. (1997).Multiple endocrine abnormalities of the growth hormone and insulin-like growth factor axis in patients withanorexia nervosa: Effect of short- and long-term weight recuperation. Journal of Clinical Endocrinology andMetabolism, 82, 2084–2092.
Boland, B., Beguin, C., Zech, F., Desager, J.P., & Lambert, M. (2001). Serum beta-carotene in anorexia nervosapatients: A case control study. International Journal of Eating Disorders, 30, 299–305.
Brotman, A.W., Rigotti, N., & Herzog, D.B. (1985). Medical complications of eating disorders: Outpatientevaluation and management. Comprehensive Psychiatry, 26, 258–272.
Caregaro, L., Favaro, A., Santonastaso, P., Alberino, F., Di Pascoli, L., Nardi, M., Favaro, S., & Gatta, A. (2001).Insulin-like growth factor 1 (IGF-1), a nutritional marker in patients with eating disorders. Clinical Nutrition,20, 251–257.
Casper, R.C., Kirschner, B., Sandstead, H.H., Jacob, R.A., & Davis, J.M. (1980). An evaluation of trace metals,vitamins, and taste function in anorexia nervosa. American Journal of Clinical Nutrition, 33, 1801–1808.
176 Castro et al.
Castro, J., Lazaro, L., Pons, F., Halperin, I., & Toro, J. (2001). Adolescent anorexia nervosa: The catch-up effect inbone mineral density after recovery. Journal of the American Academy of Child and Adolescent Psychiatry,40, 1215–1221.
Counts, D.R., Gwirtsman, H., Carlsson, L.M., Lesem, N., & Cutler, G.B., Jr. (1992). The effect of anorexia nervosaand refeeding on growth hormone-binding protein, the insulin-like growth factors (IGFs), and the IGF-binding proteins. Journal of Clinical Endocrinology and Metabolism, 75, 762–767.
Curran-Celentano, J., Erdman, J.W., Jr., Nelson, R.A., & Grater, S.J. (1985). Alterations in vitamin A and thyroidhormone status in anorexia nervosa and associated disorders. American Journal of Clinical Nutrition, 42,1183–1191.
Fichter, M.M. (1992). Starvation-related endocrine changes. In: Halmi, K.A. (Ed.), Psychobiology and treatmentof anorexia nervosa and bulimia nervosa. Washington, D.C., American Psychiatric Press, Inc, pp. 193–219.
Fredickson, C.J. (1989). Neurobiology of zinc and zinc-containing neurons. International Review of Neurobiol-ogy, 31, 145–238.
Geiser, F., Murtz, P., Lutterbey, G., Traber, F., Block, W., Imbierowicz, D., Schilling, G., Schild, H., & Liedtke, R.(2001). Magnetic resonance spectroscopic and relaxometric determinations of bone marrow changes inanorexia nervosa. Psychosomatic Medicine, 63, 631–637.
Heer, M., Mika, C., Grzella, I., Drummer, Ch., & Herpertz-Dahlmann, B. (2002). Changes in bone turnover inpatients with anorexia nervosa during eleven weeks of inpatient dietary treatment. Clinical Chemistry, 48,754–760.
Hernandez, M., Sanchez, E., & Sobradillo, B. (2000) Curvas y tablas de crecimiento (Growth tables). In Argente, J.,Carrascosa, A., Gracia, R., & Rodrıguez-Hierro, F. (Eds.), Tratado de Endocrinologıa pediatrica y de laadolescencia [Child and Adolescent Endocrinology]. Second edition. Barcelona: Doyma, S.A. pp. 1441–1500.
Herzog, W., Deter, H.C., Fiehn, W., & Petzold, E. (1997). Medical findings and predictiors of long-term physicaloutcome in anorexia nervosa: A prospective, 12-year follow-up study. Psychological Medicine, 27, 269–279.
Humphries, L., Vivian, B., Stuart, M., & McClain, C.J. (1989). Zinc deficiency and eating disorders. Journal ofClinical Psychiatry, 50, 456–459.
Katz, R.L., Keen, C.L., Litt, I.F., Hurley, L.S., Kellams-Harrison, K.M., & Glader, L.J. (1987). Zinc deficiency inanorexia nervosa. Journal of Adolescent Health Care, 8, 400–406.
Kennedy, S.H., & Shapiro, C. (1993). Medical management of the hospitalized patient. In A.S. Kaplan & P.E. Garfinkel(Eds.), Medical issues and the eating disorders. The interface (pp. 213–238). New York: Brunner/Mazel.
Kiyohara, K., Tamai, H., Takaichi, Y., Nakagawa, T., & Kumagai, L.F. (1989). Decreased thyroidal triiodothyr-onine secretion in patients with anorexia nervosa: Influence of weight recovery American Journal of ClinicalNutrition, 50, 767–772.
Lambert, F., & Lau, B. (1976). Bone marrow hypoplasia in anorexia nervosa. European Journal of Pediatrics, 124,65–71.
Lambert, M., Hubert, C., Depresseux, G., Vande Berg, B., Thissen, J.P., Nagant de Deuxchaisnes, C., &Devogelaer, J.P. (1997). Hematological changes in anorexia nervosa are correlated with total body fat massdepletion. International Journal of Eating Disorders, 21, 329–334.
Langan, S.M., & Farrell, P.M. (1985). Vitamin E, vitamin A and essential fatty acids status of patients hospita-lized for anorexia nervosa. American Journal of Clinical Nutrition, 41, 1054–1060.
McClain, C.J., Stuart, M.A., Vivian, B., McClain, M., Talwalker, R., Snelling, L., & Humphries, L. (1992). Zincstatus before and after zinc supplementation of eating disorder patients. Journal of the American College ofNutrition, 11, 694–700.
Micheletti, A., Rossi, R., & Rufini, S. (2001). Zinc status in athletes: Relation to diet and exercise. Sports Medicine,31, 577–582.
Moyano, D., Vilaseca, M.A., Artuch, R., Valls, C., & Lambruschini, N. (1998). Plasma total-homocysteine inanorexia nervosa. European Journal of Clinical Nutrition, 52, 172–175.
Norusis, M.J. (1993). SPSS for windows base system user’s guide (Release 6.0) [Computer software]. Chicago:SPSS.
Olmedilla, B., Granado, F., Gil-Martinez, E., Blanco, I., & Rojas-Hidalgo, E. (1997). Reference values for retinol,tocopherol, and main carotenoids in serum of control and insulin dependent diabetic Spanish subjects.Clinical Chemistry, 43, 1066–1071.
Philipp, E., Pirke, K.M., Seidl, M., Tuschl, R.J., Fichter, M.M., Eckert, M., & Wolfram, G. (1988). Vitamin status inpatients with anorexia nervosa and bulimia nervosa. International Journal of Eating Disorders, 8, 209–218.
Rigaud, D., Sogni, P., Hammel, P., Melchior, J.C., Angel, L., Rozen, R., Labarre, C., Mignon, M., & Apfelbaum, M.(1989). Anorexia nervosa: Absence of sensitivity to nutritional protein markers. Study of 23 patients andcomparison to a paired group with colonic Crohn’s disease. Annals Medicine Interne (Paris), 140, 86–90.
Rock, C.L., & Curran-Celentano, J. (1994). Nutritional disorder of anorexia nervosa: A review. InternationalJournal of Eating Disorders, 15, 187–203.
Rock, C.L., Gorenflo, D.W., Drewnowski, A., & Demitrac, M.A. (1996). Nutritional characteristics, eatingpathology, and hormonal status in young women. American Journal of Clinical Nutrition, 64, 566–571.
Rock, C.L., & Vasantharajan, S. (1995). Vitamin status of eating disorder patients: Relationship to clinical indicesand effect of treatment. International Journal of Eating Disorders, 18, 257–262.
Russell, J.D., Mira, M., Allen, B.J., Stewart, P.M., Vizzard, J., Arthur, B., & Beumont, P.J. (1994). Protein repletionand treatment in anorexia nervosa. American Journal of Clinical Nutrition, 59, 98–102.
Nutritional Deficiencies in Anorexia Nervosa 177

Steiner, H., & Lok, J. (1998). Anorexia nervosa and bulimia nervosa in children and adolescents: A review of thepast 10 years. Journal of the American Academy of Child and Adolescent Psychiatry, 37, 352–359.
Stoving, R.K., Flyvbjerg, A., Frystyk, J., Fisker, S., Hangaard, J., Hansen-Nord, M., & Hagen, C. (1999). Lowserum levels of free and total insulin-like growth factor I (IGF-I) in patients with anorexia nervosa are notassociated with increased IGF-binding protein-3 proteolysis. Journal of Clinical Endocrinology and Metabo-lism, 84, 1346–1350.
Tietz, N. (1994). Proteins. In C.A. Burtis & E.R. Ashwood (Eds.), Textbook of clinical chemistry (2nd ed., pp.700–704). Philadelphia: Saunders.
Van Binsbergen, C.J., Coelingh Bennink, H.J., Odink, J., Haspels, A.A., & Koppeschaar, H.P. (1990). A compara-tive and longitudinal study on endocrine changes related to ovarian function in patients with anorexianervosa. Journal of Clinical Endocrinology and Metabolism, 71, 705–711.
Van Binsbergen, C.J., Odink, J., Van den Berg, H., Koppeschaar, H., & Coelingh Benninck, H.J. (1988). Nutri-tional status in anorexia nervosa: Clinical chemistry, vitamins, iron and zinc. European Journal of ClinicalNutrition, 42, 929–937.
Winston, A.P., Jamieson, C.P., Madira, W., Gatward, N.M., & Palmer, R.L. (2000). Prevalence of thiamindeficiency in anorexia nervosa. International Journal of Eating Disorders, 28, 451–454.
178 Castro et al.







![[PPT]Anorexia Nervosa - Mr Sitar's Website - homemrsitarswebsite.wikispaces.com/file/view/Anorexia Nervosa... · Web viewWhat is the definition to this illness? Anorexia nervosa is](https://img.pdfslide.net/doc/110x75/5af162f57f8b9ad0618f592d/pptanorexia-nervosa-mr-sitars-website-nervosaweb-viewwhat-is-the-definition.jpg)