Embed Size (px)
Citation preview
Person-Centered Recovery Planning:Can we honor the PERSON & satisfy the CHART?
Janis Tondora, Psy.D.Featured Workshop
New Jersey Psychiatric Rehabilitation Association November 21, 2013
2
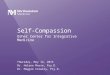
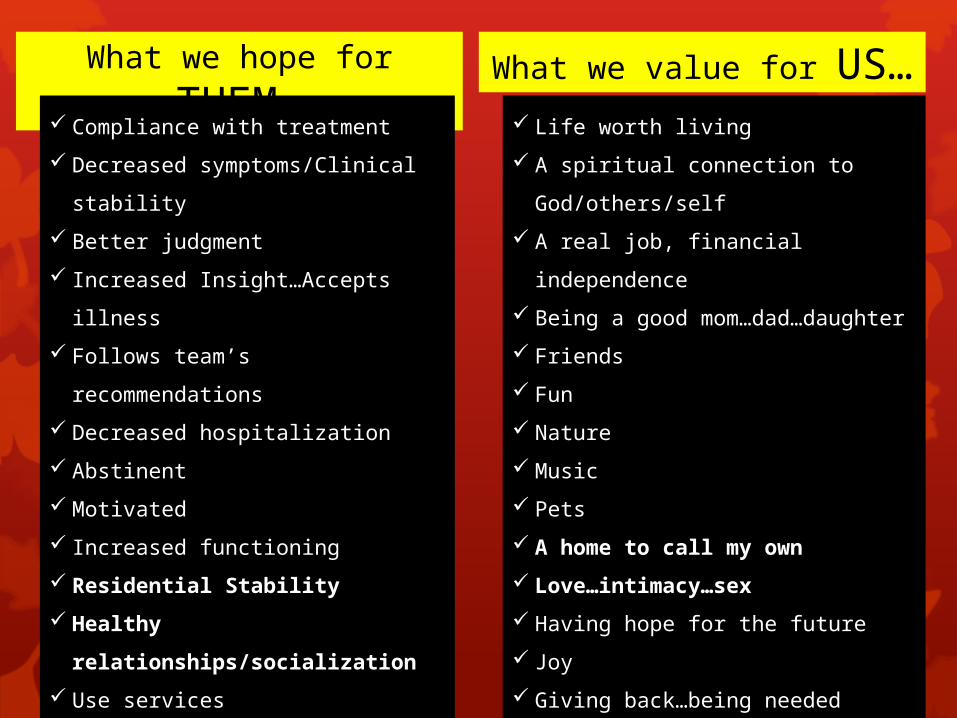
What we hope for THEM… What we value for US… Compliance with treatment
Decreased symptoms/Clinical stability
Better judgment
Increased Insight…Accepts illness
Follows team’s recommendations
Decreased hospitalization
Abstinent
Motivated
Increased functioning
Residential Stability
Healthy relationships/socialization
Use services regularly/engagement
Cognitive functioning
Realistic expectations
Attends the job program/clubhouse,
etc.
Life worth living
A spiritual connection to God/others/self
A real job, financial independence
Being a good mom…dad…daughter
Friends
Fun
Nature
Music
Pets
A home to call my own
Love…intimacy…sex
Having hope for the future
Joy
Giving back…being needed
Learning
• People with mental health and addictions issues generally want the exact same things in life as ALL people.
• People want to thrive, not just survive…
• Recovery-oriented care challenges us to move past the maintenance of clinical stability to the true pursuit of RECOVERY!
3
Beyond US and THEM
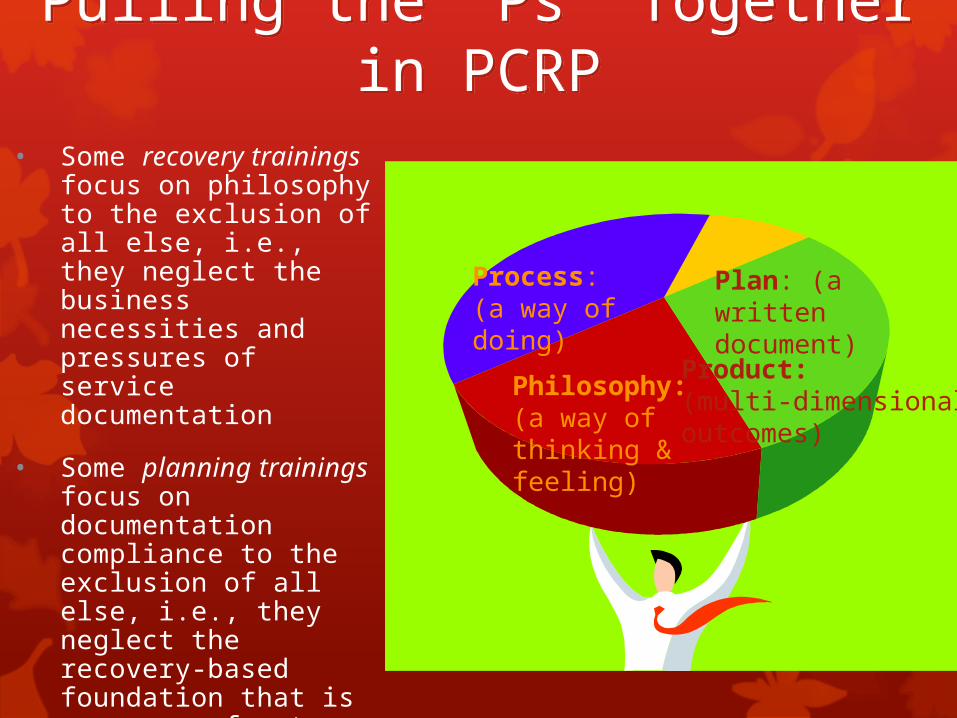
Process:(a way of doing)
Plan: (a written document)
Product: (multi-dimensional outcomes)
Philosophy: (a way of thinking & feeling)
Pulling the “Ps” Together in PCRP
Pulling the “Ps” Together in PCRP
• Some recovery trainings focus on philosophy to the exclusion of all else, i.e., they neglect the business necessities and pressures of service documentation
• Some planning trainings focus on documentation compliance to the exclusion of all else, i.e., they neglect the recovery-based foundation that is necessary for true QUALITY
• THIS workshop strives to address all the Ps!
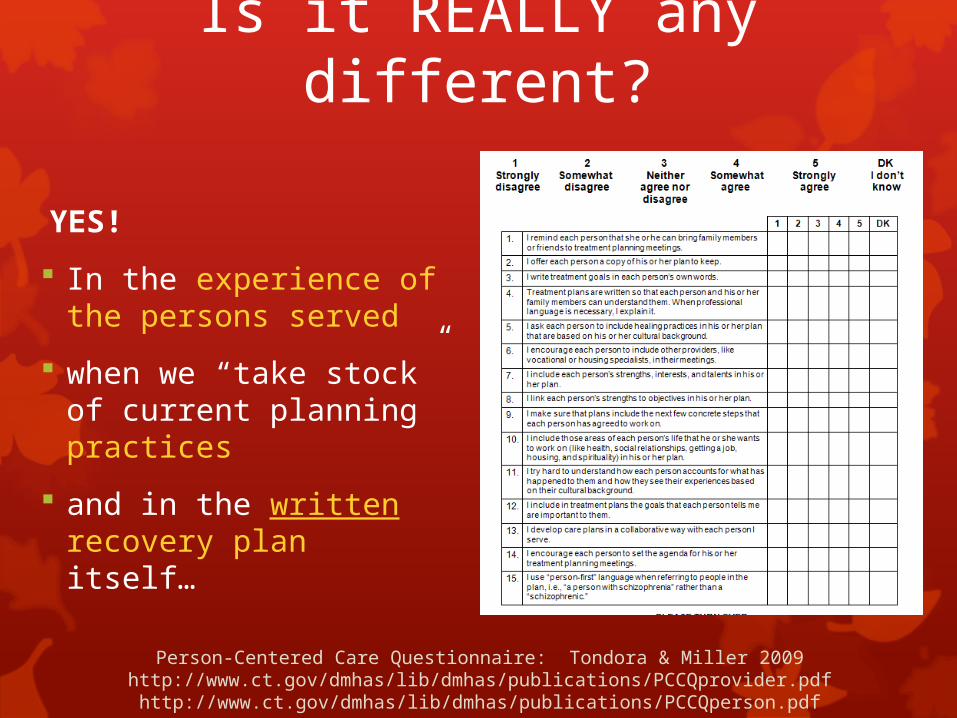
YES!
In the experience of the persons served
when we “take stock” of current planning practices
and in the written recovery plan itself…
Is it REALLY any different?
Person-Centered Care Questionnaire: Tondora & Miller 2009http://www.ct.gov/dmhas/lib/dmhas/publications/PCCQprovider.pdfhttp://www.ct.gov/dmhas/lib/dmhas/publications/PCCQperson.pdf
A Closer Look at (Sample) Key Practicesin the Process of PCRP
• Person is a partner in all planning activities/meetings; advance notice
• Person has reasonable control over logistics (e.g., time, invitees, etc.)
• Person offered a written copy
• Education/preparation regarding the process and what to expect
• Language as a key practice
This toolkit can be useful for anyone – regardless of whether they have a psychiatric condition or an addiction. Everyone needs help at times setting goals, and figuring out what they want. This toolkit has some specific parts that are helpful to people with a mental illness or addiction, but could be really used by anyone.
-Janis Tondora-Rebecca Miller-Kimberly Guy-Stephanie Lanteri
Yale Program for Recovery and Community Health© 2009
Educate and Prepare the Service User
• http://www.yale.edu/PRCH/documents/toolkit.draft.3.5.11.pdf
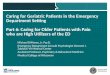
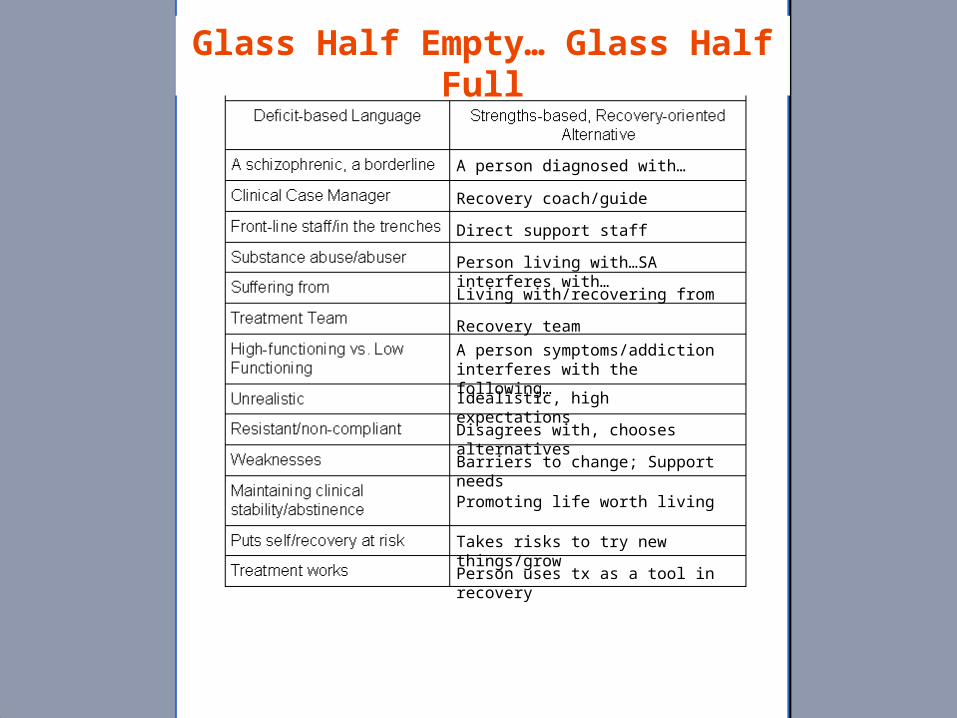
The Power of Language in Recovery Planning:
8
The Glass Half Empty, The Glass Half Full: Exercise and Group Discussion
9
A person diagnosed with…
Direct support staff
Recovery coach/guide
Recovery team
Living with/recovering from
A person symptoms/addiction interferes with the following…
Idealistic, high expectations
Disagrees with, chooses alternativesBarriers to change; Support needs
Promoting life worth living
Takes risks to try new things/grow
Person uses tx as a tool in recovery
Person living with…SA interferes with…
Glass Half Empty… Glass Half Full
A Closer Look at (Sample) Key Practicesin the Process of PCRP
• Recognize the range of contributors to the planning process (e.g., peers, natural supporters).
• Value community inclusion
• “While,” not “after”
• Trap of the one-stop shop
• Demonstrate a commitment to both outcomes and process; high expectations.
• Understand/support rights such as self-determination (e.g., role of advance directives; WRAP, etc.)
• Assess, and plan for the use of, STRENGTHS
Strengths-based Assessment
Initiates helping relationships
Ongoing process
Focus on functional abilities and impairments as opposed to symptoms per se
Comprehensive domain-based data gathering
Identifies strengths
Abilities and accomplishments
Interests and aspirations
Recovery resources and assets
Unique individual attributes
Considers stage / phase of change process11
Importance of Understanding/Formulation
• Data collected in assessment is by itself not sufficient for service planning
• The “integrated summary” (often referred to as the “formulation” in clinical settings) is essential
• Moves from what to why
• Sets the stage for prioritizing needs and goals
• Recorded in a chart narrative
• The role of culture and ethnicity is critical to true appreciation of the person served
• Shared with person served
Is the BRIDGE between the data and the plan!

• Treatment Team members arrive on time; introductions
• The person is given the team’s full attention, e.g., cell phones are turned off; there are no side-bar conversations; team member’s are not completing/reading other paperwork/texting/ responding to e-mail, etc.
• The person is not “talked about” during the meeting. All comments and questions are directed first to the individual and are a collaborative exchange between the person and his/her Treatment Team.
• “What comes next” is explained to the person, including an opportunity for them to review the plan; provide input
DURING the Meeting:Basic Ground Rules
So you try your best to implement ALL of these “key practices,” but how do we move from the PROCESS of PCRP to the DOCUMENTATION of
PCRP?
14
What next?
Simple Truth #1
• Person-Centered planning is what people want.
• Nearly every consumer of mental health services expressed the need to fully participate in his or her plan for recovery.”
The 2003 President’s Commission on Mental Health
• Research shows we traditionally underestimate consumers’ desire/willingness to partner in their care planning
Chinman, et al., 1999
Simple Truth #2
Service providers and service agencies rely on payors (Medicaid, Medicare, Managed care programs) to survive.

17
Simple Truth #3:
Serving Two Masters
Person-centeredRecoveryCommunity
integrationCore giftsPartneringSupports self-
direction
RegulatoryMedical necessityDiagnosisDocumentationComplianceBilling codes
Outcomes and Goals
Understanding
“Let’s face it: Our relationship is doomed!”
Medical Necessity
Person-Centered Care
Irreconcilable differences? Happily ever after?
(or at least a peaceful co-existence?)
A More Hopeful Proposition…
• We can balance person-centered approaches with medical necessity/regulations in creative ways to move forward in partnership with persons in recovery.
• We can create a plan that honors the person and satisfies the chart!
• In other words: PCP is not soft!
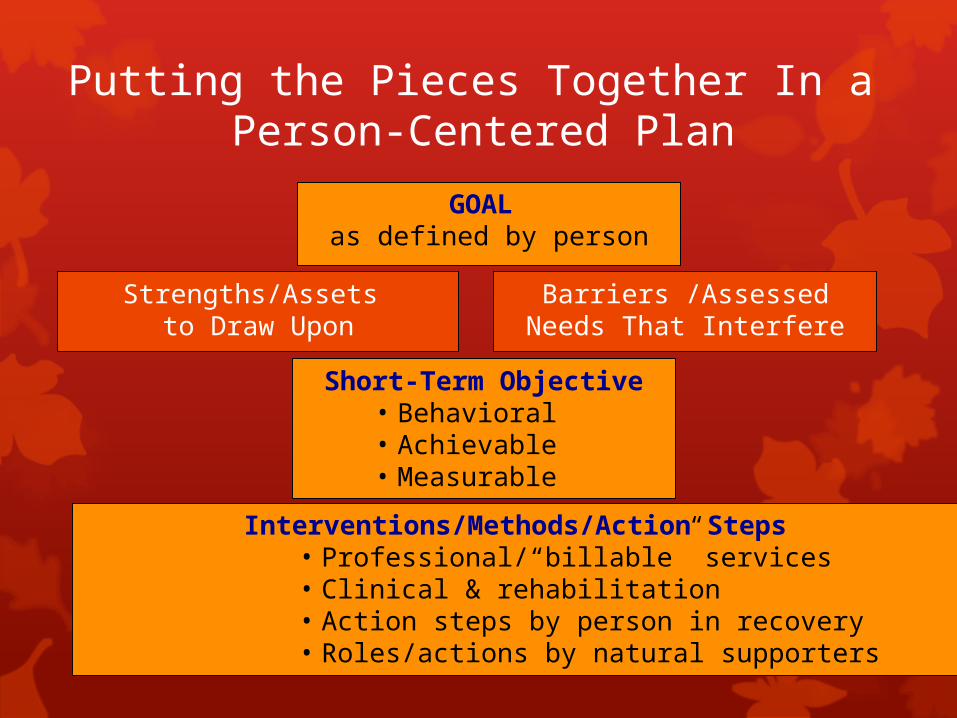
Putting the Pieces Together In a Person-Centered Plan
GOAL as defined by person
Strengths/Assets to Draw Upon
Barriers /Assessed Needs That Interfere
Short-Term Objective• Behavioral• Achievable• Measurable
Interventions/Methods/Action Steps• Professional/“billable” services• Clinical & rehabilitation• Action steps by person in recovery• Roles/actions by natural supporters

Goals
Long term, global, and broadly stated
Life changes as a result of services
Ideally expressed in person’s words
Written in positive terms
Consistent with desire for self-determination
may be influenced by culture and tradition
21

22
What Do People Want?
IndependenceI want to control my own money.
Work /educationI want to finish
school Spiritual issues
I want to get back to church.
Health/well-being I want to lose
weight.
To be part of the life of the community…
HousingI want to move out of the group home.
Social activities I want to join a
bowling league. Satisfying relationships
I want to see my grandkids. Valued Roles
I want to volunteer at the Senior Center.
And NOT just traditional treatment plan goals…And NOT just traditional treatment plan goals…
23
• Goal: Maintain psychiatric stability
• Objectives1. Compliance with meds2. Attend appointments with primary care provider 3. Attend all psychiatric appointments as scheduled

Active Use of Assessed Strengths
• Focus on strengths and assets that can be leveraged in the person’s Recovery Plan, i.e., strengths are not meant to “sit on a shelf”
• Where/how are you assessing and USING strengths in recovery planning in your system?
e.g., a person with a love for books might be engaged by asking him/her to help out in the facility library… a person who loves music might benefit from access to CDs/headphones as away to calm agitation… a spiritual person contemplating suicide might want direction from the chaplain… an individual with a strong connection to their cultural heritage might work on communications skills by becoming part of the cultural competence committee

Barriers/Assessed Needs
What’s getting in the way?
need for skills development
Intrusive symptoms
lack of resources
need for assistance / supports
problems in behavior
challenges in activities of daily living
threats to basic health and safety
challenges/needs as a result of a mental/ alcohol and/or drug disorder
25
Create Mr. Blake’s PCRP
Part I: Discuss integrated understanding, then identify
ONE goal, and strengths and barriers
Objectives Defined
An objective is a meaningful step (in the eyes of both the person and staff) towards achievement of the goal
Essential features:behavioralachievablemeasurabletime framedunderstandable for the person served
Objectives should be SMART
Here’s a way to evaluate your objectives. Are they SMART?
Simple or StraightforwardMeasurableAttainableRealisticTime-framed
Objectives
Simple litmus test for measurability: Read the objective out loud:
At the end of 1 month, etc., will you definitively be able to say yes / no that the objective was accomplished.
If not, the objective as written was likely too “soft” on the front end
Objectives - Wording
These terms commonly mean different things to different people. If you use them, be careful to further define them in behavioral terms, e.g., improve sleep disturbance…?? as evidenced by sleeping a minimum of 5 hours per night for 7 consecutive days.
interact appropriate normalparticipate actively increasesocialize willingly decreasecooperate calm improvecoherent relevantrescue agitated
Defaulting to Service Participation When Writing Objectives
• Goal:• I want to get my job back.
• Objectives• Comply with meds• Attend appointments with primary care
provider • Attend all psychiatric appointments as
scheduled
Objectives Should NOT be Limited to Service Participation
Wanda will voluntarily attend DBT group 2x weekly. This is about service participation. People can participate in services for
years and not achieve the intended benefits!
Objectives are about what you hope will change for the person as a result of services. Ask yourself the question: As a result of attending DBT, how do you expect the person’s
behavior/quality of life/status to change in a measurable way?
Wanda will apply mindfulness techniques to reduce instances of self-injury to no more than one per week for 2 consecutive weeks.
Objectives Should NOT be Limited to Service Participation
Goal: I want a girlfriend more than anything.
Objectives:
NOT: Patient will maintain medication compliance, attend social skills group, and meet with his/her therapist but…Stan will…
Within one week, identify 3 local places in the community she/he can go to meet others
Within 30 days, identify 3 positive coping strategies to manage anxiety in social situations Participate in one preferred social activity outside the group home per week for the next 90 days
Demonstrate 3 “conversation-starters” in session with clinician within 2 weeks
Even use those conversation starters to invite someone on a date!
Objectives Build Over Time
Assume Audrey wants to go back to work but currently, severe depression & sleep disturbance is making it difficult for her to get out of bed
34
• Over the next 90 days, Audrey will be able to get out of bed by 9am at least 4 days out of 5 M-F.
• Update: Within 3 months, Audrey will have completed a draft of her resume
• Update: Within 6 months, Audrey will be working 5 hours per week in community!
Objectives: From Learning to Doing
Client will reduce assaultive behavior.
35
• Within 90 days, Amy will identify 3 triggers to behavioral outbursts with children.
• (LEARNING objective)
• Within 90 days, Amy will have a minimum of one successful visit with her children AEB by report of Amy’s DCF Case Worker
• (BEHAVIORAL OBJECTIVE)
Objectives – Stage Responsive
Client will decrease frequency & intensity of substance use.
36
• Joe will identify a min. of 2 adverse effects that substance use has on his/her recovery within 30 days (pre-contemplative)
• Joe will be substance-free for 6 months as evidenced by self-report (action-oriented)
Create Mr. Blake’s PCRP
Part II: Write ONE S-M-A-R-T Objective for Mr. Blake
Services & Action Steps
• respect individual choice and preference
• are tailored to the stage of change/recovery
• describe medical necessity by clearly describing how services are intended to overcome that individual’s barriers
• are specific to an objective
38
• But they also incorporate actions by natural supporters and the person him/herself.
• Services & action steps include those “interventions” provided by clinical & rehab professionals which…
Professional services must specify…
WHO will provide the service, i.e., name and job title
WHAT: The TITLE of the service, e.g., Health & Wellness Group
WHEN: The SCHEDULE of the service, i.e., the time and day(s)
WHY: The individualized INTENT/PURPOSE of service
Critical Elements
Action Steps by The Person In Recovery & Natural Supporters
Traditionally, interventions in a plan include only those performed by staff. The recovery model, however, emphasizes the responsibility of a person to participate actively in his or her own care as well as the benefits of seeking contributions of “natural supports” (e.g., family, friends, advocates, & community supporters)
For each objective, you have the opportunity to specify:
“Personal Actions” (this promotes a sense of self-agency and helps to activate people in their recovery) and
“Natural Support Action” (to help the person build/expand their natural recovery network as a supplement to professional services)
An example to consider…
• Greg reports he is very lonely and that he just wants a girlfriend. He used to go to the downtown jazz fests and meet lots of people, but now he feels like a “zombie.” He is not getting out of the group home to do much of anything other than come to the Center. He wonders if this is due to his meds… Greg admits to being “terrified” to get out in community and meet women, and states that its been 10 years since he had a girlfriend. He wouldn’t know where to start…He is currently unable to take the bus and is afraid to go anywhere alone.
Goal: I want a girlfriend.
Strengths: Motivated to reduce social isolation; supportive brother; has
identified community he enjoyed in past interests(e.g., music, Chinese restaurants) well-liked by peers; humorous
Barriers/Assessed Needs/Problems: Intrusive thoughts/paranoia increase in social situations; possible
negative symptoms of schizophrenia and/or med side effects result in severe fatigue/inability to initiate; easily confused/disorganized; need for skill development to: use public transportation/increase community mobility, develop symptoms management/coping strategies, improve communication and social skills, attend to personal appearance
Objective: Greg will effectively use learned coping skills to manage
distressing symptoms to participate in a minimum of 1 preferred social activity per week for the next 90 days
Sample Plan, cont.

Interventions/Action Steps:
Jane Roe, Clinical Coordinator, to provide CBT 2X/mos. for 45 min for next 3 mos. to increase Greg’s ability to cope with distressing symptoms in social situations (teaching thought stopping, distraction techniques, deep-breathing, visualization, etc.)
Dr. X to provide Med Management, 2X/mos for 30 min for next 3 months to evaluate therapeutic impact and possible side effects to reduce fatigue and optimize functioning
John Smith, Peer Coordinator, will provide travel training 1X/wk. for 60 min 4 weeks to help him become independent with city bus (e.g., identifying most direct bus routes, rehearsing use of coping skills, role playing conversations if confused/lost, etc.)
Greg’s brother, Jim, will accompany Greg to weekly social outings over the next 3 months.
Greg will complete a daily medication side-effect log for the next 2 months while meds are evaluated and adjusted.
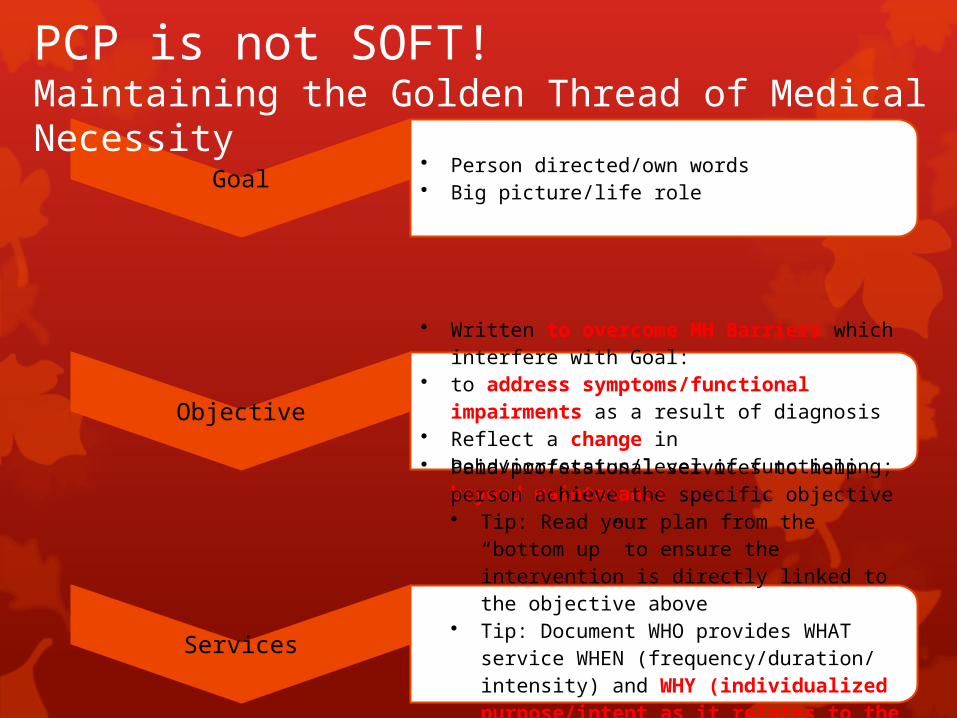
Goal• Person directed/own words• Big picture/life role
Objective
• Written to overcome MH Barriers which interfere with Goal:
• to address symptoms/functional impairments as a result of diagnosis
• Reflect a change in behavior/status/level of functioning; beyond maintenance
Services
• Paid/professional services to help person achieve the specific objective• Tip: Read your plan from the “bottom up”
to ensure the intervention is directly linked to the objective above
• Tip: Document WHO provides WHAT service WHEN (frequency/duration/ intensity) and WHY (individualized purpose/intent as it relates to the linked objective)
• Natural support/self-directed supports to help person achieve the specific objective
PCP is not SOFT!Maintaining the Golden Thread of Medical Necessity
Create Mr. Blake’s PCRP
Part III: Write a set of services/action steps reflecting BOTH professional
services as well as self-directed and natural support actions
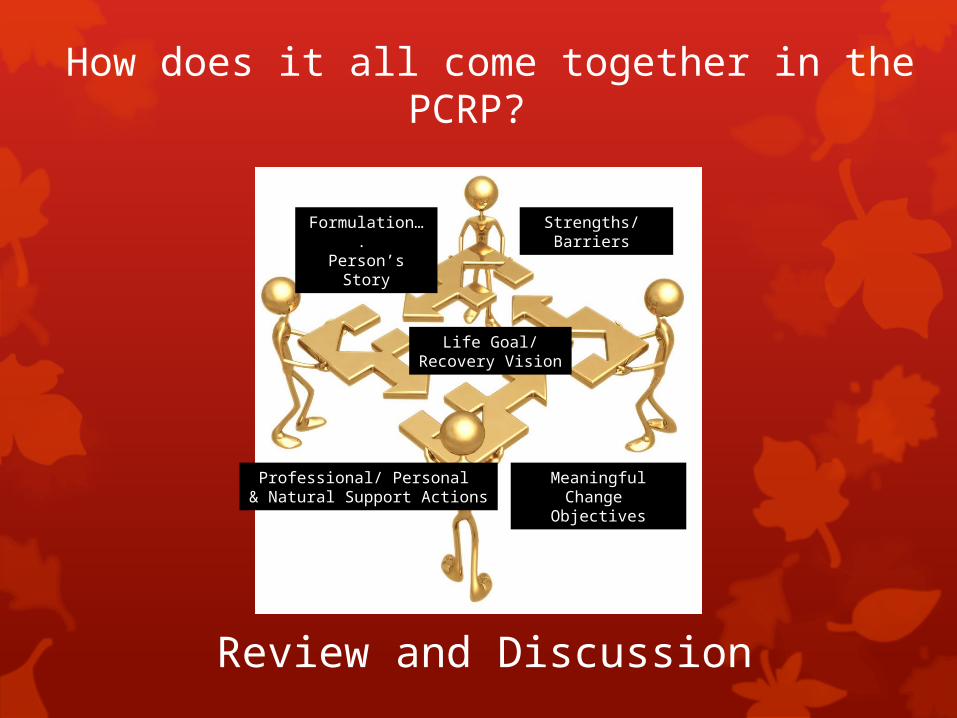
How does it all come together in the PCRP?
Review and Discussion
Life Goal/Recovery Vision
Formulation…. Person’s Story
Strengths/ Barriers
Meaningful Change Objectives
Professional/ Personal & Natural Support Actions
You CAN create a treatment plan which honors the person and satisfies the chart!
This is central to your mission to move forward in partnership with individuals and help them get back to their lives in the community as soon as possible!
In Conclusion…
“We don’t think ourselves into a new way of acting, we act ourselves into a new way of thinking.”* How will YOU be a part of
change moving forward?
*The Discipline of Getting Things Done, by Larry Bossidy and Ram Charan