Embed Size (px)
Citation preview

Personal Protective Equipment

Objective
• Choose appropriate Personal Protective Equipment (PPE) equipment and use without contamination
• Handouts/Materials: – One set of WHO recommended PPE for each person – Water based paint (red) – Step-by-step guide (photocopy) – Competency Checklist (photocopy)

INTRODUCTION
PPE
December 19, 2014

Prior to entering the patient isolation rooms/areas, ensure that all visitors and health-care workers rigorously use personal protective equipment (PPE) and perform hand hygiene.
-WHO 2014

PPE Guidance
• PPE recommendations similar between organizations (MSF, CDC, WHO)
• Adaptations and discussions are ongoing
• 3 Important Principles: • Principle #1: Rigorous and repeated
training • Principle #2: No skin exposure when PPE
is worn • Principle #3: Trained monitor
CDC 2014 http://www.cdc.gov/media/releases/2014/fs1020-ebola-personal-protective-equipment.html

Principle #1: Rigorous and repeated training • Focusing only on PPE gives a false sense of
security of safe care and worker safety. • Training is critical to ensure infection control.
– Ensure all HCWs practice numerous times – Make sure HCWs understand how to appropriately
use the equipment – Especially the step by step donning and doffing of
PPE
CDC 2014 http://www.cdc.gov/media/releases/2014/fs1020-ebola-personal-protective-equipment.html
Principle #2: No skin exposure when PPE is worn
• Two specific, recommended PPE options with equivalent protection if worn, donned and doffed correctly: – coverall/body suit – N-95/PAPR
• Designated areas for putting on and taking off PPE – Ensure that space and lay-out allows for clear separation between
low-risk and high-risk areas
• Step-by-step PPE removal instructions including: – Disinfecting visibly contaminated PPE using an 1:10 bleach
disinfectant wipe prior to taking off equipment – Disinfection of gloved hands using either an 1:10 bleach
disinfectant wipe or alcohol-based hand sanitizer between steps of taking off PPE
CDC 2014 http://www.cdc.gov/media/releases/2014/fs1020-ebola-personal-protective-equipment.html
Principle #2: No skin exposure when PPE is worn
PPE recommended for healthcare workers caring for patients with Ebola includes:
– Double gloves – Boot covers or fluid resistant boots – Coverall:
• Single use fluid resistant or impermeable. – Respirators, including either N95 respirators or powered
air purifying respirator(PAPR) – Full-face shield or goggles – Hoods to ensure complete coverage of the head and neck – Apron that is waterproof and covers the torso to the level
of the mid-calf CDC 2014; Images Johns Hopkins Health System

Principle #3: Trained monitor • CDC is recommending a trained monitor
– Actively observe and supervise each worker taking PPE on and off
– To ensure each worker follows the step by step processes, especially to disinfect visibly contaminated PPE
– Can spot any missteps in real-time and immediately address
CDC 2014 http://www.cdc.gov/media/releases/2014/fs1020-ebola-personal-protective-equipment.html

PPE
• Nurse.com, 10/31/14 – “The idea of a trained observer highlights some
practices we should be doing every day,” “There are many more things that could be on the horizon when it comes to infection, and the CDC’s new guidelines are a reminder that we have the ability to watch out for each other. Small decisions like pointing out an error or reminding someone about something can mean the difference in infection and prevention.”
Linda Greene, MPS, RN, CIC, an infection prevention manager at Highland Hospital in Rochester, N.Y., and a member of the regulatory review panel for the Association
for Professionals in Infection Control and Epidemiology.

Use of a Trained Observer • The sequence and actions involved in each donning and doffing
step are critical to avoiding exposure, a trained observer: – will read aloud to the healthcare worker each step in the procedure
checklist and visually confirm and document that the step has been completed correctly.
• The trained observer is a dedicated individual with the sole responsibility of ensuring adherence to the entire donning and doffing process.
• The trained observer will be knowledgeable about all PPE recommended in the facility’s protocol and the correct donning and doffing procedures, including disposal of used PPE, and will be qualified to provide guidance and technique recommendations to the healthcare worker.
• The trained observer will monitor and document successful donning and doffing procedures, providing immediate corrective instruction if the healthcare worker is not following the recommended steps.
• The trained observer should know the exposure management plan in the event of an unintentional break in procedure.

Recommended PPE for Trained Observer during Observations of PPE Doffing • The trained observer should not enter the room of a patient with Ebola, but
will be in the PPE removal area to observe and assist with removal of specific components of PPE.
• The observer should not participate in any Ebola patient care activities while conducting observations.
• The following PPE are recommended for trained observers: – Single-use (disposable) fluid-resistant or impermeable gown that extends to at
least mid-calf or coverall without integrated hood. – Single-use (disposable) full face shield. – Single-use (disposable) nitrile examination gloves with extended cuffs. Two
pairs of gloves should be worn. At a minimum, outer gloves should have extended cuffs.
– Single-use (disposable) fluid-resistant or impermeable shoe covers or fluid-resistant boots
• Trained observers should don and doff selected PPE according to standard procedures.
• If the trained observer assists with PPE doffing, then the trained observer should disinfect outer-gloved hands with an Bleach disinfectant wipe or ABHR immediately after contact with healthcare worker’s PPE.

More than PPE is needed • PPE is Only One Aspect of Infection Control • It is critical to focus on other prevention activities
to halt the spread of Ebola in healthcare settings, including: – Prompt screening and triage of potential patients – Designated site managers to ensure proper
implementation of precautions – Limiting personnel in the isolation room – Effective environmental cleaning
CDC 2014 http://www.cdc.gov/media/releases/2014/fs1020-ebola-personal-protective-equipment.html

PPE COMPONENTS
December 19, 2014

Under the PPE For wearing in low-risk area • Scrub suit (washable or
disposable) • Covered toes, fluid and
puncture resistant boots Launder scrubs and clean boots at health facility

Gloves • Intended to prevent skin contact with hazardous
substances, e.g. body fluids
• Do not reuse disposable gloves
• Double gloves are recommended
• Gloves with long cuffs offer more protection
• Use correct size
• Apply hand hygiene to soiled gloves as soon as possible to avoid transfer of microorganisms to other patients or environments.
Slide adapted from World Health Organization

Boot Covers • Protects the boot from gross contamination • Fluid resistant or impermeable
• Remove carefully by stepping on the back of the boot cover and only touch the inside of the covers once removed
Slide adapted from World Health Organization

Coverall or Body Suit
• Protects skin • Prevents soiling of clothing • Fluid resistant or impermeable
• Remove a soiled garment as promptly as possible and apply hand hygiene to avoid transfer of microorganisms to other environments.
Slide adapted from World Health Organization

Apron
Apron protects front of coverall from gross contamination with infectious body fluids resulting in safer removal Essential if: • Strenuous activity with risk of disrupting the coverall • Large amount of blood and body fluids expected
Slide adapted from World Health Organization

Mask
• Protects the mucosa of nose and mouth from droplets, spills and splashes – Wear masks tightly to the face – Discard immediately after use – If wet or dirty with secretions, it must be changed
promptly (ie must leave high risk area and remove PPE)
Aerosol Generating Procedures
• Wear a respirator for any procedures that stimulate coughing or promote generation of aerosols
• Different models available • Aerosols
– Tiny particles < 5 µm – Float on air currents for long distances
Source: World Health Organization 2014

Aerosol Generating Procedures
• Aerosol generating procedures include: – Aerosolized or nebulized medication administration – Diagnostic sputum induction – Bronchoscopy – Airway suctioning – Intubation – Positive pressure ventilation via facemask
• For Ebola patient, avoid as much as possible due to potential for virus to become aerosolized
Source: World Health Organization 2014
Fit test ≠ seal check
• Fit test evaluates the existence of leaks at the moment it is performed for the model being tested – The conditions during the test may not be the same as "real life" – In the real life the type of respirator may differ from the one fit tested
• Seal check – helps check if the respirator is well adjusted to the face – should be done before EACH USE
• Users should be trained on how to use the respirator
Slide used with permission from World Health Organization

Particulate Respirator Seal Check • Cup the respirator in your hand
with the nosepiece at your fingertips allowing the headbands to hang freely below your hand
• Position the respirator under your chin with the nosepiece up
Slide used with permission from World Health Organization
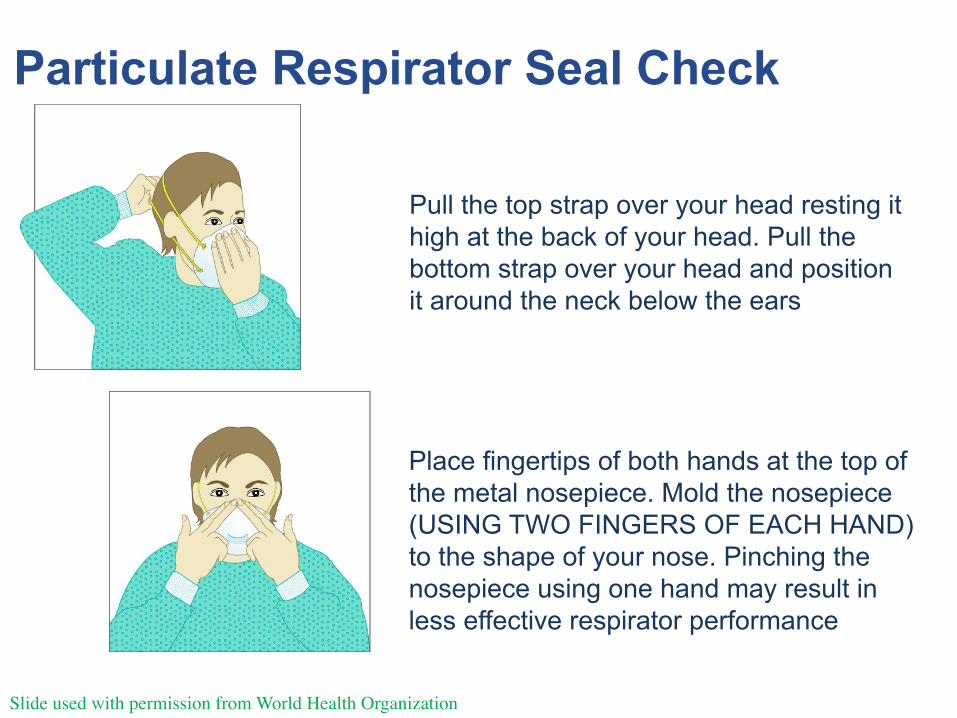
Pull the top strap over your head resting it high at the back of your head. Pull the bottom strap over your head and position it around the neck below the ears
Place fingertips of both hands at the top of the metal nosepiece. Mold the nosepiece (USING TWO FINGERS OF EACH HAND) to the shape of your nose. Pinching the nosepiece using one hand may result in less effective respirator performance
Slide used with permission from World Health Organization
Particulate Respirator Seal Check

Particulate Respirator Seal Check
Cover the front of the respirator with both hands, being careful not to disturb the position of respirator
Positive seal check § Exhale sharply. A positive
pressure inside the respirator = no leakage. If leakage, adjust position and/or tension straps.
§ Retest the seal and repeat the steps until respirator is sealed properly
Negative seal check § Inhale deeply. If no leakage, negative
pressure will make respirator cling to your face
§ Leakage will result in loss of negative pressure in the respirator due to air entering through gaps in the seal
Slide used with permission from World Health Organization
DO THIS EACH TIME YOU PUT ON
MASK

Eye protection
Face shield
Goggles Visor

PPE USE
December 19, 2014

Designating Areas for PPE Donning and Doffing • Facilities should ensure that space and layout allow for clear
separation between high risk and low risk areas. • It is critical that physical barriers (e.g., plastic enclosures) be used
where necessary, along with visible signage, to separate distinct areas and ensure a one-way flow of care moving from low risk areas (e.g., area where PPE is donned and unused equipment is stored) to the patient room and to the PPE removal area (area where PPE is removed and discarded).
• Post signage to highlight key aspects of PPE donning and doffing, including: – Designating low risk vs high risk areas – Reminding healthcare workers to wait for a trained observer before
removing PPE – Reinforcing need for slow and deliberate removal of PPE to prevent self-
contamination – Reminding healthcare workers to perform disinfection of gloved hands in
between steps of the doffing procedure.
December 19, 2014

Designate the following areas with appropriate signage: • PPE Storage and Donning Area
– This is an area outside the Ebola patient room (e.g., a nearby vacant patient room, a marked area in the hallway outside the patient room) where clean PPE is stored and where healthcare workers can don PPE before entering the patient’s room.
– Do not store potentially contaminated equipment, used PPE, or waste removed from the patient’s room in this area.
– Waste must not pass through this area, if it does it must be properly contained.

Preparation and Planning
• Prepare designated area to put on PPE(in low-risk)
• Guarantee hand hygiene facility • Guarantee recommended PPE
– Adequate supplies – Adequate space to put on

PPE Removal Area
• This is an area in proximity to the patient’s room (e.g., anteroom or adjacent vacant patient room that is separate from the clean area) where healthcare workers leaving the patient’s room can doff and discard their PPE.
• Some steps of the PPE removal process may be performed in a clearly designated area of the patient’s room near the door, provided these steps can be seen and supervised by a trained observer (e.g., through a window such that the healthcare worker doffing PPE can still hear the instructions of the trained observer).
• Do not use this clearly designated area for any other purpose. • Stock gloves in a clean section of the PPE removal area accessible
to the healthcare worker while doffing.

PPE Removal Area • In the PPE removal area, provide supplies for disinfection of PPE
and for performing hand hygiene and space to remove PPE. • Provide leak-proof infectious waste containers for discarding used
PPE. • Perform frequent environmental cleaning and disinfection of the
PPE removal area, including upon completion of doffing procedure by healthcare workers.

PPE Removal Area
• If a facility must use the hallway outside the patient room as
the PPE removal area: – construct physical barriers to close the hallway to through traffic and
thereby create an anteroom – should make sure that this hallway space complies with fire-codes. – Restrict access to this hallway to essential personnel who are properly
trained on recommended infection prevention practices for the care of Ebola patients.
• Facilities should consider making showers available for use by healthcare workers after doffing of PPE/end of shift.

PPE Use
• Avoid reuse of disposable PPE items – Reprocessed disposable PPE may not provide the same
protective efficacy and safety as new PPE – Reuse may increase the risk of infection in HCWs
Slide used with permission from WHO

PPE Use if Supplies are Limited
• If resources are limited and disposable PPE items are not available
• properly disinfect reusable items after each use
• Avoid wastage: – Critically evaluate situations in which PPE is indicated – Batch clinical care during each entry to the patient's room – Work from suspect to confirmed cases – Work from clean to dirty procedures – Prioritize for scenarios that have been consistently associated with
increased risk of pathogen transmission • Use of unnecessary PPE should be avoided
– Training is not unnecessary use
Slide used with permission from World Health Organization


December 19, 2014

Occasions for additional PPE
• Environmental cleaning • Handling Infectious Waste • Activities that might damage exam gloves
Source: World Health Organization 2014

Important Points about wearing PPE for Ebola
Before entering the isolation room/area: – Collect all equipment needed (time out) – Go to bathroom – Perform hand hygiene – Put on PPE
• in the order that ensures adequate placement of PPE items
• prevents self-contamination and self-inoculation while using and taking off PPE
Slide used with permission from World Health Organization

Important Points about wearing PPE for Ebola
• Instructions should be displayed on the wall.
• Supervised by another trained member of the team (buddy).
• A mirror can also help to check PPE
Images: http://www.ibtimes.co.uk/ebola-liberia-photos-west-point-slum-sealed-prevent-spread-disease-1462247
Slide used with permission from World Health Organization

RE-PROCESSING PPE
December 19, 2014

Cleaning PPE
• If necessary clean visors, goggles, boots: – Wear PPE – Clean with soap and water to remove any organic
matter – Prepare 0.5% chlorine solution daily – Immerse PPE fully overnight (minimum 30 minutes) – Rinse thoroughly with water and dry – Initial cleaning materials = infectious waste – Disinfection solution = pour down drain
December 19, 2014
Image: who.int Reference: WHO, 2014

How much PPE do I need? Things to consider: • Duration of each entry (in PPE) • Estimated number of entries per shift • Number of people caring for patient per shift • Number of days for each patient Additional considerations: • Lab and medical procedures per person • Time for re-processing of reusable PPE
ADD EXTRA 10% AS BUFFER UNEXPTECTED

HEAT - RELATED ILLNESS
December 19, 2014

Heat Related Illness
• Heat illness is a serious risk while wearing PPE in tropical conditions
• It is preventable • Heat storage is the major cause • Hydration is important but will not affect heat
storage • Team protocols are required for:
• Prevention • Heat illness monitoring • Heat illness treatment
Slide used with permission from World Health Organization

Heat storage
• YOU MUST PACE YOURSELF AND NOT OVER-EXERT – If you do not your core temp will rise rapidly and reach
critical levels in under one hour. – Plan your day – Limit time in PPE (45-1hr minutes) – Make sure you are hydrated
• Symptoms are a continuum of mild to moderate to severe and even life threatening

Heat Related Illness Spectrum
System Heat Cramps Heat exhaus0on Heat stroke
Temperature >380C >40.50C or 104.90 F
Skin Temperature Normal Normal or cool and clammy
Hot and dry (50% cases)
Sweat Rate Increased Increased or decreased
Decreased
Urine Output Normal Oliguria Anuria
GI Thirst Nausea +/-‐ vomiRng Nausea and vomiRng
CVS Tachycardia Hypotension +/-‐ Circulatory Collapse
CNS Nil Uncoordinated, Irritable or confused
Delirium/seizure/coma
Other Thirst Renal Failure Liver Failure DIC

Resources WHO 2014 Interim Infection Prevention and Control Guidance for Care of Patients with Suspected or Confirmed Filovirus Haemorrhagic Fever in Health-Care Settings, with Focus on Ebola http://apps.who.int/iris/bitstream/10665/130596/1/WHO_HIS_SDS_2014.4_eng.pdf?ua=1&ua=1 CDC 2014Guidance on Personal Protective Equipment To Be Used by Healthcare Workers During Management of Patients with Ebola Virus Disease in U.S. Hospitals, Including Procedures for Putting On (Donning) and Removing (Doffing) http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html

![aloqm 100] held — 6 JO alou ppe— 9 ppe ppe —L SŒOI-D d]eqs ... · aloqm 100] held — 6 JO alou ppe— 9 ppe ppe —L SŒOI-D d]eqs — papuadsns — pawawînv S-3d13-]8 qaqgqÐ](https://img.pdfslide.net/doc/110x75/5e6e0ef84965d5587c49d91e/aloqm-100-held-a-6-jo-alou-ppea-9-ppe-ppe-al-soi-d-deqs-aloqm-100.jpg)