Embed Size (px)
Citation preview
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 1 of 29Section 2D – Batch 2014
COMPREHENSIVE TABLE OF DRUGS1st Shifting Period
NOTE: Should there be any discrepancies between this table and what’s written in the transes, please consult KATZUNG for confirmation and go instead with what’s indicated in the textbook. Thank you!CHOLINERGIC AGONISTS (PARASYMPATHOMIMETICS)
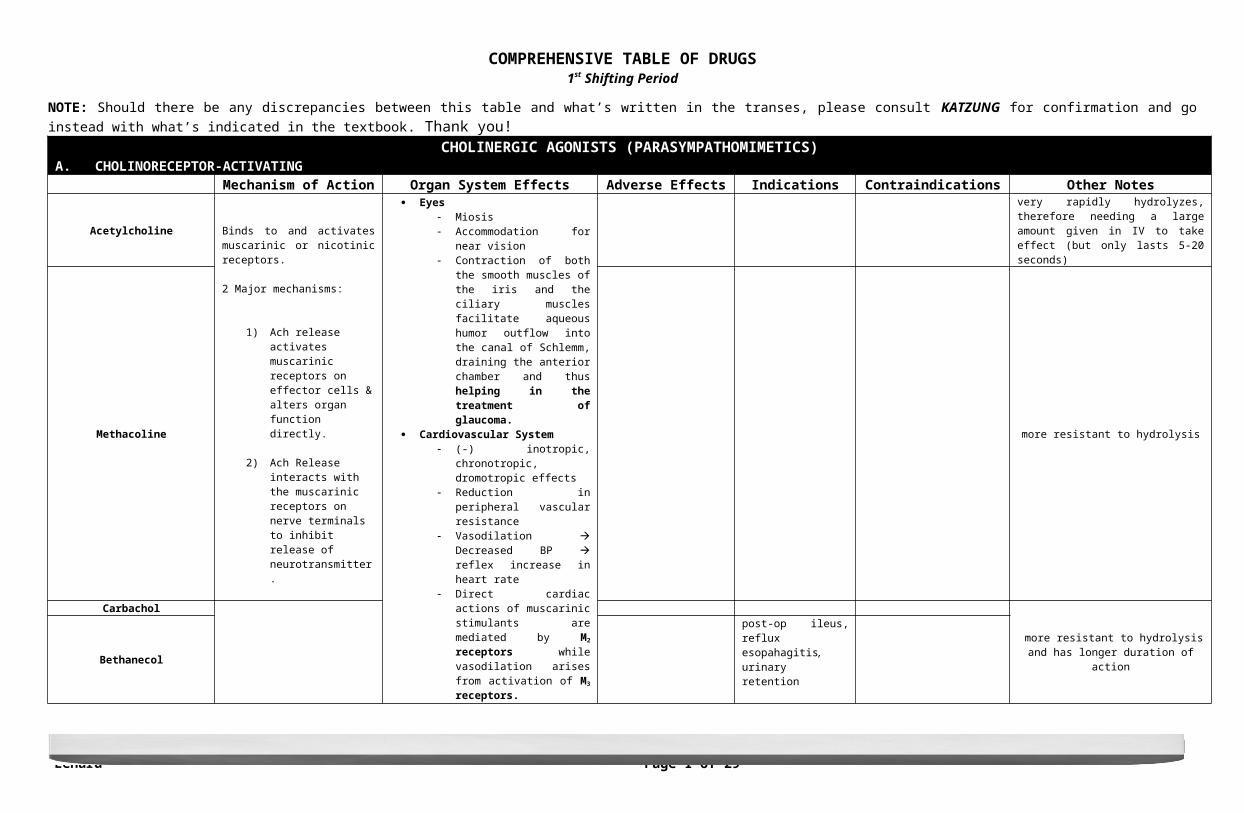
A. CHOLINORECEPTOR-ACTIVATINGMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
AcetylcholineBinds to and activates muscarinic or nicotinic receptors.
2 Major mechanisms:
1) Ach release activates muscarinic receptors on effector cells & alters organ function directly.
2) Ach Release interacts with the muscarinic receptors on nerve terminals to inhibit release of neurotransmitter.
Eyes Miosis Accommodation for near vision Contraction of both the smooth
muscles of the iris and the ciliary muscles facilitate aqueous humor outflow into the canal of Schlemm, draining the anterior chamber and thus helping in the treatment of glaucoma.
Cardiovascular System (-) inotropic, chronotropic,
dromotropic effects Reduction in peripheral vascular
resistance Vasodilation Decreased BP
reflex increase in heart rate Direct cardiac actions of
muscarinic stimulants are mediated by M2 receptors while vasodilation arises from activation of M3 receptors.
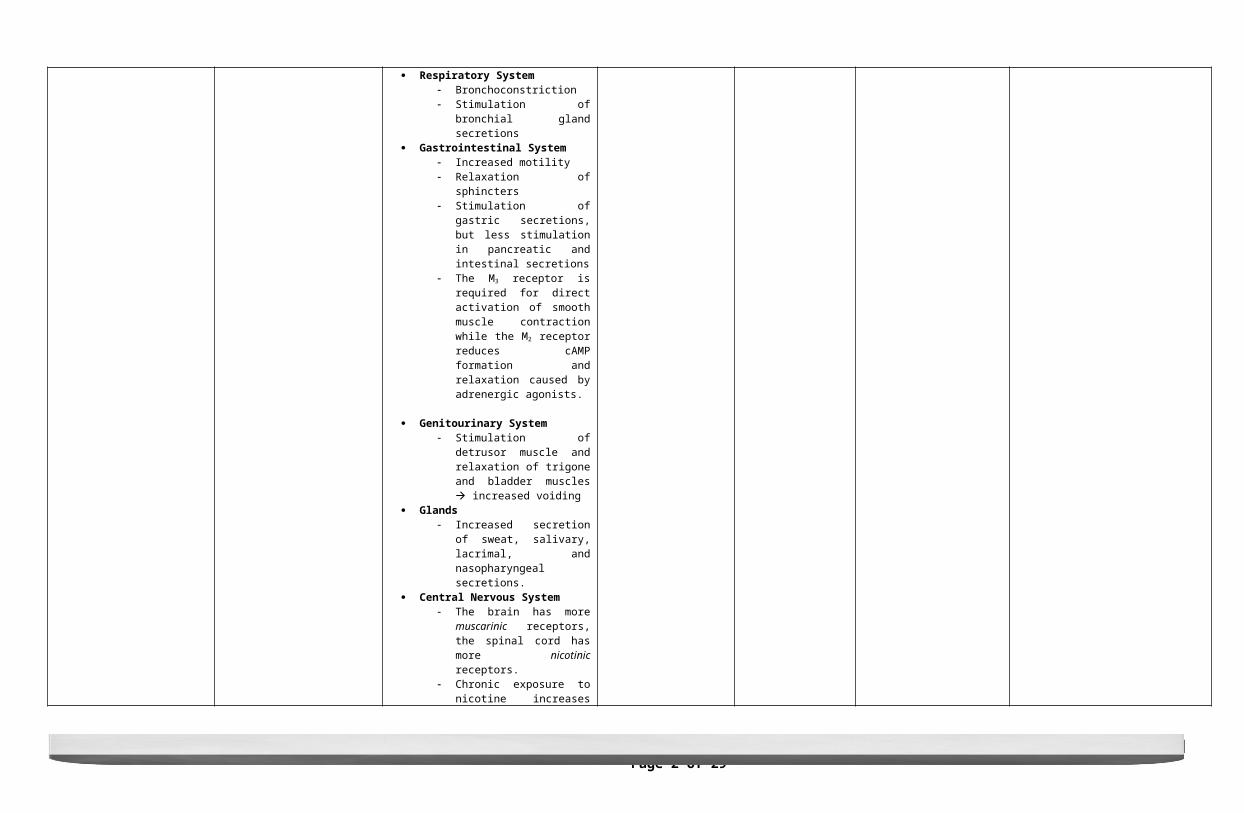
Respiratory System Bronchoconstriction Stimulation of bronchial gland
secretions Gastrointestinal System
Increased motility Relaxation of sphincters Stimulation of gastric secretions,
but less stimulation in pancreatic and intestinal secretions
The M3 receptor is required for direct activation of smooth muscle contraction while the M2 receptor reduces cAMP formation and relaxation caused by adrenergic agonists.
Genitourinary System Stimulation of detrusor muscle and
relaxation of trigone and bladder muscles increased voiding
Glands Increased secretion of sweat,
salivary, lacrimal, and nasopharyngeal secretions.
Central Nervous System The brain has more muscarinic
very rapidly hydrolyzes, therefore needing a large amount given in IV to take effect (but only lasts 5-20 seconds)
Methacoline more resistant to hydrolysis
Carbachol
more resistant to hydrolysis and has longer duration of actionBethanecol
post-op ileus, reflux esopahagitis, urinary retention
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 2 of 29Section 2D – Batch 2014
receptors, the spinal cord has more nicotinic receptors.
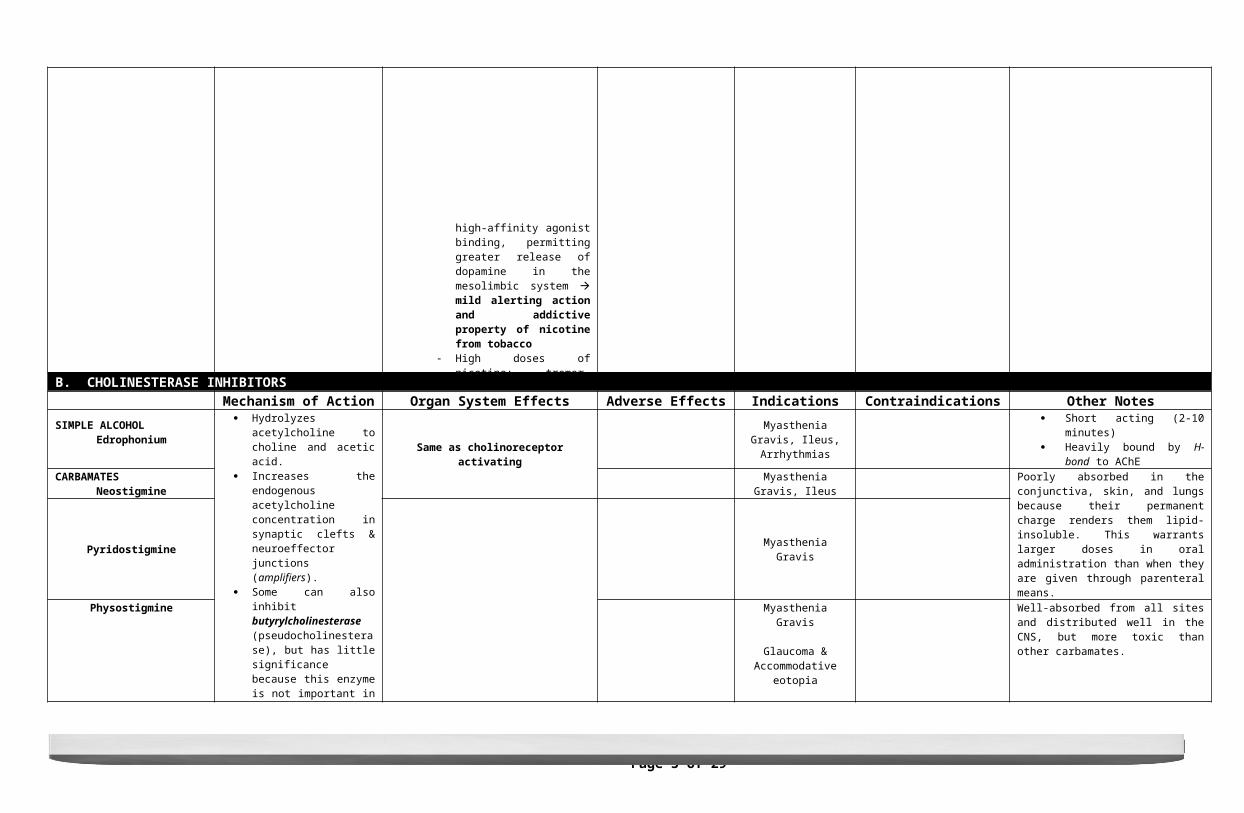
Chronic exposure to nicotine increases high-affinity agonist binding, permitting greater release of dopamine in the mesolimbic system mild alerting action and addictive property of nicotine from tobacco
B. CHOLINESTERASE INHIBITORSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
SIMPLE ALCOHOLEdrophonium
Hydrolyzes acetylcholine to choline and acetic acid.
Increases the endogenous acetylcholine concentration in synaptic clefts & neuroeffector junctions (amplifiers).
Some can also inhibit butyrylcholinesterase (pseudocholinesterase), but has little significance because this enzyme is not important in the physiologic termination of synaptic acetylcholine action.
Same as cholinoreceptor activating
Myasthenia Gravis, Ileus, Arrhythmias
Short acting (2-10 minutes) Heavily bound by H-bond to AChE
CARBAMATESNeostigmine Myasthenia Gravis, Ileus Poorly absorbed in the conjunctiva, skin, and
lungs because their permanent charge renders them lipid-insoluble. This warrants larger doses in oral administration than when they are given through parenteral means.
Pyridostigmine Myasthenia Gravis
Physostigmine
Myasthenia Gravis
Glaucoma & Accommodative eotopia
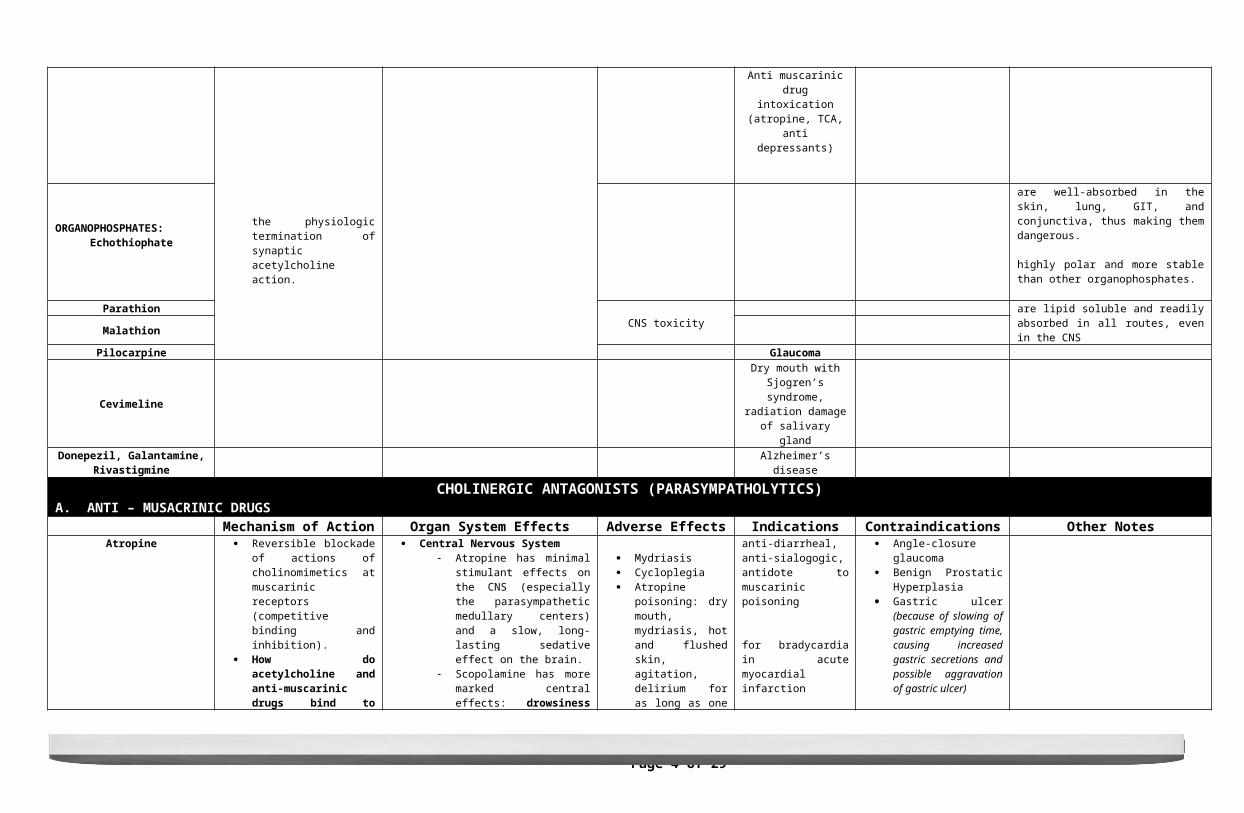
Anti muscarinic drug intoxication (atropine, TCA,
anti depressants)
Well-absorbed from all sites and distributed well in the CNS, but more toxic than other carbamates.
ORGANOPHOSPHATES:Echothiophate
are well-absorbed in the skin, lung, GIT, and conjunctiva, thus making them dangerous.
highly polar and more stable than other organophosphates.
Parathion CNS toxicity are lipid soluble and readily absorbed in all routes, even in the CNSMalathion
Pilocarpine Glaucoma
CevimelineDry mouth with Sjogren’s
syndrome, radiation damage of salivary gland
Donepezil, Galantamine, Rivastigmine Alzheimer’s disease
CHOLINERGIC ANTAGONISTS (PARASYMPATHOLYTICS)A. ANTI – MUSACRINIC DRUGS
Mechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 3 of 29Section 2D – Batch 2014
Atropine
Reversible blockade of actions of cholinomimetics at muscarinic receptors (competitive binding and inhibition).
How do acetylcholine and anti-muscarinic drugs bind to muscarinic receptors? Aspartate in the third transmembrane segment of the muscarinic receptors forms a nitrogen bond with the nitrogen ion of acetylcholine and the anti-muscarinic drugs, which explains their competitive binding.
When atropine binds to the muscarinic receptor, it prevents two mechanisms: the release of IP3 and the inhibition of adenylyl cyclase.
Since the blockade produced by these drugs is reversible, their effects can be overcome by increased concentrations of acetylcholine or other muscarinic agonists.
Because they do not block nicotinic receptors, these drugs have little to no action at skeletal neuromuscular junctions or autonomic ganglia.
Muscarinic receptors are constitutively active, and drugs that block the actions of acetylcholine are inverse agonists that shift the equilibrium of the receptor to its inactive state.
Most sensitive in salivary, bronchial, and sweat glands.
Least sensitive in gastric parietal cells.
Atropine more effectively blocks exogenously-administered cholinoceptor agonists than endogenously-released acetylcholine.
Central Nervous System Atropine has minimal stimulant
effects on the CNS (especially the parasympathetic medullary centers) and a slow, long-lasting sedative effect on the brain.
Scopolamine has more marked central effects: drowsiness and amnesia; can also cause excitement, agitation, hallucinations, and coma in toxic doses.
Reduction of tremors in Parkinson’s disease. Parkinsonian tremors are caused by a relative excess of cholinergic activity because of a deficiency of dopaminergic activity in the basal ganglia-striatum system.
Motion sickness appears to involve muscarinic cholinergic transmission. Best alleviated by scopolamine.
Eyes The pupillary constrictor muscle
depends on muscarinic cholinergic activation. This activation is blocked by anti-muscarinic drugs and results in mydriasis (pupillary dilation).
Cyclopegia – weakening the contraction of the ciliary muscle, resulting in the loss of the ability to accommodate and thus cannot focus on near vision.
Decreased lacrimal secretion Cardiovascular System
Tachycardia due to sensitivity of the sinoatrial node to muscarinic receptor blockade (particularly the prejunctional M1 receptors) that results in vagal slowing. Lower doses sometimes produce initial bradycardia before tachycardia manifests.
Reduced PR interval in the ECG – due to blocking of muscarinic receptors in AV node
Constriction of coronary arteries and skeletal muscle vessels; can also cause cutaneous vasodilation in upper parts of the body in toxic doses.
Has little effect on blood pressure. Respiratory System
Bronchodilation
Mydriasis Cycloplegia Atropine poisoning: dry
mouth, mydriasis, hot and flushed skin, agitation, delirium for as long as one week. Remember: “Dry as a bone, blind as a bat, red as a beet, mad as a hatter.”
Hyperthermia, especially in children
anti-diarrheal, anti-sialogogic, antidote to muscarinic poisoning
for bradycardia in acute myocardial infarction
for routine pre-operative medications to counter the increase in airway secretions and laryngospasms induced by anesthetics
Angle-closure glaucoma Benign Prostatic
Hyperplasia Gastric ulcer (because of
slowing of gastric emptying time, causing increased gastric secretions and possible aggravation of gastric ulcer)
Scopolamine
anti-spasmodic, anti-motion sickness
for reduced amnesia associated with surgical or obstetric delivery
for routine pre-operative medications to counter the increase in airway secretions and laryngospasms induced by anesthetics
rapidly and widely distributed in the CNS, where it has a greater effect there than other anti-muscarinic drugs.
Dicyclomine anti-spasmodicBenzropine Anti - parkinsonism
Homatropine
mydriatic, cycloplegic
for synechia (adhesion in uveitis and iritis)
Also used for complete ophthalmologic examination through induction of temporary ciliary paralysis
IpratropiumTiotropium
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 4 of 29Section 2D – Batch 2014
Reduced tracehobronchial secretions
The effectiveness of non-selective anti-muscarinic drugs are not as useful in treating COPD because the blockade of M2 receptors on postganglionic parasympathetic nerves can oppose the bronchodilation caused by block of M3 receptors.
Gastrointestinal System Blockade of muscarinic receptors
cannot totally abolish GI activity because of influences from local hormones and non-cholinergic neurons in the enteric nervous system.
Decreased volume of pepsin, acid, and mucin secretion but only in large doses of atropine.
Decreased motility from stomach to the colon
Intestinal paralysis caused by anti-muscarinic drugs is temporary; peristalsis is usually restored after 1-3 days of anti-muscarinic therapy.
Anti-muscarinic drugs have a
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 5 of 29Section 2D – Batch 2014
Oxybutynin
for bladder spasm after urologic surgery and reducing urinary incontinence with neurologic diseases; this drug is selective for M3
receptors.
Propiverineis also used to reduce incontinence and has lesser CNS toxicity.
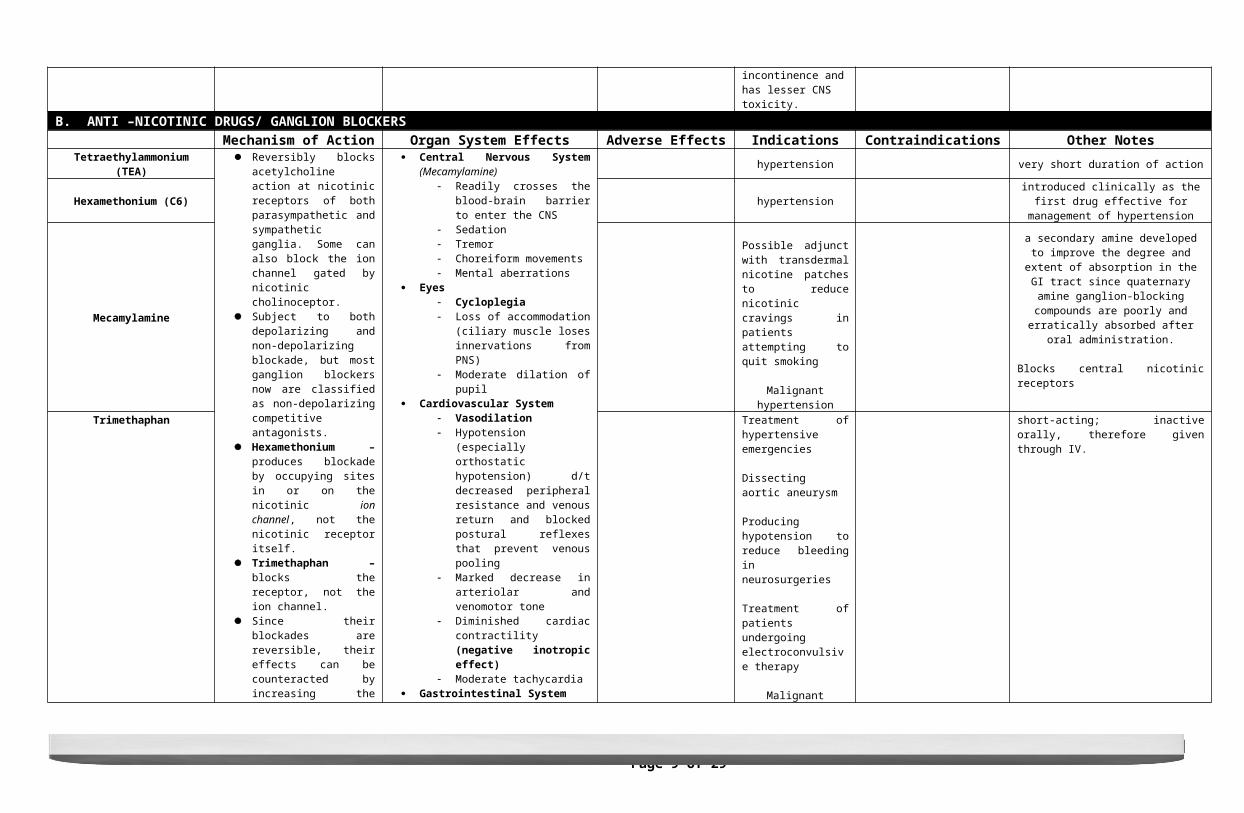
B. ANTI –NICOTINIC DRUGS/ GANGLION BLOCKERSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Tetraethylammonium (TEA)
Reversibly blocks acetylcholine action at nicotinic receptors of both parasympathetic and sympathetic ganglia. Some can also block the ion channel gated by nicotinic cholinoceptor.
Subject to both depolarizing and non-depolarizing blockade, but most ganglion blockers now are classified as non-depolarizing competitive antagonists.
Hexamethonium – produces blockade by occupying sites in or on the nicotinic ion channel, not the nicotinic receptor itself.
Trimethaphan – blocks the receptor, not the ion channel.
Since their blockades are reversible, their effects can be counteracted by increasing the concentration of acetylcholine or other agonists.
Central Nervous System (Mecamylamine) Readily crosses the blood-brain
barrier to enter the CNS Sedation Tremor Choreiform movements Mental aberrations
Eyes Cycloplegia Loss of accommodation (ciliary
muscle loses innervations from PNS)
Moderate dilation of pupil Cardiovascular System
Vasodilation Hypotension (especially orthostatic
hypotension) d/t decreased peripheral resistance and venous return and blocked postural reflexes that prevent venous pooling
Marked decrease in arteriolar and venomotor tone
Diminished cardiac contractility (negative inotropic effect)
Moderate tachycardia Gastrointestinal System
Reduced secretion, but not enough to effectively treat peptic ulcer disease
Profound inhibition of motility constipation
Genitourinary System Hesitancy in urination Urinary retention in men with BPH Erection and ejaculation may be
prevented by moderate doses Reduced thermoregulatory
sweating
hypertension very short duration of action
Hexamethonium (C6) hypertension introduced clinically as the first drug effective for management of hypertension
Mecamylamine
Possible adjunct with transdermal nicotine patches to reduce nicotinic cravings in patients attempting to quit smoking
Malignant hypertension
a secondary amine developed to improve the degree and extent of absorption in the GI tract
since quaternary amine ganglion-blocking compounds are poorly and erratically absorbed
after oral administration.
Blocks central nicotinic receptors
Trimethaphan
Treatment of hypertensive emergencies
Dissecting aortic aneurysm
Producing hypotension to reduce bleeding in neurosurgeries
Treatment of patients undergoing electroconvulsive therapy
Malignant hypertension
short-acting; inactive orally, therefore given through IV.
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 6 of 29Section 2D – Batch 2014
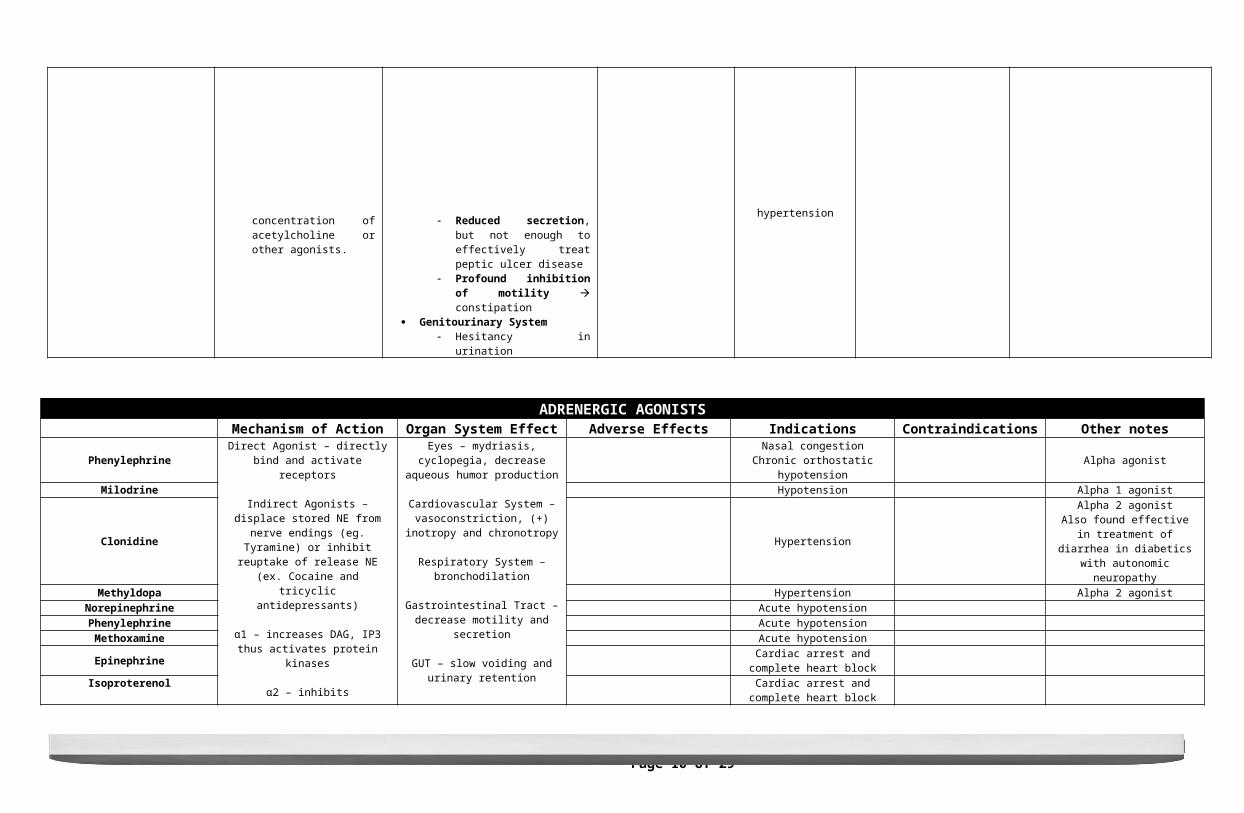
ADRENERGIC AGONISTSMechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
Phenylephrine
Direct Agonist – directly bind and activate receptors
Indirect Agonists – displace stored NE from nerve endings (eg. Tyramine) or
inhibit reuptake of release NE (ex. Cocaine and tricyclic antidepressants)
α1 – increases DAG, IP3 thus activates protein kinases
α2 – inhibits adenylcyclase thus decreases CAMP
β1,2,3 – stimulates adenylyl cyclase, increases ATP to CAMP conversion, increases Ca influx inside myocardial cells, promotes relaxation of smooth
muscle
D1 – stimulates adenylcyclase, vasodilation
D2 – inhibits adenylyl cyclase, opens K channels, decreases Cainfux
Eyes – mydriasis, cyclopegia, decrease aqueous humor production
Cardiovascular System – vasoconstriction, (+) inotropy and
chronotropy
Respiratory System – bronchodilation
Gastrointestinal Tract – decrease motility and secretion
GUT – slow voiding and urinary retention
Glands – decrease sweat, lacrimal, nasopharyngeal constriction
CNS - stimulant
Endocrine -
Beta - increase lipolysis, glycogenolysis, insulin
Alpha - inhibit or opposite alpha
Nasal congestionChronic orthostatic hypotension Alpha agonist
Milodrine Hypotension Alpha 1 agonist
Clonidine Hypertension
Alpha 2 agonistAlso found effective in treatment of diarrhea in diabetics with autonomic
neuropathyMethyldopa Hypertension Alpha 2 agonist
Norepinephrine Acute hypotensionPhenylephrine Acute hypotensionMethoxamine Acute hypotension
Epinephrine Cardiac arrest and complete heart block
Isoproterenol Cardiac arrest and complete heart block
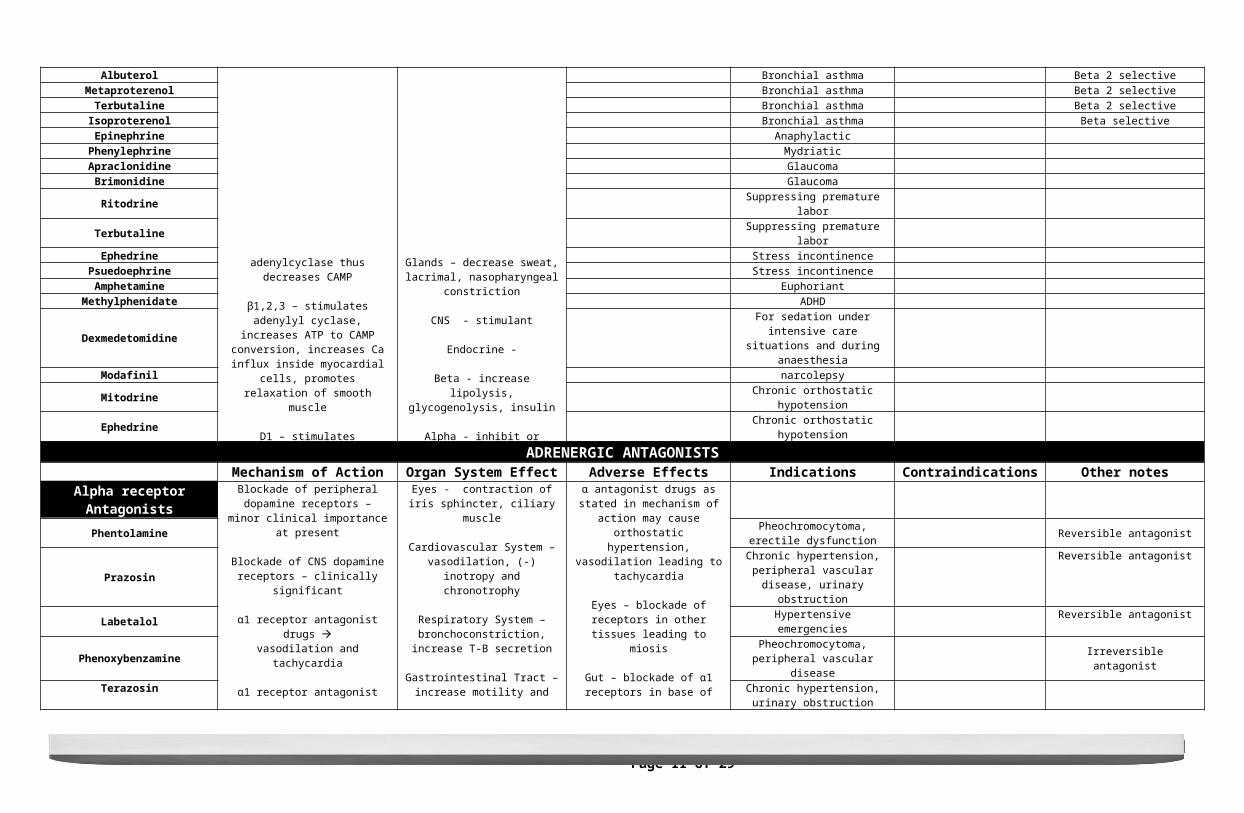
Albuterol Bronchial asthma Beta 2 selectiveMetaproterenol Bronchial asthma Beta 2 selective
Terbutaline Bronchial asthma Beta 2 selectiveIsoproterenol Bronchial asthma Beta selectiveEpinephrine Anaphylactic
Phenylephrine MydriaticApraclonidine GlaucomaBrimonidine Glaucoma
Ritodrine Suppressing premature laborTerbutaline Suppressing premature laborEphedrine Stress incontinence
Psuedoephrine Stress incontinenceAmphetamine Euphoriant
Methylphenidate ADHD
Dexmedetomidine For sedation under intensive care situations and during anaesthesia
Modafinil narcolepsyMitodrine Chronic orthostatic hypotensionEphedrine Chronic orthostatic hypotension
ADRENERGIC ANTAGONISTSMechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
Alpha receptor Antagonists Blockade of peripheral dopamine receptors – minor clinical importance at
present
Blockade of CNS dopamine receptors – clinically significant
α1 receptor antagonist drugs vasodilation and tachycardia
α1 receptor antagonist drugs acts on receptors on vascular smooth muscle decreased arteriolar and venous tone
Eyes - contraction of iris sphincter, ciliary muscle
Cardiovascular System – vasodilation, (-) inotropy and chronotrophy
Respiratory System – bronchoconstriction, increase T-B
secretion
Gastrointestinal Tract – increase motility and secretion
α antagonist drugs as stated in mechanism of action may cause
orthostatic hypertension, vasodilation leading to tachycardia
Eyes – blockade of receptors in other tissues leading to miosis
Gut – blockade of α1 receptors in base of bladder and prostate leading to resistance to urine flow and urinary
retention
Phentolamine Pheochromocytoma, erectile dysfunction Reversible antagonist
Prazosin Chronic hypertension, peripheral vascular disease, urinary obstruction
Reversible antagonist
Labetalol Hypertensive emergencies Reversible antagonist
Phenoxybenzamine Pheochromocytoma, peripheral vascular disease Irreversible antagonist
Terazosin Chronic hypertension, urinary obstruction
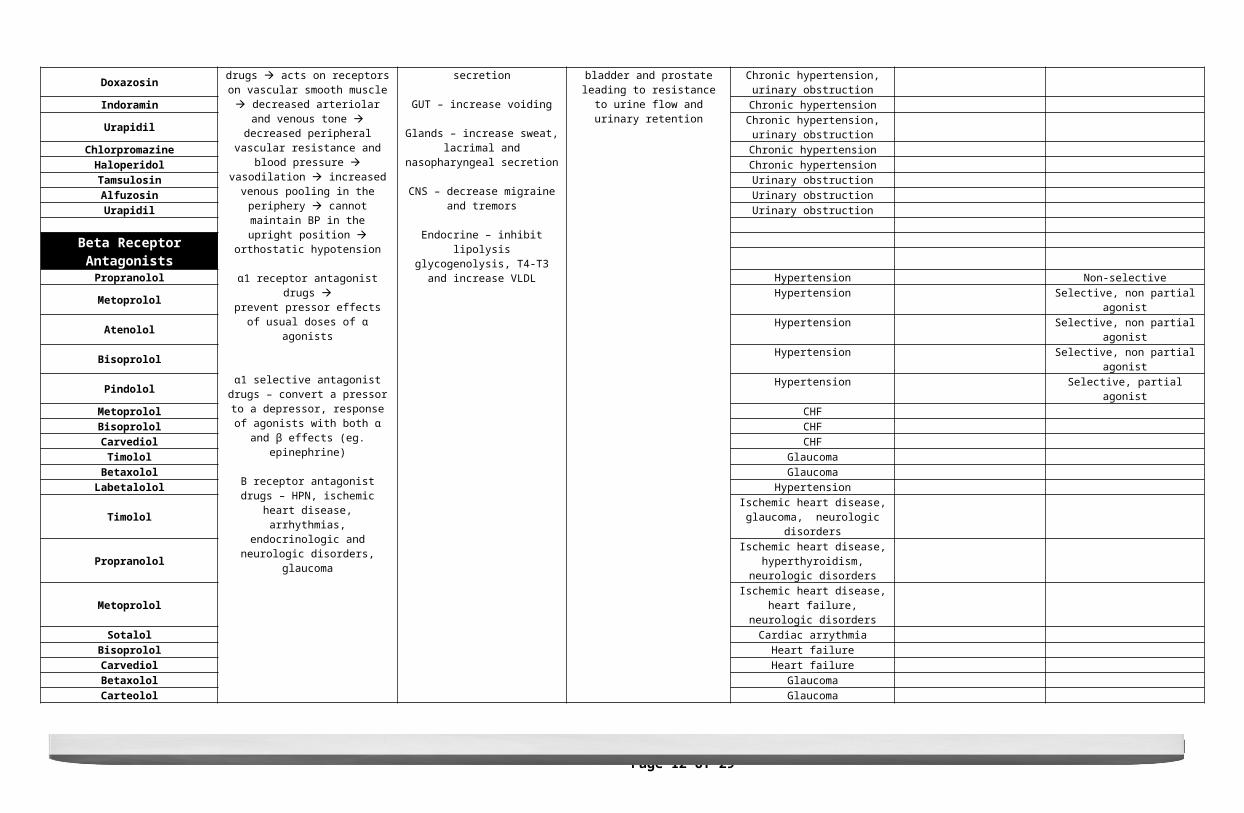
Doxazosin Chronic hypertension, urinary obstruction
Indoramin Chronic hypertension
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 7 of 29Section 2D – Batch 2014
decreased peripheral vascular resistance and blood pressure vasodilation
increased venous pooling in the periphery cannot maintain BP in the upright position orthostatic hypotension
α1 receptor antagonist drugs prevent pressor effects of usual doses of
α agonists
α1 selective antagonist drugs – convert a pressor to a depressor, response of
agonists with both α and β effects (eg. epinephrine)
B receptor antagonist drugs – HPN, ischemic heart disease, arrhythmias,
endocrinologic and neurologic disorders,
GUT – increase voiding
Glands – increase sweat, lacrimal and nasopharyngeal secretion
CNS – decrease migraine and tremors
Endocrine – inhibit lipolysis glycogenolysis, T4-T3 and increase
VLDL
Urapidil Chronic hypertension, urinary obstruction
Chlorpromazine Chronic hypertensionHaloperidol Chronic hypertensionTamsulosin Urinary obstructionAlfuzosin Urinary obstructionUrapidil Urinary obstruction
Beta Receptor AntagonistsPropranolol Hypertension Non-selectiveMetoprolol Hypertension Selective, non partial agonist
Atenolol Hypertension Selective, non partial agonistBisoprolol Hypertension Selective, non partial agonistPindolol Hypertension Selective, partial agonist
Metoprolol CHFBisoprolol CHFCarvediol CHFTimolol Glaucoma
Betaxolol GlaucomaLabetalolol Hypertension
Timolol Ischemic heart disease, glaucoma, neurologic disorders
Propranolol Ischemic heart disease, hyperthyroidism, neurologic disorders
Metoprolol Ischemic heart disease, heart failure, neurologic disorders
Sotalol Cardiac arrythmiaBisoprolol Heart failureCarvediol Heart failureBetaxolol GlaucomaCarteolol Glaucoma
Levobunolol GlaucomaMetipranolol Glaucoma
Atenolol Neurologic disordersNadol Neurologic disorders
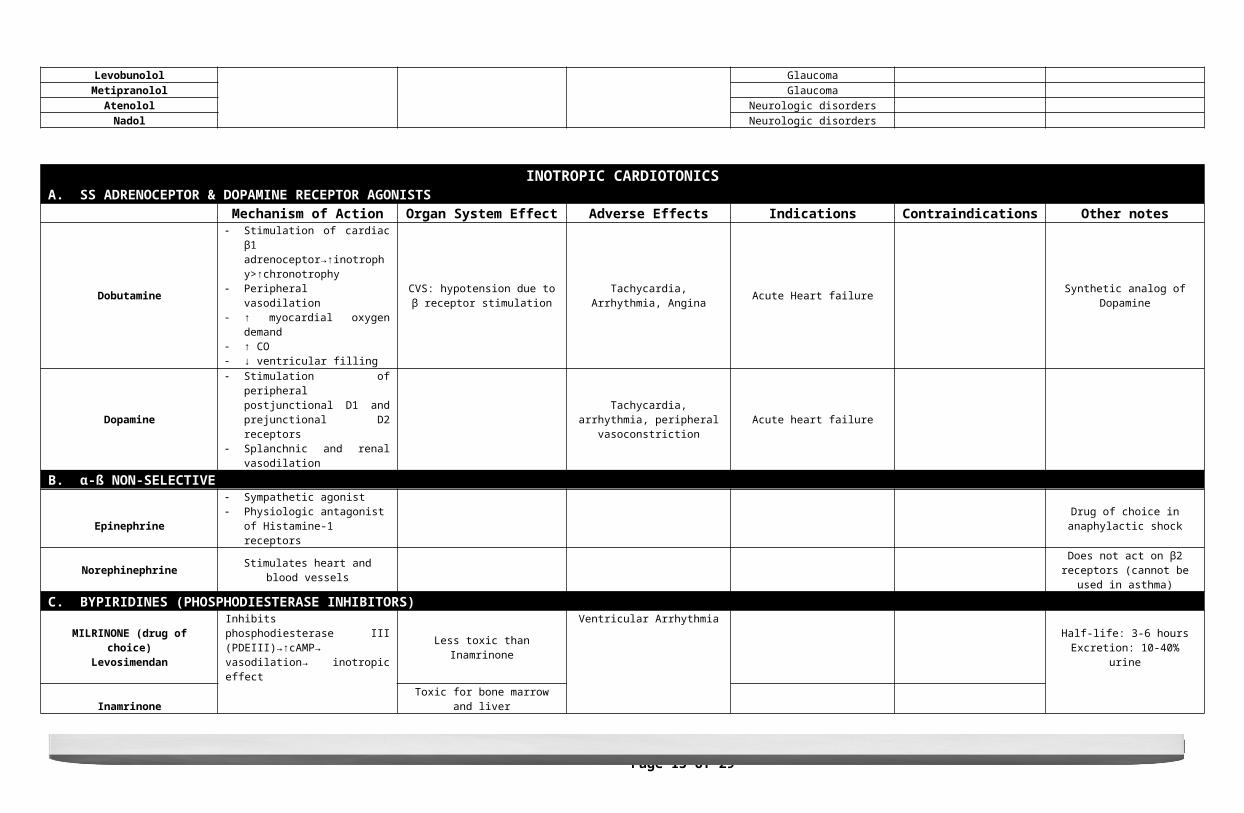
INOTROPIC CARDIOTONICSA. ADRENOCEPTOR & DOPAMINE RECEPTOR AGONISTSẞ
Mechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
Dobutamine
Stimulation of cardiac β1 adrenoceptor→↑inotrophy>↑chronotrophy
Peripheral vasodilation ↑ myocardial oxygen demand ↑ CO ↓ ventricular filling
CVS: hypotension due to β receptor stimulation Tachycardia, Arrhythmia, Angina Acute Heart failure Synthetic analog of Dopamine
Dopamine
Stimulation of peripheral postjunctional D1 and prejunctional D2 receptors
Splanchnic and renal vasodilation
Tachycardia, arrhythmia, peripheral vasoconstriction Acute heart failure
B. α-ß NON-SELECTIVE
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 8 of 29Section 2D – Batch 2014
Epinephrine
Sympathetic agonist Physiologic antagonist of Histamine-1
receptorsDrug of choice in anaphylactic shock
Norephinephrine Stimulates heart and blood vessels Does not act on β2 receptors (cannot be used in asthma)
C. BYPIRIDINES (PHOSPHODIESTERASE INHIBITORS)
MILRINONE (drug of choice)Levosimendan Inhibits phosphodiesterase III
(PDEIII)→↑cAMP→ vasodilation→ inotropic effect
Less toxic than Inamrinone
Ventricular Arrhythmia Half-life: 3-6 hoursExcretion: 10-40% urine
Inamrinone Toxic for bone marrow and liver
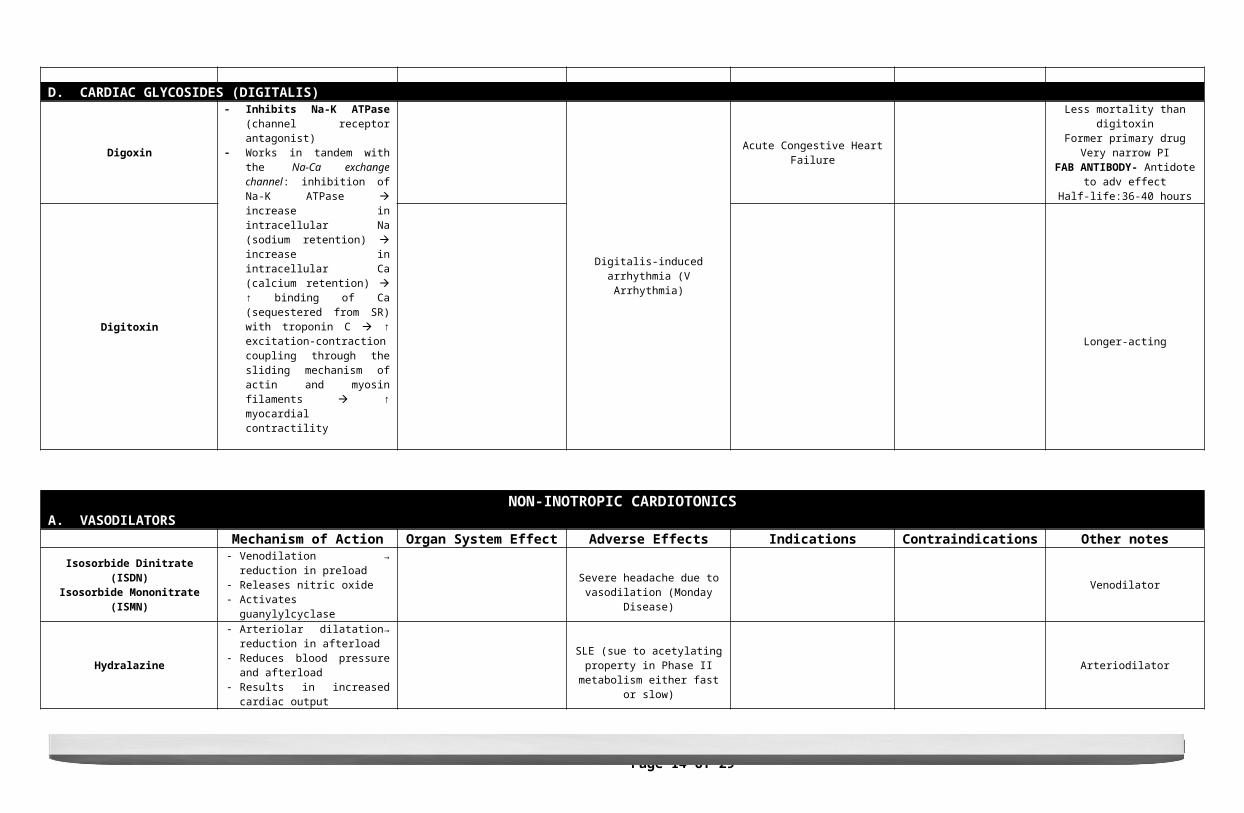
D. CARDIAC GLYCOSIDES (DIGITALIS)
Digoxin
Inhibits Na-K ATPase (channel receptor antagonist)
Works in tandem with the Na-Ca exchange channel: inhibition of Na-K ATPase increase in intracellular Na (sodium retention) increase in intracellular Ca (calcium retention) ↑ binding of Ca (sequestered from SR) with troponin C ↑ excitation-contraction coupling through the sliding mechanism of actin and myosin filaments ↑ myocardial contractility
Digitalis-induced arrhythmia (V Arrhythmia)
Acute Congestive Heart Failure
Less mortality than digitoxinFormer primary drug
Very narrow PIFAB ANTIBODY- Antidote to adv
effectHalf-life:36-40 hours
DigitoxinLonger-acting
NON-INOTROPIC CARDIOTONICSA. VASODILATORS
Mechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notesIsosorbide Dinitrate (ISDN)
Isosorbide Mononitrate (ISMN)
Venodilation → reduction in preload Releases nitric oxide Activates guanylylcyclase
Severe headache due to vasodilation (Monday Disease)
Venodilator
Hydralazine
Arteriolar dilatation→ reduction in afterload
Reduces blood pressure and afterload Results in increased cardiac output
SLE (sue to acetylating property in Phase II metabolism either fast or
slow)
Arteriodilator
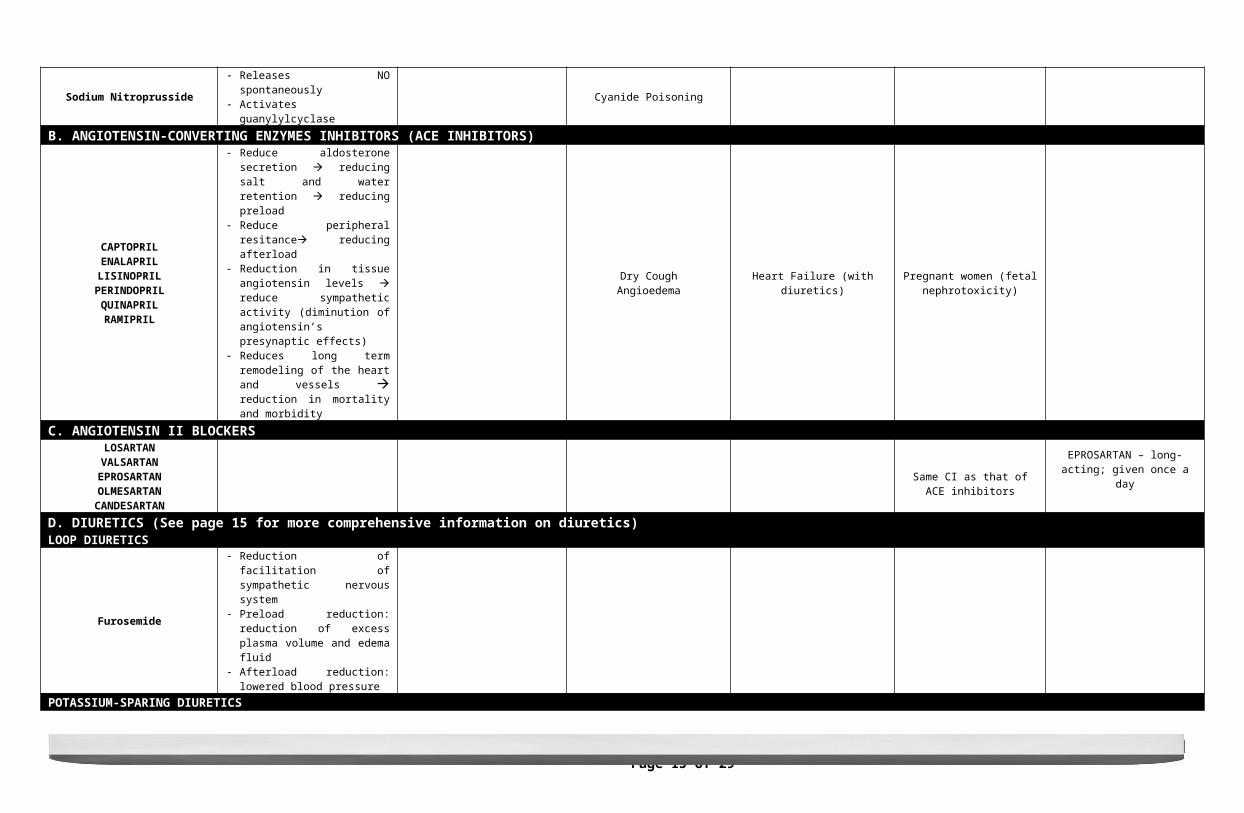
Sodium Nitroprusside Releases NO spontaneously Activates guanylylcyclase Cyanide Poisoning
B. ANGIOTENSIN-CONVERTING ENZYMES INHIBITORS (ACE INHIBITORS)CAPTOPRILENALAPRILLISINOPRIL
PERINDOPRILQUINAPRILRAMIPRIL
Reduce aldosterone secretion reducing salt and water retention reducing preload
Reduce peripheral resitance reducing afterload
Reduction in tissue angiotensin levels reduce sympathetic activity (diminution of angiotensin’s presynaptic effects)
Reduces long term remodeling of the
Dry CoughAngioedema
Heart Failure (with diuretics) Pregnant women (fetal nephrotoxicity)
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 9 of 29Section 2D – Batch 2014
heart and vessels reduction in mortality and morbidity
C. ANGIOTENSIN II BLOCKERSLOSARTAN
VALSARTANEPROSARTANOLMESARTAN
CANDESARTAN
Same CI as that of ACE inhibitors
EPROSARTAN – long-acting; given once a day
D. DIURETICS (See page 15 for more comprehensive information on diuretics)LOOP DIURETICS
Furosemide
Reduction of facilitation of sympathetic nervous system
Preload reduction: reduction of excess plasma volume and edema fluid
Afterload reduction: lowered blood pressure
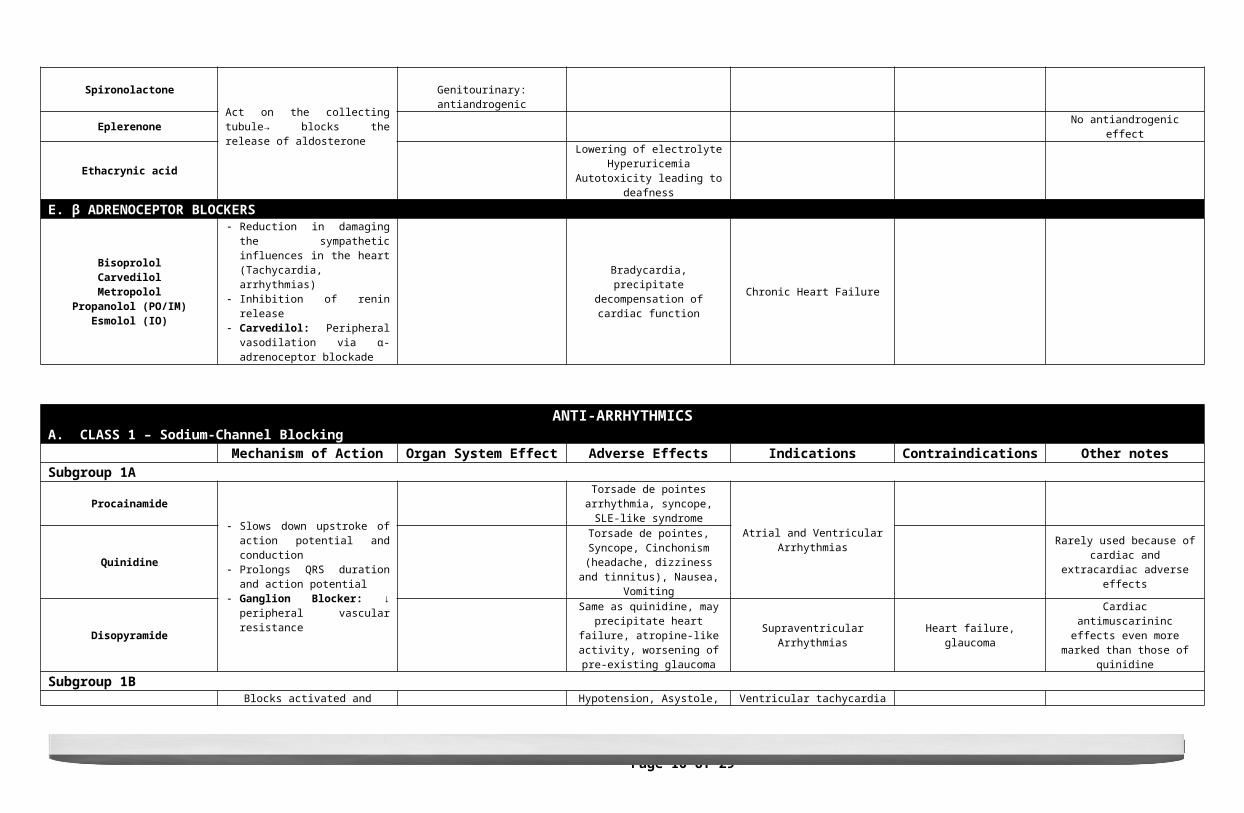
POTASSIUM-SPARING DIURETICS
SpironolactoneAct on the collecting tubule→ blocks the release of aldosterone
Genitourinary: antiandrogenicEplerenone No antiandrogenic effect
Ethacrynic acidLowering of electrolyte
HyperuricemiaAutotoxicity leading to deafness
E. β ADRENOCEPTOR BLOCKERSBisoprololCarvedilolMetropolol
Propanolol (PO/IM)Esmolol (IO)
Reduction in damaging the sympathetic influences in the heart (Tachycardia, arrhythmias)
Inhibition of renin release Carvedilol: Peripheral vasodilation via
α-adrenoceptor blockade
Bradycardia, precipitate decompensation of cardiac function Chronic Heart Failure
ANTI-ARRHYTHMICSA. CLASS 1 – Sodium-Channel Blocking
Mechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notesSubgroup 1A
Procainamide Slows down upstroke of action potential and conduction
Prolongs QRS duration and action potential
Ganglion Blocker: ↓ peripheral vascular resistance
Torsade de pointes arrhythmia, syncope, SLE-like syndrome
Atrial and Ventricular ArrhythmiasQuinidine
Torsade de pointes, Syncope, Cinchonism (headache, dizziness and
tinnitus), Nausea, Vomiting
Rarely used because of cardiac and extracardiac adverse effects
DisopyramideSame as quinidine, may precipitate heart failure, atropine-like activity,
worsening of pre-existing glaucomaSupraventricular Arrhythmias Heart failure, glaucoma Cardiac antimuscarininc effects even
more marked than those of quinidine
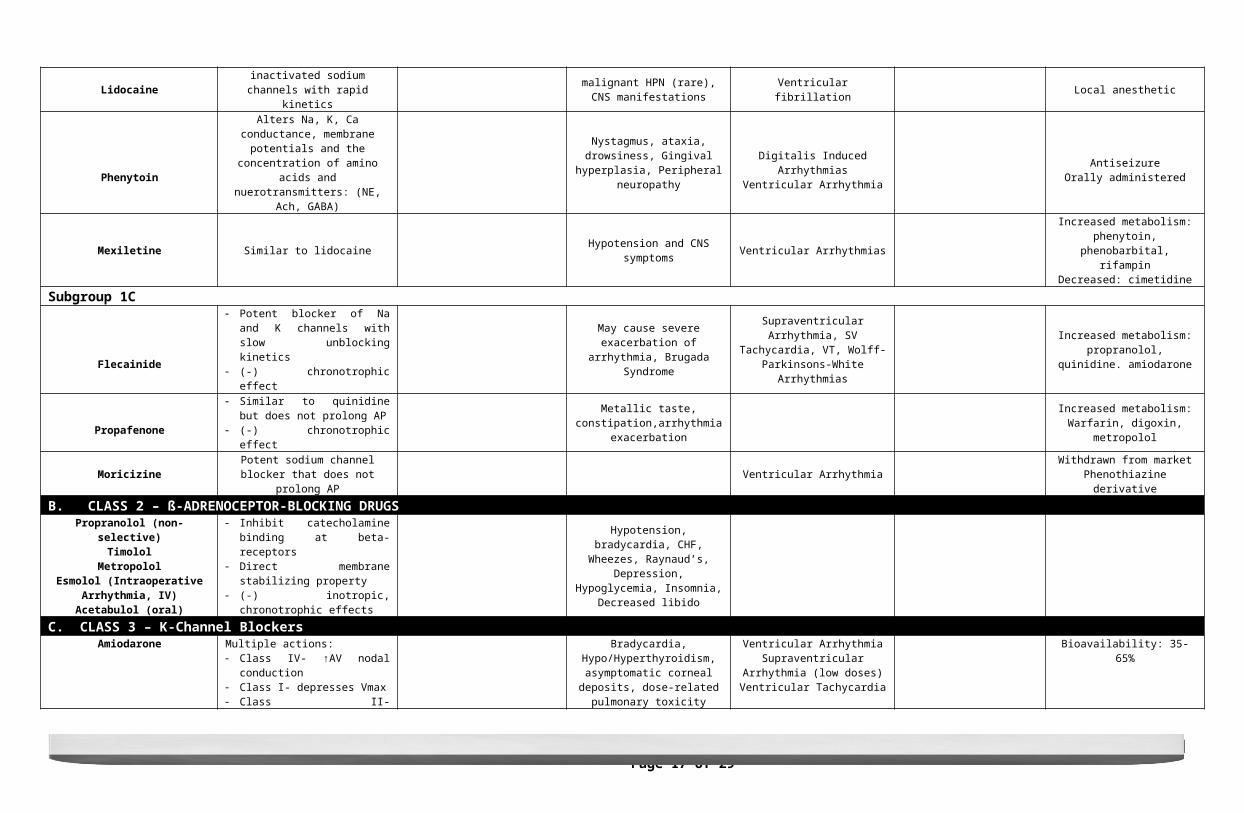
Subgroup 1B
LidocaineBlocks activated and inactivated sodium
channels with rapid kineticsHypotension, Asystole, malignant HPN (rare), CNS manifestations
Ventricular tachycardiaVentricular fibrillation Local anesthetic
Phenytoin
Alters Na, K, Ca conductance, membrane potentials and the concentration of amino
acids and nuerotransmitters: (NE, Ach, GABA)
Nystagmus, ataxia, drowsiness, Gingival hyperplasia, Peripheral
neuropathyDigitalis Induced Arrhythmias
Ventricular ArrhythmiaAntiseizure
Orally administered
Mexiletine Similar to lidocaine Hypotension and CNS symptoms Ventricular Arrhythmias Increased metabolism: phenytoin,
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 10 of 29Section 2D – Batch 2014
phenobarbital, rifampinDecreased: cimetidine
Subgroup 1C
Flecainide
Potent blocker of Na and K channels with slow unblocking kinetics
(-) chronotrophic effect
May cause severe exacerbation of arrhythmia, Brugada Syndrome
Supraventricular Arrhythmia, SV Tachycardia, VT, Wolff-Parkinsons-
White Arrhythmias
Increased metabolism: propranolol, quinidine. amiodarone
Propafenone
Similar to quinidine but does not prolong AP
(-) chronotrophic effect
Metallic taste, constipation,arrhythmia exacerbation
Increased metabolism: Warfarin, digoxin, metropolol
Moricizine Potent sodium channel blocker that does not prolong AP Ventricular Arrhythmia Withdrawn from market
Phenothiazine derivativeB. CLASS 2 – ß-ADRENOCEPTOR-BLOCKING DRUGS
Propranolol (non-selective)Timolol
MetropololEsmolol (Intraoperative Arrhythmia, IV)
Acetabulol (oral)
Inhibit catecholamine binding at beta-receptors
Direct membrane stabilizing property (-) inotropic, chronotrophic effects
Hypotension, bradycardia, CHF, Wheezes, Raynaud’s, Depression,
Hypoglycemia, Insomnia, Decreased libido
C. CLASS 3 – K-Channel Blockers
AmiodaroneMultiple actions: Class IV- ↑AV nodal conduction Class I- depresses Vmax Class II- noncompetitively blocks α
and β
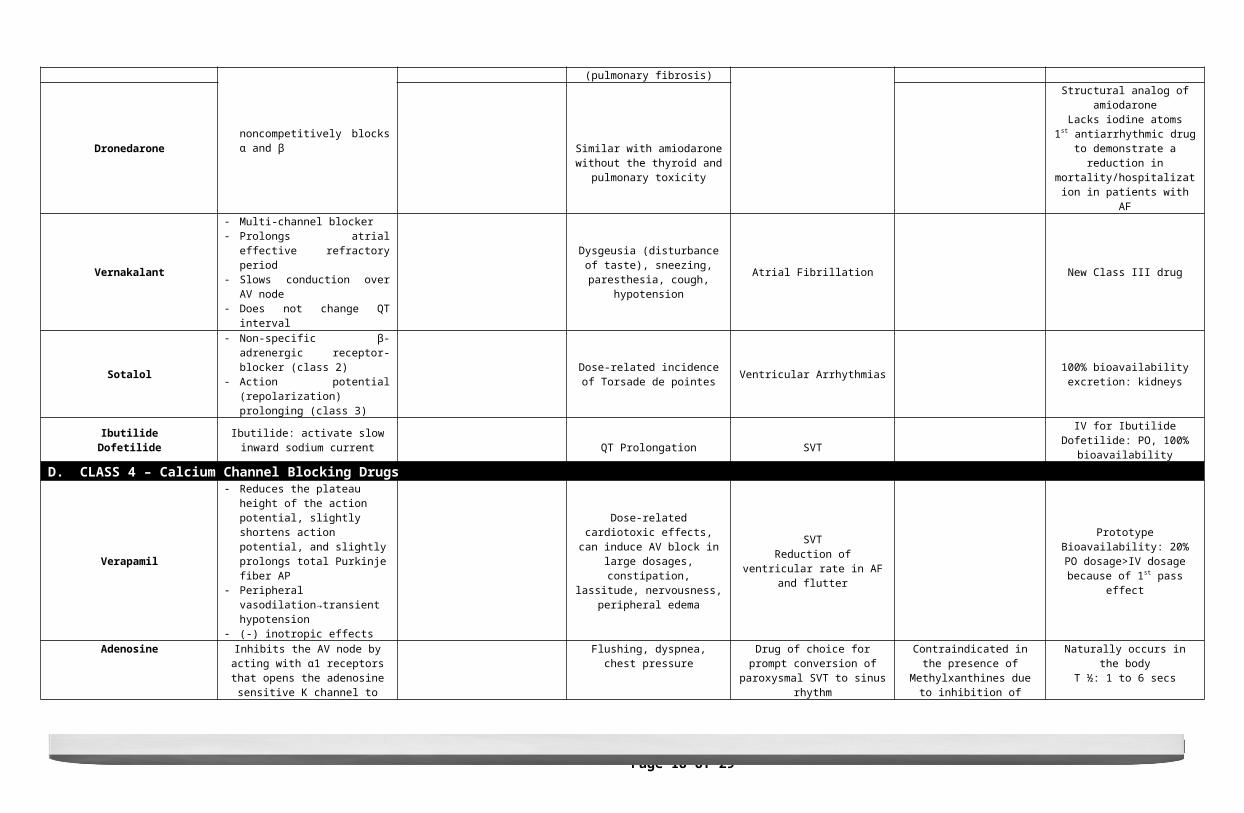
Bradycardia, Hypo/Hyperthyroidism, asymptomatic corneal deposits, dose-related pulmonary toxicity (pulmonary
fibrosis) Ventricular ArrhythmiaSupraventricular Arrhythmia (low
doses)Ventricular Tachycardia
Bioavailability: 35-65%
Dronedarone Similar with amiodarone without the thyroid and pulmonary toxicity
Structural analog of amiodaroneLacks iodine atoms
1st antiarrhythmic drug to demonstrate a reduction in
mortality/hospitalization in patients with AF
Vernakalant
Multi-channel blocker Prolongs atrial effective refractory
period Slows conduction over AV node Does not change QT interval
Dysgeusia (disturbance of taste), sneezing, paresthesia, cough,
hypotensionAtrial Fibrillation New Class III drug
Sotalol
Non-specific β-adrenergic receptor-blocker (class 2)
Action potential (repolarization) prolonging (class 3)
Dose-related incidence of Torsade de pointes Ventricular Arrhythmias 100% bioavailability
excretion: kidneys
IbutilideDofetilide
Ibutilide: activate slow inward sodium current QT Prolongation SVT
IV for IbutilideDofetilide: PO, 100% bioavailability
D. CLASS 4 – Calcium Channel Blocking Drugs
Verapamil
Reduces the plateau height of the action potential, slightly shortens action potential, and slightly prolongs total Purkinje fiber AP
Peripheral vasodilation→transient hypotension
(-) inotropic effects
Dose-related cardiotoxic effects, can induce AV block in large dosages,
constipation, lassitude, nervousness, peripheral edema
SVTReduction of ventricular rate in AF and
flutter
PrototypeBioavailability: 20%
PO dosage>IV dosage because of 1st pass effect
Adenosine
Inhibits the AV node by acting with α1 receptors that opens the adenosine
sensitive K channel to hyperpolarize and inhibit AV node and indirectly inhibit
calcium channel opening
Flushing, dyspnea, chest pressure Drug of choice for prompt conversion of paroxysmal SVT to sinus rhythm
Contraindicated in the presence of Methylxanthines due to inhibition of
action
Naturally occurs in the bodyT ½: 1 to 6 secs
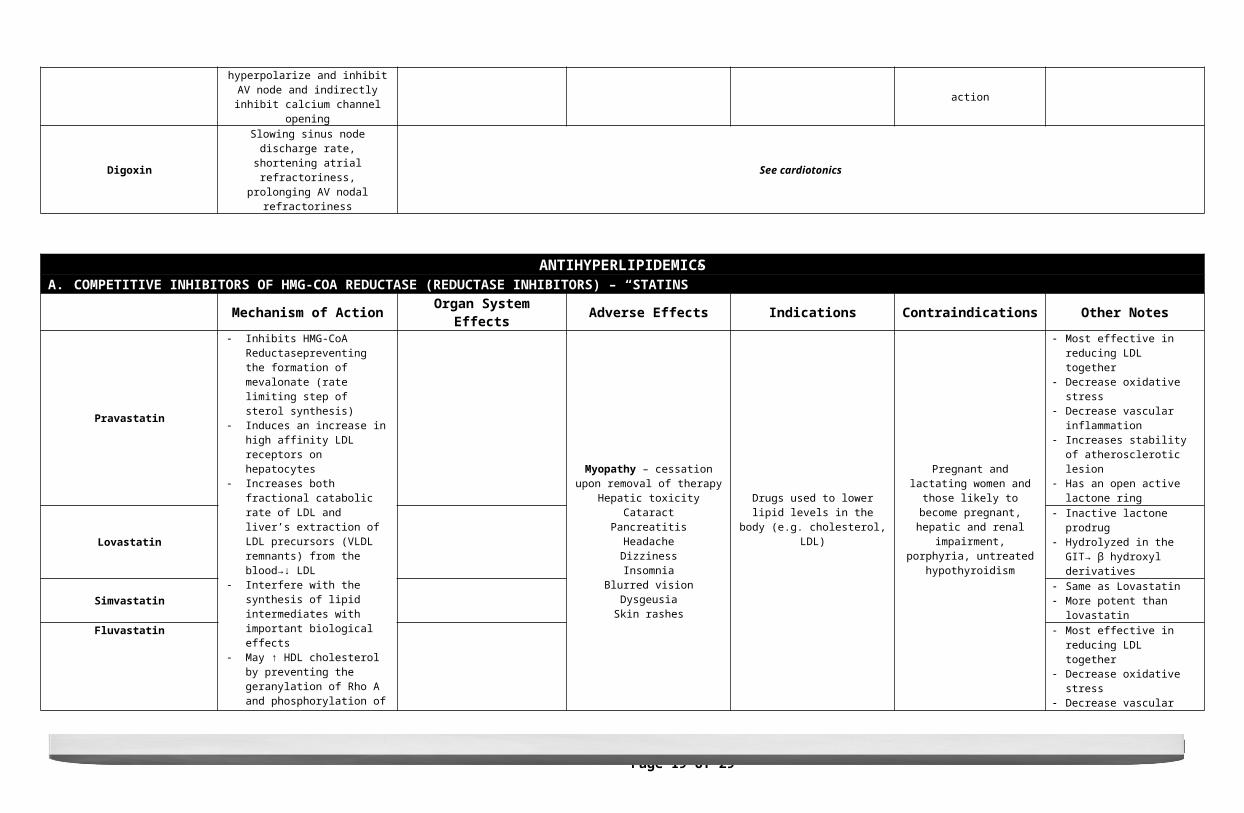
DigoxinSlowing sinus node discharge rate,
shortening atrial refractoriness, prolonging AV nodal refractoriness
See cardiotonics
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 11 of 29Section 2D – Batch 2014
ANTIHYPERLIPIDEMICSA. COMPETITIVE INHIBITORS OF HMG-COA REDUCTASE (REDUCTASE INHIBITORS) – “STATINS”
Mechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Pravastatin Inhibits HMG-CoA
Reductasepreventing the formation of mevalonate (rate limiting step of sterol synthesis)
Induces an increase in high affinity LDL receptors on hepatocytes
Increases both fractional catabolic rate of LDL and liver’s extraction of LDL precursors (VLDL remnants) from the blood→↓ LDL
Interfere with the synthesis of lipid intermediates with important biological effects
May ↑ HDL cholesterol by preventing the geranylation of Rho A and phosphorylation of peroxisome proliferator-activated receptor (PPARa)- factor that regulates APO A1 transcription
Myopathy – cessation upon removal of therapy
Hepatic toxicityCataract
PancreatitisHeadacheDizzinessInsomnia
Blurred visionDysgeusiaSkin rashes
Drugs used to lower lipid levels in the body (e.g. cholesterol, LDL)
Pregnant and lactating women and those likely to become pregnant,
hepatic and renal impairment, porphyria, untreated
hypothyroidism
Most effective in reducing LDL together
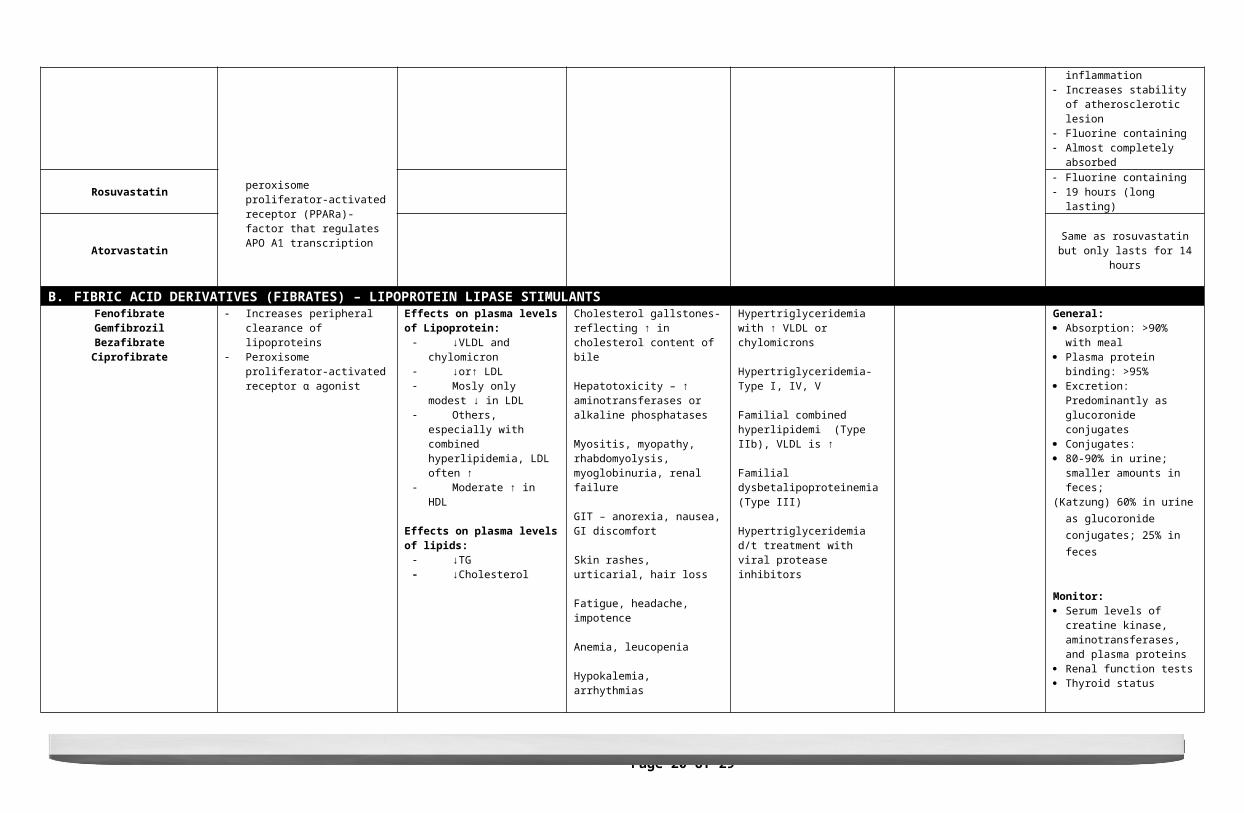
Decrease oxidative stress Decrease vascular inflammation Increases stability of
atherosclerotic lesion Has an open active lactone ring
Lovastatin Inactive lactone prodrug Hydrolyzed in the GIT→ β
hydroxyl derivatives
Simvastatin Same as Lovastatin More potent than lovastatin
Fluvastatin
Most effective in reducing LDL together
Decrease oxidative stress Decrease vascular inflammation Increases stability of
atherosclerotic lesion Fluorine containing Almost completely absorbed
Rosuvastatin Fluorine containing 19 hours (long lasting)
Atorvastatin Same as rosuvastatin but only lasts for 14 hours
B. FIBRIC ACID DERIVATIVES (FIBRATES) – LIPOPROTEIN LIPASE STIMULANTSFenofibrateGemfibrozilBezafibrateCiprofibrate
Increases peripheral clearance of lipoproteins
Peroxisome proliferator-activated receptor α agonist
Effects on plasma levels of Lipoprotein: ↓VLDL and chylomicron ↓or↑ LDL Mosly only modest ↓ in
LDL Others, especially with
combined hyperlipidemia, LDL often ↑
Moderate ↑ in HDL
Effects on plasma levels of lipids: ↓TG ↓Cholesterol
Cholesterol gallstones- reflecting ↑ in cholesterol content of bile
Hepatotoxicity – ↑ aminotransferases or alkaline phosphatases
Myositis, myopathy, rhabdomyolysis, myoglobinuria, renal failure
GIT – anorexia, nausea, GI discomfort
Skin rashes, urticarial, hair loss
Fatigue, headache, impotence
Anemia, leucopenia
Hypokalemia, arrhythmias
↓ WBC or Hct
Hypertriglyceridemia with ↑ VLDL or chylomicrons
Hypertriglyceridemia- Type I, IV, V
Familial combined hyperlipidemi (Type IIb), VLDL is ↑
Familial dysbetalipoproteinemia (Type III)
Hypertriglyceridemia d/t treatment with viral protease inhibitors
General: Absorption: >90% with meal Plasma protein binding: >95% Excretion: Predominantly as
glucoronide conjugates Conjugates: 80-90% in urine; smaller amounts
in feces;(Katzung) 60% in urine as
glucoronide conjugates; 25% in feces
Monitor: Serum levels of creatine kinase,
aminotransferases, and plasma proteins
Renal function tests Thyroid status
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 12 of 29Section 2D – Batch 2014
T ½: Fenofibrate- 20 hrsGemfibrozil- 1.5 hrsClofibrate- 15 hrs.
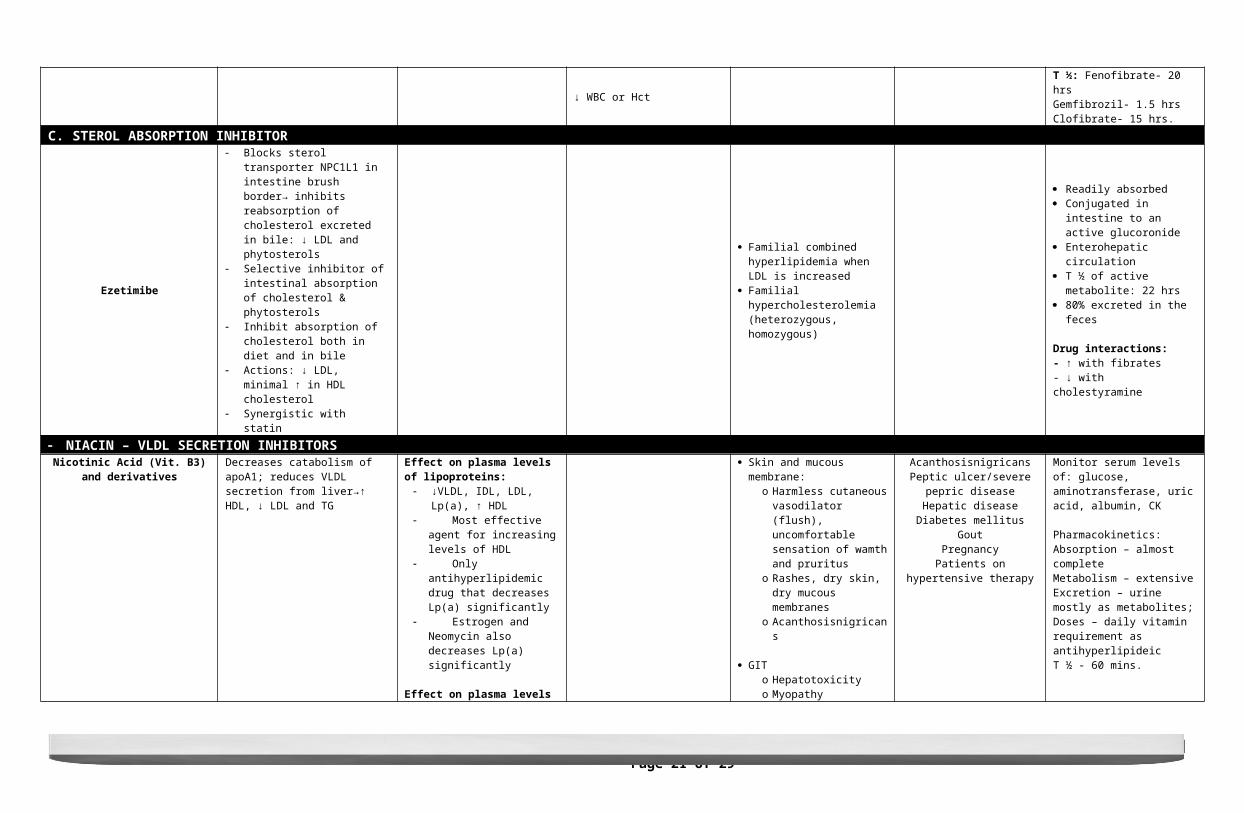
C. STEROL ABSORPTION INHIBITOR
Ezetimibe
Blocks sterol transporter NPC1L1 in intestine brush border→ inhibits reabsorption of cholesterol excreted in bile: ↓ LDL and phytosterols
Selective inhibitor of intestinal absorption of cholesterol & phytosterols
Inhibit absorption of cholesterol both in diet and in bile
Actions: ↓ LDL, minimal ↑ in HDL cholesterol
Synergistic with statin
Familial combined hyperlipidemia when LDL is increased
Familial hypercholesterolemia (heterozygous, homozygous)
Readily absorbed Conjugated in intestine to an
active glucoronide Enterohepatic circulation T ½ of active metabolite: 22 hrs 80% excreted in the feces
Drug interactions:- ↑ with fibrates- ↓ with cholestyramine
NIACIN – VLDL SECRETION INHIBITORS
Nicotinic Acid (Vit. B3) and derivativesDecreases catabolism of apoA1; reduces VLDL secretion from liver→↑ HDL, ↓ LDL and TG
Effect on plasma levels of lipoproteins: ↓VLDL, IDL, LDL, Lp(a), ↑ HDL Most effective agent for
increasing levels of HDL Only antihyperlipidemic
drug that decreases Lp(a) significantly
Estrogen and Neomycin also decreases Lp(a) significantly
Effect on plasma levels of lipids: ↓ TG ↓ Cholesterol
Other effects: ↓ Fibrinogen ↑ Tissue plasminogen activator
Skin and mucous membrane:o Harmless cutaneous
vasodilator (flush), uncomfortable sensation of wamth and pruritus
o Rashes, dry skin, dry mucous membranes
o Acanthosisnigricans
GITo Hepatotoxicityo Myopathyo Metabolic: Hyperglycemia,
Hyperuricemia
CVS: Arrhythmia, hypotension Ocular toxicity: Amblyopia
(reversible)- reduced vision in an eye not correctable by a manifest refraction; Maculopathy
AcanthosisnigricansPeptic ulcer/severe pepric disease
Hepatic diseaseDiabetes mellitus
GoutPregnancy
Patients on hypertensive therapy
Monitor serum levels of: glucose, aminotransferase, uric acid, albumin, CK
Pharmacokinetics:Absorption – almost completeMetabolism – extensiveExcretion – urine mostly as metabolites;Doses – daily vitamin requirement as antihyperlipideicT ½ - 60 mins.
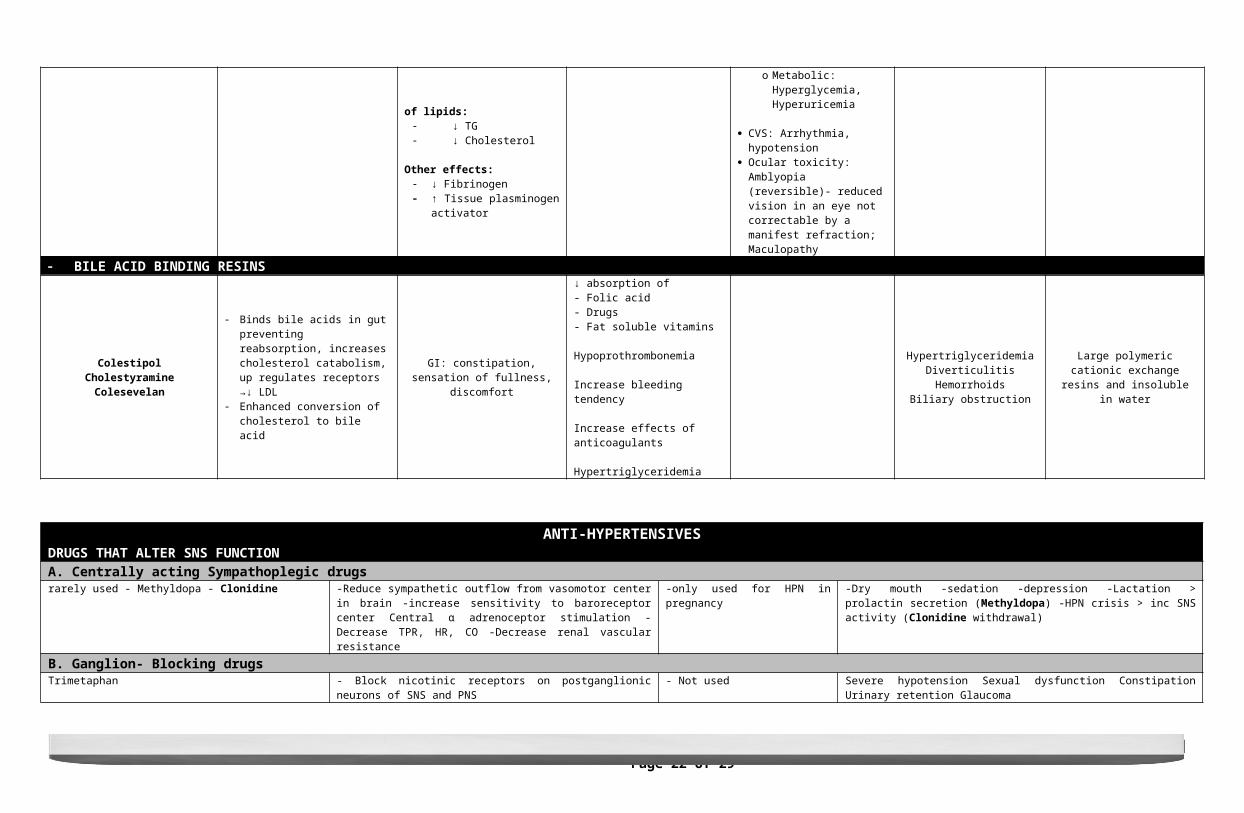
BILE ACID BINDING RESINS
ColestipolCholestyramine
Colesevelan
Binds bile acids in gut preventing reabsorption, increases cholesterol catabolism, up regulates receptors →↓ LDL
Enhanced conversion of cholesterol to bile acid
GI: constipation, sensation of fullness, discomfort
↓ absorption of- Folic acid- Drugs- Fat soluble vitamins
Hypoprothrombonemia
Increase bleeding tendency
Increase effects of anticoagulants
Hypertriglyceridemia
HypertriglyceridemiaDiverticulitisHemorrhoids
Biliary obstruction
Large polymeric cationic exchange resins and insoluble in water
ANTI-HYPERTENSIVES
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 13 of 29Section 2D – Batch 2014
DRUGS THAT ALTER SNS FUNCTION A. Centrally acting Sympathoplegic drugs rarely used - Methyldopa - Clonidine -Reduce sympathetic outflow from vasomotor center in brain -increase sensitivity
to baroreceptor center Central α adrenoceptor stimulation -Decrease TPR, HR, CO -Decrease renal vascular resistance
-only used for HPN in pregnancy -Dry mouth -sedation -depression -Lactation > prolactin secretion (Methyldopa) -HPN crisis > inc SNS activity (Clonidine withdrawal)
B. Ganglion- Blocking drugs Trimetaphan - Block nicotinic receptors on postganglionic neurons of SNS and PNS - Not used Severe hypotension Sexual dysfunction Constipation Urinary retention Glaucoma
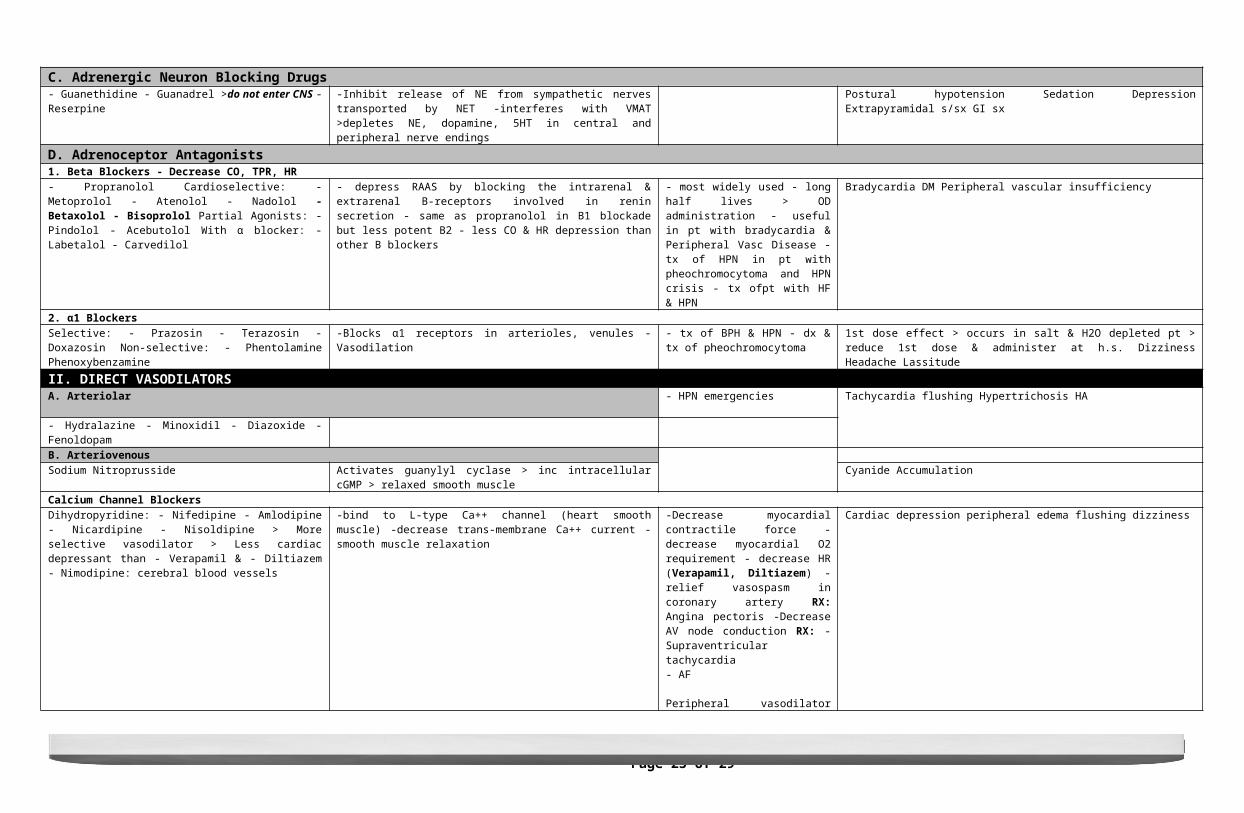
C. Adrenergic Neuron Blocking Drugs - Guanethidine - Guanadrel >do not enter CNS - Reserpine -Inhibit release of NE from sympathetic nerves transported by NET -interferes
with VMAT >depletes NE, dopamine, 5HT in central and peripheral nerve endings
Postural hypotension Sedation Depression Extrapyramidal s/sx GI sx
D. Adrenoceptor Antagonists 1. Beta Blockers - Decrease CO, TPR, HR - Propranolol Cardioselective: - Metoprolol - Atenolol - Nadolol - Betaxolol - Bisoprolol Partial Agonists: - Pindolol - Acebutolol With α blocker: - Labetalol - Carvedilol
- depress RAAS by blocking the intrarenal & extrarenal B-receptors involved in renin secretion - same as propranolol in B1 blockade but less potent B2 - less CO & HR depression than other B blockers
- most widely used - long half lives > OD administration - useful in pt with bradycardia & Peripheral Vasc Disease - tx of HPN in pt with pheochromocytoma and HPN crisis - tx ofpt with HF & HPN
Bradycardia DM Peripheral vascular insufficiency
2. α1 Blockers Selective: - Prazosin - Terazosin - Doxazosin Non-selective: - Phentolamine Phenoxybenzamine
-Blocks α1 receptors in arterioles, venules -Vasodilation - tx of BPH & HPN - dx & tx of pheochromocytoma
1st dose effect > occurs in salt & H2O depleted pt > reduce 1st dose & administer at h.s. Dizziness Headache Lassitude
II. DIRECT VASODILATORS A. Arteriolar - HPN emergencies Tachycardia flushing Hypertrichosis HA
- Hydralazine - Minoxidil - Diazoxide - Fenoldopam
B. Arteriovenous Sodium Nitroprusside Activates guanylyl cyclase > inc intracellular cGMP > relaxed smooth muscle Cyanide AccumulationCalcium Channel BlockersDihydropyridine: - Nifedipine - Amlodipine - Nicardipine - Nisoldipine > More selective vasodilator > Less cardiac depressant than - Verapamil & - Diltiazem - Nimodipine: cerebral blood vessels
-bind to L-type Ca++ channel (heart smooth muscle) -decrease trans-membrane Ca++ current -smooth muscle relaxation
-Decrease myocardial contractile force - decrease myocardial O2 requirement - decrease HR (Verapamil, Diltiazem) -relief vasospasm in coronary artery RX: Angina pectoris -Decrease AV node conduction RX: - Supraventricular tachycardia - AF
Peripheral vasodilator RX: - HPN - Raynaud’s phenomenon
Nicardipine RX: Severe HPN – thru IV
Cardiac depression peripheral edema flushing dizziness
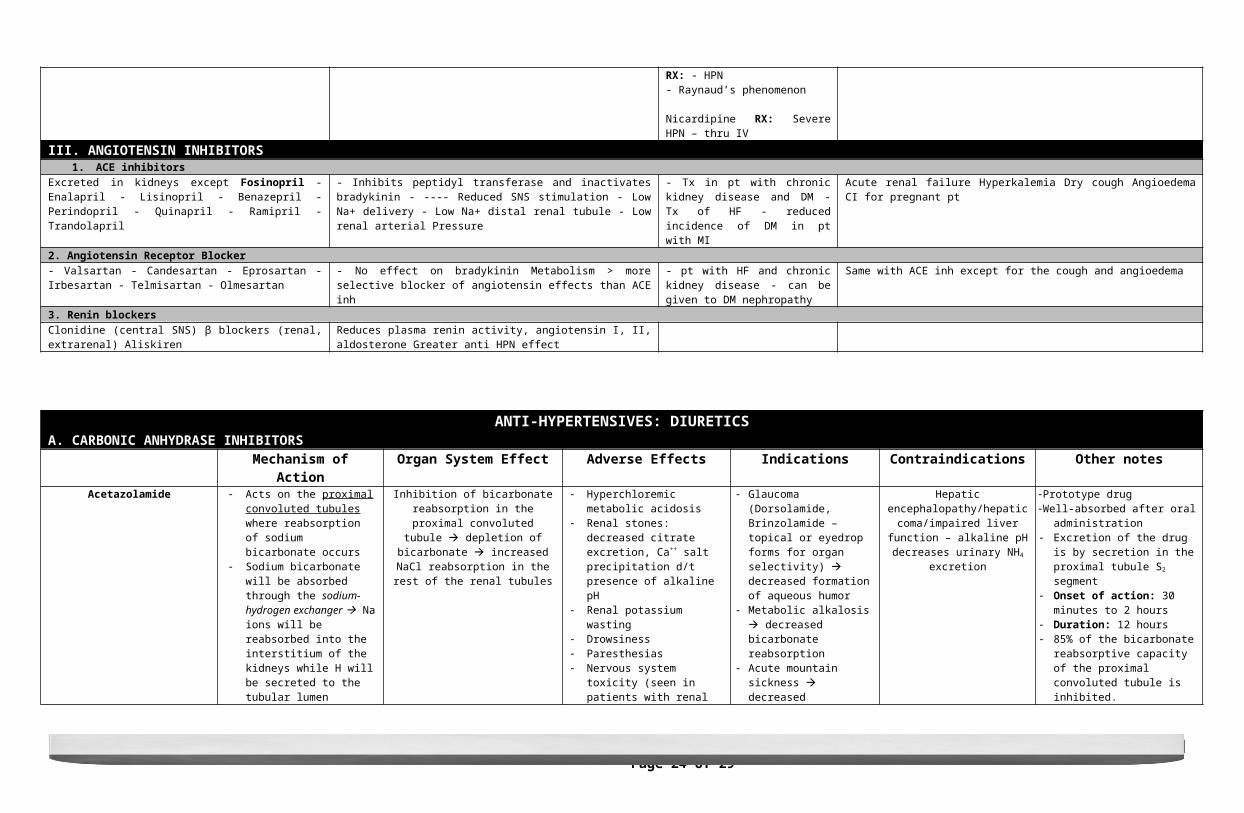
III. ANGIOTENSIN INHIBITORS 1. ACE inhibitors
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 14 of 29Section 2D – Batch 2014
Excreted in kidneys except Fosinopril - Enalapril - Lisinopril - Benazepril - Perindopril - Quinapril - Ramipril - Trandolapril
- Inhibits peptidyl transferase and inactivates bradykinin - ---- Reduced SNS stimulation - Low Na+ delivery - Low Na+ distal renal tubule - Low renal arterial Pressure
- Tx in pt with chronic kidney disease and DM - Tx of HF - reduced incidence of DM in pt with MI
Acute renal failure Hyperkalemia Dry cough Angioedema CI for pregnant pt
2. Angiotensin Receptor Blocker - Valsartan - Candesartan - Eprosartan - Irbesartan - Telmisartan - Olmesartan
- No effect on bradykinin Metabolism > more selective blocker of angiotensin effects than ACE inh
- pt with HF and chronic kidney disease - can be given to DM nephropathy
Same with ACE inh except for the cough and angioedema
3. Renin blockers Clonidine (central SNS) β blockers (renal, extrarenal) Aliskiren Reduces plasma renin activity, angiotensin I, II, aldosterone Greater anti HPN
effect
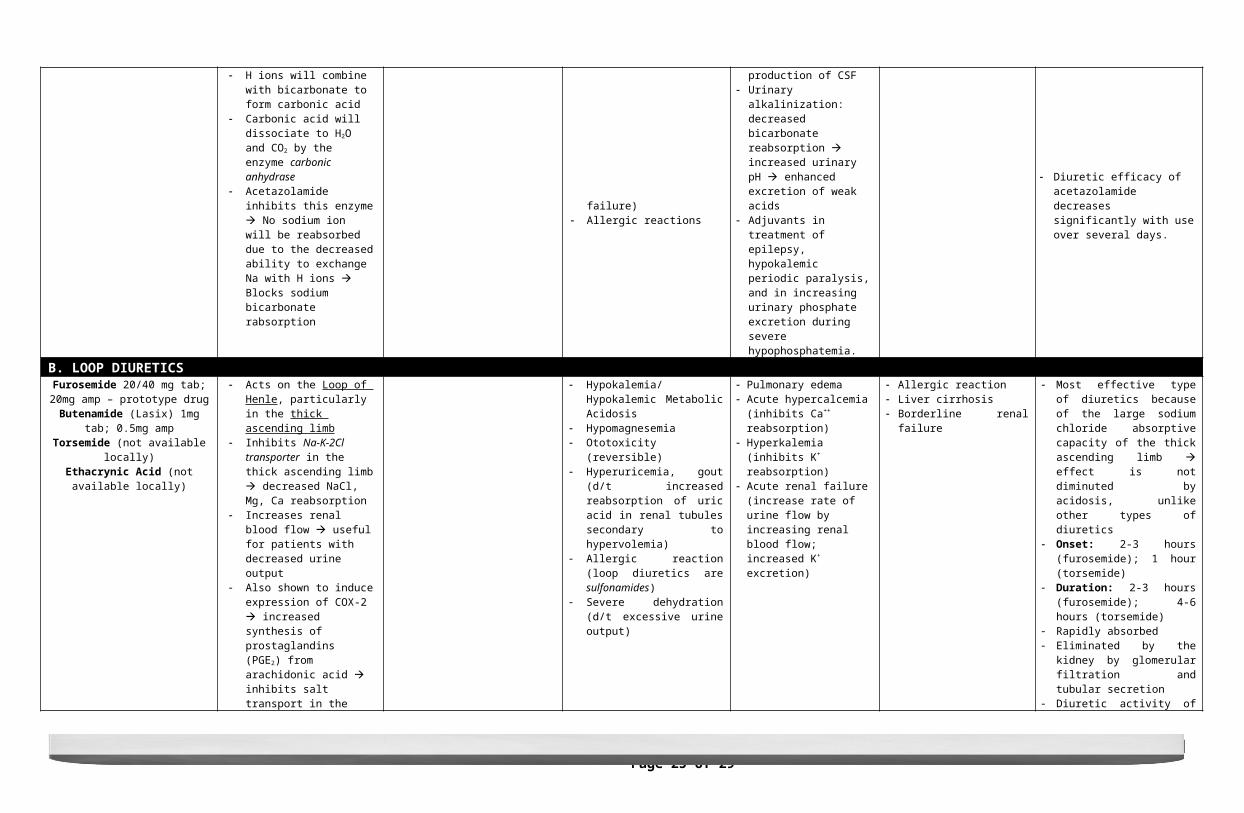
ANTI-HYPERTENSIVES: DIURETICSA. CARBONIC ANHYDRASE INHIBITORS
Mechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
Acetazolamide
Acts on the proximal convoluted tubules where reabsorption of sodium bicarbonate occurs
Sodium bicarbonate will be absorbed through the sodium-hydrogen exchanger Na ions will be reabsorbed into the interstitium of the kidneys while H will be secreted to the tubular lumen
H ions will combine with bicarbonate to form carbonic acid
Carbonic acid will dissociate to H2O and CO2 by the enzyme carbonic anhydrase
Acetazolamide inhibits this enzyme No sodium ion will be reabsorbed due to the decreased ability to exchange Na with H ions Blocks sodium bicarbonate rabsorption
Inhibition of bicarbonate reabsorption in the proximal convoluted tubule
depletion of bicarbonate increased NaCl reabsorption in the rest of the renal
tubules
Hyperchloremic metabolic acidosis Renal stones: decreased citrate
excretion, Ca++ salt precipitation d/t presence of alkaline pH
Renal potassium wasting Drowsiness Paresthesias Nervous system toxicity (seen in
patients with renal failure) Allergic reactions
Glaucoma (Dorsolamide, Brinzolamide – topical or eyedrop forms for organ selectivity) decreased formation of aqueous humor
Metabolic alkalosis decreased bicarbonate reabsorption
Acute mountain sickness decreased production of CSF
Urinary alkalinization: decreased bicarbonate reabsorption increased urinary pH enhanced excretion of weak acids
Adjuvants in treatment of epilepsy, hypokalemic periodic paralysis, and in increasing urinary phosphate excretion during severe hypophosphatemia.
Hepatic encephalopathy/hepatic coma/impaired liver function –
alkaline pH decreases urinary NH4
excretion
Prototype drugWell-absorbed after oral administration Excretion of the drug is by secretion
in the proximal tubule S2 segment Onset of action: 30 minutes to 2
hours Duration: 12 hours 85% of the bicarbonate reabsorptive
capacity of the proximal convoluted tubule is inhibited.
Diuretic efficacy of acetazolamide decreases significantly with use over several days.
B. LOOP DIURETICSFurosemide 20/40 mg tab; 20mg amp –
prototype drugButenamide (Lasix) 1mg tab; 0.5mg amp
Torsemide (not available locally)Ethacrynic Acid (not available locally)
Acts on the Loop of Henle, particularly in the thick ascending limb
Inhibits Na-K-2Cl transporter in the thick ascending limb decreased NaCl, Mg, Ca reabsorption
Increases renal blood flow useful for patients with decreased urine output
Also shown to induce expression of COX-2 increased synthesis of prostaglandins (PGE2) from arachidonic acid inhibits salt
Hypokalemia/Hypokalemic Metabolic Acidosis
Hypomagnesemia Ototoxicity (reversible) Hyperuricemia, gout (d/t increased
reabsorption of uric acid in renal tubules secondary to hypervolemia)
Allergic reaction (loop diuretics are sulfonamides)
Severe dehydration (d/t excessive urine output)
Pulmonary edema Acute hypercalcemia (inhibits
Ca++ reabsorption) Hyperkalemia (inhibits K+
reabsorption) Acute renal failure (increase rate
of urine flow by increasing renal blood flow; increased K+ excretion)
Allergic reaction Liver cirrhosis Borderline renal failure
Most effective type of diuretics because of the large sodium chloride absorptive capacity of the thick ascending limb effect is not diminuted by acidosis, unlike other types of diuretics
Onset: 2-3 hours (furosemide); 1 hour (torsemide)
Duration: 2-3 hours (furosemide); 4-6 hours (torsemide)
Rapidly absorbed Eliminated by the kidney by
glomerular filtration and tubular secretion
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 15 of 29Section 2D – Batch 2014
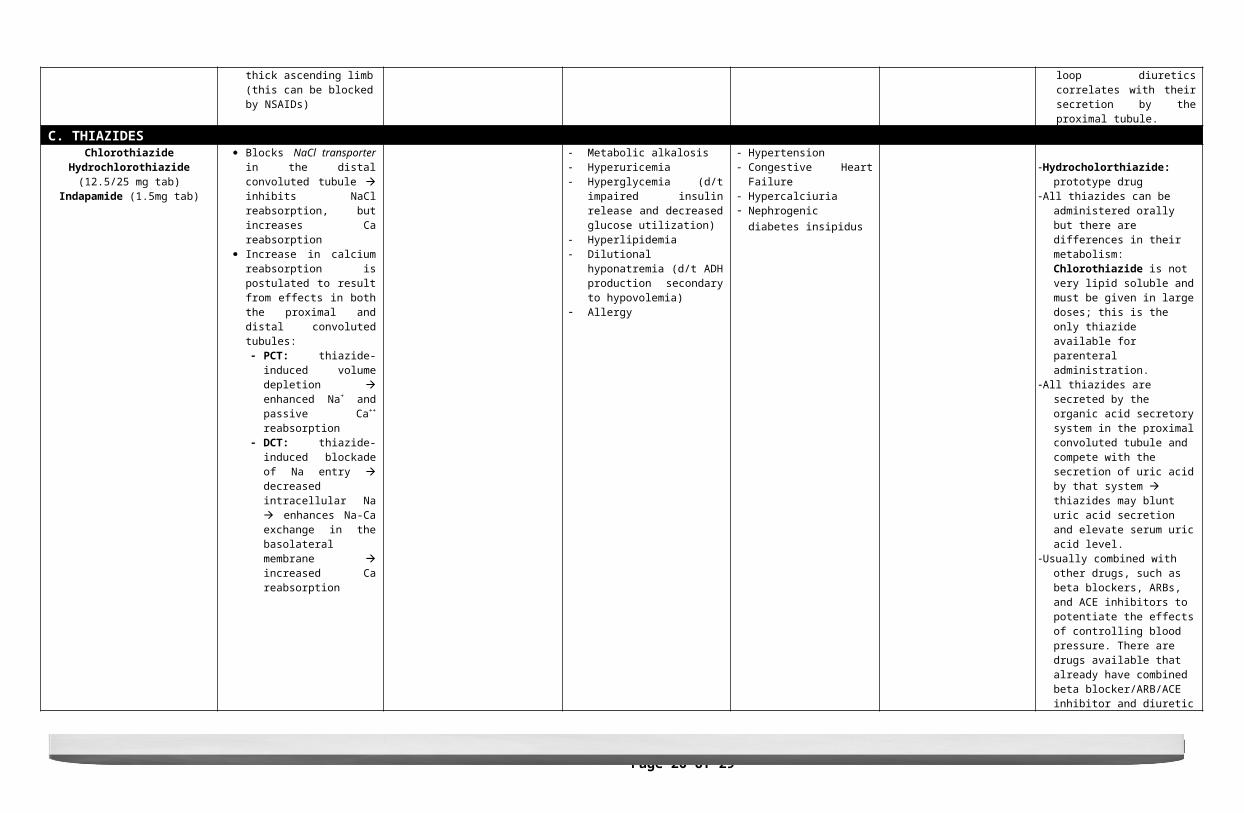
transport in the thick ascending limb (this can be blocked by NSAIDs)
Diuretic activity of loop diuretics correlates with their secretion by the proximal tubule.
C. THIAZIDES
ChlorothiazideHydrochlorothiazide (12.5/25 mg tab)
Indapamide (1.5mg tab)
Blocks NaCl transporter in the distal convoluted tubule inhibits NaCl reabsorption, but increases Ca reabsorption
Increase in calcium reabsorption is postulated to result from effects in both the proximal and distal convoluted tubules: PCT: thiazide-induced
volume depletion enhanced Na+ and passive Ca++ reabsorption
DCT: thiazide-induced blockade of Na entry decreased intracellular Na enhances Na-Ca exchange in the basolateral membrane increased Ca reabsorption
Metabolic alkalosis Hyperuricemia Hyperglycemia (d/t impaired
insulin release and decreased glucose utilization)
Hyperlipidemia Dilutional hyponatremia (d/t ADH
production secondary to hypovolemia)
Allergy
Hypertension Congestive Heart Failure Hypercalciuria Nephrogenic diabetes insipidus
Hydrocholorthiazide: prototype drugAll thiazides can be administered orally
but there are differences in their metabolism: Chlorothiazide is not very lipid soluble and must be given in large doses; this is the only thiazide available for parenteral administration.
All thiazides are secreted by the organic acid secretory system in the proximal convoluted tubule and compete with the secretion of uric acid by that system thiazides may blunt uric acid secretion and elevate serum uric acid level.
Usually combined with other drugs, such as beta blockers, ARBs, and ACE inhibitors to potentiate the effects of controlling blood pressure. There are drugs available that already have combined beta blocker/ARB/ACE inhibitor and diuretic effects.
However, if diuretics are to be given with calcium channel-blockers, they should be given separately.
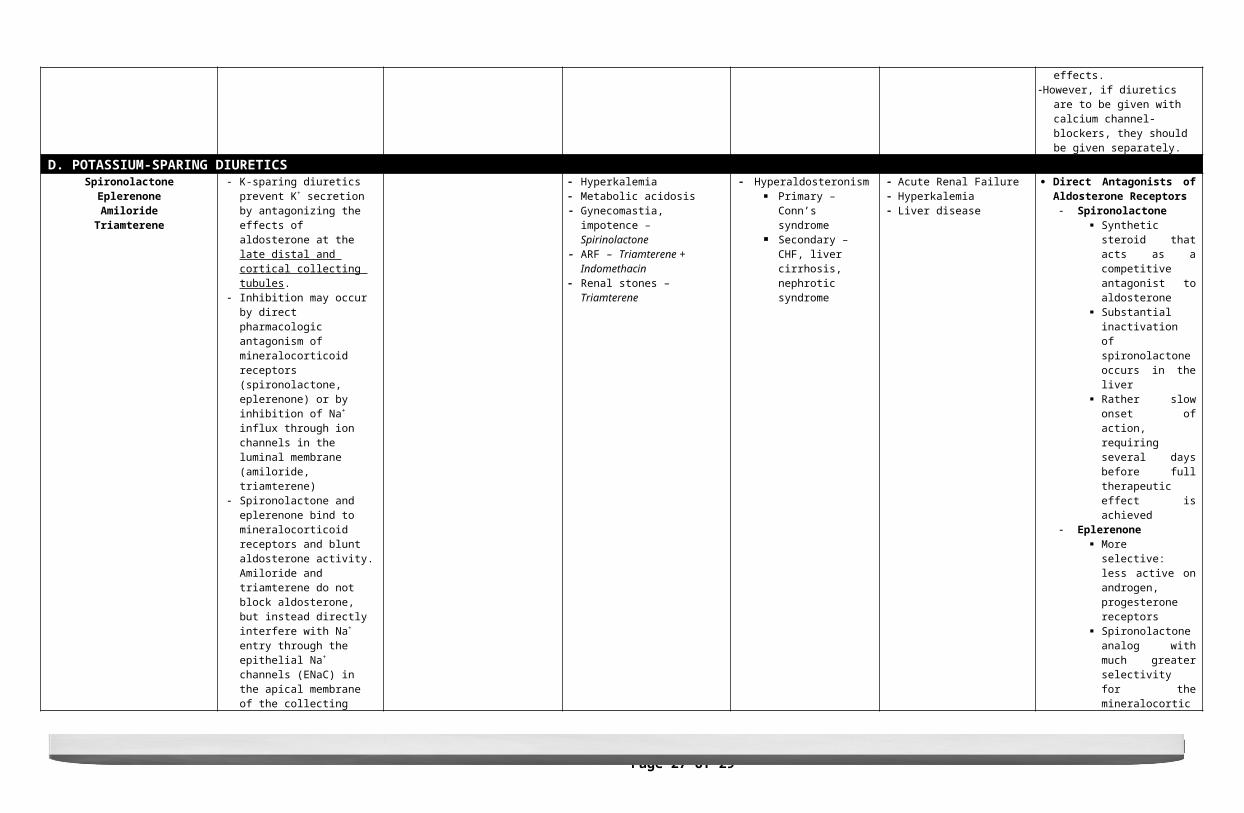
D. POTASSIUM-SPARING DIURETICSSpironolactone
EplerenoneAmiloride
Triamterene
K-sparing diuretics prevent K+ secretion by antagonizing the effects of aldosterone at the late distal and cortical collecting tubules.
Inhibition may occur by direct pharmacologic antagonism of mineralocorticoid receptors (spironolactone, eplerenone) or by inhibition of Na+ influx through ion channels in the luminal membrane (amiloride, triamterene)
Spironolactone and eplerenone bind to mineralocorticoid receptors and blunt aldosterone activity. Amiloride and triamterene do not block aldosterone, but instead directly interfere with Na+ entry through the epithelial Na+ channels (ENaC) in the apical membrane of the collecting tubule. Since K+ secretion is coupled with Na+ entry in this segment, these agents are also effective potassium-sparing
Hyperkalemia Metabolic acidosis Gynecomastia, impotence –
Spirinolactone ARF – Triamterene + Indomethacin Renal stones – Triamterene
Hyperaldosteronism Primary – Conn’s
syndrome Secondary – CHF, liver
cirrhosis, nephrotic syndrome
Acute Renal Failure Hyperkalemia Liver disease
Direct Antagonists of Aldosterone Receptors Spironolactone
Synthetic steroid that acts as a competitive antagonist to aldosterone
Substantial inactivation of spironolactone occurs in the liver
Rather slow onset of action, requiring several days before full therapeutic effect is achieved
Eplerenone More selective: less
active on androgen, progesterone receptors
Spironolactone analog with much greater selectivity for the mineralocorticoid receptor
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 16 of 29Section 2D – Batch 2014
diuretics
Several hundred-fold less active on androgen and progesterone receptors than spironolactone
Fewer adverse effects Inhibitors of Na+ influx through
ion channels in luminal membrane Amiloride Triamterene
Metabolized in the liver, but renal excretion is a major route of elimination for the active form and the metabolites
Because triamterene is extensively metabolized, it has a shorter half-life and must be given more frequently than amiloride (which is not metabolized)
Amiloride and triamterene are direct inhibitors of Na+ influx in the CCT (cortical collecting tubule).
E. OSMOTIC DIURETICS
Mannitol
Osmotic diuretics have their major effect in the proximal tubule and the descending limb of Henle's loop. Through osmotic effects, they also oppose the action of ADH in the collecting tubule.
Prevents the normal absorption of water by interposing a countervailing osmotic force resulting to increased urine volume.
Increase in urine flow rate decreases the contact time between fluid and the tubular epithelium, thus reducing Na+ as well as water reabsorption.
Decreases intracranial pressure Decreases intraocular pressure
Congestive heart failure Increased ECF volume Hyponatremia Dehydration
Mannitol – prototypic drug; the only osmotic diuretic available
Mannitol is poorly absorbed by the GI tract, and when administered orally it causes osmotic diarrhea. For systemic effect, mannitol must be given parenterally.
F. ADH AGONISTSVasopresin
Desmopresin
Renal action appears to be mediated primarily via V2 receptors although V1a
receptors may also be involved.Central Diabetes Insipidus
G. ADH RECEPTOR ANTAGONISTSConivaptan (only drug approved for use)
LixivaptanTolvaptan
ADH antagonists inhibit the effects of ADH in the collecting tubule
Both lithium and demeclocycline appear to reduce the formation of cyclic adenosine monophosphate
Nephrogenic Diabetes Insipidus Syndrome of Inappropriate Diuretic Hormone (SIADH)
Congestive Heart Failure
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 17 of 29Section 2D – Batch 2014
(cAMP) in response to ADH
ANTI-ANGINAA. NITRATES
Mechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
NitroglycerinIsosorbide Dinitrate (ISDN)
Isosorbide Mononitrate (ISMN)
Nitrates will be removed of its nitrate group by Gluthatione S-Transferase
which will release the free nitrate. The free nitrate will then be converted to nitric oxide. The nitric oxide causes activation of guanylylcyclase and an
increase in cGMP which, in turn, would cause smooth muscle relaxation as
stated in the previous mode of action.
dilation of veins – decreased preload (venous return)
dilation of arteries – decreased LV volume and wall tension (decrease afterload)
Hypotension because it is not only the coronary vessels that are dilated but also the other blood vessels (peripheral blood vessels)
Tachycardia Severe headache (due to
vasodilation of cerebral vessels)
Angina Increased intracranial pressure
Nitroglycerin considered as the
prototype of the group not sensitive to sunlight
but may lose its potency due to volatilization and adsorption to plastic surfaces, therefore it should be kept in a tightly closed glass containers
Isosorbide dinitrate/mononitrate sublingual administration
to prevent first pass effect in the liver
can also be given transdermally by placing a patch on any part of the chest or even in the abdomen; will be absorbed in the skin mucous membrane and will produce the therapeutic effect
Onset: 1-3 minutes Duration: 15-30 minutes Types of Administration: SL,
Transdermal, SR 1-3 minutes of administration would
provide immediate relief of the chest pain. If the chest pain is not relieved, wait for another 15 minutes then administer again (duration of action: 15-30 minutes). If the chest pain is not yet relieved by this, the patient must have a probable MI and should be admitted immediately to an ICU.
Slow Release tablets: used as maintenance given once a day
B. SILDENAFIL, TADANAFIL, VARDENAFILSildenafilTadanafilVardenafil
Sildenafil is a drug used for the treatment of impotence or erectile
dysfunction which blocks the action of phosphodiesterase. By blocking PDE,
there will be an increase in cGMP
Sexual impotenceErectile dysfunction
Patients taking nitrates
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 18 of 29Section 2D – Batch 2014
which will result to relaxation. This mode of action can also aggravate the
hypotensive effects of the nitrates.C. NEW DRUGS FOR ANGINA
Nicorandil
Activate cardiac potassium channels thereby hyperpolarizing the smooth muscle membrane therefore decreasing heart rate (myocardial protection)
Can also release nitric oxide in the endothelium thereby dilating the coronary vessels
Decreased HRDilation of coronary vessels
Better than the nitrates Available in 5, 10, 20 mg doses
and is given twice a day every 12 hours
A nicotinamide nitrate ester
TrimetazidineInhibit oxidation of fatty acids in the myocardium thereby improving the
metabolic status of ischemic tissues
20 mg (given 3x a day) 35 mg (every 12 hrs)
RanolizineBlocks the late Na current also blocking the calcium causing decrease myocardial contractility
Decreased myocardial contractility
IvabradineInhibits hyperpolarization by the activated Na channels in the SA node thereby decreasing heart rate
Decreased HROther effects similar to calcium channel
blockers
MUCOKINETICS (EXPECTORANTS)A. DIRECTLY-ACTING
Mechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
Guaiphenesin/Guaifenesin
Decrease sputum viscosity and increase sputum volume thereby
decreasing difficulty in expectorationNausea, gastric disturbances,
drowsiness and rashProductive cough Hypersensitivity
Na+, K+ citrate/acetate Increase bronchial secretion by salt
action ↑ Na content→↑ H2O content
Productive cough
B. REFLEXLY-ACTING
Ammonium chloride
Cause irritative action on bronchial mucosa resulting to production of excess respiratory tract fluid w/c is easier to cough
Nausea and vomitingProductive cough Irritant to gastric mucosa
Potassium Iodide Productive coughC. MUCOLYTIC
Bromhexine
Depolymerizes polysaccharide directly as well as by liberating lysosomal
enzymes w/c breaks down the fiber network in the tenacious sputum
Rhinorrhea, lacrimation, gastric irritation Productive cough
Hypersensitivity
Ambroxol
Makes the phlegm in the airway thinner and less sticky by increasing
the body’s natural production of surfactant (anti-glue)
Mild GI effects and allergic reactionProductive cough
Hypersensitivity, epileptic patients Metabolite of Bromhexine
Acetylcysteine Splits disulphide bonds linking proteins in the mucus thereby reducing mucus
viscosityProductive cough Hypersensitivity Also used in management of
paracetamol poisoning
Carbocisteine Liquefies viscid sputum Nausea, gastric discomfort, GI bleeding, skin rash Productive cough Hypersensitivity, Active peptic ulcer,
children under 2 years old
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 19 of 29Section 2D – Batch 2014
ANTITUSSIVESA. NARCOTIC ANTITUSSIVE
Mechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
Codeine Directly suppresses cough center by binding to distinct receptors in medulla
(TD)Sedations, nausea, constipationHigher dose: respiratory depression,
drowsinessDry cough Asthmatic px, px with diminished
respiratory reserves
Pholcodeine- has similar efficacy as codeine with longer duration
(12hrs) with no analgesic or addictive property
B. NON-NARCOTIC ANTITUSSIVESDextromethorpan Depress cough center in medulla and
increasing the threshold for coughStupor, ataxia, respiratory depression,
convulsion in children Spasmodic cough children below 6 yrs., px taking MOA inhibitors A synthetic compound
Noscapine Depress coughHeadache and Nausea Spasmodic cough *Asthmatic patients
Equally antitussive as codeineNo narcotic, analgesic or dependance properties
C. ANTI-HISTAMINICS
ChlorpheniramineDiphenhydramine
PromethazineSedative and anti-cholinergic action Urinary retention
Blurred vision
DrowsinessNauseaVomiting
ConstipationHeadache
Lack selectivity for cough centersNo efficacy in asthma
ANTI-ASTHMA(BRONCHODILATOR RELIEVERS AND CONTROLLERS)
A. ß2 AGONISTSMechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
TerbutalineAlbuterol
SalbutamolFenoterol Promotes bronchodilation
Activate G protein→↑ cAMP→↓ intracellular Ca
Throbbing headache, Tremors, tachycardia, palpitation Asthma
R isomer activate beta receptorS isomer causes inflammation
FormoterolSalmeterol
Long actingNo anti-inflammatory property
B. SYMPATHOMIMETICEpinephrine Bronchodilation CV: vasoconstriction Tachycardia, arryhtmia, worsening of
angina pectoris Status asthmaticus Onset- 15 mins.Duration- 60-90 mins.
C. MUSCARINIC ANTAGONISTSAtropine
Inhibit the effect of acetylcholine at muscarinic receptors
Treatment of asthma
Prototype drug
IpratropiumOnly have partial reversible property
for COPDInhibits M3 receptors
Tiotropium Dizziness, ↑ intraocular pressure, tachycardia
Approved as treatment for COPD
D. METHYLXANTHINES
Theophylline
Uncertain: phosphodiesterase inhibition, adenosine receptor
antagonist (Katzung)
Res: bronchodilationCV: cardiac stimulation
Musculoskeletal: increased skeletal muscle strength (diaphragm)
Anorexia, nausea, vomiting, abdominal discomfort, anxiety, headache, seizures, arrhythmias, insomnia Asthma, COPD Narrow therapeutic window
Aminophylline IV Competitive nonselective PDE inhibitor
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 20 of 29Section 2D – Batch 2014
Non selective adenosine receptor antagonist
Res: bronchodilation Bronchial asthma Less potent and shorter acting than theophylline
ANTI-ASTHMA(ANTI-INFLAMMATORY CONTROLLERS)
A. CORTICOSTEROIDSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
ORAL:
Prednisone , Methyprednisolone (dose depend on severity)INHALED: Budesonide, Fluticasone (Long Acting q 12 hrs)
Reduce airway reactivity Increase airway diameter Inhibit lymphocytic,
eosinophilic airway mucosal inflammation
Reduce frequency of asthma attacks
Potentiate effects of β2
agonists
Oropharyngeal candidiasis – inhaled give spacer devices
Hoarseness – advise to drink H20 or gurgle after inhaler
Adrenal insufficiency – best time 8am to mimic diurnal variation
Slow growth rate – children
Osteoperosis - cataract
effective in improving all indices of asthma control—severity of symptoms, tests of airway caliber and bronchial reactivity, frequency of exacerbations, and quality of life
Corticosteroid + LABA (Long Acting β2 Agonist) ( inhaled)
Budesonide + Formeterol Fluticasone + Salmeterol
(Seretide)
B. ANTI-LEUKOTRIENES
5 – lipoxygenase inhibitor ( not available ) ZileutonLTD4 – receptor Antagonist Montelukast, Zafirlukast (available in market)
liver toxicity
prevent Leukotriene synthesis Prevent LT action Bronchoconstriction, bronchial reactivity,
mucosal edema, mucus hypersecretion
C. MAST CELL STABILIZERS
INHALED:Na Cromoglycate
– inhibits degranulation of mast cell (inhibits histamine & serotonin)
Aspirin-induced asthma
Cromolyn, Nedocromil Inhibit antigen, exercise- induced asthma, slightly bronchial reactivityInhibit mast cell degranulation Produces an alteration in the function of delayed chloride channels in the cell membrane, inhibiting cell activation. This action on airway nerves is thought to be responsible for nedocromil's inhibition of cough; on mast cells, for inhibition of the early response to antigen challenge; and on eosinophils, for inhibition of the inflammatory
are minor and are localized to the sites of deposition.
throat irritation cough mouth dryness rarely, chest
tightness, and wheezing
can be prevented by inhaling a 2-adrenoceptor agonist before cromolyn or nedocromil
allergic rhinoconjunctivitisApplying the solution by nasal spray or eye drops several times a day is effective in about 75% of patient
Cromolyn - poorly absorbed from the gastrointestinal tract and must be inhaled as a microfine powder or aerosolized solution. Nedocromil also has a very low bioavailability and is available only in metered-dose aerosol form.
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 21 of 29Section 2D – Batch 2014
response to inhalation of allergens
treatment Serious adverse
effects are rare Reversible
dermatitis, myositis, or gastroenteritis
D. METHYLXANTHINES
Theophylline, theobromine, caffeine
Inhibit phosphodiesterase, increase CAMP ( relax smooth muscle, cardiac stimulation, bronchodilation) in some tissues including CGMPPDE4 appears to be the most directly involved in actions of methylxanthines on airway smooth muscle and on inflammatory cells. The inhibition of PDE4 in inflammatory cells reduces their release of cytokines and chemokines, which in turn results in a decrease in immune cell migration and activation Another proposed mechanism is inhibition of cell-surface receptors for adenosine. These receptors modulate adenylyl cyclase activity, and adenosine has been shown to provoke contraction of isolated airway smooth muscle and histamine release from airway mast cells. It has been shown, however, that xanthine derivatives devoid of adenosine antagonism (eg, enprofylline) may be potent in inhibiting bronchoconstriction in asthmatic subjects.-research suggests that the efficacy of theophyllines may be due to a third mechanism of action: enhancement of histone deacetylation. Acetylation of core histones is necessary for activation of inflammatory gene transcription. Corticosteroids act, at least in part, by recruiting histone deacetylases to the site of inflammatory gene transcription, an action enhanced by low-dose theophylline.
CNS: nervousness, tremors, arousalCVS: + chronotropy, inotropy GIT: stimulate acid, enzyme secretion ( give after meals)Kidneys: Increase GFR, Reduce tubular Na reabsorption ( weak diuretics)Respiratory: relax musclesSkeletal muscles: improve contraction of diaphragm
Pentoxyfylline – decrease blood viscosity ( for Reynaud or stroke due to thrombosis)Their major source is beverages (tea, cocoa, and coffee, respectively)The importance of theophylline as a therapeutic agent in the treatment of asthma has waned as the greater effectiveness of inhaled adrenoceptor agents for acute asthma and of inhaled anti-inflammatory agents for chronic asthma has been established, but theophylline's very low cost is an important advantage for economically disadvantaged patients in societies in which health care resources are limited.
E. ANTI – IgE MONOCLONAL ANTIBODIESOmalizumab inhibits binding of IgE to mast
cellsFor chronic severe asthma
decreases frequency & severity of asthma exacerbations
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 22 of 29Section 2D – Batch 2014
inadequate control by high dose inhaled steroid + LABA
with IgE mediated sensitivity
AUTACOIDSRole MOA Organ System Effects Antagonists
1. HISTAMINE Found in skin, GI
mucosa, lungs, liver, placenta, brain
Mediator of immediate allergic & inflammatory reactions
Gastric acid secretion
Binds with membrane receptors:H1*smooth muscle *endothelium
H2*gastric mucosa *cardiac muscle *brain *immune cells
H3*pre-synaptic brain *myenteric plexus
H4*eosinophils *neutrophils *CD4T cells
CNS*stimulate sensory nerve endings (pain, itch) CVS *vasodilatation* (+) inotropy * (-) chronotropy *fluid transudation
RS *bronchoconstriction (H1)
GIT*increased intestinal motility* increased gastric acid* increased pepsin *Intrinsic Factor secretion
I. Physiologic Antagonist EpinephrineII. Inhibitors of Histamine ReleaseCromolyn, Nedocromil, β2 agonists inhibits degranulation of mast cells III. Histamine Receptor AntagonistA. H1 Receptor Antagonists (1st Generation) for hypersensitivity reactions1. Sedation (1st generation, side effect) Highly sedative
Diphenhydramineq6-8Dimhenhydrinateq8Promethazine (parenteral)Hydroxyzine (itarax) LA
Moderately SedativeBuclizine (appetite stimulant)Cinnarizine (vertigo/motion sickness)Meclizine PheniramineCyproheptadine
Mild SedativeChlorpheniramineClemastine LADimethidineMethdilazine NAMepyramine NATriprolidine NACyclizine NA
2.Anti-emetic, anti-nausea (Meniere’s syndrome) Rx: Scopolamine (not available)Promethazine (IM) DimenhydrinateCyclizine Meclizine (Bonamine)BetahistineCenarizine
3.Anti-Parkinsonism suppress extra-pyramidal symptoms
Rx: Diphenhydramine
4.Anti-cholinergic urinary retention, blurred vision (side effects)
High anti-cholinergic actionPromethazineDiphenhydramine (Benadryl)DimenhydrinatePheniramineCyproheptadine
Low anti-cholinergic actionChlorpheniramineHydroxyzine
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 23 of 29Section 2D – Batch 2014
CyclizineMeclizine
Minimal/ absent anti-cholinergic actionClemastineTerfenadine (arrhythmia effect)AstemizoleLoratidine (Alerta)EbastineCetirizine
5.Adrenoceptor-blocking (α) orthostatic hypotension
Rx: Promethazine (should be in supine postion)
6. Serotonin blocking Cyproheptadine (appetite stimulant)
7.Allergy Urticaria, Allergic rhinitisSide Effects/ToxicitySedation, decreased alertness & concentration, motor incoordination, light-headedness, dryness of mouth, urinary hesitancy, blurring of visionCyclizine, Meclizine teratogenicB. H1 Blockers (2nd generation) Higher H1 selectivity No anti-cholinergic side effects no CNS depressant property (Do not potentiate
alcohol, benzodiazepine) Inhibit late phase allergic reaction by acting on
LT, anti-platelet activating effect Poor anti-pruritic, anti-emetic, anti-tussive
properties Used for: Allergic rhinitis, conjunctivitis, hay
fever, urticaria, atopic eczema, acute allergic reactions
LoratadineDesloratadine Cetirizine inhibits H release & cytotoxic mediators from platelets & eosinophil chemotaxis AzelastineEbastine Terfenadine blocks cardiac K+ channels (overdose); Torsades de pointes Fexofenadine no arrhthymogenic potential
C. H1 Blockers (3rd generation)Levocetirizine
D. H2 Blockers Anti-ulcer Cimetidine Cytochrome P450 inhibitor, anti-androgen effects
RanitidineFamotidineNizatidine
SEROTONIN Major source in
intestines (90%) Platelets Brainstem (mood,
sleep, appetite, pain perception, temperature & BP regulation, vomiting)
Synthesized from tryptophan
Degraded by MAO 5HT1,2,3,4,5,6,7
receptors
CNS*Vomiting*Pain*Itch*Bezold-Jarisch reflex (5HT3) *chemoreceptor reflex – marked outflow of vagal stimulation to the heart bradycardia
CVS *vasoconstriction (5HT2) except skeletal muscle, heart *platelet aggregation
RS *bronchoconstriction (5HT2)
GIT *increases motility thru ACh (5HT4)
I. Serotonin (5-HT) AgonistsA. 5HT1A ReceptorBuspirone (anxiolytic)B. 5HT1D ReceptorAmlotriptan NASumatriptan Zolmitriptan (constrict cerebral vessel)(migraine headache)C. 5HT4-Cisapride(toxic)Tegaserod (partial agonist) irritable bowel syndromeII. Serotonin (5-HT) Antagonists1. 5HT1-5HT2 Methysergide
2. 5HT2 Ketanserin blocks platelet aggregation for stroke Ritanserindecreases thromboxane formation for stroke
3. 5HT2, H1 Cyproheptadin for cold-induced urticaria for carcinoid syndrome4. 5HT3 Ondansetron chemotherapy-induced nausea & vomitingTherapeutic Uses
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 24 of 29Section 2D – Batch 2014
Skeletal muscles *serotonin syndrome (5HT2) – *hyperthermia
1. controls S/S carcinoid, post-gastrectomy dumping syndrome Cyproheptadine sedative, stimulates appetite, good anti-pruritic
2. Raynaud’s disease Ketanserin blocks platelet aggregation for stroke Ritanserindecreases thromboxane formation for stroke
3. Anti-emetic (anti-cancer, radiotherapy) Ondansetron
4. Migraine prophylaxis, Carcinoid,post-gastrectomy dumping syndrome
Methysergide
5. Migraine (better tolerated) SumatriptanZolmitriptan
6. Schizophrenia RisperidineClozapine
ERGOT ALKALOIDSMechanism of Action Organ System Effect Adverse Effects Indications Contraindications Other notes
Amine Alkaloids Ergometrine Ergonomine
Amino Acid/Peptide Alkaloids Ergotamine Regotoxine
Semi-Synthetic Alkaloids Ergometrine Ergonomine
agonist, partial agonist, antagonist at α receptors, serotonin receptors, CNS
dopamine receptors
CNS – powerful hallucinogen (Lysergic Acid Diethylamide or LSD)
Bromocriptine inhibits prolactin CVS – vasoconstriction d/t partial
agonist effects at α adrenoceptors
Nausea, vomiting (high dose) Prolonged vasospasm
gangrene, bowel infarction Drowsiness, hallucinations
Ergotamine, Ergonovine, Methysergide – migraine headache (partial agonist α & 5HT2)
Uterus – postpartum hemorrhage, induces labor
Ergonovine, Oxytocin (parenteral), Methylergometrine (Methergine) parenteral or oral
EICOSANOIDSMechanism of Action Organ System Effect Adverse
EffectsIndications Contraindications Other notes
Arachidonic AcidProstaglandins
Arachidonic Acid Oxygenated by 4 routes:
Lipoxygenase: HETEs, leukotrienes, lipoxins
Cytochrome P450 (epoxygenase) – EETs, vasodilator
Icoeicosanoid: Isoprostane, vasoconstrictor
Cyclooxygenase: PG, prostacyclin, thromboxane
PGH synthase-1 (COX-1): gastric epithelial protection
PGH synthase-2 (COX-2): source in inflammation
ProstaglandinBind to receptors on cell surface
CVS TXA2, PGF2α – vasoconstriction,
bronchoconstriction, contraction of uterus
PGI2/prostacyclin, PGE1 – vasodilatation, bronchodila, relaxes uterus
Epoprostenol (PGI2) – pulmonary HPN
Alprostadil (PGE1) – patency of DA COX inhibitor (Indomethacin) –
closes ductus arteriosus GIT
Misoprostol/cytotec (PGE1) – for peptic ulcer (NSAID- induced), for abortion
Enprostil NA (PGE) – inhibit HCl secretion
Respiratory System PGE2, PGI2 – bronchodilatation
Lipid-derived autacoids Oxygenation products of polyunsaturated long chain fatty acids Plant & fish oil precursors Arachidonic Acid – most important precursor
Eicosanoid Inhibitors Corticosteroids: inhibits all pathways by stimulating synthesis of
inhibitory protein, inhibit phospholipase A prevent arachidonic acid release
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): blocks prostaglandin & thromboxane formation by inhibiting cyclooxygenase activity
Aspirin (Acetylsalicylic Acid) – irreversible acetylation of platelet cyclooxygenase (other drugs not irreversible); inhibits TXA2 synthesis
Mechanism of action: irreversibly inhibits platelet COX1 (8-10 days)
Indications: transient ischemic attack (TIA), CAD (coronary artery disease)
Adverse Effects: Gastric/duodenal ulcer
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 25 of 29Section 2D – Batch 2014
PGD2, TXA2 – bronchoconstriction PGF2α, LT – bronchoconstriction
Platelet aggregation PGD2, PGE2, PGI2 – inhibit TXA2 – stimulate Aspirin – inhibits platelet COX1
Kidney PGE2, PGI2 – vasodilatation TXA2 – vasoconstriction
Reproductive system PGF2α, PGE2- uterine contraction,
soften cervix Dinoprostone, Misoprostol,
Carboprost PGE2, PGF2α – SE dysmenorrhea
(take NSAIDs) Alprostadil (PGE1) – relax smooth
muscle of corpora cavernosa for erectile dysfunction
Effects of lipooxygenase, cytochrome P450 metabolites: CVS
12Hydroxyeicosatetraenoic (HETE) – chemoattractant for smooth muscles
LTC4, LTD4 – myocardial depressant, constriction of coronary arteries
GIT LTB4 – chemoattractant for PMNs
Respiratory LTC4, LTD4 – bronchoconstriction,
mucus secretion, plasma exudation Blood
LTB4 – chemoattractant for T cell, eosinophils, monocytes, mast cells
Renal System 20 HETE – vasoconstriction EET – vasodilatation, natriuresis
Hepatotoxic Allergy (most common)
Non-selective COX inhibitors – blocks prostaglandin, TXA2 synthesis
Pyrazone – Phenylbutazone, Oxybutazone Indole – Indomethacin, Sulindac Propionic acid – Ibuprofen, Naproxen, ketoprofen Anthranilic acid – Mefenamic acid Aryl-acetic acid – Diclofenac Oxicam – Piroxicam, Tenoxicam Pyrolopyrole – Ketorolac
COX-2 Selective Inhibitors Mechanism of action: bind to and block active site of
COX2 enzyme (reversible) Less GI effects, no platelet effect Adverse Effects:
Fluid retention Hypertension Hepatotoxic Nephrotoxic Rashes
VASOACTIVE PEPTIDESANGIOTENSIN RECEPTOR ANTAGONISTS
Mechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Valsartan Selective competitive antagonist of angiotensin AT1 receptors
Arteriolar dilationdecreased aldosterone secretionincreased sodium and water excretion
Hypertension Eprosartan, irbesartan, candesartan, olmesartan, telmisarta - similar to valsartan
CONVERTING ENZYME INHIBITORSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
EnalaprilInhibits conversion of angiotensin I to angiotensin II
Arteriolar dilationdecreased aldosterone secretionincreased sodium and water excretion
Hypertension heart failure Captopril and many others -similar to enalapril
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 26 of 29Section 2D – Batch 2014
RENIN INHIBITORSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Aliskiren Inhibits catalytic activity of reninArteriolar dilationdecreased aldosterone secretionincreased sodium and water excretion
Hypertension
KININ ANTAGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
IcatibantSelective antagonist of kinin B2
receptorsBlocks effects of kinins on pain, hyperalgesia, and inflammation
Potential use for inflammatory pain and inflammation
VASOPRESSIN AGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Arginine vasopressinAgonist of vasopressin V1 (and V2) receptors Vasoconstriction Vasodilatory shock Terlipressin - more selective for V1 receptor
VASOPRESSIN ANTAGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Conivaptan Antagonist of vasopressin V1 (and V2) receptors
VasodilationPotential use in hypertension and heart failure hyponatremia
Relcovaptan – increased selectivity for V1
receptor
NATRIURETIC PEPTIDESMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Nesiritide Agonist of natriuretic peptide receptors Increased sodium and water excretionvasodilation Heart failure
VASOPEPTIDASE INHIBITORSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
OmapatrilatDecreases metabolism of natriuretic peptides and formation of angiotensin II Vasodilation
increased sodium and water excretion Hypertension heart failure
ENDOTHELIN ANTAGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
BosentanNonselective antagonist of endothelin ETA and ETB receptors Vasodilation Pulmonary arterial
hypertension Sitaxsentan, Ambrisentan - selective for ETA
receptors
VASOACTIVE INTESTINAL PEPTIDE AGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Under developmentSelective and nonselective agonists of VPAC1 and VPAC2 receptors
VasodilationMultiple metabolic, endocrine, and other effects
Type 2 diabetes chronic obstructive pulmonary disease
SUBSTANCE P ANTAGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
AprepitantSelective antagonist of tachykinin NK1
receptorsBlocks several central nervous system effects of substance P
Prevention of chemotherapy-induced nausea and vomiting
Monique · Wine · Jamie · Juria · Lenard PHARMACOLOGY: COMPREHENSIVE TABLE OF DRUGS (1st Shifting Period) | Page 27 of 29Section 2D – Batch 2014
NEUROTENSIN AGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
PD149163 Agonist of central neurotensin receptors Interacts with central dopamine systems
Potential for treatment of schizophrenia and Parkinson's disease
NEUROTENSIN ANTAGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
MeclinertantAntagonist of central and peripheral neurotensin receptors
Blocks some central and peripheral (vasodilator) actions of neurotensin None identified
CALCITONIN GENE-RELATED PEPTIDE ANTAGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
BIBN4096BSAntagonist of calcitonin gene-related peptide (CGRP)
Blocks some central and peripheral (vasodilator) actions of CGRP Migraine
NEUROPEPTIDE Y ANTAGONISTSMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
BIBP3226Selective antagonist of neuropeptide Y1
receptorsBlocks vasoconstrictor response to neurotensin
None identified
Urotensin AntagonistsMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
PalosuranPeptide antagonist of urotensin receptors
Blocks potent vasoconstrictor action of endothelin Diabetic renal failure
NITRIC OXIDEMechanism of Action Organ System Effects Adverse Effects Indications Contraindications Other Notes
Nitric Oxide
NO activates soluble guanylyl cyclase to elevate cGMP levels in vascular
smooth muscle
1. blood vessels vasodilator inhibits PMN adhesion to endothelium
2. respiratory system relax smooth muscles for pulmonary hypertension and ARDS
3. platelets inhibits platelet adhesion, aggregation,
enhance fibrinolysis4. CNS
modifies NT release, learning & brain development
Methemoglobinemia
Hypoxic respiratory failure and pulmonary hypertension Inhaled gas





























