Embed Size (px)
Citation preview

3/11/2013
1
Lory Bright‐Long, MD, CMDMedical Director, Maria Regina Residence
Psychiatry Consultant, LISVH
Clinical Assistant Professor of Psychiatry, SUNY Stony Brook
631‐299‐3006
ObjectivesAt the conclusion of this session the participant will:
Be prepared to discuss the scope and severity of the epidemiology of dementia
Demonstrate an understanding of the complexities of the neurobehavioral aspects of dementia
Recognize the societal and regulatory pressures associated with dementia care in today’s skilled nursing homes
Be able to educate staff about general trends in non‐pharmacological treatment of dementia behaviors
Be able to offer specific guidance about treatment of distressing behaviors
PET Scan of 20-Year-Old Brain PET Scan of 80-Year-Old Brain
PET and Aging
ADEAR, 2003

3/11/2013
2
Nosology of MCI
NORMAL
AGIN
G
AAMI
MCla
AACD
CIN
D
DEMENTIA
Cognitive Functionin
g
Lower
Higher
Nosological Categories
AAMI= Age‐associated memory impairment, 1 SD below young norms
MCIa= (amnestic) mild cognitive impairment, 1.5 SD below peer norms
AACD= Age‐associated cognitive decline,1 cognitive domain SD below peer
CIND= Cognitive impairment not dementia,> 1 cognitive domain (s) impaired
Moderate to Severe Memory Impairment(defined as recall of 4 or less words out of 20)
0
5
10
15
20
25
30
35
65-69 70-74 75-79 80-84 85+ all65+
MenWomen
Health and Retirement Study, Civilian/Non-institutional Population

3/11/2013
3
Impact on Baby Boomers14 million baby boomerscan expect to develop dementia, including Alzheimer’s disease
~ one in five women
~ one in seven men
~ more women than men will develop dementia because women live longer, on average
The Scope of the IssueRaising dementia numbers: Reported in 2010
(Chen, et al) at least 39.4% of NH residents had cognitive impairment, 80% with behavioral symptoms associated with dementia
2004: ADAMS reviewed representative community persons with dementia 21% AD, 5%CV, 26.8% other were prescribed antipsychotics
2007: Of 2.1 million residents, 304,983 (14%) had at least one Medicare claim for an atypical antipsychotic during the six-month period and represented 1/3 cost of care
Bhattacharjee S, et al. Psychotropic drug utilization among eldernursing home residents in the United States Psychiatric Services2010; 61:655-660.
3/11/2013
4
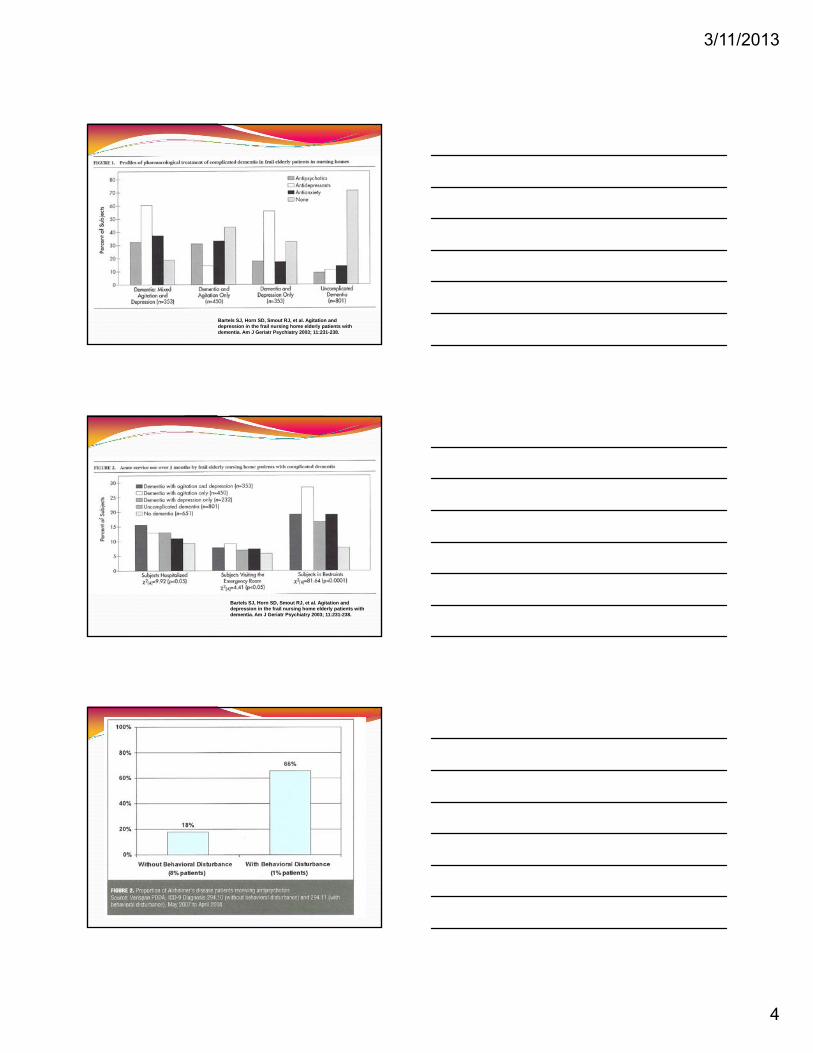
Bartels SJ, Horn SD, Smout RJ, et al. Agitation and depression in the frail nursing home elderly patients with dementia. Am J Geriatr Psychiatry 2003; 11:231-238.
Bartels SJ, Horn SD, Smout RJ, et al. Agitation and depression in the frail nursing home elderly patients with dementia. Am J Geriatr Psychiatry 2003; 11:231-238.

3/11/2013
5
Safely Reduce Hospital Readmissions: By March 2015, reduce the number of hospital readmissions within 30 days during a SNF stay by 15 percent.Increase Staff Stability: By March 2015, reduce turnover among nursing staff (RN, LPN/LVN, CNA) by 15 percent.Increase Customer Satisfaction: By March 2015, increase the number of customers who would recommend the facility to others up to 90 percent.Safely Reduce the Off-Label Use of Antipsychotics: By December 2012, reduce the off-label use of antipsychotic drugs by 15 percent.
Dementia Impacts What Is Important
Possessions
Volunteer Work
Pets
Laughter
Respect
Children
Pain free Religion
GardeningTravel
MarriageProperty
Job
Education
Money
Sports
Hearing
Eyesight
VacationsReading
Walking
Home
Right NOW
I believe that behavior itself is not a disease. Simply put, behavior is communication. In people whose ability to communicate with words is limited (such as patients with dementia), communication tends to be more nonverbal (i.e. behavioral). Our challenge is to figure out what they are trying to say, and if they are in distress, to identify the underlying causes and precipitants. Many of the behaviors that are commonly observed in patients with dementia and that are often labeled as difficult, challenging, or bad, such as agitation, wandering, yelling, inappropriate urination, and hitting are typically reactive, almost reflexive behaviors that occur in response to a perceived threat or other misunderstanding among patients who by the definition of their underlying illness have an impaired ability to understand. ... Jonathan M. Evans, MD, MPH, FACP,
CMDVice President, AMDA−Dedicated to Long Term Care Medicine

3/11/2013
6
THE WHERE AND WHY DEMENTIA HAPPENS…
Causes of Dementia
Morris JC. Clin Geriatr Med. 1994;10:257-276
Alzheimer’s disease60%
Vascular Dementia16%
AD with infarcts
8%
AD with Parkinson’s
disease8%Parkinson’s
disease withdementia
3%
Other dementias5%
Lewy Body Dementia10 – 20 %
Vascular Dementia
CORTICAL= Amnesia, Aphasia, 4 As Apraxia, Anomia
SUBCORTICAL= Dysmnesia, Delay, 4 Ds Dysexecutive sx,
Depletion
HIVDirect
neurotoxicityy

3/11/2013
7
DIFFERENTIAL DIAGNOSIS FOR MENTAL STATUS/MOOD CHANGES
D= DELIRIUM, Drugs, Depression
E= Eyes, Ears, Environment
M= Metabolic (heart, lung, liver, kidneys)
E= Endocrine (diabetes, thyroid)
N= Neurological, Normal Pressure
Hydrocephalus, Nutritional
T= Tumor, Trauma
I= Infection (CNS, general), Impaction
A= Anemia, ALCOHOL
Worsening ofDementia
Risk Factors
VulnerabilityAge
Preexisting cognitive impairmentPrevious delirium
CNS disorder, Basal ganglia disorder Increased blood brain permeability
EnvironmentalSocial isolationVisual deficits
Hearing deficitsImmobility
Novel environsStress
MedicalPAIN
Severity of comorbidityBurns
HIV/AIDSOrgan insufficiency
InfectionHypoxemia
FractureHypo/Hyperthermia
MetabolicDehydrationLow albumin
DrugPolypharmacyDrug/alcoholPsychoactive
Anticholinergics
SurgicalPerioperative
Type of surgeryEmergency ProcedureDuration of surgery
00
3030
MM
SE
MM
SE
Repetitive / Forgetful
Loss of ADLs
Behavioral Problems
NH Placement
Death
YearsGauthier, 1996
The Progression of Alzheimer’s Disease
Caregiver Distress
Difficulty with Complex Tasks
Early/ Mild Moderate Severe
No Treatment
AChI
AChI + Namenda

3/11/2013
8
Positron Emission Tomography (PET) Alzheimer’s Disease Progression vs. Normal Brains
G. Small, UCLA School of Medicine.
NormalEarly
Alzheimer’sLate
Alzheimer’s Child
Principles of Dementia Care Something can be done at all stages!
Excess disability is multi‐determined
Residual strengths matter
Presume the person has feelings and needs, even if not verbalized
Think of yourself and loved one as a unit
Continuing education and support is crucial
Sometimes behaviors require medication
Ensure safety, dignity, and quality of life
The Who, What, Where, When, Why, and How of Behaviors
Who has behavioral changes ?
What is a behavior?
Where to these behaviors happen ?
When do behaviors happen?
Why do behaviors happen ?
How do we handle behaviors ?

3/11/2013
9
PEAK FREQUENCY OFBEHAVIORAL SYMPTOMS AS AD PROGRESSES
Jost BC, Grossberg GT. J Am Geriatr Soc. 1996;44:1078‐1081
Months Before/After Diagnosis
‐40 ‐30 ‐20 ‐10 0 10 20 30
Frequency (% of Patients) 100
80
60
40
20
0
Agitation
DiurnalRhythm
Irritability
WanderingAggression
HallucinationsMoodChange
SociallyUnacc.
Delusions
Sexually InappropriateAccusatory
SuicidalIdeation
Paranoia
Depression
Anxiety
SocialWithdrawal
Incidence of Behaviors Apathy (72%)
Agitation (60%)
Anxiety (45%)
Irritability (42%)
Motor restlessness (38%)
Disinhibition (36%)
Sleep disturbance (24%)
Depression (23%)
Delusions (22%)
Hallucinations (10%)
The Stages of Alzheimer’s Disease
Mild Moderate SevereMild Moderate Severe
Memory lossLanguage
problemsMood and
personalitychanges
Diminishedjudgment
Withdrawal from activities
Require assistance with all IADLs*
Unable to learn or recall new info
Long-term memoryaffected
Behavioral,personality changes
Wandering, paranoia,aggression,
Placement initiated
Loss of ADL’sIncontinenceDysphagiaMuteMotor
disturbancesUnstable gait BedriddenPlacement
common
Stage
Symptoms
*IADLs = Instumental Activities of Daily Life phone,banking,shopping)

3/11/2013
10
THE A–B‐C‐Ds of Behavior Assessment
A
The antecedent – What happens before the behavior
B
The Behavior – Describe
C
The Consequence – What happens after the behavior. Are there rewards or negative results?
D
THE DANGEROUSNESS‐ FOR BOTH THE INDIVIDUAL AND THE CAREGIVER
Describe Specific Target Symptoms
Physical1,2 Verbal1,2 PassiveHitting Threats Silence
Pacing Accusations Poor po intakeKicking Name-calling WithdrawalBiting Obscenities Dead weightPushing Complaining ListlessSpitting Attention-seeking Hand wringingScratching Screaming Blank Stare
1. Cohen-Mansfield J. Int Psychogeriatr. 1996(Summer);8(2):233-245. (Review)2. Tariot PN, Mack JL, Patterson MB, et al. Am J Psychiatry. 1995(Sept);152(9):1349-1357
ANGER: A feeling of displeasure resulting from injury, mistreatment, opposition and usually showing itself in a desire to fight back at the supposedcause of this feeling
When are you more likely to feel angry?
confronted with something you don’t understand ?
slighted ?
someone does not listen to you ?
something unjust occurs ?
unfairly accused ?
you don’t get your way ?
you’re tired ?
impatient ?

3/11/2013
11
AGITATION: Physical or vocal behavior that is distressing to the individual or those around the person and not in response to a specific need.
Despite the physical or vocal behavior, it is NOT agitation if there is a physical or emotional unmet need
A catch‐all term that has little meaning
Learn to describe the behavior specifically
Learn to quickly assess the situation for causes of distress
Behavioral Interventions
Behavioral contracting
Behavioral modification and token systems
Brief directive psychotherapy
Desensitization
Distraction
Family therapy
Group therapy
Hypnosis
Milieu and attitude therapy
Paradoxical therapy
Reframing the problem
Relaxation training
Reminiscence and milestoning
Time out
Validation
Restrictive and aversive therapies (Only in special units)
GENERAL TIPS IN ADDRESSING BEHAVIORS:
Modify the setting to “fit” demented resident’s needs, not vise versa.
Socialization to decrease loneliness, increase self esteem and well being.
Integrating with community and familiar activities, especially intergenerational.
When there is aggression, investigate roles of caregiver
Offer a variety of choices but limit decision‐making.

3/11/2013
12
Offer a variety of choices but limit decision‐making..
Listen to what the person is trying to say (Validation)
I want to go home: “I’m lonely”, “I’m lost”, “Nothing looks familiar”
I have to get to work: “I don’t feel important now”, “I need something to do”,
Where is my mother?: “I have to be taken care of…”
MORE GENERAL TIPS IN ADDRESSING BEHAVIORS:
RESISTIVENESS:
CalmnessMatter-of-factExplain each procedure simplyPrivacy and modesty are keyOffer single steps Offer opportunity to participateTalk during process.
SUSPICIOUSNESS:
BE CALM Please don’t take it personally Avoid arguments.
Do not whisper or discuss things in front of the person as if they are not there
Help look for missing items Know hiding places Keep duplicates Reduce clutter Always check the waste baskets and
pockets
3/11/2013
13
Aggression severe restlessness: BE CALM
Try music
Find constructive tasks
Use food and other pleasant distractions
HAVE AN EMERGENCY PLAN
Wandering:Identification
Label rooms and objects
Use pictures
Monitoring
Mental
Learning
Creativity
Flexibility
Focus
Examples of VALIDATION Rose has to get home to feed her children lunch.
Bud has to catch a bus into the City.
All Irene can do is rock
Herb pounds on the desk or the chair table or anything he can get his hands on
Helen seems angry (or sad, or frightened) most of the time

3/11/2013
14
Physical
Exercise
Diet
Sleep
Share symptoms with your doctor
Avoid medicating oneself
Increases strength and vigor, therefore, increase opportunities for more interaction.
Decreases depression, therefore, increases self esteem and well being.
Fatigues elders, therefore, decreases wandering, agitation, pestering.
Keeps person active in day, therefore, resynchronizes schedule for night‐time sleep.
Fostering reminiscence and relationships.
Dementia – TreatmentNon‐pharmacologic alternatives to antipsychotics: Evidence grades from A (strongest) to D (weakest)
RCT: randomized controlled trial
Treatment Evidence/Results
Caregiver psycho education/support Several positive RCT’s (evidence grade A)
Music Therapy 6 RCT’s positive in the short term (evidence grade B)
Cognitive stimulation therapy Three‐quarters of RCT’s showed some benefit (evidence grade B)
Snoezelen therapy (controlled multisensory stimulation)
3 RCT’s with positive short‐term benefits (evidence grade B)
Behavioral management therapies (by professionals)
Largest RCT’s with some benefits (evidence grade B)
Staff training/education Several positive studies of fail‐to‐goodmethodological quality (evidence Grade B)
Reality orientation therapy Best RCT showed no benefit (evidence grade D)
Teaching caregivers behavioral management techniques
Overall inconsistent results (evidence Grade D)
42

3/11/2013
15
Dementia – TreatmentNon‐pharmacologic alternatives to antipsychotics:
Evidence grades from A (strongest) to D (weakest)
RCT: randomized controlled trial
Treatment Evidence/Results
Simulated presence therapy Only 1 RCT which was negative (evidence grade D)
Validation therapy 1 year RCT with mixed results (evidence grade D)
Reminiscence therapy A few small studies with mixed methodologies (evidence grade D)
Therapeutic activity programs (such as exercises, puzzle play)
Varied methods and inconsistent results (evidence grade D)
Physical environment stimulation (such as altered visual stimuli, mirrors, signs)
Generally poor methodology and inconsistent results; best results with obscuring exits to decrease exit‐seeking (evidence grade D)
43
Emotional
Getting and giving love
Joy
Awareness of one’s emotions
Control over reaction to emotions
THE BILL OF RIGHTS1. Know one’s diagnosis2. Have appropriate/ongoing medical care3. Have the opportunity to be productive in
work and play as long as possible4. To be treated like an adult, not a child5. To have expressed feelings taken seriously6. To be free of unnecessary medications7. To be in a safe, structured, predictable
environment8. To have meaningful activities available9. To have the opportunity to be outdoors10. To have physical contact11. To have those around me know of my
background, culture, and values12. To be cared for by people who are trained
in dementia care

3/11/2013
16
Spiritual
Connection with something bigger than self
Values
May or may not be about organized religion
Symptoms and Syndromes Overlap

3/11/2013
17
Neurotransmitter Deficiencies in AD
Nucleus basalisof Meynert
(acetylcholine)
Raphe nuclei(serotonin)
Locus ceruleus(norepinephrine)
Examples of Use of Metaphors “Depressive”
Irritable, pessimistic, sad, weepy, socially withdrawn,vegetative features
A place for antidepressant trial
“Psychotic” Angry when approached, overly suspicious, fragmented speech/thinking
A place for possible antipsychotic medications
“Manic” Euphoric, irritable, accelerated, hypersexual, silly
A place for mood stabilizers
Medications Available
Cognitive enhancers
Cholinergic medications
NMDA receptor blockers
Antidepressants
Mood Stabilizers (AED)
Antipsychotics
Anxiolytics
Hypnotics
Barbituates / Miscellaneous

3/11/2013
18
Maher, et al. Efficacy and comparativeEffectiveness of atypical antipsychotic medications for off-label uses in adults
Dementia – TreatmentPharmacologic alternatives to antipsychotics:
Treatment Evidence/Results
Selective serotonin reuptake inhibitors
2 positive studies with citalopram (more effective than placebo for agitation in 1 trial and equivalent to risperidone for psychosis and agitation with greater tolerability in the other); 2 negative trials with sertraline
Other antidepressants 1 study showed trazodone was equivalent to haloperidol for agitation, with greater tolerability; another found trazodone was no different from placebo; other agents have only case reports or open label trials
Anticonvulsants 3 trials showed divalproex was equivalent to haloperidol for agitation, with greater tolerability problems in both; other agents tried only in case reports or open‐label trials
Benzodiazepines/ anxiolytics
3 trials showed oxazepam, alprazolam, diphenhydramine, and buspirone were equivalent to haloperidol in effects on agitation, but none used a placebo control; trials had problematic methodologies and indicated cognitive worsening with some agents (especially diphenhydramine)
Cognitive enhancers Some evidence of modest benefit in mostly post‐hoc data analyses in trials designed to assess cognitive variables and often among participants with overall mild psychiatric symptoms; prospective studies of rivastigmine and donepezil specifically designed to assess neuropsychiatric symptoms have found no difference compared with placebo
Miscellaneous drugs Failed trial of transdermal estrogen in men; small study showed propranolol (average dose 106 mg/d) more effective than placebo 53
SIDE EFFECTS AS A DECISION-MAKING TOOL

3/11/2013
19