Embed Size (px)
Citation preview

Peter J F Baskett
Hypovolaemic shock is a clinical state in which tissue perfusion is renderedrelatively inadequate by loss of blood or plasma after injury to the vascularfree.
A reduction in blood volume produces a fall in systolic pressure, whichtriggers a sympathetic catecholarnine response that results in peripheralvasoconstriction, a rise in pulse rafe, and a reduction in pulse pressure. Therachycardia and increased cardiac contractility lead to an increasedmvocardial oxygen requirement.
"Blood flow to the skin and peripheral tissues is reduced in an effort topreserve reasonable perfusion of vital organs such as the brain, heart, liver,and kidneys. If there is continuing blood loss inadequate tissue perfusionresults in anaerobicmetabolism, acidosis, and reduction in the performanceof the vital organs. Further myocardial depression accelerates ibis process,and pain stimuli add to the sympathetic outburst.
Pathophysiology of hypovolaemic shock.
The following are early symptoms and signs ofhypovolaemic shock. They reflect the underlyingpathophysiology .
Classification of hYPovolaemic shock according to blood 1055
Classl Classll Class 111 Class IV
Blood loss:
PercentageVolume (mi)
Blood pressure:
SystolicDiastolic
<15750
15-30800- 1500
30-401500-2000
>40>2000
UnchangedUnchanged
Normal Reduced Very lowRaised Reduced Very low or
unrecordable100-120 120 (Thready) >120 (Very
thready)Slow (>2s) Slow (>2s) UndetectableNormal Tachypnoea Tachypnoea
(>20/min) (>20/min)20-30 10-20 0-10
Pulse (beats/min) Slight
tachycardiaCapillary refill NormalRespiratory rafe Normal
Urinary flow rate >30(ml/h}Extremities Colour normal Paje Pale Paje and coldComplexion Normal Paje Pale AshenMental state Alert Anxious or Anxious, Drowsy,
agressive agressive. or confused, ordrowsy unconscious
.Hypotension (due to hypovolaemia, perhapsfollowed by myocardial insufficiency).Skin pallor (vasoconstriction due tocatecholamine release).Tachycardia (due to catecholamine release).Confusion, aggression, drowsiness, and coma(due to cerebral hypoxia and acidosis).Tachypnoea (due to hypoxia and acidosis).General weakness (due to hypoxia andacidosis).Thirst (due to hypovolaemia).Reduced urine output (due to reducedperfusion).
Symptoms of hypovolaemia according to bloodloss
In most cases the signs and symptoms can berelated to the amount of blood loss, which can be--~ classified in four broad groups (classes I-IV).
In previously healthy young adults systolic pressure is often preserveddespite quite appreciable blood loss (1'5-2'0 litres) owing to the effectiveresponse to sympathetic stimulation. Eventually, however, there is aprecipitous fall as the myocardium suddenly fails because of hypoxia andacidosis. Conversely, patients with coronary arterial disease may becomehypotensive because of myocardial insufficiency after only modest bloodlosses of up to 500 mI.
Blood loss Class Symptoms(mi)
<750-1500 11
NoneCardiovascular signs due tocatecholamine release:thirst. weakness. tachypnoeaSystolic pressure fallsSystolic pressure becomesunreadable
Patients receiving certain drugs (for exaw:- ~e, j) blockers) mar not be ableto produce an appropriate sympathetic response and may also becomehypotensive after modest blood loss. Also, it must be taken into accountthat intravascular loss is accompanied by additional fluid deplerion of theinterstitial space, whÍch amounts to about 25% ofthe overt blood loss.
-2000>2000
111
IV
BMJ VOLUME 300 2 JUNE 1990 1453
Gencrally. losses of up to 750 mI (class 1) (ISl!iu of the circulating blo\~\'olume) Jo not generate an~' pronounceJ signs or symptoms. Furthcrhaemorrhage. amounting to 1'51itres :..clas:; 11). produces cardiovasc.:ularsigns ofc.:atecholamine release. thirst, weakness, and tachypnoea, Svstolicpres:;ure continues to fatI a:; blood 10:;s mounts to 21itres (class 111) añd oftenbecomes unreaJable after 2-5.3.0 litre:; \c1ass IV) have been (ost,
Resuscitation of patients withtrauma
(1) Adequate pulmonary oxygenation
(2) Control of haemorrhage
(3) Replacement of lost volume
The objective of the management of hypovolaemic shock is to maintaintissue oxygenation anJ restore it to normal values. This entails applying thebasic principies of resuscitation of patients with trauma. Resuscitation isfollowed by definitive treatment ~incluJing surgery).
(4) Monitoring the effects-ofj.1Y. (2). and(3) .
(5) Support of myocardial contractility
~61 Relief of pain ~-
Pulmonary oxygenationTo ensure optimal pulmonary oxygenation patients with hypovolaemic
shock should have a clear airway and be adequately ventilated with oxygenat a high inspired concentration. Unconscious patients with severe shockshould be intubated and ventilated with 100% oxygen, and care should betaken to exclude impairment of ventilation due to pneumothorax,haemothorax, or diaphragmatic elevation caused by gastric distenúon.
Peripheral haemorrhage should be controlled by elevation of the injuredpart and by placing a firm pad and bandage over the wound. Tourniquetsare rarely advised though may be essential and are relatively harrnless inpatients who are going to undergo amputation. Probing in the wound tosearch for ruptured vessels is not recommended outside the operating room.
Control oí haemorrhage
For peripheral haemorrhage:"Pans in the air. press on the hole"
Replacement of loss-~~' { \.
r:'\ -¡: \..'i) sternomastOtd\!J muscle
Carotid artery
~ ' ~ Intemal jugular
" /-"veln
~ -Clavlcle\ ~'I '-Subclavian vein
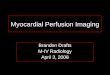
Losses of blood should be replacedintravenously in response to clinical signs andsymptoms and in all patients estimated to havelost more than 750 mI.@ f ~
Carotid artery~Internal j~gUla~ vein ~1 (
\ ~\\ ,"-I ¡.!, ",! --7
1 ntravenous cannulationThe site of haemorrhage should be considered
carefully when cannulation is undertaken. Thereis little point in setting up an infusion in aninjured limb or in the femoral vein in a patientwith pelvic or abdominal injuries. With Ibisproviso the peripheral veins ofthe arm, ifaccessible, are traditionally preferred forcannulation. There is much to be said, however,for more central access through a short cannula inthe subclavian or internal jugular vessels, whichare less subject to constriction and feed almostdirectly into the right atrium. Preference for oneor other site is individual according to experience
Iand expertise. In patients with injuries of theneck and arms the femoral vein is preferable. IVenous cut clown techniques are time Iconsuming, rarely necessary, and usually lesseffective iban direct cannulation of a central vein.1
f~\)~' \\.~ )
~
0 d
l Subclav '\ ,
I -\\ \~ -J'.--
Cannulation 01 the jugular vein ((a) and (b)) and 01 the subclavian vein ((c)
and (d)).
AI
{~-i~nominate vein\\ ""'\ Superior vena
\ cava
"
The diameter of the can nula in a cannula over needle svstem should benot less than 14 gauge. Cannulas of 10 gauge can be easily inserted into theinternal iugular or subclavian veins. Long liDes from the antecubital fossaare not suitable for rapid transfusion as the ftow rafe is inversely related to
the length of the catheter.
2 Jl'NE 19tBMJ VOLUME 3001454
Intravenous fluid replacement inhaemorrhagic shock
Class 1 251 Ringer-lactate
Ihaemorrhage solution or 101150ml (15~~)) polygelatin
Class 11 1.01 polygelatin plus 151
(haemorrhage 800 Ringer-lactate solution-1500ml (15-30%))
Choice 01 intra-z'enous jluid
Inrravenous fluids should be given ro resrore an adequare circularing bloodvolume. Normal elecrrolyre and coagularion consriruenrs and colloidosmoric pressure and a packed cell volume above30% are necessary roensure adequare oxygen car~.ing capaciry. The choice of inrravenous fluidsin clinical pracrice líes among crysralloid, colloid, and albumin solurions;bh)od in rhe !orm of \\'hole blood or packed red cells; and a judicious mix ofallofrhese.
Class 11I 10 I Ringer-lactaté-(haemorrhage solutionplus o-si1500-2000 mi (30- polygelatin plus 10-1 5140%)) wholebloodor1-0-1-SI
equal volumes ofconcentrated red cells
--~ and polygeiatin
Colloid solutions replace intravascular loss and restore haemodynamicvalues towards normal. They do not replace interstitialloss. Crystalloidsolutions replace borh intersririal and intiavascular loss, but large volumesare required to restore normal haemodynamics. In pracrice, a combinarionof a crystalloid solution and a colloid solution should be given to patientswith blood loss of more chao llitre.
Class IV
(haemorrhage2000 mi (48%»)
10 I Ringer-lactatesolution plus 1-0 Ipolygelatin plus 2-0 Iwhole blood or 2-0 I equalvolumes concentratedred cells and polygelatinor hetastarch
Colloíd solutíons are generally iso-oncotic and may be used to replace lostvolumes of blood on al: 1 basis, restoring haemodynamic variables tonormal values. Polygelatins are cheap and effective blood volumeexpanders. They have a long shelf life of six years, a half life in vivo of six toeight hours, and a low index of causing anaphylatic reactions. Haemaccelhas a similar electrolyte content ro plasma whereas Gelofusine contains verylitrle potassium. Both are suitable for replacing blood losses of up to llirreand in patients with more extensive haemorrhage when used in ~ombinarionwirh blood rransfusion ro maintain a packed cell volume of 30%.
Hetastarch (6% in isotonic saline) is an effective blood substirure inpatients with mild and moderare bl00d loss. It is more expensive than rhepolygelatins bur has a much longer halflife (12 ro 14 hours) in rhecirculation. CaTe must be raken, rherefore, to avoid circulation overloadwhen blood is transfused at a later stage to restore the packed cell volume.The incidence ofanaphylactic reactions is low.Intravenous replacement fluids.
Crystalloid solutions -Ringer-lactate solution may be used in patientswith mild class 1 haemorrhage of up to 15% of blood volume. Replacementvolumes should be three to four times the estimated loss as the electrolytesolution is distributed throughout the extracellular (intravascular andinterstitial) space. The volume should be increased to compensate for urineloss. Vascular support with isotonic electrolyte solutions is short lived.
Intravenous infusion in a military surgery.
Disadvantages of blood transfusionin hypovolaemic shock
.Time is reQuired to group and cross matchindividua! units of blood.Blood has a high viscosity and themicrocirculation in shock may be improvedby a reduction in packed cel! volume
.Blood sto red for more than a few days hasa high potassium ion concentration and theplatelets and white cells fragment rapidly,losing normal function
.Blood and certain blood products may beinfected. (The risk of acQuiring HIV infectionfrom transfused blood has been virtuallyeliminated in the United Kingdom)
Blood- Whole blood or packed red cells are required in patients withmoderate and major blood loss to maintain a packed cell volume of 30%. 1 t isnot desirable to strive for higher values in the early stages of volumeresuscitation as a modest reduction in packed cell volume allowsimprovement in the rnicrocirculation, especially in the presence ofarteriolar vasoconstriction.
Though whole blood is the ideal replacement in patients with majorhaemorrhage, limitations of supply mar dictate that concentrated red cellsare used, diluted to normal values of packed cell volume by concurrenttransfusion of polygelatin or hetastarch.
Trauma and obstetric centres should retain a small number of relativelyfresh units of O negative blood for immediate transfusion in cases of severe,life threatening haemorrhage.
Blood transfused rapidly should be warmed before infusion to maximiseflow rates and to minimise the risk of cardiac arrhvthmia and corehypothermia. Blood filters havé not been proved (o be of value.
BMJ VOLUME 300 2 jUNE 1990 1455
,-\ulvlvgvus blovd -In parients wirh severe rhoracic or abdominal injuries"clean" blood may be aspirated from the cavity, anricoagulated, andrerurned ro rhe parit:nt rhrough an inrravenous cannula using a "cell sa\'t:r"system. Autologous blood is valuable in patients with majar vascularinjuries of rhe rhorax and abdomt:n and in rhose with a ruptured liver orspleen, bur clearly rhe procedure cannot be applit:d in patients withabdominal trauma who ha ve a ruprured bowel or in thost: \vith thoracictrauma who have oesophageal or lung damage. The rranstusion ofamologous blood has several advantages, particularly if blood ora patient'sblood group is in short supply. The blood is the parienr's o\vn, fret: ofinft:ction, warm, and immt:diarely available.
Coagulation problemsCoagulation problems occur in patiems with massive blood loss beca use
of dilution with blood substitutes and the fact that coagulation factorsdeteriorate rapidly in stored blood. ,\\oreover, tissue destruction releasesvarious products that inhibit the normal coagulation process. The clottingprocess should be monitored by regular screening and deficiencies treateddefinitively rather than by infusion of valuable fresh frozen plasma andplatelets on an arbitrary basis.
Aspiration of "clean" blood from the cavity.
Monitoring progress and treatment
Variables to monitor inhypovolaemic shock
.Pulse rate.Arterial pressure
.Pulsepressure.Central venous pressure
.Urinaryoutput.Changes in the electrocardiogram
.Temperature
.Peripheral oxygen saturation
.Mental state
Requirements for bloodvolume replacement should be based on all offactors in the box, particularly pulse cate, arterial pulse and central venouspressures, peripheral oxygen saturation, and urine flow cates. Transfusionshould be continued to produce an adequate arterial pressure, a urine flowof SO ml/h, and a central venous pressure that responds to a rapid infusion of200 mI by a sustained rise of more than 3 cm H2Oover the previous value.
If these variables improve and the improvement is maintained thenclearly the blood loss is under control. Failure to maintain the improvedvalues indicates continuing loss and requires further transfusion and earlysurgery. If the patient does not respond satisfactorily to transfusions thecate ofloss is exceeding the fastest possible cate of intravenous replacement.This is usually associated with majar thoracic, abdominal, or pelvicinjuries. In such instances the Patient must be taken to the operating roomfor immediate thoracotomy or laparotomy and bleeding controlled withclamps or packs, or both, while the anaesthetist "catches up" with thetransfusion requirements. Salvage of autologou~ ~ma~. ~. ap~priate.
.-,,- ¿...
-.: .-, ";,}c :'cA rising central venous pressure~ted Withaldw artért~Pressure,
tachycardia, and a reduced uritíe'outPQ\indicates. tensiOD pneumothorax,cardiac tamponade, or cardiac f~Cardiac tamponade is treated bythoracotomy, sometimes preceded 'by relief needle paracentesis. In patientsrequiring inotropic support because of myocardial failure measurement ofpulmonary wedge pressure with a Swan-Ganz catheter may be helpful incomparing individual ventricular load and performance. In most patientswith previously normal hearts, however, the central venous pressure andthe pulmonary artery wedge pressure follow each other closely and the extraexpense of this invasive technique is unjustified.
/~
/
Cardiac contractility and renal output
A patient with a previously impaired myocardium may need inotropicsupport with dopamine and dobutamine. Such support is not a substitutefor adequate volume replacement but is used to enhance myocardialcontraction if required. Rates of dopamine infusion should be confined to"renal" doses (up to S ¡.lg/kg/h) that enhance urine output. Higher dosescause vasoconstriction and tachycardia, which results in an increase inmyocardial oxygen demand that may not be achievable because ofinadequate myocardial blood flow. Dobutamine should than be added to
improve myocardial performance.
Inotropic drugs.
2 jUNE 199~BMJ VOLU.\iE 3001456