Embed Size (px)
Citation preview

Pharmacodynamic Measurements ofImmunosuppression in Healthy IndividualsA Comparison of the Tuberculin Skin Test and Tuberculin-StimulatedLymphocyte Proliferation in Whole Blood
Dave Singh,1 Ashley Woodcock1 and George Booth2
1 Medicines Evaluation Unit, North West Lung Research Centre, Wythenshawe, Manchester, UK2 Clinical Pharmacology and Respiratory and Inflammation Research Area, AstraZeneca, Alderley Park, Macclesfield, UK
Abstract Objectives: Studies of novel immunosuppressive agents using small numbers of healthy volunteers requirevalidated methods for detecting pharmacodynamic effects. We investigated the ability of tuberculin-stimulatedlymphocyte proliferation in whole blood and the tuberculin skin test to assess immunosuppression in healthyvolunteers.
Methods: This was a parallel-group, placebo-controlled study. Five weeks after a tuberculin test, 14 studyparticipants received either placebo or prednisolone (30mg or 60mg) once daily for 7 days. Blood samples werecollected before the first dose and at 2 hours post-first dose for assessment of lymphocyte proliferation. On day5, a repeat skin test was administered.
Results: Lymphocyte proliferation was reduced in all ten study participants who received prednisolone (meanreduction: 30mg = 77.5%, 60mg = 77%; p < 0.01 compared with placebo) with no reduction in any of the placebogroup. While prednisolone reduced skin test size in seven study participants, there was an increase in threeparticipants and no overall significant effect compared with placebo (p > 0.05).
Conclusion: Lymphocyte proliferation in whole blood was able to detect pharmacological immunosuppressionin healthy individuals, while the tuberculin skin test did not. This whole blood method may have applicationsfor detecting the effects of novel compounds in future healthy volunteer studies.
ORIGINAL RESEARCH ARTICLE Int J Pharm Med 2003; 17 (3-4): 131-1361364-9027/03/0003-0131/$30.00/0
© Adis Data Information BV 2003. All rights reserved.
Phase 1 studies of novel therapeutic agents in healthy volun-
teers usually assess safety and tolerance, and pharmacokinetics.
Pharmacodynamic models can also be used in these studies toassess the effects of the drug. The assessment of pharmacological
activity in Phase 1 studies can provide information that can be
used to design later phase patient studies, e.g. choice of dose in
Phase 2 studies.
Immunosuppressive drugs may cause adverse effects in
healthy volunteers. Consequently, Phase 1 studies using these
agents are usually of short duration and involve small sample
sizes, so that the drug can be assessed without exposing unneces-sary numbers of volunteers to potential adverse effects. Pharmaco-
dynamic methods that are used in such studies, therefore, need to
be able to detect drug effects in small sample sizes.
The injection of tuberculin purified protein derivative (PPD)
into the skin causes a delayed-type hypersensitivity reaction.[1,2]
This skin reaction has been used in placebo-controlled studies toinvestigate the immunomodulatory effects of drugs in healthy
individuals; cimetidine and evening primrose oil increase tuber-
culin reaction size,[3,4] while ranitidine has no effect.[5] However,
there have been no studies in healthy individuals investigating
the inhibition of the tuberculin skin test by an immunosuppres-
sive agent. Consequently, the potential usefulness of the tubercu-
lin skin test as a pharmacodynamic model in Phase 1 studies of
novel immunosuppressive agents is not known.Glucocorticoids are commonly-used immunosuppressive
drugs, with many of their effects mediated through inhibition of
lymphocyte and macrophage activity.[6] Skin delayed-type hy-

persensitivity is characterised by an increase in the number oflymphocytes and macrophages.[1,2] Thus, glucocorticoids wouldbe expected to inhibit the development of the tuberculin skinreaction.
Isolated peripheral blood mononuclear cells are often usedto assess immune function in vitro. However, the separation pro-cedure can be time consuming and can lead to the loss of essentialinhibitory or stimulatory factors and the pre-activation of cells.[7-9]
Whole blood cell culture methods are not affected by these prob-lems as there is no separation procedure. These methods havebeen used to study the immunosuppressive effects of drugs ex-vivo after administration to healthy individuals as the concentra-tion of drug in culture is not affected by the separation proce-dure.[10-13] We have previously shown that tuberculin causes Tlymphocyte proliferation in whole blood that is dependent on: (i)major histocompatibility complex class II signalling via the T-cell receptor; (ii) co-stimulation; and (iii) the actions of interleu-kin (IL)-2.[14] Novel immunosuppressive drugs are currently be-ing developed that interfere with antigen-induced T-cell activationthrough these molecular mechanisms.[15,16] Tuberculin-stimu-lated lymphocyte proliferation in whole blood may, therefore, bean appropriate method for assessing pharmacological immuno-suppression in humans. This whole blood cell culture method hasbeen used to assess the effects of immunosuppressive drugs invitro.[14] However, to our knowledge, tuberculin-stimulated lym-phocyte proliferation in whole blood has not been used for inves-tigating the effects of immunosuppressive drugs ex-vivo after oraladministration in healthy individuals.
The aim of the current study was to assess the ability of thetuberculin skin test and tuberculin-stimulated lymphocyte prolif-eration in whole blood to measure the immunosuppressive activ-ity of the glucocorticoid prednisolone in a placebo-controlled,healthy-volunteer study. This study was purposefully designedwith a small sample size to assess these methods using a similarstudy design to those commonly used in Phase 1 studies of novelimmunosuppressive agents.
Methods
Study Participants
Healthy males (i.e. without any significant medical condi-tions and taking no medications) participated in this study, whichwas approved by the independent local research ethics commit-tee. Written informed consent was obtained from all participants.A screening tuberculin skin test was initially performed in orderto identify individuals with delayed-type hypersensitivity to tu-berculin; 29 study participants were administered a 10-unit test
into the volar aspect of the forearm using the Mantoux technique.10 units PPD-Weybridge (Evans Medical, Leatherhead, UK) wasused; this is bioequivalent to 10 tuberculin units PPDS (an inter-national standard PPD).[17] All tests were administered between9 and 11am either by a physician with considerable experienceusing the method or by a nurse who had been trained by thephysician. Fifteen study participants (aged 19–50 years, mean 35years) who developed >5mm induration after 48–72 hours wererecruited into the study. These individuals were all EuropeanCaucasians (14 were born in the UK and one in Spain). Thirteenstudy participants had a history of Bacille Calmette-Guérin(BCG) vaccination, and three participants were current smokers.
Study Design
This was a parallel-group, double-blind, placebo-controlledstudy (see table I), conducted in the Clinical Pharmacology Unitat AstraZeneca Pharmaceuticals (Alderley Edge). Five weeks af-ter the screening tuberculin test (Test 1), the 15 study participantswere randomised to receive either placebo, prednisolone 30mgor prednisolone 60mg once daily for 7 days. Study participantswere required to attend the Clinical Pharmacology Unit each dayso that the study medication could be administered under directsupervision between 8 and 9am, thus ensuring compliance. Onday 5, a repeat 10 tuberculin unit test (test 2) was administeredimmediately after dosing. This was read at 48 and 72 hours post-injection by the same observer who measured test 1. Blood sam-ples were collected before the first dose (on day 1), and at 2 hourspost-dose (the known time to reach maximum concentration fol-lowing drug administration [tmax] for prednisolone[18]).
Tuberculin-Induced Lymphocyte ProliferationBlood samples were collected into plastic tubes containing
10 units/mL sodium heparin and stimulated with tuberculin usingthe method we have previously described;[14] briefly, blood wasdiluted 1 : 5 using supplemented Rosewell Park Memorial Ins-titute (RPMI) 1640 medium and incubated with tuberculin PPD(1000 units/mL) for 96 hours. Diluted whole blood incubatedwithout tuberculin (i.e. with RPMI 1640 medium alone) was usedfor control values. To assess proliferation, 1 μCi/well of tritiated
Table I. Study design
Day
1 2–4 5 6 7 8
Blood samples •Treatment dose • • • • •Tuberculin injection •Read tuberculin test • •
132 Singh et al.
© Adis Data Information BV 2003. All rights reserved. Int J Pharm Med 2003; 17 (3-4)

thymidine was added for the final 24 hours. The cultures werethen harvested on to glass fibre filters and radioactivity assessedby liquid scintillation counting. The results were expressed as a‘stimulation index’:
Stimulation index = counts per minute + tuberculin/countsper minute in controls.
Lymphocyte CountsBlood collected into ethylene diamine tetra-acetic acid tubes
was analysed for lymphocyte counts using an automated Coultercounter.
Plasma Prednisolone LevelsHeparinised whole blood samples were centrifuged for 10
minutes at 1000G. The resulting plasma samples were transferredto polypropylene tubes and frozen immediately at –70°C for lateranalysis. Prednisolone pharmacokinetics were determined usingliquid-liquid extraction of prednisolone and the internal standardmethylprednisolone, and detection by high performance liquidchromatography. This method had a lower limit of quantitationof 10 μg/L. The intra- and inter-day variabilities of the methodwere below 4.9% and 10.1%, respectively. Absolute recovery ofprednisolone was 64.8%, and of the internal standard, 69.3%.
Statistical Methods
Power calculations were based on a preliminary study inwhich 12 healthy male study participants were administered a10-unit tuberculin test into the volar aspect of the forearm, andthe reaction measured at 48 and 72 hours. This was repeated 6weeks later using the other forearm. There was a significant in-crease in the size of induration after repeat testing at 48 hours(mean difference 7.1mm, 95% confidence interval [CI] 3.6–10.6mm, p = 0.002). At 72 hours, the increase in size did not reachthe level of statistical significance (mean difference 2.7mm, 95%CI 0.1–5.3mm, p = 0.07). Power calculations using an analysisof covariance (ANCOVA) model estimated that a sample size offive study participants per group would allow 90% power to de-tect 50% inhibition of the tuberculin skin reaction caused by pre-dnisolone compared with placebo, while four study participantsper group would allow 88% power to detect 55% reduction ininduration size.
The effects of prednisolone compared with placebo using thewhole blood proliferation assay and tuberculin skin testing wereanalysed using ANCOVA. Pearson’s correlation coefficient wasused to assess the relationship between changes in lymphocyteproliferation and: (i) lymphocyte counts; and (ii) skin test reac-tion size.
Results
Although 15 study participants were randomised into thisstudy, one participant was withdrawn prior to commencementdue to an acute illness. This participant had been randomised intothe placebo group, leaving four participants in this group.
Tuberculin-Induced Lymphocyte Proliferation
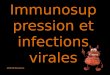
Tuberculin-induced lymphocyte proliferation was reduced at2 hours in all ten study participants who received prednisolone(figure 1). The mean reduction in proliferation was 77.5% in the
Stim
ulat
ion
inde
x
0
20
40
60
80
100
120
140 Prednisolone 60mg
0
20
40
60
80
100
120
140 Prednisolone 30mg
0
20
40
60
80
100
120
140
Pre-dose 2h post-dose
Placebo
Time
Fig. 1. The effect of prednisolone on tuberculin-induced cell proliferation in whole blood.Individual data shown.
Table II. The effect of prednisolone on tuberculin-stimulated whole bloodlymphocyte proliferationa
Mean at 0h(SD)
Mean at 2h(SD)
Mean differenceb (95% CI)
Placebo 43.7 (33.4) 52.6 (31.7) 8.9 (0.1 to 17.7)
Prednisolone(30mg)
62.0 (53.3) 14.0 (9.9) –48.0 (–90.8 to –5.2)
Prednisolone(60mg)
33.5 (22.1) 7.7 (8.9) –25.8 (–40.8 to –10.8)
a Units are SI.
b Difference = 2h – 0h.
CI = confidence interval; SD = standard deviation.
Measurements of Immunosuppression in Healthy Individuals 133
© Adis Data Information BV 2003. All rights reserved. Int J Pharm Med 2003; 17 (3-4)

group treated with 30mg prednisolone and 77% in the grouptreated with 60mg prednisolone (table II). These changes werestatistically significant compared with placebo (p < 0.01 for com-parisons of both the 30mg and 60mg treatment groups).
At 2 hours post-dose, plasma prednisolone levels weregreater in the participants treated with 60mg (mean [SD]; 639μg/L [124]) than those treated with 30mg (mean [SD]; 414 μg/L[40]). However, there was no correlation between plasma pred-nisolone concentrations and inhibition of proliferation (r = 0.14,p > 0.05). Prednisolone caused a decrease in lymphocyte countsat 2 hours compared with pre-dose (for the ten prednisolone-treated participants, mean [SD]; 0.9 [0.2] versus 1.4 [0.2]109cells/L, respectively) while there was no reduction with pla-cebo (mean [SD]; 1.7 [0.2] versus 1.6 [0.5] 109cells/L, respec-tively). There was no correlation between change in lymphocytecount and inhibition of proliferation (r = –0.34, p > 0.05).
Repeat Tuberculin Testing
The effect of prednisolone on the tuberculin reaction wasvariable (figure 2); while induration in seven of the ten studyparticipants was reduced (with complete inhibition in three par-ticipants), there was an increase of >6mm in three participants.Overall, there was a small mean decrease in induration at test 2in the prednisolone-treated groups at both 48 and 72 hours (table
III). However, these changes were not statistically significantlydifferent from placebo (p > 0.05 for all comparisons of pred-nisolone and placebo groups at both 48 and 72 hours). There wasno correlation between the plasma prednisolone concentrationsand change in tuberculin reaction size in the ten participantstreated with prednisolone (r = –0.27, p > 0.05).
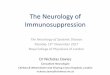
Figure 3 shows that in the three study participants who hadno inhibition of the skin reaction with prednisolone, there wasstill significant inhibition (>50%) of lymphocyte proliferation inwhole blood. There was a significant correlation between inhibi-tion of skin test reaction and lymphocyte proliferation (r = 0.7, p =0.02).
Discussion
In healthy participants, we found that tuberculin-stimulatedlymphocyte proliferation in whole blood was significantly inhib-ited by prednisolone, while the tuberculin skin test was not. Thisdifference was due to the variability of the skin response to pred-nisolone; some participants had complete inhibition of the reac-tion, while others had an increase in reaction size. This contrastswith tuberculin-induced lymphocyte proliferation, which was re-duced in all of the participants treated with prednisolone.
The differences in the inhibitory effects of prednisolone onthe response to tuberculin in whole blood and the skin are prob-ably due to the ‘booster’ effect. This phenomenon, after repeattuberculin skin testing, is well recognised and is thought to bedue to the boosting of diminished cell-mediated immunity.[19]
The booster effect is defined as an increase in the diameter ofinduration of >6mm after a repeat test.[19] The booster effect isknown to vary between population groups, being dependent onprevious mycobacterial and BCG exposure rates. We have pre-
05
1015202530
Baseline test Repeat test
Placebo
Prednisolone 60mg
0
5
10
15
20
25
30
0
5
10
15
20
25
30 Prednisolone 30mg
Indu
ratio
n di
amet
er (
mm
)
Fig. 2. The effect of prednisolone on the tuberculin test. Individual data (mean of 48-and 72-hour readings) shown.
Table III. The effect of prednisolone on repeat tuberculin testsa
Test 1 mean(SD)
Test 2 mean(SD)
Mean differenceb (95% CI)
48hPlacebo 9.1 (3.7) 12.4 (6.9) 3.3 (–5.6 to 12.9)
Prednisolone (30mg) 13.4 (5.1) 9.3 (10.3) –4.1 (–11.9 to 3.7)
Prednisolone (60mg) 14.1 (3.9) 11.1 (11.9) –2.9 (–15.9 to 10.1)
72hPlacebo 11.3 (6.0) 10.2 (7.6) –1.2 (–7.8 to 5.4)
Prednisolone (30mg) 13.2 (5.3) 9.2 (10.9) –3.9 (–11.8 to 4.0)
Prednisolone (60mg) 15.0 (3.6) 12.8 (10.6) –2.2 (–13.1 to 8.7)
a Units are mm.
b Difference = test 2 – test 1.
CI = confidence interval; SD = standard deviation.
134 Singh et al.
© Adis Data Information BV 2003. All rights reserved. Int J Pharm Med 2003; 17 (3-4)

viously shown that boosting does occur in a proportion of studyparticipants in the UK.[20]
In the current study, prednisolone did not inhibit boosting ofthe skin reaction in three study participants. However, wholeblood tuberculin-induced lymphocyte proliferation was inhibitedin these three participants. Thus, these three participants weresensitive to the effects of glucocorticoids, as demonstrated inwhole blood, but the booster effect in the skin overcame thisinhibition. There was a significant correlation between inhibitionof lymphocyte proliferation and delayed-type hypersensitivity,with a trend for participants with resistance to the effects of pred-nisolone in the skin also to have less inhibition of proliferationin whole blood. Further studies with larger sample sizes are re-quired to confirm this observation.
Studies in patients have shown that prednisolone can inhibitthe tuberculin skin test.[21,22] However, there have been no similarstudies using glucocorticoids in healthy individuals. Althoughthe tuberculin test has been used in placebo-controlled healthyvolunteer studies to demonstrate drug effects,[3,4] there are im-portant differences in the design of these studies compared withthe current study: (i) the previous studies were designed to detectan increase in tuberculin reaction size caused by the drug com-pared with placebo, in contrast to inhibition of delayed-type hy-persensitivity in the current study; and (ii) previous studies usedpopulation groups where repeat tuberculin testing caused noboosting. It is possible that prednisolone would have displayedgreater inhibitory effects on repeated tuberculin tests in a groupof individuals who displayed no boosting, but further studies areneeded to confirm this.
‘First time into human’ studies assessing pharmacokineticsand safety often use similar group sizes to the current study, i.e.4–6 study participants per dose group. Pharmacodynamic meth-ods that are used in such studies should, therefore, be able todemonstrate pharmacological effects with these sample sizes. Wedeliberately chose a small sample size for this study so that thetwo pharmacodynamic methods could be assessed under condi-tions similar to a Phase 1 study. Despite the relatively small sam-ple size used in this study, there was adequate statistical powerto detect approximately 50% inhibition of the skin test caused byprednisolone compared with placebo.
Multiple doses of prednisolone were used prior to adminis-tration of a repeated tuberculin skin test as this allowed a greateropportunity for immunosuppressive effects to be observed in theskin when compared with, for example, a single dose. This designis similar to the previous healthy volunteer studies of the effectsof drugs on the tuberculin skin test.[3-5] Therefore, it is unlikelythat the lack of inhibition of the skin reaction in some individualswas due to inadequate length of drug administration.
We chose to assess whole blood tuberculin-induced lympho-cyte proliferation at 2 hours as this is the known tmax for pred-nisolone,[18] this providing the maximal opportunity to observeimmunosuppression. The similar results obtained for the 30mgand 60mg groups at this time-point suggest that inhibition ofproliferation was near maximal, i.e. at the top of the dose re-sponse curve. We have previously shown that this whole-bloodmethod can detect dose-response effects in vitro.[14] It would beinteresting to evaluate the ability of this method to detect dose-response effects ex-vivo after oral administration. This couldhave been achieved in a similar study to ours by using multipleblood sampling over 24 hours to assess proliferation as pred-nisolone concentrations decline. We did not study this in the cur-rent study as our primary aim was to compare the two pharmaco-dynamic methods, and not to assess dose-response relationships.
Prednisolone caused a reduction in lymphocyte counts. Thisis a well-recognised phenomenon.[12,23] We found no correlationbetween the reduction in lymphocyte counts and the magnitudeof inhibition of lymphocyte proliferation. Therefore, it is likelythat the inhibition of mononuclear cell function in whole bloodex-vivo caused by prednisolone was due predominantly to directpharmacological effects rather than reduced cell numbers in cul-ture.
Conclusion
We have shown that tuberculin-stimulated lymphocyte pro-liferation in whole blood can be used to demonstrate the effectsof prednisolone in a healthy volunteer study with a small samplesize, and so may be a useful pharmacodynamic method for futurePhase 1 studies. However, in our study population, the tuberculinskin test was not able to demonstrate glucocorticoid effects usinga small sample size. This finding indicates that further studies
0
20
40
60
80
100
−80 −60 −40 −20 0 20 40 60 80 100
Inhibition of skin test (%)
Inhi
bitio
n of
lym
phoc
yte
prol
ifera
tion
(%)
Fig. 3. Relationship between inhibition of skin test and lymphocyte proliferation in tenindividuals treated with prednisolone (r = 0.7, p = 0.02).
Measurements of Immunosuppression in Healthy Individuals 135
© Adis Data Information BV 2003. All rights reserved. Int J Pharm Med 2003; 17 (3-4)

(e.g. using larger sample sizes or different study populationswhere there is no booster effect) are needed to determine theappropriate use of the tuberculin skin test as a pharmacodynamicmeasurement in Phase 1 studies.
Acknowledgements
This study was funded entirely by AstraZeneca Pharmaceuticals. Duringthe study, Dave Singh’s salary was paid by AstraZeneca, and George Boothis an employee of AstraZeneca.
References1. Gibbs J, Ferguson J, Brown R, et al. Histometric study of the localisation of
lymphocyte subsets and accessory cells in human Mantoux reactions. J ClinPathol 1984; 37: 1227-34
2. Chu C, Field M, Andrew D, et al. Detection of cytokines at the site of tuberculin-induced delayed type hypersensitivity in man. Clin Exp Immunol 1992; 90:522-9
3. Snyman J, Meyer E, Schoeman H. Cimetidine as modulator of the cell-mediatedimmune response in vivo using the tuberculin skin test as parameter. Br J ClinPharmacol 1990; 29: 257-60
4. Dirks J, Van Aswegan C, Du Plessis D, et al. Effect of evening primrose oil onmonocyte chemotactic protein-1 and tumour necrosis factor-alpha levels dur-ing delayed type hypersensitivity immune responses. Med Sci Res 1998; 26:567-9
5. Yap J, Wang Y. The effect of ranitidine on the tuberculin skin test. Int J TubercLung Dis 1998; 2: 344-7
6. Barnes PJ. Molecular mechanisms of corticosteroids in allergic diseases. Allergy2001; 56: 928-36
7. De Groote D, Zangerle P, Gevaert Y, et al. Direct stimulation of cytokines (IL-1β,TNF-α, IFN-γ and GM-CSF) in whole blood: comparison with isolated PBMCstimulation. Cytokine 1992; 4: 239-48
8. Yaqoob P, Newsholme E, Calder P. Comparison of cytokine production in cul-tures of whole human blood and purified mononuclear cells. Cytokine 1999;11: 600-5
9. Kasahara K, Strider R, Chensue S, et al. Mononuclear cell adherence inducesneutrophil chemotactic factor (interleukin-8) gene expression. J LeukocyteBiol 1991; 50: 287-95
10. Bleeker M, Netea M, Kullberg B, et al. The effects of dexamethasone and chlor-promazine on tumour necrosis factor-alpha, interleukin-1β, interleukin-1 re-ceptor antagonist and interleukin-10 in human volunteers. Immunology 1997;91: 548-52
11. Chakraborty A, Blum R, Cutler D, et al. Pharmacoimmunodynamic interactions
of interleukin-10 and prednisolone in healthy volunteers. Clin Pharmacol Ther
1999; 65: 304-18
12. Steer J, Vuong Q, Joyce D. Suppression of human monocyte tumour necrosis
factor-α release by glucocorticoid therapy: relationship to systemic
monocytopaenia and cortisol suppression. Br J Clin Pharmacol 1997; 43: 383-9
13. Stein M, Murray J, Wood A. Inhibition of stimulated interleukin-2 production in
whole blood: a practical measure of cyclosporin effect. Clin Chem 1999; 45:
1477-84
14. Singh SD, Booth CG. Tuberculin-induced lymphocyte proliferation in whole
blood: an antigen specific method for assessing immunosuppressive agents. J
Immunol Methods 2002; 260: 149-56
15. Burastero S, Rossi G. Immunomodulation by interference with co-stimulatory
molecules: therapeutic perspectives in asthma. Thorax 1999; 54: 554-7
16. Denton M, Magee C, Sayegh M. Immunosuppressive strategies in transplantation.
Lancet 1999; 353: 1083-91
17. Seibert F, DuFour E. Comparison between the international standard tuberculins,
PPD-S and old tuberculin. Am Rev Tuberc 1954; 69: 585-94
18. Gambertoglio J, Amend W, Benet L. Pharmacokinetics and bioavailability of
prednisone and prednisolone in healthy volunteers and patients: a review. J
Pharmacokinet Biopharm 1980; 8: 1-31
19. Menzies R. Interpretation of repeated tuberculin tests. Am J Respir Crit Care Med
1999; 159: 15-21
20. Singh D, Sutton C, Woodcock A. Repeat tuberculin testing in BCG-vaccinated
subjects in the United Kingdom: the booster effect varies with the time of
reading. Am J Respir Crit Care Med 2001; 164: 962-4
21. Bovornkitti S, Kangsadal P, Sathirapat P, et al. Reversion and reconversion rate
of tuberculin skin reactions in correlation with the use of prednisolone. Dis
Chest 1960; 38: 51-5
22. Sousa A, Lane S, Atkinson B, et al. The effects of prednisolone on the cutaneous
tuberculin response in patients with corticosteroid-resistant bronchial asthma.
J Allergy Clin Immunol 1996; 97: 698-706
23. Pountain G, Keogan M, Hazleman B, et al. Effects of single dose compared with
three days prednisolone treatment of healthy volunteers: contrasting effects on
circulating lymphocyte subsets. Clin Pathol 1993; 46: 1089-92
Correspondence and offprints: Dr Dave Singh, Medicines Evaluation Unit,North West Lung Research Centre, South Manchester University HospitalsTrust, Southmoor Road, Wythenshawe, Manchester, M23 9LT, UK.E-mail: [email protected]
136 Singh et al.
© Adis Data Information BV 2003. All rights reserved. Int J Pharm Med 2003; 17 (3-4)