Embed Size (px)
Citation preview

1
Croatia
PHARMACEUTICAL COUNTRY PROFILE
2
Croatia Pharmaceutical Country Profile
Published by Ministry of Health and Social Welfare in collaboration with the World Health Organization
01/06/2011
Any part of this document may be freely reviewed, quoted, reproduced, or translated in full or in part, provided that the source is acknowledged. It may not be sold, or used in
conjunction with commercial purposes or for profit.
This document was produced with the support of the World Health Organization (WHO) Croatia Country Office, and all reasonable precautions have been taken to verify the information contained herein. The published material does not imply the expression of any opinion
whatsoever on the part of the World Health Organization, and is being distributed without any warranty of any kind – either expressed or implied. The responsibility for interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for
damages arising from its use.
3
Foreword
The 2011 Pharmaceutical Country Profile for Croatia has been produced by the
Ministry of Health and Social Welfare, in collaboration with the World Health
Organization.
This document contains information on existing socio-economic and health-
related conditions, resources; as well as on regulatory structures, processes and
outcomes relating to the pharmaceutical sector in Croatia. The compiled data
comes from international sources (e.g. the World Health Statistics1,2), surveys
conducted in the previous years and country level information collected in 2011.
The sources of data for each piece of information are presented in the tables that
can be found at the end of this document.
It is my hope that partners, researchers, policy-makers and all those who are
interested in the Croatia pharmaceutical sector will find this profile a useful tool to
aid their activities.
Name: Ante - Zvonimir Golem, MD Ministry of Health and Social Welfare: State Secretary for Health and Social Welfare Date: 01/06/2011
4
Table of content
Foreword...............................................................................................................3
Table of content ....................................................................................................4
Introduction ...........................................................................................................1
Section 1 - Health and Demographic Data ........................................................7
Section 2 - Health Services ................................................................................9
Section 3 - Policy Issues ..................................................................................13
Section 4 – Medicines Trade and Production.................................................14
Section 5 – Medicines Regulation ...................................................................16
Section 6 - Medicines Financing......................................................................26
Section 7 - Pharmaceutical procurement and distribution in the public
sector .................................................................................................................29
Section 8 - Selection and rational use of medicines......................................30
Section 9 - Household data/access .................................................................33
5
Introduction
This Pharmaceutical Country Profile provides data on existing socio-economic
and health-related conditions, resources, regulatory structures, processes and
outcomes relating to the pharmaceutical sector of Croatia. The aim of this
document is to compile all relevant, existing information on the pharmaceutical
sector and make it available to the public in a user-friendly format. In 2010, the
country profiles project was piloted in 13 countries
(http://www.who.int/medicines/areas/coordination/coordination_assessment/en/in
dex.html). During 2011, the World Health Organization has supported all WHO
Member States to develop similar comprehensive pharmaceutical country
profiles.
The information is categorized in 9 sections, namely: (1) Health and
Demographic data, (2) Health Services, (3) Policy Issues, (4) Medicines Trade
and Production (5) Medicines Regulation, (6) Medicines Financing, (7)
Pharmaceutical procurement and distribution, (8) Selection and rational use, and
(9) Household data/access. The indicators have been divided into two categories,
namely "core" (most important) and "supplementary" (useful if available). This
narrative profile is based on data derived from both the core and supplementary
indicators. The tables in the annexes also present all data collected for each of
the indicators in the original survey form. For each piece of information, the year
and source of the data are indicated; these have been used to build the
references in the profile and are also indicated in the tables. If key national
documents are available on-line, links have been provided to the source
documents so that users can easily access these documents.
The selection of indicators for the profiles has involved all technical units working
in the Essential Medicines Department of the World Health Organization (WHO),
as well as experts from WHO Regional and Country Offices, Harvard Medical
6
School, Oswaldo Cruz Foundation (known as Fiocruz), University of Utrecht, the
Austrian Federal Institute for Health Care and representatives from 13 pilot
countries.
Data collection in all 193 member states has been conducted using a user-
friendly electronic questionnaire that included a comprehensive instruction
manual and glossary. Countries were requested not to conduct any additional
surveys, but only to enter the results from previous surveys and to provide
centrally available information. To facilitate the work of national counterparts, the
questionnaires were pre-filled at WHO HQ using all publicly-available data and
before being sent out to each country by the WHO Regional Office. A coordinator
was nominated for each of the member states. The coordinator for Croatia was
Sibila Žabica.
The completed questionnaires were then used to generate individual country
profiles. In order to do this in a structured and efficient manner, a text template
was developed. Experts from member states took part in the development of the
profile and, once the final document was ready, an officer from the Ministry of
Health certified the quality of the information and gave formal permission to
publish the profile on the WHO web site.
This profile will be regularly updated by the Ministry of Health and Social Welfare.
Comments, suggestions or corrections may be sent to:
Sibila Žabica
7
Section 1 - Health and Demographic Data
This section gives an overview of the demographics and health status of Croatia.
1.1 Demographics and Socioeconomic Indicators
The total population of Croatia in 2008 was 4,423,000 with an annual population
growth rate of -0.4%3. The annual GDP growth rate is -5.8%. The GDP per capita
was US$14,251 (at the current exchange ratei)4.
Around 15% of the population is under 15 years of age, and 23% of the
population is over 60 years of age. The urban population currently stands at 57%
of the total population. The fertility rate in Croatia is 1.4 births per woman3.
About 2% of the population is living with less than $1.25/day (international PPP).
The share of national income held by the lowest 20% of the population is 8.8%5.
The adult literacy rate for the population over 15 years is 99%3.
1.2 Mortality and Causes of Death
The life expectancy at birth is 73 and 80 years for men and women respectively6.
The infant mortality rate (i.e. children under 1 year) is 5.3/ 1,000 live births. For
children under the age of 5, the mortality rate is 6.1/ 1,000 live births. The
maternal mortality rate is 13.5/ 100,000 live births7.
The top 10 diseases causing mortality in Croatia are [Croatian National Institute
of Public Health (CNIPH) (2009)]:
Disease
1 Ischemic heart diseases
2 Cerebrovascular diseases
3 Malignant neoplasms of trachea, bronchus and lung
4 Heart failure
5 Malignant neoplasms of colon, rectum and anus
6 Bronchitis, emphysema, asthma
i Exchange rate: 1 HRK = 0.1969 USD as of 06/06/2011 (d/m/y)
8
7 Hypertensive diseases
8 Diabetes mellitus
9 Atherosclerosis
10 Chronic liver diseases, fibrosis and cirrhosis
The top 10 diseases causing morbidity in Croatia are [Croatian National Institute
of Public Health (CNIPH) (2009)]
Disease
1 Senile cataract
2 Malignant neoplasm of bronchus and lung
3 Cerebral infarction
4 Mental and behavioural disorders due to use of alcohol
5 Angina pectoris
6 Choleithiasis
7 Pneumonia
8 Chronic disease of tonsils and adenoids
9 Inguinal hernia
10 Acute myocardial infarction
The adult mortality rate for both sexes between 15 and 60 years is 115/ 1,000
population, while the neonatal mortality rate is 4.3/ 1,000 life births3,7. The age-
standardised mortality rate for non-communicable diseases 578/ 100,000, of
which 318/ 100,000 are for cardiovascular diseases and 166/ 100,000for
cancer2,8. The mortality rate for HIV/AIDS is 0.18/ 100,000 and 2.7/ 100,000 for
tuberculosis. The mortality rate for Malaria is 0/ 100,0002,6,7.
9
Section 2 - Health Services
This section provides information regarding health expenditures and human
resources for health in Croatia. The contribution of the public and private sector
to overall health expenditure is shown and the specific information on
pharmaceutical expenditure is also presented. Data on human resources for
health and for the pharmaceutical sector is provided as well.
2.1 Health Expenditures
In Croatia, the total annual expenditure on health (THE) in 2008 was 26,787.46
million HRK (US$5,274.69 million)9. The total annual health expenditure was
8.4% of the GDP. The total annual expenditure on health per capita was 6,056
HRK (US$1,233])10.
The general governmentii health expenditure (GGHE) in 2008, as reflected in the
national health accounts (NHA) was 22,734 million HRK (US$4,629 million).
That is, 85% of the total expenditure on health, with a total annual per capita
public expenditure on health of 5,140 HRK (US$1,047). The government annual
expenditure on health represents 18% of the total government budget. Private
health expenditure covers the remaining 15% of the total health expenditure9.
Of the total population, 99% is covered by a public health service, public health
insurance or social insurance, or other sickness funds and 16% is covered by a
private health insurance11.
Total pharmaceutical expenditure (TPE) in Croatia in 2008 was 3,392 million
HRK (US$690.8 million), which is a per capita pharmaceutical expenditure of 766
HRK (US$156). The total pharmaceutical expenditure accounts for 1.1% of the
GDP and makes up 13% of the total health expenditure (Figure 1)11.
ii According to the NHA definition, by "government expenditure" it is meant all expenditure from public sources, like central government, local government, public insurance funds and parastatal companies.

10
Figure 1: Share of Total Pharmaceutical Expenditure as percentage of the Total
Health Expenditure (2008) The THE in 2008 was 26,787.46 million HRK
(US$5,274.69 million)
[National Health Accounts data (2008) & Croatian Institute for Health Insurance (HZZO) (2008)]
Social security expenditure makes up 91% of government expenditure on health.
Private out-of-pocket expenditure as % of private health expenditure is 93%.
Premiums for private prepaid health plans are 7.0% of total private health
expenditure9.
2.2 Health Personnel and Infrastructure
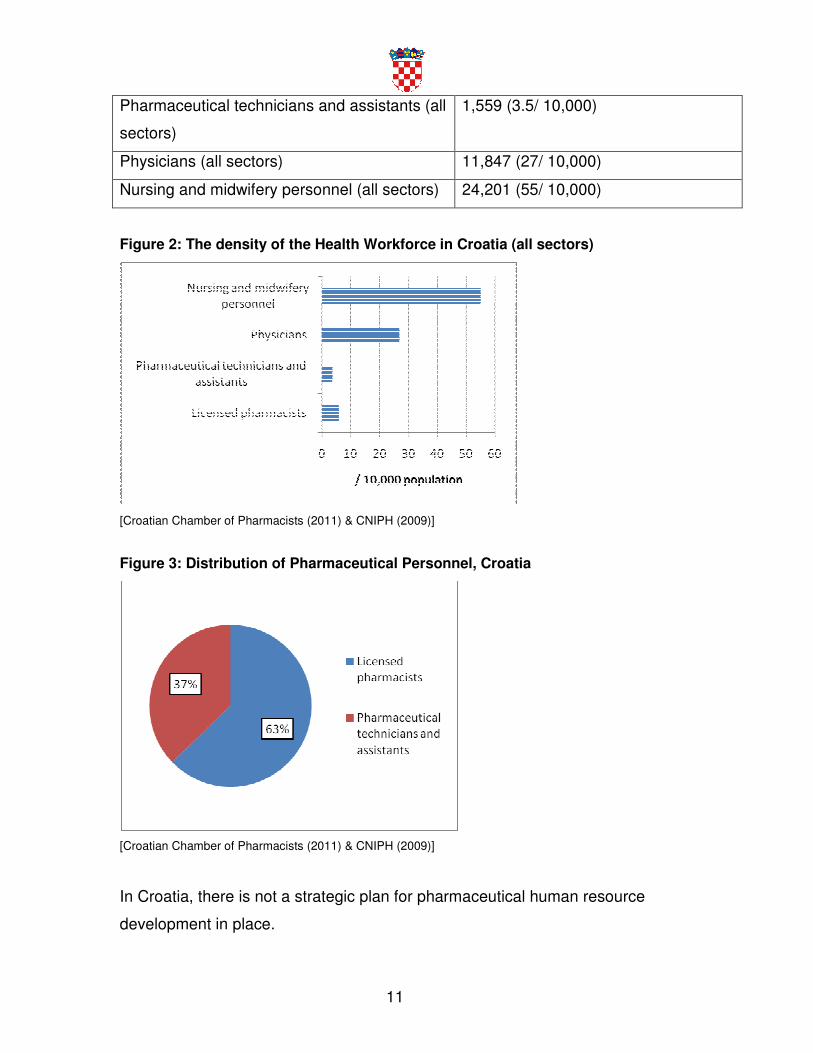
The health workforce is described in Table 1 below and in Figure 2 and 3. There
are 2,985 (5.9/ 10,000) licensed pharmacists, of which 1,415 (3.2/10,000) work in
the public sector. There are 1,559 (3.5/ 10,000) pharmaceutical technicians and
assistants (in all sectors)7,12.
There are 11,847 (27/ 10,000) physicians and 24,201 (55/ 10,000) nursing and
midwifery personnel in Croatia. The ratio of doctors to pharmacists is 4 and the
ratio of doctors to nurses and midwifery personnel is 0.57.
Table 1: Human resources for health in Croatia7
Human Resource
Licensed pharmacists (all sectors) 2,985 (5.9/ 10,000)
Pharmacists in the public sector 1,415 (3.2/10,000)
11
Pharmaceutical technicians and assistants (all
sectors)
1,559 (3.5/ 10,000)
Physicians (all sectors) 11,847 (27/ 10,000)
Nursing and midwifery personnel (all sectors) 24,201 (55/ 10,000)
Figure 2: The density of the Health Workforce in Croatia (all sectors)
[Croatian Chamber of Pharmacists (2011) & CNIPH (2009)]
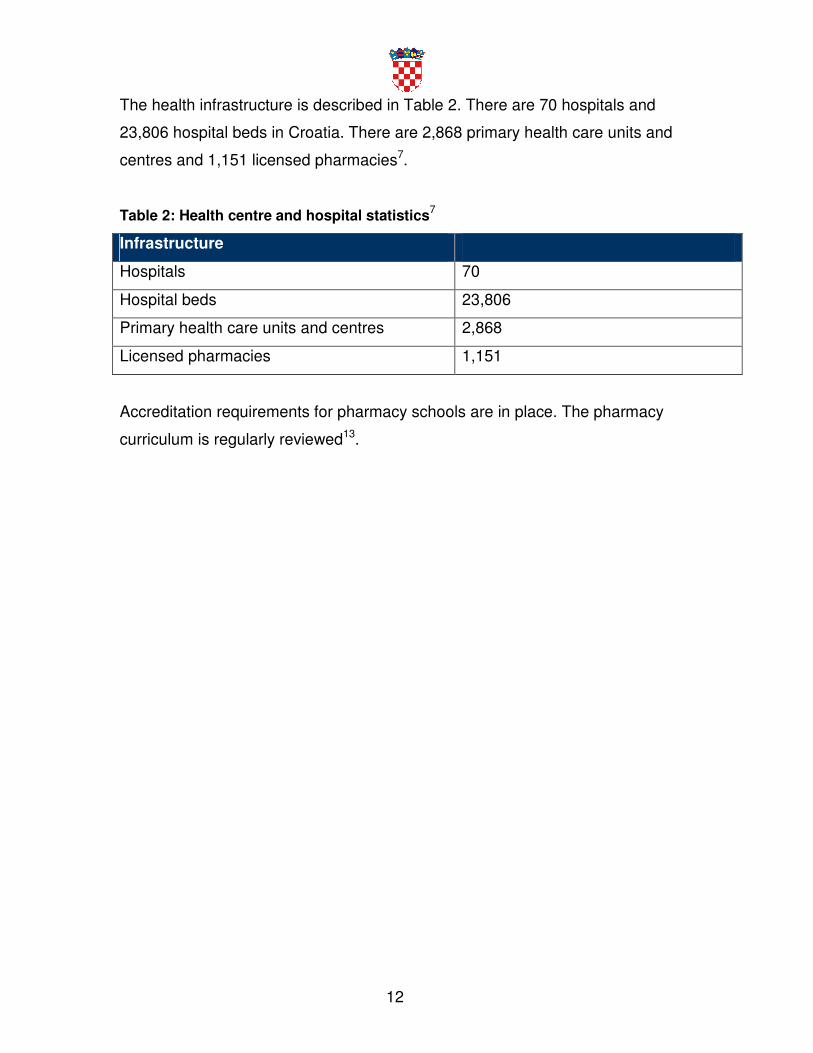
Figure 3: Distribution of Pharmaceutical Personnel, Croatia
[Croatian Chamber of Pharmacists (2011) & CNIPH (2009)]
In Croatia, there is not a strategic plan for pharmaceutical human resource
development in place.
12
The health infrastructure is described in Table 2. There are 70 hospitals and
23,806 hospital beds in Croatia. There are 2,868 primary health care units and
centres and 1,151 licensed pharmacies7.
Table 2: Health centre and hospital statistics7
Infrastructure
Hospitals 70
Hospital beds 23,806
Primary health care units and centres 2,868
Licensed pharmacies 1,151
Accreditation requirements for pharmacy schools are in place. The pharmacy
curriculum is regularly reviewed13.
13
Section 3 - Policy Issues
This section addresses the main characteristics of the pharmaceutical policy in
Croatia. The many components of a national pharmaceutical policy are taken
from the WHO publication “How to develop and implement national drug policy”
(http://apps.who.int/medicinedocs/en/d/Js2283e/). Information about the capacity
for manufacturing medicines and the legal provisions governing patents is also
provided.
3.1 Policy Framework
In Croatia, a National Health Policy (NHP) exists14. It was updated in 2006. An
associated National Health Policy implementation plan written in 2006 also
exists15.
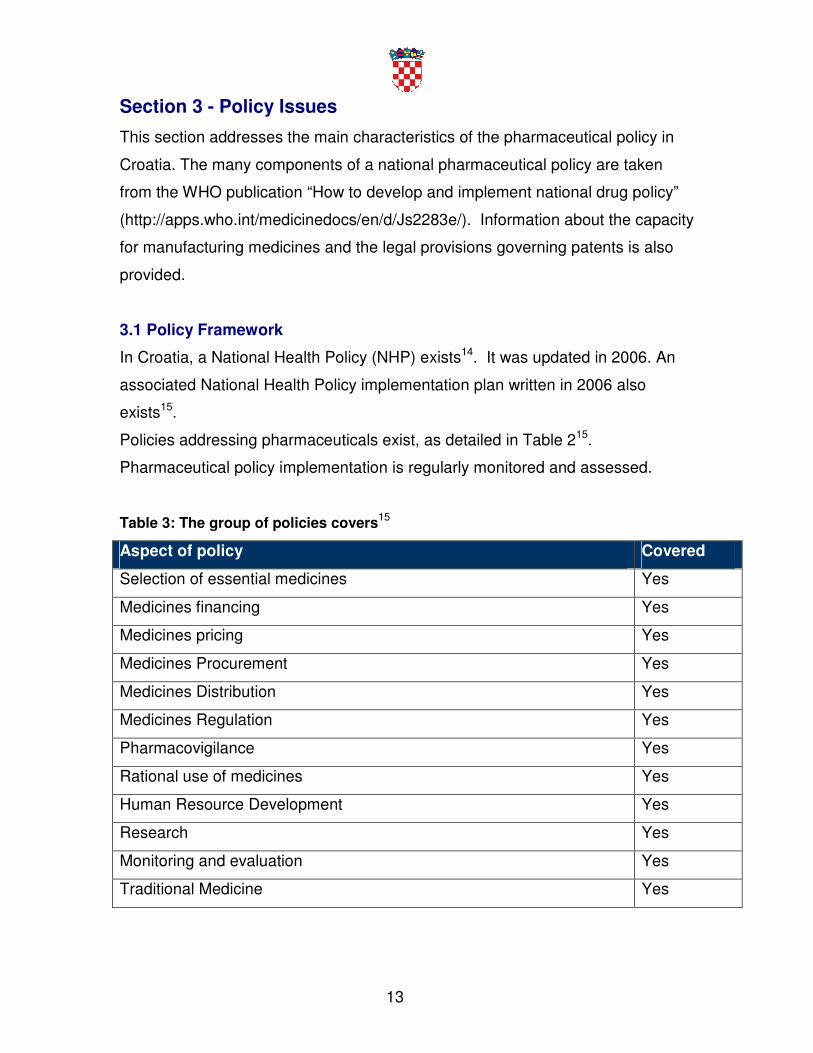
Policies addressing pharmaceuticals exist, as detailed in Table 215.
Pharmaceutical policy implementation is regularly monitored and assessed.
Table 3: The group of policies covers15
Aspect of policy Covered
Selection of essential medicines Yes
Medicines financing Yes
Medicines pricing Yes
Medicines Procurement Yes
Medicines Distribution Yes
Medicines Regulation Yes
Pharmacovigilance Yes
Rational use of medicines Yes
Human Resource Development Yes
Research Yes
Monitoring and evaluation Yes
Traditional Medicine Yes
14
Section 4 – Medicines Trade and Production
4.1 Intellectual Property Laws and Medicines
Croatia is a member of the World Trade Organization16. Legal provisions granting
patents to manufacturers exist. These cover pharmaceuticals, laboratory supplies,
medical supplies and medical equipment17.
Intellectual Property Rights are managed and enforced by the State Intellectual
Property Office, http://www.dziv.hr.
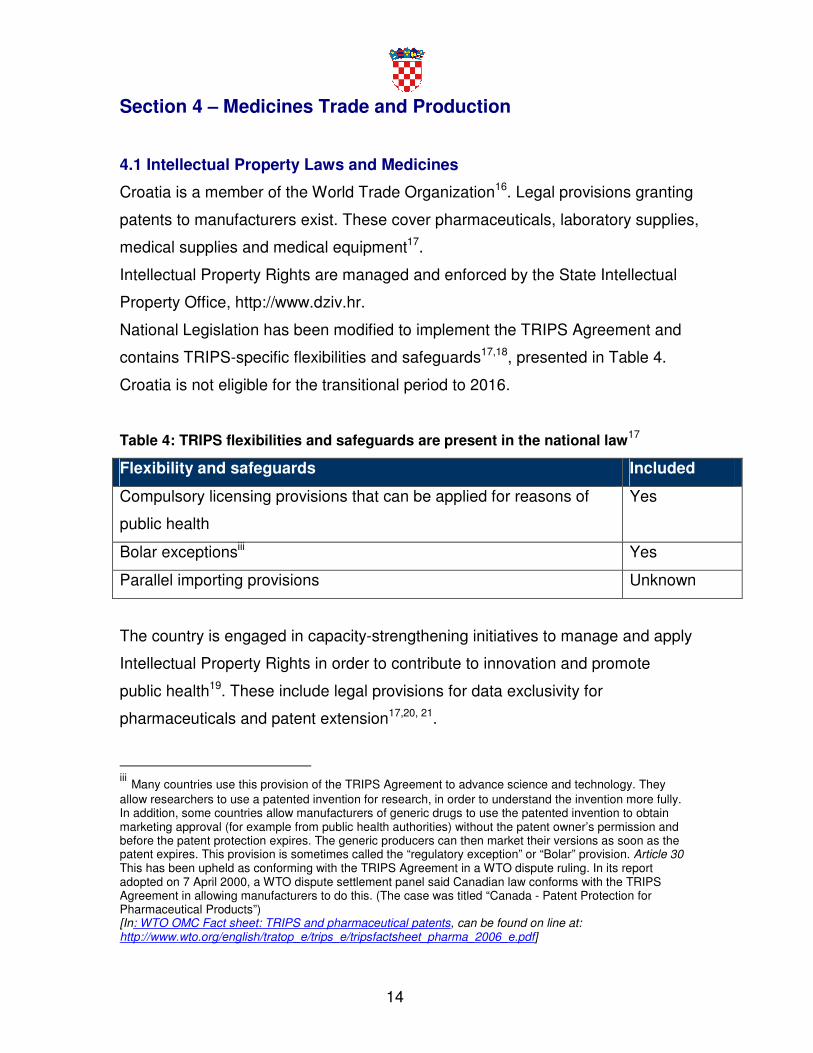
National Legislation has been modified to implement the TRIPS Agreement and
contains TRIPS-specific flexibilities and safeguards17,18, presented in Table 4.
Croatia is not eligible for the transitional period to 2016.
Table 4: TRIPS flexibilities and safeguards are present in the national law17
Flexibility and safeguards Included
Compulsory licensing provisions that can be applied for reasons of
public health
Yes
Bolar exceptionsiii Yes
Parallel importing provisions Unknown
The country is engaged in capacity-strengthening initiatives to manage and apply
Intellectual Property Rights in order to contribute to innovation and promote
public health19. These include legal provisions for data exclusivity for
pharmaceuticals and patent extension17,20, 21.
iii Many countries use this provision of the TRIPS Agreement to advance science and technology. They allow researchers to use a patented invention for research, in order to understand the invention more fully. In addition, some countries allow manufacturers of generic drugs to use the patented invention to obtain marketing approval (for example from public health authorities) without the patent owner’s permission and before the patent protection expires. The generic producers can then market their versions as soon as the patent expires. This provision is sometimes called the “regulatory exception” or “Bolar” provision. Article 30 This has been upheld as conforming with the TRIPS Agreement in a WTO dispute ruling. In its report adopted on 7 April 2000, a WTO dispute settlement panel said Canadian law conforms with the TRIPS Agreement in allowing manufacturers to do this. (The case was titled “Canada - Patent Protection for Pharmaceutical Products”) [In: WTO OMC Fact sheet: TRIPS and pharmaceutical patents, can be found on line at: http://www.wto.org/english/tratop_e/trips_e/tripsfactsheet_pharma_2006_e.pdf]
15
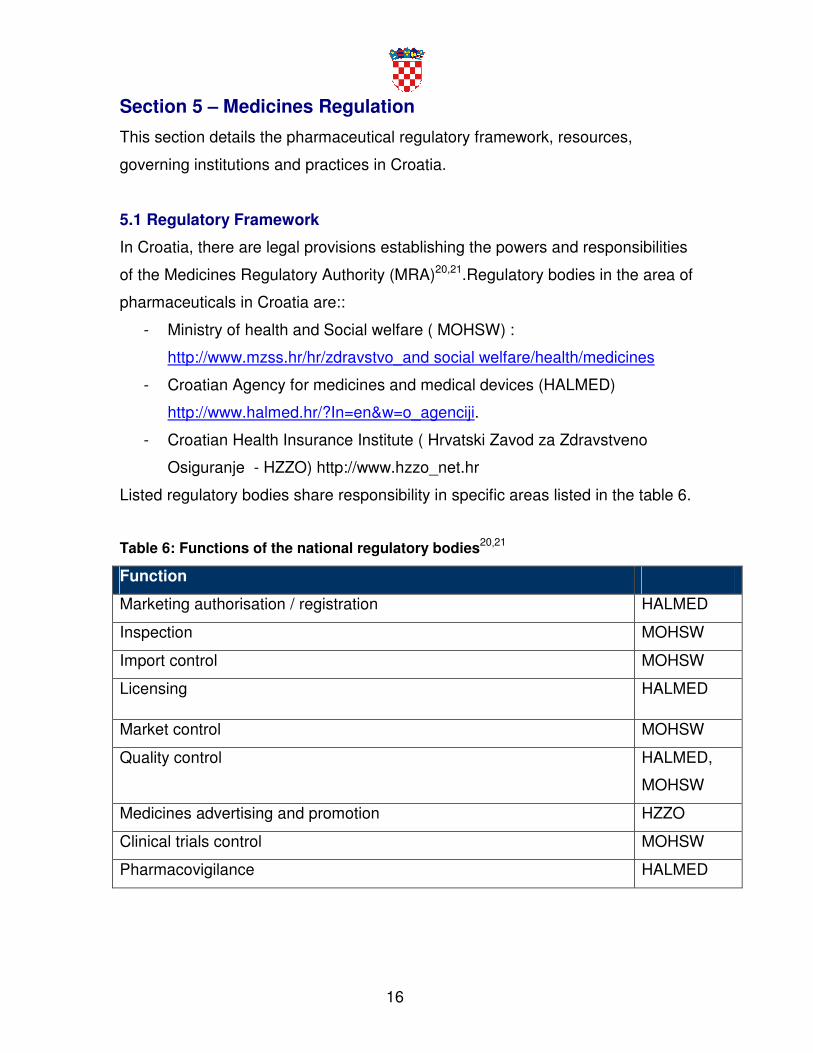
4.2 Manufacturing
There are 16 licensed pharmaceutical manufacturers in Croatia19. Manufacturing
capabilities are presented in Table 5 below.
Table 5: Croatia manufacturing capabilities19
Manufacturing capabilities
Research and Development for discovering new active substances Yes
Production of pharmaceutical starting materials (APIs) Yes
The production of formulations from pharmaceutical starting material Yes
The repackaging of finished dosage forms Yes
In 2011, domestic manufacturers held 20% of the market share by value
produced. The percentage of market share by volume produced by domestic
manufacturers is 33%. Five multinational pharmaceutical companies currently
manufacture medicines locally. Four of these five Croatian companies which are
now part of multinational companies. The 5th manufacturer is originally from
another country and established a production site in Croatia. There are 16
manufacturers that are Good Manufacturing Practice (GMP) certified19.
16
Section 5 – Medicines Regulation
This section details the pharmaceutical regulatory framework, resources,
governing institutions and practices in Croatia.
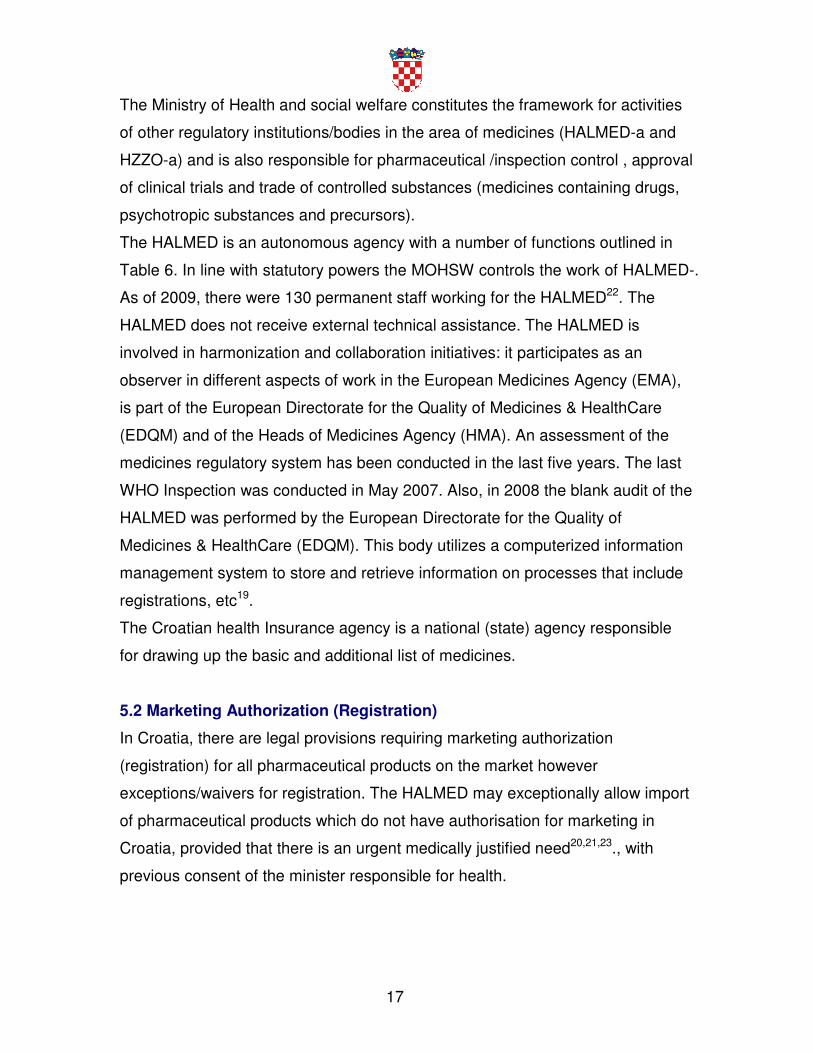
5.1 Regulatory Framework
In Croatia, there are legal provisions establishing the powers and responsibilities
of the Medicines Regulatory Authority (MRA)20,21.Regulatory bodies in the area of
pharmaceuticals in Croatia are::
- Ministry of health and Social welfare ( MOHSW) :
http://www.mzss.hr/hr/zdravstvo_and social welfare/health/medicines
- Croatian Agency for medicines and medical devices (HALMED)
http://www.halmed.hr/?In=en&w=o_agenciji.
- Croatian Health Insurance Institute ( Hrvatski Zavod za Zdravstveno
Osiguranje - HZZO) http://www.hzzo_net.hr
Listed regulatory bodies share responsibility in specific areas listed in the table 6.
Table 6: Functions of the national regulatory bodies20,21
Function
Marketing authorisation / registration HALMED
Inspection MOHSW
Import control MOHSW
Licensing HALMED
Market control MOHSW
Quality control HALMED,
MOHSW
Medicines advertising and promotion HZZO
Clinical trials control MOHSW
Pharmacovigilance HALMED
17
The Ministry of Health and social welfare constitutes the framework for activities
of other regulatory institutions/bodies in the area of medicines (HALMED-a and
HZZO-a) and is also responsible for pharmaceutical /inspection control , approval
of clinical trials and trade of controlled substances (medicines containing drugs,
psychotropic substances and precursors).
The HALMED is an autonomous agency with a number of functions outlined in
Table 6. In line with statutory powers the MOHSW controls the work of HALMED-.
As of 2009, there were 130 permanent staff working for the HALMED22. The
HALMED does not receive external technical assistance. The HALMED is
involved in harmonization and collaboration initiatives: it participates as an
observer in different aspects of work in the European Medicines Agency (EMA),
is part of the European Directorate for the Quality of Medicines & HealthCare
(EDQM) and of the Heads of Medicines Agency (HMA). An assessment of the
medicines regulatory system has been conducted in the last five years. The last
WHO Inspection was conducted in May 2007. Also, in 2008 the blank audit of the
HALMED was performed by the European Directorate for the Quality of
Medicines & HealthCare (EDQM). This body utilizes a computerized information
management system to store and retrieve information on processes that include
registrations, etc19.
The Croatian health Insurance agency is a national (state) agency responsible
for drawing up the basic and additional list of medicines.
5.2 Marketing Authorization (Registration)
In Croatia, there are legal provisions requiring marketing authorization
(registration) for all pharmaceutical products on the market however
exceptions/waivers for registration. The HALMED may exceptionally allow import
of pharmaceutical products which do not have authorisation for marketing in
Croatia, provided that there is an urgent medically justified need20,21,23., with
previous consent of the minister responsible for health.
18
Mutual recognitions mechanisms are not in place. Explicit and publicly available
criteria exist for assessing applications for marketing authorization of
pharmaceutical products23.
In 2011, there were 3,773 pharmaceutical products registered in Croatia24. There
are legal provisions requiring the HALMED to make the list of registered
pharmaceutical products publicly available and update it regularly. This register is
updated every year. The updated list can be accessed through:
http://narodne-novine.nn.hr/clanci/sluzbeni/2010_06_71_2146.html.
Medicines are always registered by their INN (International Non-proprietary
Names) + MAH (or manufacturer) or Brand name + INN25. Legal provisions
require a fee to be paid for Medicines Market Authorization (registration) based
on applications23.
Marketing Authorization holders are required by law to provide information about
variations to the existing Marketing Authorization. Legally, a Summary of Product
Characteristics (SPC) of the medicines that are registered is required to be
published. Furthermore, legal provisions requiring the establishment of an expert
committee involved in the Marketing Authorization process are in place.
Possession of a Certificate for Pharmaceutical Products (that accords with the
WHO Certification scheme) is required as part of the Marketing Authorization
application. By law, potential conflict of interests for experts involved in the
assessment and decision-making for registration must be declared. Applicants
may legally appeal against HALMED decisions20,25.
The registration fee (per application) for a pharmaceutical product containing a
New Chemical Entity (NCE) or a generic product is the same: US$ 5,05023.
The time limit imposed for the assessment of all Marketing Authorization
applications is 7 months20,23.
5.3 Regulatory Inspection
In Croatia, legal provisions exist allowing for the appointment of pharmaceutical
inspectors of the Ministry of Health and Social Welfare. Legal provisions exist
permitting inspectors to inspect premises where pharmaceutical activities are
19
performed; such inspections are required by law and are a pre-requisite for the
licensing of both public and private facilities. Where inspections are legal
requirements, these are the same for public and private facilities20.
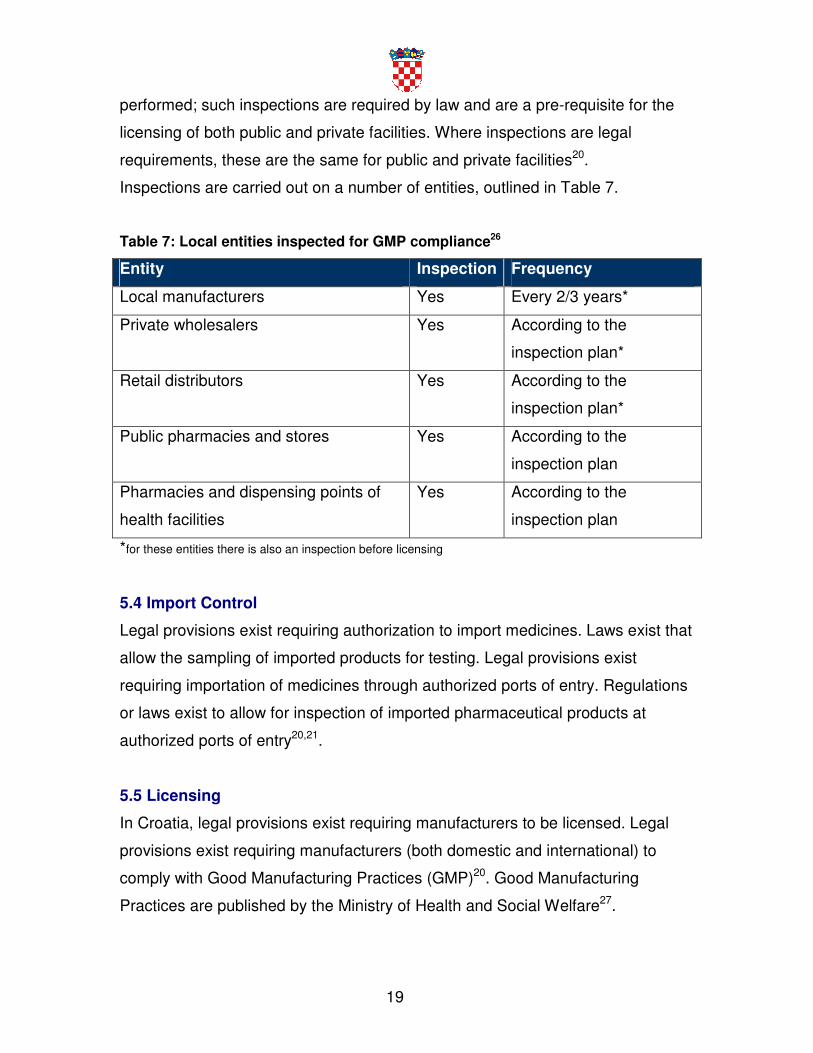
Inspections are carried out on a number of entities, outlined in Table 7.
Table 7: Local entities inspected for GMP compliance26
Entity Inspection Frequency
Local manufacturers Yes Every 2/3 years*
Private wholesalers Yes According to the
inspection plan*
Retail distributors Yes According to the
inspection plan*
Public pharmacies and stores Yes According to the
inspection plan
Pharmacies and dispensing points of
health facilities
Yes According to the
inspection plan
*for these entities there is also an inspection before licensing
5.4 Import Control
Legal provisions exist requiring authorization to import medicines. Laws exist that
allow the sampling of imported products for testing. Legal provisions exist
requiring importation of medicines through authorized ports of entry. Regulations
or laws exist to allow for inspection of imported pharmaceutical products at
authorized ports of entry20,21.
5.5 Licensing
In Croatia, legal provisions exist requiring manufacturers to be licensed. Legal
provisions exist requiring manufacturers (both domestic and international) to
comply with Good Manufacturing Practices (GMP)20. Good Manufacturing
Practices are published by the Ministry of Health and Social Welfare27.
20
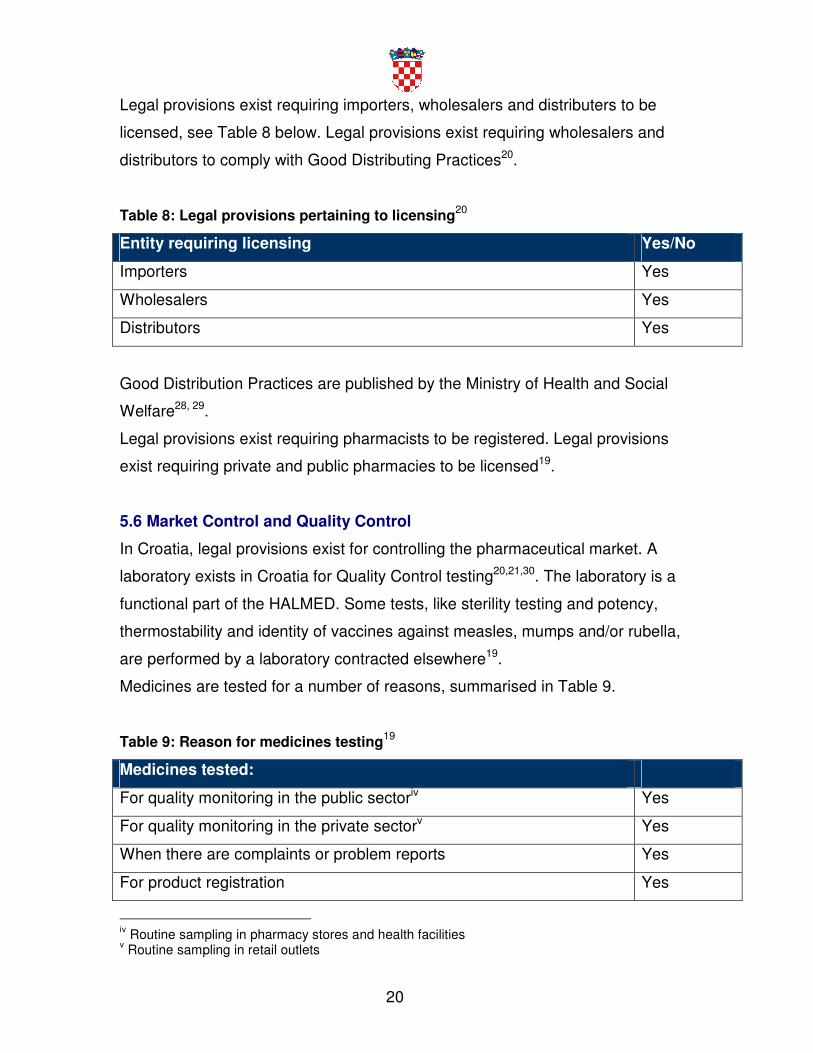
Legal provisions exist requiring importers, wholesalers and distributers to be
licensed, see Table 8 below. Legal provisions exist requiring wholesalers and
distributors to comply with Good Distributing Practices20.
Table 8: Legal provisions pertaining to licensing20
Entity requiring licensing Yes/No
Importers Yes
Wholesalers Yes
Distributors Yes
Good Distribution Practices are published by the Ministry of Health and Social
Welfare28, 29.
Legal provisions exist requiring pharmacists to be registered. Legal provisions
exist requiring private and public pharmacies to be licensed19.
5.6 Market Control and Quality Control
In Croatia, legal provisions exist for controlling the pharmaceutical market. A
laboratory exists in Croatia for Quality Control testing20,21,30. The laboratory is a
functional part of the HALMED. Some tests, like sterility testing and potency,
thermostability and identity of vaccines against measles, mumps and/or rubella,
are performed by a laboratory contracted elsewhere19.
Medicines are tested for a number of reasons, summarised in Table 9.
Table 9: Reason for medicines testing19
Medicines tested:
For quality monitoring in the public sectoriv Yes
For quality monitoring in the private sectorv Yes
When there are complaints or problem reports Yes
For product registration Yes
iv Routine sampling in pharmacy stores and health facilities v Routine sampling in retail outlets
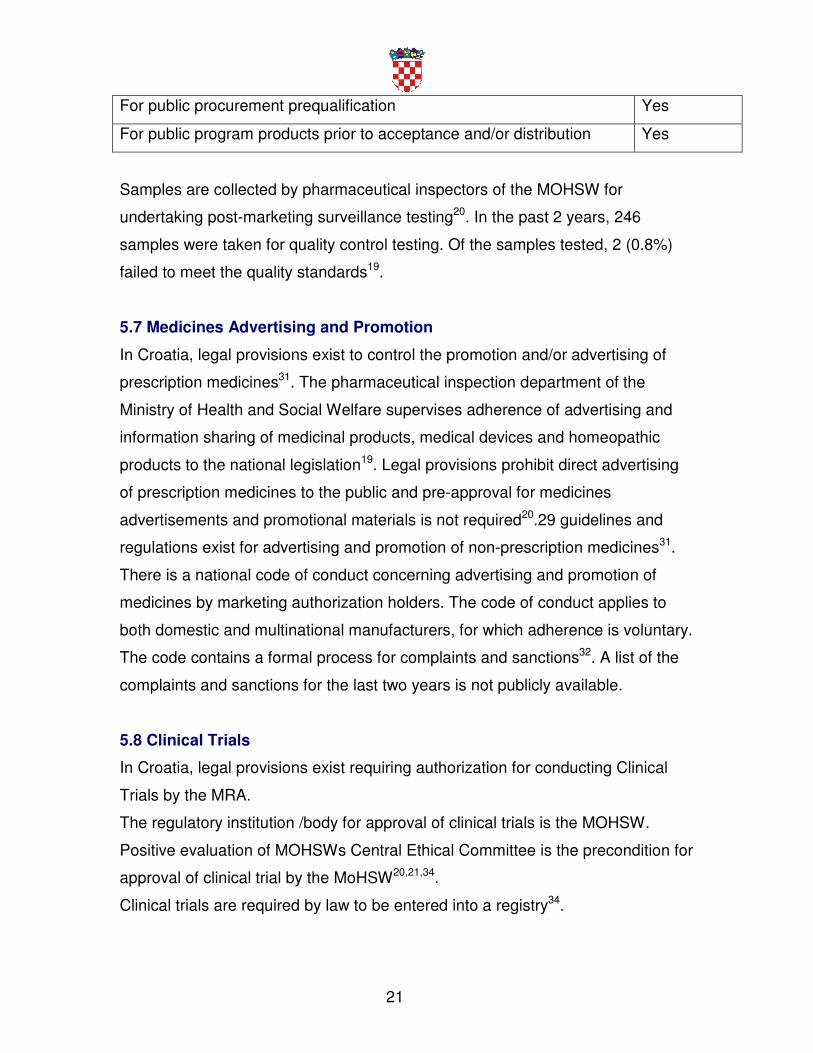
21
For public procurement prequalification Yes
For public program products prior to acceptance and/or distribution Yes
Samples are collected by pharmaceutical inspectors of the MOHSW for
undertaking post-marketing surveillance testing20. In the past 2 years, 246
samples were taken for quality control testing. Of the samples tested, 2 (0.8%)
failed to meet the quality standards19.
5.7 Medicines Advertising and Promotion
In Croatia, legal provisions exist to control the promotion and/or advertising of
prescription medicines31. The pharmaceutical inspection department of the
Ministry of Health and Social Welfare supervises adherence of advertising and
information sharing of medicinal products, medical devices and homeopathic
products to the national legislation19. Legal provisions prohibit direct advertising
of prescription medicines to the public and pre-approval for medicines
advertisements and promotional materials is not required20.29 guidelines and
regulations exist for advertising and promotion of non-prescription medicines31.
There is a national code of conduct concerning advertising and promotion of
medicines by marketing authorization holders. The code of conduct applies to
both domestic and multinational manufacturers, for which adherence is voluntary.
The code contains a formal process for complaints and sanctions32. A list of the
complaints and sanctions for the last two years is not publicly available.
5.8 Clinical Trials
In Croatia, legal provisions exist requiring authorization for conducting Clinical
Trials by the MRA.
The regulatory institution /body for approval of clinical trials is the MOHSW.
Positive evaluation of MOHSWs Central Ethical Committee is the precondition for
approval of clinical trial by the MoHSW20,21,34.
Clinical trials are required by law to be entered into a registry34.
22
Legal provisions exist for GMP compliance of investigational products33. Sponsor
investigators are legally required to comply with Good Clinical Practices (GCP).
National GCP regulations are published by the MOHSW34. Legal provisions
permit the inspection of facilities where clinical trials are performed20,21,34.
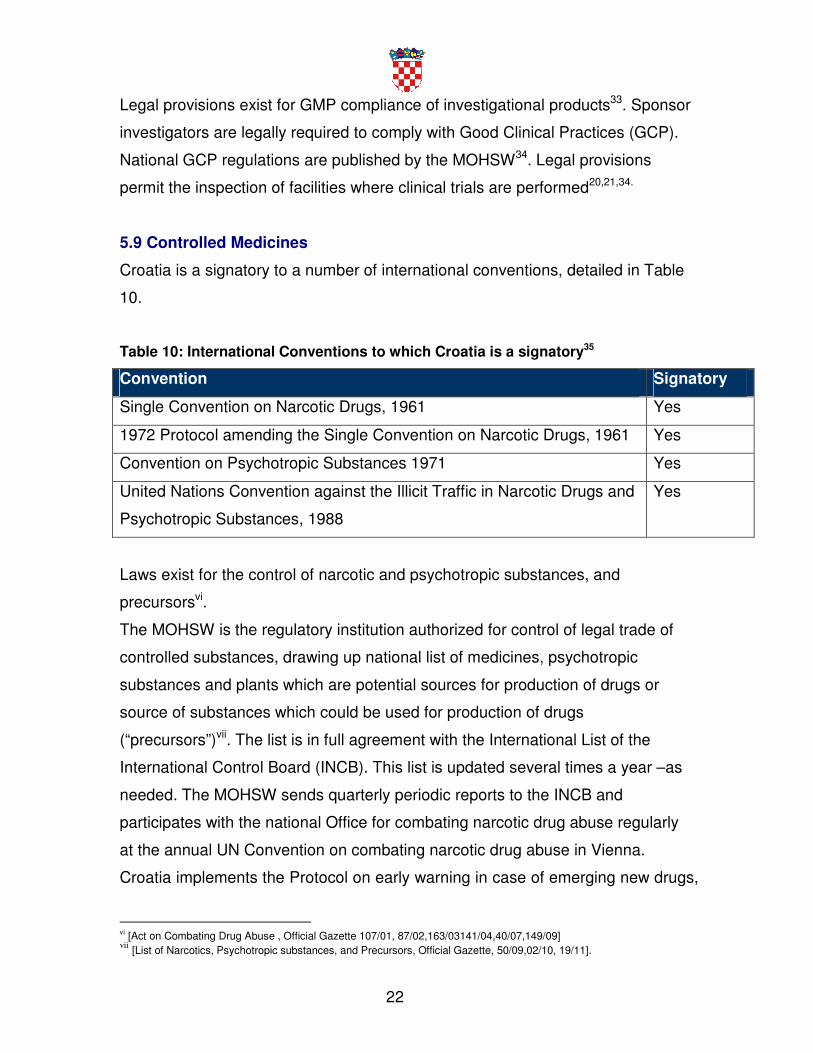
5.9 Controlled Medicines
Croatia is a signatory to a number of international conventions, detailed in Table
10.
Table 10: International Conventions to which Croatia is a signatory35
Convention Signatory
Single Convention on Narcotic Drugs, 1961 Yes
1972 Protocol amending the Single Convention on Narcotic Drugs, 1961 Yes
Convention on Psychotropic Substances 1971 Yes
United Nations Convention against the Illicit Traffic in Narcotic Drugs and
Psychotropic Substances, 1988
Yes
Laws exist for the control of narcotic and psychotropic substances, and
precursorsvi.
The MOHSW is the regulatory institution authorized for control of legal trade of
controlled substances, drawing up national list of medicines, psychotropic
substances and plants which are potential sources for production of drugs or
source of substances which could be used for production of drugs
(“precursors”)vii. The list is in full agreement with the International List of the
International Control Board (INCB). This list is updated several times a year –as
needed. The MOHSW sends quarterly periodic reports to the INCB and
participates with the national Office for combating narcotic drug abuse regularly
at the annual UN Convention on combating narcotic drug abuse in Vienna.
Croatia implements the Protocol on early warning in case of emerging new drugs,
vi [Act on Combating Drug Abuse , Official Gazette 107/01, 87/02,163/03141/04,40/07,149/09] vii
[List of Narcotics, Psychotropic substances, and Precursors, Official Gazette, 50/09,02/10, 19/11].
23
being implemented by the national Office for combating narcotic drug abuse,
MoHSW, Croatian National Institute of Public Health, Ministry of Internal Affairs
and Customs.
The Republic of Croatia is in the process of completing negotiations for EU
accession. Over the past years Croatia has been harmonising its legislation,
including legislation on drugs, with the EU legislation, thus ensuring the
registration and placement of numerous drugs containing narcotics and
psychotropic substances on the Croatian market, including drugs intended for
treatment of chronic pain, as well as drugs for the treatment of addicts.
Following WHO Guidelines on Pain Management and trying to ensure availability
of drugs containing opiates intended for pain management, the following
medicines have been enlisted on the Basic list of drugs: eight (8) morphine
preparations, five (5) hydromorphone preparations, two (2) oxycodone
preparations, pethidine, sixteen (16) preparations of various dosage fentanyl
patches, two pentazocine preparations, six (6) preparations of various dosage
buprenorphine patches and as many as 39 preparations of non-opioid analgesic
tramadole in various forms (capsules, pills, retard-pills, suppository, solutions for
injections), emphasizing that all these drugs are prescription drugs and are
completely free of charge, for outward as well as hospital patients.
Methadone has also been enlisted on the Basic list of drugs; it is completely free
of charge for the management of chronic pain of end-stage patients, as well as
for the treating opiate addicts.
The annual consumption of Morphine is 1.840380 mg/capita36.
The legal provisions and regulations for the control of narcotic and psychotropic
substances, and precursors have been reviewed by a WHO International Expert
or Partner Organization to assess the balance between the prevention of abuse
and access for medical need. These provisions were last reviewed in 2007.
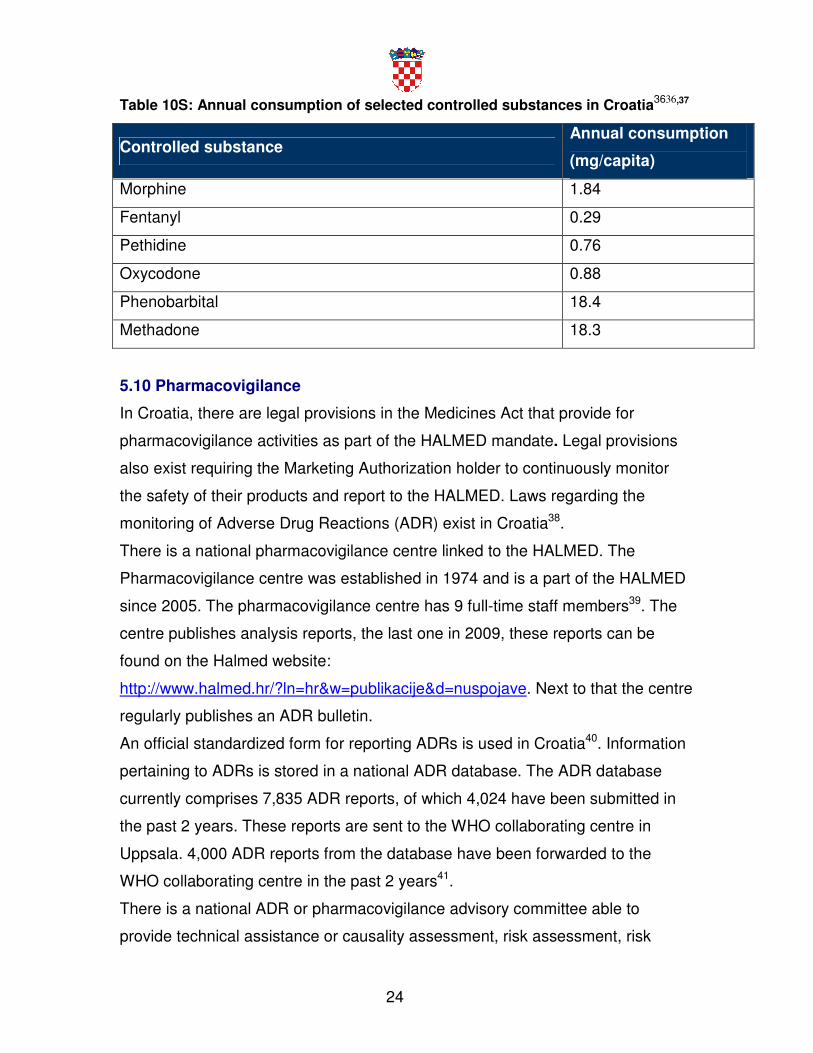
Figures regarding the annual consumption of certain controlled substances in the
country are outlined in Table 10S below.
24
Table 10S: Annual consumption of selected controlled substances in Croatia3636,37
Controlled substance Annual consumption
(mg/capita)
Morphine 1.84
Fentanyl 0.29
Pethidine 0.76
Oxycodone 0.88
Phenobarbital 18.4
Methadone 18.3
5.10 Pharmacovigilance
In Croatia, there are legal provisions in the Medicines Act that provide for
pharmacovigilance activities as part of the HALMED mandate. Legal provisions
also exist requiring the Marketing Authorization holder to continuously monitor
the safety of their products and report to the HALMED. Laws regarding the
monitoring of Adverse Drug Reactions (ADR) exist in Croatia38.
There is a national pharmacovigilance centre linked to the HALMED. The
Pharmacovigilance centre was established in 1974 and is a part of the HALMED
since 2005. The pharmacovigilance centre has 9 full-time staff members39. The
centre publishes analysis reports, the last one in 2009, these reports can be
found on the Halmed website:
http://www.halmed.hr/?ln=hr&w=publikacije&d=nuspojave. Next to that the centre
regularly publishes an ADR bulletin.
An official standardized form for reporting ADRs is used in Croatia40. Information
pertaining to ADRs is stored in a national ADR database. The ADR database
currently comprises 7,835 ADR reports, of which 4,024 have been submitted in
the past 2 years. These reports are sent to the WHO collaborating centre in
Uppsala. 4,000 ADR reports from the database have been forwarded to the
WHO collaborating centre in the past 2 years41.
There is a national ADR or pharmacovigilance advisory committee able to
provide technical assistance or causality assessment, risk assessment, risk

25
management, case investigation and, where necessary, crisis management
including crisis communication in Croatia. A clear communication strategy for
routine communication and crises communication exists1919.
A number of steps are being considered in order to enhance the
pharmacovigilance system. These include: electronic report submission via the
HALMED website for patients and healthcare professionals, or direct from the
local healthcare database from healthcare professionals, direct communication to
reporters, more safety information for patients on the HALMED's web site and
strenghening of PSUR analysis and RMP analysis by the HALMED staff1919.
26
Section 6 - Medicines Financing
In this section, information is provided on the medicines financing mechanism in
Croatia, including the medicines coverage through public and private health
insurance, use of user charges for medicines and the existence of public
programmes providing free medicines. Policies and regulations affecting the
pricing and availability of medicines (e.g. price control and taxes) are also
discussed.
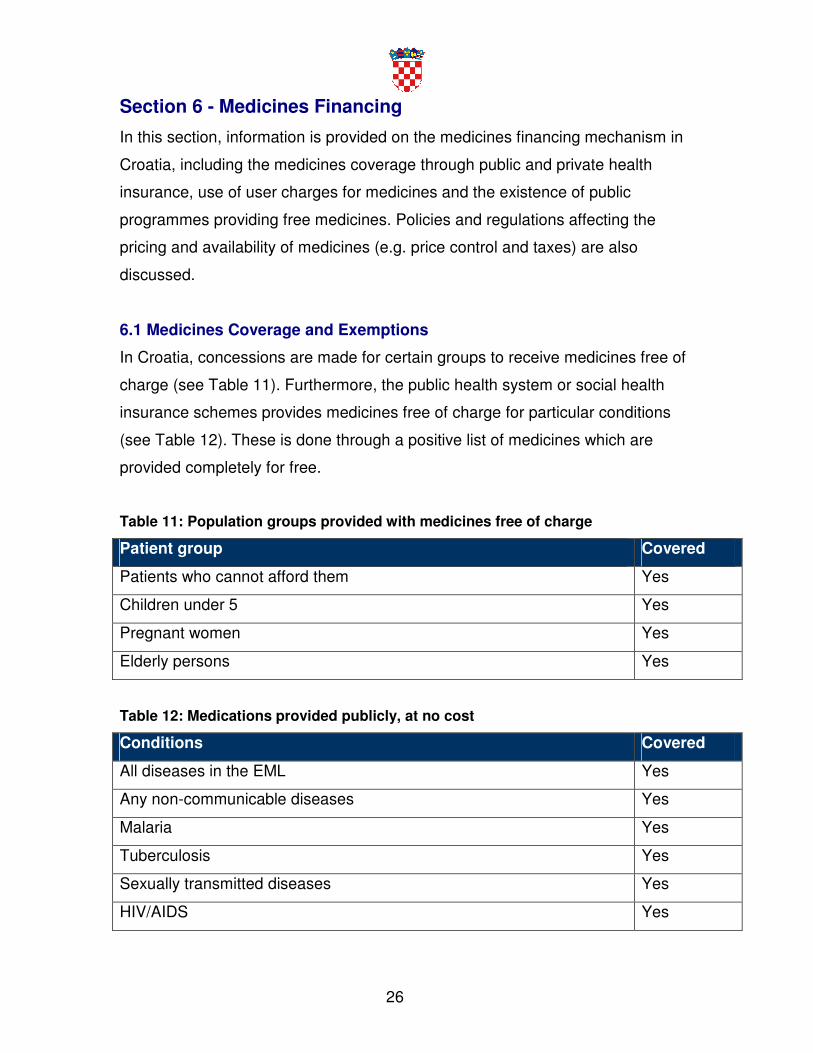
6.1 Medicines Coverage and Exemptions
In Croatia, concessions are made for certain groups to receive medicines free of
charge (see Table 11). Furthermore, the public health system or social health
insurance schemes provides medicines free of charge for particular conditions
(see Table 12). These is done through a positive list of medicines which are
provided completely for free.
Table 11: Population groups provided with medicines free of charge
Patient group Covered
Patients who cannot afford them Yes
Children under 5 Yes
Pregnant women Yes
Elderly persons Yes
Table 12: Medications provided publicly, at no cost
Conditions Covered
All diseases in the EML Yes
Any non-communicable diseases Yes
Malaria Yes
Tuberculosis Yes
Sexually transmitted diseases Yes
HIV/AIDS Yes
27
Expanded Program on Immunization (EPI) vaccines for children Yes
The Croatian Institute for Health Insurance implements two lists, the basic list
with all essential medicines covered by mandatory insurance and the
complementary list with medicines covered partially through mandatory
insurance, and partially by out of pocket payments. Medicines are free of charge
if they are in the positive list, regardless of the situation (age, financial status, in-
patient, out-patient etc) of patient42,43.
Private health insurance schemes do not provide medicines coverage.
6.2 Patients Fees and Copayments
Co-payments or fees for consultations are levied at the point of delivery.
Furthermore, there are copayments or fee requirements imposed for medicines.
There is a prescription fee for all reimbursable medicines of HRK 10 (US$ 2) per
prescription. Revenue from fees or from the sale of medicines is not used to pay
the salaries or supplement the income of public health personnel in the same
facility44.
6.3 Pricing Regulation for the Private Sectorviii
In Croatia, there are legal or regulatory provisions affecting pricing of medicines.
These provisions are aimed at the level of wholesalers and retailers; the
maximum wholesale mark-up is 8.5%. There is no retail mark-up for medicines
on the lists of the Croatian Institute for Health Insurance. The government runs
an active national medicines price monitoring system for retail prices.
Regulations exist mandating that retail medicine price information should be
publicly accessible. This information can be found on the internet and in the
Official Gazette4343.
6.4 Prices, Availability and Affordability of Key Medicines
It is unknown if an WHO/HAI pricing survey has been conducted in Croatia
viii This section does not include information pertaining to the non-profit voluntary sector

28
6.5 Price Components and Affordability
In 2009, a survey on medicine price components was conducted in Croatia. The
median cumulative percentage mark-up between the Manufacturer Selling Price
(MSP)/Cost Insurance and Freight (CIF) price and final medicine price for a
basket of key medicines was 8.5% in the public sector and 8.5+35% in the
private sector43.
6.6 Duties and Taxes on Pharmaceuticals (Market)
Croatia imposes duties on imported active pharmaceutical ingredients (APIs) and
duties on imported finished products are also imposed. Value-added tax (VAT) or
other taxes are not imposed on finished pharmaceutical products which are on
the positive lists. However there is a 23% VAT imposed on medicines which are
not included in the lists.45
29
Section 7 - Pharmaceutical procurement and distribution in the
public sector
This section provides a short overview on the procurement and distribution of
pharmaceuticals in the public sector of Croatia.
7.1 Public Sector Procurement
Public sector procurement in Croatia is decentralized and for hospitals only.
Public sector request for tender documents and tender awards are publicly
available. Procurement is based on the prequalification of suppliers, there needs
to be a bank transfer confirmation and a bank guarantee46.
There is a written public sector procurement policy. Legal provisions do not exist
that give priority to locally produced goods in public procurement46.
The key functions of the procurement unit and those of the tender committee are
clearly separated47.
A process exists to ensure the quality of products that are publicly procured. The
quality assurance process includes the pre-qualification of products and suppliers.
A list of pre-qualified suppliers and products is available20. A list of samples
tested during the procurement process and the results of quality testing is not
available. The tender methods employed in public sector procurement include,
international competitive tenders and direct purchasing46.
7.2 Public Sector Distribution
The government supply system department in Croatia does not have a Central
Medical Store at National Level and there are no public warehouses in the
secondary tier of the public sector distribution.
7.3 Private Sector Distribution
Legal provisions exist for licensing wholesalers and distributors in the private
sector20. There are national guidelines on Good Distribution Practices (GDP). A
licensing authority that issues GDP licenses exists2020. A list of GDP certified
wholesalers and distributors exists in the private sector48.
30
Section 8 - Selection and rational use of medicines
This section outlines the structures and policies governing the selection of
essential medicines and promotion of rational drug in Croatia.
8.1 National Structures
A National Essential Medicines List (EML) exists. The EML was lastly updated in
2011 and is publicly available. There are currently 770 medicines on the EML.
Selection of medicines for the EML is undertaken through a written process. A
mechanism aligning the EML with the Standard Treatment Guidelines (STGs) is
in place42.
National Standard Treatment Guidelines (STGs) for the most common illnesses
are produced and endorsed by the professional societies of the Croatian Medical
Association. There are STGs for the most common illnesses that cover primary
care (updated in 2011), secondary care (updated in 2011) and paediatric
conditions (updated in 2011). These are issued by the Croatian Institute for
Health Insurance and they are published in the reimbursement lists. All public
health facilities have a copy of the EML and the STGs4242.
Public education campaigns on rational medicine use topics have been
conducted in the last few years.
There is a national programme or committee, involving government, civil society,
and professional bodies, to monitor and promote rational use of medicines46.
A written National Strategy for containing antimicrobial resistance exists49.
Croatia’s Essential Medicines List (EML) includes formulations specifically for
children. Criteria for the selection of medicines in the EML are explicitly
documented. A national medicines formulary does exist4242.
A funded national intersectoral task force to coordinate the promotion of the
appropriate use of antimicrobials and prevention of the spread of infection exists.
A national reference laboratory or other institution has responsibility for
coordinating epidemiological surveillance of antimicrobial resistance50.
31
8.2 Prescribing
Legal provisions exist to govern the licensing and prescribing practices of
prescribers. Furthermore, legal provisions restricting dispensing by prescribers
exist. Prescribers in the private sector do not dispense medicines44.
There are regulations requiring hospitals to organize/develop Drug and
Therapeutics Committees (DTCs). Where there are requirements for DTCs, more
than half of the hospitals have one51.
The training curriculum for doctors is made up of a number of core components
detailed in Table 1313.
Table 13: Core aspects of the medical training curriculum13
Curriculum Covered
The concept of EML Yes
Use of STGS Yes
Pharmacovigilance Yes
Problem based pharmacotherapy Yes
Mandatory continuing education that includes pharmaceutical issues is required
for doctors and nurses13.
Prescribing by INN name is not obligatory in the public and private sector52.
A professional association code of conduct which governs the professional
behaviour of doctors exists. Similarly a professional association code of conduct
governing the professional behaviour of nurses exists5151.
8.3 Dispensing
Legal provisions in Croatia exist to govern dispensing practices of
pharmaceutical personnel. The basic pharmacist training curriculum includes a
spectrum of components as outlined in Table 1444,5151,5252.
Table 14: Core aspects of the pharmacist training curriculum44,5151,52
Curriculum Covered
32
The concept of EML Yes
Use of STGS Yes
Drug information Yes
Clinical pharmacology Yes
Medicines supply management Yes
Mandatory continuing education that includes rational use of medicines is
required for pharmacists and medical doctors, especially for general practitioners
(GP) 44,5151,52.
Substitution of generic equivalents of the same price or lower than paid by the
national insurance company at the point of dispensing is allowed in public and
private sector facilities. Sometimes antibiotics are sold over-the-counter without a
prescription. Injectable medicines are not sold over-the-counter without a
prescription44,5151,52.
A professional association code of conduct which governs the professional
behaviour of pharmacists exists.
In Croatia prescriptions can only be prescribed by licensed MDs and given away
by licensed pharmacists holding valid work permits.
33
Section 9 - Household data/access
This section provides information derived from past household surveys in Croatia
regarding actual access to medicines by normal and poor households.
In Croatia, of the adult patients with an acute condition in a two-week recall
period, 99% took all medicines prescribed by an authorized prescriber.
Of the adult patients from poor households with an acute condition in a two-week
recall period coming, 91% took all medicines prescribed by an authorized
prescriber,
Of the adult patient population with chronic conditions, 95% took all medicines
prescribed by an authorized prescriber. In comparison, 97% of adult patients with
chronic conditions coming from poor households took all medicines prescribed by
an authorized prescriber.
Of the children from poor households with acute condition in a two-week recall
period, 88% took all medicines prescribed by an authorized prescriber.
34
List of key reference documents:
1 World Health Organization (WHO) (2010), “World Health Statistics 2010”, WHO Press, Geneva. Available
online: http://www.who.int/whosis/whostat/2010/en/index.html.
2 World Health Organization (WHO) (2009), “World Health Statistics 2009”, WHO Press, Geneva. Available
online: http://www.who.int/whosis/whostat/2009/en/index.html.
3 World Health Organization (WHO) (2008), “World Health Statistics 2008”, WHO Press, Geneva
4 World Bank data (2009) 5 World Bank data (2005) 6 Central Bureau of Statistics (CBS) (2009)
7 Croatian National Institute of Public Health (CNIPH) (2009) 8 World Health Organization (WHO) (2004), “World Health Statistics 2004”, WHO Press, Geneva 9 National Health Accounts data (2008) 10 Calculated based on data provided in [3,9] 11 Croatian Institute for Health Insurance (HZZO) (2008) 12 Croatian Chamber of Pharmacists (2011) 13 Ministry of Health and Social Welfare, unpublished data (2011) 14 Ministry of Health and Social Welfare, NACIONALNU STRATEGIJU RAZVITKA ZDRAVSTVA
2006-2011 (2011)
Available online: http://www.nhs.hr/download/Nacionalna_strategija_razvitka_zdravstva_2006_-
_2011.pdf, accessed at June 2011 15 Ministry of Health and Social Welfare (2006)
16 World Trade Organization (WTO) (2000) 17 Official Journal (2004)
Available online: http://www.nn.hr, accessed at June 2011
18 Official Journal (2000)
Available online: http://www.nn.hr, accessed at June 2011 19 Halmed, unpublished data (2011) 20 Act on Medicinal Products Official Gazette 71/07 (2007); 45/09( 2009)
Available online: http://www.halmed.hr/upl/zakoni/zakoni_5_en.pdf, accessed at June 2011
Act on Amendments to the Medicinal Products Act, Official Gazette 45/09 (2009)
Available online: http://www.halmed.hr/upl/zakoni/zakoni_1_10_en.pdf, accesed at June 2011
21 Act on Medical Devices Official Gazette 67/08( 2008) 22 World Health Organization (2009) 23 Halmed website (2007)
35
Available online: http://www.halmed.hr/?ln=en&w=usluge, accessed at June 2011 24 Halmed website (2011)
Available online: http://www.halmed.hr/?ln=en&w=lijekovi, accessed at June 2011
25 Ordinance on the Procedure and Method for Granting Marketing Authorisations for Medicinal
Products, Official Gazette No. 113/08 (2007)
Available online: http://www.halmed.hr/upl/zakoni/zakoni_29_en.pdf, accessed at June 2011
Ordinance on Amendments to the Ordinance on the Procedure and Method for Granting
Marketing Authorisations fom Medicinal products Official Gazette No. 155/09 (2009)
http://narodne-novine.nn.hr/clanci/sluzbeni/2009_12_155_3831.html
26 Ordinance on conditions and procedure of determining GMP compliance, issuing a
manufacturing license and GMP certificate, Official Gazette 74/09 (2009)
Available online: http://narodne-novine.nn.hr/clanci/sluzbeni/2009_06_74_1774.html accessed at
June 2011 27 Ministry of Health and Social Welfare website (2009)
Available online: http://www.mzss.hr/hr/zdravstvo_i_socijalna_skrb/zdravstvo/lijekovi, accessed at
June 2011
28 Ordinance on good practice in wholesale distribution of medicinal products, Official Gazette
29/05 (2005)
Available online: http://narodne-novine.nn.hr/clanci/sluzbeni/288028.html, accessed at June 2011
29 Ordinance on the conditions and the procedure of obtaining the for the wholesale distribution of
medicinal products and the import and export of medicinal products, Official Gazette 29/05 (2005)
Available online: http://narodne-novine.nn.hr/clanci/sluzbeni/288031.html, accessed at June 2011
30 Ordinance on quality control of medicinal products, Official Gazette 56/05 (2005)
Available online: http://narodne-novine.nn.hr/clanci/sluzbeni/288592.html, accessed at June 2011
31 Ordinance on advertising and information sharing on medicinal products, Official Gazette
118/09 (2009)
Available online: http://narodne-novine.nn.hr/clanci/sluzbeni/2009_09_118_2913.html, acessed at
June 2011
Ordinance of Amendments to the Ordinance on advertising and information sharing on medicinal
products, Official Gazette 140/09 (2009)
http://narodne-novine.nn.hr/clanci/sluzbeni/2009_11_140_3429.html 32 CARPC Code of Conduct (1994)
Available online: http://www.carpc.hr/download/22-document.pdf, accessed at June 2011
36
33 Ministry of Health and social Welfare,, Ordinance on Good Manufacturing Practice ( GMP)
Official Gazette 74/09 ( 2009.) 34 Ministry of Health and social Welfare, (2007) Ordinance on Clinical Trials and Good Clinical
Practice, Official Gazette 14/10, 127/10 ( 2010.)
35 International Narcotics Control Board (1993)
36 International Narcotics Control Board (2009) 37 Halmed (2009) 38 ORDINANCE ON PHARMACOVIGILANCE (2007)
Available online: http://www.halmed.hr/upl/zakoni/zakoni_37_en.pdf, accessed at June 2011 39 Halmed website (2011)
Available online: http://www.halmed.hr/pdf/o_agenciji/Organigram-09072010-en.pdf, accessed at
June 2011 40 Halmed website, standardized forms for ADRs (2009)
Available online:
• http://www.halmed.hr/pdf/farmakovigilancija/Obrazac_1-
Obrazac_za_prijavu_nuspojava_lijekova-zdravstveni_radnici.pdf;
• http://www.halmed.hr/pdf/farmakovigilancija/Obrazac_2-
Obrazac_za_prijavu_nuspojava_cjepiva.pdf;
• http://www.halmed.hr/pdf/farmakovigilancija/Obrazac_3-
Pacijenti_nuspojava_lijekovi_ozujak-2010_finalno.pdf; accessed at June 2011 41 VigiFlow, unpublished data (2011)
42 Ordinance on Establishing the criteria for inclusion of medicines in the basic and the
supplementary reimbursement list of the Croatia Institute for Health Insurance (2009)
Available online: http://narodne-novine.nn.hr/clanci/sluzbeni/2009_12_155_3831.html, accessed
at June 2011 43 Ordinance on Establishing the criteria for wholesale pricing of medicines and the method for
reporting wholesale prices (2009)
Available online: http://narodne-novine.nn.hr/clanci/sluzbeni/2009_12_155_3832.html, accessed
at June 2011 44 Compulsory Health Insurance Act (2011)
Available online: http://narodne-novine.nn.hr/clanci/sluzbeni/2011_04_49_1097.html, accessed at
June 2011 45 Ministry of Finance, unpublished data (2011)
46 Croatian Institute for Health Insurance, unpublished data (2011)
37
47 World Health Organization (WHO ), WHO Level 1 Survey, Geneva (2007)
48 Halmed website, list of certified wholesalers and distributors (2011)
Available online: http://www.halmed.hr/?ln=en&w=promet_lijekova, accessed at June 2011 49 Intersectoral Coordination Mechanism for the Control of Antimicrobial Resistance (ISKRA)
Available online: http://iskra.bfm.hr/eng/, accessed at June 2011
50 Croatian National Institute of Public Health
Available online: http://www.hzjz.hr/epocetna.htm, accessed at June 2011
51 Act of Health Care, Official Gazette 150/08, 155/09, 71/10, 139/10 & 22/11 (2009)
52 Ordinance on establishing for classification of medicines and prescribing and dispensing of
prescription, Official Gazette 82/10 (2010).





























